
Abstract
Objective
This longitudinal study investigated the pathways from childhood socioemotional characteristics and cognitive skills to health behaviours in midlife. Methods: Participants in the Jyväskylä Longitudinal Study of Personality and Social Development (JYLS) were followed from age 8 (n = 369) to age 50 (n = 271). Outcomes included physical activity, smoking, alcohol consumption and body mass index (BMI) assessed at ages 36, 42 and 50. Predictors were socioemotional characteristics (behavioural activity, negative emotionality, and well-controlled behaviour) and parents’ occupational status collected at age 8, cognitive skills (school success at age 14 and the highest education at age 27) and adulthood personality traits (extraversion, neuroticism and conscientiousness). Longitudinal path modelling was used for analyses. Results: Well-controlled behaviour and extraversion predicted physical activity in women. Behavioural activity predicted alcohol consumption in women and smoking in men. Negative emotionality was not directly connected to health behaviours. Adulthood neuroticism was associated with smoking in men and with alcohol-related problems in both men and women. There were some indirect paths from childhood socioemotional characteristics to midlife health behaviours through cognitive skills. None of the study variables predicted midlife BMI. Conclusions: Childhood socioemotional characteristics have some predictive value on midlife health behaviours, both directly and through cognitive skills.
Supplemental data for this article is available online at https://doi.org/10.1080/08870446.2022.2041639 .
Introduction
Midlife health behaviours are important predictors of later life health and functional capacity (Artaud et al., Citation2016; Sabia et al., Citation2014). Previous research suggests that individual differences in personality are linked to various health behaviours in adulthood (e.g. Turiano et al., Citation2018), partly through educational attainment (Hampson et al., Citation2015). Even though personality and educational attainment interlink during life, these two factors are rarely studied together beyond childhood and in relation to adult health behaviours. Using data from the ongoing Finnish Jyväskylä Longitudinal Study of Personality and Social Development (JYLS) (Pulkkinen, Citation2017), collected at several points over a 42-year period, we examined the trajectories of childhood and early adulthood socioemotional characteristics and cognitive skills to measures of health behaviours in early middle age – namely, physical activity, smoking, alcohol use and body mass index (BMI).
Individual differences in behaviour and reaction styles are already apparent in small children. We use the term socioemotional characteristics to refer to ‘the integral role of emotions and emotion regulation in the process of socialization, involving the interaction of an individual’s innate endowments and external influences’ (Pulkkinen et al., Citation2012, p. 1283). These childhood characteristics form a basis for the development of personality traits later in life (Caspi, Citation2000), which are fivefold: neuroticism, extraversion, conscientiousness, openness (to experience) and agreeableness (McCrae & Costa, Citation2003). In this study, we focused on three childhood socioemotional characteristics, defined within a two-dimensional model of self-regulation (Pulkkinen, Citation2017, p. 50): behavioural activity (representing the dimension for activity vs. passivity) and well-controlled behaviour and negative emotionality (representing the opposite poles of the dimension for high vs. low self-regulation). In adulthood, their closest conceptual counterparts are extraversion, conscientiousness and neuroticism, respectively (Pulkkinen et al., Citation2012). These personality characteristics, particularly behavioural activity/extraversion and well-controlled behaviour/conscientiousness, have shown some continuity from childhood to adulthood (Caspi, Citation2000; Hampson & Goldberg, Citation2006; McCrae et al., Citation2000; Pulkkinen et al., Citation2012).
Children who score high in negative emotionality tend more towards aggressive or anxious reactions in new or stressful events (Pulkkinen et al., Citation2012). Childhood negative emotionality and related traits (e.g. neuroticism) are linked to increased BMI (Pulkki-Råback et al., Citation2005) and alcohol consumption in adulthood (Hampson et al., Citation2006; Pitkänen et al., Citation2008). Aggressive behaviour in childhood was found to associate with smoking and, among men, with heavier alcohol consumption in young adulthood (Pulkkinen, Citation1983). Childhood neuroticism seems to be unrelated to adulthood physical activity and smoking (Hampson et al., Citation2007), but adulthood neuroticism has been found to associate with a number of unhealthy behaviours, such as smoking (Malouff et al., Citation2006; Terracciano & Costa, Citation2004), heavy alcohol consumption (Malouff et al., Citation2007), inactivity (Kekäläinen et al., Citation2020; Sutin et al., Citation2016; Wilson & Dishman, Citation2015) and obesity (Gerlach et al., Citation2015; Sutin et al., Citation2011).
Children who score high in well-controlled behaviour tend more towards constructive or compliant behaviour in conflict situations (Pulkkinen et al., Citation2012). These kinds of self-discipline and impulse control can be important characteristics when developing healthy habits (Hampson et al., Citation2016). Childhood well-controlled behaviour and conscientiousness have been consistently linked to health-promoting behaviours in adulthood (Hampson et al., Citation2006, Citation2015, Citation2016; Pitkänen et al., Citation2008; Pluess & Bartley, Citation2015; Tucker et al., Citation1995). The association of childhood conscientiousness with adulthood health behaviours remained even when adulthood conscientiousness was taken into account (Hampson et al., Citation2015; Pluess & Bartley, Citation2015). In adulthood, conscientiousness seems to be the most important personality trait in relation to health and health behaviours, as it has been found to consistently associate with physical activity, non-smoking, healthy BMI and responsible alcohol consumption (Bogg & Roberts, Citation2004; Friedman et al., Citation1995; Hakulinen et al., Citation2015; Jokela et al., Citation2013; Malouff et al., Citation2006, Citation2007; Terracciano & Costa, Citation2004; Wilson & Dishman, Citation2015).
While negative emotionality and neuroticism are linked to health-damaging behaviour, and the opposite is the case for well-controlled behaviour and conscientiousness, behavioural activity and extraversion may predict both health-damaging and health-promoting behaviours. Behavioural activity relates to energetic behaviour and frequent contact with others (Pulkkinen et al., Citation2012). Studies have consistently found a positive link between physical activity and being extraverted or energetic in childhood (Hampson et al., Citation2007; Kern et al., Citation2010; Tucker et al., Citation1995) as well as in adulthood (Karvonen et al., Citation2020; Sutin et al., Citation2016; Wilson & Dishman, Citation2015). However, the enjoyment of social situations may also increase the likelihood of using alcohol in adulthood, and both childhood behavioural activity (Pitkänen et al., Citation2008; Tucker et al., Citation1995) and adulthood extraversion (Hakulinen et al., Citation2015) have been associated with heavy alcohol use.
The mechanisms underlying the associations between childhood personality and adulthood health behaviours may be related to socioeconomic status (SES), particularly education. Conscientiousness especially was found to positively associate with later education (Judge et al., Citation1999), and the role of conscientiousness on health behaviours and health was found to be partly mediated by higher educational attainment (Hampson et al., Citation2015). Higher education, usually completed by early adulthood, provides wide-ranging occupational prospects as well as opportunities for increased income and wealth (Matthews & Gallo, Citation2011). It is also an accurate measure for individuals outside the labour force (Matthews & Gallo, Citation2011). Knowledge related to health can be received through education (Adler & Newman, Citation2002), and it can help in developing cognitive skills (i.e. decision-making) that may explain lifestyle choices (Baker et al., Citation2011). In general, higher education is associated with better health and health behaviours (Davies et al., Citation2018), such as non-smoking and a lower risk of obesity (Cheng et al., Citation2020; Cohen et al., Citation2013; Gilman et al., Citation2003). Previous research has found opposing associations between education and occupational physical activity (negative) and leisure-time physical activity (positive) (Beenackers et al., Citation2012). The relationship between education and alcohol use is more complex, as previous studies suggest that higher education is associated with more frequent alcohol consumption but less frequent binge drinking (Collins, Citation2016; Rosoff et al., Citation2021).
In addition to the associations between adulthood education and health behaviours, SES and adult health behaviours are also interlinked over the long run. Higher parental SES early in life has been associated with more frequent participation in leisure-time physical activity (Elhakeem et al., Citation2015; Juneau et al., Citation2015), and with a decreased risk of smoking (Puolakka et al., 2018; Tian et al., Citation2019), obesity (Tamayo et al., Citation2010), and alcohol-related problems (Barr et al., Citation2018; Pitkänen et al., Citation2008) in later adulthood. The relationship between parental SES and adult health behaviours seems to be partially mediated by the individual’s own education (Elhakeem et al., Citation2015; Puolakka et al., 2018; Tian et al., Citation2019). For example, the individual´s school success in adolescence is a stronger predictor of lower adulthood drinking behaviour (Pitkänen et al., Citation2008), and the individual’s own education and social class are stronger predictors of lower midlife smoking (Cheng & Furnham, Citation2016) than parental SES. Moreover, parental SES has been associated with their children’s personality development: in adulthood, compared with the children of less-educated parents, the children of more highly educated parents score higher in the personality traits of openness and extraversion and lower in neuroticism (Jonassaint et al., Citation2011; Sutin et al., Citation2017).
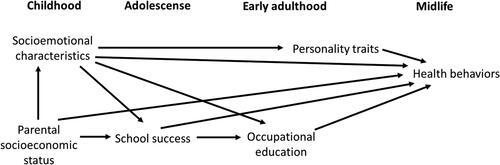
These complex relationships between childhood personality characteristics, cognitive skills, and adulthood health behaviours are rarely studied together. The purpose of this study was to examine longitudinal paths from childhood socioemotional characteristics and cognitive skills to midlife health behaviours (). Because we aimed to study the simultaneous associations of all study variables with midlife health behaviours, we analysed paths from all childhood socioemotional characteristics, parental SES, cognitive skills and adulthood personality traits to midlife health behaviours. We assumed that child socioemotional characteristics are linked to midlife health behaviours through adulthood personality traits. We further expected that parental SES is associated with midlife health behaviours via one’s own adolescent and adulthood academic achievements. Finally, we hypothesised that child socioemotional characteristics contribute to educational achievement, which in turn is related to health behaviours.
Figure 1. The study framework.
Methods
Participants
The data were drawn from the ongoing JYLS, which began in 1968 (Pulkkinen, Citation2017). Twelve complete classes of second graders (N = 369, 196 boys and 173 girls) were randomly selected from the Jyväskylä area in Central Finland. Most of the participants were born in 1959 and were an average of 8 years old. The present analyses utilised five data collection waves, conducted at the age of 14 in 1974 (retention rate 96%), 27 in 1986 (87%), 36 in 1995 (85%), 42 in 2001 (77%) and 50 in 2009 (73%) (Pulkkinen, Citation2017, p. 18). Sixty percent (n = 222) of the initial sample have participated in all six data collections from age 8 to age 50, and at least some information from childhood to adulthood is available for 95% of the participants (Metsäpelto et al., Citation2010; Pulkkinen, Citation2017, pp. 19–20).
During the data collection waves in childhood, the school authorities approved the data collection. In adulthood, the participants themselves provided the consent. At ages 8 and 14, the main data collection methods were teacher ratings and peer nominations. From age 27 onwards, the main data collection methods were questionnaires and personal interviews. At ages 42 and 50, medical examinations were also conducted, and the Ethical Committee of the Central Finland Health District approved the data collection. For further information on each of the data collection waves, see Pulkkinen (Citation2017). The data and documentation related to the variables are stored in the Finnish Social Science Data Archive (FSD).
Measures
Socioemotional characteristics in childhood, behavioural activity, well-controlled behaviour, and negative emotionality (Pulkkinen et al., Citation2012) were assessed at age 8. The teacher rated each pupil for different items on a scale from 0 (never observed the characteristic in question in the pupil) to 3 (the characteristic in question is very prominent in the pupil) in relation to children of the same age and sex, and the mean scores for each socioemotional characteristic were computed. Behavioural activity was assessed by three items (e.g. ‘always busy and plays eagerly with other children’ and ‘always silent and does not care to be busy’). Well-controlled behaviour was assessed by four items designed to measure constructiveness, representing actively coping with a problem (‘tries to act reasonably’), positive thinking and active confrontations (‘thinks that if one negotiates, everything will be better’), considering others with helpfulness and empathy (‘sides with smaller and weaker peers’), and reliability (‘is considered a reliable classmate’); three items measured compliance, representing suppression of negative emotions (‘never quarrels with others’), regulating emotions with compensatory activities (‘dislikes squabbling company and leaves it for something else’) and prudence (‘is peaceable and patient’); and one item measured emotional stability (‘always tries to be friendly to others’) (Pulkkinen, Citation2017, p. 24). Negative emotionality was assessed by eight items measuring aggressiveness (e.g. ‘hurts another child when angry’); three items measured anxiety (e.g. ‘cries easily’); and five items measured low self-control (e.g. ‘is inattentive and lacks concentration in his or her work’) (Pulkkinen et al., Citation2012). Cronbach’s alphas (α) were 0.77 for behavioural activity, 0.91 for well-controlled behaviour and 0.8 for negative emotionality.
Personality traits in adulthood were assessed at age 33, in 1992, when the NEO Personality Inventory (Costa & McCrae, Citation1985) was standardised in the non-Indo-European languages. The test is an authorised adaptation of the NEO-PI, in which about one-quarter (181) of the items were substitutes for the original American items (Pulver et al., Citation1995). The participants were asked to rate whether they agreed with the items on a 5-point response scale, ranging from 0 = strongly disagree to 4 = strongly agree. Mean scores were calculated for all five traits, of which neuroticism (48 items, α = 0.92), extraversion (48 items, α = 0.88) and conscientiousness (18 items, α = 0.82) were used in this study.
Cognitive skills were estimated from school success and occupational education. School success at age 14 was indicated by the GPA (grade point average) of all subjects evaluated by teachers on the scale from 4 = very poor to 10 = excellent, collected from school archives (Pitkänen et al., Citation2008). Occupational education was evaluated on the basis of the highest occupational educational attainment at age 27. It was categorised as 1 = no occupational education or short courses only, 2 = vocational school, 3 = vocational college or polytechnic and 4 = university degree (Kokko et al., Citation2003).
Parents’ occupational status when participants were 8 years old was obtained from the teachers and coded, based on the father’s (or mother’s, if the sole provider) occupation, as 1 = blue-collar, 2 = lower white-collar and 3 = upper white-collar (Pitkänen et al., Citation2005). For further analysis, two dummy coded variables were produced: medium vs. other (1 = lower white-collar, 0 = blue- or upper white-collar) and high vs. other (1 = upper white-collar and 0 = blue- or lower white-collar).
Health behaviours
Physical activity was assessed with the question ‘How often do you take exercise (including incidental exercise) or pursue sports in your leisure time?’ at ages 42 and 50 (Kekäläinen et al., Citation2019). Answers were given on a 7-point scale ranging from 1 = never to 7 = practically every day. Information about physical activity frequency at age 36 was not available.
Smoking was assessed at ages 36, 42 and 50 with the question ‘Do you smoke or have you ever smoked?’ Responses ranged from 0 = never to 6 = daily (Kokkonen et al., Citation2002). The options were recoded to never smoking (= 0), ever smoking (i.e. does not smoke now but have smoked previously) (= 1), sometimes smoking (i.e. does smoke at the moment but not daily) (= 2) and daily smoking (= 3).
Alcohol consumption was evaluated by the annual quantity of and problems related to alcohol consumption (Pulkkinen & Pitkänen, Citation1994; Pitkänen et al., Citation2008). The annual quantity of alcohol consumption was calculated based on a question measuring both the frequency and quantity of alcohol use: ‘How much alcohol do you take at one time? If you have quit, please refer to the situation before you had quit. Circle the most appropriate frequency option on each line.’ Quantity options (from 1 = one portion or less to 5 = at least 13 portions, at age 36 and to 7 = 20 or more portions at a time, at ages 42 and 50) were given on the first column, and seven possible frequency options (from 1 = not at all to 7 = 6–7 times a week) were given for each line. The annual quantity of alcohol consumption in grams was calculated by multiplying the number of portions by the frequency of drinking and summing the products from each line together. The sum was multiplied by 12 (one portion = 12 g of alcohol). Because of skewed distribution, cube root transformations of alcohol variables were used in the analyses. Problems related to alcohol consumption were assessed by the Cut down, Annoyed, Guilt and Eye-opener (CAGE) questionnaire, developed for screening alcohol-related problems (Ewing, Citation1984). The questionnaire includes four questions: ‘Have you ever felt the need to Cut down on your drinking?’ ‘Have you felt Annoyed by criticism of your drinking?’ ‘Do you feel Guilty about your drinking?’ and ‘Have you ever had a drink in the morning to get rid of a hangover (an Eye-opener)?’ The responses were no (= 0), sometimes (= 1) and often (= 2), and sum scores were calculated (Pitkänen et al., Citation2008). Cronbach´s alphas were 0.80, 0.84 and 0.82 at ages 36, 42 and 50, respectively.
BMI was calculated from weight and height with the formula weight/height2. Weight and height were self-reported at age 36 and measured by a study nurse or doctor at ages 42 and 50 (Kinnunen et al., Citation2012).
Attrition analysis and representativeness of the sample
The retention rates remained high in midlife data collections (85% at age 36, 77% at 42 and 73% at 50). The participants did not participate in every data collection method (i.e. life situation questionnaire, personal interview and health examination), but almost all (99.6–100%) who participated returned the life situation questionnaire in midlife, which included information about health behaviours.
The demographic characteristics of the sample studied at ages 36, 42 and 50 were comparable to those of the respective Finnish cohort born in 1959 regarding, for example, marital status, family type, number of children and employment (Metsäpelto et al., Citation2010; Pulkkinen, Citation2017). Participants who participated in personality measures at age 33 and in general at age 50 did not differ from non-participants in childhood socioemotional characteristics, school success, or parental SES (Kinnunen et al., Citation2012; Pulkkinen, Citation2017, pp. 19–21). However, participants who were heavy alcohol users at age 42 were less likely than the other participants to participate in the study at age 50 (Pulkkinen, Citation2017, pp. 19–21), and participants in health examinations at ages 42 and 50 had more well-controlled behaviour at age 8 than non-participants (Kinnunen et al., Citation2012).
Statistical analysis
For descriptive purposes, bivariate correlations, frequencies, percentages, means and standard deviations of all variables were computed with SPSS Statistics software version 24.0 (IBM Corporation, 2016; Armonk, NY). Path modelling was used to analyse associations between variables. The hypothesised life-course pathways between childhood socioemotional characteristics, parental SES, cognitive skills, adulthood personality traits and health behaviours in midlife (depicted in ) were tested using likelihood ratio and Wald tests in the Mplus statistical modelling program version 7.3 (Los Angeles, CF) (Muthén & Muthén, Citation2017), with the maximum likelihood (ML) estimator adapted for data missing at random (MAR). Because the focus was on relationships between personality characteristics and midlife health behaviours and not changes in health behaviours during midlife, averaged scores of health behaviours (physical activity, smoking, alcohol consumption and BMI) were calculated for path models. The p values were not adjusted for multiple testing. The fit of the model was evaluated using likelihood ratio test statistics: the comparative fit index (CFI) and the root mean square error of approximation (RMSEA). The model fit was considered adequate if the following thresholds were met: p > .05, CFI ≥ 0.95 and RMSEA ≤ 0.06.
It has been previously shown, from both the present JYLS dataset and the findings of other studies, that women and men have different associations between childhood characteristics and adulthood health behaviours (Hampson et al., Citation2006; Pitkänen et al., Citation2008). Therefore, the two-group approach was used to analyse sex differences. A model with the associations shown in set free was compared to models where regression paths, means, variances, and covariances were set to be equal for men and women.
Results
Descriptive results
Descriptive statistics for study variables are presented in , and frequencies for ordinal variables (education, smoking and physical activity) are presented in the Supplementary material (). Some of the descriptive results and sex differences have been previously reported, but the sample compositions were somewhat different. At age 8, girls scored higher than boys in well-controlled behaviour, and boys scored higher in negative emotionality (cf. Pulkkinen et al., Citation2012). Girls had better school success than boys at age 14, and women had more education than men at age 27 (cf. Kokko et al., Citation2003). Women scored higher on neuroticism at age 33 (cf. Kokko et al., Citation2013). Men had higher BMI (cf. Kinnunen et al., Citation2012), increased alcohol consumption, more alcohol-related problems (cf. Pitkänen et al., Citation2008), and were more likely to be smokers at ages 36, 42 and 50. Women were more physically active at ages 42 and 50 (cf. Karvonen et al., Citation2020). The correlations between study variables are shown in the Supplementary material 1 () and detailed descriptive statistics in Supplementary material 2.
Table 1. Descriptive statistics for study variables.
Table 2. Standardised direct and total indirect effects on midlife health behaviours in women (n = 173).
Table 3. Standardised direct and total indirect effects on midlife health behaviours in men (n = 196).
Longitudinal path model
Two-group modelling showed that, when all path coefficients were constrained equally for men and women, model fit was not statistically significantly worse when compared to the fit of a model with path coefficients estimated freely for the sexes (χ2(70) = 82.09, p = .153), indicating that regression paths did not differ between the sexes. However, model fit was statistically significantly worse when equality constraints were also placed on means (χ2(83) = 227.73, p < .001), variances (χ2(83) = 132.99, p < .001), covariances (χ2(89) = 126.92, p = .005) or all of these together (χ2(115) = 317.56, p < .001). The results are shown from the two-group model in which all parameters were estimated separately for men and women. This model had adequate fit (likelihood ratio test: χ2(30) = 39.38, p = .117, RMSEA = 0.041 and CFI = 0.989). The standardised direct and total indirect associations with health behaviours in midlife are presented for women in and men in . The same model is presented in as a summarised version with only statistically significant paths. The output for path model is shown in Supplementary material 2.
Figure 2. Longitudinal path model for the associations between personality characteristics, cognitive skills and midlife health behaviours. Note. Only significant paths with standardised path coefficients are shown separately for women/men. Coefficients p < .05 are in bold. SES: socioeconomic status; C: conscientiousness; E: extraversion; N: neuroticism; BMI: body mass index.
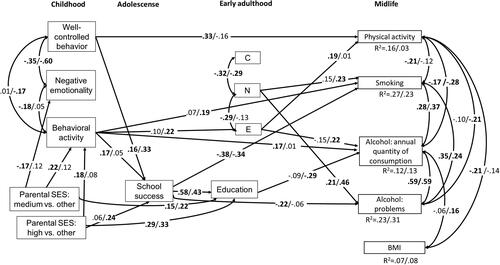
Several direct associations were found. In women, well-controlled behaviour in childhood was positively associated with physical activity in midlife (β = 0.33, p <.001). Increased behavioural activity in childhood predicted increased alcohol consumption in women (β = 0.17, p = .042) and smoking in men (β = 0.19, p = .007). Of adulthood personality traits, higher extraversion predicted increased physical activity in women (β = 0.19, p =.039) and increased alcohol consumption in men (β = 0.22, p = .017). In addition, higher neuroticism predicted increased smoking in men (β = 0.23, p = .007) and alcohol-related problems in men (β = 0.46, p < .001) and women (β = 0.21, p = .032). Lower school success in adolescence predicted increased smoking in men (β = −0.34, p < .001) and women (β = −0.37, p < .001). Lower education predicted increased alcohol consumption in men (β = −0.29, p = .003). None of the variables predicted physical activity in men or BMI in men and women.
There were also some statistically significant indirect associations. In women, childhood behavioural activity had statistically significant negative total indirect associations with smoking (β = −0.08, p = .033) and alcohol problems (β = −0.06, p = .044), but none of the specific indirect associations were statistically significant. In men, increased well-controlled behaviour was indirectly associated with decreased smoking (β = −0.12, p = .003), and this indirect association went through higher school success (β = −0.11, p = .005). In addition, even though the total indirect association between parental SES (high vs. other) was not statistically significant, higher parental SES in childhood had an indirect association with lower smoking through school success (β = −0.08, p = .008). Higher parental SES (high vs. other: β = −0.12, p = .005 and medium vs. other: β = −0.07, p = .029) and higher school success (β = −0.12, p = .007) had statistically significant total indirect associations with lower alcohol consumption. These total indirect associations were explained mainly by the specific indirect associations through education: β = −0.10, p = .009 for high parental SES vs. other, β = −0.06, p = .021 for medium parental SES vs. other and β = −0.12, p = .007 for school success. For high parental SES vs. other, the indirect path through school success and education was also statistically significant (β = −0.03, p = .032). High parental SES had also a statistically significant total indirect association with decreased alcohol problems, but none of the specific indirect associations were statistically significant.
Discussion
The purpose of this longitudinal study was to investigate the pathways of socioemotional characteristics and cognitive skills from childhood through early adulthood to health behaviours in early middle age. The main results were that these pathways were interrelated. In addition, family background contributed to the cognitive skills pathways. For socioemotional characteristics, it was found that, in women, well-controlled behaviour, which represents increased self-regulation in childhood, predicted physical activity in middle age. The direct association was statistically significant, and the path through its early adulthood conceptual counterpart, conscientiousness, was not statistically significant. The corresponding path was not significant in men, but in men, increased well-controlled behaviour indirectly predicted decreased smoking through increased cognitive skills. Negative emotionality, which represents decreased self-regulation in childhood, correlated negatively with well-controlled behaviour in childhood, and it had no additional statistically significant contribution to health behaviours in women or men. Its conceptual counterpart, adult neuroticism, predicted alcohol-related problems in men and women and also smoking in men. Within the two-dimensional framework of socioemotional behaviour, behavioural activity in childhood was assessed with a scale score indicating propensity of activity, excluding the following qualitatively described types of activity: well-controlled activity (constructiveness) and low-controlled activity (aggression) (Pulkkinen, Citation2017). In women, increased behavioural activity directly predicted increased alcohol consumption. In men, behavioural activity predicted smoking directly and its conceptual counterpart, adult extraversion and predicted alcohol consumption. Higher parental SES was associated with decreased alcohol consumption and smoking through the cognitive skills pathway in men. School success was also associated with decreased smoking in men and women.
Regarding the different aspects of health behaviours, the results suggest, first, that childhood well-controlled behaviour and adulthood extraversion predicted midlife physical activity in women. This is in line with findings concerning adult dysregulation, suggesting that childhood conscientiousness plays a role in lifespan health behaviours (Hampson et al., Citation2015) and suggesting a positive association between extraversion and physical activity in middle-aged women (Karvonen et al., Citation2020; Kekäläinen et al., Citation2019). It is possible that calm and constructive behaviour in childhood develops into self-discipline and impulse control in adulthood, which are important in turning exercise intentions into actual behaviour. People scoring high in extraversion may seek situations where they can be active (Wilson & Dishman, Citation2015). However, it was surprising that, unlike in previous research (e.g. Wilson & Dishman, Citation2015), neither conscientiousness nor neuroticism in adulthood were associated with physical activity. In men, the personality characteristics and cognitive skills included in this study explained only 3% of the variance in midlife physical activity. Physical activity might be explained by other individual (e.g. health status and motivation), interpersonal (e.g. social support), and environmental (e.g. sport facilities and the natural environment) characteristics commonly linked to physical activity behaviours (Bauman et al., Citation2012).
Second, higher scores in behavioural activity in childhood and neuroticism in adulthood were directly associated with smoking in men. Previous studies suggested that, in women, higher sociability and, in men, higher cheerfulness in childhood are associated with adulthood smoking (Tucker et al., Citation1995). These results may indicate the importance of a social component to engage in smoking. However, it was suggested that the positive association between social personality and smoking has diminished as social perceptions of smoking have become more negative over time (Malouff et al., Citation2006). This may explain why neuroticism was the only adulthood personality trait associated with smoking. The positive association between neuroticism and smoking was in line with previous studies (Cheng & Furnham, Citation2016; Malouff et al., Citation2006; Terracciano & Costa, Citation2004) and may be explained by both the lower impulse control associated with neuroticism and the more complex biological and genetic systems related to serotonin and dopamine (Terracciano & Costa, Citation2004). Consistent with the literature based on studies with larger sample sizes (Cheng & Furnham, Citation2016; Malouff et al., Citation2006; Terracciano & Costa, Citation2004), conscientiousness correlated negatively with smoking. However, the link was not statistically significant in the path model. Also, school success in adolescence was negatively associated with smoking in both men and women. Because smoking is typically taken up before higher education, school success may be a better predictor of smoking than later education (Gilman et al., Citation2003), and also personality in adolescence may be a more important predictor than personality in midlife (Pluess & Bartley, Citation2015).
Third, higher scores in childhood behavioural activity in women and higher adulthood extraversion in men predicted heavier alcohol consumption, and higher neuroticism predicted alcohol-related problems in both sexes. Previous studies (Hakulinen et al., Citation2015; Malouff et al., Citation2007; Tucker et al., Citation1995), including results from a study using the same original sample and somewhat different alcohol variables and ages (Pitkänen et al., Citation2008), suggested that the role of personality characteristics varies between drinking patterns. Our analysis suggests that social behaviour captured by behavioural activity and extraversion were associated with increased drinking, whereas neuroticism was linked to alcohol-related problems. In addition to personality, increased cognitive skills and higher parental SES through cognitive skills predicted lower alcohol consumption and alcohol-related problems, as was previously suggested using somewhat different alcohol variables and ages (Pitkänen et al., Citation2008). Previous studies suggested that higher education is linked to, for example, increased drinking, taking alcohol with meals and drinking more wine (Rosoff et al., Citation2021), but fewer alcohol-related problems and decreased binge drinking (Collins, Citation2016).
Fourth, in contrast to previous findings (Cheng et al., Citation2020; Cohen et al., Citation2013; Jokela et al., Citation2013; Sutin et al., Citation2011), no evidence was found of associations between socioemotional characteristics, personality, cognitive skills and BMI in the longitudinal model. Our longitudinal model explains only 7–8% of the variance in midlife BMI. However, the correlations (Supplementary material 1) showed that education and in women also school success and conscientiousness were linked to lower midlife BMI, and in women neuroticism to higher BMI. It is likely that with a larger sample size some of these associations may have reached statistical significance. It is also possible that other factors not included in the present analyses were related to obesity in this sample. These might include marital status, number of children, psychological distress, locus of control and other health behaviours (Ali & Lindström, Citation2006; Cheng & Furnham, Citation2019; Gomersall et al., Citation2014). In addition, there could be culture- and time-related differences in socio-economic inequalities in BMI and obesity: for example, the inequalities seem to be wider in southern Europe than in Finland (Roskam & Kunst, Citation2008), and emerge already in childhood among later-born cohorts (i.e. those born in 2001 compared with those born in 1946–1970) (Bann et al., Citation2018).
The limitations of this study should be considered when interpreting the results. First, this was an exploratory study, and the p values were not adjusted for multiple testing. Compared to large population studies (e.g. British cohort studies with n≈17,000), this relatively small sample may have lacked the statistical power needed to detect all existing associations. For example, many associations that were found in descriptive correlational analyses did not reach statistical significance in the path model when analysed together with all the other variables. The results should be repeated with other samples. Second, the measures of health behaviours had some limitations. Information about physical activity at age 36 was not available, and at ages 42 and 50, physical activity was assessed by a single question asking about the frequency of leisure-time physical activity. The limited question and temporal variety in physical activity levels may explain the lack of associations with physical activity in men. The data did not include questions about nutrition and eating behaviour. BMI is only a surrogate of obesity and body composition and may be misleading for people with well-developed muscles (Prentice & Jebb, Citation2001). In addition, a more detailed analysis of smoking (e.g. initiation vs. cessation) and alcohol use (e.g. binge drinking) were not the focus of this study. Lastly, there may be multiple other factors than those included in this study that relate to midlife health behaviours across the lifespan. These other factors may explain the low amount of variance observed, particularly for BMI in both men and women and physical activity in men.
This study contributes to our understanding of longitudinal relationships between personality, education, and health behaviours. The unique and major strength of this study is the longitudinal data collected at several points over 42 years with a relatively low attrition rate. However, the fact that participants who were heavy alcohol users at age 42 were less likely than the other participants to participate in the study at age 50 may have attenuated associations. The sample also well represents the Finnish age cohort in the adult data collection phases (Pulkkinen, Citation2017). Using repeated concurrent measures of health behaviours, we attempted to reduce bias related to retrospective measures (e.g. recall bias) and single measurement points (e.g. effects of extraordinary life situations on results). In addition, this study covered four measures of health behaviours (i.e. physical activity, smoking, alcohol consumption and BMI), which are all important predictors of public health.
Midlife physical activity, smoking, alcohol consumption, and obesity are complex behaviours that are affected by multiple factors over the life course. This study suggests that childhood socioemotional characteristics and cognitive skills can predict some part of the physical activity, smoking, and alcohol-related behaviours in midlife. Considering personality characteristics and cognitive skills may help to identify risk groups for later health-damaging behaviours.
Supplemental Material
Download MS Word (28.8 KB)Supplemental Material
Download MS Word (30.4 KB)Disclosure statement
The authors declare no competing interests.
Additional information
Funding
Notes on contributors
Tiia Kekäläinen
Tiia Kekäläinen contributed to conceptualisation, formal analysis, and writing – original draft. Jenni Karvonen contributed to conceptualisation and writing – original draft. Timo Törmäkangas contributed to formal analysis and writing – review & editing. Lea Pulkkinen contributed to data curation, conceptualisation, investigation, methodology, resources, and writing – review & editing. Katja Kokko contributed to conceptualisation, investigation, funding acquisition, supervision, and writing – review & editing.
References
- Adler, N. E., & Newman, K. (2002). Socioeconomic disparities in health: Pathways and policies. Health Affairs (Project Hope), 21(2), 60–76. https://doi.org/10.1377/hlthaff.21.2.60
- Ali, S. M., & Lindström, M. (2006). Socioeconomic, psychosocial, behavioural, and psychological determinants of BMI among young women: Differing patterns for underweight and overweight/obesity. European Journal of Public Health, 16(3), 324–330. https://doi.org/10.1093/eurpub/cki187
- Artaud, F., Sabia, S., Dugravot, A., Kivimaki, M., Singh-Manoux, A., & Elbaz, A. (2016). Trajectories of unhealthy behaviors in midlife and risk of disability at older ages in the Whitehall II Cohort Study. The Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 71(11), 1500–1506. https://doi.org/10.1093/gerona/glw060
- Baker, D. P., Leon, J., Greenaway, E. G. S., Collins, J., & Movit, M. (2011). The Education effect on population health: A reassessment. Population and Development Review, 37(2), 307–332. https://doi.org/10.1111/j.1728-4457.2011.00412.x
- Bann, D., Johnson, W., Li, L., Kuh, D., & Hardy, R. (2018). Socioeconomic inequalities in childhood and adolescent body-mass index, weight, and height from 1953 to 2015: An analysis of four longitudinal, observational, British birth cohort studies. The Lancet Public Health, 3(4), e194–e203. https://doi.org/10.1016/S2468-2667(18)30045-8
- Barr, P. B., Silberg, J., Dick, D. M., & Maes, H. H. (2018). Childhood socioeconomic status and longitudinal patterns of alcohol problems: Variation across etiological pathways in genetic risk. Social Science & Medicine (1982), 209, 51–58. https://doi.org/10.1016/j.socscimed.2018.05.027
- Bauman, A. E., Reis, R. S., Sallis, J. F., Wells, J. C., Loos, R. J., & Martin, B. W. (2012). Correlates of physical activity: Why are some people physically active and others not? The Lancet, 380(9838), 258–271. https://doi.org/10.1016/S0140-6736(12)60735-1
- Beenackers, M. A., Kamphuis, C. B. M., Giskes, K., Brug, J., Kunst, A. E., Burdorf, A., & van Lenthe, F. J. (2012). Socioeconomic inequalities in occupational, leisure-time, and transport related physical activity among European adults: A systematic review. The International Journal of Behavioral Nutrition and Physical Activity, 9, 116. https://doi.org/10.1186/1479-5868-9-116
- Bogg, T., & Roberts, B. W. (2004). Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychological Bulletin, 130(6), 887–919.
- Caspi, A. (2000). The child is father of the man: Personality continuities from childhood to adulthood. Journal of Personality and Social Psychology, 78(1), 158–172. https://doi.org/10.1037//0022-3514.78.1.158
- Cheng, H., & Furnham, A. (2016). The Big-Five personality traits, maternal smoking during pregnancy, and educational qualifications as predictors of tobacco use in a nationally representative sample. PLoS One, 11(1), e0145552. https://doi.org/10.1371/journal.pone.0145552
- Cheng, H., & Furnham, A. (2019). Childhood locus of control and self-esteem, education, psychological distress and physical exercise as predictors of adult obesity. Journal of Public Health (Oxford), 41(3), 439–446. https://doi.org/10.1093/pubmed/fdy125
- Cheng, H., Montgomery, S., Green, A., & Furnham, A. (2020). Biomedical, psychological, environmental and behavioural factors associated with adult obesity in a nationally representative sample. Journal of Public Health, 42(3), 570–578. https://doi.org/10.1093/pubmed/fdz009
- Cohen, A. K., Rai, M., Rehkopf, D. H., & Abrams, B. (2013). Educational attainment and obesity: A systematic review. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 14(12), 989–1005. https://doi.org/10.1111/obr.12062
- Collins, S. E. (2016). Associations between socioeconomic factors and alcohol outcomes. Alcohol Research: Current Reviews, 38(1), 83–94.
- Costa, P. T., & McCrae, R. R. (1985). The NEO personality inventory manual. Psychological Assessment Resources.
- Davies, N. M., Dickson, M., Davey Smith, G., van den Berg, G. J., & Windmeijer, F. (2018). The causal effects of education on health outcomes in the UK Biobank. Nature Human Behaviour, 2(2), 117–125. https://doi.org/10.1038/s41562-017-0279-y
- Elhakeem, A., Cooper, R., Bann, D., & Hardy, R. (2015). Childhood socioeconomic position and adult leisure-time physical activity: A systematic review. The International Journal of Behavioral Nutrition and Physical Activity, 12, 92. https://doi.org/10.1186/s12966-015-0250-0
- Ewing, J. A. (1984). Detecting alcoholism. The CAGE questionnaire. JAMA, 252(14), 1905–1907. https://doi.org/10.1001/jama.1984.03350140051025
- Friedman, H. S., Tucker, J. S., Schwartz, J. E., Martin, L. R., Tomlinson-Keasey, C., Wingard, D. L., & Criqui, M. H. (1995). Childhood conscientiousness and longevity: Health behaviors and cause of death. Journal of Personality and Social Psychology, 68(4), 696–703. https://doi.org/10.1037/0022-3514.68.4.696
- Gerlach, G., Herpertz, S., & Loeber, S. (2015). Personality traits and obesity: A systematic review. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 16(1), 32–63. https://doi.org/10.1111/obr.12235
- Gilman, S., Abrams, D., & Buka, S. (2003). Socioeconomic status over the life course and stages of cigarette use: Initiation, regular use, and cessation. Journal of Epidemiology and Community Health, 57(10), 802–808. https://doi.org/10.1136/jech.57.10.802
- Gomersall, S. R., Dobson, A. J., & Brown, W. J. (2014). Weight gain, overweight, and obesity: Determinants and health outcomes from the Australian Longitudinal Study on Women’s Health. Current Obesity Reports, 3(1), 46–53. https://doi.org/10.1007/s13679-013-0077-4
- Hakulinen, C., Elovainio, M., Batty, G. D., Virtanen, M., Kivimäki, M., & Jokela, M. (2015). Personality and alcohol consumption: Pooled analysis of 72,949 adults from eight cohort studies. Drug and Alcohol Dependence, 151, 110–114. https://doi.org/10.1016/j.drugalcdep.2015.03.008
- Hampson, S. E., Edmonds, G. W., Barckley, M., Goldberg, L. R., Dubanoski, J. P., & Hillier, T. A. (2016). A Big Five approach to self-regulation: Personality traits and health trajectories in the Hawaii longitudinal study of personality and health. Psychology, Health & Medicine, 21(2), 152–162. https://doi.org/10.1080/13548506.2015.1061676
- Hampson, S. E., Edmonds, G. W., Goldberg, L. R., Dubanoski, J. P., & Hillier, T. A. (2015). A life-span behavioral mechanism relating childhood conscientiousness to adult clinical health. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 34(9), 887–895. https://doi.org/10.1037/hea0000209
- Hampson, S. E., & Goldberg, L. R. (2006). A first large cohort study of personality trait stability over the 40 years between elementary school and midlife. Journal of Personality and Social Psychology, 91(4), 763–779. https://doi.org/10.1037/0022-3514.91.4.763
- Hampson, S. E., Goldberg, L. R., Vogt, T. M., & Dubanoski, J. P. (2006). Forty years on teachers’ assessments of children’s personality traits predict self-reported health behaviors and outcomes at midlife. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 25(1), 57–64. https://doi.org/10.1037/0278-6133.25.1.57
- Hampson, S. E., Goldberg, L. R., Vogt, T. M., & Dubanoski, J. P. (2007). Mechanisms by which childhood personality traits influence adult health status: Educational attainment and healthy behaviors. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 26(1), 121–125. https://doi.org/10.1037/0278-6133.26.1.121
- Jokela, M., Hintsanen, M., Hakulinen, C., Batty, G. D., Nabi, H., Singh-Manoux, A., & Kivimäki, M. (2013). Association of personality with the development and persistence of obesity: A meta-analysis based on individual-participant data. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 14(4), 315–323. https://doi.org/10.1111/obr.12007
- Jonassaint, C. R., Siegler, I. C., Barefoot, J. C., Edwards, C. L., & Williams, R. B. (2011). Low life course socioeconomic status (SES) is associated with negative NEO PI-R personality patterns. International Journal of Behavioral Medicine, 18(1), 13–21. https://doi.org/10.1007/s12529-009-9069-x
- Judge, T. A., Higgins, C. A., Thoresen, C. J., & Barrick, M. R. (1999). The Big Five personality traits, general mental ability, and career success across the lifespan. Personnel Psychology, 52(3), 621–652. https://doi.org/10.1111/j.1744-6570.1999.tb00174.x
- Juneau, C. E., Benmarhnia, T., Poulin, A. A., Côté, S., & Potvin, L. (2015). Socioeconomic position during childhood and physical activity during adulthood: A systematic review. International Journal of Public Health, 60(7), 799–813. https://doi.org/10.1007/s00038-015-0710-y
- Karvonen, J., Törmäkangas, T., Pulkkinen, L., & Kokko, K. (2020). Associations of temperament and personality traits with frequency of physical activity in adulthood. Journal of Research in Personality, 84, 103887. https://doi.org/10.1016/j.jrp.2019.103887
- Kekäläinen, T., Freund, A. M., Sipilä, S., & Kokko, K. (2019). Cross-sectional and longitudinal associations between leisure lime physical activity, mental well-being and subjective health in middle adulthood. Applied Research in Quality of Life, 15, 1099–1116 https://doi.org/10.1007/s11482-019-09721-4
- Kekäläinen, T., Laakkonen, E. K., Terracciano, A., Savikangas, T., Hyvärinen, M., Tammelin, T. H., Rantalainen, T., Törmäkangas, T., Kujala, U. M., Alen, M., Kovanen, V., Sipilä, S., & Kokko, K. (2020). Accelerometer-measured and self-reported physical activity in relation to extraversion and neuroticism: A cross-sectional analysis of two studies. BMC Geriatrics, 20(1), 264. https://doi.org/10.1186/s12877-020-01669-7
- Kern, M. L., Reynolds, C. A., & Friedman, H. S. (2010). Predictors of physical activity patterns across adulthood: A growth curve analysis. Personality & Social Psychology Bulletin, 36(8), 1058–1072. https://doi.org/10.1177/0146167210374834
- Kinnunen, M. L., Metsäpelto, R.-L., Feldt, T., Kokko, K., Tolvanen, A., Kinnunen, U., Leppänen, E., & Pulkkinen, L. (2012). Personality profiles and health: Longitudinal evidence among Finnish adults. Scandinavian Journal of Psychology, 53(6), 512–522. https://doi.org/10.1111/j.1467-9450.2012.00969.x
- Kokko, K., Bergman, L. R., & Pulkkinen, L. (2003). Child personality characteristics and selection into long-term unemployment in Finnish and Swedish longitudinal samples. International Journal of Behavioral Development, 27(2), 134–144. https://doi.org/10.1080/01650250244000137
- Kokko, K., Tolvanen, A., & Pulkkinen, L. (2013). Associations between personality traits and psychological well-being across time in middle adulthood. Journal of Research in Personality, 47(6), 748–756. https://doi.org/10.1016/j.jrp.2013.07.002
- Kokkonen, M., Kinnunen, T., & Pulkkinen, L. (2002). Direct and indirect effects of adolescent self-control of emotions and behavioral expression on adult health outcomes. Psychology & Health, 17(5), 657–670. https://doi.org/10.1080/08870440290025849
- Malouff, J. M., Thorsteinsson, E. B., Rooke, S. E., & Schutte, N. S. (2007). Alcohol involvement and the Five-Factor model of personality: A meta-analysis. Journal of Drug Education, 37(3), 277–294. https://doi.org/10.2190/DE.37.3.d
- Malouff, J. M., Thorsteinsson, E. B., & Schutte, N. S. (2006). The five-factor model of personality and smoking: A meta-analysis. Journal of Drug Education, 36(1), 47–58. https://doi.org/10.2190/9EP8-17P8-EKG7-66AD
- Matthews, K. A., & Gallo, L. C. (2011). Psychological perspectives on pathways linking socioeconomic status and physical health. Annual Review of Psychology, 62, 501–530. https://doi.org/10.1146/annurev.psych.031809.130711
- McCrae, R. R., & Costa, P. T. J. (2003). Personality in adulthood. A Five-Factor theory perspective. (2nd ed.). The Guilford Press.
- McCrae, R. R., Costa, P. T., Jr, Ostendorf, F., Angleitner, A., Hrebickova, M., Avia, M. D., Sanz, J., Sanchez-Bernardos, M. L., Kusdil, M. E., Woodfield, R., Saunders, P. R., & Smith, P. B. (2000). Nature over nurture: Temperament, personality, and life span development. Journal of Personality and Social Psychology, 78(1), 173–186.
- Metsäpelto, R.-L., Polet, J., Kokko, K., Rantanen, J., Kinnunen, M.-L., Pitkänen, T., Lyyra, A.-L., & Pulkkinen, L. (2010). Tutkimuksen toteutus. In L. Pulkkinen & K. Kokko (Eds.), Keski-ikä elämänvaiheena. Jyväskylän yliopiston psykologian laitoksen julkaisuja 352 (Vol. 1, pp. 5–19). University of Jyväskylä.
- Muthén, L. K. and Muthén, B. O. (1998-2017). Mplus User’s Guide (8th Ed). Los Angeles, CA: Muthén & Muthén.
- Pitkänen, T., Kokko, K., Lyyra, A.-L., & Pulkkinen, L. (2008). A developmental approach to alcohol drinking behaviour in adulthood: A follow-up study from age 8 to age 42. Addiction, 103(s1), 48–68. https://doi.org/10.1111/j.1360-0443.2008.02176.x
- Pitkänen, T., Lyyra, A.-L., & Pulkkinen, L. (2005). Age of onset of drinking and the use of alcohol in adulthood: A follow-up study from age 8-42 for females and males. Addiction (Abingdon, England), 100(5), 652–661. https://doi.org/10.1111/j.1360-0443.2005.01053.x
- Pluess, M., & Bartley, M. (2015). Childhood conscientiousness predicts the social gradient of smoking in adulthood: A life course analysis. Journal of Epidemiology and Community Health, 69(4), 330–338. https://doi.org/10.1136/jech-2014-204263
- Prentice, A. M., & Jebb, S. A. (2001). Beyond body mass index. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 2(3), 141–147. https://doi.org/10.1046/j.1467-789x.2001.00031.x
- Pulkkinen, L. (1983). Youthful smoking and drinking in a longitudinal perspective. Journal of Youth and Adolescence, 12(4), 253–283. https://doi.org/10.1007/BF02088726
- Pulkkinen, L. (2017). Human development from middle childhood to middle adulthood: Growing up to the middle-aged (In collaboration with Katja Kokko). Routledge. https://doi.org/10.4324/9781315732947
- Pulkkinen, L., Kokko, K., & Rantanen, J. (2012). Paths from socioemotional behavior in middle childhood to personality in middle adulthood. Developmental Psychology, 48(5), 1283–1291. https://doi.org/10.1037/a0027463
- Pulkkinen, L., & Pitkänen, T. (1994). A prospective study of the precursors to problem drinking in young adulthood. Journal of Studies on Alcohol, 55(5), 578–587. https://doi.org/10.15288/jsa.1994.55.578
- Pulkki-Råback, L., Elovainio, M., Kivimäki, M., Raitakari, O., & Keltikangas-Järvinen, L. (2005). Temperament in childhood predicts body mass in adulthood: The cardiovascular risk in young finns study. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 24(3), 307–315. https://doi.org/10.1037/0278-6133.24.3.307
- Pulver, A., Allik, J., Pulkkinen, L., & Hämäläinen, M. (1995). A Big Five personality inventory in two non-Indo-European languages. European Journal of Personality, 9(2), 109–124. https://doi.org/10.1002/per.2410090205
- Puolakka, E., Pahkala, K., Laitinen, T. T., Magnussen, C. G., Hutri-Kähönen, N., Männistö, S., Pälve, K. S., Tammelin, T., Tossavainen, P., Jokinen, E., Smith, K. J., Laitinen, T., Elovainio, M., Pulkki-Råback, L., Viikari, J. S. A., Raitakari, O. T., & Juonala, M. (2018). Childhood socioeconomic status and lifetime health behaviors: The Young Finns Study. International Journal of Cardiology, 258, 289–294. https://doi.org/10.1016/j.ijcard.2018.01.088
- Roskam, A. J. R., & Kunst, A. E. (2008). The predictive value of different socio-economic indicators for overweight in nine European countries. Public Health Nutrition, 11(12), 1256–1266. https://doi.org/10.1017/S1368980008002747
- Rosoff, D. B., Clarke, T. K., Adams, M. J., McIntosh, A. M., Davey Smith, G., Jung, J., & Lohoff, F. W. (2021). Educational attainment impacts drinking behaviors and risk for alcohol dependence: Results from a two-sample Mendelian randomization study with ∼780,000 participants. Molecular Psychiatry, 26(4), 1119–1114. https://doi.org/10.1038/s41380-019-0535-9
- Sabia, S., Elbaz, A., Rouveau, N., Brunner, E. J., Kivimaki, M., & Singh-Manoux, A. (2014). Cumulative associations between midlife health behaviors and physical functioning in early old age: A 17-year prospective cohort study. Journal of the American Geriatrics Society, 62(10), 1860–1868. https://doi.org/10.1111/jgs.13071
- Sutin, A. R., Ferrucci, L., Zonderman, A. B., & Terracciano, A. (2011). Personality and obesity across the adult life span. Journal of Personality and Social Psychology, 101(3), 579–592. https://doi.org/10.1037/a0024286
- Sutin, A. R., Luchetti, M., Stephan, Y., Robins, R. W., & Terracciano, A. (2017). Parental educational attainment and adult offspring personality: An intergenerational life span approach to the origin of adult personality traits. Journal of Personality and Social Psychology, 113(1), 144–166. https://doi.org/10.1037/pspp0000137
- Sutin, A. R., Stephan, Y., Luchetti, M., Artese, A., Oshio, A., & Terracciano, A. (2016). The five-factor model of personality and physical inactivity: A meta-analysis of 16 samples. Journal of Research in Personality, 63, 22–28. https://doi.org/10.1016/j.jrp.2016.05.001
- Tamayo, T., Herder, C., & Rathmann, W. (2010). Impact of early psychosocial factors (childhood socioeconomic factors and adversities) on future risk of type 2 diabetes, metabolic disturbances and obesity: A systematic review. BMC Public Health, 10, 525. https://doi.org/10.1186/1471-2458-10-525.
- Terracciano, A., & Costa, P. T. (2004). Smoking and the five-factor model of personality. Addiction (Abingdon, England), 99(4), 472–481. https://doi.org/10.1111/j.1360-0443.2004.00687.x
- Tian, J., Gall, S., Patterson, K., Otahal, P., Blizzard, L., Patton, G., Dwyer, T., & Venn, A. (2019). Socioeconomic position over the life course from childhood and smoking status in mid-adulthood: Results from a 25-year follow-up study. BMC Public Health, 19(1), 169. https://doi.org/10.1186/s12889-019-6483-0
- Tucker, J. S., Friedman, H. S., Tomlinson-Keasey, C., Schwartz, J. E., Wingard, D. L., Criqui, M. H., & Martin, L. R. (1995). Childhood psychosocial predictors of adulthood smoking, alcohol consumption, and physical activity. Journal of Applied Social Psychology, 25(21), 1884–1899. https://doi.org/10.1111/j.1559-1816.1995.tb01822.x
- Turiano, N. A., Hill, P. L., Graham, E. K., & Mroczek, D. K. (2018). Associations between personality and health behaviors across the life span. In C. D. Ryff & R. F. Krueger (eds.), The Oxford Handbook of Integrative Health Science. Oxford University Press (pp. 305—316). https://doi.org/10.1093/oxfordhb/9780190676384.013.20
- Wilson, K. E., & Dishman, R. K. (2015). Personality and physical activity: A systematic review and meta-analysis. Personality and Individual Differences, 72, 230–242. https://doi.org/10.1016/j.paid.2014.08.023