
ABSTRACT
Objectives
This paper explores the decision-making processes involved in giving physiotherapy students responsibility on clinical placement and the impact on their developing professional autonomy.
Methods
The qualitative study, using semi-structured interviews, involved physiotherapy students and clinical educators (CEs) from two higher education institutions, one in Australia, and the other in the United Kingdom (UK).
Findings
Findings led to the development of a heuristic framework of ‘graduated supervision,’ a process of progressively less direct observation and monitoring of students as clinical proficiency improved. By focusing on the measured exposure of students to increasing complexity and inverse levels of supervision, the framework captures tacit practices, and consistent, yet varied facilitation strategies adopted across specialties, and evident in clinical education settings in both countries. The framework formalizes, for the first time, assumptions and expectations previously unacknowledged. Factors identified as affecting students’ progress toward autonomy include the student/CE relationship, the development of mutual trust through ongoing dialogue, and the importance of formal discussions at the commencement of a clinical placement to establish learning goals, preferred supervision styles and learner responsibilities.
Conclusion
Insights have significance for the CE community, and students who at times have to second-guess what is required of them and how they might excel on clinical placement.
Introduction
Despite the ubiquity and common sense of facilitating physiotherapy students’ autonomy (i.e. independent practice) in physiotherapy clinical education through progressively decreasing levels of supervision, clinical educators’ judgments regarding increasing students’ responsibility in the clinic, and how students conceptualize the progression to greater autonomy, has received scant attention. However, it has been acknowledged that students feel ill-prepared, anxious, and uncertain about working independently at the beginning of their clinical education (Lahteenmaki, Citation2005; Trede, Mischo-Kelling, Gasser, and Pulcini, Citation2015).
Previous research identified taking on responsibilities as an important aspect of experiential learning for undergraduate physiotherapy students, emphasizing the impact of being given or denied responsibility on placement on students’ developing professional capability (Clouder, Citation2009). This research identified how during a clinical placement, opportunity, risk and trust are important factors which students have to negotiate in moving toward autonomous practice. A subsequent study investigating clinical educators’ (CEs) perspectives on the interplay between autonomy, risk, and responsibility identified the ubiquity of risk, and the relationship between trust and trustworthiness. Exploring clinical workplaces as learning spaces, Patton, Higgs, and Smith (Citation2018) identify how supervisors regulate students’ access to activities and relationships and how their innate ability to trust students to be safe and students’ level of confidence determine student engagement with professional practice. In this study, students attributed experiencing different levels of independence to the willingness of supervisors to trust them to be safe with patients rather than their abilities.
These findings pointed to the perceived importance of understanding ‘graduated supervision’ a process by which CEs gradually decrease observation and monitoring of students as their clinical capability and confidence increases (Clouder and Adefila, Citation2017). Similar, and related concepts have been identified. For example, there are parallels with Ten Cate’s (Citation2013) concept of ‘entrustable professional activities’ (EPA) developed for trainee medics. EPAs are tasks given to trainees once they have developed sufficient competence to carry them out that become progressively more difficult or sophisticated (Ten Cate, Citation2013). Pedagogical models also exist outside of health. For example, professional preparation for teacher education continues to be informed by the concept of ‘gradual release of responsibility’ (GRR). Originally introduced by Pearson and Gallagher (Citation1983) in relation to teaching comprehension, GRR developed from a three-stage model: teacher modeling, guided practice and student application and responsibility, to include a fourth stage of collaboration. The GRR model has since been used in a wide variety of contexts to structure learning and development with the gradual handing over of responsibility to the learner. However, Fisher (Citation2008) observed that GRR is not necessarily a linear process and that students can fluctuate between the components as they ‘mastered skills, strategies and standards’ highlighting that moving toward autonomous practice is not straightforward.
How successful release of responsibility in a clinical setting might be achieved, and how strategies can vary depending on CEs’ experience, pedagogical training, philosophy, and different models of supervision (Baldry Currens and Bithell, Citation2003; DeClute and Ladyshewsky, Citation1993; Lekkas et al., Citation2007) provided a stepping off point for the current study. Research in medical education, focusing specifically on the development of trust (Hauer et al., Citation2015) has reinforced findings in physiotherapy clinical education but suggests that supervisors’ trust is based on trainee competence and leadership, or from their own perspective of needing to provide more or less supervision. The supervisors used comparisons with a standard, direct observation of the trainee as a team leader or care provider, and stakeholder input from team members, patients, and families to infer trustworthiness in trainees (Hauer et al., Citation2015). Another study focusing on medical and veterinary clinical teachers’ decision variables and the information used to ground decisions to trust learners, using the structured consensus method of the Nominal Group Technique to generate decision variables, identified a range of skills and qualities falling into five categories: ability, humility, integrity, reliability and adequate exposure (Duijn, Welink, Bok, and Ten Cate, Citation2018).
The influence of the student/CE relationship on the clinical supervisory process also appears to be fundamental for facilitating learning and development (Brown et al., Citation2011; Kilminster, Cottrell, Grant, and Jolly, Citation2007; Laitinen-Vaananen, Talvitie, and Luukka, Citation2007). Effective student/CE relationships have previously been associated with ‘critical companionship’ (Titchen, Citation2001) while Wearne, Dornan, Teunissen, and Skinner (Citation2012) referred to the ‘educational alliance provid[ing] a platform for all other aspects of learning.’ Research across a range of allied health professions suggests students particularly value: good CE feedback skills (Perram et al., Citation2016); upfront discussions (Brown et al., Citation2011); and dynamic two-way exchange (Yeldon et al., Citation2018). Links between pedagogy and the relational nature of learning in practice appear crucial.
Sheu, Kogan, and Hauer's (Citation2017) investigation of the impact of supervisor experience on trust, supervision, and subsequent trainee learning for internal medicine residents suggested that supervisors’ approaches to trust and supervision changes with experience. Whereas less experienced supervisors are rule-based, and determine trust on task completion, drawing on their own experiences to guide supervision, experienced supervisors have greater confidence to determine trust holistically. They check key aspects of patient care selectively and covertly, reflect on individual experiences, and feel comfortable managing clinical problems and gauging trainee abilities. Overall, the research suggests that supervisors need to learn to trust themselves before trusting others. Perhaps this insight hints at the importance of preparatory training. Certainly, CE training is something of a taken-for-granted component of becoming a CE and developing such self-confidence and sensitivity in supervisory decision-making, yet research literature on the impact of training appears to be lacking. Trainees’ perspectives highlight how preferences and learning needs shift over time suggesting the need for CEs to be flexible and adaptive (Sheu, Kogan, and Hauer, Citation2017). Sklar and McMahon (Citation2019) indicated that CEs progressively withdraw their level of supervision as trust in the student develops over time suggesting the need for repeated exposure for trust to be optimally developed.
Our review of related research literature reveals some evidence of useful models akin to graduated supervision but a lack of a specific and explicit pedagogy to support students’ progress toward greater trust and autonomous practice in the clinical setting. These insights into approaches to developing autonomous practice in trainees have been developed mostly from the perspective of supervisors/mentors rather that from a student/mentee perspective, and even fewer put these perspectives together to consider a viable pedagogy. Although graduated supervision, logically hinges on developing mutual trust, which has been shown to impact on student confidence (Clouder and Adefila, Citation2017), there is a gap in understanding of what autonomy looks like, explicit strategies of supervision used to facilitate autonomy, and factors that influence the decision-making process in granting of responsibility that offers an opportunity to enhance autonomy. The aim to build on the existing knowledge base in acknowledging gaps in understanding of graduated supervision sets the scene for the current study which sought to explore the perspectives of both physiotherapy students and CEs in the United Kingdom (UK) and Australia. The research questions were: 1) What are the decision-making criteria and facilitating strategies that CEs use when increasing students’ autonomy on clinical placement; and 2) How do the criteria and strategies used by CEs relate to students’ perceptions of their readiness to accept greater autonomy?
Research context
Our study explored perceptions of students and CEs associated with two physiotherapy programs: a 3-year degree based in the United Kingdom (UK), and a 4-year degree in Australia. The clinical supervision model in the UK was 1:1 (1 clinical educator/1 student). The 1:1 model remains the most common in the UK despite pressure on placement availability although occasionally two CEs may share responsibility for a student. At the time of writing, students rotated through a variety of specialties during the second and third years of the program to expose them to working with a range of clients, in primary and secondary care settings, schools, hospices, and the independent sector. Typical day-to-day activities for the students would include having hands on teaching, assessing and treating patients/clients, contributing to patient/client notes, interprofessional interaction with the wider team and debrief sessions with the CE. Their performance was formally assessed by the CE in collaboration with a university visiting tutor. By the third year of their program, they would be expected to have developed sufficiently to settle into a new placement relatively quickly and to take responsibility for a small caseload in consultation with their CE.
In the Australian program, participants were sought from clinical placements which had a dedicated clinical educator provided by the University with a 4:1 ratio of students to educators in year 3, and 5:1 in year 4. Students typically would manage the assessment, treatment, and case notes of their patients/clients with support and feedback from their educator as well undertake interprofessional interaction with the wider team as appropriate. Students in their fourth year are expected to manage a higher caseload and practice more autonomously than students undertaking third-year placements. Students and educators were drawn from clinical placements in hospital, rehabilitation, and ambulatory care settings. Students' performance was assessed mostly commonly by two CEs who shared the supervision over a week. The CEs in the Australian program did not carry a clinical load while supervising students, while those in the UK maintained their own clinical caseload.
Clinical education training was in place in both countries. In the UK, new educators complete basic training during a one-day course and then advanced training on an annual basis. Basic training covers the structure of the program, expectations of CEs and students, objective setting and an in-depth introduction to assessment processes. Advanced training has varied to include updates as well as scenario-based learning focusing on issues including, making reasonable adjustments for inclusion of disabled students, and developing reflective practice capabilities. In Australia, new educators complete a one-day or half-day training session which included training in the use of the national assessment tool (i.e. Assessment of Physiotherapy Practice), expectations of CEs and students, and providing feedback. In both countries, training was supplemented by a clinical educators’ handbook and a clinical educators’ resources webpage.
Methodology
Research design
An exploratory qualitative research approach, using in-depth interviews, was adopted as a means of exploring physiotherapy CEs’ and students’ respective perceptions regarding the progression of student autonomy on clinical placement. This approach was deemed suitable since as Reiter (Citation2017) suggested exploratory research involves a process of “making sense” of a phenomenon which is ‘gradual and characterized by reformulating and adapting explanations, theories, and initial hypotheses inductively.’ As qualitative research also does not usually claim to achieve generalizability or prediction, the small sample size and particularity of contexts in this study can only lead to uncovering practices that might prove transferrable if others can see the relevance and applicability to their personal circumstances (Tight, Citation2017). A cross-sectional study design was used in order to explore the differences and similarities (Hall, Citation2008) among pairs, or dyads, of physiotherapy students and their CEs. As well as providing a means of assessing how practices take place in existing settings without the need for interventional design (Barratt, Kirwan, and Shantikumar, Citation2018), cross-sectional designs also provide an opportunity to examine a range of factors, which in this case have been described as complex decision-making processes and variables linked to increased autonomy (Clouder and Adefila, Citation2017), particularly interrogating the relationships between the variables (Patton, Citation2015). Semi-structured interview schedules, revised from an earlier study, guided one-to-one, CE and student, interviews. Broadly, CE interview questions focused on judgments for granting greater responsibility, explicit strategies for facilitating greater autonomy and factors impacting on the granting of responsibility. Students’ interview questions focussed on whether explicit measures were in place regarding learning goals and expectations and strategies for achieving goals and progressing autonomy, CE support toward learning and greater autonomy, and the basis of students’ perceptions of readiness for increased autonomy. The interviews of between 20 and 60 minutes duration were conducted at the end of placement, primarily in the placement setting, were audio-taped and transcribed verbatim. All four interviewers were independent of interviewees and experienced at conducting interviews. Three were physiotherapists in academia and the fourth was a research assistant. All were female. Ethical approval was obtained at each institution. Written informed consent was obtained from all participants prior to interviews commencing.
Participants
Purposive sampling, consistent with a qualitative approach not aimed at claims of generalizability, involves identifying and selecting individuals that are knowledgeable about or experienced with a phenomenon of interest whose perspectives inform the research questions (Cresswell and Plano Clark, Citation2011). In this research, purposive sampling meant seeking to recruit students nearing the end of their programs who had potentially begun to operate with greater autonomy, paired with their CEs experienced in supervising pre-registration students. In the UK, students were briefed about the study in a lecture prior to a placement block and CEs were notified during an annual update workshop. Students volunteering to be involved secured involvement of their CEs in the UK. In Australia, e-mail invitations were sent to clinical educators and matched students asking for volunteers to take part in the study. The use of matched pairs of students and CEs offered the opportunity to explore discrepancies in perceptions of events and experiences, which sampling independent groups of students and CEs would not have provided. The clinical settings for placement experiences included seven National Health Service Trust sites in the UK Midlands and three university-linked sites in an Australian city. Specialties included in the UK were neurology, musculoskeletal, pediatrics, outpatients and inpatients and in Australia specialties were the same except for the inclusion of cardiorespiratory and the exclusion of pediatrics. Seven pairs of CEs and students participated in the UK, and five CEs and eight students supervised by these CEs took part in Australia (). CE participants were predominantly female but both years of experience as a clinician and as a CE were wide ranging.
Table 1. Profile of participants.
Data analysis
The UK and Australian team members were in regular contact via videoconferencing and e-mail. Data saturation, the stage at which no new insights or themes are observed in the data (Saunders et al., Citation2018) was reached after a total of 27 interviews. All interviews were transcribed producing a total of 308 pages of transcription with a mean length of 11.4 pages. A staged process informed an inductive thematic analysis of interview data (Braun and Clarke, Citation2006). The process was data driven in that it involved coding the data without trying to fit it into a preexisting coding frame. This process included six stages: 1) reading and re-reading transcripts and noting initial ideas; 2) generating initial codes; 3) searching for themes; 4) reviewing themes; 5) naming themes and defining specifics; and 6) reporting, including selecting extracts aligned to the research questions. Initially, the Australian and UK researchers coded their respective transcripts independently on the first reading of their raw data. Raw data and the codes were shared across the team. These were read prior to examining the initial codes together as a larger team where variations were considered with the aim of developing overall agreement. Codes were both semantic based on spoken word or latent representing underlying ideas, assumptions, and conceptualizations (Braun and Clarke, Citation2006). Although pre-defined questions shaped the interview schedules, themes emerged during the reflexive and iterative process of viewing and grouping codes ensuring credibility and confirmability (Braun and Clarke, Citation2006). Reviewing their initial work on thematic analysis, Braun and Clarke (Citation2019) noted that conceptualizations of a theme differ and that often themes are simply ‘domain summaries’ generated from data collection questions, which are presented as themes without any real analysis at a deeper level. These they consider to ‘constitute under-developed themes’ (Braun and Clarke, Citation2019). In contrast and in agreement with their approach we sought to go beyond summarizing the data to look for patterns of ‘shared meaning.’ This is a creative and interpretive process of refining themes which they see as ‘produced at the intersection of the researcher’s theoretical assumptions, their analytic resources and skill, and the data themselves’ (Braun and Clarke, Citation2019).
Findings
The research findings are presented under themes that relate to the research questions. Together they build a picture from both student and CE perspectives to understand how graduated supervision works.
Judging readiness for autonomy
How CEs and students conceptualize autonomy and the necessary capabilities that underpin it influences judgments of readiness for increased exposure and perceptions of preparedness, respectively. illustrates areas of specific shared perceptions and areas that students under-estimate in terms of importance. While students had a broad conception of readiness and identified affective associations, such as feeling more confident, less stressed, and less constrained to try things out with movement toward autonomy, CEs understandably, focused very much on instrumental and tangible signs of readiness, such as students’ self-awareness of their own abilities, taking initiative, and positive response to feedback.
Table 2. Matches and mismatches in CEs’ and students’ conceptions of criteria used to judge students’ readiness to act autonomously on clinical placement.
University protocols (e.g. professional behavior, and safety) inevitably influenced CEs’ considerations regarding levels of autonomy, as did clinical education models. In the Australian context, CEs responsible for several students found that numbers and variability in students’ competence could make judging readiness to take on responsibility difficult due to limited time for individual student observations and one-to-one discussions:
Our ratio is 5 to 1, and so that gets pretty busy sometimes, especially when you’ve got 4 of them lining up and you’re talking to one of them to go through clinical reasoning, because you feel pushed, because you need to get them back to the patient otherwise the patient’s sitting there, sometimes for an hour and a half they’re there for, which is a very long time … we try and stagger the diary but it never happens, you know they all walk out at the same time, it just always happens (AUSCE1).
Not wanting to keep patients waiting also applied in the UK where working around other health professionals’ schedules, service standards, and busy caseloads were apparent. A CE explained:
There’s the regulation that every patient has to be seen five times a week for 45 minutes a session so you’ve got standards … We’ve got a lot of stats and targets to meet as well so it’s making sure that that’s all done (UKCE6).
As has been identified previously, responsibility/autonomy given was generally based on students’ readiness, rather than stage of course, illustrating how CEs’ decision-making was based on weighting each individual’s capabilities, rather than assuming blanket progress.
You could have a second-year student who’s really good and you could have a third-year student who’s not as good … it’s not a case of they’re a third-year so we give them work because we expect them to be better (UKCE5).
However, another CE reflected how:
‘It’s very hard at the beginning to judge a student’s [progress]’ (UKCE2).
Probing for understanding was very much part of one CEs approach:
I questioned her …, why did you ask that question, what were you thinking, what were your findings … what were you trying to differentiate there? She understood what I was asking her (UKCE7).
Others discussed a variety of strategies to assess students’ capability:
Quite early on I’ll give them a lot of things to do repetitively. Going and taking down a subjective history from the medical notes or going and starting a social history from the patient. And just start increasing those little things (UKCE6).
It’s quite a gradual process … but probably starts off with giving them small opportunities to do things on placement supervised and then if they do that well, you let them do something independently that you know is quite safe, because safety is probably one of the big things that you want. So then I usually give them opportunity to try something on their own and then depending how that goes, you get that bit of trust that you go to the next step (AUSCE3).
Observations of students’ practice played a significant role in providing the insight that CEs needed to judge a student’s ability, especially during the earlier stages of a clinical placement. However, discussion with the student provided crucial access to thinking and reasoning processes. As one CE stated:
If those kinds of things were vocalized then that gives me a better understanding of her thought processes … then to be able to know that I can leave her to do those things and become more autonomous and take on more responsibility (UKPT6).
Typically, discussions focused on information gathered, interpretations/synthesis, planning, management options, and rationale for choices (as key sections of patient assessment and management). A student reflected:
By going through cases with [CE] and showing her that we could reason through it by ourselves, she was putting less and less input in as the time went on. I think just showing her, like verbally talking to her through a case and saying what we were going to do, gave her the confidence that we weren’t going to sort of do anything that was going to harm the patient, and also reading through their notes and reporting to her what the important things were. She would read the notes before we would and then give her a handover and she would sort of have an idea, just making sure we don’t miss anything (AUSST4).
Further insight was gained by CEs asking colleagues for their feedback, reading students’ notes, completed reflections and reasoning forms, whereas direct assessment of practical ability might be tested by having the student practice a technique on the CE. Students appreciated this input:
Practice and getting feedback and saying yeah I’ve had a go with that or yes I’ve had someone sort of check up on me or give me feedback (AUSST7).
The 4:1 ratio of students to CEs operating in Australia meant that students could more readily benefit from peer support and learning, and CEs were able to target students most in need of support:
With my first students a couple of them I’ve seen during pre-clinical and I knew that they were very good. So I did not concentrate on them too much. I concentrated on the other two who I knew were a little bit weaker (AUSCE2).
Strategies that foster progress
Both students and CEs were able to identify strategies that contributed toward students’ progress in terms of taking on greater levels of responsibility. CEs who were approachable and encouraged contact and tailored supervision to individual students’ needs, inviting students’ input into when and how feedback is given, were deemed highly influential. One CE related:
I’ve got one student who is very academic … from overseas, so language was the big issue. Her knowledge was probably better than mine, to some extent, because she could just absorb it. But her language skills … And that was where we really had to work (UKPT3).
In setting the scene for the placement, a pre-placement discussion and agreement of learning goals, to establish learner responsibilities, were deemed very important, as was the selection of appropriate patients with a gradual increase in complexity. Collaborative planning around relative responsibilities and preferred teaching and learning styles, with checks in place to monitor effectiveness and satisfaction, were crucial:
With complicated patients I tend to lose confidence … so he gave me very easy conditions – very easy patients … very straight forward and then during the third week he started to just give me just a bit harder … when he saw me a bit struggling and start to lose confidence he would jump in and help me. Otherwise he just left me to do everything – because I think this is the best way when you try to do stuff and you’re like doing everything by yourself and you don’t need any help and giving more confidence (AUSST8).
When preparation and monitoring were less formal, students failed to recognize their importance thus compromising their chances of improvement. CEs were often able to direct students to additional learning resources but finding opportunities to practice/test skills depended on both CEs and students identifying appropriate opportunities and capitalizing on them. Reflecting the comment made by the student above, CEs reported closer monitoring of weaker students, generally spending more time with them but as a consequence giving them less scope to develop autonomy:
[If] their handling skills weren’t good or they were putting a patient at risk, then obviously that’s something that we address and work on more … they would have less responsibility as opposed to somebody who was really, really good (UKCE5).
One of the most important strategies that prompted a range of views, was that of CE feedback. Despite students being unanimous in wanting and valuing feedback, and CEs recognizing its importance, opinions differed on its timing and the helpfulness of observation, interruption, and assistance. While one student suggested that ‘not always being watched was a good thing, (AUSST4) another reflected:
One CE’s way of support was better for me [and] how I learn; she would jump in which I liked … I would rather be corrected on the spot with the patient; Other CEs tended to stand back and give feedback later – I felt I was wasting the patient’s time (AUSST5).
However, differences in levels of autonomy afforded and reactions to being watched and interrupted depended in part on the practice context. This was evident in the distinction between teaching/feedback and autonomy in low-risk versus high-risk settings, such as an Intensive Care Unit or in the case of an acute musculoskeletal problem, where both CEs and students recognized the need, often linked to safety, for closer supervision. One student recognized the importance of knowing their limitations and implications:
Because it’s the educator that is liable for us and they oversee everything we do and I think if they give a student a task to do and it’s done unsafely, for example, then it falls back onto the educator. So there is always that extra caution that you get, but again, I think that can be avoided by having an open relationship. If the student doesn’t feel confident they should say and seek help rather than going in head strong (UKST1).
Attitudes to feedback impacting on the scope of progress were undoubtedly influenced by factors such as the student’s personality, self-awareness and confidence, knowledge and reasoning, and communication and procedural skills. As one student reflects:
I was that cautious person who was quite quiet, but I think I’ve learnt as well that you have to go out and seek these things, you have to seek the opportunities in order to get more experience (UKST1).
The importance of the relational context
Students identified how relationship building in a relatively short timescale was challenging and this was compounded by encountering highly varied working practices that inevitably impacted on progress. This was highlighted by a student who was able to compare returning to a setting with which s/he was familiar:
In this [placement] - I knew how it worked so I could come in and say right I’ll do this and this. But on other placements it’s been difficult because it’s a completely different way of working (UKST3).
The impact of the student/CE relationship was identified as a theme that seemed to underpin the previous themes in that the strategies and criteria used by CEs to inform judgments about students’ readiness for increased autonomy are bound up in the mutually reinforcing actions and responses from students and CEs, that cement working relationships.
Findings confirm prior knowledge that a student/CE relationship based on mutual trust is fundamental to student progression toward autonomous practice. Trust and trustworthiness are developed in tandem as a two-way process that is delicate and highly relational but clearly dependent on key indicators of readiness. One student reflected:
[The relationship] is very important because if they’re supportive … you’re more willing to try different things and you’re not so afraid of failing. Understand[ing] that you’re a student … and not expecting you to be perfect on day one. I think that’s really important, and to be able to communicate (AUSST5).
Another student recognized:
I think trust goes both ways. If they’ve got trust in you … you feel a lot more confident that you actually can do it (AUSST4).
The antithesis was confirmed by another student:
I didn’t feel that I had a very open relationship with her, I didn’t feel that I could make mistakes and talk about them (UKST1).
The importance of trusting positive support, good communication and students’ being able to negotiate opportunities to excel was also acknowledged by CEs:
To have a relationship where they feel that they can talk to you and that they trust you. Being able to talk to me is really important for my understanding of where they’re at (UKCE6).
Confidence was cumulative and boosted by a CE’s belief in the student’s capacity to successfully execute tasks; feeling that they were ‘believed in’ empowered students to be less fearful to try different approaches:
It gives you the confidence to know that your educator trusts you and then you’ve got the confidence to say I can do it without any sort of – they just believe that you can do it so it gives you the feeling that you can do it. You’re always nervous the first time you get given a completely new things to do (AUSST6).
Discussion
The aim of the current research was to investigate the decision-making criteria and facilitating strategies that CEs use when increasing students’ autonomy on clinical placement and to discover to what extent they relate to students’ perceptions of their readiness to accept greater autonomy in an attempt to understand the concept of graduated supervision. In fact, we identified a concerning mismatch between CEs’ and students’ conceptions of criteria used to judge students’ readiness to act autonomously on clinical placement. This puts students at a clear disadvantage in terms of their learning and placement outcomes, and possibly explains why students feel ill-prepared, anxious, and uncertain about working independently (Lahteenmaki, Citation2005; Trede, Mischo-Kelling, Gasser, and Pulcini, Citation2015). Yet, our findings suggest that such a mismatch in understanding might be readily addressed through guidance during pre-clinical discussions focused on ensuring that CE’s decision-making criteria and strategies they will employ to facilitate increased autonomy are explicit and transparent to students, and that there are ongoing discussions and negotiations on optimizing the effectiveness of learning experiences.
To date, the practical aspects of decision-making have been implicit, and the decision-making criteria largely tacit, resulting in a lack of a formal pedagogy to offer new CEs or students to guide clinical education. Findings are synthesized to form a framework of decision-making criteria that brings CEs’ tacit knowledge into view for the first time. Theoretically, the contribution made by the study () is to define and illustrate the concept of graduated supervision as the measured exposure to tasks of increasing complexity and corresponding inverse levels of need of supervision resulting in a pedagogy of ‘placement learning and responsible practice.’ The underpinning conception of gradually shifting responsibility from teacher to learner has synergies with the concept of GRR (Fisher, Citation2008; Pearson and Gallagher, Citation1983).
Figure 1. A framework to illustrate decision-making, task exposure and graduated supervision.
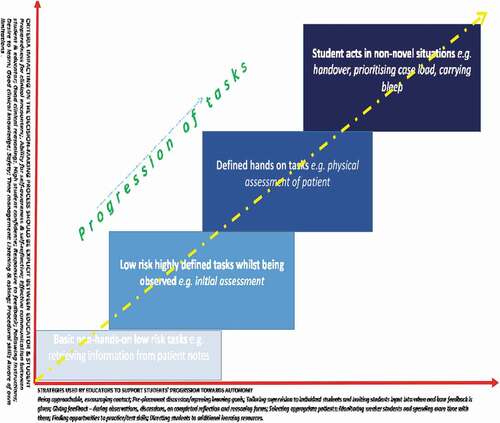
illustrates the interaction between elements that demonstrates how CEs progressively expose students to more complex tasks that extend their capabilities. The tasks might be similar to those identified as EPA tasks given to trainees once they have developed sufficient competence to carry them out that become progressively more difficult or sophisticated (Ten Cate, Citation2013). However, the study adds to existing knowledge (Clouder, Citation2009; Clouder and Adefila, Citation2017) by elucidating combined CE and student perspectives to reveal not only where mismatches in expectations exist but also how mutual trust develops. CEs must establish in the first few days of the placement whether a student ‘does exactly as asked’ as an early indicator of trustworthiness. At each stage in this stepped process, the CE judges competence, confidence, and trustworthiness. Initially, CEs might allow students to observe a new assessment, ask questions of the CE and make their own observations/interpretations of the encounter demonstrating knowledge, inquisitiveness, and ability to ascertain and interpret key information. The routine of brief and debrief, in the form of reporting back to the CE, as well as continual dialogue previously advocated (Brown et al., Citation2011; Yeldon et al., Citation2018) was crucial at every stage of the process evident in our findings. Observation by the CE might be initially at close quarters, then at a distance and eventually through others as workload increases in terms of numbers and patient complexity, reinforcing insights developed by Hauer et al. (Citation2015).
The principle of progressive exposure to increasing levels of autonomy in the context of practice complexity offers a pedagogy to promote student autonomy on placement. CE decision-making draws on a series of ‘tests,’ ranging from basic non-hands on tasks to operating with increased personal autonomy in non-novel situations. The framework illustrates how CEs act as gatekeepers, regulators, brokers and ‘critical companions’ (Patton, Higgs, and Smith, Citation2018; Titchen, Citation2001) as progression is reliant on the students’ demonstrating competence, capability and reliability (Duijn, Welink, Bok, and Ten Cate, Citation2018), which invoke CEs trust and inform judgment of students’ readiness to progress. Success is fostered through feedback and explicit discussions to establish learning goals, supervision style and learner responsibilities followed by skilled facilitation within a supportive yet critical mentoring relationship (Brown et al., Citation2011; Titchen, Citation2001; Yeldon et al., Citation2018). As such, this study complements Patton, Higgs, and Smith (Citation2018) study that identified ‘workplace influences, engagement with professional practice, clinical educators’ intentions and actions and students’ dispositions and experiences’ as multiple influences on students’ clinical learning.
The current study did not seek to establish specific connections between training and supervisory practices, although training did cover content such as giving feedback that is likely to have influenced CE/student interaction. This would be a rich area for further research. Neither did the study set out to focus on comparing the models of supervision per se and the implications of a dedicated CE working with multiple students as opposed to a CE responsible for a single student who also maintained a clinical workload. However, notwithstanding these differences, CE’s decision-making criteria for increasing students’ responsibility, their strategies for facilitating autonomy, and students’ perceptions regarding readiness for greater autonomy were similar between the two models. While differences such as competing work demands versus the challenges of supervising multiple students would be expected to impact on supervision logistics, it did not appear to affect the common experiences uncovered in the two groups of CE’s and students. Successful clinical education occurs in both models possibly for different reasons. A direct comparison of the models in one setting would enable benefits or limitations of these clinical education models to be more explicitly explored. Despite variability in context and supervisory arrangements, and temporary glitches while settling into new placements and establishing credibility, the students in the current study reported gaining in confidence, especially in areas such as performing in front of their CEs, dealing with complex patients and taking on leadership roles, through gradual exposure to greater challenges and increased responsibility. This highlights the importance of the underpinning relational aspects of practice and the effects on students’ learning that is emphasized by those students who experienced relational difficulties that they perceived hindered their progress toward autonomy. In addition, findings suggest that despite the progressive set of tasks varying according to specialty, the basic framework holds across areas of practice, and between Australia and the UK. As such the framework provides a pedagogical approach of significance for students and CEs previously tacit, and not formally recognized or documented.
Research quality
Grbich (Citation2010) suggested that trustworthy research is based on congruence between the research paradigm chosen to frame the research, the research aim and questions, and the research design. This study has aimed to achieve this alignment. Furthermore, Guba and Lincoln's (Citation1989) constituents of trustworthiness (i.e credibility, confirmability, dependability, and transferability) can be demonstrated. Credibility can be claimed due to the researchers’ experience of, and immersion in, the field, the use of the dyads to incorporate student and CE perspectives as ‘expert’ participants focusing on the same concept, and a rich data set that the researchers were confident had reached saturation (Morse, Citation2015). The use of dyads and cross referencing of perspectives also supports confirmability alongside an audit trail that was used to track codes and the development of shared meaning in the production of themes. The inquiry audit also ensures dependability. We aimed to achieve transferability by the faithful representation of participant perspectives with which CEs and students might identify and translate into their own contexts.
Study strengths and limitations
The focus on practices associated with placement experiences in two physiotherapy programs, at opposite sides of the world and within very different health and educational contexts limits the generalizability of findings. However, this was not the objective and they are likely to resonate with students and CEs nationally and internationally. Potential for transferability (Tight, Citation2017) is noted in the convergence of practical strategies, decision-making criteria and concepts across the two programs, despite different clinical education models, varied settings for practice, and year levels of the students. Nevertheless, although findings appeared to be similar this may simply be coincidental. It is the nature of qualitative research to present insight that then might be used to generate discussion and further research in other contexts and possibly at scale.
Conclusion
This paper has proposed a formalized pedagogy of previously taken-for-granted strategies and clinical decision-making criteria to promote student autonomy on placement that emerged from addressing the first research question. As a heuristic device the pedagogy of placement learning and responsible practice assesses readiness to progress autonomous practice by capturing tacit practices adopted across specialties, and evident in clinical education settings in both Australia and the United Kingdom. In response to the second research question, the research has uncovered a discrepancy between how CEs and students understand autonomy and the use of the strategies, such as feedback, and criteria such as responsiveness to feedback, at play that together inform CE decision-making processes. We suggest that this discrepancy may be due to the ubiquitous yet implicit nature of the teaching and learning processes that occur on placement. The pedagogy makes the gradual transfer of responsibility to students more explicit than we found it to be in the situations studied and provides a blueprint for accelerating students’ progress toward becoming confident autonomous practitioners by formalizing some of the assumptions and expectations previously unacknowledged. Factors that have been identified as affecting progress through graduated supervision, include the student/clinical educator relationship, the development of mutual trust through ongoing dialogue, and the importance of formal discussions at the commencement of a clinical placement that establishes expectations, aspirations, and responsibilities of students and their CEs right from the start. As such, the study contributes to the evidence-base and understanding of the factors that impact on the effectiveness of the clinical education of physiotherapy students.
Disclosure statement
The authors report no conflict of interest.
References
- Baldry Currens J, Bithell CP 2003 The 2:1 clinical placement model: Perceptions of clinical educators and students. Physiotherapy 89: 204–218. doi:10.1016/S0031-9406(05)60152-6.
- Barratt H, Kirwan M, Shantikumar S 2018 Design, applications, strengths and weaknesses of cross-sectional, analytical studies (including cohort, case-control and nested case-control studies), and intervention studies. Health knowledge, Department of Health Public Action Support Team (PHAST) https://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a-epidemiology/cs-as-is.
- Braun V, Clarke V 2006 Using thematic analysis in psychology. Qualitative Research in Psychology 3(2): 77–101. doi:10.1191/1478088706qp063oa.
- Braun V, Clarke V 2019 Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health 11(4): 589–597. doi:10.1080/2159676X.2019.1628806.
- Brown T, Williams B, McKenna L, Palermo C, McCall L, Roller L, Hewitt L, Molloy L, Baird M, Aldabah L 2011 Practice education learning environments: The mismatch between perceived and preferred expectations of undergraduate health science students. Nurse Education Today 31(8): 22–28. doi:10.1016/j.nedt.2010.11.013.
- Clouder DL 2009 “Being responsible”: Students’ perspectives on trust, risk and work-based learning. Teaching in Higher Education 14: 289–301. doi:10.1080/13562510902898858.
- Clouder DL, Adefila A 2017 Empowerment of physiotherapy students on placement: The interplay between autonomy, risk and responsibility. Physiotherapy Theory and Practice 33(11): 859–868. doi:10.1080/09593985.2017.1357153.
- Cresswell JW, Plano Clark VL 2011 Designing and conducting mixed method research (2nd ed), Thousand Oaks, CA: Sage.
- DeClute J, Ladyshewsky RK 1993 Enhancing clinical competence using a collaborative clinical education model. Physical Therapy 73(10): 683–697. doi:10.1093/ptj/73.10.683.
- Duijn CC, Welink LS, Bok HG, Ten Cate O 2018 When to trust our learners? Clinical teachers’ perceptions of decision variables in the entrustment process. Perspectives on Medical Education 7(3): 192–199. doi:10.1007/s40037-018-0430-0.
- Fisher D 2008 Effective use of the gradual release of responsibility model, p. 2. New York: Macmillan/McGraw-Hill.
- Grbich C 2010 Interpreting quality in interpretive research. In: Higgs J, Cherry N, Macklin R, Ajjawi R (Eds) Researching practice: A discourse on interpretive methodologies, pp. 153–163. Rotterdam: Sense.
- Guba EG, Lincoln YS 1989 Fourth generation evaluation. London: Sage.
- Hall J 2008 Cross-sectional survey design. In: Lavrakas PJ (Ed) Encyclopedia of survey research methods, pp. 173–174. Thousand Oaks, CA: Sage.
- Hauer KE, Oza SK, Kogan JR, Stankiewicz CA, Stenfors-Hayes T, Ten Cate O, Batt J, O’Sullivan P 2015 How clinical supervisors develop trust in their trainees: A qualitative study. Medical Education 49(8): 783–795. doi:10.1111/medu.12745.
- Kilminster S, Cottrell D, Grant J, Jolly B 2007 AMEE guide no. 27: Effective educational and clinical supervision. Medical Teacher 29(1): 2–19. doi:10.1080/01421590701210907.
- Lahteenmaki M-L 2005 Reflectivity in supervised practice: Conventional and transformative approaches to physiotherapy. Learning in Health and Social Care 4(1): 18–28. doi:10.1111/j.1473-6861.2005.00080.x.
- Laitinen-Vaananen S, Talvitie U, Luukka M-R 2007 Clinical supervision as an interaction between the clinical educator and the student. Physiotherapy Theory and Practice 23(2): 95–103. doi:10.1080/09593980701212018.
- Lekkas P, Larsen T, Kumar S, Grimmer K, Nyland L, Chipchase L, Jull G, Buttrum P, Carr L, Finch J 2007 No model of clinical education for physiotherapy students is superior to another: A systematic review. Australian Journal of Physiotherapy 53(1): 19–28. doi:10.1016/S0004-9514(07)70058-2.
- Morse JM 2015 Critical analysis of strategies for determining rigor in qualitative inquiry. Qualitative Health Research 25(9): 1212–1222. doi:10.1177/1049732315588501.
- Patton MQ 2015 Qualitative research & evaluation methods: Integrating theory and practice. 4th ed. London: Sage.
- Patton N, Higgs J, Smith M 2018 Clinical learning spaces: Crucibles for practice development in physiotherapy clinical education. Physiotherapy Theory and Practice 34(8): 589–599. doi:10.1080/09593985.2017.1423144.
- Pearson PD, Gallagher MC 1983 The instruction of reading comprehension. Contemporary Educational Psychology 8(3): 317–344. doi:10.1016/0361-476X(83)90019-X.
- Perram A, Hills C, MacDonald-Wicks L, Johnston C, James D, Warren-Forward H 2016 Characteristics of an ideal practice educator: Perspectives from undergraduate students in diagnostic radiography, nuclear medicine, nutrition and dietetics, occupational therapy, physiotherapy and radiation therapy radiography. Radiography 22(4): 295–305. doi:10.1016/j.radi.2016.04.007.
- Reiter B 2017 Theory and methodology of exploratory social science research. International Journal of Science and Research Methodology 5: 129–150.
- Saunders B, Sim J, Kingstone T, Baker S, Waterfield J, Bartlam B, Burroughs H, Jinks C 2018 Saturation in qualitative research: Exploring its conceptualization and operationalization. Quality and Quantity 52(4): 1893–1907. doi:10.1007/s11135-017-0574-8.
- Sheu LE, Kogan JR, Hauer KE 2017 How supervisor experience influences trust, supervision, and trainee learning. Academic Medicine 92(9): 1320–1327. doi:10.1097/ACM.0000000000001560.
- Sklar DP, McMahon GT 2019 Trust between teachers and learners. JAMA 321(22): 2157–2158. doi:10.1001/jama.2018.22130.
- Ten Cate O 2013 Nuts and bolts of entrustable professional activities. Journal of Graduate Medical Education 5(1): 157–158. doi:10.4300/JGME-D-12-00380.1.
- Tight M 2017 Understanding case study research: Small-scale research with meaning. London: Sage.
- Titchen A 2001 Critical companionship: A conceptual framework for developing expertise. In: Higgs J, Titchen A (Eds) Practice, knowledge and expertise in the health professions, pp. 80–90. Oxford: Butterworth Heinemann.
- Trede F, Mischo-Kelling M, Gasser EM, Pulcini S 2015 Assessment experiences in the workplace: A comparative study between clinical educators’ and their students’ perceptions. Assessment and Evaluation in Higher Education 40(7): 1002–1016. doi:10.1080/02602938.2014.960363.
- Wearne S, Dornan T, Teunissen PW, Skinner T 2012 General practitioners as supervisors in postgraduate clinical education: An integrative review. Medical Education 46(12): 1161–1173. doi:10.1111/j.1365-2923.2012.04348.x.
- Yeldon J, Wilson R, Laferriere J, Arseneau G, Gu S, Hall M, Norman KE, Yoshida K, Mori B 2018 Let’s talk about the talk: Exploring the experience of discussing student performance at the mid- and final points of the clinical internship. Physiotherapy Canada 70(3): 240–248. doi:10.3138/ptc.2016-96.