
ABSTRACT
HIV viral load (VL) monitoring can reinforce antiretroviral therapy (ART) adherence. Standard VL testing requires high laboratory capacity and coordination between clinic and laboratory which can delay results. A randomized trial comparing point-of-care (POC) VL testing to standard VL testing among 150 adolescents and young adults, ages 10-24 years, living with HIV in Haiti determined if POC VL testing could return faster results and improve ART adherence and viral suppression. Participants received a POC VL test with same-day result (POC arm) or a standard VL test with result given 1 month later (SOC arm). POC arm participants were more likely to receive a test result within 6 weeks than SOC arm participants (94.7% vs. 80.1%; p1000 copies/ml and low self-reported ART adherence was stronger in the POC arm (OR: 6.57; 95%CI: 2.12-25.21) than the SOC arm (OR: 2.62; 95%CI: 0.97-7.44) suggesting more accurate self-report in the POC arm. POC VL testing was effectively implemented in this low-resource setting with faster results and is a pragmatic intervention that may enable clinicians to identify those with high VL to provide enhanced counseling or regimen changes sooner.
Trial registration: ClinicalTrials.gov identifier: NCT03288246.
Introduction
Globally four million adolescents and young adults (AYA) ages 15–24 are living with HIV (UNAIDS, Citation2018). Access to antiretroviral therapy (ART) has made it increasingly possible to provide life-saving HIV treatment in this vulnerable population. The goal of ART is to achieve viral suppression to re-establish immunological function, prevent further morbidity and mortality, and curb further HIV transmission. However, AYA have poorer ART adherence than all other age groups and are twice as likely to have an unsuppressed viral load (VL) (Kapogiannis et al., Citation2020; Nachega et al., Citation2009; Slogrove et al., Citation2017).
The World Health Organization (WHO) recommends HIV VL monitoring to regularly assess the effectiveness of ART (WHO, Citation2015). A high VL can indicate inadequate ART adherence or potential drug resistance and requires prompt enhanced adherence counseling or a change in ART regimen for those on a failing regimen (Phillips et al., Citation2015; WHO, Citation2013). Given AYA are at higher risk for unsuppressed VL and will require ART for years longer than adults, identifying poor adherence and preventing treatment failure with VL monitoring is important for this age group.
Standard laboratory-based HIV VL testing requires a high level of technical expertise and laboratory capacity which are commonly only established in large, central laboratories and not available on-site at clinics. Thus, coordinated transfer of specimens and results between the clinic and off-site laboratory is necessary which involves multiple patient visits for testing and receipt of results, and risks significant delays and/or misplaced or lost samples and results. On-site, point-of-care (POC) HIV VL testing can reduce this logistical complexity.
Returning and discussing VL results can reinforce ART adherence and support viral re-suppression (Bonner et al., Citation2013; Roberts et al., Citation2016; Wilson et al., Citation2009), thus a POC VL test with timely return of the result could enhance the impact of adherence counseling and lead to improved outcomes. Quicker VL test results could enable clinicians to provide real-time feedback about adherence and make clinical decisions about appropriate treatment sooner.
We conducted a randomized trial to evaluate whether POC VL testing could more efficiently return test results, and affect outcomes including ART adherence and viral suppression among AYA living with HIV and on ART in Port-au-Prince, Haiti.
Methods
Study site
This study was conducted at GHESKIO, the French acronym for the Haitian Group for the Study of Kaposi’s Sarcoma and Opportunistic Infections, an HIV/AIDS clinic in Port-au-Prince, Haiti. GHESKIO provides HIV care to over 700 AYA living with HIV and on ART. GHESKIO has an on-site satellite laboratory which performs rapid HIV testing and a large centralized laboratory approximately 1 hour drive from its primary patient clinic where all other HIV, CD4, and VL tests are performed in high throughput machines.
Study design
We conducted an unblinded randomized trial to test the hypothesis that POC VL testing will return VL test results sooner, and improve outcomes compared to standard laboratory-based VL testing (NCT03288246). Details of the research protocol have been previously published (Reif et al., Citation2020). The randomized design was chosen to evaluate a tightly defined health services intervention and limit bias from confounders. The trial was conducted in a resource-limited setting to enhance potential reproducibility of findings in similar settings. Individual participants were randomized 1:1 to either the point-of-care (POC) or standard of care (SOC) arms using a randomization software program. In the POC arm, VL tests were completed on-site and results returned with adherence counseling the same day. In the SOC arm, VL tests were completed according to standard care by transporting blood samples to the central laboratory and results returned with adherence counseling one month later. Participants in both arms received the same WHO-recommended adherence counseling guided by the VL test result (ICAP, Citation2018; WHO, Citation2017). The key difference between arms was the timing of adherence counseling – the same day as testing for the POC arm vs. one month later for the SOC arm. The protocol was approved by the ethics committees at Weill Cornell Medicine, GHESKIO, and Columbia University.
Study population
Eligibility criteria were age 10–24 years, aware of HIV status, on ART ≥6 months, with permanent residence in Port-au-Prince. Exclusion criteria were pregnancy, tuberculosis co-infection or other co-morbidities which would require additional clinical care. Participants ≥18 years provided written consent and <18 years provided written assent with written parental or guardian consent.
POC arm
All VL tests for participants in the POC arm were performed on the Cepheid GeneXpert system using Xpert HIV-1 Viral LoadTM cartridges (Cepheid, Sunnyvale, CA). A GeneXpert 4-module instrument was placed at the on-site laboratory and operated by laboratory technicians. This system uses individual cartridges which perform integrated extraction and quantitative real-time PCR for measurement of HIV-1 RNA. Processing the assay includes centrifuging the blood sample for 15 minutes to separate plasma, and then 90 minutes of run-time. Participants were asked to arrive before 11 am to allow time for same-day processing. When VL test results were ready, the laboratory technician called the study nurse for pick-up and the study nurse provided the result coupled with adherence counseling to the participant. If the result was not available the same-day, the participant returned for the result and adherence counseling as soon as available.
SOC arm
All VL tests for participants in the SOC arm were transported to the central laboratory and processed in weekly batches in a fully automated Abbott m2000sp/m200rt system (Abbott, Des Plaines, IL). Once available, results were manually entered by laboratory staff into an excel spreadsheet, emailed to the clinic, and manually entered by data management staff into the electronic medical record (EMR). At the next monthly visit the clinician retrieved the result from the EMR to return to the participant with adherence counseling. The timing of this process depended on the volume of samples needing to be processed, as well as laboratory and data management staffing.
Study procedures
VL testing was done at month 1 and month 6 in both arms. Following Haitian national guidelines, those with a VL ≥1000 copies/mL at month 1 had a repeat VL test at month 4. A questionnaire capturing socio-demographic and clinical history data was administrated at study enrollment. A VL knowledge questionnaire was administered at enrollment and 1 month after receiving VL results. Adherence assessments were administered at months 1, 4, and 6 (Supplementary Table 1).
Dried blood spots (DBS) collected from the first 62 participants enrolled (31 in each arm) who were receiving tenofovir in their ART regimen at the 6-month time point were tested for tenofovir-diphosphate (TDF-DP). TDF-DP drug level was measured using liquid chromatography-tandem mass spectrometry at the Colorado Antiviral Pharmacology Laboratory at the University of Colorado (Castillo-Mancilla et al., Citation2013).
Objectives, outcomes and measurements
The primary objective was to evaluate the adequacy of implementation of POC VL testing compared to standard laboratory-based VL testing. Completion of each VL testing step was assessed in each arm as well as the timing of each step. The primary outcome was defined as the proportion of participants in each arm to receive the VL test result within 6 weeks of sample collection. A 6-week window was allowed to take into account scheduling around school, work, or holidays. Reasons for failure to achieve any step and the duration of time between each step were ascertained.
Secondary objectives were to evaluate the effect on ART adherence, VL, and participant understanding of the relationship between ART adherence and VL at month 6. Self-reported ART adherence was measured using a modified AIDS Clinical Trials Group (ACTG) questionnaire (Chesney et al., Citation2000; Intasan et al., Citation2014; Reynolds et al., Citation2007). Three questions assessed self-reported adherence over the preceding 7 days: (1) the number of missed doses; (2) a scale rating of how good a job the participant did taking ART as prescribed; and (3) a scale rating of how often the participant took ART as prescribed. Optimal adherence was defined as a response of <2 doses, “very good”, and “always”, on questions 1, 2, and 3, respectively. Responses were recoded with equal weighting to create a standardized score out of 100 with 100 representing the best possible adherence. A composite 3-question score was created with equal weighting for the standardized score on each question.
ART adherence was also measured by TDF-DP drug level (f/mol per DBS), reported as mean and standard deviation (SD), and interpreted as the number of doses per week, categorized as: <2 doses, 2–3 doses, 4–6 doses, or 7 doses (optimal adherence).
VL tests in both arms were processed with the standard laboratory-based VL assay (Abbott) and these data used for the VL endpoints. The Cepheid Xpert assay and Abbott assay have the same threshold of detection (40 copies/mL) and are highly concordant (Ceffa et al., Citation2016; Gueudin et al., Citation2016).
Participants’ understanding of the relationship between VL and ART adherence was measured. Understanding of this relationship was defined as answering 3/5 (60%) questions correctly on an adapted questionnaire (Jones et al., Citation2013; Ownby et al., Citation2013; Tique et al., Citation2017) administered one month after receiving the VL result and adherence counseling.
Sample size
The study was powered to detect a 20% increase in the proportion of participants who received a VL result within 6 weeks of sample collection (i.e., primary outcome) and a 25% increase in the proportion of participants with a VL <1000 copies/mL (i.e., secondary outcome). A sample size of 124 (62 per arm) was chosen assuming 70% of participants would receive the VL test result within 6 weeks of sample collection in the SOC arm versus 90% in the POC arm, and 40% would have a VL <1000 copies/mL at month 6 in the SOC arm versus 65% in the POC arm. Assuming 85% follow-up, we enrolled 150 participants (75 per arm).
Analysis
The analysis was intent-to-treat comparing outcomes by arm of all 150 participants enrolled. Statistical comparisons of outcomes between arms used Chi-square tests for categorical variables, and t-tests for normally distributed continuous variables. McNemar tests were used for statistical differences between participants’ baseline and follow-up results. Logistic regression was used to examine associations between variables. All p-values are 2-tailed. All analyses were performed using R 3.6.3.
Results
Between 3 May 2018 and 16 April 2019, a total of 160 participants were screened for eligibility and 150 were enrolled and randomized (). Participant follow-up and data collection completed 30 January 2020. Participant median age was 20 years (IQR 18–22), 60% were male, and 70% had acquired HIV perinatally. The average age at ART initiation was 13 years with an average time on ART of 6 years. At ART initiation, a large majority of participants were prescribed an NRTI + NNRTI regimen, according to national guidelines. By the time of study enrollment, 45% had been switched to an NRTI + PI regimen or an NRTI + INSTI regimen. At study enrollment, 57% of participants had a VL <1000 copies/mL. Socio-demographic and clinical measurements were similar between arms at enrollment ().
Figure 1. Flow diagram of participant screening, enrollment, and follow-up.
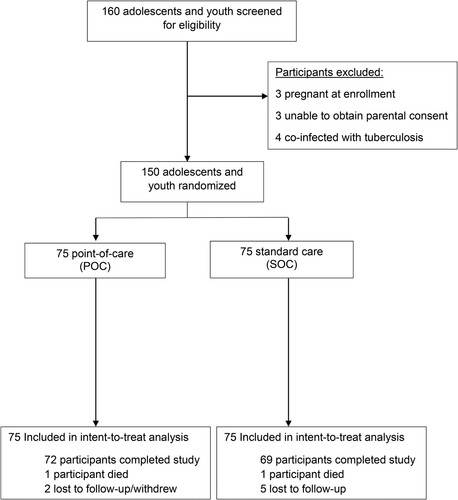
Table 1 . Clinical and socio-demographic characteristics at study enrollment and ART initiation of 150 participants ages 10–24 years enrolled in HIV care at GHESKIO in Port-au-Prince, Haiti.
Implementation outcomes
Participants in the POC arm were more likely to receive the VL test result within 6 weeks of blood collection than participants in the SOC arm (94.7% vs. 80.1%; p < 0.01) (). In the POC arm, median time between blood collection and participant receipt of results, for those who received a result the same day, was 2.7 hours (IQR: 2.5-3.2; range: 1.7–6.0). A total of 81.8% (148/181) of POC VL tests processed were returned the same day. When a POC VL test result was not returned the same day (33/181; 18.2%), the median time to receipt of result was 7 days (IQR 6–20; range: 1–36). In contrast, in the SOC arm, the median time between blood collection and availability of the result in the EMR was 8 days (IQR: 6–13; range: 5–39), and median time to participant receipt of the result was 30 days (IQR: 28–35; range: 19–126).
Table 2 . Implementation outcomes for point-of-care VL testing vs. standard laboratory VL testing.
The most common reason a POC VL test result was not returned the same day was that the clinic closed before assay processing completed (21/33; 63.6%). In 71.4% (15/21) of these instances, the participant arrived at the clinic after 11am. Other reasons included: the participant opted not to wait for the assay to be processed (8/33; 24.2%) or there was a stock-out of the cartridges the day of the VL test (4/33; 12.1%). When the result was not returned the same day, 90.9% (30/33) were still returned within 6 weeks. In total, of all the VL tests completed in the POC arm, only 1.7% (3/181) of results were not returned the same day and the participant did not return to receive the result within 6 weeks.
In the SOC arm, when a VL result was not returned within 6 weeks, the primary reason was the participant missed the next monthly visit, even when the result was available in the EMR (76.9%; 20/26). In the remaining 23.1% (6/26), the participant attended the visit but the result was unavailable because of a delay in either performing the assay at the central laboratory or relaying the result to the clinic.
The total amount of time spent in the clinic for VL testing and receipt of results was similar between the two arms despite the extra time for processing the POC VL test. In the POC arm, when blood collection, return of the VL test result, and adherence counseling were all completed in one visit, the visit lasted a median of 4.1 hours (IQR 3.6–4.7; range 2.7–5.8). In the SOC arm, two visits were required – one for blood collection and one for returning the VL result and adherence counseling. The visit for blood collection lasted a median of 1.9 hours (IQR 1.8–2.3; range 1.0–3.4) and the visit for returning the VL result and adherence counseling lasted a median of 1.9 hours (IQR 1.5–2.2; range 1.2–2.9). Combined, the two visits lasted a median of 3.9 hours (IQR 3.3–4.4, range 2.5–5.2).
Over the course of the study, 10 participants were observed to have treatment failure, defined as two consecutive VL measurements >1000 copies/mL, six (8.0%) in the POC arm and four (5.3%) in the SOC arm. All were switched to a second line regimen. In the POC arm, five switched the day of the blood draw, and one, who chose not to wait for the VL result, was switched at the next visit 29 days later. In the SOC arm, all four were switched at the next monthly visit, with a median time between blood draw and regimen change of 36.5 days (IQR 29–58.25; range 28–64).
ART adherence outcomes
Self-reported ART adherence was assessed before each VL test in both arms and TDF-DP drug levels were measured as a biomarker to compare with self-report. Self-reported adherence appeared to be worse in the POC arm (mean adherence score 75.6 (SD 26.6)) than the SOC arm (mean adherence score 87.1 (SD 18.7), p < 0.01)) (). However, TDF-DP drug levels were close to identical between the two arms, suggesting no difference in ART adherence between the arms. The mean TDF-DP fmol/punch was 993 in the POC arm and 866 in the SOC arm (p = 0.56) (). An unanticipated finding that explains this discrepancy is that self-reported ART adherence at month 6 was more strongly related to VL in the POC arm than in the SOC arm, indicating more accurate adherence reporting in the POC arm. In the POC arm, participants who reported sub-optimal adherence on any of the three questions were significantly more likely to have a VL ≥1000 copies/mL (OR: 6.6; 95% CI: 2.1–25.2), whereas in the SOC arm, the association was weaker (OR: 2.6; 95% CI: 0.9–7.4) (). TDF-DP drug levels were also more strongly related to self-reported ART adherence in the POC arm versus the SOC arm, further evidence of the increased accuracy of self-reported ART adherence in the POC arm (Supplementary Table 2).
Figure 2. Association of sub-optimal self-reported ART adherence and VL >1000 copies/mL at month 6.
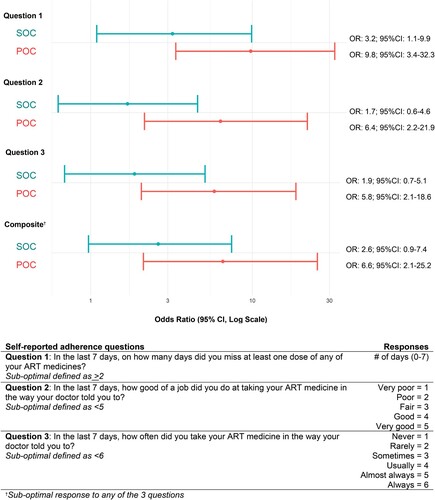
Table 3. Self-reported ART adherence by randomization arm at month 1 and month 6.
Table 4a. TDF-DP drug level outcomes by randomization arm and VL among first 62 participants enrolled at month 6.
Viral load outcomes
There were no differences in VL outcomes at month 6 in intent-to-treat analyses, if restricted to those with 6 month data, or in sensitivity analyses considering those lost to follow-up as failures (). Similar proportions in both arms changed VL status between months 1 and 6: 14.7% (11/75) in the POC arm and 13.3% (10/75) in the SOC arm achieved a VL <1000 copies/mL after being unsuppressed at month 1; 12.0% (9/75) in the POC arm and 14.7% (11/75) in the SOC arm experienced viral rebound (p = 0.87).
Table 4b . Viral load outcomes by randomization arm at month 6.
Risk factors for worse VL outcomes were younger age, longer time on treatment, and perinatal infection (relative to behavioral infection). In multivariable analysis, only perinatal infection was associated with worse VL after adjusting for age and duration of treatment. Participants who had acquired HIV perinatally were more likely to have a VL ≥1000 copies/mL (OR: 1.8; 95% CI: 0.9–4.0; p = 0.11) than those who acquired HIV behaviorally (Supplementary Table 3). Self-reported ART adherence and TDF-DP drug levels were similarly lower in perinatally-infected participants than in behaviorally-infected participants (Supplementary Tables 4a and 4b).
There was no difference between arms in understanding of the relationship between ART adherence and VL, though both arms improved in knowledge between baseline and follow-up (Supplemental Table 5).
Discussion
POC VL testing was effectively and efficiently integrated into a low-resource clinical setting and a majority of participants received test results the same day. POC VL testing also appeared to lead to more accurate self-reported ART adherence. This may enable clinicians to identify AYA with poor ART adherence and high VL and provide counseling or regimen changes sooner, preventing or mitigating HIV disease progression or the development of ART drug resistance.
Onsite POC VL testing reduced inefficiencies in the VL testing process. Even in limited instances when the result was not available the same day, multiple process steps were eliminated (e.g., transporting, batching, and data entry) and clinicians could access the result, identify a high VL, and schedule a visit within days. Enhanced adherence counseling, recommended by the WHO before an ART regimen change, is an important VL monitoring step (ICAP, Citation2018; WHO, Citation2013; WHO, Citation2017). Studies in low-resource settings have shown the time between identifying a high VL and beginning enhanced adherence counseling can range between 8 and 12 weeks (Diress et al., Citation2019; Nicholas et al., Citation2019). Decreasing this gap to a matter of days can decrease the time spent on an ineffective ART regimen or prevent the emergence of drug resistance.
Outcomes in the SOC arm were likely better than expected in routine care because of study-related retention activities or selection of more compliant participants in research, resulting in an underestimate of the positive impact of POC VL testing. Prior review of routine care at GHESKIO found 68% of adolescents were retained in care at 12 months, less than the 93% follow-up achieved in our study (Reif et al., Citation2016). Loss and inconsistent HIV care – disengaging and re-engaging from regular follow-up – is common among adolescents (Griffith & Agwu, Citation2017; Mark et al., Citation2017; Murray et al., Citation2017). Completing VL testing over multiple visits risks patient loss before poor outcomes can be identified and addressed. While the POC arm may have also achieved more optimal follow-up as research participants, POC VL testing is completed in a single visit making a difference in consistency of care less influential on outcomes.
An unexpected observed benefit of POC testing was improved accuracy of self-reported ART adherence. POC participants were more forthcoming about sub-optimal ART adherence, improving the accuracy, and thus the utility, of an easy and affordable adherence measurement (Simoni et al., Citation2006; Stirratt et al., Citation2015). We hypothesize there may be several issues accounting for more accurate self-reporting. First, the study was unblinded, and participants completed an adherence assessment before VL testing. POC participants likely anticipated the immediate VL result which would validate their self-report, and in turn, more honestly reported sub-optimal adherence. Second, a same day VL result could have made adherence counseling more personal, less abstract. The VL result was a direct indication of the participant’s current VL, having been measured from the blood sample taken that day. The counseling message could be centered around “your VL today”, and directly linked to negative consequences on health outcomes.
VL outcomes did not differ by arm. This is disappointing and may suggest that our study population, 70% of which acquired HIV perinatally and were highly ART-experienced, may experience a combination of drug fatigue and encountering new challenges as they age into adolescence that put them a heightened risk for poor adherence (Bikaako-Kajura et al., Citation2006; Lowenthal et al., Citation2014; Makadzange et al., Citation2015). Further, the proportion of our study population who remained on NNRTI ART regimens may have developed resistance rendering any adherence changes alone, insufficient to improve viral suppression. In contrast to our findings, the STREAM trial evaluated POC VL testing among adults in South Africa receiving their first VL test 6 months after initiating ART, and found that 90% of participants achieved a VL <200 copies/mL, compared to 76% of participants receiving standard laboratory testing (Drain et al., Citation2020). POC VL testing in a less ART-experienced AYA population may result in similar positive effects on VL outcomes.
We note several limitations. A POC VL test is narrow in scope as an intervention to address multi-pronged barriers to poor ART adherence. POC VL testing could be used in concert with additional interventions to address diverse challenges (Belzer et al., Citation2018; Cluver et al., Citation2016; Dillingham et al., Citation2018; MSF, Citation2016). Further, a participant on an ineffective drug regimen will not achieve viral suppression even with perfect adherence. However, the WHO-recommended guidelines for identifying treatment failure once high VL is detected and switching ART regimens is to first provide enhanced adherence counseling and establish an accurate adherence measurement. A POC VL test may enable clinicians to accurately assess adherence sooner leading to a faster switch to a more effective ART drug regimen, if indicated.
Conclusion
In conclusion, POC VL testing more efficiently returned VL test results. By optimizing an essential HIV health service like VL monitoring, particularly for a high-risk population with persistently poor HIV outcomes, POC VL testing could reduce barriers to improving ART adherence and viral suppression.
Supplemental Material
Download MS Word (395.5 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Belzer, M. E., MacDonell, K. K., Ghosh, S., Naar, S., McAvoy-Banerjea, J., Gurung, S., Cain, D., Fan, C. A., & Parsons, J. T. (2018). Adaptive antiretroviral therapy adherence interventions for youth living With HIV through text message and cell phone support with and without incentives: Protocol for a sequential multiple assignment randomized trial (SMART). JMIR Research Protocols, 7(12), e11183. https://doi.org/10.2196/11183
- Bikaako-Kajura, W., Luyirika, E., Purcell, D. W., Downing, J., Kaharuza, F., Mermin, J., Malamba, S., & Bunnell, R. (2006). Disclosure of HIV status and adherence to daily drug regimens among HIV-infected children in Uganda. AIDS and Behavior, 10(4 Suppl), S85–S93. https://doi.org/10.1007/s10461-006-9141-3
- Bonner, K., Mezochow, A., Roberts, T., Ford, N., & Cohn, J. (2013). Viral load monitoring as a tool to reinforce adherence: A systematic review. Journal of Acquired Immune Deficiency Syndromes, 64(1), 74–78. https://doi.org/10.1097/QAI.0b013e31829f05ac
- Castillo-Mancilla, J. R., Zheng, J. H., Rower, J. E., Meditz, A., Gardner, E. M., Predhomme, J., Fernandez, C., Langness, J., Kiser, J. J., Bushman, L. R., & Anderson, P. L. (2013). Tenofovir, emtricitabine, and tenofovir diphosphate in dried blood spots for determining recent and cumulative drug exposure. AIDS Research and Human Retroviruses, 29(2), 384–390. https://doi.org/10.1089/AID.2012.0089. Epub 2012 Oct 10.
- Ceffa, S., Luhanga, R., Andreotti, M., Brambilla, D., Erba, F., Jere, H., Mancinelli, S., Giuliano, M., Palombi, L., & Marazzi, M. C. (2016). Comparison of the Cepheid GeneXpert and Abbott M2000 HIV-1 real time molecular assays for monitoring HIV-1 viral load and detecting HIV-1 infection. Journal of Virological Methods, 229, 35–39. https://doi.org/10.1016/j.jviromet.2015.12.007
- Chesney, M. A., Ickovics, J. R., Chambers, D. B., Gifford, A. L., Neidig, J., Zwickl, B., & Wu, A. W. (2000). Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: The AACTG adherence instruments. Patient Care Committee & Adherence Working Group of the outcomes Committee of the adult AIDS Clinical Trials Group (AACTG). AIDS Care, 12(3), 255–266. https://doi.org/10.1080/09540120050042891
- Cluver, L. D., Toska, E., Orkin, F. M., Meinck, F., Hodes, R., Yakubovich, A. R., & Sherr, L. (2016). Achieving equity in HIV-treatment outcomes: Can social protection improve adolescent ART-adherence in South Africa? AIDS Care, 28(Suppl 2), 73–82. https://doi.org/10.1080/09540121.2016.1179008
- Dillingham, R., Ingersoll, K., Flickinger, T. E., Waldman, A. L., Grabowski, M., Laurence, C., Wispelwey, E., Reynolds, G., Conaway, M., & Cohn, W. F. (2018). Positivelinks: A mobile Health intervention for retention in HIV care and clinical outcomes with 12-month follow-up. AIDS Patient Care and STDs, 32(6), 241–250. https://doi.org/10.1089/apc.2017.0303
- Diress, G., Dagne, S., Alemnew, B., Adane, S., & Addisu, A. (2019). Viral load suppression after enhanced adherence counseling and Its predictors among high viral load HIV seropositive people in North Wollo Zone Public Hospitals, Northeast Ethiopia, 2019: Retrospective cohort study. AIDS Research and Treatment, 2020, 8909232. https://doi.org/10.1155/2020/8909232
- Drain, P. K., Dorward, J., Violette, L. R., Quame-Amaglo, J., Thomas, K. K., Samsunder, N., Ngobese, H., Mlisana, K., Moodley, P., Donnell, D., Barnabas, R. V., Naidoo, K., Abdool Karim, S. S., Celum, C., & Garrett, N. (2020). Point-of-care HIV viral load testing combined with task shifting to improve treatment outcomes (STREAM): findings from an open-label, non-inferiority, randomised controlled trial. The Lancet. HIV, 7(4), e229–e237. https://doi.org/10.1016/S2352-3018(19)30402-3
- Griffith, D. C., & Agwu, A. L. (2017). Caring for youth living with HIV across the continuum: Turning gaps into opportunities. AIDS Care, 29(10), 1205–1211. https://doi.org/10.1080/09540121.2017.1290211
- Gueudin, M., Baron, A., Alessandri-Gradt, E., Lemée, V., Mourez, T., Etienne, M., & Plantier, J. C. (2016). Performance evaluation of the new HIV-1 quantification assay, Xpert HIV-1 viral load, on a wide panel of HIV-1 variants. JAIDS Journal of Acquired Immune Deficiency Syndromes, 72(5), 521–526. https://doi.org/10.1097/QAI.0000000000001003
- ICAP at Columbia University. (2018). Viral load monitoring and enhanced adherence counseling flipchart: Adolescents. Retrieved May 2, 2018 from, http://icapcolumbiaedu/resources/detail/viral-load-toolkit-flipcharts
- Intasan, J., Bunupuradah, T., Vonthanak, S., Kosalaraksa, P., Hansudewechakul, R., Kanjanavanit, S., Ngampiyaskul, C., Wongsawat, J., Luesomboon, W., Apornpong, T., Kerr, S., Ananworanich, J., Puthanakit, T., & PREDICT Study Group (2014). Comparison of adherence monitoring tools and correlation to virologic failure in a pediatric HIV clinical trial. AIDS Patient Care and STDs, 28(6), 296–302. https://doi.org/10.1089/apc.2013.0276
- Jones, D., Cook, R., Rodriguez, A., & Waldrop-Valverde, D. (2013). Personal HIV knowledge, appointment adherence and HIV outcomes. AIDS and Behavior, 17(1), 242–249. https://doi.org/10.1007/s10461-012-0367-y
- Kapogiannis, B. G., Koenig, L. J., Xu, J., Mayer, K. H., Loeb, J., Greenberg, L., Monte, D., Banks-Shields, M., Fortenberry, J. D., & Adolescent Medicine Trials Network for HIV/AIDS Interventions (2020). The HIV continuum of care for adolescents and young adults attending 13 urban US HIV care centers of the NICHD-ATN-CDC-HRSA SMILE collaborative. JAIDS Journal of Acquired Immune Deficiency Syndromes, 84(1), 92–100. https://doi.org/10.1097/QAI.0000000000002308
- Lowenthal, E. D., Bakeera-Kitaka, S., Marukutira, T., Chapman, J., Goldrath, K., & Ferrand, R. A. (2014). Perinatally acquired HIV infection in adolescents from sub-Saharan Africa: A review of emerging challenges. The Lancet Infectious Diseases, 14(7), 627–639. https://doi.org/10.1016/S1473-3099(13)70363-3
- Makadzange, A. T., Higgins-Biddle, M., Chimukangara, B., Birri, R., Gordon, M., Mahlanza, T., McHugh, G., van Dijk, J. H., Bwakura-Dangarembizi, M., Ndung'u, T., Masimirembwa, C., Phelps, B., Amzel, A., Ojikutu, B. O., Walker, B. D., & Ndhlovu, C. E. (2015). Clinical, virologic, immunologic outcomes and emerging HIV drug resistance patterns in children and adolescents in public ART care in Zimbabwe. PloS One, 10(12), e0144057. https://doi.org/10.1371/journal.pone.0144057
- Mark, D., Armstrong, A., Andrade, C., Penazzato, M., Hatane, L., Taing, L., Runciman, T., & Ferguson, J. (2017). HIV treatment and care services for adolescents: A situational analysis of 218 facilities in 23 sub-Saharan african countries. Journal of the International AIDS Society, 20(Suppl 3), 21591. https://doi.org/10.7448/IAS.20.4.21591
- Medecins Sans Frontieres Khayelisha. (2016). Youth linkage and retention interventions from HIV diagnosis to adult care transition: Report and toolkit. MSF.
- Murray, K. R., Dulli, L. S., Ridgeway, K., Dal Santo, L., Darrow de Mora, D., Olsen, P., Silverstein, H., & McCarraher, D. R. (2017). Improving retention in HIV care among adolescents and adults in low- and middle-income countries: A systematic review of the literature. PloS one, 12(9), e0184879. https://doi.org/10.1371/journal.pone.0184879
- Nachega, J. B., Hislop, M., Nguyen, H., Dowdy, D. W., Chaisson, R. E., Regensberg, L., Cotton, M., & Maartens, G. (2009). Antiretroviral therapy adherence, virologic and immunologic outcomes in adolescents compared with adults in Southern Africa. JAIDS Journal of Acquired Immune Deficiency Syndromes, 51(1), 65–71. https://doi.org/10.1097/QAI.0b013e318199072e
- Nicholas, S., Poulet, E., Wolters, L., Wapling, J., Rakesh, A., Amoros, I., Szumilin, E., Gueguen, M., & Schramm, B. (2019). Point-of-care viral load monitoring: Outcomes from a decentralized HIV programme in Malawi. Journal of the International AIDS Society, 22(8), e25387. https://doi.org/10.1002/jia2.25387
- Ownby, R. L., Waldrop-Valverde, D., Hardigan, P., Caballero, J., Jacobs, R., & Acevedo, A. (2013). Development and validation of a brief computer-administered HIV-Related Health Literacy Scale (HIV-HL). AIDS and Behavior, 17(2), 710–718. https://doi.org/10.1007/s10461-012-0301-3
- Working Group on Modelling of Antiretroviral Therapy Monitoring Strategies in Sub-Saharan Africa, Phillips, A., Shroufi, A., Vojnov, L., Cohn, J., Roberts, T., Ellman, T., Bonner, K., Rousseau, C., Garnett, G., Cambiano, V., Nakagawa, F., Ford, D., Bansi-Matharu, L., Miners, A., Lundgren, J. D., Eaton, J. W., Parkes-Ratanshi, R., Katz, Z., … Revill, P. (2015). Sustainable HIV treatment in Africa through viral-load-informed differentiated care. Nature, 528(7580), S68–S76. https://doi.org/10.1038/nature16046
- Reif, L. K., Belizaire, M. E., Seo, G., Rouzier, V., Severe, P., Joseph, J. M., Joseph, B., Apollon, S., Abrams, E. J., Arpadi, S. M., Elul, B., Pape, J. W., McNairy, M. L., Fitzgerald, D. W., & Kuhn, L. (2020). Point-of-care viral load testing among adolescents and youth living with HIV in Haiti: A protocol for a randomized trial to evaluate implementation and effect. BMJ Open, 10(8), e036147. https://doi.org/10.1136/bmjopen-2019-036147
- Reif, L. K., Bertrand, R., Benedict, C., Lamb, M. R., Rouzier, V., Verdier, R., Johnson, W. D., Pape, J. W., Fitzgerald, D. W., Kuhn, L., & McNairy, M. L. (2016). Impact of a youth-friendly HIV clinic: 10 years of adolescent outcomes in Port-au-Prince, Haiti. Journal of the International AIDS Society, 19(1), 20859. https://doi.org/10.7448/IAS.19.1.20859
- Reynolds, N. R., Sun, J., Nagaraja, H. N., Gifford, A. L., Wu, A. W., & Chesney, M. A. (2007). Optimizing measurement of self-reported adherence with the ACTG adherence questionnaire: A cross-protocol analysis. JAIDS Journal of Acquired Immune Deficiency Syndromes, 46(4), 402–409. https://doi.org/10.1097/qai.0b013e318158a44f
- Roberts, T., Cohn, J., Bonner, K., & Hargreaves, S. (2016). Scale-up of routine viral load testing in resource-poor settings: Current and future implementation challenges. Clinical Infectious Diseases, 62(8), 1043–1048. https://doi.org/10.1093/cid/ciw001
- Simoni, J. M., Kurth, A. E., Pearson, C. R., Pantalone, D. W., Merrill, J. O., & Frick, P. A. (2006). Self-report measures of antiretroviral therapy adherence: A review with recommendations for HIV research and clinical management. AIDS and Behavior, 10(3), 227–245. https://doi.org/10.1007/s10461-006-9078-6
- Slogrove, A. L., Mahy, M., Armstrong, A., & Davies, M. A. (2017). Living and dying to be counted: What we know about the epidemiology of the global adolescent HIV epidemic. Journal of the International AIDS Society, 20(Suppl 3), 21520. https://doi.org/10.7448/IAS.20.4.21520
- Stirratt, M. J., Dunbar-Jacob, J., Crane, H. M., Simoni, J. M., Czajkowski, S., Hilliard, M. E., Aikens, J. E., Hunter, C. M., Velligan, D. I., Huntley, K., Ogedegbe, G., Rand, C. S., Schron, E., & Nilsen, W. J. (2015). Self-report measures of medication adherence behavior: Recommendations on optimal use. Translational Behavioral Medicine, 5(4), 470–482. https://doi.org/10.1007/s13142-015-0315-2
- Tique, J. A., Howard, L. M., Gaveta, S., Sidat, M., Rothman, R. L., Vermund, S. H., & Ciampa, P. J. (2017). Measuring health literacy among adults with HIV infection in Mozambique: Development and validation of the HIV literacy test. AIDS and Behavior, 21(3), 822–832. https://doi.org/10.1007/s10461-016-1348-3
- UNAIDS. (2018). Youth and HIV. Mainstreaming a three-lens approach to youth participation. https://wwwunaidsorg/sites/default/files/media_asset/youth-and-hiv_enpdf
- Wilson, D., Keiluhu, A. K., Kogrum, S., Reid, T., Seriratana, N., Ford, N., Kyawkyaw, M., Talangsri, P., & Taochalee, N. (2009). HIV-1 viral load monitoring: An opportunity to reinforce treatment adherence in a resource-limited setting in Thailand. Transactions of the Royal Society of Tropical Medicine and Hygiene, 103(6), 601–606. https://doi.org/10.1016/j.trstmh.2008.11.007
- World Health Organization. (2013). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection.
- World Health Organization. (2017). Topics at a glance. Adolescent Health. HIV and Youth. Geneva: World Health Organization. Retrieved 11/11/2017, from http://www.who.int/maternal_child_adolescent/topics/adolescence/hiv/en/
- World Health Organization. (2017). Adapting and implementing new recommendation on HIV patient monitoring. Geneva. World Health Organization. Available from: https://apps.who.int/iris/bitstream/handle/10665/255867/WHO-HIV-2017.13-eng.pdf?sequence=1.
- World Heatlh Organization. (2015). HIV treatment and care, what's New in service delivery fact sheet. WHO. http://apps.who.int/iris/bitstream/10665/204461/1/WHO_HIV_2015.46_eng.pdf?ua=1
