
ABSTRACT
Increasing public investments in distributed platform infrastructures created new opportunities for economic growth and social welfare but simultaneously were associated with growing societal distrust in science’s power to solve societal problems. The concept of Responsible Research and Innovation was advanced as providing mechanisms to recouple science and society ensuring that research and innovation continues to uphold its societal duties. In this paper, we explore the extent to which it is possible to identify repertoires of responsible innovation behaviour within extant regional research and innovation networks through the way that these innovation networks draw on informal regional innovation resources. We distinguish two kinds of regional innovation network, those based on primarily synthetic knowledge bases, and those based on primarily analytic knowledge bases, in the eHealth sector where there are substantive societal concerns regarding responsibility and innovation. We contend it appears that the coupling of patients to innovation networks through their prior association with innovators (e.g. as patients) affects the scope for responsibility. We therefore contend that more attention is required for understanding the dynamics of citizen-innovator coupling in regional innovation networks if responsibility is to become a more common systemic property.
1. Introduction
Contemporary growth has become dependent on public sector investments creating increasingly complicated technological infrastructure systems platforms (Asheim, Citation2012). Policy-makers and multilateral organizations enthusiastically embraced these approaches because of their potential to better drive neo-endogenous growth and create place-specific local value propositions allowing those regions to occupy high-value positions within global value chains (Hollands, Citation2008). These investments occur within public-private partnerships, where private partners may lack suitable incentives to promote public value, creating the risks of public value failure, undermining public support for those investments (Bozeman, Citation2002).
The Responsible Research and Innovation (RRI) agenda emerged from efforts to restore this trust, proposing a conceptual framework for ensuring scientists and innovations sufficiently receive appropriate societal signals to steer their innovation projects to address public concerns (Stilgoe, Owen, & Macnaghten, Citation2013). Scientists and innovators continually taking choices related to future activities based upon anticipating how their peers will judge their choices, reflecting ‘weak signals’ within their wider networks. RRI processes seek to proactively encourage scientists and innovators to prospectively anticipate how various publics may respond to their research and innovation processes’ outcomes. But scientists and innovators are already embedded in knowledge networks (Kitcher, Citation2001) and RRI processes ignore the importance of these existing networks which also channel signals to scientists and innovators (Ribeiro et al., Citation2018). This has may make RRI elective for innovators rather than essential, an additional set of tasks and pressures prescribed to those already under severe pressures of uncertainty. Effectively achieving RRI therefore requires innovators to fit responsible behaviours within their knowledge networks (Walhout et al., Citation2016).
Regional innovation has its own internal logics and norms around meeting market needs that may leave little direct autonomy for innovators to respond to societal signals, even where these societal signals are promoted as being worthy of consideration (Fitjar, Benneworth, & Asheim, Citation2019). But the coherence of regional innovation spaces partly derives from the informal regional collectivities that shape interaction and knowledge exchange (Adam & Westlund, Citation2013). These informal regional collectivities (a kind of regional social/ cultural capital) represent an innovation resource embodying regional interests and desires. In this paper we explore whether this informal regional capital can influence innovation trajectories in ways that make them more socially responsible. We follow Asheim and Coenen (Citation2005) and Liu, Chaminade, and Asheim (Citation2013) in noting that the dominant ‘knowledge base’ (use-driven/ synthetic or science driven/ analytic) of an innovation activity affects its associated innovation networks structure and governance. We ask:
How do the dominant knowledge bases within regional innovation systems affect how responsible practices can become embedded in innovation trajectories?
2. Literature review
2.1. A micro-level perspective on knowledge actor dynamics
There is an increasing recognition that we live in a ‘knowledge economy’ where places’ wealth depends upon receiving, processing, converting and exploiting knowledge capital through innovation processes (Temple, Citation1998). The importance of proximity to knowledge transfer, exchange and innovation gives the regional scale a significance in the geography of innovation (Lawson & Lorenz, Citation1999). Cooke (Citation2005) argued that systematic linkages build up in regions to constitute a regional innovation system (RIS) comprising distinctive subsystems (knowledge producers, knowledge exploiters, intermediaries, policy-makers and regional culture). The systemic nature of regional innovation provide places’ economic trajectories with a persistent character: changing regional innovation outcomes requires altering these evolutionary trajectories (Kogler, Citation2015). Regional trajectories change when local networks become more attractive to external investors, making regions more of a ‘place to be’ for particular knowledge actors (Yeung, Citation2009). The popularity of the RIS concept has led to its increasingly mechanical treatment overlooking the fact that these networks and interactions depend upon individual innovators (Asheim, Citation2012; Uyarra et al., Citation2017). Innovators take decisions based on their own preferences influenced by their wider networks within which they access various kinds of resource. Those individuals’ mutual familiarity and knowledge represents via spill-over effects a more general territorial resource (Adam & Westlund, Citation2013), and regional systems can be changed by individuals through acts of institutional entrepreneurship (Benneworth, Pinheiro, & Karlsen, Citation2017; Sotarauta, Citation2016).
Research and innovation advances through a form of distributed coordination in which innovators undertake acts of prospective anticipation. In choosing which of several uncertain futures to pursue, individuals shape their behaviours and decisions on the basis of their expectations of later consequences (Gläser, Citation2012). The overall effect of this is that technological problems are formulated and proposed, and resources allocated to solve those problems, on the basis of anticipated responses. This anticipation process is shaped by collective beliefs held in various kinds of epistemic communities (Haas, Citation1992) about what is good and bad, allowing those norms to shape progress. Those communities also signal in various ways (whether publication or technological standards) what is considered ‘good’ ‘knowledge’ and who are good knowledge creators (legitimate community members; Roberts, Citation2014). This dual signalling (prospective/ retrospective) allows these knowledge communities to progress on the basis of collective community understandings of ‘goodness’ (Kogan, Citation2005).
Amin and Roberts have pointed to the ways in which these communities become territorialized, and in which local communities of practice achieve more epistemic characteristics (Citation2008). Innovation networks serve partly as neutral platforms for exchanging knowledge between geographically-proximate partners. But they also serve for signals determining what constitutes ‘good’ solutions as the basis for prospectively selecting knowledge creation activities, as what Walhout et al. (Citation2016) call informal governance networks, which collectively defines which kinds of knowledge are deemed interesting, acceptable and desirable (Fitjar et al., Citation2019).
2.2. Towards a regional conceptualization of RRI
This characteristic of regional innovation networks as transmitting value signals becomes increasingly important in the context of RRI. Rene von Schomberg defines RRI thus:
a transparent, interactive process by which societal actors and innovators become mutually responsive to each other with a view to the (ethical) acceptability, sustainability and societal desirability of the innovation process and its marketable products (Von Schomberg, Citation2011, p. 9).
Owen, Macnaghten, and Stilgoe (Citation2012) identify three arrangements delivering RRI (a) democratic governance of the research, development and innovation systems, (b) the institutionalization of feedback into decision-making and (c) acknowledgement of the collective nature of the risk and uncertainty of innovation processes. Stilgoe et al. (Citation2013) highlight four RRI processes, namely anticipation, reflexivity, inclusion and responsiveness. Anticipation involves researchers seeking to systematically anticipate their knowledge projects’ wider societal implications; reflexivity involves researchers questioning the assumptions and normative ethical positions underpinning knowledge activities; inclusion is the systematic approach of all stakeholders (not just the most powerful or visible) for feedback; finally, that inclusion should provide real opportunities to influence the innovation trajectory (responsiveness).
Each dimension involves societal signals being given to innovators and the effects of those signals depends at least partly on their relative strength. Innovators continually anticipate their activities’ outcomes albeit not always seeking to maximize these responsibility outcomes. Likewise, responsibility in reflexivity means systemically including the notion of responsibility as one element of ‘good’ knowledge processes in these wider governance networks. Inclusion involves connecting with new stakeholders but innovators already have contacts with stakeholders; additional inclusion changes the governance network’s topology rather than straightforwardly importing responsibility into decision-making.
Although their concept can be critiqued for obscuring power, encouraging a replication of existing power structures (Genus & Iskandarova, Citation2018), the presence of these processes does represent an antecedent of the development of responsibility. Our concern with the concept is that is lacks a straightforward conception of place for research and innovation to be responsible towards. This has driven placeless responsibility discourses in which innovators – active in global networks – (Fitjar et al., Citation2019) ignore those localities in which they carry out their innovation networks, regarding them as epiphenomenal, what Law called ‘small and incoherent’ (2004), denying them influence in these innovation processes.
To reinsert this regional power dimension, we note that ‘regional culture’ can represent a innovation resource and therefore can influence the decisions taken within innovation activities (Cooke, Citation2005; Paasi, Citation2013). This regional culture can therefore provide signals to innovators taking decisions in their innovation processes. These signals may in turn correspond with Stilgoe et al. (Citation2013)’s responsibility repertoires, making those innovators sensitive and responsive to regional needs, desires and norms. If this condition were to be fulfilled (‘regional cultural signals steering innovators to enact responsibility repertoires’) this would represent a regional variant of RRI.
2.3. Responsibility in networks with analytic vs synthetic knowledge-bases
We operationalize responsibility as four kinds of repertoires within innovators’ decision-making processes. As well as global and regional factors (Cooke, Citation2005), regional innovation networks are shaped by the nature of the knowledge they seek to transform (Gibbons, Citation2000; Isaksen & Karlsen, Citation2010; Trippl, Citation2011) We here distinguish three knowledge types, namely synthetic, analytic and symbolic (Asheim & Coenen, Citation2005; Asheim & Coenen, Citation2006; Liu et al., Citation2013). The first is synthetic knowledge, from which value is created through its application and combination with other kinds of knowledge to apply it to create solutions to particular kinds of problem (e.g. engineering knowledge). Analytic knowledge is created within primarily scientific contexts (the domain of creation) and value is created through its transformation into a domain of application (e.g. via a patent in biotechnology). Symbolic knowledge creates value through its appreciation and consumption as a cultural product (e.g. constructing new kinds of cultural genre, not further considered until the conclusions).
We use this distinction to operationalize two approaches by which regional cultural signals could potentially become significant within regional innovation networks (see also ). In regional innovation networks where synthetic knowledge is the dominant base, regional anticipation involves establishing projects to create benefits for regional beneficiaries in ways that envisaged better futures for those beneficiaries after the innovation process’ completion. Regional reflexivity involves partners rethinking innovation to create alternative forms of value and to drive shifts in value systems (social as well as technological innovation). Regional inclusion involves ensuring that the desired beneficiaries of this improved future are connected to the innovation activities with the opportunities to express views on it. Regional responsiveness involves regional partners contributing to innovation processes in various ways, such as lead users and testers, and their preferences and knowledge being incorporated into the innovation process thereby shaping its ultimate direction.
Table 1. Dimensions of responsibility in regional innovation networks with analytic vs synthetic knowledge Cases.
Conversely, in networks dominated by analytic knowledge, regional anticipation would involve knowledge producers thinking seriously about the potential impacts of their research in the future, involving local partners to tailor those future scenarios to regional contexts. Regional reflexivity would involve knowledge producers testing their ideas and developments against local norms and values. Regional inclusion involves listening to a wide range of stakeholder groups, and in particular, beyond vested interests and ‘the usual suspects’ to allow authentic societal expression over these directions. Finally, regional responsiveness would involve knowledge exchange and co-creation with regional partners in which regional partners were able to actively contribute to the ongoing knowledge creation activities.
3. Methodology: studying RRI as governance
In this paper, we explore the extent to which non-instrumental regional characteristics (hereafter referred to as regional ‘culture’) become influential (or not) within innovation processes in ways that correspond with enacting responsible behavioural repertoires. This is an exploratory piece of research where we proposed a process model ( above) of the incorporation of regional culture into innovation decision-making. We therefore seek to gather individual-level data, to firstly map out their innovation decision-making, and then to focus on the responsibility repertoires evident in them and in particular the uptake of regional culture in these repertoires. We focus specifically on this regional dimension because of the critique of RRI of being insufficiently rooted to particular societal norms and values.
We constructed this as a qualitative case study to try to perceive observe how regional context and knowledge base affects the dynamics of regional RRI. We gathered appropriate data and structured that data according to our framework. Health and telemedicine was selected because responsible e-Health innovation demands responding to societal and patient voices in innovation processes that are (a) heavily institutionalized (as medicine) and (b) very technology focused (more detail is provided in 4.1). We selected one case study corresponding to each knowledge base, including one case driven primarily by practitioners and one where a spin-off company was established to exploit a technology emerging from a European Research Framework-funded project (see 4.3).
We chose to investigate these case studies in the Dutch Overijssel province because the Provincial government identified e-Health and telemedicine as a strategic economic opportunity, seeking to stimulate innovation in this sector to drive innovation-led growth. We identified two e-health/telemedicine innovation projects in which efforts had been made to secure user and patient input. The case studies were carried out between February and August 2017, and involved gathering secondary material as well as identifying our knowledge from previous projects about the sector to help build depth in the case study (Benneworth et al., Citation2017; Benneworth & Hospers, Citation2007; Benneworth & Pinheiro, Citation2017). Primary data included a total of 11 key informants interviews (those (a) actively involved in developing the innovation, (b) mediating between innovators and ‘public users’ or (c) with specialist knowledge of the regional e-Health/ Telemedicine sector context). Interviews were undertaken from May to August 2017, lasting 60–90 min; the interview instrument was in Dutch, although the interview language was pragmatically agreed between interviewer and interviewee; the majority of interviews were carried out in Dutch, with other interviews in English and German.
From these interviews two stylized narratives were produced of each innovation and research process, firstly mapping the regional innovation networks associated with the innovations, and the ways these networks linked actors with regional knowledge base (Section 5), and potential responsibility repertoires within these stylized narratives, linked to the regional knowledge base (Section 6). These stylized analyses provided the basis to answer the question, to consider whether responsibility can be built into regional innovation processes. We acknowledge that this approach is exploratory, stylized and about identifying general tendencies and lines of force within our case study, and it does not allow us to make definitive statements about RRI. However, it rather provides the basis to reflect exploratorily upon the theoretically derived model proposed above for understanding responsibility around regional research and innovation.
4. Introduction to the case studies
4.1. eHealth
eHealth has emerged as a novel technological field providing health services using new technologies novel capacities to create more efficient health care. They might range in their complexity from the purely administrative, managing appointments or repeat prescriptions, to sensor technologies that monitor patient vital signs for chronic or acute issues, through to real-time remote diagnosis and involvement of medical professionals remotely delivering health services (Kos, Sedlar, & Pustisek, Citation2016; Peeters et al., Citation2016). Many drivers underpins eHealth’s growth, which may improve the quality of delivery, patient outcomes and safety, whilst also reducing cost. eHealth also increases the capacity of patients with chronic conditions to self-manage their conditions (Dimitrova, Citation2013; Horn et al., Citation2016; Peeters et al., Citation2016). Demographic ageing makes eHealth particularly attractive, a way of achieving two goals simultaneously, ensuring that elderly patients receive the care they expect whilst simultaneously ensuring that the costs associated with providing that care do not rise exponentially. eHealth has the potential to bundle social care provision with medical services and through coordinating service delivery to therefore reduce the overall cost of provision.
Health policy makers enthusiastic have been about eHealth’s to transform healthcare (Dimitrova, Citation2013). But at the same time it is notable that that policy-maker enthusiasm has not been matched by the rate at which it has been taken up in primary healthcare. Developing eHealth products is extremely complex because the business of providing healthcare is also very complex, requiring coordination between many providers to intervene around a single patient (Dimitrova, Citation2013; Horn et al., Citation2016). Although eHealth promises to facilitate patient-centred coordination, in practice ensuring that eHealth systems allow the right professionals to be aware of patient needs in a timely way to coordinate with other providers is a conundrum. This partly relates to the fact that complex healthcare is not merely a relationship between patient and providers, but also between other informal care providers such as family members and friends. Those uncomfortable with their new roles and framings that eHealth brings have been resistant; general practitioners may resent the technological upgrading and the need for infrastructures and skills that are incidental to what they see as their vocation (Peeters et al., Citation2016), whilst patients groups have resisted the loss of privacy and the need for often vulnerable patients to take their own responsibility for maintaining their own health (Oudshoorn, Citation2011).
4.2. Dutch healthcare system
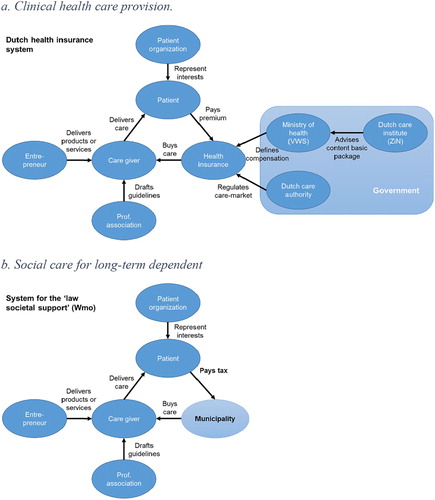
In 2006, the Dutch healthcare system was liberalized from a mix of single-payer and health insurance to a purely health insurance-based system. Health insurance is compulsory; every resident is required to purchase a basic package; this covers essential services, and the level of basic coverage provided is set in a negotiation between the Ministry of Public Health, Welfare and Sport, and the Dutch Care Institute. Individual residents may also purchase additional insurance for dental, physiotherapy and health services, and vary the level of their own contributions (see (a)). Social care for elderly citizens is covered by a separate system which underwent a substantial reform (involving 40% budget cuts) in 2014 (Janssen, Citation2014). Social care covers the modifications that are required to allow elderly people to live at home independently, and may include home help, medical devices, domestic technologies and rehabilitation services. A key principle of this reform is of self-reliance: care users are expected to receive care from friends and family, and only where that care is not available will the municipality make an assessment and release funds. This makes carers (‘mantelzorgers’) a key stakeholder in the delivery of care services (see (b)).
Figure 1. An overview of the parallel policy systems around Dutch health care. Source: Authors’ own design.
4.3 The two case studies and their ‘regional’ contexts
We present examples of two innovation networks relating respectively to synthetic and analytic innovation networks; we have pseudonymized the two cases as CareConnect (synthetic) and Personalized Pooled Care (analytic). More information is provided on these two cases below (See also Konrad et al., Citationin press). Both of the cases are located in Overijssel, a Province in the east of the Netherlands, relatively poor in the Dutch context, and is not a main national growth centre. Since the 1990s, the Province has sought to promote regional economic development through innovation, and since the 2000s has included health care technologies as eligible for public subsidy support.
The first case is CareConnect (CC), an online communication platform that creates a network around the client or patient, and between caregivers, family members and caretakers (more detailed information is provided in Konrad, Schulze Greiving, & Benneworth, Citationin press). CC emerged out of the changes to Dutch care rules outlined above; funding fewer elderly care home places forced a care home in one village in Overijssel to close. Care providers came together to provide continuity of health care in patients own homes via a platform to support elderly and people with chronic diseases who need regular help and care to be able to live at home for a longer period. Participating stakeholders includes pharmacies, homecare, physiotherapists, hospitals, general practitioners and the municipality. CC provides a secure online system where patients and carers can pose questions sent to other parties in the network, allowing a rapid response time. Typical messages sent via CC are updates on medication used, pharmacy orders or questions about care. This way, the involved parties remain simultaneously apprised of the patient’s and interventions made by other actors, with the overall aim to increase the quality and efficiency of the care provided to that patient.
The second case is Personalized Pooled Care (PPC), an eHealth product originating from the European Commission funded project ‘CareMonitor’ (CM) supporting active and healthy ageing and independent living, in which the Twente partner played a leading role. The platform mainly targets elderly people and other patients with chronic diseases, specifically COPD (Chronic Obstructive Pulmonary Disease) and MCI (Mild Cognitive Impairment or incipient dementia). The Overijssel work was undertaken by a hospital in Twente, in the east of the region, focusing on the COPD elements of the system, in which they had experience because of their above average incidence of and mortality from COPD (Volksgezondheidzorg, Citation2018). The product consists of a sensing environment, for example the home of the patient, which collects various data regarding the user and environment via medical and environmental sensors, with environmental control provided via actuators. Patients can directly interact with the environment by using audio/video devices and sensors; the sensing environment monitors patients’ daily activity and medical condition (e.g. pulse, oxygen saturation etc.) their sleeping patterns and the quality of the sleep. The environment is designed to motivate patients to reach their daily fitness goal, containing educational and cognitive gaming, and a calendar with reminders for daily medication and meals. Domotics are used to control the home environment. Recorded data is processed and stored in a pooled data sharing service, with doctors, family members, care recipients able to access these data in various configurations.
5. The regionality of the innovation networks
The first step of the analysis was to consider the extent to which the innovation activities constituted a regional network, and the contacts that this gave to societal partners in ways that created resources that could support these responsibility repertoires. CareConnect emerged from an existing set of practices between connected partners, originally centred around a General Practice and a care home for elderly patients. This existing local practice network was transformed into an innovation network in response to wider changes in the health system, and achieved a degree of regionality when it attracted the support from the province as a potential model for cutting home care costs in the east of the Netherlands. It is possible to see regional culture reflected in the CareConnect idea: Twente is a region that has a high degree of self-organization (Beugelsdijk & van Schaik, Citation2005) and social capital, preserved to this day in terms of the sense of ‘noaberschap’ in which people take immediate responsibility for one another (Vedder, Citation2014). That had a clear impact on the ways in which the locals wanted to implement the WMO reforms and the closure of the care home, to not simply leave people to their own devices but to ensure that care was provided effectively and socially (Versluis, Citation2017). This in turn shaped the decision space within which CC wanted to operate, and which they had to exert agency given the massive funding cuts they faced.
PPC began as an international R&D network with a node in Twente because of a local rehabilitation hospital’s expertise, derived from very strong existing patient networks, which whilst not related to innovation created a knowledge resource that helped to solve the impersonality of the overall innovation process. It is likewise possible to see the region reflected in PPC’s institutional context, where the rehabilitation hospital was created as a national facility for Dutch military action in Indonesia but was located in Twente, a region with a high level of industrialization in rather physically intense and unhealthy industry (textiles). The hospital shifted to dealing with industrial disease, PPC was dealing with industrial diseases – COPD in particular – that have a much higher prevalence than in other parts of the country. Therefore the hospital’s interests became enmeshed in the question of providing good treatment for industrial disease sufferers, precisely because that is what it meant to be (amongst other things) a rehabilitation hospital in Twente. Rehabilitation meant dealing with at least in part the conditions of industrial disease, not just caused by the working conditions but also the working class lifestyles (more generally unhealthy) that were associated with them that led to conditions like COPD. More information on these two networks is provided below.
5.1. Regional innovation networks rooted in synthetic knowledge – CareConnect
The CareConnect innovation project involved the care providers from the patients previously served in the care home, and in particular a local health care practice who had close contact with their clients and previously had coordinated amongst themselves and with carers’ relatives when providing care to residents. They came together to develop a digital communications platform to replace the coordination and oversight that had previously been provided through informal exchanges in the Health Center between GPs, nurses, physiotherapists and a pharmacy. A foundation CareConnect was provided to oversee the development of a communications platform, and that Foundation received several small subsidies to help with establishing the platform. The software was sourced from a company whose founder had had a disabled daughter and who was inspired by his own situation to develop a technology platform to help deal with the coordination problem that he had heard of from others in his wider peer network. The software was launched then adapted in response to user feedback, before being upscaled and sold to customers elsewhere facing similar situations.
The innovation was notionally led by the Foundation CareConnect, but the purpose of the Foundation was to develop a service for the lead users, the GPs and the nursing service. Funding to help develop the service was provided by the municipality (out of their care fund) and the Province (as an innovation subsidy). Outside of the region, the insurance companies played a very important role in setting the rules for the kinds of services which were eligible for reimbursement. The challenge in constructing an effective innovation network was in ensuring the platform reflected the interests of carers and patients were visible in parallel with meeting the technical and professional needs of doctors and nurses. The practitioner network appeared to be initially focused on addressing interaction between GPs and nurses, each with their own differently organized approaches; both professionalized groups were much better structured than the carers, and there was evidence related in the interviews that this led to less consideration for carers’ needs. Both groups certainly talked in ways that recognized the services that carers provided to patients, but also were seen as a potential source of interference in care provision. The Foundation therefore chose to pay particular to ensuring that the interests of the patients and carers were visible in the overall innovation process.
5.2. Regional innovation networks rooted in analytic knowledge – personalized pooled care
The PPC product emerged from a European Framework project (CareMonitor) a cross-European consortium involving partners with prior experience of co-operation and expertise in developing technologies for chronic sickness management. The regional partner was a regional hospital created in 1948 specifically for the rehabilitation of troops injured in decolonization actions in what is today Indonesia, that has subsequently developed as a leading centre of expertise and excellence in rehabilitation (see Benneworth & Hospers, Citation2007) for more information. The Twente hospital partner assumed the responsibility for the work package on Chronic Obstructive Pulmonary Disorder (COPD), a life-limiting lung disease associated with exposure to airborne particulates (such as in industry or from smoking, both activities with historically above average incidence in Twente). The Twente team drew on existing links with COPD patients to develop a comprehensive intervention system to support COPD patients, including monitoring physical signals and sleep, providing stimuli for activity, coaching behaviour and communicating with care providers. The company PPC was founded at the end of the process in Belgium to try to raise capital to commercialize the platform, which was applicable to COPD, mild cognitive impairment (early stage dementia) and Age Related Impairment.
Innovators drew upon the regional innovation network in various ways during the innovation process. During proof of concept, the hospital developed a set of patient profiles based on their existing knowledge of COPD patients in Twente, and used those to develop a set of use scenarios for a platform. Although focus groups were held to create a product specification for a visual interface, they were held in in Denmark, Italy and Austria, not Twente. The hospital were responsible for developing the visual interface and after negative feedback from the four countries (including the Netherlands) a local visual designer was hired to create an attractive front end. This prototype was then tested with 28 COPD patients in Twente, drawing on their existing contact networks. These patients used the system for 4 weeks at home, to provide data on which elements of the system were used; the trials were too short to meaningfully develop data on the efficacy. Once the decision was taken to upscale via a spin-out company then the regional user influence largely disappeared as the company was created in Brussels. Even though the hospital were involved in the upscaling project, and the Twente scientist was part of the newly formed company, the commercialization focused on rewriting the software to improve functionality and convert it to a smartphone application. From this point, regional innovation networks were not evident in the innovation process.
6. Responsibility within regional innovation networks
The second analytic step was to stylize the loci of responsibility repertoires (or their absence) within these regional innovation networks. In both the cases, the pre-existing networks formed the basis for shaping reflection, and therefore can be regarded as providing a resource that stimulated RRI. However, the use of these existing networks brought a hybridity to them: by ‘hybridity’ here we mean that there were two very distinct sub-networks with their own logics evident in the innovation network. One sub-network was a ‘knowledge’ network that was primarily related to the technicalities of the innovation, whilst the other was a ‘service’ network specifically focused on providing care within legal requirements and ethical norms to extremely vulnerable patents. This hybridity created tensions within the networks that also in turn created tensions around the delivery of RRI, and it was notable that in both cases, the innovation subnetworks only really involved the care networks in a meaningful way in response to pressure from actors in their innovation networks outwith their regional networks. These findings are summarized in below, and more information is provided on these repertoires and their regionality thereafter.
Table 2 . The dynamics of regional Responsible Research and Innovation repertoires in synthetic and analytic innovation networks.
6.1. Responsibility repertoires drawing on synthetic knowledge bases – CareConnect
In the case of CareConnect, it is possible to consider the extent to which this innovation was responsible, reflecting the initially proposed framework. The innovators themselves were very busy with trying to solve an immediate urgent problem to anticipate long-term trends; it was only the health insurance companies who were attempting to find solutions to rising health costs that anticipated these changes. In terms of reflection, the patients were not the most important users of the innovation, and it was only through a degree of self-awareness of the care providers that allowed them to ensure that efforts were made to ensure that the innovation delivered against patient needs. Inclusion was provided by the existing informal micro-networks by which care providers and carers intervened to support individual patients; there was no effort to widen this to include patients unlike those in the existing cohort, something quite important considering the relative homogeneity of the patient group. In terms of responsiveness, there were relatively few opportunities to allow patients to shape innovation; what responsiveness there was, was second order, with care providers practices shaping the innovation (they should also be primarily focusing on patients). The Foundation put considerable effort into ensuring that the client rather than providers were central to the innovation process, which had a divergent effect, encouraging the focus on one single user group rather than suppliers but at the same time reducing the idea of ‘publics’ to a generic version of those patients currently being served by CC.
In terms of the extent to which the ‘regionality’ was visible in these responsibility repertoires, the innovation took place in a village in the rural part of a peripheral region, with a high degree of resident homogeneity and high personal contact and continuity in health services (in contrast to policlinics in the West of the Netherlands). This influenced the ways in which ‘societal’ interests emerged as influential or not in these networks. Firstly, the innovation sought to reproduce an informal network as a technological intervention, and therefore the regionality is highly evident in the efforts to foreground the patients (rather than care providers) as the users for the technology, with these local networks influencing reflection practices, foregrounding patients. At the same time, this homogeneity undermined the inclusion practices, because they reduced the idea of ‘patients’ to those patients currently benefiting from CC’s platform, rather than those that might later be able to benefit from the CC platform something not immediately applicable once the technology started to travel. However, one interviewee reported that it was more an unwillingness to adopt a technology from the East of the Netherlands (perceived as ‘backwards’), than its specificity to the residents of the east of the Netherlands, that was a barrier for its adoption in the Netherlands’ urban core. Thirdly, it was necessary to construct a new body (the Foundation) to ensure a degree of (second-order) responsiveness, highlighting the extent to which a formal governance ‘fix’ (a foundation) was required in order to provide what is often assumed to take place automatically through informal emergent scientific governance practices. Finally, the clear power imbalance to determine the rules of the game led to regional partners being reactive to external circumstances; the emergent effect of this was that the power of anticipation was framed by health insurers. Outside of this project, they have been criticized in Netherlands for prioritizing cost reduction over patients’ needs but at the same time, they were also willing to engage with and discuss their customers’ (patients) needs with the innovators.
6.2. Responsibility repertoires drawing on analytic knowledge bases – personal pooled care
In terms of the responsibility repertoires relating to PPC, anticipation of user interests was included primarily through the creation of personas, scenarios and user cases, from literature and from prior experience with patients, after the funding was in place; the choice of project was primarily led by technological opportunity. In terms of reflection, it took an intervention from the European Commission mid-term review to ensure that users were consulted around the interface; prior to that there was relatively little reflection beyond the project team. Inclusion in the project was extremely pragmatic, with those users being included and represented in various ways based on their past acquaintance with the researchers, giving it sometimes an ad hoc nature, although views and interests were heard in various ways of patients but also of care providers. The responsiveness of the innovation process was limited by the fact that by the time that users were actively consulted (in the interface development) there was relatively little space to adapt the interface to user needs; the complexity of the innovation process made it hard to include user voices in the overall project development.
In terms of the regionality of these repertoires, we here highlight four dimensions, reflecting that providing attention for a common local disease and using local knowledge created a hybridity in linking innovation networks with patient networks, something with which not all patients were comfortable. First, in developing the COPD protocols, the hospital drew on its prior knowledge of COPD and this clearly reflected the fact the preponderance of COPD cases regionally (although the hospital’s patients were drawn more widely than just the Twente region alone). Second, regional actors provided preference data from the 28 installed prototypes, in terms of revealing which of the applications were more or less popular, and also the feedback from the users and their carers on the interface.
Third, regional agency was not actively visible in the initial approach, and it took the intercession from the European Commission for them to take the user interface back to users, giving the network a hybrid patient-innovation characteristic. The user data from the testing treated the users as subjects and whilst it might have reflected some degree of regional preference, was strongly shaped by the technological decisions. Fourth was the uncomfortable fit of the two roles expected of users within these hybrid networks, as vulnerable patients struggling with an emotionally burdening condition, and as representatives of societal interests in the innovation process. This left the regional ‘societal interest’ evident and present although strongly framed and conditioned by the overall setup of the project; there was no strong user-producer network able to influence spin-off strongly shaped by scientific network’s international governance.
7. Discussion and conclusions
In this paper we sought to address the question of how knowledge bases within regional innovation systems affect the ways in which responsible practices can become embedded in innovation trajectories. We have identified in both cases that the regional innovation networks were dependent upon the ways that the pre-existing service networks were coupled to these regional knowledge networks. It appears that the strength of the coupling of those users to the innovation networks as a consequence of the transformation from practice into innovation network affected the scope for responsibility repertoires within these regional innovation networks. This relationship between service networks to innovation interests defines the space available for user interests to play a substantive role in these emergent governance networks, and therefore our findings suggest that this coupling between these two sub-networks plays a substantive role in defining the space available for regional partners to enact responsibility repertoires.
Our first finding was thus that an important driver in shaping responsibility was the dependence of innovation networks on prior practice/ service networks, whether directly as in providing first order users for the innovation prior to upscaling (CC) or indirectly by providing knowledge bases from which to develop interventions (PPC). The regionality of these networks was defined by the ‘coupling’ between health care providers and their patients around innovation activities, beyond straightforward ‘user-producer’ relationships. The innovation networks depended in various ways on relationships of care from medical staff to vulnerable patients, and this clearly influenced the responsibility. In both cases, this brought the duty to the patients into innovation considerations, boosting reflection and responsiveness, but at the same time limiting inclusion to the existing patient group to whom there was this duty.
The first visible distinction between the two knowledge bases comes in the strength of the coupling of the patients to the innovation network. In the synthetic knowledge base network, the patients were ‘strongly coupled’ to the innovation network because their interests were paramount, increasing responsiveness and anticipation by knowledge creators. Even if the view of ‘patients’ was limited to the immediate user group of the platform, the overarching concern was in ‘what worked’ for patients. Conversely, in the analytic knowledge base system the patients were a means to an end, and the hybridity was more uncomfortable, requiring more intermediation and negotiation. Innovators were primarily concerned with harvesting the knowledge of patients for inclusion in their research process, even if in their other relationships with these patients they were concerned with their health and rehabilitation.
This coupling property also affected inclusion practices, with stronger coupling being associated in our two cases with weaker inclusion and reflection. In the strongly-coupled (synthetic) case, we see prospective reflectiveness and inclusion were restricted to the immediate patient circle of the care home. The homogeneity of that patient group shaped the ways that innovators reflected on the impacts of their innovations and precluded extending considerations of user needs to other more diverse societal groups. In the weakly coupled (analytic) case, we see that this lack of coupling facilitated these processes; the reflection process was deliberately synoptic, defining particular kinds of potential user scenarios as the basis for defining the product specification. This ensured it was not tightly coupled to the needs of regional patients, indeed to the point where this lack of coupling was raised as becoming a weak point because of this lack of responsiveness highlighted above.
These case studies suggest that responsibility within regional innovation networks appears related to the underling practice networks which couple users to innovators, and the strength of that coupling. Coupling appears of itself to be advantageous in providing pathways for user signals to be received and incorporated in these emergent regional innovation governance networks. Strong coupling appears to be associated with improving responsiveness whilst reducing inclusion and reflectiveness; weak coupling appears to be associated with stronger anticipation and reflection but correspondingly weaker responsiveness. This provides a potentially interesting model for further exploration of responsibility within regional innovation systems, because there is clearly the scope for policy-makers to stimulate innovation in ways that irrespective of the underlying knowledge bases stimulates particular kinds of coupling.
We have not in this paper been able to consider symbolic knowledge bases, and we see this as one potential fruitful avenue for further research, particularly given recent controversies about cultural appropriation and artwashing (cf. Pritchard, Citation2017). There is a tendency to treat symbolic knowledge as the raw material for cultural production and consumption without due consideration of the extent to which this is societally desirable (Asheim, Grillitsch, & Trippl, Citation2017). That has the effect of framing the individual as a consumer of that knowledge rather than as a co-owner and co-producer, whilst residents are arguably far more involved in the production of local symbolic knowledge resources than they are with either analytic or synthetic knowledge resources (Brennan, Flint, & Luloff, Citation2009). More consideration is required for the mechanisms by which symbolic knowledge-based innovations are coupled with regional communities and the ways in which these regional cultures, norms and values find expression within symbolic innovation processes.
We acknowledge that this as a relatively small scale exploratory study which sought to explore responsibility repertoires in regional innovation networks in a stylized way and in particular to explore the role of place in RRI. Therefore in the context of this special issue, we acknowledge we should be modest in making more general claims about the nature of responsibility within regional innovation networks and systems. At the same time, this issue of coupling does come some way to identifying a potential mechanism by which geography considerations can be included within RRI, namely to ensure that these informal regional collectivities are included within processes seeking to build responsibility, and not just simply a default to engaging individuals within a region as being in some way able to articulate this collectiveness.
More generally, this helps to reinforce the idea of RRI and in particular its placelessness and resistance to being pinned down to place-specific ideas of society. This suggests for innovation to be responsible, it has to be coupled with informal collectivities at the scale of the space across which it might operate, be they local, regional, national, European or indeed global. And indeed, it is this understanding of these informal collectivities and they ways they can be coupled to innovation activities in ways that allows the collectivities to play meaningful roles in decision making that essential to realize a truly responsible approach to research and innovation that can harness the undoubted potential of technology to realize better societal futures.
Acknowledgements
Many thanks are also due to the interviewees in Overijssel who made their time available for the research. Many thanks are also due to the guest editors and two anonymous referees for their thoughtful and provocative response to the original version of the manuscript. The author would also like to record their thanks to Joost Kuipers of the Province of Overijssel for empirical and financial support. Any errors or omissions remain of course the authors’ responsibility.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Paul Benneworth http://orcid.org/0000-0003-0539-235X
Additional information
Funding
Related Research Data
References
- Adam, F., & Westlund, H. (Eds.). (2013). Innovation in socio-cultural context. London: Routledge.
- Amin, A., & Roberts, J. (2008). Knowing in action: Beyond communities of practice. Research Policy, 37(2), 353–369. doi: 10.1016/j.respol.2007.11.003
- Asheim, B. (2012). The changing role of learning regions in the globalizing knowledge economy: A theoretical re-examination. Regional Studies, 46(8), 993–1004. doi: 10.1080/00343404.2011.607805
- Asheim, B., Grillitsch, M., & Trippl, M. (2017). Introduction: Combinatorial knowledge bases, regional innovation, and development dynamics. Economic Geography, 90(5), 429–435.
- Asheim, B. T., & Coenen, L. (2005). Knowledge bases and regional innovation systems: Comparing Nordic clusters. Research Policy, 34(8), 1173–1190. doi: 10.1016/j.respol.2005.03.013
- Asheim, B. T., & Coenen, L. (2006). Contextualising regional innovation systems in a globalising learning economy: On knowledge bases and institutional Frameworks. The Journal of Technology Transfer, 31(1), 163–173. doi: 10.1007/s10961-005-5028-0
- Benneworth, P., & Hospers, G. J. (2007). The new economic geography of old industrial regions: Universities as global – local pipelines. Environment and Planning C: Government and Policy, 25(6), 779–802. doi: 10.1068/c0620
- Benneworth, P., & Pinheiro, R. (2017). Regional upgrading in the periphery: A view from the ‘rich’ Northern European cousins. In M. Fonseca & U. Fratesi (Eds.), Regional Upgrading in Southern Europe: Spatial dimensions and human capital (pp. 299–321). Dordrecht: Springer Verlag.
- Benneworth, P., Pinheiro, S. R., & Karlsen, J. (2017). Strategic agency and institutional change: Investigating the role of universities in regional innovation systems (RISs). Regional Studies, 51(2), 235–248. doi: 10.1080/00343404.2016.1215599
- Beugelsdijk, S., & van Schaik, T. (2005). Social capital and growth in European regions: An empirical test. European Journal of Political Economy, 21(2), 301–324. doi: 10.1016/j.ejpoleco.2004.07.004
- Bozeman, B. (2002). Public-value failure: When efficient markets may not do. Public Administration Review, 62(2), 145–161. doi: 10.1111/0033-3352.00165
- Brennan, M. A., Flint, C. G., & Luloff, A. E. (2009). Bringing together local culture and rural development: Findings from Ireland, Pennsylvania and Alaska. Sociologia Ruralis, 49(1), 97–112. doi: 10.1111/j.1467-9523.2008.00471.x
- Cooke, P. (2005). Regionally asymmetric knowledge capabilities and open innovation: Exploring ‘globalisation 2’ – a new model of industry organisation. Research Policy, 34, 1128–1149. doi: 10.1016/j.respol.2004.12.005
- Dimitrova, R. (2013). Growth in the intersection of eHealth and active and healthy ageing. Technology and Health Care, 21(2), 169–172. doi: 10.3233/THC-130727
- Fitjar, R. D., Benneworth, P. S., & Asheim, B. T. (2019). Towards regional responsible research and innovation? Integrating RRI and RIS3 in European innovation policy. Science and Public Policy. doi:10.1093/scipol/scz029
- Genus, A., & Iskandarova, M. (2018). Responsible innovation: Its institutionalisation and a critique. Technological Forecasting and Social Change, 128, 1–9. doi: 10.1016/j.techfore.2017.09.029
- Gibbons, M. (2000). Mode 2 society and the emergence of context-sensitive science. Science and Public Policy, 27(3), 159–163. doi: 10.3152/147154300781782011
- Gläser, J. (2012). How does governance change research content? On the possibility of a sociological middle-range theory linking science policy studies to the sociology of scientific knowledge. The Technical University Technology Studies Working Paper series, TUTS-WP-1-2012.
- Haas, P. M. (1992). Epistemic communities and international policy coordination. International Organization, 46(1), 1–35. Winter. MIT Press, doi: 10.1017/S0020818300001442
- Hollands, R. G. (2008). Will the real smart city please stand up? Intelligent, progressive or entrepreneurial? City, 12(3), 303–320. doi: 10.1080/13604810802479126
- Horn, G., et al. (2016). An architecture for using commodity devices and smart phones in health systems. In 2016 IEEE Symposium on Computers and Communication (ISCC).
- Isaksen, A., & Karlsen, J. (2010). Different modes of innovation and the challenge of connecting universities and industry: Case studies of two regional industries in Norway. European Planning Studies, 18(12), 1993–2008. doi: 10.1080/09654313.2010.516523
- Janssen, R., Innovatieroutes in de zorg. 2014, Zorg voor innoveren: netwerkbijeenkomst ‘decentraliseren=innoveren’, Utrecht.
- Kitcher, P. (2001). Science, truth and democracy. Oxford: Oxford University Press.
- Kogan, M. (2005). Modes of knowledge and patterns of power. Higher Education, 49(1-2), 9–30. doi: 10.1007/s10734-004-2911-9
- Kogler, D. F. (2015). Editorial: Evolutionary economic geography – theoretical and empirical progress. Regional Studies, 49(5), 705–711. doi: 10.1080/00343404.2015.1033178
- Konrad, K., Schulze Greiving, V., & Benneworth, P. S. (in press). The role of user-led regional innovation networks in shaping responsible innovation in eHealth: Lessons from the East of the Netherlands. In T. Iakovleva, L. Foss, & J. Bessant (Eds.), Responsible innovation in the e-health sector. Cheltenham: Edward Elgar.
- Kos, A., Sedlar, U., & Pustisek, M. (2016). Research and innovation in ICT with examples in the field of eHealth and wellbeing. In S. Loshkovska & S. Koceski (Eds.), ICT innovations 2015: Emerging technologies for better living (pp. 1–10). Berlin: Springer-Verlag Berlin.
- Lawson, C., & Lorenz, E. (1999). Collective learning, tacit knowledge and regional innovative capacity. Regional Studies, 33(4), 305–317. doi: 10.1080/713693555
- Liu, J., Chaminade, C., & Asheim, B. (2013). The geography and structure of global innovation networks: A knowledge base perspective. European Planning Studies, 21(9), 1456–1473. doi: 10.1080/09654313.2012.755842
- Oudshoorn, N. (2011). Telecare technology and the transformation of health care. Health, technology and society, ed. A. Webster Hampshire: Palgrave MacMillan.
- Owen, R., Macnaghten, P., & Stilgoe, J. (2012). Responsible Research and innovation: From science in society to science for society, with society. Science and Public Policy, 39, 751–760. doi: 10.1093/scipol/scs093
- Paasi, A. (2013). Regional planning and the mobilization of ‘regional identity’: From bounded spaces to relational complexity. regional Studies, 47(8), 1206–1219. doi: 10.1080/00343404.2012.661410
- Peeters, J. M., et al. (2016). Use and uptake of eHealth in general practice: A cross-sectional survey and focus group study among health care users and general practitioners. JMIR Medical Informatics, 4(2), e11. doi: 10.2196/medinform.4515
- Pritchard, S. (2017). ‘Art washing: Social capital & anti-gentrification activism. In Colouring-in culture. Retrieved from http://colouringinculture.org/blog/artwashingsocialcapitalantigentrification
- Ribeiro, B., Bengtsson, L., Benneworth, P., Bührer, S., Castro-Martínez, E., Hansen, M., … Shapira, P. (2018). Introducing the dilemma of societal alignment for inclusive and responsible research and innovation. Journal of Responsible Innovation, 5(3), 316–331. doi: 10.1080/23299460.2018.1495033
- Roberts, J. (2014). Community and the dynamics of spatially distributed knowledge production: The case of Wikipedia. In R. Rutten, P. Benneworth, D. Irawati, & F. Boekema (Eds.), The social dynamics of innovation networks (pp. 179–200). London: Routledge.
- Sotarauta, M. (2016). An actor-centric bottom-up view of institutions: Combinatorial knowledge dynamics through the eyes of institutional entrepreneurs and institutional navigators. Environment and Planning C: Government and Policy, 1–16. doi: 10.1177/0263774X16664906
- Stilgoe, J., Owen, R., & Macnaghten, P. (2013). Developing a framework for responsible innovation. Research Policy, 42(9), 1568–1580. doi: 10.1016/j.respol.2013.05.008
- Temple, J. (1998). The new growth evidence. Journal of Economic Literature, 37(1), 112–156.
- Trippl, M. (2011). Regional innovation systems and knowledge-sourcing activities in traditional industries—evidence from the Vienna food sector. Environment and Planning A, 43(7), 1599–1616. doi: 10.1068/a4416
- Vedder, H. H. (2014). Good neighbourliness in a sustainable European internal electricity market: A tale of communities and uncommunautaire thinking. Available at SSRN 2589022.
- Versluis, P. (2017). Wie zorgt voor onze ouderen in landelijke gebieden? Interview Aanjagers Nederland Zorgt Voor Elkaar. Sociaal Bestek, 79(5), 59–61.
- Volksgezondheidzorg. (2018). COPD: Regionaal. Retrieved from https://www.volksgezondheidenzorg.info/onderwerp/copd/regionaal-internationaal/regionaal
- Von Schomberg, R. (2011). Towards responsible research and innovation in the information and communication technologies and security technologies Fields. Brussels: European Commission, Directorate General for Research and Innovation.
- Walhout, B., Walhout, B., Kuhlmann, S., Ordonez Matamoros, H. G., & Edler, J. (2016). Res-AGorA concepts and approach. In R. Lindner, S. Kuhlmann, S. Randles, B. Bedsted, G. Gorgoni, E. Griessler, A. Loconto, … N. Mejlgaard (Eds.), Navigating towards shared responsibility in research and innovation: Approach, process and results of the Res-AGorA Project (pp. 46–53). Karlsruhe: Fraunhofer ISI.
- Yeung, H. W. (2009). Situating regional development in the competitive dynamics of global production networks: An East Asian perspective. In H. W. Yeung (Ed.), Globalizing regional development in east Asia: Production networks, clusters, and entrepreneurship (pp. 5–30). London: Routledge.
- Uyarra, E., Flanagan, K., Magro, E., Wilson, J., & Sotarauta, M. (2017). Understanding regional innovation policy dynamics: Actors, agency and learning. Environment and Planning C: Politics and Space, 35(4), 559–568.