
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Studies investigating the efficacy of errorless learning (EL), a rehabilitation method in which the occurrence of errors during learning are eliminated, have predominantly involved patients with memory impairment. However, the most recent perspective on the underlying mechanism of EL explicitly takes executive processes into account. The aim of this study was to investigate whether EL of object locations is beneficial for memory performance compared to trial-and-error learning (TEL) in patients with acquired brain injury (ABI) experiencing executive deficits (N = 15) and matched healthy controls (N = 15). Participants completed an EL and TEL condition of a computerized spatial learning task, in which the location of everyday objects had to be memorized. The number of errors made during learning was predetermined, varying from 0 (EL condition) to 1, 2, 3, 4 or 5 errors (TEL condition). Results showed a beneficial effect of EL on memory performance in both ABI patients and controls (p < .001), but this advantage was not larger in ABI patients compared to controls and was not moderated by the amount of errors made during learning.
Introduction
Acquired brain injury (ABI), injury to the brain due to either a traumatic or a non-traumatic aetiology, is often accompanied by cognitive deficits in attention, speed of processing, memory and executive functioning (Sun et al., Citation2014). Such deficits are associated with less vocational and community involvement (Ponsford et al., Citation2014; Watson et al., Citation2020), and poorer quality of life (Dijkers, Citation2004). Although cognitive rehabilitation includes a wide range of evidence-based interventions to compensate for impaired cognitive deficits and to improve quality of life (Cicerone et al., Citation2000, Citation2019), approximately 40% of patients with ABI still require support in post-injury daily life (Ponsford et al., Citation2014).
One rehabilitation principle that can be applied to specifically train everyday activities is errorless learning (EL). In this approach, the occurrence of errors during learning is eliminated or reduced in order to minimize the competition between correct and erroneous responses during later recall (Baddeley & Wilson, Citation1994). In this regard, EL differs fundamentally from trial-and-error learning (TEL), in which the interference of errors during learning is not prevented. Based on the EL literature in adults with ABI, Evans (Citation2018) concluded that the findings concerning the superiority of EL over TEL are mixed in this patient population. Some studies have found beneficial effects of EL of word lists on later recall relative to TEL (e.g., Baddeley & Wilson, Citation1994; Page et al., Citation2006; Ueno et al., Citation2009). However, when using more ecologically relevant tasks, the beneficial effects of EL have not been established so clearly and consistently (e.g., Haslam et al., Citation2011; Lloyd et al., Citation2009). A possible contributing factor to the mixed pattern of findings is that the cognitive mechanisms underlying EL and TEL learning, respectively, are still unclear (Bertens & Brazil, Citation2018).
Most studies so far have predominantly investigated the beneficial effect of EL in patients with memory impairments. With respect to the sources of this beneficial effect, Baddeley and Wilson (Citation1994) proposed that amnesic individuals rely more heavily on their relatively intact implicit memory, which is unable to support conscious processing of errors that may occur during learning. When errors occur during learning in these patients, both correct and incorrect memory traces may be consolidated via implicit memory to a similar extent, making it difficult to distinguish between them during retrieval. Hunkin et al. (Citation1998) proposed another mechanism and stated that the EL advantage observed in amnesic patients may be facilitated through “residual explicit memory”, as they found no relationships between other measures of implicit learning and the benefit of EL.
A more recent perspective on the underlying mechanisms of EL and TEL highlights a potential role for executive function, as error correction requires executive control, such as the ability to detect and monitor errors and to adjust behaviour based on feedback (Bertens & Brazil, Citation2018; Clare & Jones, Citation2008). Moreover, Broadway et al. (Citation2019) suggested that executive functions may mediate memory performance in patients with mild traumatic brain injury as they make less use of compensation strategies. EL and TEL have been investigated extensively in ABI (see Evans, Citation2018, for an overview). However, only a few studies have systematically examined the effects of EL on memory performance in executively impaired patients with ABI (e.g., Baddeley & Wilson, Citation1994; Cohen et al., Citation2010; Fish et al., Citation2007), explicitly taking performance differences in executive functioning across individuals into account.
The purpose of the present study was to examine whether EL contributes to better learning performance than TEL in ABI patients with executive deficits compared to matched controls using a novel paradigm, the Drawer task (Scheper et al., Citation2019, Citation2021). In this paradigm, the frequency of errors made during the acquisition phase can be manipulated (i.e., 0 incorrect responses in the EL condition or 1, 2, 3, 4, or 5 incorrect responses in the TEL condition). In previous studies, we showed a beneficial effect of EL in healthy young and older adults with intact memory and error-monitoring processing, but the number of errors made during the acquisition phase of TEL did not affect the later recall performance (Scheper et al., Citation2019, Citation2021). However, Clare and Jones (Citation2008) concluded that the effect of error frequency on memory performance may be more profound in patients with cognitive impairments, such as ABI patients. We hypothesized that ABI patients would perform worse than healthy controls on the Drawer task in general, and also expected better performance following EL compared to TEL across groups. Since introducing more errors will put a larger burden on the already vulnerable cognitive control system in the ABI group, we also hypothesized that a larger amount of incorrect responses made during learning would result in worse memory performance in patients with ABI, but not in the control group. Finally, we sought to gain a better understanding of the mechanisms subserving EL by exploring the relationship between memory and executive functions in EL and TEL.
Methods
Participants
Power calculations for the primary analyses of comparing the performances after EL and TEL, assuming a medium effect size (r = 0.30), a power of (1-β) = 0.85 and a presumed correlation among repeated measurements of 0.50, indicated that a minimum sample size of 14 per group was needed. In this study, we used a mixed design and recruited 15 healthy participants and 15 patients with non-progressive ABI, mainly stroke and traumatic brain injury, who experienced executive deficits as quantified with a neuropsychological assessment. The exclusion criteria included inability to speak or understand Dutch, having a neurodegenerative disorder, severe premorbid psychiatric problem (unrelated to the ABI), substance abuse, and severe cognitive comorbidity (such as having an amnesic syndrome, neglect, or aphasia). The ABI patients were assessed at least three months following their injury. Recruitment of the patients took place at the Rehabilitation Medical Centre Klimmendaal in Arnhem, and the outpatient clinic of the department of Neurorehabilitation of the Sint Maartenskliniek in Nijmegen, the Netherlands. Both episodic memory and executive functions were assessed in the patient group using the Delayed Story Recall subtest of the Rivermead Behavioural Memory Test-Third Edition (RBMT-3; Wilson et al., Citation2008) and the Brixton Spatial Anticipation test (Burgess & Shallice, Citation1997). To standardize the performance scores, the raw scores of both the Delayed Story Recall subtest and the Brixton Spatial Anticipation test were converted to z scores based on the group means, with higher scores indicating a better performance.
The controls were recruited via the network of the researchers. Exclusion criteria for the control group included severe head trauma, neurological or (self-reported) psychiatric disorders. summarizes the participants’ characteristics. The groups did not differ with respect to age, sex distribution or intelligence as estimated with the Dutch version of the National Adult Reading Test (p-values ≥ .107; Schmand et al., Citation1992). The study was approved by the ethics review committee of the Faculty of Social Sciences of Radboud University (NL38019.091.11). Participation was voluntary and written informed consent was obtained from all participants, in accordance with the Declaration of Helsinki.
Table 1. Demographic characteristics of the patients with acquired brain injury (ABI) and the controls.
Materials
A computerized spatial learning and memory task (i.e., the Drawer task) was used to examine learning performance of both patients with ABI and controls in both an EL and TEL condition (Scheper et al., Citation2019). During the acquisition phase, 20 everyday objects were sequentially shown at the bottom of a computer screen. Participants were instructed to find these objects in a 5 × 5 chest of drawers by clicking with the mouse on a drawer of their choice without a time limit. After finding the object, participants were instructed to memorize the location of the correct drawer. The order in which the EL and TEL conditions were administered was counterbalanced across subjects (see for a schematic representation of a sample trial of the Drawer task), and a separate set of instructions was given for each condition. The participants were given different instructions in the two learning conditions concerning the placement of the objects, while the other instructions (e.g., to memorize the correct object locations) were the same.
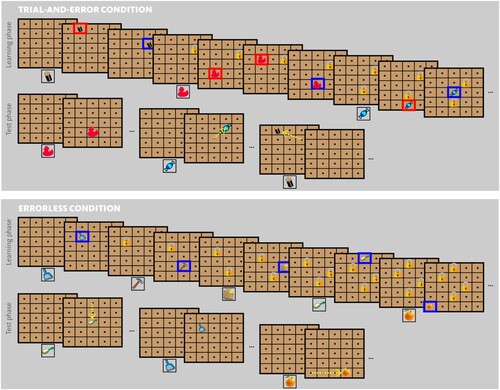
Figure 1. Schematic representation of a sample trial of the Drawer task. In the learning phase of trial-and-error learning (TEL; top panel) participants are asked to find the correct drawer in which a particular item (e.g., a battery) should be stored. If an incorrect drawer is selected, a red square appears and the participant has to select another drawer, until the correct drawer is found. Then, a blue square appears indicating the participant has to memorize the object location and that drawer is subsequently “locked”. Then, the next object is shown (e.g., rubber ducky), which has to be found. Importantly, the number of trials required before finding the correct drawer is predetermined, thus allowing the experimenter to control the number of errors committed during TEL (e.g., 1, 2, 3, 4 or 5 errors). In the learning phase of errorless learning (EL; bottom panel) participants are asked to place a particular item (e.g., a dustpan) randomly into an unlocked drawer and memorize the drawer in which the object was stored. After each learning phase, the locks are removed once all the items have been stored and each item is presented at the bottom of the screen once again during the test phase (recall stage). In the test phase, the objects appeared in random order and the participant are asked to place them in the correct drawer. The yellow arrows indicate the displacement score for items incorrectly placed.
During the EL condition, participants were instructed to randomly place the 20 objects into one of the unlocked drawers by mouse click. After the participant placed an object in a specific drawer, this was highlighted by a blue outline followed by a lock appearing on the chosen drawer, indicating that no other object could be stored in this drawer. Participants were instructed to memorize the correct location of each object placed in a drawer for later recall. As every first allocation was considered to be correct, no errors could occur during the acquisition.
In the TEL condition, participants were instructed to find out in which drawer 20 different common objects were stored, and after being successful, to remember the correct drawer. When participants chose the incorrect drawer, this drawer was outlined in red and participants had to continue looking for the correct drawer in which the object was located. When the correct drawer was chosen, participants saw a blue outline followed by a lock, indicating that no other object could be found in this drawer. The amount of “errors” made by the participants (1, 2, 3, 4 or 5) before they found the correct drawer in which the object should be stored was predetermined with 4 trials per error frequency manipulation (e.g., if an object was “found” after two clicks, one “error” was made). That is, the target location for each item was not pre-set, but determined by the participants after N clicks, of which the participant was unaware. To prevent participants from anticipating the error frequency, objects with different error frequencies were pseudo-randomly presented.
A self-paced recall phase followed immediately after each acquisition condition. In the recall phase, an identical 5 × 5 chest of drawers was presented without any locks. The objects allocated to the drawers during learning were sequentially and randomly shown at the bottom of the screen. Participants were given one attempt to place the object in the drawer in which the object was previously found or stored during the EL or TEL acquisition phase. No feedback about their performance was given. The performance of the participants during the free recall phase after, respectively, EL and TEL, was measured by the “error score” and “distance score”. The “error score” was measured as the mean of the sum of incorrectly recalled locations across participants. Every incorrect allocation of an object in a drawer during the recall phase, irrespective of which incorrect drawer, was counted as an error with a maximum of 20 errors per participants. The “distance score” was measured by the average of the absolute distance in arbitrary units between the target location and the recalled location across all 20 objects (see also Scheper et al., Citation2019, for details about the measurements).
Data analysis
First, two repeated measures General Linear Model (rm-GLM) analyses were conducted with Group (ABI vs. no ABI) as between-subject factor, Learning condition (EL vs. TEL) as within-subject factor and either the error score or the distance score as dependent variable to examine whether the EL performance was superior to TEL in ABI patients and matched controls.
To address our research question about the impact of error frequency during the TEL-acquisition on the later recall, two rm-GLM analyses were performed with Group (ABI vs. no ABI) as between-subject factor, Error frequency (performance on the 1, 2, 3, 4 and 5-error items) as within-subject factor and, respectively, the error score and distance score as dependent variable. Effect sizes are interpreted in accordance with the conventions as proposed by Cohen (Citation1992): : small: 0.01, medium: 0.06, large: 0.14; r: small: 0.10, medium: 0.30, large: 0.50.
To examine the relationship between deficits in executive functions and memory in ABI patients and the performance after EL and TEL, we performed exploratory analyses using Spearman’s rank correlations in the ABI group due to the small sample size.
Results
shows the results for each of the measurements after EL and TEL per group. Overall, ABI patients performed worse on the memory recall test than controls, irrespective of the EL or TEL condition, with a large effect size (F(1,28) = 5.79, p = .023, = .171). In both groups, the amount of errors at recall was significantly lower after EL compared to TEL, again with a large effect size (F(1,28) = 43.8, p < .001,
= .610). For the error score, no interaction between Group and Learning condition was found (F(1,28) = 1.59, p = .218,
= .054), indicating that, although ABI patients made more errors overall than controls, they benefited as much from EL compared to TEL as controls.
Figure 2. The mean error score and distance score for the patients with acquired brain injury (ABI) and the healthy controls (± SEM) per learning condition. *p < .05; **p < .01.
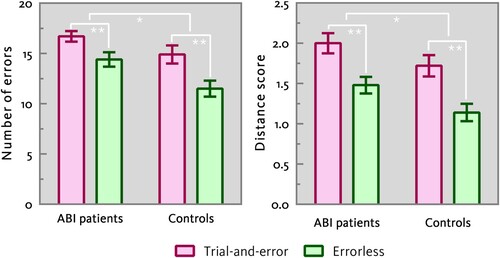
With respect to the displacement score, a large group difference was found between ABI patients and controls. ABI patients selected drawers which were further away from the correct drawer relative to controls (F(1,28) = 4.34, p = .046, = .134). Moreover, irrespective of group, a large performance difference was found between EL and TEL, in that EL resulted in a better performance at recall. That is, after EL drawers were selected that were closer to the correct ones, compared to TEL (F(1,28) = 48.4, p < .001,
= .633). No significant interaction effect was found between group and learning condition (F(1,28) = .151, p = .700,
= .005), meaning that EL results in better subsequent recall, that is, placing the objects closer to the correct drawer, compared to TEL, but the ABI patients benefitted as much as controls from EL relative to TEL.
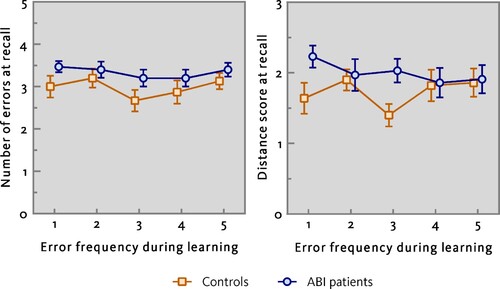
Furthermore, analysis of error scores indicated that the groups’ performance did not differ at recall and that there was no effect of Error frequency (Group: F(1,28) = 2.97, p = .096, = .096; Error frequency: F(4,112) = 1.77, p = .140,
= .059). This was also not the case for distance scores (Group: F(1,28) = 2.27, p = .143,
= .075; Error frequency: F (4,112) = .673, p = .612,
= .023; see also ). Also, no Group × Error frequency interaction effect was found (Error score: F(4,112) = .327, p = .859,
= .012; Distance score: F(4,112) = 1.80, p = .133,
= .061), indicating that after making a first error during learning, the occurrence of the second, third, fourth and fifth error had no additional detrimental effect on later recall performances.
Figure 3. The error score and distance score (± SEM) for each error frequency (1, 2, 3, 4, and 5 error trials) in the trial-and-error condition for the patients with acquired brain injury (ABI) and the healthy controls.
Exploratory analyses relating recall performance after EL and TEL to executive function and episodic memory in ABI patients demonstrated a significant and strong negative relationship between executive function (as measured with the Brixton Spatial Anticipation Test) and the Drawer task performance after TEL (error score: r = −.546, p = .035; distance score: r = −.720, p = .002), but no significant correlation with performance after EL (error score: r = −.191, p = .495; distance score: r = −.421, p = .118; see also ). Episodic memory (index by the delayed Story Recall) was not significantly associated with the performance on the Drawer task after EL (error score: r = −.134, p = .633; distance score: r = −.136, p = .682) or TEL (error score: r = .121, p = .667; distance score: r = .201, p = .473). These results indicate that better executive function is associated with a better performance after TEL.
Table 2. The correlations between the performances on Brixton Spatial Anticipation test and Delayed Story Recall of the Rivermead Behavioural Memory Test-Third Edition (RBMT-3) and the performance after errorless learning (EL) and trial-and-error learning (TEL) in the patients with acquired brain injury.
Discussion
In this study, we examined the effect of EL and TEL on memory recall in ABI patients with executive deficits compared to matched healthy controls using a spatial learning task. Results show a clear overall EL advantage on later recall of object locations, both in patients with ABI and in matched controls. Although ABI patients produced more errors on object location recall after both EL and TEL compared to matched controls, no difference was found with respect to the extent to which both groups benefitted from EL. Also, performance was unaffected by the number of errors made during the acquisition phase of TEL. In other words, memory recall was affected by whether or not errors occurred during learning, not by the frequency with which the errors were committed. In addition, we found that better executive function was associated with a better performance after TEL.
The beneficial effect of EL is consistent with previous findings in ABI patients by, for instance, Tailby and Haslam (Citation2003) and Ueno et al. (Citation2009), who used word-list learning tasks, and O’Neill et al. (Citation2010), who taught patients to put on a prosthetic limb. The EL advantage suggests that the occurrence of an object at a location that is not the object’s eventual target location, but may be a target location of a different object, may act as a source of interference during learning, causing difficulty in storage and/or retrieval of the correct memory traces. Postma et al. (Citation2018) found evidence for such an interference effect in amnesic patients with executive deficits on an object location memory task, demonstrating worse performance for those objects that were previously studied and tested at other locations compared to objects that had not been presented and tested at other locations. Worse executive function may thus especially hamper storage and retrieval of object-locations in an error-prone situation (e.g., our TEL condition). While poor performances on executive function was related to worse performance after TEL, no association was found between episodic memory function and recall on the Drawer task after either TEL or EL. As executive dysfunction has been linked to poor error-monitoring ability (Silver & Goodman, Citation2007), poor error monitoring may explain the observed relation between worse executive function and a detrimental effect of errors during learning on later recall.
The finding that recall performance was only influenced by whether or not an error was made during learning (but not by the error frequency) is in line with our previous findings in both healthy young and older adults (Scheper et al., Citation2019, Citation2021). Future research is needed on the impact and mechanisms of error frequency during learning on memory, as well as error monitoring, for instance using patients with memory deficits (e.g., individuals with mild cognitive impairment).
One limitation of our study is the relatively small sample size, which may have increased the risk of type II errors. Moreover, the localizations of the brain injuries in the ABI group are heterogeneous and there was a large variation in time since injury (5–336 months). However, we argue that this heterogeneity adds to the external validity as our sample is representative of the chronic ABI population in rehabilitation settings (e.g., Covington & Duff, Citation2021). Moreover, one could argue that in the EL condition, the correct object locations were subject-generated, whilst in the TEL condition, this was not the case (or at least the participants were not aware of this). Eliminating systematic differences between the two learning conditions as much as possible, other than the number of erroneous responses, is a challenge for all studies in the field of errorless learning (resulting in differences in stimulus presentation, participant engagement, or task duration in previous studies). A systematic comparison of our “active” EL condition versus a more “passive” condition in which, for instance, the correct location is highlighted and the participant has to place the correct object at that location (cf. Kessels et al., Citation2005) would be interesting for future study.
To conclude, our findings suggest a beneficial effect of EL compared to TEL on spatial memory, although the memory performance was not influenced by the error frequency during learning. By examining the relationship between both episodic memory and executive functioning on recall after TEL and EL in our sample, our results provide new insight into the underlying mechanisms of EL, which may have clinical relevance as well. That is, we demonstrated that patients with poor executive functioning are more susceptible to the detrimental effects of errors during the acquisition of new episodic information than those with better executive function. Such knowledge may facilitate the development or improvement of other cognitive rehabilitation interventions, such as errorless Goal Management Training (Bertens et al., Citation2015) and other (errorless) compensation strategy training aimed at improving, for instance, error monitoring, self-regulation skills, or problem-solving skills (Leshner et al., Citation2013; Ownsworth, Citation2018). Finally, it should be mentioned that errors may also have positive effects on learning, which was, for instance, demonstrated in the acquisition of goal-directed everyday activities in a group of severe TBI patients, with better generalized of skills to related tasks after error-based learning compared to EL (Ownsworth et al., Citation2017). Future research is needed to examine to what extent EL and TEL rely on executive function and to further identify the neuropsychological characteristics of individuals whom may or may not benefit from errorless and errorful learning.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Baddeley, A., & Wilson, B. A. (1994). When implicit learning fails: Amnesia and the problem of error elimination. Neuropsychologia, 32(1), 53–68. https://doi.org/10.1016/0028-3932(94)90068-X
- Bertens, D., & Brazil, I. A. (2018). Cognitive and neural correlates of errorless learning. In C. Haslam & R. P. C. Kessels (Eds.), Errorless learning in neuropsychological rehabilitation: Mechanisms, efficacy and application (pp. 26–40). Routledge.
- Bertens, D., Kessels, R. P. C., Fiorenzato, E., Boelen, D. H. E., & Fasotti, L. (2015). Do old errors always lead to new truths? A randomized controlled trial of errorless Goal Management Training in brain-injured patients. Journal of the International Neuropsychological Society, 21(8), 639–649. https://doi.org/10.1017/S1355617715000764
- Broadway, J. M., Rieger, R. E., Campbell, R. A., Quinn, D. K., Mayer, A. R., Yeo, R. A., Wilson, J. K., Gill, D., Fratzke, V., & Cavanagh, J. F. (2019). Executive function predictors of delayed memory deficits after mild traumatic brain injury. Cortex, 120, 240–248. https://doi.org/10.1016/j.cortex.2019.06.011
- Burgess, P. W., & Shallice, T. (1997). The hayling and brixton tests. Thames Valley Test Company.
- Cicerone, K. D., Dahlberg, C., Kalmar, K., Langenbahn, D. M., Malec, J. F., Bergquist, T. F., Felicetti, T., Giacino, J. T., Harley, J. P., Harrington, D. E., Herzog, J., Kneipp, S., Laatsch, L., & Morse, P. A. (2000). Evidence-based cognitive rehabilitation: Recommendations for clinical practice. Archives of Physical Medicine and Rehabilitation, 81(12), 1596–1615. https://doi.org/10.1053/apmr.2000.19240
- Cicerone, K. D., Goldin, Y., Ganci, K., Rosenbaum, A., Wethe, J. V., Langenbahn, D. M., … Harley, J. P. (2019). Evidence-based cognitive rehabilitation: Systematic review of the literature from 2009 through 2014. Archives of Physical Medicine and Rehabilitation, 100(8), 1515–1533. https://doi.org/10.1016/j.apmr.2019.02.011
- Clare, L., & Jones, R. S. (2008). Errorless learning in the rehabilitation of memory impairment: A critical review. Neuropsychology Review, 18(1), 1–23. https://doi.org/10.1007/s11065-008-9051-4
- Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037/0033-2909.112.1.155
- Cohen, M., Ylvisaker, M., Hamilton, J., Kemp, L., & Claiman, B. (2010). Errorless learning of functional life skills in an individual with three aetiologies of severe memory and executive function impairment. Neuropsychological Rehabilitation, 20(3), 355–376. https://doi.org/10.1080/09602010903309401
- Covington, N. V., & Duff, M. C. (2021). Heterogeneity is a hallmark of traumatic brain injury, not a limitation: A new perspective on study design in rehabilitation research. American Journal of Speech-Language Pathology, 30(2S), 974–985. https://doi.org/10.1044/2020_AJSLP-20-00081
- Dijkers, M. P. (2004). Quality of life after traumatic brain injury: A review of research approaches and findings. Archives of Physical Medicine and Rehabilitation, 85(Suppl 2), 21–35. https://doi.org/10.1016/j.apmr.2003.08.119
- Evans, J. (2018). Application of errorless learning in adults acquired brain injury rehabilitation. In C. Haslam & R. P. C. Kessels (Eds.), Errorless learning in neuropsychological rehabilitation: Mechanisms, efficacy and application (pp. 58–81). Routledge.
- Fish, J., Evans, J. J., Nimmo, M., Martin, E., Kersel, D., Bateman, A., Wilson, B. A., & Manly, T. (2007). Rehabilitation of executive dysfunction following brain injury: “Content-free” cueing improves everyday prospective memory performance. Neuropsychologia, 45(6), 1318–1330. https://doi.org/10.1016/j.neuropsychologia.2006.09.015
- Haslam, C., Hodder, K. I., & Yates, P. J. (2011). Errorless learning and spaced retrieval; How do these methods fare in healthy and clinical populations? Journal of Clinical and Experimental Neuropsychology, 33(4), 432–447. https://doi.org/10.1080/13803395.2010.533155
- Hunkin, N. M., Squires, E. J., Parkin, A. J., & Tidy, J. A. (1998). Are the benefits of errorless learning dependent on implicit memory? Neuropsychologia, 36(1), 25–36. https://doi.org/10.1016/S0028-3932(97)00106-1
- Kessels, R. P. C., Te Boekhorst, S., & Postma, A. (2005). The contribution of implicit and explicit memory to the effects of errorless learning: A comparison between young and older adults. Journal of the International Neuropsychological Society, 11, 144–151. https://doi.org/10.1017/S1355617705050174
- Leshner, A. F., Tom, S. R., & Kern, R. S. (2013). Errorless learning and social problem-solving ability in schizophrenia: An examination of the compensatory effects of training. Psychiatry Research, 206(1), 1–7. https://doi.org/10.1016/j.psychres.2012.10.007
- Lloyd, J., Riley, G. A., & Powell, T. E. (2009). Errorless learning of novel routes through a virtual town in people with acquired brain injury. Neuropsychological Rehabilitation, 19(1), 98–109. https://doi.org/10.1080/09602010802117392
- O’Neill, B., Moran, K., & Gillespie, A. (2010). Scaffolding rehabilitation behaviour using a voice-mediated assistive technology for cognition. Neuropsychological Rehabilitation, 20(4), 509–527. https://doi.org/10.1080/09602010903519652
- Ownsworth, T. (2018). Errors: Friend or foe? The theory and evidence base fot error-based learning. In C. Haslam & R. P. C. Kessels (Eds.), Errorless learning in neuropsychological rehabilitation: Mechanisms, efficacy and application (pp. 164–179). Routledge.
- Ownsworth, T., Fleming, J., Tate, R., Beadle, E., Griffin, J., Kendall, M., Schmidt, J., Lane-Brown, A., Chevignard, M., & Shum, D. H. K. (2017). Do people with severe traumatic brain injury benefit from making errors? A randomized controlled trial of error-based and errorless learning. Neurorehabilitation and Neural Repair, 31(12), 1072–1082. https://doi.org/10.1177/1545968317740635
- Page, M., Wilson, B. A., Shiel, A., Carter, G., & Norris, D. (2006). What is the locus of the errorless-learning advantage? Neuropsychologia, 44(1), 90–100. https://doi.org/10.1016/j.neuropsychologia.2005.04.004
- Ponsford, J. L., Downing, M. G., Olver, J., Ponsford, M., Acher, R., Carty, M., & Spitz, G. (2014). Longitudinal follow-up of patients with traumatic brain injury: Outcome at two, five, and ten years post-injury. Journal of Neurotrauma, 31(1), 64–77. https://doi.org/10.1089/neu.2013.2997
- Postma, A., Morel, S. G., Slot, M. E., Oudman, E., & Kessels, R. P. C. (2018). Forgetting the new locations of one’s keys: Spatial-memory interference in Korsakoff’s amnesia. Experimental Brain Research, 236(7), 1861–1868. https://doi.org/10.1007/s00221-018-5266-7
- Scheper, I., Brazil, I. A., De Bruijn, E. R. A., Mulder-Hanekamp, L., & Kessels, R. P. C. (2021). Prevention is better than cure: Effects of errors on memory performance during spatial learning in healthy aging. Aging Clinical and Experimental Research, 33(4), 997–1003. https://doi.org/10.1007/s40520-020-01603-2
- Scheper, I., de Bruijn, E. R. A., Bertens, D., Kessels, R. P. C., & Brazil, I. A. (2019). The impact of error frequency on errorless and errorful learning of object locations using a novel paradigm. Memory, 27(10), 1371–1380. https://doi.org/10.1080/09658211.2019.1661493
- Schmand, B., Lindeboom, J., & van Harskamp, F. (1992). Nederlandse Leestest voor Volwassenen: handleiding [Dutch adult reading test: Manual]. Swets & Zeitlinger.
- Silver, H., & Goodman, C. (2007). Impairment in error monitoring predicts poor executive function in schizophrenia patients. Schizophrenia Research, 94(1-3), 156–163. https://doi.org/10.1016/j.schres.2007.04.019
- Sun, J.-H., Tan, L., & Yu, J.-T. (2014). Post-stroke cognitive impairment: Epidemiology, mechanisms and management. Annals of Translational Medicine, 2(8), 80. https://doi.org/10.3978/j.issn.2305-5839.2014.08.05
- Tailby, R., & Haslam, C. (2003). An investigation of errorless learning in memory-impaired patients: Improving the technique and clarifying theory. Neuropsychologia, 41(9), 1230–1240. https://doi.org/10.1016/S0028-3932(03)00036-8
- Ueno, H., Maruishi, M., Miyatani, M., Muranaka, H., Kondo, K., Ohshita, T., & Matsumoto, M. (2009). Brain activations in errorless and errorful learning in patients with diffuse axonal injury: A functional MRI study. Brain Injury, 23(4), 291–298. https://doi.org/10.1080/02699050902794855
- Watson, P. A., Gignac, G. E., Weinborn, M., Green, S., & Pestell, C. (2020). A meta-analysis of neuropsychological predictors of outcome following stroke and other non-traumatic acquired brain injuries in adults. Neuropsychologiy Review, 30(2), 194–223. https://doi.org/10.1007/s11065-020-09433-9
- Wilson, B. A., Greenfield, E., Clare, L., Baddeley, A., Cockburn, J., Watson, P., … Nannery, R. (2008). Rivermead behavioural memory test (3rd ed.). Pearson.