
Abstract
The Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico is a five-century institution that, besides the unique clinical role in the center of Milan, may rely on benefactor donations such as fields and farming houses not far from the city, for a total of 8500 ha, all managed by the “Sviluppo Ca’ Granda’ Foundation”. Presently, the main products of these fields are represented by rice and cow’s milk. During the latest years, farmers and managers have developed a model of sustainable food production, with great attention to the product quality based on compositional analysis and functional nutritional characteristics. This experience represents a new holistic model of food production and consumption, taking great care of both sustainability and health.
Introduction
Food choices made by consumers have a major effect on health and wellbeing, and the importance of a balanced diet is well-known. Apart from their energy and nutrients, food products should also be evaluated for safety, sustainability and impact on the environment, which in turn may affect human societies and wellbeing (FAO Citation2013; Ioannidis Citation2013). Taking into consideration all of these aspects may lead to an innovative and virtuous “holistic” model of food production and distribution.
When it comes to sustainability, a potentially ideal model should include a short food chain, easy traceability, feasibility and finalization, in terms of advantage for all potential stakeholders (Food Chain Evaluation Consortium Citation2014). This last step may require functional properties definition of a specific food product towards consumers on one side, as well as a positive economic impact on the producers on the other. The development and exploitation of this type of model could be of particular interest for settings and institutions laying within the framework of health and healthcare.
The Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico (the Hospital from now on) is a five-century old Institution taking care of sick people in Milan. Through its history, the Hospital has become a widespread entity, mainly thanks to bequests from donors, inclusive of fields and farming houses. In September 2014, the Fondazione Sviluppo Ca’ Granda (the Foundation from now on) was established in order to handle the assets and to promote Hospital scientific research thanks to the conferred agricultural heritage. Presently, the main food products originating from the Foundation's fields and farms are represented by rice and cow’s milk (Riva & Mazzoleni Citation2012).
Within this context, the aim of the present report was to evaluate three food products (milk and two rice varieties) grown and produced within the Foundation's estate and characterised by a very short food chain. The three products have been evaluated in terms of nutritional composition and functional effects in humans (for rice), keeping into account for the global cost/benefit balance. When standardized, this model could represent a reference for other similar institutions and settings.
Materials and methods
Food products
The three foods grown and produced within in the Foundation's estate were milk, produced by Holstein Friesians race cows, and two varieties of rice: Arborio and Carnaroli, both Japonica group cultivars of Oryza sativa.
The Arborio rice is cultivated and treated at the Azienda Agricola Corte Grande, located in Linarolo (Pavia). The Carnaroli variety is produced at the Azienda Agricola Forni Francesco, Cascina Lasso, Morimondo (Milan). Cows are raised at the Azienda Agricola Cazzalini, Morimondo (Milan). The cooperative “Latte Varese”, where the milk is pasteurized, is located in Varese (Varese). All these locations are placed within 40 km from Milan Downtown.
The two varieties of rice can be purchased directly at the production site, while milk is usually sold to milk processing factories that, in turn, sell it to consumers. As a new experimental step to approach consumers, from October to December 2015, these products were sold in a temporary store within the Hospital.
Preparation and treatment
Fresh milk (whole and semi-skimmed) was pasteurized at 72 °C for approximately 15–20 s. Semi-skimmed milk (1.5% fat) was defatted by a centrifugal separation. Rice varieties were refined by mechanical removal of bran and germ.
Composition of food items
Rice varieties were analyzed for starch (AOAC Method 996.11), sugar (AACCI Method 80-04.01), protein (AOAC Method 992.23), lipid composition (AOAC Method 922.06), dietary fiber (AOAC method 985.29) and amino acid composition by high performance liquid chromatography (HPLC). Gluten was analyzed by ELISA (EZ Gluten™ test, ELISA Technologies, Gainesville, FL). Vitamins were determined by HPLC. Mycotoxins were analyzed by ELISA (AgraQuant®-Romer Labs, Union, MO).
The milk was analyzed for sugar (AOAC 980.13), protein (AOAC 920.105), lipid composition (gas chromatography with flame ionization detector) and amino acid composition by HPLC (Marino Citation2010). Vitamins were determined by HPLC. Inductive Coupled Plasma with optical emission spectroscopy (ICP–OES) was used for quantification of minerals.
In vivo functional measurements
The glycemic index (GI) and insulinemic responses after rice consumption by healthy volunteers have been taken into consideration as the main metabolically relevant functional evaluations.
Eleven healthy subjects agreed to participate in the study. They were between 25 and 35 years old, with normal Body Mass Index (range 18–25 kg/m2) and a written informed consent, according to the Declaration of Helsinki on human rights. Signs of metabolic syndrome (Eckel et al. Citation2010) were exclusion criteria. Drugs and diseases interfering with carbohydrates metabolism, as well excessive alcohol intake (30 g/day for males and 20 g/day for females) and pregnancy were considered exclusion criteria.
The GI was measured according to International Standard (ISO Citation2010) and insulin levels were measured through electrochemiluminescent immunoassay at the same time points used for GI testing.
The study protocol was approved by Ethical Committee of Milan – B Area.
Statistical analysis
Data are expressed as mean ± standard deviation. Two-tailed Student’s t-test (p < .05) was used to identify differences between GI values and insulin IAUCs (SPSS Statistical Software, ver 20.0, IBM, Chicago, IL).
Results
Nutritional values of the two rice varieties (Carnaroli and Arborio) and of both whole and low fat milk are reported in and , respectively.
Table 1. Rice composition.
Table 2. Milk composition.
Regarding rice GI and insulinemic response, all the 11 subjects (82% female; age 29.5 years; range 26–34 years; BMI 22.4 ± 1.5) completed reference and rice tests. Milk curves were not investigated since consumption of 1110 mL of product, necessary to provide 50 g of carbohydrates, was not considered to be well tolerated, while lower amounts of milk provided unreliable results.
Postprandial glycemic and insulin responses are reported in for the two types of rice. Carnaroli and Arborio rice GI were 46.3 ± 11.3 and 48.6 ± 21.1, respectively. The difference between the two rices was not statistically significant (p = .86).
Figure 1. Glycemic (solid line) and insulinemic (dotted line) responses with Arborio (Panel 1) and Carnaroli rices (Panel 2).
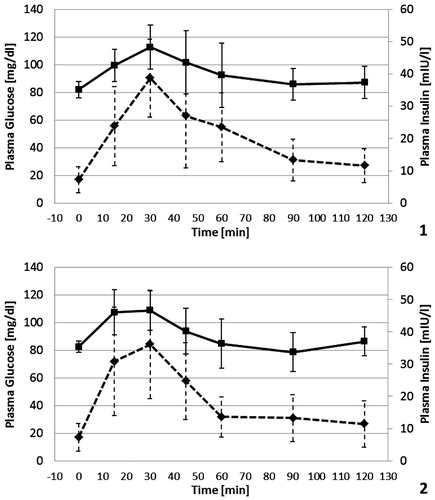
The mean value of incremental area under the curve for insulin (IAUC) after ingestion of Arborio rice was 1432 ± 576 mIU/L*min, while the IAUC after Carnaroli rice was 1512 ± 669 mIU/L*min. The two values were equivalent (p = .8).
Discussion
We have here described a very special model of food production and distribution, which, as said before, could be of particular interest for settings and institutions laying within the framework of health and healthcare. The uniqueness of this model lays in the fact that all food chain steps are supervised by the Foundation and the Hospital, whose primary purposes are, respectively, estates management and health and wellbeing of patients and, more extensively, of the community.
Since environmental integrity, local traditions and short distance between production and consumption are respected, we may assume that this model falls within the worldwide accepted definition of sustainability.
From a nutritional viewpoint, the composition of these foods shows a profile falling within the optimal range of reference counterparts (Souci et al. Citation2008).
Analyzing the results for the glucose and insulin curves, we may observe that the GI values fall within the lower values observed among all the types of rice (Kaur et al. Citation2016) and even below the threshold of low GI foods, that is ≤55 (Wolever et al. Citation2006). Rice is generally considered a high GI food, but this depends on varietal, compositional and processing factors. Being rice a major contributor to glycemic load in many populations, the possibility to have low GI rice varieties that can elicit favorable insulinemic response is of primary interest, especially considering health effects of these parameters. As a matter of fact, the results here described are of value since they suggest that rice produced in this model system may maintain characteristics able to improve its impact on health (Food Chain Evaluation Consortium Citation2014). The insulinemic response could also be considered relatively low with respect to previously published data on the topic (Jung et al. Citation2009; Lin et al. Citation2010; Tan et al. Citation2015).
On the whole, the novelty of this holistic model here described may contribute to increase sustainability and health promotion strategies elsewhere. In addition, this model highlights the leading role of a healthcare institution taking care of patients and of the local community. This should be properly emphasized worldwide and followed as an example. Actually, in a moment in time where we experience a continuous change in food availability and quality strictly connected to globalization, the advantages offered by this model of food production and distribution should be explored in depth across different settings, as it has the potential of improving wellbeing at many levels.
Hopefully, in the next future, this model could be extended to other institutions and food products, in order to establish an innovative approach able to improve at the same time efficiency of public intervention, community health (either in terms of prevention and therapeutic regimens) and local socioeconomic and environmental impact.
Acknowledgements
The help in measuring and interpretating food composition by Prof. Alberto Battezzati, University of Milan, is gratefully acknowledged.
Disclosure statement
The authors declare no conflict of interest regarding this research.
Funding
The study was funded by Sviluppo Ca’ Granda’ Foundation, Milan.
References
- Eckel RH, Alberti KG, Grundy SM, Zimmet PZ. 2010. The metabolic syndrome. Lancet. 375:181–183.
- Food and Agriculture Organization of the United Nations (FAO). 2009. How to feed the world in 2050. Rome: FAO.
- Food and Agriculture Organization of the United Nations (FAO). 2013. Healthy people depend on healthy food systems. Rome: FAO.
- Food Chain Evaluation Consortium. 2014. Scoping study. Delivering on EU food safety and nutrition in 2050 – scenarios of future change and policy responses. Brussels, Belgium: European Commission.
- Ioannidis JPA. Implausible results in human nutrition research. 2013. Definitive solutions won’t come from another million observational papers or small randomized trials. BMJ. 347:f6698.
- ISO. International Standards Organization. 2010. Food products – determination of the glycaemic index (GI) and recommendation for food classification. Geneva, Switzerland: International Standards Organization. ISO 26642–2010.
- Jung EY, Suh HJ, Hong WS, Kim DG, Hong YH, Hong IS, Chang UJ. 2009. Uncooked rice of relatively low gelatinization degree resulted in lower metabolic glucose and insulin responses compared with cooked rice in female college students. Nutr Res. 29:457–461.
- Kaur B, Ranawana V, Henry J. 2016. The glycemic index of rice and rice products: a review, and table of GI values. Crit Rev Food Sci Nutr. 56:215–236.
- Lin MHA, Wu MC, Lu S, Lin J. 2010. Glycemic index, glycemic load and insulinemic index of Chinese starchy foods. World J Gastroenterol. 16:4973–4979.
- Marino R. 2010. Technical note: rapid method for determination of amino acids in milk. J Dairy Sci. 93:2367–2370.
- Riva MA, Mazzoleni D. 2012. The Ospedale Maggiore Policlinico of Milan. J Med Pers. 10:136–138.
- Souci SW, Fachmann W, Kraut H. 2008. Food composition and nutrition tables. 7th ed. Stuttgart, Germany: MedPharm Scientific Publishers.
- Tan VMH, Wu T, Henry CJ, Lee YS. 2015. Glycaemic and insulin responses, glycaemic index and insulinaemic index values of rice between three Asian ethnic groups. Br J Nutr. 113:1228–1236.
- Wolever TM, Yang M, Zeng XY, Atkinson F, Brand-Miller JC. 2006. Food glycemic index, as given in glycemic index tables, is a significant determinant of glycemic responses elicited by composite breakfast meals. Am J Clin Nutr. 83:1306–1312.