Abstract
Objective
This study aimed to compare the differences between the framing of intention (approach vs. avoidance) and the type of self-regulatory capacity (planning vs. inhibition) to predict two behaviours (alcohol vs. vegetable consumption). Interaction effects between temporal self-regulation theory constructs were also explored.
Methods
UK participants were recruited online (N = 254) and completed measures of intention (approach and avoidance), self-regulatory capacity (planning and inhibition), and behavioural prepotency (habit) related to alcohol and vegetable consumption. One week later, consumption was assessed.
Results
Habit strength and approach-intentions consistently predicted consumption across each model for both behaviours. There was mixed support for avoidance-intentions and self-regulatory capacity variables in predicting consumption. Planning was more important in vegetable consumption than in alcohol consumption, and avoidance-intentions were only predictive in alcohol consumption. Inhibition was not significant for either behaviour. The interaction between approach-intention and planning was the only significant moderation detected and was only present in vegetable consumption.
Conclusion
The framing of intentions and the sub-facet of self-regulatory capacity are important to consider when attempting to explain health behaviours. Furthermore, theoretically defined moderation between temporal self-regulation theory variables might also depend on the type of behaviour and specific measured used to capture self-regulatory capacity.
Introduction
Globally, the majority of the burden of disease and mortality is related to chronic conditions, which, before COVID-19, exceeded the burden from all communicable diseases combined (Centers for Disease Control and Prevention, Citation2021). Health risk behaviours including unhealthy diet, smoking and alcohol consumption, are major contributors to chronic diseases (World Health Organization, Citation2009). However, the mechanisms underlying health behaviours are poorly understood, and in particular, why interventions aiming to change intentions sometimes fail to translate to actual behaviour (Sheeran, Citation2002).
Many researchers have attempted to account for this disparity between intention and behaviour, otherwise known as the intention-behaviour gap (Sniehotta et al., Citation2005a). Temporal self-regulation theory was specifically proposed to accomplish this by considering both rational and automatic processes of behaviour (Hall & Fong, Citation2007). According to Hall and Fong (Citation2007), intention, behavioural pre-potency (e.g., past behaviour, cues, and habit) and self-regulatory capacity (e.g., self-control, planning and executive function) will directly predict behaviour. Additionally, behavioural pre-potency and self-regulatory capacity will moderate the intention-behaviour relationship (Hall & Fong, Citation2007).
Temporal self-regulation theory and its constructs, whether used within the theoretical framework or outside of it, has contributed to bridging the intention-behaviour gap. For example, theoretical studies demonstrate the additional variance post-intentional constructs (i.e., behavioural prepotency and self-regulatory capacity) are able to explain in various health behaviours (e.g., Charlesworth et al., Citation2022; Dorina et al., Citation2021; Liddelow et al., Citation2022; McAlpine & Mullan, Citation2021). Research which incorporates aspects of its constructs outside of the theoretical framework (e.g., habit-based interventions) also contribute to bridging the gap by demonstrating success in changing behaviour (Feldhacker et al., Citation2023; Watson et al., Citation2023). But inconsistencies are observed for the importance of the constructs and the proposed moderating effects across behaviours (Dorina et al., Citation2023). For example, while self-control was a significant predictor of safe food handling behaviours, intention and habit were not significant predictors (Charlesworth et al., Citation2021). However, intention and habit were significant predictors of sugar sweetened beverage consumption while self-control was not (McAlpine & Mullan, Citation2021). Similar inconsistencies are observed for the proposed interaction effects (Frye & Shapiro, Citation2021; Liddelow et al., Citation2021; Murray & Mullan, Citation2019), therefore the role of intention, habit and self-control need to be further explored to better understand the mechanisms of behaviour.
The role of intention
Intentions are thought to be the strongest predictors of behaviour (McEachan et al., Citation2011). However, intentions do not always predict behaviour, especially when framed contradictory to the behaviour (i.e., to avoid), rather than in-line with the behaviour (i.e., to approach) (e.g., Charlesworth et al., Citation2022; Kothe et al., Citation2015). A recent meta-analysis revealed that intention-behaviour relationships were stronger for approach behaviours compared to avoidance behaviours, but notes that the directionality of intention (i.e., whether it is coded as approach or avoidance) may contribute to this (Dorina et al., Citation2023). This is supported somewhat by work in the neuroscience space which suggests that although there is some overlap, cognitive processes underlying approach and avoidance behaviour differ (McNaughton et al., Citation2016), thus it seems unreasonable to classify each as the direct opposite of the other. However little research has sought to compare both types of framing within the same study. As the framing of intentions on the influence of behaviour is not well understood, further exploration is needed to understand the mechanism of behaviour change.
The role of habit
Strong habits are predictive of future behaviour, occurring even in the absence of intention (Kwasnicka et al., Citation2016). However, it is argued that habits are still goal-directed (Kruglanski & Szumowska, Citation2020), and are more salient for simple and hedonic behaviours with immediate rewards than complex and distal benefit behaviours with non-immediate rewards (Mullan & Novoradovskaya, Citation2018). Therefore, established habits to perform a certain behaviour may contradict intentions to enact another behaviour (Brown et al., Citation2021). It can also be expected that established habits to perform a behaviour may weaken the influence of intentions to enact a behaviour (Gardner et al., Citation2020), however the evidence as to when and how habit can influence an intention to avoid a behaviour is less clear. Hence, further research is needed to better understand the role of habits in the context of intentional framing to better understand the mechanisms of behaviour.
The role of self-control
Greater self-control is linked with better health outcomes and greater ability to translate intentions into behaviour (Hofmann et al., Citation2008). However, self-control is multi-faceted (Hofmann et al., Citation2009; Miyake et al., Citation2000), including components such as the ability to inhibit immediate impulses (Baumeister et al., Citation2007), and planning to initiate and maintain behaviours (Sniehotta et al., Citation2005b). Hence, different aspects of self-control may be more relevant for various purposes and behaviour types (e.g., inhibition is likely to be important in resisting temptations for simple and hedonic behaviours and planning is likely to be important in enacting complex and distal benefit behaviours). But the importance of the different aspects of self-control on various behaviour types is not well understood, and further research is needed to understand how to change behaviour effectively.
The interactions between intention, habit, and self-control
Fundamental to temporal self-regulation theory, Hall and Fong (Citation2007) also proposed moderating roles for behavioural prepotency and self-regulatory capacity on the intention-behaviour relationship. However, vast inconsistencies occur across studies that report on these interactions, whereby interactions occur for some behaviours like medication adherence (Liddelow et al., Citation2021), but not for others such as safe food handling (Fulham & Mullan, Citation2011). Even within the same behaviour, different research has demonstrated different interactions (McAlpine & Mullan, Citation2021; Moran & Mullan, Citation2021). Furthermore, interaction effects seem to be more commonly observed among behavioural prepotency variables (Evans et al., Citation2017; Jones & Schüz, Citation2022; Liddelow et al., Citation2021; McAlpine & Mullan, Citation2021) as opposed to self-regulatory capacity variables (Black et al., Citation2017; Liddelow et al., Citation2021). Understanding the conditions in which each of these constructs are conducive to moderating the intention-behaviour relationship is critical for theoretical advancement, and subsequent practical application.
Attempts to synthesise these findings in the literature result in the framing of intentions as either approach or avoidance as one potential explanation for the discrepancies in interaction effects which has not been assessed as of yet. For example, when assessing the same behaviour in sugar-sweetened beverage consumption, moderation of the intention-behaviour relationship by behavioural prepotency was only present when intentions were framed as avoidant (McAlpine & Mullan, Citation2021) as opposed to approach (Moran & Mullan, Citation2021). This is somewhat supported by the work of Jones and Schüz (Citation2022), whereby they also demonstrated an interaction between behavioural prepotency (measured as social cues) and intentions to quit smoking (behavioural avoidance). Here, the intention is framed so as to avoid (quit) the behaviour where in contrast, there is a lack of evidence for support of an interaction when smoking intentions are framed as approach.
Another suggestion to explain the mixed findings, is that the type of self-regulatory capacity assessed may play a role in whether or not this construct moderates the intention-behaviour relationship. For instance, planning seems to be the most consistent moderator (Black et al., Citation2017; Liddelow et al., Citation2021) with other measures such as inhibition and trait self-control often exhibiting no interaction at all (Crandall et al., Citation2019; Evans et al., Citation2017; Fulham & Mullan, Citation2011; McAlpine & Mullan, Citation2021; Moran & Mullan, Citation2021; Murray & Mullan, Citation2019). Consideration of the specific sub-facet used to assess self-regulatory capacity seems to be as important as the framing of the direction of intention. However, given these interactions were assessed across multiple different behaviours, comparison of the moderating effect of different self-regulatory variables across the same behaviour will provide a deeper insight into these inconsistencies.
The present study
The aim of this study is therefore to explore the highlighted discrepancies by testing the importance of intention (both approach and avoidance), behavioural-prepotency (habit), and self-regulatory capacity (both inhibition and planning) across two different behaviours in vegetable consumption (a complex and distal benefit behaviour) and alcohol consumption (a simple and hedonic behaviour). The secondary aim is to explore the moderating effects between these variables across both behaviours. Specifically, we hypothesise that:
H1: Intentions (both approach and avoidance), habit and self-regulatory capacity (both inhibition and planning) will significantly predict both behaviours (alcohol and vegetable consumption).
H2: Approach-intentions will account for greater variance in behaviour than avoidance-intentions.
H3: Planning will account for greater variance in vegetable consumption than alcohol consumption.
H4: Inhibition will account for greater variance in alcohol consumption than vegetable consumption.
H5: Habit, planning, and inhibition will significantly moderate the relationships between approach-intentions and both behaviours, and avoidance-intentions and both behaviours. Specifically;
H5a: Habit will moderate the relationship between approach-intention and behaviour such that stronger habits will strengthen the relationship.
H5b: Habit will moderate the relationship between avoidance-intention and behaviour such that stronger habits will weaken the relationship.
H5c: Planning will moderate the approach-intention and behaviour relationship but not the avoidance-intention and behaviour relationship
H5d: Inhibition will moderate the relationship between both intention types (approach and avoidance) and behaviour such that stronger levels of inhibition will increase the relationship.
Methods
Participants
Two-hundred and fifty-two participants were recruited in waves through the paid participation platform Prolific between July and August 2022 at different days and times throughout the week. Participants were all living in the UK, had to be over 18 years of age, and normally consume vegetables and alcohol in an average week.
Procedure
A prospective correlational design was used to collect data at two time points. At time one, baseline questionnaires were administered to collect data pertaining to both alcohol and vegetable consumption including past behaviour, intention to consume, intention to avoid consuming, habit strength, and plans to consume. Baseline measures also assessed basic demographic information and levels of inhibition not specific to either behaviour. One week later, participants were invited to complete part two which assessed consumption of both alcohol and vegetables over the previous week. A total of 252 participants completed part two and were included in the final sample. This study was approved by the Curtin University Human Research Ethics Committee, Approval Number HRE2022-0353 and participants gave informed consent before participating.
Measures
Approach-intention
To assess intentions to consume, a basic two-item measure relating to Ajzen’s theory of planned behaviour (Ajzen, Citation1991) was adapted to suit the current research purposes. The two items (e.g., ‘I intend to ensure that I drink alcohol over the next week’) are scored on a 7-point Likert scale with response options that range from 1 = ‘strongly disagree’, to 7 = ‘strongly agree’, and are summed so that higher scores reflected higher intentions to consume alcohol. The same questions were adapted for vegetable consumption (i.e., ‘drink alcohol’ changed to ‘eat vegetables’). Cronbach’s were excellent for the present sample (see ).
Table 1. Means, standard deviations, Cronbach’s alpha and correlation coefficients between age, all predictor variables and behaviour.
Avoidance-intention
For avoidance-intentions other studies using temporal self-regulation theory have used the same measure as above, with wording changed to reflect intention to avoid (McAlpine & Mullan, Citation2021). This approach was used in the present research with the adapted two items used for each behaviour, scored in the same manner so that higher scores represented stronger intentions to avoid consuming. Cronbach’s alpha ranged from .87 to .93 for the present sample (see ).
Behavioural prepotency
Habit strength
Habit strength is often used as the sole measure for behavioural prepotency (Allom et al., Citation2018), given its consistently strong association with health behaviours when compared to other measures such as environmental cues, and past behaviour (McAlpine & Mullan, Citation2021; Moran & Mullan, Citation2021). The self-report behavioural automaticity index (SRBAI; Gardner et al., Citation2012), adapted from the self-report habit index (Verplanken & Orbell, Citation2003) was used to assess the habitual tendency for each of the behaviours, and consists of an anchor statement which describes the behaviour in question (e.g., ‘Drinking alcohol is something…’), followed by four items (e.g., ‘I do frequently’). Response options for each item are scored on a 7-point Likert scale ranging from 1 = ‘strongly disagree’, to 7 = ‘strongly agree’ and were averaged so that higher scores represent stronger habitual tendencies to consume alcohol and vegetables respectively. Scores ranged from 1 to 7, and Cronbach’s alpha was acceptable (see ).
Self-regulatory capacity
Planning
The Action Planning and Coping Scale (Sniehotta et al., Citation2005b) was used to assess whether participants had formed separate behaviour-specific plans to consume alcohol and vegetables. The Action Planning and Coping Scale measures behaviour-specific action planning and coping planning ability (Sniehotta et al., Citation2005b), however only the action planning component was deemed relevant for the present research. The action planning component consists of anchor statement (e.g., ‘I have made a detailed plan regarding…’), followed by four items which ask about when, where, how, and how often to engage in the behaviour (drink alcohol or eat vegetables). Responses are given on a 4-point Likert scale which range from 1 = ‘completely disagree’, to 4 = ‘completely agree’, and the items were averaged to contain a total score which ranged from 1-4, whereby higher scores indicate stronger plans for consumption. Cronbach’s alphas were excellent for both behaviours in the present sample (see ).
Inhibition
Participant’s inhibition levels were measured using the Resisting Temptation subscale of the Implicit Theory of Willpower scale (ITW-RT; Job et al., Citation2010). The measure assesses the degree of alignment with a limited theory of willpower for resisting temptations, i.e. whether participants believe that resisting temptations drains cognitive resources which weakens the ability to resist subsequent temptations (Bernecker & Job, Citation2017). Higher scores represent alignment with a more limited resource theory which is associated with poorer performance in self-control tasks (Bernecker & Job, Citation2017; Job et al., Citation2015). The subscale contains six items (e.g., ‘When situations accumulate that challenge you with temptations, it gets more and more difficult to resist the temptations’), which are scored on a 6-point Likert scale with response options ranging from 1 = ‘strongly disagree’, to 6 = ‘strongly agree’. Items are averaged and the present sample ranged from 1.33 to 6 so that higher scores therefore represented lower ability to inhibit impulses. Cronbach’s alpha for this scale was acceptable (see ).
Behaviour
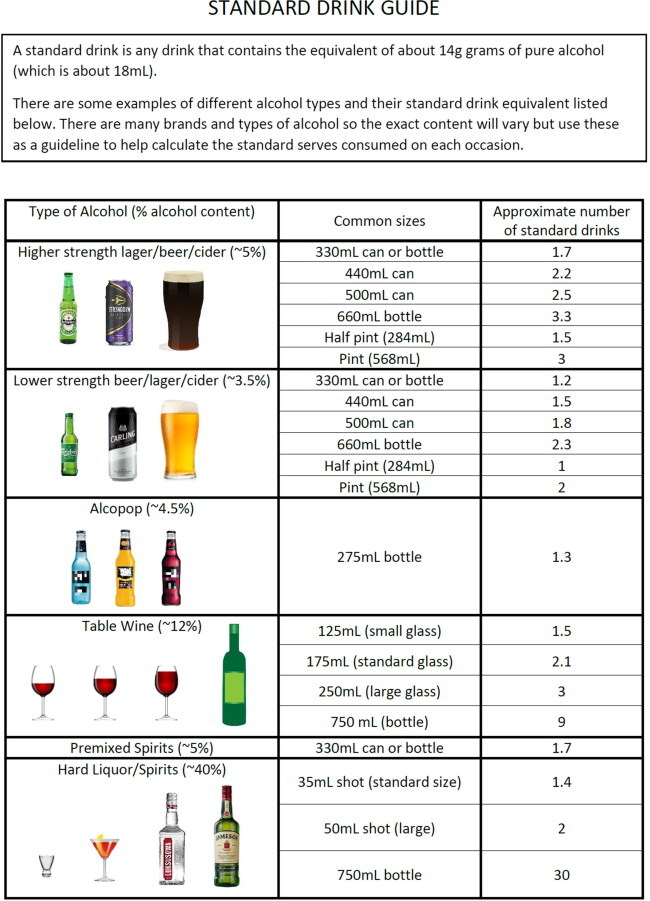
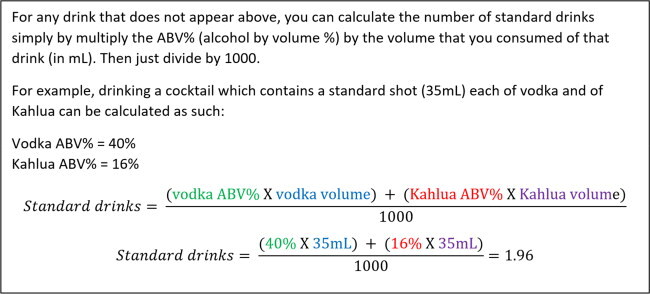
Both behaviours were measured retrospectively using the timeline follow-back method (Sobell & Sobell, Citation1992). Participants were instructed to recall special events that had occurred on each day (birthdays, whether working from home, bank holidays, etc.) which can improve recall by using salient properties of special events to rescue the memory for weaker events, in this case food and drink recall (Dunsmoor et al., Citation2022). They were then instructed to recall the number of standard serves they had consumed over the previous week. Visual aids were also included to help participant establish their consumption in number of standard serves.
Alcohol
For alcohol consumption, NHS guidelines (National Health Service, Citation2021) were used to develop examples of typical drinks accompanied with pictorial guides depicting how many standard serves were contained in common serving sizes (e.g., one pint of lower strength beer = two serves). These guides were given to participants alongside a standard serve calculator to help calculate serves for any type of alcohol not included in the examples (see Appendix A for more details). Scores for each time period were summed to create a total score for standard alcohol serves consumed during the prior week.
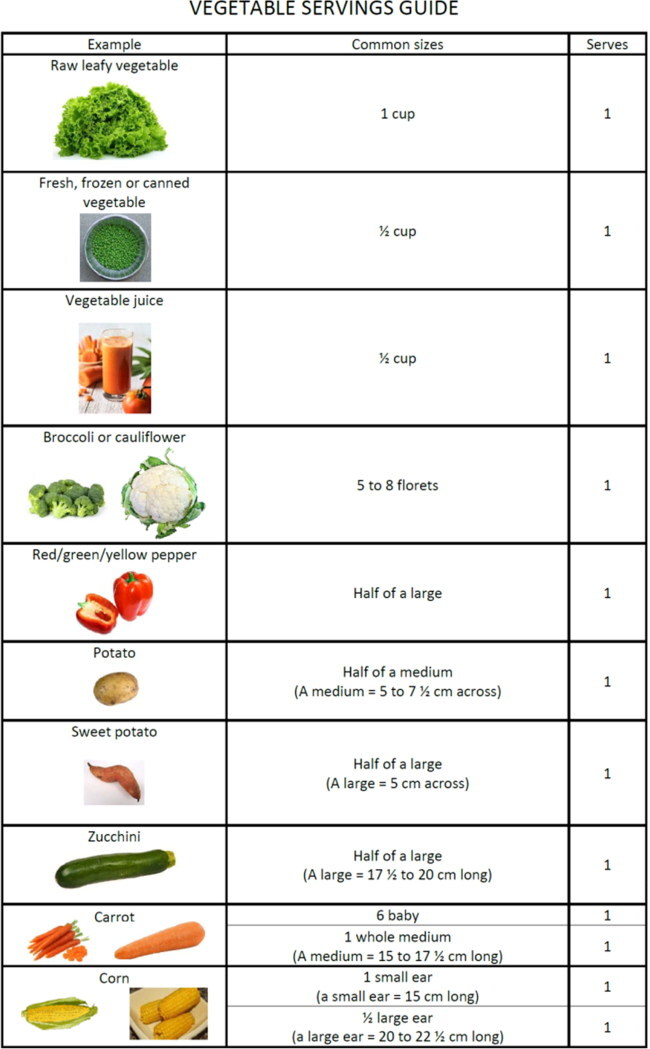
Vegetables
Similarly to alcohol, guidelines were used to establish standard serving sizes for vegetables (American Heart Association, Citation2017; British Heart Foundation, Citation2022). A pictorial guide with examples were given for common vegetables (see Appendix A for more details). Although it was planned to assess vegetable consumption over the previous week, pilot testing revealed that confidence in the recall of vegetable consumption was substantially lower than that of alcohol, and dietary recall accuracy diminishes over time (Smith, 1991). Therefore, only the most recent three days were retained for vegetable serves so as to increase accuracy of recall, and account for at least one weekday, since research also demonstrates that consumption behaviour can change during week and weekend days (An, Citation2016).
Demographics
Demographic questions were asked at baseline and included age, gender, highest level of education and ethnicity ().
Table 2. Sample demographics.
Statistical analyses
IBM SPSS (v. 27) was used for all analytic procedures. To assess the association of demographic variables with each of the outcome variables, bivariate correlations and point-biserial correlations were used for age and gender respectively. Spearman’s rho correlation coefficient was calculated to assess the relationship between education and behaviour. A one-way between groups ANOVA was used to determine whether behaviour differed by ethnicity group. Gender was the only demographic variable significantly associated with an outcome variable and was only related to alcohol consumption. As such, demographic variables were not included in subsequent analyses with the exception of gender, which was a covariate for all models assessing alcohol.
To determine the association between temporal self-regulation theory predictor variables (intention, avoidance-intention, habit, planning, and inhibition) and each behaviour, individual multiple regression analyses were conducted. This meant for each behaviour there were four models; two intention models (one for each measure of self-regulatory capacity, i.e., planning vs. inhibition), and two avoidance-intention models. For each model, variables were entered in the order specified by the theory (Hall & Fong, Citation2007), whereby related control variables were entered in block one, intention was entered in block two, habit (as a measure of behavioural prepotency) was entered in block three, and the respective self-regulatory capacity variable entered in block four.
To assess hypotheses relating to the moderation effects of predictor variables, for each model, two-way interaction terms were entered into the penultimate block, and the three-way interaction term was entered into the final block. Bonferroni corrections were applied to each of the four models when interpreting statistical significance.
Results
Prior to analyses, data were cleaned and screened for missingness and responses to the timeline follow-back were examined for errors. There were 54 participants with at least one missing value on one of the 42 response options (a morning, day, and evening period for each of the 7 days across both behaviours). Five of these cases were confirmed via follow-up as meaning no consumption for that period, 22 had entered values on other periods of the timeline and had accompanying notes which allowed us to infer that it meant no consumption, and the remaining 27 were left as missing since they did not complete all of part two, or consumption could not be inferred as zero. Missing values analysis revealed no significant difference on any variable between completers and non-completers, except for one of the habit items whereby non-completers were more likely to report higher scores than those who completed all of part two (2.64 compared to 1.97), t(28.1) = −2.3 (p = .027). The remaining 12 cases with at least one missing value reported across all variables had their missing values imputed using expectation maximisation.
Before conducting multiple regression analyses the assumptions for hierarchical multiple regression were tested. Normality was initially deemed to have been violated whereby Shapiro-Wilks demonstrated a significant departure from normality for all variables. However, given that large sample sizes tend to violate Shapiro-Wilks test (Ghasemi & Zahediasl, Citation2012), that multiple regression is robust to minor violations of normality when the sample size is large (Schmidt & Finan, Citation2018) and that inspection of the histograms looked reasonable for most variables, only the intention variables, and the outcome variables were considered for transformation.
The distribution of the approach-intention items demonstrated irregularities as an artefact of the phrasing of each of the two items, such that most participants responded with the same response option for each item, but a small subset of participants did not, which resulted in the majority of responses summing to a multiple of two, and a small fraction summing to an odd number. This is consistent in previous literature using a two-item measure (McAlpine & Mullan, Citation2021), thus odd scores were rounded down which resulted in a marked visual improvement in the shape of the distribution. The distribution of the outcome variables were affected by outliers on the upper end of each behaviour, and a bias towards zero responses, so were transformed by applying the square root function, and then dragging outliers back to within 3SD of the mean, which resulted in an improvement in the skewness values in each case.
No further violations of assumptions were encountered, except for at least two multivariate outliers being identified in each model. However, for all cases in each model, Cook’s value indicated that these were non-influential and therefore they were ignored.
Alcohol consumption
Model 1: intention and planning
Results from Model 1 revealed that after accounting for the statistically significant 6.4% of variance explained in alcohol by gender F (1, 249) = 17.12, p < .001, a further statistically significant 16.1% was accounted for by intention to consume ΔF (1, 248) = 51.58, p < .001. Habit was a significant predictor in block three accounting for an additional 2.3% of variance, ΔF (1, 247) = 7.56, p < .01. When added in block four, planning did not account for a significant additional proportion of variance, p = .618. In combination, the predictors accounted for a significant 24.9% of the variance in alcohol consumption, adjusted R2 = .24, F (4, 246) = 20.41, p < .001, and gender, intention and habit were all significantly unique contributors to the model in the final block (see for partial regression coefficients). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Table 3. Standardised (β), unstandardised (B), and partial regression coefficients (sr2) for each model predicting alcohol and vegetable consumption.
Model 2: intention and inhibition
Results from model 2 are identical to those of Model 1, with the exception of the final block, where inhibition did not account for any additional variance in alcohol consumption, p = .125. In combination the predictors accounted for a significant 25.6% of variance in the outcome variable, adjusted R2 = .24, F (4, 246) = 21.12, p < .001, and gender intention and habit were all significantly unique contributors to the model in the final block (). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Model 3: avoidance-intention and planning
Results from Model 3 revealed that after accounting for the statistically significant 6.4% of variance explained in alcohol by gender F (1, 249) = 17.12, p < .001, a further statistically significant 15.0% was accounted for by intentions to avoid, ΔF (1, 248) = 47.52, p < .001. Habit was a significant predictor in block three accounting for an additional significant 4.3%, ΔF (1, 247) = 14.45, p < .001. When added in block four, planning was not a significant predictor, p = .083. In combination, the predictors accounted for a significant 26.7% of the variance in alcohol consumption, adjusted R2 = .26, F (4, 246) = 22.43, p < .001, and gender, avoidance-intentions and habit were all significantly unique contributors to the model in the final block (). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Model 4: avoidance-intention and inhibition
Results from model 4 are identical to those of Model 1, with the exception of the final block, where inhibition did not account for any additional variance in alcohol consumption, p = .197. In combination the predictors accounted for a significant 26.3% of variance in the outcome variable, adjusted R2 = .25, F (4, 246) = 21.97, p < .001, and gender, avoidance-intentions and habit were all significantly unique contributors to the model in the final block (). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Vegetable consumption
Model 1: approach-intention and planning
Results from Model 1 revealed that intention was a significant predictor in block one, and accounted for 7.5% of the variance in vegetable consumption, F (1, 250) = 20.29, p < .001. Habit accounted for a further significant 3.7% of the variance in block two, ΔF (1, 249) = 10.50, p < .001. Planning did not account for any significant additional variance in block three, p = .084. When added in the final block, the interaction term between intention and planning was statistically significant, ΔF (1, 247) = 6.92, p = .009 In combination, the predictors accounted for a significant 14.7% of the variance, adjusted R2 = .13, F (4, 247) = 10.64, p < .001, and intention, habit, and the interaction term between intention and planning were all significantly unique contributors to the model in the final block ().
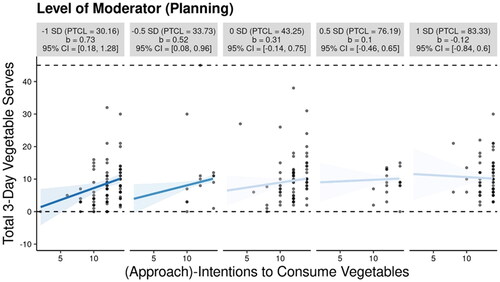
To further interpret the interaction effect, methods outlined by McCabe et al. (Citation2018) were used to demonstrate the intention-behaviour relationship at different levels of planning. The InterActive software overcomes common shortcomings of typical visual representation techniques by showing the regression line, accompanied by the 95% CI, and the underlying data points for each meaningfully chosen level of the moderator. In this case −1 SD, −0.5 SD, 0 SD, 0.5 SD, and 1 SD around the mean were chosen because there were minimal data points at the ±2 SD levels of the moderator). The interactions shown () were controlled for levels of habit (Cohen et al., Citation2003). shows that intention had a significant and positive association with consumption, only for those with weaker plans, whereby stronger intentions to consume vegetables translated to higher levels of vegetable consumption. Intention was not significantly associated with consumption when plans were medium (0 SD) or strong (0.5-1 SD).
Figure 1. Planning Moderating the Intention-Behaviour Relationship for Vegetable Consumption. Note. PTCL = Percentile. CI = Confidence Interval.
Model 2: approach-intention and inhibition
Results from Model 2 are identical to those of Model 1, with the exception of the final block, where inhibition was entered in place of planning. Similarly to planning, inhibition did not account for any additional variance in the model beyond what could already be explained by intention and habit, p = .063. In combination the predictors accounted for a significant 12.5% of the variance, adjusted R2 = .11, F (3, 248) = 11.78, p < .001, and intention and habit were both significantly unique contributors to the model in the final block (). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Model 3: avoidance-intention and planning
Results from Model 3 revealed that avoidance-intentions did not account for significant variance in vegetable consumption, p = .352. When added in block two, habit accounted for a significant 6.6% of the variance, ΔF (1, 249) = 16.68, p < .001. Unlike model 1, planning accounted for a significant additional 2.4% of the variance in vegetable consumption when added in block three, ΔF (1, 248) = 6.42, p = .012. In combination the predictors accounted for a significant 9.0% of the variance in vegetable consumption, adjusted R2 = .08, F (3, 248) = 8.14, p < .001, and habit and planning were both significantly unique contributors to the model in the final block (). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Model 4: avoidance-intention and inhibition
The results from Model 4 are identical to those of Model 3, with the exception of the final block, where inhibition was entered in place of planning. Unlike Model 3, block three (inhibition) did not account for significant variance over and above what could already be explained by habit, p = .217. In combination, the predictors accounted for a significant 7.2% of variance in vegetable consumption, adjusted R2 = .06, F (3, 248) = 6.39, p < .001, and habit was a significantly unique contributor to the model in the final block (). No interaction terms were significant in subsequent blocks so were excluded from the final model.
Discussion
The results demonstrate mixed support for our hypotheses. In line with temporal self-regulation theory, we hypothesized that all predictor variables would account for a statistically significant proportion of variance in the outcome variables in their respective models. While this was the case for intention and habit, avoidance-intention and self-regulatory capacity variables (planning and inhibition) were only significant in some models. Specifically, avoidance-intention was only significant for alcohol consumption models and not for vegetable consumption models, and planning was only a significant unique predictor for vegetable consumption in the avoidance-intention model. This is likely due to avoidance-intentions being harder to follow through with for alcohol than for vegetables due to other factors including addictive properties (Nutt & Peters, Citation1994) as well as social cues (Stanesby et al., Citation2019) which are less likely to be present to the same degree in vegetable consumption.
Although avoidance-intentions were not a significant predictor in every model, these findings do still support our second hypothesis, whereby approach-intentions would account for greater variance than avoidance-intentions. This is evident in our results where avoidance-intentions accounted for less variance than intention in alcohol models, and no variance at all in vegetable models. This can also be supported in literature where studies that measure avoidance-intentions seem to report less variance explained (McAlpine & Mullan, Citation2021) when compared to those that measure approach-intentions in the same behaviour (Moran & Mullan, Citation2021). The imperfect negative correlations (r < .60) between approach and avoidance-intentions within the same behaviours should also be noted as it supports the idea that these processes are not direct opposites of one another and more consideration should be given to the framing of intention when assessing health behaviours.
We found limited support for the importance of planning and inhibition. Planning was only important in the avoidance-intention vegetable model and not for any other model. This may be explained partially by the overlap in constructs of planning and intention such that when measuring intention in the same direction as planning (i.e., intending to consume), the variance accounted for in consumption by planning is already accounted for by intentions. However, when assessing intentions to avoid, planning is able to explain some unaccounted-for variance in the outcome variable which would otherwise have been explained by intention. This was not replicated for alcohol consumption, and thus shows partial support for our hypothesis that planning is more important for vegetable consumption than for alcohol.
Unfortunately, the same cannot be said for inhibition, as it was not significantly related to either outcome variable in any of the models. There is, therefore, insufficient evidence to reject the null hypothesis, and we cannot conclude that the components of self-regulatory capacity which align with inhibiting impulses or resisting temptations are more important for simple hedonic behaviours than for more complex behaviours with distal benefits. One explanation for the null findings here pertains to the measurement of inhibition as a self-report measure. Given that inhibition is argued to occur more as a controlled suppression of an automatic or prepotent response (Miyake et al., Citation2000) than as a reflective process, individuals may be poor at identifying true inhibitory capacity, and state-based measures such as a Stroop task may be more appropriate for future research, particularly given the associations they have demonstrated with other health behaviours (Hall et al., Citation2006).
In relation to our final hypotheses, the lack of consistent moderating effects, underscores the inconsistencies which are demonstrated in the literature, in that moderation was only demonstrated for planning in one of the behaviours we examined. Intention was unimportant at high levels of planning but was important for low levels. This initially seems contrary to research which identified that coping planning increased the intention-behaviour relationship (Brown et al., Citation2018). However, coping planning and action planning are different constructs (Sniehotta et al., Citation2005b), so it is possible that individuals who had more detailed (action) plans, did not need to rely on intentions to translate into behaviour since they had plans instead. This could explain why those with weak plans, were able to translate intentions into behaviour more easily. For example, an individual in this circumstance may have had to rely on intentions more, by intending to take the opportunity to consume vegetables when it arose, rather than make explicit plans.
In contrast, inhibition did not moderate the intention-behaviour relationship in neither the approach models nor the avoidance models. This finding is often reported when examining health behaviours (Booker & Mullan, Citation2013; Crandall et al., Citation2019; McAlpine & Mullan, Citation2021) and although this did not align with our hypothesis, it does add to the growing body of literature that suggests that perhaps inhibitory control does not moderate intention-behaviour relationship, even for simple hedonic behaviours. Overall, the findings help advance theoretical knowledge by demonstrating that interaction effects between temporal self-regulation theory constructs depend on both the type of behaviour as well as the measure used to represent its constructs. This has important implications for research and practice as it highlights that different sub-facets of self-regulatory capacity (i.e., planning over inhibition) may interact differently with intentions. Furthermore, understanding which elements of self-control are important for which behaviours could help facilitate development of evidence-based interventions to change behaviour and improve health.
At the overall level, vegetable models were able to account for more variance in behaviour than alcohol models. This is consistent with other theoretical models such as the theory of planned behaviour. Meta-analytic procedures demonstrate that diet behaviours are better predicted by its constructs than risk behaviours like drinking alcohol (McEachan et al., Citation2011). The reasons for this are unclear, however, the influence of affective variables in health behaviours have been shown to be important contributors to both healthy eating and alcohol use (Conner & Norman, Citation2021; Lawton et al., Citation2009). Importantly, for risk behaviours, affect is more predictive of behaviour when there is incongruence between the perceived benefits and affective enjoyment of enacting that behaviour (Lawton et al., Citation2009). But for promoting behaviours, the opposite trend is observed, whereby greater incongruence tends to weaken the predictive capability of affect on behaviour (Lawton et al., Citation2009). As such, it might be that neglecting important affective components of behaviour leads to comparatively weaker estimations of behaviour for risk behaviours compared to health promotion behaviours. Alternatively, habit predicted vegetable consumption marginally better than alcohol consumption in the present study and given the integral role of habits for healthy eating (Van’t Riet et al., Citation2011), differences might also be attributed to this.
Aside from the theoretical contributions, the present research also has some important practical implications. Although habit was a slightly better predictor for vegetable consumption than alcohol, habit was still a significant and unique predictor of behaviour for every model. This adds to the mass of literature which highlights the importance of habit in promoting health (Mergelsberg et al., Citation2021; Van’t Riet et al., Citation2011; Wood & Neal, Citation2016) and provides rationale for the development of habit-based interventions. These interventions may seek to target habit formation for healthy eating (Watson et al., Citation2023; Wood & Neal, Citation2016), but may also seek to incorporate elements of habit theory to break detrimental habits (Lally & Gardner, Citation2013). Efficacy of the latter strategy has not been documented extensively in the context of alcohol use which signals an important avenue for future research.
A limitation of this study was the use of self-report recall for both forms of behaviour. Although the proxy measure of confidence demonstrated that the error associated with recall of alcohol consumption was likely negligible, confidence in recall for vegetable consumption was notably poorer. This would no doubt increase measurement error and may also have contributed to the comparatively smaller proportion of variance explained by vegetable models than alcohol models. However, recall error has been a pervasive problem in much of the research that involves food recall (Subar et al., Citation2015), and no self-report measure is free from error (Archundia Herrera & Chan, Citation2018). To limit the impact of this however, recall from only the most recent three days were used, since recall accuracy for foods are generally believed to decrease over time (Park et al., Citation2018).
Conclusions
The present research extends on temporal self-regulation theory research in the important space of predicting health behaviours by comparing results across two distinctly different behaviours. Comparison of approach vs avoidance intention models demonstrated that making intentions to avoid a particular behaviour seem to be harder to follow through with than making intentions to engage in behaviour, evidenced by the comparatively smaller variance explained by avoidance-intentions in each model. Partial support was also garnered for the importance of planning as both a predictor and a moderator for more complex behaviours with distal benefits, exemplified by vegetable consumption in this study. Equally important was the comparison with the behavioural counterpart in alcohol consumption as a simple hedonic behaviour, which demonstrated no associations with planning, nor were any interaction effects present. This suggests that future research should carefully consider the type of behaviour being assessed in order to decide when planning ought to play a role in predicting behaviour or moderating the intention-behaviour relationship. Although inhibition was unable to predict either behaviour, the findings suggest that if an effect is present, state-measures of inhibition may be important to properly capture its role in predicting health behaviours.
Disclosure statement
The authors report there are no competing interests to declare.
Data availability
The data that support the findings of this study are openly available in Open Science Framework at osf.io/av8g6
Additional information
Funding
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-T
- Allom, V., Mullan, B., Clifford, A., & Rebar, A. (2018). Understanding supplement use: An application of temporal self-regulation theory. Psychology, Health & Medicine, 23(2), 178–188. https://doi.org/10.1080/13548506.2017.1339893
- American Heart Association. (2017). What’s a serving? https://www.heart.org/-/media/AHA/H4GM/Infographics/Fruits-and-Vegetables-Serving-Size-infographic.jpg
- An, R. (2016). Weekend-weekday differences in diet among U.S. adults, 2003–2012. Annals of Epidemiology, 26(1), 57–65. https://doi.org/10.1016/j.annepidem.2015.10.010
- Archundia Herrera, M. C., & Chan, C. B. (2018). Narrative review of new methods for assessing food and energy intake. Nutrients, 10(8), 1064. https://doi.org/10.3390/nu10081064
- Baumeister, R. F., Vohs, K. D., & Tice, D. M. (2007). The strength model of self-control. Current Directions in Psychological Science, 16(6), 351–355. https://doi.org/10.1111/j.1467-8721.2007.00534.x
- Bernecker, K., & Job, V. (2017). Implicit theories about willpower in resisting temptations and emotion control. Zeitschrift Für Psychologie, 225(2), 157–166. https://doi.org/10.1027/2151-2604/a000292
- Black, N., Mullan, B., & Sharpe, L. (2017). Predicting heavy episodic drinking using an extended temporal self-regulation theory. Addictive Behaviors, 73(October), 111–118. https://doi.org/10.1016/j.addbeh.2017.04.017
- Booker, L., & Mullan, B. (2013). Using the temporal self-regulation theory to examine the influence of environmental cues on maintaining a healthy lifestyle. British Journal of Health Psychology, 18(4), 745–762. https://doi.org/10.1111/bjhp.12015
- British Heart Foundation. (2022). Portion guide: Vegetables. https://www.bhf.org.uk/informationsupport/support/healthy-living/healthy-eating/healthy-eating-toolkit/food-portions/vegetables
- Brown, D. J., Charlesworth, J., Hagger, M. S., & Hamilton, K. (2021). A dual-process model applied to two health-promoting nutrition behaviours. Behavioral Sciences, 11(12), 170. https://www.mdpi.com/2076-328X/11/12/170 https://doi.org/10.3390/bs11120170
- Brown, D. J., Hagger, M. S., Morrissey, S., & Hamilton, K. (2018). Predicting fruit and vegetable consumption in long-haul heavy goods vehicle drivers: Application of a multi-theory, dual-phase model and the contribution of past behaviour. Appetite, 121, 326–336. https://doi.org/10.1016/j.appet.2017.11.106
- Centers for Disease Control and Prevention. (2021). About global NCDs. https://www.cdc.gov/globalhealth/healthprotection/ncd/global-ncd-overview.html#:∼:text=Noncommunicable%20diseases%20(NCDs)%2C%20such,all%20communicable%20disease%20deaths%20combined.
- Charlesworth, J., Green, A., & Mullan, B. (2022). Exploring rational and automatic processes in parents’ snack and beverage provision: The role of self-control, intention, and counter-intentional habit. Appetite, 178, 106185. https://doi.org/10.1016/j.appet.2022.106185
- Charlesworth, J., Mullan, B., & Moran, A. (2021). Investigating the predictors of safe food handling among parents of young children in the USA. Food Control, 126, 108015. https://doi.org/10.1016/j.foodcont.2021.108015
- Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression/correlation analysis for the behavioral sciences (3rd ed.). Lawrence Erlbaum Associates, Inc.
- Conner, M., & Norman, P. (2021). Predicting long-term healthy eating behaviour: Understanding the role of cognitive and affective attitudes. Psychology & Health, 36(10), 1165–1181. https://doi.org/10.1080/08870446.2020.1832675
- Crandall, A., Cheung, A., Young, A., & Hooper, A. P. (2019). Theory-based predictors of mindfulness meditation mobile app usage: A survey and cohort study. JMIR mHealth and uHealth, 7(3), e10794. https://doi.org/10.2196/10794
- Dorina, I., Mullan, B., Boyes, M., & Liddelow, C. (2023). Utility of temporal self-regulation theory in health and social behaviours: A meta-analysis. British Journal of Health Psychology, 28(2), 397–438. https://doi.org/10.1111/bjhp.12631
- Dorina, I., Mullan, B., & Novoradovskaya, E. (2021). Applying temporal self-regulation theory to identify correlates of soft plastic recycling in Australia. Australian Journal of Psychology, 73(4), 512–522. https://doi.org/10.1080/00049530.2021.2002125
- Dunsmoor, J. E., Murty, V. P., Clewett, D., Phelps, E. A., & Davachi, L. (2022). Tag and capture: How salient experiences target and rescue nearby events in memory. Trends in Cognitive Sciences, 26(9), 782–795. https://doi.org/10.1016/j.tics.2022.06.009
- Evans, R., Norman, P., & Webb, T. L. (2017). Using temporal self-regulation theory to understand healthy and unhealthy eating intentions and behaviour. Appetite, 116, 357–364. https://doi.org/10.1016/j.appet.2017.05.022
- Feldhacker, D. R., Ikiugu, M. N., Fritz, H., Schweinle, W. E., & Wang, H. (2023). Habit formation intervention to improve Type 2 diabetes self-management behaviors: A feasibility study. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association, 77(6), 7706205100. https://doi.org/10.5014/ajot.2023.050351
- Frye, W. S., & Shapiro, S. K. (2021). The role of executive functioning on the intention-behaviour relationship of health behaviours: A temporal self-regulatory perspective. Psychology & Health, 36(5), 612–627. https://doi.org/10.1080/08870446.2020.1767778
- Fulham, E., & Mullan, B. (2011). Hygienic food handling behaviors: Attempting to bridge the intention-behavior gap using aspects from temporal self-regulation theory. Journal of Food Protection, 74(6), 925–932. https://doi.org/10.4315/0362-028X.JFP-10-558
- Gardner, B., Abraham, C., Lally, P., & de Bruijn, G.-J. (2012). Towards parsimony in habit measurement: Testing the convergent and predictive validity of an automaticity subscale of the Self-Report Habit Index. The International Journal of Behavioral Nutrition and Physical Activity, 9(1), 102. https://doi.org/10.1186/1479-5868-9-102
- Gardner, B., Lally, P., & Rebar, A. L. (2020). Does habit weaken the relationship between intention and behaviour? Revisiting the habit-intention interaction hypothesis. Social and Personality Psychology Compass, 14(8), e12553. https://doi.org/10.1111/spc3.12553
- Ghasemi, A., & Zahediasl, S. (2012). Normality tests for statistical analysis: A guide for non-statisticians. International Journal of Endocrinology and Metabolism, 10(2), 486–489. https://doi.org/10.5812/ijem.3505
- Hall, P. A., Elias, L. J., & Crossley, M. (2006). Neurocognitive influences on health behavior in a community sample. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 25(6), 778–782. https://doi.org/10.1037/0278-6133.25.6.778
- Hall, P. A., & Fong, G. T. (2007). Temporal self-regulation theory: A model for individual health behavior. Health Psychology Review, 1(1), 6–52. https://doi.org/10.1080/17437190701492437
- Hofmann, W., Friese, M., & Strack, F. (2009). Impulse and self-control from a dual-systems perspective. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 4(2), 162–176. https://doi.org/10.1111/j.1745-6924.2009.01116.x
- Hofmann, W., Friese, M., & Wiers, R. W. (2008). Impulsive versus reflective influences on health behavior: A theoretical framework and empirical review. Health Psychology Review, 2(2), 111–137. https://doi.org/10.1080/17437190802617668
- Job, V., Bernecker, K., Miketta, S., & Friese, M. (2015). Implicit theories about willpower predict the activation of a rest goal following self-control exertion. Journal of Personality and Social Psychology, 109(4), 694–706. https://doi.org/10.1037/pspp0000042
- Job, V., Dweck, C. S., & Walton, G. M. (2010). Ego depletion—is it all in your head?: Implicit theories about willpower affect self-regulation. Psychological Science, 21(11), 1686–1693. https://doi.org/10.1177/0956797610384745
- Jones, C. M., & Schüz, B. (2022). Stable and momentary psychosocial correlates of everyday smoking: An application of Temporal Self-Regulation Theory. Journal of Behavioral Medicine, 45(1), 50–61. https://doi.org/10.1007/s10865-021-00248-4
- Kothe, E. J., Sainsbury, K., Smith, L., & Mullan, B. A. (2015). Explaining the intention–behaviour gap in gluten-free diet adherence: The moderating roles of habit and perceived behavioural control. Journal of Health Psychology, 20(5), 580–591. https://doi.org/10.1177/1359105315576606
- Kruglanski, A. W., & Szumowska, E. (2020). Habitual behavior is goal-driven. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 15(5), 1256–1271. https://doi.org/10.1177/1745691620917676
- Kwasnicka, D., Dombrowski, S. U., White, M., & Sniehotta, F. (2016). Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychology Review, 10(3), 277–296. https://doi.org/10.1080/17437199.2016.1151372
- Lally, P., & Gardner, B. (2013). Promoting habit formation. Health Psychology Review, 7(sup1), S137–S158. https://doi.org/10.1080/17437199.2011.603640
- Lawton, R., Conner, M., & McEachan, R. (2009). Desire or reason: Predicting health behaviors from affective and cognitive attitudes. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 28(1), 56–65. https://doi.org/10.1037/a0013424
- Liddelow, C., Mullan, B., & Boyes, M. (2021). Understanding the predictors of medication adherence: Applying temporal self-regulation theory. Psychology & Health, 36(5), 529–548. https://doi.org/10.1080/08870446.2020.1788715
- Liddelow, C., Mullan, B., Boyes, M., & Ling, M. (2022). Can temporal self-regulation theory and its constructs predict medication adherence? A systematic review and meta-analysis. Health Psychology Review, 17(4), 578–613. https://doi.org/10.1080/17437199.2022.2127831
- McAlpine, T., & Mullan, B. A. (2021). The role of environmental cues in sugar-sweetened beverage consumption using a temporal self-regulation theory framework. Appetite, 169(2), 105828. https://doi.org/10.1016/j.appet.2021.105828
- McCabe, C. J., Kim, D. S., & King, K. M. (2018). Improving present practices in the visual display of interactions. Advances in Methods and Practices in Psychological Science, 1(2), 147–165. https://doi.org/10.1177/2515245917746792
- McEachan, R. R. C., Conner, M., Taylor, N. J., & Lawton, R. J. (2011). Prospective prediction of health-related behaviours with the theory of planned behaviour: A meta-analysis. Health Psychology Review, 5(2), 97–144. https://doi.org/10.1080/17437199.2010.521684
- McNaughton, N., DeYoung, C. G., & Corr, P. J. (2016). Approach/avoidance. In J. R. Absher & J. Cloutier (Eds.), Neuroimaging personality, social cognition, and character (pp. 25–49). Elsevier. https://doi.org/10.1016/C2013-0-18623-0
- Mergelsberg, E. L. P., Mullan, B. A., Allom, V., & Scott, A. (2021). An intervention designed to investigate habit formation in a novel health behaviour. Psychology & Health, 36(4), 405–426. https://doi.org/10.1080/08870446.2020.1779272
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100. https://doi.org/10.1006/cogp.1999.0734
- Moran, A., & Mullan, B. (2021). Exploring temporal self-regulation theory to predict sugar-sweetened beverage consumption. Psychology & Health, 36(3), 334–350. https://doi.org/10.1080/08870446.2020.1774055
- Mullan, B., & Novoradovskaya, E. (2018). Habit mechanisms and behavioural complexity. In B. Verplanken (Ed.), The psychology of habit: Theory, mechanisms, change, and contexts (pp. 71–90). Springer International Publishing. https://doi.org/10.1007/978-3-319-97529-0_5
- Murray, K. S., & Mullan, B. (2019). Can temporal self-regulation theory and ‘sensitivity to reward’ predict binge drinking amongst university students in Australia? Addictive Behaviors, 99, e106069. https://doi.org/10.1016/j.addbeh.2019.106069
- National Health Service. (2021). Alcohol units. https://www.nhs.uk/live-well/alcohol-advice/calculating-alcohol-units/
- Nutt, D. J., & Peters, T. J. (1994). Alcohol: The drug. British Medical Bulletin, 50(1), 5–17. https://doi.org/10.1093/oxfordjournals.bmb.a072883
- Park, Y., Dodd, K. W., Kipnis, V., Thompson, F. E., Potischman, N., Schoeller, D. A., Baer, D. J., Midthune, D., Troiano, R. P., Bowles, H., & Subar, A. F. (2018). Comparison of self-reported dietary intakes from the automated self-administered 24-h recall, 4-d food records, and food-frequency questionnaires against recovery biomarkers. The American Journal of Clinical Nutrition, 107(1), 80–93. https://doi.org/10.1093/ajcn/nqx002
- Schmidt, A. F., & Finan, C. (2018). Linear regression and the normality assumption. Journal of Clinical Epidemiology, 98, 146–151. https://doi.org/10.1016/j.jclinepi.2017.12.006
- Sheeran, P. (2002). Intention—behavior relations: A conceptual and empirical review. European Review of Social Psychology, 12(1), 1–36. https://doi.org/10.1080/14792772143000003
- Smith, A. F. (1991). Cognitive processes in long-term dietary recall. Vital and Health Statistics, Series 6 (No. 4). National Center for Health Statistics. https://stacks.cdc.gov/view/11186/cdc_DS1.pdf
- Sniehotta, F. F., Scholz, U., & Schwarzer, R. (2005a). Bridging the intention–behaviour gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychology & Health, 20(2), 143–160. https://doi.org/10.1080/08870440512331317670
- Sniehotta, F. F., Schwarzer, R., Scholz, U., & Schüz, B. (2005b). Action planning and coping planning for long-term lifestyle change: Theory and assessment. European Journal of Social Psychology, 35(4), 565–576. https://doi.org/10.1002/ejsp.258 https://doi.org/10.1002/ejsp.258]
- Sobell, L. C., & Sobell, M. B. (1992). Timeline follow-back: A technique for assessing self-reported alcohol consumption. In Measuring alcohol consumption (pp. 41–72). Springer. https://doi.org/10.1007/978-1-4612-0357-5_3
- Stanesby, O., Labhart, F., Dietze, P., Wright, C. J. C., & Kuntsche, E. (2019). The contexts of heavy drinking: A systematic review of the combinations of context-related factors associated with heavy drinking occasions. PloS One, 14(7), e0218465. https://doi.org/10.1371/journal.pone.0218465
- Subar, A. F., Freedman, L. S., Tooze, J. A., Kirkpatrick, S. I., Boushey, C., Neuhouser, M. L., Thompson, F. E., Potischman, N., Guenther, P. M., Tarasuk, V., Reedy, J., & Krebs-Smith, S. M. (2015). Addressing current criticism regarding the value of self-report dietary data. The Journal of Nutrition, 145(12), 2639–2645. https://doi.org/10.3945/jn.115.219634
- Van’t Riet, J., Sijtsema, S. J., Dagevos, H., & De Bruijn, G.-J. (2011). The importance of habits in eating behaviour. An overview and recommendations for future research. Appetite, 57(3), 585–596. https://doi.org/10.1016/j.appet.2011.07.010
- Verplanken, B., & Orbell, S. (2003). Reflections on past behavior: A self-report index of habit strength. Journal of Applied Social Psychology, 33(6), 1313–1330. https://doi.org/10.1111/j.1559-1816.2003.tb01951.x
- Watson, S., McCrum, L.-A., McGuinness, B., Cardwell, C., Clarke, M., Woodside, J. V., McKenna, G., & McGowan, L. (2023). Establishing healthy eating ‘habits’: A pilot randomised controlled trial of a habit-based dietary intervention following oral rehabilitation for older adults. Nutrients, 15(3), 731. https://doi.org/10.3390/nu15030731
- Wood, W., & Neal, D. T. (2016). Healthy through habit: Interventions for initiating & maintaining health behavior change. Behavioral Science & Policy, 2(1), 71–83. https://doi.org/10.1177/237946151600200109
- World Health Organization. (2009). Global health risks: Mortality and burden of disease attributable to selected major risks. https://apps.who.int/iris/handle/10665/44203
Appendix A