
Abstract
Nonadherence to medicines is a global problem compromising health and economic outcomes for individuals and society. This article outlines how adherence is defined and measured, and examines the impact, prevalence and determinants of nonadherence. It also discusses how a psychosocial perspective can inform the development of interventions to optimise adherence and presents a series of recommendations for future research to overcome common limitations associated with the medication nonadherence literature. Nonadherence is best understood in terms of the interactions between an individual and a specific disease/treatment, within a social and environmental context. Adherence is a product of motivation and ability. Motivation comprises conscious decision-making processes but also from more ‘instinctive’, intuitive and habitual processes. Ability comprises the physical and psychological skills needed to adhere. Both motivation and ability are influenced by environmental and social factors which influence the opportunity to adhere as well as triggers or cues to actions which may be internal (e.g. experiencing symptoms) or external (e.g. receiving a reminder). Systematic reviews of adherence interventions show that effective solutions are elusive, partly because few have a strong theoretical basis. Adherence support targeted at the level of individuals will be more effective if it is tailored to address the specific perceptions (e.g. beliefs about illness and treatment) and practicalities (e.g. capability and resources) influencing individuals’ motivation and ability to adhere.
Introduction
The prevalence of long-term health conditions is high and rising with an ageing population. In the USA, an estimated 117 million people are living with a long-term condition (Ward et al., Citation2014). In the UK, it is estimated that 15 million people live with a chronic physical illness, with this estimated to increase to 18 million by 2025 (Abraham et al., Citation2016). The prescription of a pharmaceutical medicine is one of the most common interventions in developed health economies where medicines are essential treatments for most long-term conditions. However, nonadherence remains a significant barrier to achieve optimum outcomes from appropriately prescribed medicines, especially in long-term conditions. In a classic review, the World Health Organisation (WHO) estimated that around half of medicines prescribed for long-term conditions were not taken as advised (Sabaté, Citation2003; Simpson et al., Citation2006), and a 2018 report from the Organisation for Economic Co-operation and Development estimated that poor adherence results in 200,000 premature deaths in Europe each year (Organisation for Economic Co-operation and Development (OECD, Citation2018). The high health and economic costs of nonadherence are a considerable challenge to society and the economy, representing a fault line in medicine.
The adherence literature is vast with a PubMed search with the keywords (‘medication adherence’, ‘medication nonadherence’, ‘medication non-adherence’) retrieving 41,655 results, with 20,662 results from the last 5 years alone. An exhaustive review of this literature is beyond the scope of this article, which aims to provide an overview, identifying key themes and issues and providing a framework for understanding the causes on nonadherence and the implications for the design of interventions. We will discuss how adherence is defined and measured, and review the prevalence, impact and determinants of nonadherence. Finally, we will consider interventions to support adherence and discuss future directions for research and practice.
Definitions and measurement of adherence
Terminology
Adherence may be defined as ‘the extent to which the patient’s behaviour matches agreed recommendations from the prescriber’ (Horne et al., Citation2005, p.33). The term adherence has generally replaced compliance which was prevalent in older articles. Compliance may be defined as the extent to which the patient’s behaviour matches the prescriber’s recommendations (Haynes et al., Citation1979; Horne et al., Citation2005). However, this term has been criticised because it seems to denote a relationship in which the role of the clinician is to decide on the appropriate treatment, issue the relevant instructions and the role of the patient is to passively ‘follow the doctor’s orders’ (Horne et al., Citation2005). Conversely, adherence recognises the importance of patient autonomy and that an ‘agreement’ is implicit in adherence. The term concordance has also been used in relation to medication taking behaviour, referring to the interaction between patient and prescriber and the degree to which their views about the prescription agree. However, the term does not describe patient behaviour and cannot be used as a synonym for adherence (Horne et al., Citation2005).
Beyond terminology, the definition of adherence becomes even more controversial. This is simple if adherence is conceptualised as an ‘all or nothing’ response in which the patient either follows the prescriber’s instruction to the letter (adherence) or deviates from it in some way (nonadherence). But such a strict definition is of little use in practice. The extent of adherence necessary to achieve the desired effect varies between medicines and between and within individuals. A cut off of 80% is often used to categorise patients into adherent vs. nonadherent groups (Nieuwlaat et al., Citation2014). Such categorisations are based on estimates of the level of nonadherence that is likely to be clinically significant. However, this varies between patients and medicines and cut-offs can only provide approximate indicators of clinical relevance.
The behavioural components of medication adherence
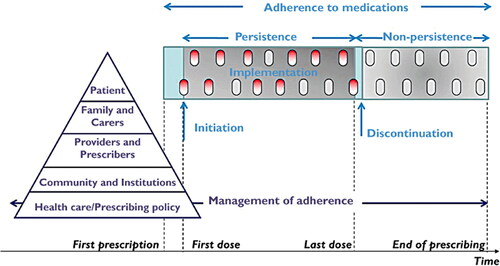
Vrijens et al. (Citation2012) developed a taxonomy for medication-taking behaviour; separating adherence into three behavioural components: initiation, implementation and discontinuation (). Initiation refers to the patient taking the first dose of a prescribed medication. Once treatment has been initiated, implementation refers to the extent to which a patient’s behaviour corresponds with the prescribed dosing regimen. Discontinuation refers to the last dose of the medication taken. An additional term, persistence, refers to the length of time between initiation and discontinuation, and non-persistence is where the patient unilaterally decides to stop the medication early without consulting the prescriber.
Figure 1. Illustration of the process of adherence to medication (light blue) and the process of management of adherence (dark blue). Reprinted from Vrijens et al. (Citation2012).
Measurement techniques
There is also widespread variation in how nonadherence is measured, with limitations associated with each. For example, direct observation or electronic adherence monitoring has been suggested to be the ‘gold standard’ of adherence measurement (Chan et al., Citation2013). However, these methods can be costly and invasive, whereas other non-invasive methods that are easier to administer tend to be more subjective in nature. The range of measures used in the literature adds to the complexity of the subject and makes synthesising the nonadherence literature challenging.
Objective measures
Objective measures of adherence include measures such as direct observations of the patient taking a medication, detection of the drug in the bloodstream or urine and electronic monitoring. Measuring drug concentration in the bloodline has been used to assess adherence and is often considered to be the most objective method. However, it is invasive and risky and due to variations in how drugs are prescribed by individuals (pharmacokinetics), the amount of drug in the blood does not always equate to the amount taken and is therefore not a reliable method for assessing adherence. As well as measuring drug levels in the blood, clinical parameters can also be used as an indication of adherence. For example, one of the most commonly used methods for determining adherence to anti-retroviral medication in HIV is the achievement of undetectable viral load, as this was thought not to be possible without high levels of adherence. However, as modern treatment improves and becomes more forgiving to missed doses, it has been suggested that suppression of viral load may no longer be an indicator of high rates of adherence (Castillo-Mancilla & Haberer, Citation2018).
A less invasive method is to count how many doses a patient takes using electronic monitors. One way of measuring this is via electronic monitoring through devices such as medication event monitoring systems (MEMS) caps. This records when a packet of medication has been opened. MEMS caps are currently considered to be one of the best measures of adherence because they provide reliable and more detailed data about patient adherence including dose timings, intervals, time and frequency. However, the use of MEMS caps has been criticised because they do not provide data on whether the medication was ingested, nor any reasons for nonadherence. In addition, for research to be considered ethical, patients must be informed in advance of testing that their adherence behaviour is being measured, which can lead to patients temporarily improving their behaviour to match the expectations of both the prescriber and observer.
Prescription refill rates have been used to assess adherence. Discontinuation can also be measured by identifying gaps in prescription refill. This method is widely used, especially in the USA, because data can be easily collected on a very large scale. However, much like with MEMS caps, this method does not necessarily provide data on how much medication a patient has ingested. Obtaining accurate medication start dates can be difficult as the container specifies the date dispensed or collected, rather than the date started.
Newer advances in measurement include wearable devices and smart pills, such as the Ingestible Sensor System (Eisenberger et al., Citation2013), where microsensors are incorporated into oral pharmaceuticals. These microsensors are activated once the tablet is ingested and send a signal to an adhesive personal monitor worn by the patient, which transmits data to a smartphone. Similar tools include necklaces that can detect swallowing (Kalantarian et al., Citation2016) and smart watches to detect pill bottle opening, pill removal and other pill taking behaviours (Kalantarian et al., Citation2015). Whilst these devices have clear potential in providing reliable measurement of whether a pill has been taken, there are considerable drawbacks around patient acceptability, and concerns that these technologies are an unwelcome form of surveillance (Aldeer et al., Citation2018; Kamal et al., Citation2020) which could compromise the doctor/patient relationship (Martani et al., Citation2020).
Self-report measures
Self-report methods such as validated questionnaires, interviews and medication diaries are commonly used because they are simple to administer and low cost, with the ability to reach large numbers of respondents (Holmes et al., Citation2014). Self-report measures can be considered advantageous because they allow for the measurement of both intentional (e.g. a deliberate decision not to take a medicine) and unintentional (e.g. forgetting to take a medicine) nonadherence. However, reports of nonadherence are often more reliable than reports of adherence due to recall and self-presentational bias (a tendency to respond in ways that are perceived to be socially desirable).
Despite these limitations, research suggests that these self-report methods (especially questionnaire and diary methods) may have some level of agreement with more objective measures of adherence (Selinger et al., Citation2019; Shi et al., Citation2010). These self-report measures are the most feasible and easy to implement both within clinical practice and research, and although subjective, procedures can be put in place in efforts to improve reliability, such as the use of validated scales, using optimised question response formats and reducing social desirability biases by using non-judgemental statements to normalise nonadherence (Chan et al., Citation2020).
Variation across measurement techniques
There are several available methods to measure nonadherence, each of which may provide considerably different estimations of adherence. For example, a review of adherence in breast cancer survivors found that estimates of adherence to endocrine therapy varied considerably when measured using MEMS (93%), self-report (82%) and prescription refill rates (75%) (Moon et al., Citation2017). There are strengths and weaknesses associated with each measure; consequently, there remains no current ‘gold standard’ for measuring adherence. Objective measures of adherence are often preferred by researchers and clinicians; however, these measures may not always be as effective as they seem. For example, most methods do not provide a wholly accurate and reliable measure of adherence, and those that do are often impractical to implement which limits their utility, whereas subjective measures are cheap and easy to implement, providing that their limitations are understood and accounted for. Despite the limitations of self-report methods, a meta-analysis of 35 studies has shown that the majority of studies reported moderate (62.7%) or high (11.6%) correlations between self-report methods and MEMS, although self-report questionnaires did show higher rates of adherence (9.2% difference) (Monnette et al., Citation2018).
Another consideration is that some self-report measures of adherence such as the Medication Adherence Report Scale (MARS) (Chan et al., Citation2020) assess adherence behaviour (what the person did with the medication). Other measures are less specific to adherence behaviour. For example, the Morisky Medication Adherence Scales (MMAS-8 and MMAS-4) (Moon et al., Citation2017; Morisky et al., Citation1986) include items assessing the reason for nonadherence (e.g. missing medications if I feel better) and the Intentional Nonadherence Scale (INAS) encompasses adherence behaviours and the potential reasons for nonadherence (e.g. beliefs about treatment) (Weinman et al., Citation2018). Differences in what adherence scales are actually measuring can make it difficult to adequately compare the performance of self-report adherence measures across studies. presents an overview of methods for measuring medication adherence, and the advantages and disadvantages associated with each.
Combining methods
There is increasing interest in combining techniques for measuring adherence (Dobbels et al., Citation2010). For example, combining self-report measures capturing actual medication-taking behaviour, with objective forms of adherence such as prescription refill rates or electronic monitoring to produce amalgamated, comprehensive assessments of adherence could function to improve measurement accuracy (Chan et al., Citation2020). It would, therefore, be useful for future research to explore a combined approach to measuring nonadherence. Further, in clinical practice, most nonadherence is likely to be undisclosed (Horne et al., Citation2005); therefore, it is also important that methods for eliciting honest disclosure and non-judgemental discussions surrounding medication-taking behaviour within medical consultations are developed.
Health impact of nonadherence
The implicit assumption behind adherence interventions is that adherence improves patient outcomes. This premise was not, however, thoroughly tested until DiMatteo et al. (Citation2002) reviewed 63 studies investigating the relationship between adherence to medical advice (including prescribed medication, diet modification, physical activity and eye patching) and outcomes (including survival, reported pain, blood pressure control, visual acuity, cholesterol levels and organ rejection). Overall, the odds of having a good treatment outcome were three times higher amongst high adherers than low adherers. Further, the increased likelihood of individuals dying as a result of ‘poor’ adherence compared to those with ‘good adherence’ is 2–3 fold (OECD, Citation2018; Simpson et al., Citation2006). It has been suggested that increasing medication adherence may have a greater impact on the health of the population than improvements in any specific medical treatment (Haynes et al., Citation2002). Not taking a medication as prescribed is likely to mean the patient is not receiving the full therapeutic benefit of the medication.
Depending on the role and outcome of a given medicine, the impact of nonadherence is likely to be more problematic for some health conditions compared with others. Nonadherence and non-initiation are arguably most important in those health conditions in which nonadherence has been demonstrated to have an impact on clinical outcomes (e.g. increase in severity of symptoms, morbidity and mortality) such as HIV, cancer, diabetes, asthma, cardiovascular disease (CVD), mental illness, organ transplant, etc. (Horne et al., Citation2005). For example, a study of over 8000 breast cancer survivors found that early discontinuation of endocrine therapy was associated with a 26% increase in all-cause mortality, and of the women that continued treatment, nonadherence was associated with a 49% increase in all-cause mortality (Hershman et al., Citation2011). Similarly, low adherence has been associated with increased risk of mortality in CVD (Khalaf et al., Citation2021), diabetes (Ho et al., Citation2006) and end-stage renal disease (Saran et al., Citation2003).
However, it is important to recognise that nonadherence may not always be bad for the patient. It may be protective if the prescription is inappropriate and potentially toxic, or have a neutral effect if the prescription is sub-optimal (Horne et al., Citation2005). In their classic review of the topic, Sackett et al. (Citation1985) consider the prescription of a medicine to be a ‘therapeutic experiment’, the outcome of which is influenced by actions of the prescriber, in selecting an appropriate diagnosis and treatment, as well as the patient in adhering to the regimen. However, if the prescription was evidence-based and appropriate for the patient, then we can probably assume that higher adherence will be associated with greater therapeutic efficacy (Horne et al., Citation2005).
In a review of adherence to long-term therapies the WHO noted that the impact of nonadherence grows as the burden on chronic disease grows worldwide and that the poor are disproportionately affected with a ‘two-way interdependent relationship between economic poverty and chronic disease’ (Sabaté, Citation2003, p.8).
Costs of nonadherence
Nonadherence can have numerous costs in addition to the missed opportunity for health gain for the patient. Nonadherence to medication places a substantial financial burden on healthcare systems. It has recently been estimated that nonadherence costs the European union €80–125 billion each year (European Union/European Commission, Citation2011), and the US $105 billion per year (OECD, 2018). These increased costs are largely driven through increased resource use, with nonadherent patients having higher odds of hospital admissions and Accident and Emergency (A&E) visits (Lee et al., Citation2016; Mongkhon et al., Citation2018; Sun et al., Citation2008), in addition to the costs associated with wasted medications - with unused medicine costs in the UK exceeding £300 million each year (Trueman et al., 2010).
Prevalence of nonadherence
Although it is widely cited that up to 50% of medications are not taken as prescribed (Sabaté, Citation2003), these rates vary considerably across different treatments and conditions, and even within conditions based on the definition and measurement of nonadherence, as well as the stage of nonadherence outlined by Vrijens et al. (Citation2012).
At initiation, it is estimated that around 20–30% of new prescriptions do not get filled (Fischer et al., Citation2011; OECD, Citation2018; Sabaté, Citation2003). A recent systematic review compared initiation rates across asthma, chronic obstructive pulmonary disease (COPD), depression, diabetes mellitus, hyperlipidaemia, hypertension and osteoporosis and found rates of non-initiation were highest amongst those with osteoporosis and hyperlipidaemia (25%) and lowest in those with depression (12%) and diabetes (10%) (Cheen et al., Citation2019).
The majority of research on adherence focuses on implementation, with between 50% and 70% of patients estimated to take their medicine as prescribed, although this varies considerably across conditions. Briesacher et al. (Citation2008) compared adherence rates, measured using prescription refill rates, for 706,032 patients with gout, hypercholesteremia, hypertension, hypothyroidism, osteoporosis, seizure disorders and type 2 diabetes. Adherence rates were highest in hypertension, with 72% of participants having an 80% adherence rate, compared to 55%, 51% and 36% for those with hypercholesteremia, osteoporosis and gout, respectively.
Non-persistence with medicines prescribed for long-term conditions is often problematic with rates of non-persistence increasing steadily from initiation to 2 years (OECD, Citation2018; Yeaw et al., Citation2009). For example, estimates suggest that 16–50% of patients with hypertension discontinue treatment completely within the first 12 months of initiation (Brown & Bussell, Citation2011). Estimates also suggest that 73% of patients with diabetes are persistent 6 months after initiation, with only 39% persistent at 2 years (OECD, Citation2018), and 25–50% of patients with hypercholesterolemia discontinue their statin medication within the first 6–12 months since initiation (Svensson et al., Citation2015). One study exploring adherence to urate-lowering therapy in a large cohort study of 9823 patients with gout found that within 12-month of initiation, non-persistence rates were 56% (Solomon et al., Citation2008). In a longitudinal database study of 4783 patients with hypertension, approximately only 50% of patients who were prescribed an antihypertensive drug continued taking it 12 months after initiation (Vrijens et al., Citation2008).
Correlates and determinants of nonadherence
Studies have identified numerous correlates of nonadherence, with one review of 51 systematic reviews extracting nearly 800 individual factors associated with medication-taking behaviour (Kardas et al., Citation2013). The sheer complexity of the topic presents a challenge for the development of interventions to improve adherence. Unsurprisingly, an important aspect of the adherence literature over the past few decades has been the search for a pragmatic framework to summarise and categorise the numerous correlates of adherence/nonadherence and guide the development of interventions. In a classic review of adherence, the WHO suggested five categories of adherence-related factors that could be targeted in interventions to improve adherence: (i) condition related, (ii) therapy related, (iii) socio-economic-related, (iv) healthcare and system-related and (v) patient-related factors (Sabaté, Citation2003). The approach is based on the observation that adherence can be influenced by a wide range of factors both personal and environmental but also that characteristics of the disease or regimen can also influence adherence. However, when comparing across studies conditions and contexts, the evidence relating to the relative importance of these factors is mixed with many apparent contradictions and conflicting findings as exemplified below using the WHO category labels.
Condition-related factors
Some studies suggest that nonadherence is generally higher in chronic conditions than acute (Cramer et al., Citation2003; Haynes et al., Citation2002; Jackevicius et al., Citation2002; Sustersic et al., Citation2019). Adherence to prophylactic medicines prescribed to prevent a disease may be lower than those to medicines prescribed to treat a disease after diagnosis. For example, a meta-analysis found only 17% of high-risk women prescribed tamoxifen to prevent breast cancer fill their prescription (Smith et al., Citation2016). This is considerably lower than the estimated 75% of those already diagnosed with breast cancer (Sheppard et al., Citation2018). Evidence on the importance of illness severity or disability in predicting adherence is more mixed. Whilst some reviews have suggested that the more severe illness symptoms or disability are, the more adherent a patient is likely to be (Brandes et al., Citation2009; Costello et al., Citation2008; Heestermans et al., Citation2016), other studies (Khdour et al., Citation2012; Lee et al., Citation2018) and reviews (Broekmans et al., Citation2009; Jackson et al., Citation2010) suggest this not to be the case with either null or opposite results. It is clear that severity or seriousness of the condition per se does not determine adherence, as clinically significant rates of nonadherence have been found in life-threatening conditions such as cancer (McGrady & Pai, Citation2019), HIV (Ortego et al., Citation2011) and heart disease (Gupta et al., Citation2021). There is consistent evidence that the presence of comorbid conditions such as depression, anxiety and drug or alcohol misuse can negatively impact adherence (Arrieta et al., Citation2013; DiMatteo et al., Citation2000; Kader et al., Citation2015; Khdour et al., Citation2012; Langebeek et al., Citation2014; Lee et al., Citation2016; Rehm et al., Citation2017; Smaje et al., Citation2018; Yu et al., Citation2018).
Therapy-related factors
Characteristics of a medication regimen can act as barriers to adherence. Although there is little consensus regarding the definition of regime complexity, it comprises various aspects of a regimen, such as number of medicines, number of doses, dose form and the requirement of additional instructions to accompany its use (e.g. to crush tablets, take with a specific fluid or food) (George et al., Citation2004). Some conditions have a relatively simple medication regimen, for example hypercholesterolemia is most commonly treated by taking statins, whereas treatment for non-insulin dependent diabetes can comprise sulfonylurea, biguanide, aspirin, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers and statins. Research clearly suggests that regimen complexity may impede adherence (DiMatteo et al., Citation2012; Liddelow et al., Citation2020; Manzano-García et al., Citation2018; Pantuzza et al., Citation2017). However, reducing the frequency of dosage administrations does not always solve the problem (Claxton et al., Citation2001; Ingersoll & Cohen, Citation2008). We need to look beyond regimen complexity to see how the regimen impacts on the individual (Cooper et al., Citation2010). Some research suggests that the effectiveness of a medicine in terms of symptom relief is related to adherence (Costello et al., Citation2008; Croome et al., Citation2017; Kardas et al., Citation2013; Munro et al., Citation2007; van der Laan et al., Citation2017; Weiner et al., Citation2008), but this is not consistent across studies (Lacro et al., Citation2002; Olthoff et al., Citation2005).
Social and economic factors
Higher costs of drugs (co-payments) and lack of adequate medical/prescription coverage are associated with decreased odds of adherence across conditions (Gourzoulidis et al., Citation2017; Hershman et al., Citation2015; Kardas et al., Citation2013; Sadigh et al., Citation2021; Vermeire et al., Citation2001). There is evidence in some conditions, such as cancer, that a better financial or socioeconomic status has a positive impact on adherence (Hershman et al., Citation2015; Roberts et al., Citation2015), but many other conditions show inconsistent results (Alsabbagh et al., Citation2014; Gast & Mathes, Citation2019; Kardas et al., Citation2013). The impact of economic factors on adherence is complex and an individual’s behaviour in response to financial strains cannot be predicted solely based on their level of income or financial burden, with many patients continuing to take mediation in the face of many financial constraints (Piette et al., Citation2006). The impact of drug costs and income on adherence may vary across different socioeconomic groups, with white Americans and older patients being less likely to see the effect of financial pressures on adherence (Steinman et al., Citation2001). There is evidence that social support, particularly with regards to the quality of the support rather than the mere presence of other people, is associated with increased odds of adherence (DiMatteo, Citation2004; Kardas et al., Citation2013). However, this is not consistently seen across the literature (Gast & Mathes, Citation2019; Ladin et al., Citation2018). There is evidence from conditions such as TB and HIV that social stigma associated with a condition can be associated with decreased adherence, due to fear of disclosure and avoidance of taking medications in public places (Munro et al., Citation2007; Rintamaki et al., Citation2019).
Healthcare and system-related factors
Research suggests poor medication distribution services and long waiting times (Hardon et al., Citation2007), insufficient reimbursement from health insurance plans (Kang et al., Citation2018) and short consultations (Weiss et al., Citation2015) may contribute to nonadherence. Further, research suggests that better patient–clinician communication (e.g. support and trust in a patient-clinician relationship) facilitates adherent behaviour (Beckmann et al., Citation2021; Jackson et al., Citation2010; Kvarnström et al., Citation2021; Matthias et al., Citation2012; Wilson et al., Citation2010). Shared decision making in a consultation opens a dialogue between the patient and clinician through which relevant factors such as possible adverse side-effects, comparative treatment effectiveness and unrealistic expectations can be discussed; the importance of each may vary depending on a patient’s individual circumstances. Reviews demonstrate that patients who engage in shared decision making about their treatment are more likely to be adherent to treatment, compared with those who do not (Ben-Zacharia et al., Citation2018; Joosten et al., Citation2008; Lofland et al., Citation2017; Wheeler et al., Citation2019). For example, a prospective cohort study of 881 women taking tamoxifen for breast cancer found that those who were satisfied with the role they had in their medication decision making process were significantly more likely to be adherent compared with those who were not (Kahn et al., Citation2007).
Patient-related factors
Many studies have investigated the role of patient factors, such as educational status, knowledge and personality and socio-demographic factors such as age and gender as determinants of adherence but the evidence is mixed and sometimes contradictory. There is some evidence suggesting adherence varies with age, although this is not shown consistently. For example, whilst some studies suggest that older adults (e.g. >65) are more likely to be adherent (Chan et al., Citation2010; Curkendall et al., Citation2013; Gemeda et al., Citation2012; Karamanidou et al., Citation2008; Kardas et al., Citation2013; Leclerc et al., Citation2013), other studies (e.g. Hershman et al., Citation2015) and reviews (e.g. Moon et al., Citation2017) show older adults to be less likely to be adherent. Further, some reviews also suggest younger adults to be less adherent (e.g. Karamanidou et al., Citation2008; Moon et al., Citation2017; Weingarten & Cannon, Citation1988), or no relationship between age and adherence at all (Jackson et al., Citation2010).
Some evidence suggests adherence to be associated with ethnicity, with white patients reporting the highest rates of adherence, even when controlling for variables such as income and education (Chan et al., Citation2010; Gast & Mathes, Citation2019; Lewey et al., Citation2013; Moon et al., Citation2019; Simoni et al., Citation2012). However, this is not a consistent finding with some reviews suggesting no relationship (Karamanidou et al., Citation2008; Kardas et al., Citation2013). Further, there is also mixed evidence for other socio-economic factors such as gender, marital status and education (Briesacher et al., Citation2008; Chan et al., Citation2010; Gast & Mathes, Citation2019; Jackson et al., Citation2010; Kardas et al., Citation2013; Manteuffel et al., Citation2014; Reisner et al., Citation2009). Research investigating the relationship between patient knowledge and adherence is inconclusive (Gray et al., Citation2018; Shahin et al., Citation2019). Although some studies report a positive relationship between patient knowledge and adherence (Beer & Skarbinski, Citation2014; Paczkowska et al., Citation2021; Tomaszewski et al., Citation2017), the size of these effects are often small, and other studies have found no evidence of this relationship (Chen et al., Citation2014; Lin et al., Citation2017; Smalls et al., Citation2012). A similar picture emerges in the relationship between health literacy and nonadherence. Some studies report a positive relationship between health literacy and adherence (Barat et al., Citation2001; Lindquist et al., Citation2012); however, meta-analyses suggest any effect is only small (Miller, Citation2016; Zhang et al., Citation2014).
Relatively few studies have examined the relationship between personality traits and adherence (Emilsson et al., Citation2011; Horne, Citation2011). One study suggested that although the role of personality may be indirect, personality traits may influence the beliefs an individual has about their asthma medicines (Emilsson et al., Citation2011). In particular, all five key personality traits (Openness, Conscientiousness, Extraversion, Agreeableness and Neuroticism) were found to be related to judgements about how necessary asthma medication was relative to concerns about taking it, which in turn related to increased adherence.
A comprehensive review commissioned by the UK National Institute of Health Research (NIHR), noted that adherence rates vary not just between people but within the same person over time and across treatments (Horne et al., Citation2005). It was clear that nonadherence is best understood in terms of the interaction between an individual and a particular disease and/or treatment. The review adopted the Perceptions and Practicalities Approach (PaPA), developed by Horne and described below.
The Perceptions and Practicalities Approach (PaPA): a patient centred framework for explaining nonadherence and designing interventions
The PaPA offers a pragmatic framework to understand the fundamentals of adherence, which can guide the development of interventions to support adherence by focussing on the interaction between an individual and their treatment, as recommended in the NICE Medicines Adherence Guidelines (Nunes et al., Citation2009). The PaPA applies health psychology theory and research to delineate the ‘core’ components of adherence support, and highlights the perceptual factors (e.g. medication necessity beliefs, concerns and emotions) and practicalities (e.g. resources and capabilities) that need to be considered and addressed (Horne, Citation2001; Horne et al., Citation2005). The PaPA presents a pragmatic framework from which to understand both intentional (a deliberate decision to not take medicine as prescribed) and unintentional nonadherence (e.g. capacity and resource limitations), and is grounded in the proposition that although a range of intrinsic and extrinsic factors are relevant to adherence, they act through two key factors: motivation and ability.
Whilst much research has sought to identify the role of sociodemographic factors (DiMatteo, Citation2004; Gast & Mathes, Citation2019; Karamanidou et al., Citation2008; Kardas et al., Citation2013; Moon et al., Citation2017; Vangeli et al., Citation2015) and other factors widely assumed to be associated with adherence such as the severity of illness symptoms, prognosis or disability (Bouwman et al., Citation2017; Briesacher et al., Citation2008; DiMatteo, Citation2004; Moon et al., Citation2017), there is huge variation in nonadherence estimates across the literature, with evidence being inconsistent and relationships often indirect. A sociodemographic/trait characteristics approach to understanding adherence has inherent limitations in relation to the design of interventions to support optimal adherence. Even if stable associations existed between sociodemographic or trait characteristics, they would serve to identify certain ‘at risk’ groups so that interventions could be targeted, but could do little to inform the type or content of these interventions (Horne, Citation2011). In contrast, the PaPA proposes that because adherence rates vary not just between individuals but within the same individual over time and across treatment, adherence/nonadherence is best understood in terms of the interaction between an individual and particular disease/treatment. That is not to say that sociodemographic or dispositional characteristics are irrelevant. Rather, the associations with adherence appear to be indirect and are best explained by the influence of sociodemographic and dispositional characteristics on other relevant parameters. For example, correlations between adherence and educational status or race may simply be a reflection of income and ability to afford prescription costs (Piette et al., Citation2006). The key is to understand how sociodemographic and environmental factors influence an individuals’ motivation and ability to engage with the treatment (Horne et al., Citation2019).
An individuals’ motivation can result from conscious decision-making processes and more instinctive, intuitive processes (Kahneman, Citation2012). Similarly, a variety of factors influence an individuals’ ability (e.g. knowledge, clarity of prescribing instructions) (Horne et al., Citation2005; Piette et al., Citation2006). Although some literature suggests that older adults (e.g. >65) may be more likely to be adherent (e.g. Chan et al., Citation2010; Curkendall et al., Citation2013; Gemeda et al., Citation2012; Leclerc et al., Citation2013), the PaPA posits that instead of being a product of age itself, adherence may instead be reflective of how an individual’s age impacts on their motivation and ability to engage with treatment. For example, research has suggested that older adults may be more anxious about their mortality which in turn may increase motivations to adhere (Boyer et al., Citation1990). Research also suggests the presence of comorbid conditions such as depression, anxiety, and drug/alcohol abuse can impact negatively on adherence (Arrieta et al., Citation2013; DiMatteo et al., Citation2000; Kader et al., Citation2015; Khdour et al., Citation2012; Langebeek et al., Citation2014; Lee et al., Citation2018; Rehm et al., Citation2017; Smaje et al., Citation2018; Yu et al., Citation2018). However, these factors may correlate with poor adherence by impeding a patients’ ability to take medicines as prescribed.
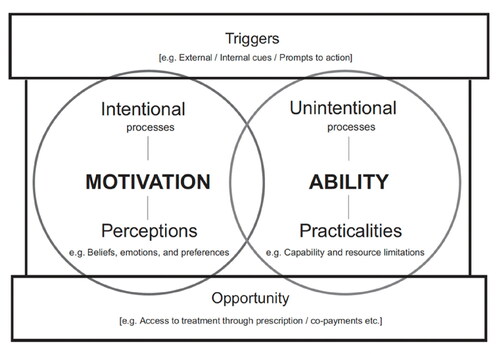
An individuals’ motivation and ability can be influenced by a range of extrinsic factors which facilitate or enable adherent behaviour () such as poor medication distribution services and long waiting times (Hardon et al., Citation2007), insufficient reimbursement from health insurance plans (Kang et al., Citation2018), length of consultation (Weiss et al., Citation2015), having a supportive social network (DiMatteo, Citation2004) and the quality of the communication with healthcare professionals. The importance of such factors is also recognised and represented in the ‘Opportunity’ construct proposed in the Capability Opportunity Motivation-Behaviour (COM-B) model (Michie et al., Citation2011) and the Motivation Opportunity Ability (MOA) model (Ölander & ThØgersen, Citation1995) of behaviour change. The Fogg Behavioural Model (FBM) also highlights the role of these external factors, however replacing ‘Opportunity’ with ‘Triggers’ (Fogg, Citation2009), which can be internal and external and influence both an individual’s motivation and ability. For example, experiencing disease symptoms may motivate adherence if the medicine is believed to be effective in alleviating them.
Figure 2. Perceptions and Practicalities Approach (PaPA) incorporating opportunity and triggers. Reprinted from Horne et al. (Citation2019).
The central role of beliefs
As shown in , a key factor influencing a patient’s motivation to adhere to medication is the beliefs they hold about the treatment and their illness. This is recognised in the Common Sense Model (CSM) of self-regulation which seeks to understand the processes through which individuals make sense of their illness (Leventhal et al., Citation1992, Citation2016). These beliefs sit across five core domains: i) ‘identity’ describing beliefs about the labelling of symptoms and illness, ii) ‘causes’ describing individuals’ perceived causes of their illness, iii) ‘timeline’ describing individuals’ beliefs about the duration of the illness or symptoms, iv) ‘consequences’ describing beliefs about the physical, social and emotional impact the illness has or may have, and v) ‘control’ which describes beliefs about whether the illness can be treated and cured, and the extent to which an individual believes this to be controllable by either themselves or a medical provider.
From a theoretical perspective, the CSM would assume that those who consider the consequences of their illness to be more severe, would be more adherent to prescribed treatment (Llewellyn et al., Citation2003; Schüz et al., Citation2014). However, empirical studies suggest there to only be a weak relationship between illness beliefs and adherence (Aujla et al., Citation2016). The explanatory power of the CSM strengthens as its content becomes more specific to the health behaviour in question (Francis et al., Citation2012), and therefore to gain a better understanding of nonadherence, it is essential to consider how an individual perceives their treatment, as a more proximal driver of medication-taking behaviour (Horne, Citation2003; Horne et al., Citation2019).
Early studies of beliefs about medicines described two types of beliefs: i) specific beliefs about a particular medicine and ii) generalised beliefs about medicines as a class of treatment (Horne et al., Citation1999).
Specific medication beliefs: The Necessity Concerns Framework (NCF)
Studies investigating the beliefs patients hold about treatment have indicated two key types of beliefs influencing adherence: beliefs about how necessary the patient feels a treatment is for them (necessity beliefs), and how concerned they are about taking the treatment (NCF; Horne et al., Citation1999).
Necessity beliefs
Necessity beliefs are representative of a patient’s perceived need for a medicine, or the perception of how able a patient is to cope without their medicine. They can be thought of as the answer to two questions: ‘How much do I need this treatment to achieve a goal that’s important to me?’ and ‘How much can I get away with without using it?’. Perceived necessity is not a form of efficacy belief: people might believe that a treatment will be effective but not that they need it. They might have a low necessity belief even if they understand the scientific evidence for the potential benefits of treatment. This might occur because people do not ‘value’ that particular benefit or perceive it to be important enough to overcome concerns about taking the medicine.
Beliefs about the necessity of a medication can be influenced by how someone perceives their illness. To be convinced of a personal need for ongoing medication, people must first perceive a good fit between the problem (the illness or condition) and the solution (the medicine) (Horne et al., Citation2007; Horne & Weinman, Citation2002). Until they experience a chronic condition, most people’s experience of illness is symptomatic and acute. However, for many long-term conditions the medical rationale for maintenance treatment is based on a prophylaxis model where the benefits of treatment are often silent and long-term. This may be in stark contrast to the intuitive model of ‘no symptoms; no problem’. Similarly, missing doses may not lead to an immediate deterioration in symptoms, reinforcing the erroneous perception that high adherence to the medication may not be necessary. Related to this is the fact that people often stop taking treatment when they judge that the condition has improved. These judgments are often based on potentially misleading symptom perceptions rather than on objective clinical indicators of disease severity (Cooper et al., Citation2009). Determining the necessity of a treatment may also be influenced by notions of self. There has been disappointingly little research in this area, but perceptions that one can resist the progress of disease by drawing on sources of ‘inner strength’, ‘hardiness’ or by keeping a ‘positive outlook’ emerged as reasons for deciding not to start clinically indicated antiretroviral treatments in interviews with human immunodeficiency virus (HIV) positive men (Cooper et al., Citation2002).
The importance of necessity beliefs in explaining nonadherence has been demonstrated across a range of chronic health conditions (Clatworthy et al., Citation2009; Foot et al., Citation2016; Mitzel & Vanable, Citation2020; West et al., Citation2020). For example, a meta-analysis of 94 studies (N = 25,072) found significant relationships between necessity beliefs and adherence with every standard deviation increase in necessity beliefs increasing the odds of non-adherence by a factor of 1.7 (OR = 1.742, 95% CI [1.569, 1.934]) (Horne et al., Citation2013).
Medication concerns
Individuals report a range of concerns about taking medicines. Perhaps the most obvious of which surrounds medicine side effects and the wider disruption to daily life sometimes caused by medicines. This is illustrated in one study by Ogden and Sidhu (Citation2006) who interviewed 12 participants taking orlistat for weight management and findings suggested that for some, the experience of unpleasant and highly visible medicine side-effects was related to nonadherence to orlistat. The impact of medication side-effects on nonadherence has been studied widely, although has not been demonstrated consistently (Costello et al., Citation2008; Croome et al., Citation2017; Kardas et al., Citation2013; Lacro et al., Citation2002; Munro et al., Citation2007; Olthoff et al., Citation2005; van der Laan et al., Citation2017; Weiner et al., Citation2008; Yeam et al., Citation2018). There is evidence to suggest that perceptions of side effects (e.g. how confident someone feels about managing the side effects or the relative importance of these side effects against necessity beliefs) may be more important influencers of adherence than the physical experience of side effects (Shelby et al., Citation2014). Many people also have concerns that regular medication usage may lead to long-term harmful effects or dependence (Chater et al., Citation2014; Horne et al., Citation1999).
Other commonly reported concerns relate to immunity or tolerance to medicines changing over time, and preferences for alternative or natural medicine or therapies (Gill & Williams, Citation2001; Horne et al., Citation2009). These concerns are commonly reported by patients across a range of illnesses, illness states and population groups (Chapman et al., Citation2014; Clatworthy et al., Citation2009; Horne et al., Citation1999; Horne, Citation2001; Horne et al., Citation2009). Concerns can also be reflective of the meanings that individuals attach to medicines, and changes in how individuals see themselves and how they perceive they are seen by others. Regularly taking a medicine may be an unwelcome reminder of an illness that has a negative impact on how people see themselves or perceive they are seen by others, and therefore nonadherence may sometimes function as an implicit strategy to protect their sense of self (Cooper et al., Citation2002; Horne, Citation2003).
There is consistent evidence across conditions to show the importance of medication concerns in understanding adherence (Clatworthy et al., Citation2009; Foot et al., Citation2016; Mitzel & Vanable, Citation2020; West et al., Citation2020). For example, one meta-analysis of 94 studies (N = 25,072) found significant relationships between adherence and reported concerns, with the odds of adherence decreasing by a factor of 2 with every standard deviation increase in concerns (OR = 0.502, 95% CI: [0.450, 0.560]) (Horne et al., Citation2013). Another review in HIV showed that concerns had a small but clinically significant impact on HIV treatment adherence (Mitzel & Vanable, Citation2020).
The necessity-concerns differential
Although both necessity beliefs and concerns are independent predictors of adherence, it is perhaps more valuable to understand the interaction between the two. For example, research suggests that holding strong beliefs that a medicine is necessary does not necessarily lead to adherence, unless it is coupled with low concerns about taking a medicine (West et al., Citation2020). Additionally, research indicates that an individual with high necessity beliefs and high concerns may be more likely to experience uncertainty and be less likely to be adherent (Moon et al., Citation2017). To assess the extent to which necessity beliefs and concerns may be weighed up against each other, the Necessity Concerns differential (NCD) can be used, whereby an individuals’ average concerns about a medicine is subtracted from their average beliefs about the necessity of taking a medicine (Horne et al., Citation2004). A positive NCD score indicates that ratings of personal need for the medication are relatively greater than ratings of concern. Although there are methodological limitations with this approach, a meta-analysis of 94 studies demonstrated the NCD (r = 0.24) to be a stronger predictor of medication adherence compared with necessity beliefs (r = 0.17) or concerns (r = −0.18) alone (Foot et al., Citation2016). Findings indicated that those who had greater concerns about medicines compared to their necessity beliefs were significantly less adherent.
General beliefs and medicines and pharmaceutical schema
Representations of specific medicines are influenced by more general beliefs (social representations) about medicines as a class of treatment (Horne et al., Citation1999). Many people are suspicious of pharmaceuticals, perceiving them to be fundamentally harmful, addictive substances that should not be taken for long periods of time, and which tend to be over-prescribed by doctors (Horne et al., Citation1999). Moreover, the dangerous aspects of medication are often linked to their ‘chemical’/’unnatural’ origins and to suspicions of the pharmaceutical industry as well as wider concerns about science, medicine and technology (Faasse et al., Citation2009; Green et al., Citation2013; Gupta & Horne, Citation2001; Horne et al., Citation1999; Howland, Citation2020; Petrie et al., Citation2005).
People also vary in their perceptions of personal sensitivity to the effects of medicines, with many believing that they are more sensitive than other people to the effects of medicines. People with this view tend to have more negative views about pharmaceutical medicines and vaccinations, and to be more reluctant to take medication or receive vaccinations (Horne et al., Citation2013). Taken together these sets of beliefs about medicines and about self in relation to medicines can be thought of as ‘pharmaceutical schema’, or how ideas about pharmaceuticals are organised.
Negative pharmaceutical schema are associated with greater concerns that specific medication will result in harm, greater doubts about the personal need to take it and lower reported adherence (Chapman et al., Citation2014; Horne et al., Citation2009; Tolu et al., Citation2020). They influence the way in which information about the potential benefits and harms of a specific treatment are processed. In experimental studies, people with a more negative pharmaceutical schema are more likely to think that symptoms are caused by the drug (i.e. attribute symptoms as side-effects) (Heller et al., Citation2015) and less likely to recall side-effects correctly (Heller et al., Citation2017).
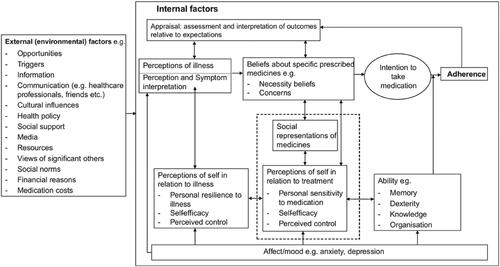
presents a high-level overview of the PaPA, summarising the interplay between perceptual and practical barriers (internal) and environmental (external) factors impacting on adherence, whereby internal factors are influenced by external factors.
Figure 3. Perceptions and Practicalities Approach – a detailed conceptual map of adherence. Reprinted from Horne et al. (Citation2019).
Future directions for research on correlates of nonadherence
Although extensive research has explored the correlates of nonadherence, as outlined above, there are considerable limitations with traditional approaches to mapping correlates of nonadherence (e.g. the WHO framework). We need research that informs the development of innovative ways to help patients get the best from effective treatments. There is already extensive research identifying correlates of nonadherence which can be used to identify risk factors for nonadherence. But we need to move beyond risk factors for nonadherence to a better understanding of how particular correlates impact on individuals over time and across treatments. We therefore recommend that future research should seek to do the following:
Focus on the interaction between an individual and a particular disease/treatment
A key limitation with traditional approaches of mapping correlates of nonadherence is that the extent to which a given correlate will be influential will vary from one individual to another, and even within the same individual over time (Horne et al., Citation2005). We therefore suggest that future research focuses on the interaction between an individual and a particular disease and/or treatment. There is need for a better understanding of how the potential determinants of adherence impact on the motivation and ability of individuals to adhere to the recommendations over time and across different treatment modalities. In particular, it would be useful for future research to elucidate possible mechanisms of interaction in order to inform theoretical frameworks that can form the foundations of pragmatic interventions. We need a better understanding of how societal factors (e.g. access to resources and treatment opportunities) and environmental factors (e.g. culture and healthcare systems) impact on individuals by influencing modifiable correlates of nonadherence.
Focus on modifiable factors relating to nonadherence
Another limitation with sociodemographic/trait characteristic approaches to exploring correlates of nonadherence is that they often focus on identifying unmodifiable factors relating to nonadherence. Even if stable associations existed between characteristics, these often only serve to identify groups ‘at risk’ of nonadherence, without furthering our understandings of why, or what we can do about it (Horne, Citation2011). We therefore highlight that a key priority for future research should be to identify modifiable factors relating to nonadherence which can then be the focus of adherence support interventions at the level of the individual. Further, it would also be helpful for research to consider how unmodifiable factors, such as age or culture may act through modifiable factors, such as an individuals’ motivation and/or ability to take a treatment, for example, by influencing perceptual (e.g. how necessary they perceive their treatment to be) and practical barriers (e.g. difficulty remembering to take their treatment) towards taking their treatment.
Apply theoretical frameworks to understand correlates of nonadherence that can be used to guide intervention design
Even where modifiable factors are explored, these research approaches are often not grounded in theory. To be of most use for the development of interventions to support adherence, future research should seek to develop and apply theoretical frameworks which aim to synthesise multiple correlates into a coherent and pragmatic model that can be used to guide the development of interventions. In this article, we discuss the PaPA as an example of a framework that can be used in this way.
Triangulate measurements of nonadherence
As highlighted earlier in this article, there are several limitations associated with how nonadherence is often measured. It is therefore suggested that future research seeks to explore a combined approach to measuring nonadherence (Dobbels et al., Citation2010), whereby self-report measures are combined with objective forms of adherence measures, such as prescription refill rates or electronic monitoring to produce amalgamated, comprehensive assessments of adherence. Taking such an approach could help to improve measurement accuracy by overcoming some of the limitations associated with using single methods (Chan et al., Citation2020).
Interventions to support adherence
Given the widespread prevalence and health impact of nonadherence, and the recognition that some of the core determinants of nonadherence are modifiable, interventions to support adherence hold huge potential and may have a ‘far greater impact on the health of the population than any improvement in specific medical treatments’ (Sabaté, Citation2003, p. 21). A complication to the adherence literature is that adherence support interventions can target several different ‘levels’: i) the healthcare system (e.g. improving the opportunity to access medicines), ii) patient-provider interactions (e.g. improving clinician-patient communication) and iii) the patient (e.g. improving an individual’s motivation and ability to adhere) (Horne et al., Citation2005). Although interventions targeting social and environmental processes and factors are important, their effectiveness will also be dependent on patient-level factors, such as an individuals’ motivation and ability. Therefore, interventions targeting patient-level factors are of focus here.
Many interventions have been designed to support adherent behaviour across a range of conditions and treatments with varying degrees of efficacy (e.g. Chan et al., Citation2018; Conn et al., Citation2016; Conn & Ruppar, Citation2017; Horne, Citation1998; Kripalani et al., Citation2007; MacDonald et al., Citation2016; Nieuwlaat et al., Citation2014; Pearce et al., Citation2022). One systematic review found that only 16 out of 37 trials reported an improvement in adherence across chronic conditions, and suggested that interventions involving monitoring and feedback, or reducing dosing demands were most likely to be effective (Kripalani et al., Citation2007). Further, a large systematic review and meta-analysis of 771 intervention trials found evidence that although interventions can be successful in improving adherence, these effects are typically small, with room for improvement (average effect size r = 0.29). Findings also highlighted that interventions focussed on habit formation and behavioural strategies were most likely to be associated with improved adherence (Conn & Ruppar, Citation2017). One commonly used and successful method for habit formation is the development of implementation intentions, linking the taking of a medication to a specific environmental cue, such as brushing teeth. Implementation intentions have been shown to be an effective tool to improve adherence to medicines (Brown et al., Citation2009; Jackson et al., Citation2006; O’Carroll et al., Citation2013). For example, Brown et al. (Citation2009) showed this approach to significantly improve adherence to antiepileptic medication in a simple randomised control trial of 69 patients with epilepsy. Participants in the intervention group completed a short questionnaire linking taking their medication with a particular time, place or other activity; 93.4% of doses were taken in the intervention group compared with only 55.3% in controls.
Reviews such as these have been augmented by a series of Cochrane reviews, using stringent inclusion criteria to explore the effectiveness of interventions to improve medication adherence. The most recent review was conducted in 2014 and included 182 RCTs with a total of 46,962 participants (Nieuwlaat et al., Citation2014). The most commonly studied conditions were HIV/AIDS, psychiatric disorders, COPD, CVD or risk, hypertension and diabetes. Only 17 studies had a low risk of bias for both the study design and the primary clinical outcome; from these, three reported an improvement in adherence, and five reported an improvement in both adherence and clinical outcomes. Further, the interventions that did report an improvement in both adherence and clinical outcomes tended to be complex and difficult to implement at a low cost. For example, Ellis et al. (Citation2012) reported higher rates of adherence and lower HbA1c levels with a highly intensive, home-based tailored family multisystemic therapy-based intervention. Lester et al. (Citation2009), however, showed improvements in adherence and suppression in viral load in patients with HIV following an interactive SMS intervention, which holds more promise for successful implementation, especially in low resource settings. Overall, the authors of this review concluded that there was a lack of convincing evidence among studies with the lowest risk of bias, and that there was still a need to pursue effective interventions to support medication adherence to improve clinical outcomes (Nieuwlaat et al., Citation2014).
The disappointing findings highlighted in this Cochrane review may be due to two common limitations with adherence support interventions; (1) that they often do not have a strong theoretical basis, and (2) that few interventions address both perceptual and practical barriers to adherence. Theory-based interventions provide a better understanding of what to target in an intervention by specifying a set of potential mechanisms of change, which help to evaluate which elements work well within the intervention. They also help with replicating the intervention results and reproducing the interventions across different contexts or behaviours (Michie et al., Citation2008). Theory-based interventions also seem to be more effective in improving adherence. For example, a meta-analysis investigating the use of theory- or model-linked adherence interventions in 146 comparisons, found an overall effect size of d = 0.32 for the intervention groups compared with control groups (Conn et al., Citation2016), which although is small, is larger than for simple adherence reminder interventions reporting effect sizes around d = 0.1 (Fenerty et al., Citation2012).
Social cognition models (e.g. Theory of Planned Behaviour (TPB; Ajzen, Citation1985)) and other integrated models of behaviour change (e.g. COM-B; Michie et al., Citation2011) are often used to help us understand individual variation in health behaviours by providing a structural and systematic approach to examining the predictors and antecedents of health behaviour. In terms of applications of the TPB, a meta-analysis of 27 studies suggests adherence support interventions grounded in the TPB may be effective (Rich et al., Citation2015). Across a range of 12 chronic conditions (e.g. heart disease, hypertension, breast cancer and epilepsy) significant effect sizes ranged from r = 0.22 to r = 0.51, although most of these were either small or medium in size, particularly for the intention-behaviour relationship (Rich et al., Citation2015). In addition, a recent randomised control trial of 60 participants with asthma, demonstrated an educational intervention based on the TPB to be effective at increasing asthma control and adherence (Şanlıtürk & Ayaz-Alkaya, Citation2021). Several studies have begun to apply the COM-B to adherence support (Jackson et al., Citation2014). For example, Félix et al. (Citation2019) applied COM-B and the Behaviour Change Wheel (BCW) to their intervention to support adherence to antidiabetic medication in older adults via an anthropomorphic virtual assistant, and drew upon a range of behaviour change techniques (BCTs), such as action planning and biofeedback to address key intervention functions, such as enablement and education. Additionally, Ribaut et al. (Citation2020) have reported on their development of an intervention applying the BCW and COM-B to support adherence to immunosuppressants in allogeneic stem cell transplantation. However, as of yet, these interventions have not been formally evaluated.
In addition to lacking a strong theoretical basis, few adherence support interventions address perceptions as well as practical barriers to adherence, which may help to explain why some interventions that only tackle practical barriers often have limited effects on adherence. Although there is some evidence that strategies, such as providing home delivery of medicines free of charge can improve adherence by removing practical barriers and making it easier for patients to access their medicines (Zillich et al., Citation2012), other interventions show less positive results. For example, in a systematic review of 30 studies investigating the effectiveness of medication reminder packaging (such as weekly pill boxes), only 16 studies showed a positive effect on clinical adherence outcomes, and only three included studies were deemed methodologically strong (Boeni et al., Citation2014). Another review of 17 studies found that interventions using regimen simplification strategies were largely not effective at improving adherence (Elnaem et al., Citation2020).
Similarly, a meta-analysis and systematic review of 19 trials exploring the effectiveness of mobile phone interventions to improve adherence to antiretroviral therapy (ART) in HIV found that text message reminder interventions largely did not significantly improve adherence, however when reminders were accompanied by BCTs, links to support and interactivity, there were improvements in adherence (Shah et al., Citation2019). These findings highlight the importance of addressing both perceptions and practicalities influencing adherence. Tailoring support to the needs to the individual, as recommend in the PaPA and endorsed by the NICE guidelines in both 2009 and 2016 for involving patients in decisions about prescribed medicine and supporting adherence (Nunes et al., Citation2009), is likely to further increase the efficacy of the intervention (Mes et al., Citation2018).
The PaPA recommends that adherence support should include three core components: (1) address necessity beliefs by providing a common-sense rationale for medication necessity, which fits within the patient’s existing beliefs about the illness and treatment, (2) elicit and address concerns about the treatment and (3) address any practical barriers by making the treatment as easy and convenient as possible. In addition to addressing these three elements, a key recommendation of the PaPA is to take a ‘no-blame’ approach to facilitating informed adherence (Horne et al., Citation2019), that encourages a frank and open discussion about nonadherence that allows the patient to express any doubts or concerns about the prescription. Accurate rates of nonadherence are hard to obtain, as patients are often wary of disclosing nonadherence for fears of being branded a ‘bad patient’, disappointing the prescriber, so it remains a ‘hidden problem’ (Horne et al., Citation2005; Thorneloe et al., Citation2017).
Interventions applying the principles of the PaPA show promise in improving adherence-related perceptions and self-reported adherence across a range of health conditions (e.g. Chapman et al., Citation2020; Moon et al., Citation2019; O’Carroll et al., Citation2013; Odeh et al., Citation2019). For example, in a brief intervention to improve adherence to preventative stroke medication by O’Carroll et al. (Citation2013), 62 survivors of stroke were randomly allocated to: i) either receive a two-session intervention, through which implementation intentions were developed to help with habit formation and tackle practical barriers, and any false patient perceptions about their medication and/or illness were addressed, or ii) a control group. Findings showed in a 10% increase in adherence for the intervention group. These approaches have also been successfully delivered through digital channels (Chapman et al., Citation2020; Petrie et al., Citation2012). Success has also been demonstrated in a pharmacist-led, post-discharge telephone follow-up intervention for polypharmacy patients (Odeh et al., Citation2019). In these telephone calls, pharmacists discussed any practical or perceptual problems patients were experiencing with their treatment and illness, assessed patients’ ability to manage their medication regime and provided practical tailored advice to help patients overcome barriers to adherence. Patients in the intervention group had significantly lower hospital readmission rates, stronger medication necessity beliefs and self-reported adherence compared with controls.
The PaPA suggests that to have most success in supporting adherence, interventions should be tailored to address the specific perceptual and practical barriers experienced by an individual (Horne et al., Citation2019). This notion is supported by research that consistently demonstrates that tailored interventions are likely to be more effective than non-tailored interventions (Gatwood et al., Citation2016; Horne et al., Citation2019; Kassavou & Sutton, Citation2017, Citation2018; Lustria et al., Citation2013; Noar et al., Citation2007, Citation2011; Sainsbury et al., Citation2020). For example, a recent multivariable meta-regression analysis found that tailoring to a patient’s needs and preferences explained the largest variance in adherence effect sizes (Kassavou & Sutton, Citation2018). Once the specific perceptual and practical barriers facing that patient are elicited, interventions tailored to address these specific barriers can be used to address them. This approach has been demonstrated to be effective in improving adherence across a range of conditions and treatments such as stroke, asthma, CVD and inflammatory bowel disease (IBD) (Chapman et al., Citation2020; Clifford et al., Citation2006; O’Carroll et al., Citation2013; Odeh et al., Citation2019). For example, one intervention to improve adherence in 329 patients with IBD used a pre-screening tool to identify participants’ personal beliefs about IBD and maintenance treatment (Chapman et al., Citation2020). Personalised tailored messages then sought to address these beliefs and provided advice on tackling practical difficulties with taking their medication. At 3-month follow-up patients who received the intervention had significantly fewer concerns about taking their IBD medication, fewer doubts about the necessity of their treatment and higher reported adherence.
Ethics of adherence interventions
It is important to highlight in this article that we recognise adherence may not always be a ‘good’ or the ‘right’ thing. Medicines often have side-effects, some of which may be mild but unpleasant to experience, such as headache, nausea, fatigue, insomnia and others which may be more severe. As such, a result of encouraging patients to adhere to their prescribed medicines could be the experience of unwanted and sometimes harmful side-effects, emphasising that helping patients make informed choices about treatment should be integral to adherence support (Horne et al., Citation2019). The assumption therefore is that adherence is appropriate and beneficial if it follows a process that allows patients to participate in the decision-making process, and that an appropriate choice of medicine is facilitated by the prescriber.
Recommendations for future interventions
As highlighted above, the PaPA suggests that the key to developing effective adherence support is to make sure that both perceptual and practical barriers to adherence are considered, e.g. that interventions address both an individuals’ motivation and ability. In lieu of this, and the common limitations and challenges associated with many previous interventions to support adherence, this article concludes with our recommendations for future interventions based on principles outlined in the PaPA and endorsed by NICE.
Have a strong theoretical basis
Existing interventions often lack a strong theoretical basis, which makes it challenging to draw conclusions about why an intervention may or may not have been successful. Interventions are also often very poorly described with little clarity on what has been included in the intervention. Even when an intervention is theory based and well described, it can still be difficult to disentangle why or how it has worked, without the use of process evaluations. One approach to achieve this is through the use of the Behaviour Change Technique (BCT) Taxonomy which provides a consistent terminology for describing the active ingredients of behaviour change interventions (Abraham & Michie, Citation2008; Michie et al., Citation2013). Conducting a process evaluation and investigating mechanisms of action provides important information on how the intervention may be working to improve adherence. Therefore, future interventions should (i) clearly describe the content of their intervention, (ii) describe the theoretical basis of the intervention and (iii) conduct process evaluations to ascertain how the intervention may have worked.
Consider both perceptual and practical barriers to adherence
Interventions that seek to address both perceptual and practical barriers to adherence are likely to be more effective, especially when intentional and unintentional nonadherence are considered as separate behaviours (Horne et al., Citation2005). This is important because studies have suggested them to have unique determinants and therefore different strategies may be necessary to address each type of behaviour. Therefore, future interventions should seek to address both perceptual and practical barriers to adherence. Examples for strategies and BCTs to do so can be found in Horne et al. (Citation2019).
Tailor to an individual’s needs
Many previous interventions have employed a ‘one-size fits all’ approach, assuming barriers to adherence are similar across patients. However, both perceptions and practical barriers are likely to vary significantly between individuals and even within the same individual over time. As such, there is now a need for adherence interventions to follow principles of precision medicine, and tailor interventions to the specific barriers and issues relevant to each patient to increase the likelihood of success.
Optimise the content, context and channel of delivery
In addition to ensuring that the content of the intervention is appropriate and tailored to an individual’s needs, it is also important that the context surrounding the intervention (e.g. employment status, availability of transport, internet connection, etc.) and the channel of delivery (e.g. text messaging, digital app, healthcare professional, etc.) are optimised to the individual (Dombrowski et al., Citation2016; Horne et al., Citation2019; Tucker et al., Citation2017). For example, a digital mHealth intervention to support adherence in older adults in residential care may not be the most appropriate choice to achieve maximum engagement and efficacy. Therefore, there is value in future interventions considering the unique barriers that the channel and context surrounding the intervention may present. This could by achieved by taking a person-based approach to the design and testing of interventions by involving and consulting members of the target population (Yardley et al., Citation2015).
Consider who is at most benefit of interventions
Many adherence intervention trials do not screen for nonadherence in their participants (Jeffery et al., Citation2014), meaning that the majority of included participants may have high adherence levels, creating a ceiling effect in which it becomes difficult to show any true beneficial effects of the intervention (Mathes et al., Citation2014). Moving forwards, it is therefore suggested that researchers screen patients and invite those who are either already nonadherent or at risk for nonadherence, as these patients will benefit most from intervention. This is particularly important considering that there is already likely to be a bias in the more adherent patients being more likely to agree to take part in a trial.
Conclusions
Prescribing pharmaceutical medicines is one of the most significant investments in healthcare and is pivotal in the management of long-terms conditions that count the lion’s share of health expenditure. However, health and economic outcomes are compromised by high levels of nonadherence which are observed across disease, cultures and healthcare systems world-wide. The causes of nonadherence are complex but can best be understood in terms of the perceptions and practicalities influencing individual motivation and ability to adhere within an environmental and social context.
Studies examining patient perspectives of adherence show that nonadherence often represents a choice on the part of the patient based on their understandings and experience of the illness and treatment. These may differ from the medical view or evidence base, but often represent a ‘common-sense’ course of action in the mind of the patient. Nonadherence is often hidden because patients are often reluctant to admit to nonadherence or reveal the doubts and concerns that underpin because they fear the disapproval of healthcare providers.
Improving adherence is challenging, but recent developments in theory and research suggest that the PaPA, which emphasises a no-blame interaction with patients, in which support is tailored to identify and address the specific beliefs and abilities determining adherence, can improve adherence in cost-effective ways.
In light of common limitations associated with medication nonadherence research, this article presents a series of recommendations for future research to overcome these in terms of identifying correlates of nonadherence, and interventions to support adherence.
Permissions
is reprinted with permission from John Wiley and Sons; https://www.wiley.com/en-us/Health+Psychology%2C+2nd+Edition-p-9781405194600. is reprinted with permission from John Wiley and Sons; https://bpspubs.onlinelibrary.wiley.com/doi/10.1111/j.1365-2125.2012.04167.x. and are reprinted with permission from European Psychologist (2019),24(1), 82–96. ©2019 Hogrefe Publishing; www.hogrefe.com; https://doi.org/10.1027/1016-9040/a000353.
Table 1. Methods for measuring medication adherence.
Disclosure statement
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. Speaker engagements with honoraria with the following companies: AbbVie, Abbott, Amgen, Astellas, AstraZeneca, Boehringer Ingelheim, Biogen, Gilead Sciences, GlaxoSmithKline, Janssen, Merck Sharp Dohme, Merck, Novartis, Pfizer, Procter & Gamble, Roche, Sanofi, Shire Pharmaceuticals, TEVA, UCB. Professor Rob Horne is Founding Director of a UCL-Business company (Spoonful of Sugar Ltd) providing consultancy on treatment engagement and patient support programmes to healthcare policy makers, providers and pharmaceutical industry.
Funding
Professor Rob Horne is supported by the National Institute for Health Research (NIHR, Collaboration for Leadership in Applied Health Research and Care (CLAHRC), North Thames at Bart’s Health NHS Trust and Asthma UK (AUKCAR).
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
References
- Abraham, C., Conner, M., Jones, F., & O’Connor, D. (2016). Health psychology (2nd ed.). Routledge. https://doi.org/10.4324/9781315776453
- Abraham, C., & Michie, S. (2008). A taxonomy of behavior change techniques used in interventions. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 27(3), 379–387. https://doi.org/10.1037/0278-6133.27.3.379
- Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & J. Beckmann (Eds.), Action control: From cognition to behavior (pp. 11–39). Springer. https://doi.org/10.1007/978-3-642-69746-3_2
- Aldeer, M., Javanmard, M., & Martin, R. P. (2018). A review of medication adherence monitoring technologies. Applied System Innovation, 1(2), 14. https://doi.org/10.3390/asi1020014
- Alsabbagh, M. H. D. W., Lemstra, M., Eurich, D., Lix, L. M., Wilson, T. W., Watson, E., & Blackburn, D. F. (2014). Socioeconomic status and nonadherence to antihypertensive drugs: A systematic review and meta-analysis. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 17(2), 288–296. https://doi.org/10.1016/j.jval.2013.11.011
- Arrieta, Ó., Angulo, L. P., Núñez-Valencia, C., Dorantes-Gallareta, Y., Macedo, E. O., Martínez-López, D., Alvarado, S., Corona-Cruz, J.-F., & Oñate-Ocaña, L. F. (2013). Association of depression and anxiety on quality of life, treatment adherence, and prognosis in patients with advanced non-small cell lung cancer. Annals of Surgical Oncology, 20(6), 1941–1948. https://doi.org/10.1245/s10434-012-2793-5
- Aujla, N., Walker, M., Sprigg, N., Abrams, K., Massey, A., & Vedhara, K. (2016). Can illness beliefs, from the common-sense model, prospectively predict adherence to self-management behaviours? A systematic review and meta-analysis. Psychology & Health, 31(8), 931–958. https://doi.org/10.1080/08870446.2016.1153640
- Barat, I., Andreasen, F., & Damsgaard, E. M. S. (2001). Drug therapy in the elderly: What doctors believe and patients actually do. British Journal of Clinical Pharmacology, 51(6), 615–622. https://doi.org/10.1046/j.0306-5251.2001.01401.x
- Beckmann, K., Cahill, D., Brown, C., Van Hemelrijck, M., & Kinsella, N. (2021). Understanding reasons for non-adherence to active surveillance for low-intermediate risk prostate cancer. Translational Andrology and Urology, 10(6), 2728–2736. https://doi.org/10.21037/tau-20-1254
- Beer, L., & Skarbinski, J. (2014). Adherence to antiretroviral therapy among HIV-infected adults in the United States. AIDS Education and Prevention: Official Publication of the International Society for AIDS Education, 26(6), 521–537. https://doi.org/10.1521/aeap.2014.26.6.521
- Ben-Zacharia, A., Adamson, M., Boyd, A., Hardeman, P., Smrtka, J., Walker, B., & Walker, T. (2018). Impact of shared decision making on disease-modifying drug adherence in multiple sclerosis. International Journal of MS Care, 20(6), 287–297. https://doi.org/10.7224/1537-2073.2017-070
- Boeni, F., Spinatsch, E., Suter, K., Hersberger, K. E., & Arnet, I. (2014). Effect of drug reminder packaging on medication adherence: A systematic review revealing research gaps. Systematic Reviews, 3(1), 29. https://doi.org/10.1186/2046-4053-3-29
- Bouwman, L., Eeltink, C. M., Visser, O., Janssen, J. J. W. M., & Maaskant, J. M. (2017). Prevalence and associated factors of medication non-adherence in hematological-oncological patients in their home situation. BMC Cancer, 17(1), 739. https://doi.org/10.1186/s12885-017-3735-1
- Boyer, C. B., Friend, R., Chlouverakis, G., & Kaloyanides, G. (1990). Social support and demographic factors influencing compliance of hemodialysis patients1. Journal of Applied Social Psychology, 20(22), 1902–1918. https://doi.org/10.1111/j.1559-1816.1990.tb01517.x
- Brandes, D. W., Callender, T., Lathi, E., & O’Leary, S. (2009). A review of disease-modifying therapies for MS: Maximizing adherence and minimizing adverse events. Current Medical Research and Opinion, 25(1), 77–92. https://doi.org/10.1185/03007990802569455
- Briesacher, B. A., Andrade, S. E., Fouayzi, H., & Chan, K. A. (2008). Comparison of drug adherence rates among patients with seven different medical conditions. Pharmacotherapy, 28(4), 437–443. https://doi.org/10.1592/phco.28.4.437
- Broekmans, S., Dobbels, F., Milisen, K., Morlion, B., & Vanderschueren, S. (2009). Medication adherence in patients with chronic non-malignant pain: Is there a problem? European Journal of Pain, 13(2), 115–123. https://doi.org/10.1016/j.ejpain.2008.02.010
- Brown, I., Sheeran, P., & Reuber, M. (2009). Enhancing antiepileptic drug adherence: A randomized controlled trial. Epilepsy & Behavior, 16(4), 634–639. https://doi.org/10.1016/j.yebeh.2009.09.014
- Brown, M. T., & Bussell, J. K. (2011). Medication adherence: WHO cares? Mayo Clinic Proceedings, 86(4), 304–314. https://doi.org/10.4065/mcp.2010.0575
- Castillo-Mancilla, J. R., & Haberer, J. E. (2018). Adherence measurements in HIV: New advancements in pharmacologic methods and real-time monitoring. Current HIV/AIDS Reports, 15(1), 49–59. https://doi.org/10.1007/s11904-018-0377-0
- Chan, A. H., De Simoni, A., Wileman, V., Holliday, L., Chisari, C., Newby, C. J., Taylor, S. J., Fleming, L. J., Griffiths, C. J., & Horne, R, Cochrane Airways Group. (2018). Digital interventions to improve adherence to maintenance medication in asthma. Cochrane Database of Systematic Reviews, 5, Cd013030. https://doi.org/10.1002/14651858.CD013030
- Chan, A. H. Y., Horne, R., Hankins, M., & Chisari, C. (2020). The Medication Adherence Report Scale: A measurement tool for eliciting patients’ reports of nonadherence. British Journal of Clinical Pharmacology, 86(7), 1281–1288. https://doi.org/10.1111/bcp.14193
- Chan, A. H. Y., Reddel, H. K., Apter, A., Eakin, M., Riekert, K., & Foster, J. M. (2013). Adherence monitoring and e-health: How clinicians and researchers can use technology to promote inhaler adherence for asthma. The Journal of Allergy and Clinical Immunology, 1(5), 446–454. https://doi.org/10.1016/j.jaip.2013.06.015
- Chan, D. C., Shrank, W. H., Cutler, D., Jan, S., Fischer, M. A., Liu, J., Avorn, J., Solomon, D., Brookhart, M. A., & Choudhry, N. K. (2010). Patient, physician, and payment predictors of statin adherence. Medical Care, 48(3), 196–202. https://doi.org/10.1097/MLR.0b013e3181c132ad
- Chapman, S. C. E., Horne, R., Chater, A., Hukins, D., & Smithson, W. H. (2014). Patients’ perspectives on antiepileptic medication: Relationships between beliefs about medicines and adherence among patients with epilepsy in UK primary care. Epilepsy & Behavior, 31, 312–320. https://doi.org/10.1016/j.yebeh.2013.10.016
- Chapman, S., Sibelli, A., St-Clair Jones, A., Forbes, A., Chater, A., & Horne, R. (2020). Personalised adherence support for maintenance treatment of inflammatory bowel disease: A tailored digital intervention to change adherence-related beliefs and barriers. Journal of Crohn’s & Colitis, 14(10), 1394–1404. https://doi.org/10.1093/ecco-jcc/jjz034
- Chater, A. M., Parham, R., Riley, S., Hutchison, A. J., & Horne, R. (2014). Profiling patient attitudes to phosphate binding medication: A route to personalising treatment and adherence support. Psychology & Health, 29(12), 1407–1420. https://doi.org/10.1080/08870446.2014.942663
- Cheen, M. H. H., Tan, Y. Z., Oh, L. F., Wee, H. L., & Thumboo, J. (2019). Prevalence of and factors associated with primary medication non-adherence in chronic disease: A systematic review and meta-analysis. International Journal of Clinical Practice, 73(6), e13350. https://doi.org/10.1111/ijcp.13350
- Chen, A. M. H., Yehle, K. S., Albert, N. M., Ferraro, K. F., Mason, H. L., Murawski, M. M., & Plake, K. S. (2014). Relationships between health literacy and heart failure knowledge, self-efficacy, and self-care adherence. Research in Social & Administrative Pharmacy, 10(2), 378–386. https://doi.org/10.1016/j.sapharm.2013.07.001
- Clatworthy, J., Bowskill, R., Parham, R., Rank, T., Scott, J., & Horne, R. (2009). Understanding medication non-adherence in bipolar disorders using a Necessity-Concerns Framework. Journal of Affective Disorders, 116(1-2), 51–55. https://doi.org/10.1016/j.jad.2008.11.004
- Claxton, A. J., Cramer, J., & Pierce, C. (2001). A systematic review of the associations between dose regimens and medication compliance. Clinical Therapeutics, 23(8), 1296–1310. https://doi.org/10.1016/S0149-2918(01)80109-0
- Clifford, S., Barber, N., Elliott, R., Hartley, E., & Horne, R. (2006). Patient-centred advice is effective in improving adherence to medicines. Pharmacy World & Science, 28(3), 165–170. https://doi.org/10.1007/s11096-006-9026-6
- Conn, V. S., Enriquez, M., Ruppar, T. M., & Chan, K. C. (2016). Meta-analyses of theory use in medication adherence intervention research. American Journal of Health Behavior, 40(2), 155–171. https://doi.org/10.5993/AJHB.40.2.1
- Conn, V. S., & Ruppar, T. M. (2017). Medication adherence outcomes of 771 intervention trials: Systematic review and meta-analysis. Preventive Medicine, 99, 269–276. https://doi.org/10.1016/j.ypmed.2017.03.008
- Conn, V. S., Ruppar, T. M., Enriquez, M., & Cooper, P. (2016). Medication adherence interventions that target subjects with adherence problems: Systematic review and meta-analysis. Research in Social & Administrative Pharmacy, 12(2), 218–246. https://doi.org/10.1016/j.sapharm.2015.06.001
- Cooper, V., Buick, D., Horne, R., Lambert, N., Gellaitry, G., Leake, H., & Fisher, M. (2002). Perceptions of HAART among gay men who declined a treatment offer: Preliminary results from an interview-based study. AIDS Care, 14(3), 319–328. https://doi.org/10.1080/09540120220123694
- Cooper, V., Gellaitry, G., Hankins, M., Fisher, M., & Horne, R. (2009). The influence of symptom experiences and attributions on adherence to highly active anti-retroviral therapy (HAART): A six-month prospective, follow-up study. AIDS Care, 21(4), 520–528. https://doi.org/10.1080/09540120802301824
- Cooper, V., Horne, R., Gellaitry, G., Vrijens, B., Lange, A.-C., Fisher, M., & White, D. (2010). The impact of once-nightly versus twice-daily dosing and baseline beliefs about HAART on adherence to efavirenz-based HAART over 48 weeks: The NOCTE study. Journal of Acquired Immune Deficiency Syndromes (1999), 53(3), 369–377. https://doi.org/10.1097/QAI.0b013e3181ccb762
- Costello, K., Kennedy, P., & Scanzillo, J. (2008). Recognizing nonadherence in patients with multiple sclerosis and maintaining treatment adherence in the long term. The Medscape Journal of Medicine, 10(9), 225. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2580090/
- Cramer, J., Rosenheck, R., Kirk, G., Krol, W., Krystal, J., & Group 425, V. N. S, VA Naltrexone Study Group 425. (2003). Medication compliance feedback and monitoring in a clinical trial: Predictors and outcomes. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 6(5), 566–573. https://doi.org/10.1046/j.1524-4733.2003.65269.x
- Croome, N., Ahluwalia, M., Hughes, L. D., & Abas, M. (2017). Patient-reported barriers and facilitators to antiretroviral adherence in sub-Saharan Africa. AIDS, 31(7), 995–1007. https://doi.org/10.1097/QAD.0000000000001416
- Curkendall, S. M., Thomas, N., Bell, K. F., Juneau, P. L., & Weiss, A. J. (2013). Predictors of medication adherence in patients with type 2 diabetes mellitus. Current Medical Research and Opinion, 29(10), 1275–1286. https://doi.org/10.1185/03007995.2013.821056
- DiMatteo, M. R. (2004). Social support and patient adherence to medical treatment: A meta-analysis. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 23(2), 207–218. https://doi.org/10.1037/0278-6133.23.2.207
- DiMatteo, M. R., Giordani, P. J., Lepper, H. S., & Croghan, T. W. (2002). Patient adherence and medical treatment outcomes A meta-analysis. Medical Care, 40(9), 794–811. https://doi.org/10.1097/00005650-200209000-00009
- DiMatteo, M. R., Haskard-Zolnierek, K. B., & Martin, L. R. (2012). Improving patient adherence: A three-factor model to guide practice. Health Psychology Review, 6(1), 74–91. https://doi.org/10.1080/17437199.2010.537592
- DiMatteo, M. R., Lepper, H. S., & Croghan, T. W. (2000). Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Archives of Internal Medicine, 160(14), 2101–2107. https://doi.org/10.1001/archinte.160.14.2101
- Dobbels, F., Berben, L., De Geest, S., Drent, G., Lennerling, A., Whittaker, C., Kugler, C., Force., & The, T. T. Transplant360 Task Force (2010). The psychometric properties and practicability of self-report instruments to identify medication nonadherence in adult transplant patients: A systematic review. Transplantation, 90(2), 205–219. https://doi.org/10.1097/TP.0b013e3181e346cd
- Dombrowski, S. U., O’Carroll, R. E., & Williams, B. (2016). Form of delivery as a key ‘active ingredient’ in behaviour change interventions. British Journal of Health Psychology, 21(4), 733–740. https://doi.org/10.1111/bjhp.12203
- Eisenberger, U., Wüthrich, R. P., Bock, A., Ambühl, P., Steiger, J., Intondi, A., Kuranoff, S., Maier, T., Green, D., DiCarlo, L., Feutren, G., & De Geest, S. (2013). Medication adherence assessment: High accuracy of the new Ingestible Sensor System in kidney transplants. Transplantation, 96(3), 245–250. https://doi.org/10.1097/TP.0b013e31829b7571
- Ellis, D. A., Naar-King, S., Chen, X., Moltz, K., Cunningham, P. B., & Idalski-Carcone, A. (2012). Multisystemic therapy compared to telephone support for youth with poorly controlled diabetes: Findings from a randomized controlled trial. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 44(2), 207–215. https://doi.org/10.1007/s12160-012-9378-1
- Elnaem, M. H., Irwan, N. A., Abubakar, U., Syed Sulaiman, S. A., Elrggal, M. E., & Cheema, E. (2020). Impact of medication regimen simplification on medication adherence and clinical outcomes in patients with long-term medical conditions. Patient Preference and Adherence, 14, 2135–2145. https://doi.org/10.2147/PPA.S268499
- Emilsson, M., Berndtsson, I., Lötvall, J., Millqvist, E., Lundgren, J., Johansson, Å., & Brink, E. (2011). The influence of personality traits and beliefs about medicines on adherence to asthma treatment. Primary Care Respiratory Journal, 20(2), 141–147. https://doi.org/10.4104/pcrj.2011.00005
- European Union/European Commission. (2011). European commission/MEDI-VOICE MEDI-VOICE report summary. Project ID: 17893. European Union/European Commission. https://cordis.europa.eu/project/id/17893/reporting
- Faasse, K., Cundy, T., & Petrie, K. J. (2009). Thyroxine: Anatomy of a health scare. BMJ, 339, b5613. https://doi.org/10.1136/bmj.b5613
- Félix, I. B., Guerreiro, M. P., Cavaco, A., Cláudio, A. P., Mendes, A., Balsa, J., Carmo, M. B., Pimenta, N., & Henriques, A. (2019). Development of a complex intervention to improve adherence to antidiabetic medication in older people using an anthropomorphic virtual assistant software. Frontiers in Pharmacology, 10, 680. https://doi.org/10.3389/fphar.2019.00680
- Fenerty, S. D., West, C., Davis, S. A., Kaplan, S. G., & Feldman, S. R. (2012). The effect of reminder systems on patients’ adherence to treatment. Patient Preference and Adherence, 6, 127–135. https://doi.org/10.2147/PPA.S26314
- Fischer, M. A., Choudhry, N. K., Brill, G., Avorn, J., Schneeweiss, S., Hutchins, D., Liberman, J. N., Brennan, T. A., & Shrank, W. H. (2011). Trouble getting started: Predictors of primary medication nonadherence. The American Journal of Medicine, 124(11), 1081.e9-1081–e22. https://doi.org/10.1016/j.amjmed.2011.05.028
- Fogg, B. (2009). A behavior model for persuasive design [Paper presentation]. Proceedings of the 4th International Conference on Persuasive Technology, Claremont, CA, USA (pp. 1–7). https://doi.org/10.1145/1541948.1541999
- Foot, H., La Caze, A., Gujral, G., & Cottrell, N. (2016). The necessity–concerns framework predicts adherence to medication in multiple illness conditions: A meta-analysis. Patient Education and Counseling, 99(5), 706–717. https://doi.org/10.1016/j.pec.2015.11.004
- Francis, J. J., O’Connor, D., & Curran, J. (2012). Theories of behaviour change synthesised into a set of theoretical groupings: Introducing a thematic series on the theoretical domains framework. Implementation Science, 7(1), 35. https://doi.org/10.1186/1748-5908-7-35
- Gast, A., & Mathes, T. (2019). Medication adherence influencing factors—an (updated) overview of systematic reviews. Systematic Reviews, 8(1), 112. https://doi.org/10.1186/s13643-019-1014-8
- Gatwood, J., Balkrishnan, R., Erickson, S. R., An, L. C., Piette, J. D., & Farris, K. B. (2016). The impact of tailored text messages on health beliefs and medication adherence in adults with diabetes: A randomized pilot study. Research in Social & Administrative Pharmacy, 12(1), 130–140. https://doi.org/10.1016/j.sapharm.2015.04.007
- Gemeda, D. H., Gebretsadik, L. A., Dejene, T., Wolde, M., & Sudhakar, M. (2012). Determinants of non-compliance with antiretroviral therapy among adults living with HIV/AIDS: A systematic review. JBI Library of Systematic Reviews, 10(56), 3596–3648. https://doi.org/10.11124/jbisrir-2012-15
- George, J., Phun, Y.-T., Bailey, M. J., Kong, D. C. M., & Stewart, K. (2004). Development and validation of the medication regimen complexity index. The Annals of Pharmacotherapy, 38(9), 1369–1376. https://doi.org/10.1345/aph.1D479
- Gill, A., & Williams, A. C. (2001). Preliminary study of chronic pain patients’ concerns about cannabinoids as analgesics. The Clinical Journal of Pain, 17(3), 245–248. https://journals.lww.com/clinicalpain/Fulltext/2001/09000/Preliminary_Study_of_Chronic_Pain_Patients_.10.aspx?casa_token=WJZqc3jkXIoAAAAA:lq2t7eefKahTrwPjmnwKGEBFQSaNdIfH3CTwSSYMjcxEWoRKwP-ajv0SS4w57TuGCHOSzjJaIE0Tg-SzqD3FwUvvN5Pk5iGyq1zyqVZwFg
- Gourzoulidis, G., Kourlaba, G., Stafylas, P., Giamouzis, G., Parissis, J., & Maniadakis, N. (2017). Association between copayment, medication adherence and outcomes in the management of patients with diabetes and heart failure. Health Policy (Amsterdam, Netherlands), 121(4), 363–377. https://doi.org/10.1016/j.healthpol.2017.02.008
- Gray, W. N., Netz, M., McConville, A., Fedele, D., Wagoner, S. T., & Schaefer, M. R. (2018). Medication adherence in pediatric asthma: A systematic review of the literature. Pediatric Pulmonology, 53(5), 668–684. https://doi.org/10.1002/ppul.23966
- Green, D. W., Horne, R., & Shephard, E. A. (2013). Public perceptions of the risks, benefits and use of natural remedies, pharmaceutical medicines and personalised medicines. Complementary Therapies in Medicine, 21(5), 487–491. https://doi.org/10.1016/j.ctim.2013.07.007
- Gupta, K., & Horne, R. (2001). The influence of health beliefs on the presentation and consultation outcome in patients with chemical sensitivities. Journal of Psychosomatic Research, 50(3), 131–137. https://doi.org/10.1016/S0022-3999(00)00218-X
- Gupta, P., Voors, A. A., Patel, P., Lane, D., Anker, S. D., Cleland, J. G. F., Dickstein, K., Filippatos, G., Lang, C. C., van Veldhuisen, D. J., Metra, M., Zannad, F., Samani, N. J., Jones, D. J. L., Squire, I. B., & Ng, L. L. (2021). Non-adherence to heart failure medications predicts clinical outcomes: Assessment in a single spot urine sample by liquid chromatography-tandem mass spectrometry (results of a prospective multicentre study). European Journal of Heart Failure, 23(7), 1182–1190. https://doi.org/10.1002/ejhf.2160
- Hardon, A. P., Akurut, D., Comoro, C., Ekezie, C., Irunde, H. F., Gerrits, T., Kglatwane, J., Kinsman, J., Kwasa, R., Maridadi, J., Moroka, T. M., Moyo, S., Nakiyemba, A., Nsimba, S., Ogenyi, R., Oyabba, T., Temu, F., & Laing, R. (2007). Hunger, waiting time and transport costs: Time to confront challenges to ART adherence in Africa. AIDS Care, 19(5), 658–665. https://doi.org/10.1080/09540120701244943
- Haynes, R. B., McDonald, H. P., Garg, A., & Montague, P. (2002). Interventions for helping patients to follow prescriptions for medications. Cochrane Database of Systematic Reviews, 2, CD000011. https://doi.org/10.1002/14651858.CD000011
- Haynes, R. B., McDonald, H. P., & Garg, A. X. (2002). Helping patients follow prescribed treatment clinical applications. JAMA, 288(22), 2880–2883. https://doi.org/10.1001/jama.288.22.2880
- Haynes, R., B., Taylor, D., W., & Sackett, D. L. (1979). Compliance in health care (1st ed.). The John Hopkins University Press.
- Heestermans, T., Browne, J. L., Aitken, S. C., Vervoort, S. C., & Klipstein-Grobusch, K. (2016). Determinants of adherence to antiretroviral therapy among HIV-positive adults in sub-Saharan Africa: A systematic review. BMJ Global Health, 1(4), e000125. https://doi.org/10.1136/bmjgh-2016-000125
- Heller, M. K., Chapman, S. C. E., & Horne, R. (2015). Beliefs about medication predict the misattribution of a common symptom as a medication side effect—evidence from an analogue online study. Journal of Psychosomatic Research, 79(6), 519–529. https://doi.org/10.1016/j.jpsychores.2015.10.003
- Heller, M. K., Chapman, S. C. E., & Horne, R. (2017). No blank slates: Pre-existing schemas about pharmaceuticals predict memory for side effects. Psychology & Health, 32(4), 402–421. https://doi.org/10.1080/08870446.2016.1273355
- Hershman, D. L., Shao, T., Kushi, L. H., Buono, D., Tsai, W. Y., Fehrenbacher, L., Kwan, M., Gomez, S. L., & Neugut, A. I. (2011). Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Research and Treatment, 126(2), 529–537. https://doi.org/10.1007/s10549-010-1132-4
- Hershman, D. L., Tsui, J., Wright, J. D., Coromilas, E. J., Tsai, W. Y., & Neugut, A. I. (2015). Household net worth, racial disparities, and hormonal therapy adherence among women with early-stage breast cancer. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 33(9), 1053–1059. https://doi.org/10.1200/JCO.2014.58.3062
- Ho, P. M., Magid, D. J., Masoudi, F. A., McClure, D. L., & Rumsfeld, J. S. (2006). Adherence to cardioprotective medications and mortality among patients with diabetes and ischemic heart disease. BMC Cardiovascular Disorders, 6(1), 48. https://doi.org/10.1186/1471-2261-6-48
- Holmes, E. A. F., Hughes, D. A., & Morrison, V. L. (2014). Predicting adherence to medications using health psychology theories: A systematic review of 20 years of empirical research. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 17(8), 863–876. https://doi.org/10.1016/j.jval.2014.08.2671
- Horne, P. R. (2018). Decisions about medicines: Scientific evidence in context (Vol. 9). The Academic of Medical Sciences.
- Horne, R. (1998). Adherence to medication: A review of existing research. Adherence to treatment in medical conditions. CRC Press.
- Horne, R. (2001). Compliance, adherence and concordance. In K. Taylor & G. Harding (Eds.), Pharmacy practice (pp. 148–169). Taylor & Francis.
- Horne, R. (2003). Treatment perceptions and self-regulation. The self-regulation of health and illness behaviour. Routledge.
- Horne, R. (2011). Adherence to asthma medication: A question of ability? Primary Care Respiratory Journal: Journal of the General Practice Airways Group, 20(2), 118–119. https://doi.org/10.4104/pcrj.2011.00054
- Horne, R., Buick, D., Fisher, M., Leake, H., Cooper, V., & Weinman, J. (2004). Doubts about necessity and concerns about adverse effects: Identifying the types of beliefs that are associated with non-adherence to HAART. International Journal of STD & AIDS, 15(1), 38–44. https://doi.org/10.1258/095646204322637245
- Horne, R., Chapman, S. C. E., Parham, R., Freemantle, N., Forbes, A., & Cooper, V. (2013). Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: A meta-analytic review of the necessity-concerns framework. PLoS One, 8(12), e80633. https://doi.org/10.1371/journal.pone.0080633
- Horne, R., & Clatworthy, J. (2010). Adherence to advice and treatment. Health psychology (2nd ed.). John Wiley & Sons.
- Horne, R., Cooper, V., Gellaitry, G., Date, H. L., & Fisher, M. (2007). Patients’ perceptions of highly active antiretroviral therapy in relation to treatment uptake and adherence: The utility of the necessity-concerns framework. Journal of Acquired Immune Deficiency Syndromes (1999), 45(3), 334–341. https://doi.org/10.1097/QAI.0b013e31806910e3
- Horne, R., Cooper, V., Wileman, V., & Chan, A. (2019). Supporting adherence to medicines for long-term conditions. European Psychologist, 24(1), 82–96. https://doi.org/10.1027/1016-9040/a000353
- Horne, R., Parham, R., Driscoll, R., & Robinson, A. (2009). Patients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflammatory Bowel Diseases, 15(6), 837–844. https://doi.org/10.1002/ibd.20846
- Horne, R., & Weinman, J. (2002). Self-regulation and self-management in asthma: Exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychology & Health, 17(1), 17–32. https://doi.org/10.1080/08870440290001502
- Horne, R., Weinman, J., Barber, N., Elliot, R., & Morgan, M. (2005). Concordance, adherence and compliance in medicine taking. National co-ordinating centre for NHS service delivery and organisation R and D (pp. 1–309). NCCSDO. https://www.ahpo.net/assets/NCCSDO%20Compliance%202005.pdf
- Horne, R., Weinman, J., & Hankins, M. (1999). The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychology & Health, 14(1), 1–24. https://doi.org/10.1080/08870449908407311
- Howland, O. (2020). Fakes and chemicals: Indigenous medicine in contemporary Kenya and implications for health equity. International Journal for Equity in Health, 19(1), 199. https://doi.org/10.1186/s12939-020-01313-1
- Ingersoll, K. S., & Cohen, J. (2008). The impact of medication regimen factors on adherence to chronic treatment: a review of literature. Journal of Behavioral Medicine, 31(3), 213–224. https://doi.org/10.1007/s10865-007-9147-y
- Jackevicius, C. A., Mamdani, M., & Tu, J. V. (2002). Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA, 288(4), 462–467. https://doi.org/10.1001/jama.288.4.462
- Jackson, C. A., Clatworthy, J., Robinson, A., & Horne, R. (2010). Factors associated with non-adherence to oral medication for inflammatory bowel disease: A systematic review. The American Journal of Gastroenterology, 105(3), 525–539. https://doi.org/10.1038/ajg.2009.685
- Jackson, C., Eliasson, Â. L., Barber, N., & Weinman, J. (2014). Applying COM-B to medication adherence: A suggested framework for research and interventions. European Health Psychologist, 16(1), 1. https://scholar.google.co.uk/scholar?hl=en&as_sdt=0%2C5&as_vis=1&q=Applying+COM-B+to+medication+adherence%3A+A+suggested+framework+for+research+and+interventions.&btnG=#:∼:text=include%20citations-,%5BPDF%5D%20ehps.net,-%5BPDF%5D%20Applying
- Jackson, C., Lawton, R. J., Raynor, D. K., Knapp, P., Conner, M. T., Lowe, C. J., & Closs, S. J. (2006). Promoting adherence to antibiotics: A test of implementation intentions. Patient Education and Counseling, 61(2), 212–218. https://doi.org/10.1016/j.pec.2005.03.010
- Jeffery, R. A., Navarro, T., Wilczynski, N. L., Iserman, E. C., Keepanasseril, A., Sivaramalingam, B., Agoritsas, T., & Haynes, R. B. (2014). Adherence measurement and patient recruitment methods are poor in intervention trials to improve patient adherence. Journal of Clinical Epidemiology, 67(10), 1076–1082. https://doi.org/10.1016/j.jclinepi.2014.06.008
- Joosten, E., a G., DeFuentes-Merillas, L., Weert, G. H. d., Sensky, T., Staak, C. P. F., van der, Jong., & C. A. J., de. (2008). Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychotherapy and Psychosomatics, 77(4), 219–226. https://doi.org/10.1159/000126073
- Kader, R., Govender, R., Seedat, S., Koch, J. R., & Parry, C. (2015). Understanding the impact of hazardous and harmful use of alcohol and/or other drugs on ARV adherence and disease progression. PLoS One, 10(5), e0125088. https://doi.org/10.1371/journal.pone.0125088
- Kahn, K. L., Schneider, E. C., Malin, J. L., Adams, J. L., & Epstein, A. M. (2007). Patient centered experiences in breast cancer: Predicting long-term adherence to tamoxifen use. Medical Care, 45(5), 431–439. https://doi.org/10.1097/01.mlr.0000257193.10760.7f
- Kahneman, D. (2012). Thinking, fast and slow. Penguin Books Ltd.
- Kalantarian, H., Alshurafa, N., Nemati, E., Le, T., & Sarrafzadeh, M. (2015). A smartwatch-based medication adherence system [Paper presentation].2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA (pp. 1–6). https://doi.org/10.1109/BSN.2015.7299348
- Kalantarian, H., Motamed, B., Alshurafa, N., & Sarrafzadeh, M. (2016). A wearable sensor system for medication adherence prediction. Artificial Intelligence in Medicine, 69, 43–52. https://doi.org/10.1016/j.artmed.2016.03.004
- Kamal, S., Rosen, M. I., Lazar, C., Siqueiros, L., Wang, Y., Daar, E. S., & Liu, H. (2020). Perceptions of people living with HIV and HIV healthcare providers on real-time measuring and monitoring of antiretroviral adherence using ingestible sensors: A qualitative study. AIDS Research and Treatment, 2020, 1098109. https://doi.org/10.1155/2020/1098109
- Kang, H., Lobo, J. M., Kim, S., & Sohn, M.-W. (2018). Cost-related medication non-adherence among U.S. adults with diabetes. Diabetes Research and Clinical Practice, 143, 24–33. https://doi.org/10.1016/j.diabres.2018.06.016
- Karamanidou, C., Clatworthy, J., Weinman, J., & Horne, R. (2008). A systematic review of the prevalence and determinants of nonadherence to phosphate binding medication in patients with end-stage renal disease. BMC Nephrology, 9(1), 2. https://doi.org/10.1186/1471-2369-9-2
- Kardas, P., Lewek, P., & Matyjaszczyk, M. (2013). Determinants of patient adherence: A review of systematic reviews. Frontiers in Pharmacology, 4, 91. https://doi.org/10.3389/fphar.2013.00091
- Kassavou, A., & Sutton, S. (2017). Reasons for non-adherence to cardiometabolic medications, and acceptability of an interactive voice response intervention in patients with hypertension and type 2 diabetes in primary care: A qualitative study. BMJ Open, 7(8), e015597. https://doi.org/10.1136/bmjopen-2016-015597
- Kassavou, A., & Sutton, S. (2018). Automated telecommunication interventions to promote adherence to cardio-metabolic medications: Meta-analysis of effectiveness and meta-regression of behaviour change techniques. Health Psychology Review, 12(1), 25–42. https://doi.org/10.1080/17437199.2017.1365617
- Khalaf, K., Johnell, K., Austin, P. C., Tyden, P., Midlöv, P., Perez-Vicente, R., & Merlo, J. (2021). Low adherence to statin treatment during the 1st year after an acute myocardial infarction is associated with increased 2nd-year mortality risk—An inverse probability of treatment weighted study on 54 872 patients. European Heart Journal Cardiovascular Pharmacotherapy, 7(2), 141–147. https://doi.org/10.1093/ehjcvp/pvaa010
- Khdour, M. R., Hawwa, A. F., Kidney, J., C., Smyth, B. M., McElnay,., & J., C. (2012). Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). European Journal of Clinical Pharmacology, 68(10), 1365–1373. https://doi.org/10.1007/s00228-012-1279-5
- Kripalani, S., Yao, X., & Haynes, R. B. (2007). Interventions to enhance medication adherence in chronic medical conditions: A systematic review. Archives of Internal Medicine, 167(6), 540–550. https://doi.org/10.1001/archinte.167.6.540
- Kvarnström, K., Westerholm, A., Airaksinen, M., & Liira, H. (2021). Factors contributing to medication adherence in patients with a chronic condition: A scoping review of qualitative research. Pharmaceutics, 13(7), 1100. https://doi.org/10.3390/pharmaceutics13071100
- Lacro, J. P., Dunn, L. B., Dolder, C. R., Leckband, S. G., & Jeste, D. V. (2002). Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: A comprehensive review of recent literature. The Journal of Clinical Psychiatry, 63(10), 892–909. https://doi.org/10.4088/JCP.v63n1007
- Ladin, K., Daniels, A., Osani, M., & Bannuru, R. R. (2018). Is social support associated with post-transplant medication adherence and outcomes? A systematic review and meta-analysis. Transplantation Reviews (Orlando, FL), 32(1), 16–28. https://doi.org/10.1016/j.trre.2017.04.001
- Langebeek, N., Gisolf, E. H., Reiss, P., Vervoort, S. C., Hafsteinsdóttir, T. B., Richter, C., Sprangers, M. A., & Nieuwkerk, P. T. (2014). Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: A meta-analysis. BMC Medicine, 12(1), 142. https://doi.org/10.1186/s12916-014-0142-1
- Leclerc, E., Mansur, R. B., & Brietzke, E. (2013). Determinants of adherence to treatment in bipolar disorder: A comprehensive review. Journal of Affective Disorders, 149(1–3), 247–252. https://doi.org/10.1016/j.jad.2013.01.036
- Lee, Y.-K., Ah, Y.-M., Choi, Y. J., Cho, Y. S., Kim, K. J., & Lee, J.-Y. (2016). Antiepileptic drug adherence and persistence in children with epilepsy attending a large tertiary care children’s hospital. Epileptic Disorders: International Epilepsy Journal with Videotape, 18(4), 408–417. https://doi.org/10.1684/epd.2016.0871
- Lee, Y.-M., Kim, R. B., Lee, H. J., Kim, K., Shin, M.-H., Park, H.-K., Ahn, S.-K., Kim, S. Y., Lee, Y.-H., Kim, B.-G., Lee, H., Lee, W. K., Lee, K. S., Kim, M.-J., & Park, K.-S. (2018). Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: A cross-sectional study. Health and Quality of Life Outcomes, 16(1), 100. https://doi.org/10.1186/s12955-018-0921-z
- Lester, R. T., Mills, E. J., Kariri, A., Ritvo, P., Chung, M., Jack, W., Habyarimana, J., Karanja, S., Barasa, S., Nguti, R., Estambale, B., Ngugi, E., Ball, T. B., Thabane, L., Kimani, J., Gelmon, L., Ackers, M., & Plummer, F. A. (2009). The HAART cell phone adherence trial (WelTel Kenya1): A randomized controlled trial protocol. Trials, 10(1), 87. https://doi.org/10.1186/1745-6215-10-87
- Leventhal, H., Diefenbach, M., & Leventhal, E. A. (1992). Illness cognition: Using common sense to understand treatment adherence and affect cognition interactions. Cognitive Therapy and Research, 16(2), 143–163. https://doi.org/10.1007/BF01173486
- Leventhal, H., Phillips, L. A., & Burns, E. (2016). The Common-Sense Model of Self-Regulation (CSM): A dynamic framework for understanding illness self-management. Journal of Behavioral Medicine, 39(6), 935–946. https://doi.org/10.1007/s10865-016-9782-2
- Lewey, J., Shrank, W. H., Bowry, A. D. K., Kilabuk, E., Brennan, T. A., & Choudhry, N. K. (2013). Gender and racial disparities in adherence to statin therapy: A meta-analysis. American Heart Journal, 165(5), 665–678.e1. https://doi.org/10.1016/j.ahj.2013.02.011
- Liddelow, C., Mullan, B., Boyes, M., & McBride, H. (2020). A qualitative application of temporal self-regulation theory to understand adherence to simple and complex medication regimens. Healthcare, 8(4), 487. https://doi.org/10.3390/healthcare8040487
- Lin, A. H.-A., Kendrick, J. G., Wilcox, P. G., & Quon, B. S. (2017). Patient knowledge and pulmonary medication adherence in adult patients with cystic fibrosis. Patient Preference and Adherence, 11, 691–698. https://doi.org/10.2147/PPA.S129088
- Lindquist, L. A., Go, L., Fleisher, J., Jain, N., Friesema, E., & Baker, D. W. (2012). Relationship of health literacy to intentional and unintentional non-adherence of hospital discharge medications. Journal of General Internal Medicine, 27(2), 173–178. https://doi.org/10.1007/s11606-011-1886-3
- Llewellyn, C. D., Miners, A. H., Lee, C. A., Harrington, C., & Weinman, J. (2003). The illness perceptions and treatment beliefs of individuals with severe haemophilia and their role in adherence to home treatment. Psychology & Health, 18(2), 185–200. https://doi.org/10.1080/0887044031000098198
- Lofland, J. H., Johnson, P. T., Ingham, M. P., Rosemas, S. C., White, J. C., & Ellis, L. (2017). Shared decision-making for biologic treatment of autoimmune disease: Influence on adherence, persistence, satisfaction, and health care costs. Patient Preference and Adherence, 11, 947–958. https://doi.org/10.2147/PPA.S133222
- Lustria, M. L. A., Noar, S. M., Cortese, J., Van Stee, S. K., Glueckauf, R. L., & Lee, J. (2013). A meta-analysis of web-delivered tailored health behavior change interventions. Journal of Health Communication, 18(9), 1039–1069. https://doi.org/10.1080/10810730.2013.768727
- MacDonald, L., Chapman, S., Syrett, M., Bowskill, R., & Horne, R. (2016). Improving medication adherence in bipolar disorder: A systematic review and meta-analysis of 30 years of intervention trials. Journal of Affective Disorders, 194, 202–221. https://doi.org/10.1016/j.jad.2016.01.002
- Manteuffel, M., Williams, S., Chen, W., Verbrugge, R. R., Pittman, D. G., & Steinkellner, A. (2014). Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. Journal of Women’s Health (2002), 23(2), 112–119. https://doi.org/10.1089/jwh.2012.3972
- Manzano-García, M., Pérez-Guerrero, C., Álvarez de Sotomayor Paz, M., Robustillo-Cortés, M., de las, A., Almeida-González, C. V., & Morillo-Verdugo, R. (2018). Identification of the Medication Regimen Complexity Index as an Associated Factor of Nonadherence to Antiretroviral Treatment in HIV Positive Patients. The Annals of Pharmacotherapy, 52(9), 862–867. https://doi.org/10.1177/1060028018766908
- Martani, A., Geneviève, L. D., Poppe, C., Casonato, C., & Wangmo, T. (2020). Digital pills: A scoping review of the empirical literature and analysis of the ethical aspects. BMC Medical Ethics, 21(1), 3. https://doi.org/10.1186/s12910-019-0443-1
- Mathes, T., Pieper, D., Antoine, S.-L., & Eikermann, M. (2014). Adherence influencing factors in patients taking oral anticancer agents: A systematic review. Cancer Epidemiology, 38(3), 214–226. https://doi.org/10.1016/j.canep.2014.03.012
- Matthias, M. S., Salyers, M. P., Rollins, A. L., & Frankel, R. M. (2012). Decision making in recovery-oriented mental health care. Psychiatric Rehabilitation Journal, 35(4), 305–314. https://doi.org/10.2975/35.4.2012.305.314
- McGrady, M. E., & Pai, A. L. H. (2019). A systematic review of rates, outcomes, and predictors of medication non-adherence among adolescents and young adults with cancer. Journal of Adolescent and Young Adult Oncology, 8(5), 485–494. https://doi.org/10.1089/jayao.2018.0160
- Mes, M. A., Katzer, C. B., Chan, A. H. Y., Wileman, V., Taylor, S. J. C., & Horne, R. (2018). Pharmacists and medication adherence in asthma: A systematic review and meta-analysis. European Respiratory Journal, 52(2), 1800485. https://doi.org/10.1183/13993003.00485-2018
- Michie, S., Johnston, M., Francis, J., Hardeman, W., & Eccles, M. (2008). From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour hange techniques. Applied Psychology, 57(4), 660–680. https://doi.org/10.1111/j.1464-0597.2008.00341.x
- Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J., & Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6
- Michie, S., van Stralen, M. M., & West, R. (2011). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 6(1), 42. https://doi.org/10.1186/1748-5908-6-42
- Miller, T. A. (2016). Health literacy and adherence to medical treatment in chronic and acute illness: A meta-analysis. Patient Education and Counseling, 99(7), 1079–1086. https://doi.org/10.1016/j.pec.2016.01.020
- Mitzel, L. D., & Vanable, P. A. (2020). Necessity and concerns beliefs and HIV medication adherence: A systematic review. Journal of Behavioral Medicine, 43(1), 1–15. https://doi.org/10.1007/s10865-019-00089-2
- Mongkhon, P., Ashcroft, D. M., Scholfield, C. N., & Kongkaew, C. (2018). Hospital admissions associated with medication non-adherence: A systematic review of prospective observational studies. BMJ Quality & Safety, 27(11), 902–914. https://doi.org/10.1136/bmjqs-2017-007453
- Monnette, A., Zhang, Y., Shao, H., & Shi, L. (2018). Concordance of adherence measurement using self-reported adherence questionnaires and medication monitoring devices: An updated review. PharmacoEconomics, 36(1), 17–27. https://doi.org/10.1007/s40273-017-0570-9
- Moon, S. J., Lee, W.-Y., Hwang, J. S., Hong, Y. P., & Morisky, D. E. (2017). Accuracy of a screening tool for medication adherence: A systematic review and meta-analysis of the Morisky medication adherence scale-8. PLoS One, 12(11), e0187139. https://doi.org/10.1371/journal.pone.0187139
- Moon, Z., Moss-Morris, R., Hunter, M. S., Carlisle, S., & Hughes, L. D. (2017). Barriers and facilitators of adjuvant hormone therapy adherence and persistence in women with breast cancer: A systematic review. Patient Preference and Adherence, 11, 305–322. https://doi.org/10.2147/PPA.S126651
- Moon, Z., Moss-Morris, R., Hunter, M. S., Goodliffe, S., & Hughes, L. D. (2019). Acceptability and feasibility of a self-management intervention for women prescribed tamoxifen. Health Education Journal, 78(8), 901–915. https://doi.org/10.1177/0017896919853856
- Morisky, D. E., Green, L. W., & Levine, D. M. (1986). Concurrent and predictive validity of a self-reported measure of medication adherence. Medical Care, 24(1), 67–74. https://pubmed.ncbi.nlm.nih.gov/3945130/
- Munro, S. A., Lewin, S. A., Smith, H. J., Engel, M. E., Fretheim, A., & Volmink, J. (2007). Patient adherence to tuberculosis treatment: A systematic review of qualitative research. PLoS Medicine, 4(7), e238. https://doi.org/10.1371/journal.pmed.0040238
- Nieuwlaat, R., Wilczynski, N., Navarro, T., Hobson, N., Jeffery, R., Keepanasseril, A., Agoritsas, T., Mistry, N., Iorio, A., Jack, S., Sivaramalingam, B., Iserman, E., Mustafa, R. A., Jedraszewski, D., Cotoi, C., & Haynes, R. B, Cochrane Consumers and Communication Group. (2014). Interventions for enhancing medication adherence. Cochrane Database of Systematic Reviews, 11, CD000011. https://doi.org/10.1002/14651858.CD000011.pub4
- Noar, S. M., Benac, C. N., & Harris, M. S. (2007). Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychological Bulletin, 133(4), 673–693. https://doi.org/10.1037/0033-2909.133.4.673
- Noar, S. M., Grant Harrington, N., Van Stee, S. K., & Shemanski Aldrich, R. (2011). Tailored health communication to change lifestyle behaviors. American Journal of Lifestyle Medicine, 5(2), 112–122. https://doi.org/10.1177/1559827610387255
- Nunes, V., Neilson, J., O’Flynn, N., Calvert, N., Kuntze, S., Smithson, H., Benson, J., Blair, J., Bowser, A., Clyne, W., Crome, P., Haddad, P., Hemingway, S., Horne, R., Johnson, S., Kelly, S., Packam, B., Patel, M., & Steel, J. (2009). Medicines adherence: Involving patients in decisions about prescribed medicines and supporting adherence [Monograph]. NICE: National Institute for Health and Clinical Excellence. http://eprints.hud.ac.uk/id/eprint/14569/C:\Users\librsjt\Documents\PatelNICE76English.htm
- O’Carroll, R. E., Chambers, J. A., Dennis, M., Sudlow, C., & Johnston, M. (2013). Improving adherence to medication in stroke survivors: A pilot randomised controlled trial. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 46(3), 358–368. https://doi.org/10.1007/s12160-013-9515-5
- Odeh, M., Scullin, C., Fleming, G., Scott, M. G., Horne, R., & McElnay, J. C. (2019). Ensuring continuity of patient care across the healthcare interface: Telephone follow-up post-hospitalization. British Journal of Clinical Pharmacology, 85(3), 616–625. https://doi.org/10.1111/bcp.13839
- OECD (2018). Investing in medication adherence improves health outcomes and health system efficiency: Adherence to medicines for diabetes, hypertension, and hyperlipidaemia (OECD Health Working Papers No. 105; OECD Health Working Papers, Vol. 105. https://doi.org/10.1787/8178962c-en
- Ogden, J., & Sidhu, S. (2006). Adherence, behavior change, and visualization: A qualitative study of the experiences of taking an obesity medication. Journal of Psychosomatic Research, 61(4), 545–552. https://doi.org/10.1016/j.jpsychores.2006.04.017
- Ölander, F., & ThØgersen, J. (1995). Understanding of consumer behaviour as a prerequisite for environmental protection. Journal of Consumer Policy, 18(4), 345–385. https://doi.org/10.1007/BF01024160
- Olthoff, C. M. G., Schouten, J. S. A. G., Borne, B. W., van de., & Webers, C. A. B. (2005). Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension: An evidence-based review. Ophthalmology, 112(6), 953–961.e7. https://doi.org/10.1016/j.ophtha.2004.12.035
- Ortego, C., Huedo-Medina, T. B., Llorca, J., Sevilla, L., Santos, P., Rodríguez, E., Warren, M. R., & Vejo, J. (2011). Adherence to highly active antiretroviral therapy (HAART): A meta-analysis. AIDS and Behavior, 15(7), 1381–1396. https://doi.org/10.1007/s10461-011-9942-x
- Paczkowska, A., Hoffmann, K., Kus, K., Kopciuch, D., Zaprutko, T., Ratajczak, P., Michalak, M., Nowakowska, E., & Bryl, W. (2021). Impact of patient knowledge on hypertension treatment adherence and efficacy: A single-centre study in Poland. International Journal of Medical Sciences, 18(3), 852–860. https://doi.org/10.7150/ijms.48139
- Pantuzza, L. L., Ceccato, M., das, G. B., Silveira, M. R., Junqueira, L. M. R., & Reis, A. M. M. (2017). Association between medication regimen complexity and pharmacotherapy adherence: A systematic review. European Journal of Clinical Pharmacology, 73(11), 1475–1489. https://doi.org/10.1007/s00228-017-2315-2
- Pearce, C. J., Chan, A. H. Y., Jackson, T., Fleming, L., Foot, H., Bush, A., & Horne, R. (2022). Features of successful interventions to improve adherence to inhaled corticosteroids in children with asthma: A narrative systematic review. Pediatric Pulmonology, 57(4), 822–847. https://doi.org/10.1002/ppul.25838
- Petrie, K. J., Broadbent, E. A., Kley, N., Psych, D., Moss-Morris, R., Horne, R., & Rief, W. (2005). Worries about modernity predict symptom complaints after environmental pesticide spraying. Psychosomatic Medicine, 67(5), 778–782. https://doi.org/10.1097/01.psy.0000181277.48575.a4
- Petrie, K. J., Perry, K., Broadbent, E., & Weinman, J. (2012). A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication. British Journal of Health Psychology, 17(1), 74–84. https://doi.org/10.1111/j.2044-8287.2011.02033.x
- Piette, J. D., Heisler, M., Horne, R., & Caleb Alexander, G. (2006). A conceptually based approach to understanding chronically ill patients’ responses to medication cost pressures. Social Science & Medicine (1982), 62(4), 846–857. https://doi.org/10.1016/j.socscimed.2005.06.045
- Rehm, J., Probst, C., Shield, K. D., & Shuper, P. A. (2017). Does alcohol use have a causal effect on HIV incidence and disease progression? A review of the literature and a modeling strategy for quantifying the effect. Population Health Metrics, 15(1), 4. https://doi.org/10.1186/s12963-017-0121-9
- Reisner, S. L., Mimiaga, M. J., Skeer, M., Perkovich, B., Johnson, C. V., & Safren, S. A. (2009). A review of HIV antiretroviral adherence and intervention studies among HIV–infected youth. Topics in HIV Medicine: A Publication of the International AIDS Society, 17(1), 14–25.
- Ribaut, J., Leppla, L., Teynor, A., Valenta, S., Dobbels, F., Zullig, L. L., De Geest, S., Beckmann, S., Mielke, J., Schmid, A., Duerinckx, N., Heidegger, P., Fürmann, M., Neupert, D., Rockstein, D., Werlitz, V., Fürmann, M., Schulz, T., … Lemcke, M, the SMILe Study Team. (2020). Theory-driven development of a medication adherence intervention delivered by eHealth and transplant team in allogeneic stem cell transplantation: The SMILe implementation science project. BMC Health Services Research, 20(1), 827. https://doi.org/10.1186/s12913-020-05636-1
- Rich, A., Brandes, K., Mullan, B., & Hagger, M. S. (2015). Theory of planned behavior and adherence in chronic illness: A meta-analysis. Journal of Behavioral Medicine, 38(4), 673–688. https://doi.org/10.1007/s10865-015-9644-3
- Rintamaki, L., Kosenko, K., Hogan, T., Scott, A. M., Dobmeier, C., Tingue, E., & Peek, D. (2019). The role of stigma management in HIV treatment adherence. International Journal of Environmental Research and Public Health, 16(24), 5003. https://doi.org/10.3390/ijerph16245003
- Roberts, M. C., Wheeler, S. B., & Reeder-Hayes, K. (2015). Racial/ethnic and socioeconomic disparities in endocrine therapy adherence in breast cancer: A systematic review. American Journal of Public Health, 105(S3), e4–e15. https://doi.org/10.2105/AJPH.2014.302490
- Sabaté, E. (Ed.). (2003). Adherence to long-term therapies: Evidence for action. World Health Organization.
- Sackett, D., L., Haynes, R. B., Tugwell, P., & Gordon, H. (1985). Clinical epidemiology: A basic science for clinical medicine. Little, Brown and Company.
- Sadigh, G., Gray, R. J., Sparano, J. A., Yanez, B., Garcia, S. F., Timsina, L. R., Sledge, G. W., Cella, D., Wagner, L. I., & Carlos, R. C. (2021). Breast cancer patients’ insurance status and residence zip code correlate with early discontinuation of endocrine therapy: An analysis of the ECOG-ACRIN TAILORx trial. Cancer, 127(14), 2545–2552. https://doi.org/10.1002/cncr.33527
- Sainsbury, K., Walburn, J., Foster, L., Morgan, M., Sarkany, R., Weinman, J., & Araujo-Soares, V. (2020). Improving photoprotection in adults with xeroderma pigmentosum: Personalisation and tailoring in the ‘XPAND’ intervention. Health Psychology and Behavioral Medicine, 8(1), 543–572. https://doi.org/10.1080/21642850.2020.1840379
- Şanlıtürk, D., & Ayaz-Alkaya, S. (2021). The effect of a theory of planned behavior education program on asthma control and medication adherence: A randomized controlled trial. The Journal of Allergy and Clinical Immunology, 9(9), 3371–3379. https://doi.org/10.1016/j.jaip.2021.03.060
- Saran, R., Bragg-Gresham, J. L., Rayner, H. C., Goodkin, D. A., Keen, M. L., Van Dijk, P. C., Kurokawa, K., Piera, L., Saito, A., Fukuhara, S., Young, E. W., Held, P. J., & Port, F. K. (2003). Nonadherence in hemodialysis: Associations with mortality, hospitalization, and practice patterns in the DOPPS. Kidney International, 64(1), 254–262. https://doi.org/10.1046/j.1523-1755.2003.00064.x
- Schüz, B., Wolff, J. K., Warner, L. M., Ziegelmann, J. P., & Wurm, S. (2014). Multiple illness perceptions in older adults: Effects on physical functioning and medication adherence. Psychology & Health, 29(4), 442–457. https://doi.org/10.1080/08870446.2013.863884
- Selinger, C. P., Ochieng, A. O., George, V., & Leong, R. W. (2019). The accuracy of adherence self-report scales in patients on thiopurines for inflammatory bowel disease: A comparison with drug metabolite levels and medication possession ratios. Inflammatory Bowel Diseases, 25(5), 919–924. https://doi.org/10.1093/ibd/izy309
- Shah, R., Watson, J., & Free, C. (2019). A systematic review and meta-analysis in the effectiveness of mobile phone interventions used to improve adherence to antiretroviral therapy in HIV infection. BMC Public Health, 19(1), 915. https://doi.org/10.1186/s12889-019-6899-6
- Shahin, W., Kennedy, G. A., & Stupans, I. (2019). The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: A systematic review. Patient Preference and Adherence, 13, 1019–1035. https://doi.org/10.2147/PPA.S212046
- Shelby, R. A., Edmond, S. N., Wren, A. A., Keefe, F. J., Peppercorn, J. M., Marcom, P. K., ... & Kimmick, G. G. (2014). Self-efficacy for coping with symptoms moderates the relationship between physical symptoms and well-being in breast cancer survivors taking adjuvant endocrine therapy. Supportive Care in Cancer, 22(10), 2851–2859. https://doi.org/10.1007/s00520-014-2269-1
- Sheppard, V. B., de Mendoza, A. H., He, J., Jennings, Y., Edmonds, M. C., Oppong, B. A., & Tadesse, M. G. (2018). Initiation of adjuvant endocrine therapy in black and white women with breast cancer. Clinical Breast Cancer, 18(5), 337–346.e1. https://doi.org/10.1016/j.clbc.2017.12.002
- Shi, L., Liu, J., Fonseca, V., Walker, P., Kalsekar, A., & Pawaskar, M. (2010). Correlation between adherence rates measured by MEMS and self-reported questionnaires: A meta-analysis. Health and Quality of Life Outcomes, 8(1), 99. https://doi.org/10.1186/1477-7525-8-99
- Simoni, J. M., Huh, D., Wilson, I. B., Shen, J., Goggin, K., Reynolds, N. R., Remien, R. H., Rosen, M. I., Bangsberg, D. R., & Liu, H. (2012). Racial/Ethnic disparities in ART adherence in the United States: Findings from the MACH14 study. Journal of Acquired Immune Deficiency Syndromes (1999), 60(5), 466–472. https://doi.org/10.1097/QAI.0b013e31825db0bd
- Simpson, S. H., Eurich, D. T., Majumdar, S. R., Padwal, R. S., Tsuyuki, R. T., Varney, J., & Johnson, J. A. (2006). A meta-analysis of the association between adherence to drug therapy and mortality. BMJ, 333(7557), 15. https://doi.org/10.1136/bmj.38875.675486.55
- Smaje, A., Weston-Clark, M., Raj, R., Orlu, M., Davis, D., & Rawle, M. (2018). Factors associated with medication adherence in older patients: A systematic review. Aging Medicine, 1(3), 254–266. https://doi.org/10.1002/agm2.12045
- Smalls, B. L., Walker, R. J., Hernandez-Tejada, M. A., Campbell, J. A., Davis, K. S., & Egede, L. E. (2012). Associations between coping, diabetes knowledge, medication adherence and self-care behaviors in adults with type 2 diabetes. General Hospital Psychiatry, 34(4), 385–389. https://doi.org/10.1016/j.genhosppsych.2012.03.018
- Smith, S. G., Sestak, I., Forster, A., Partridge, A., Side, L., Wolf, M. S., Horne, R., Wardle, J., & Cuzick, J. (2016). Factors affecting uptake and adherence to breast cancer chemoprevention: A systematic review and meta-analysis. Annals of Oncology: Official Journal of the European Society for Medical Oncology, 27(4), 575–590. https://doi.org/10.1093/annonc/mdv590
- Solomon, D. H., Avorn, J., Levin, R., & Brookhart, M. A. (2008). Uric acid lowering therapy: Prescribing patterns in a large cohort of older adults. Annals of the Rheumatic Diseases, 67(5), 609–613. https://doi.org/10.1136/ard.2007.076182
- Steinman, M. A., Sands, L. P., & Covinsky, K. E. (2001). Self-restriction of medications due to cost in seniors without prescription coverage. Journal of General Internal Medicine, 16(12), 793–799. https://doi.org/10.1046/j.1525-1497.2001.10412.x
- Sun, S. X., Ye, X., Lee, K. Y., Dupclay, L., & Plauschinat, C. (2008). Retrospective claims database analysis to determine relationship between renin-angiotensin system agents, rehospitalization, and health care costs in patients with heart failure or myocardial infarction. Clinical Therapeutics, 30, 2217–2227. https://doi.org/10.1016/j.clinthera.2008.12.005
- Sustersic, M., Gauchet, A., Duvert, A., Gonnet, L., Foote, A., Vermorel, C., Allenet, B., & Bosson, J.-L. (2019). Proposal for a Global Adherence Scale for Acute Conditions (GASAC): A prospective cohort study in two emergency departments. PLoS One, 14(12), e0215415. https://doi.org/10.1371/journal.pone.0215415
- Svensson, E., Nielsen, R. B., Hasvold, P., Aarskog, P., & Thomsen, R. W. (2015). Statin prescription patterns, adherence, and attainment of cholesterol treatment goals in routine clinical care: A Danish population-based study. Clinical Epidemiology, 7, 213–223. https://doi.org/10.2147/CLEP.S78145
- Thorneloe, R. j., Griffiths, C., e., m., & Cordingley, L. (2017). Medication non-adherence: The hidden problem in clinical practice. Journal of the European Academy of Dermatology and Venereology, 31(6), 923–924. https://doi.org/10.1111/jdv.14324
- Tolu, S., Rezvani, A., Karacan, İ., Bugdayci, D., Küçük, H. C., Bucak, Ö. F., & Aydin, T. (2020). Self-reported medication adherence in patients with ankylosing spondylitis: The role of illness perception and medication beliefs. Archives of Rheumatology, 35(4), 495–505. https://doi.org/10.46497/ArchRheumatol.2020.7732
- Tomaszewski, D., Aronson, B. D., Kading, M., & Morisky, D. (2017). Relationship between self-efficacy and patient knowledge on adherence to oral contraceptives using the Morisky Medication Adherence Scale (MMAS-8). Reproductive Health, 14(1), 110. https://doi.org/10.1186/s12978-017-0374-6
- Trueman, P., Taylor, D. G., Lowson, K., Bligh, A., Meszaros, A., Wright, D., Glanville, J., Newbould, J., Bury, M., Barber, N., & Jani, Y. H. (2010). Evaluation of the scale, causes and costs of waste medicines. Report of DH funded national project. [Report]. York Health Economics Consortium and The School of Pharmacy, University of London. http://php.york.ac.uk/inst/yhec/web/news/documents/Evaluation_of_NHS_Medicines_Waste_Nov_2010.pdf
- Tucker, J. D., Tso, L. S., Hall, B., Ma, Q., Beanland, R., Best, J., Li, H., Lackey, M., Marley, G., Rich, Z. C., Sou, K.-L., & Doherty, M. (2017). Enhancing public health HIV interventions: A qualitative meta-synthesis and systematic review of studies to improve linkage to care, adherence, and retention. EBioMedicine, 17, 163–171. https://doi.org/10.1016/j.ebiom.2017.01.036
- van der Laan, D. M., Elders, P. J. M., Boons, C. C. L. M., Beckeringh, J. J., Nijpels, G., & Hugtenburg, J. G. (2017). Factors associated with antihypertensive medication non-adherence: A systematic review. Journal of Human Hypertension, 31(11), 687–694. https://doi.org/10.1038/jhh.2017.48
- Vangeli, E., Bakhshi, S., Baker, A., Fisher, A., Bucknor, D., Mrowietz, U., Östör, A. J. K., Peyrin-Biroulet, L., Lacerda, A. P., & Weinman, J. (2015). A systematic review of factors associated with non-adherence to treatment for immune-mediated inflammatory diseases. Advances in Therapy, 32(11), 983–1028. https://doi.org/10.1007/s12325-015-0256-7
- Vermeire, E., Hearnshaw, H., Van Royen, P., & Denekens, J. (2001). Patient adherence to treatment: Three decades of research. A comprehensive review. Journal of Clinical Pharmacy and Therapeutics, 26(5), 331–342. https://doi.org/10.1046/j.1365-2710.2001.00363.x
- Vrijens, B., De Geest, S., Hughes, D. A., Przemyslaw, K., Demonceau, J., Ruppar, T., Dobbels, F., Fargher, E., Morrison, V., Lewek, P., Matyjaszczyk, M., Mshelia, C., Clyne, W., Aronson, J. K., & Urquhart, J, ABC Project Team. (2012). A new taxonomy for describing and defining adherence to medications. British Journal of Clinical Pharmacology, 73(5), 691–705. https://doi.org/10.1111/j.1365-2125.2012.04167.x
- Vrijens, B., Vincze, G., Kristanto, P., Urquhart, J., & Burnier, M. (2008). Adherence to prescribed antihypertensive drug treatments: Longitudinal study of electronically compiled dosing histories. BMJ, 336(7653), 1114–1117. https://doi.org/10.1136/bmj.39553.670231.25
- Ward, B. W., Schiller, J. S., & Goodman, R. A. (2014). Multiple chronic conditions among US adults: A 2012 update. Preventing Chronic Disease, 11, E62. https://doi.org/10.5888/pcd11.130389
- Weiner, J. R., Toy, E. L., Sacco, P., & Duh, M. S. (2008). Costs, quality of life and treatment compliance associated with antibiotic therapies in patients with cystic fibrosis: A review of the literature. Expert Opinion on Pharmacotherapy, 9(5), 751–766. https://doi.org/10.1517/14656566.9.5.751
- Weingarten, M. A., & Cannon, B. S. (1988). Age as a major factor affecting adherence to medication for hypertension in a general practice population. Family Practice, 5(4), 294–296. https://doi.org/10.1093/fampra/5.4.294
- Weinman, J., Graham, S., Canfield, M., Kleinstäuber, M., Perera, A. I., Dalbeth, N., & Petrie, K. J. (2018). The Intentional Non-Adherence Scale (INAS): Initial development and validation. Journal of Psychosomatic Research, 115, 110–116. https://doi.org/10.1016/j.jpsychores.2018.10.010
- Weiss, M. C., Platt, J., Riley, R., Chewning, B., Taylor, G., Horrocks, S., & Taylor, A. (2015). Medication decision making and patient outcomes in GP, nurse and pharmacist prescriber consultations. Primary Health Care Research & Development, 16(5), 513–527. https://doi.org/10.1017/S146342361400053X
- West, L. M., Borg Theuma, R., & Cordina, M. (2020). The ‘Necessity–Concerns Framework’ as a means of understanding non-adherence by applying polynomial regression in three chronic conditions. Chronic Illness, 16(4), 253–265. https://doi.org/10.1177/1742395318799847
- Wheeler, S. B., Spencer, J., Pinheiro, L. C., Murphy, C. C., Earp, J. A., Carey, L., Olshan, A., Tse, C. K., Bell, M. E., Weinberger, M., & Reeder-Hayes, K. E. (2019). Endocrine therapy nonadherence and discontinuation in black and white women. Journal of the National Cancer Institute, 111(5), 498–508. https://doi.org/10.1093/jnci/djy136
- Wilson, S. R., Strub, P., Buist, A. S., Knowles, S. B., Lavori, P. W., Lapidus, J., & Vollmer, W. M, Better Outcomes of Asthma Treatment (BOAT) Study Group. (2010). Shared treatment decision making improves adherence and outcomes in poorly controlled asthma. American Journal of Respiratory and Critical Care Medicine, 181(6), 566–577. https://doi.org/10.1164/rccm.200906-0907OC
- Yardley, L., Morrison, L., Bradbury, K., & Muller, I. (2015). The person-based approach to intervention development: Application to digital health-related behavior change interventions. Journal of Medical Internet Research, 17(1), e4055. https://doi.org/10.2196/jmir.4055
- Yeam, C. T., Chia, S., Tan, H. C. C., Kwan, Y. H., Fong, W., & Seng, J. J. B. (2018). A systematic review of factors affecting medication adherence among patients with osteoporosis. Osteoporosis International: A Journal Established as Result of Cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA, 29(12), 2623–2637. https://doi.org/10.1007/s00198-018-4759-3
- Yeaw, J., Benner, J. S., Walt, J. G., Sian, S., & Smith, D. B. (2009). Comparing adherence and persistence across 6 chronic medication classes. Journal of Managed Care Pharmacy, 15(9), 728–740. https://doi.org/10.18553/jmcp.2009.15.9.728
- Yu, Y., Luo, D., Chen, X., Huang, Z., Wang, M., & Xiao, S. (2018). Medication adherence to antiretroviral therapy among newly treated people living with HIV. BMC Public Health, 18(1), 825. https://doi.org/10.1186/s12889-018-5731-z
- Zhang, N. J., Terry, A., & McHorney, C. A. (2014). Impact of health literacy on medication adherence: A systematic review and meta-analysis. The Annals of Pharmacotherapy, 48(6), 741–751. https://doi.org/10.1177/1060028014526562
- Zillich, A. J., Jaynes, H. A. W., Snyder, M. E., Harrison, J., Hudmon, K. S., de Moor, C., & French, D. D. (2012). Evaluation of specialized medication packaging combined with medication therapy management. Medical Care, 50(6), 485–493. https://doi.org/10.1097/MLR.0b013e3182549d48
