
Abstract
To test the validity of a modified Trier Social Stress Test (TSST) for studying stress reactivity in sexual minority women. Two hundred seventy-four female participants (66.4% Black American), half of whom identified as lesbian/gay or bisexual and half as heterosexual, completed the TSST with instructions to describe an experience of discrimination. Cortisol levels and negative emotion scores increased, and heart rate variability decreased in response to the TSST, and the magnitude of these responses varied as a function of sexual orientation and race. Women who discussed sexual orientation as a source of discrimination had greater increases in cortisol and negative mood following the TSST. The modified instructions did not compromise the validity of the TSST. Prompting participants to discuss specific sources of discrimination may be a useful adaptation of the TSST in studying minority stress reactivity.
The goal of the present study was to adapt a widely used measure of stress reactivity to study the impact of experiences with discrimination on biological systems involved in regulating the stress response. The modification included asking women to discuss a time when they had been treated unfairly and to describe how they responded to that experience. The magnitude of response to the task varied as a function of sexual orientation and race, and the topics discussed, demonstrating usefulness of the modification for studying the impact of discrimination stress of physical health.
SUMMARY
Introduction
The impact of stress exposure on systems involved in maintaining health is well documented in correlational and experimental studies (Cavigelli & Caruso, Citation2015; Karlén et al., Citation2015; Matthews & Gallo, Citation2011). Members of minority groups (e.g. Black Americans, individuals living in poverty) are more likely than those from majority groups to experience stress, including discrimination stress, which in turn is associated with compromised health (e.g. Dowd et al., Citation2014; Slopen & Williams, Citation2014). The associations among minority status, stress exposure, and health are observed relatively early in life; discrimination and unfair treatment as a result of minority status are associated with health risks among adolescents and young adults, including higher ambulatory blood pressure (Beatty & Matthews, Citation2009; Diez Roux et al., Citation2002) and higher levels of C-reactive protein (CRP) (Lande et al., Citation2008). These results are highly useful for generating and testing hypotheses regarding mechanisms that may explain greater health risks among other minority populations including lesbian/gay and bisexual (LGB) women. Compared to heterosexual women, sexual minority women report greater exposure to stressful life events and to discrimination-related life events (Meyer et al., Citation2008). Furthermore, self-report data indicate that experiences of discrimination are associated with poor health among LGB females (Lehavot & Simoni, Citation2011). Moreover, differences in self-reported health between LGB and heterosexual women are partly attributable to levels of distress (Cochran & Mays, Citation2007). Thus, the theoretical and empirical support for testing the mechanistic role of stress exposure in the development of health disparities for sexual minority women is strong.
Prior studies on potential biological markers linking sexual minority stress to health outcomes are limited. A recent systematic review indicated that less than half of studies found differences between sexual minorities and heterosexuals on biological outcomes and recommended further research focused on improving methodology and replicability (Flentje et al., Citation2020). In two studies, tests of between-group differences in diurnal cortisol revealed no significant effect of sexual minority status (Austin et al., Citation2016; Juster et al., Citation2013). In the Growing Up Today Study, sexual minority women had higher levels of diurnal salivary alpha-amylase, an indicator of sympathetic nervous system regulation, than heterosexual women; there were no differences by sexual minority status among men (Austin et al., Citation2018). In the nationally representative Add Health Study, sexual minority men had higher levels of CRP than heterosexual men, whereas sexual minority women had lower levels of CRP than heterosexual women. In a study of diurnal cortisol variation in Black and White gay and bisexual men, Black men had higher evening cortisol and larger differences between peak and lowest cortisol levels (Cook et al., Citation2017). However, few studies have explored whether actual stress reactivity differs across sexual minority stress in large, diverse samples.
To date, only two studies have examined biomarkers of stress reactivity among sexual minority participants, only one of which had a heterosexual comparison group. These studies used modified versions of the Trier Social Stress Test (TSST) (Kirschbaum et al., Citation1992). The TSST is the most widely used laboratory-based social evaluative stressor and, in several studies, instructions have been modified to increase the salience of the evaluation context. One study of 74 LGB young adults examined HPA-axis reactivity in response to a modified TSST in which participants discussed an experience in which they experienced rejection based on their sexual orientation (Hatzenbuehler & McLaughlin, Citation2014). Cortisol levels were inversely related to structural stigma in the states in which participants lived during adolescence. In another study, a convenience sample of 87 Montreal residents completed a modified TSST in which participants delivered a mock job interview speech to judges seated behind a one-way mirror (Juster et al., Citation2013). Differences by sexual minority status were found to vary by sex and type of biomarker. Among men, sexual minority status was associated with lower overall cortisol levels and higher overall heart rate, but no difference in testosterone or progesterone. Among women, sexual minority status was associated with higher post-TSST cortisol, testosterone, and progesterone levels but not heart rate (Juster et al., Citation2015, Citation2016, Citation2019). Although, the sample was primarily white (70%), strengths of the study include multimodal assessment of stress reactivity and use of a heterosexual comparison group.
Taken together, these preliminary studies provide evidence that sexual minority populations likely differ from heterosexuals in stress reactivity. Methodological innovation in sampling, stress exposure, and measurement are crucial. Most prior studies have utilized relatively small convenience samples. Studies of participants drawn from representative samples have the potential to yield more robust findings in between-group differences. Further, salience of sexual minority identity may affect response to identity-specific stressors (e.g. a sexual orientation-specific TSST), particularly among sexual minorities who may experience other sources of stigma due to gender and racial/ethnic minority status (Meyer, Citation2015). As part of a developing program of research on health disparities in sexual minority women that is inclusive of other potential intersecting identities, we used a modified version of the TSST to measure reactivity to being evaluated while describing an experience of being treated unfairly. In the present study, we test the validity of the modified instruction to describe an experience of discrimination by examining whether typical patterns of stress reactivity, defined as increases in cortisol levels and negative mood and decreases in heart rate variability (HRV), were observed as a function of both sexual and racial minority status.
Methods
Participants
Participants in the present study were selected from the Pittsburgh Girls Study (PGS), a longitudinal, community-based study of girls residing in the city of Pittsburgh in 2000 (Keenan et al., Citation2010). At the time of enrollment, the girls were between the ages of 5 and 8 years. The Health, Emotions, and Adaptation over Time (HEArT) Study, is a substudy of the PGS, for which enrollment as a lesbian/gay or bisexual (LGB) participant was based on response to a single question about sexual orientation in wave 17 of the PGS (when girls were between the ages of 22 and 25 years). All participants who identified as LGB in wave 17 were invited to participate, and a random selection of participants who had identified as heterosexual in each year of assessment (waves 10–17) otherwise matched on frequency of race and age. Of those contacted for enrollment, 6.2% refused and 4.5% agreed but did not complete a visit.
Trier Social Stress Test
Instructions for the modified TSST (Buske-Kirschbaum et al., Citation1997) were as follows: the participant was asked to think about a time when she was treated unfairly due to race, sex, age, sexual orientation, or any other personal attribute, and to describe the situation, how she responded to it, and whether she felt she had been effective in handling it. Other aspects of the TSST followed standard procedures, including 5 min to prepare a speech, a 5-min speech, a 2-min mental arithmetic (i.e. serial subtraction) task, and then, a period of recovery. The shorter-than-typical mental arithmetic component likely had little effects on the strength of the response to the TSST. Prior studies indicate that stress response is highest during the first minute of a stressor and decreases thereafter (Jamieson et al., Citation2012; McLaughlin et al., Citation2015). Moreover, a meta-analysis of variations in TSST protocol indicated that completely excluding the mental arithmetic task had no effect on the magnitude of the stress response (Goodman et al., Citation2017).
Following informed consent procedures, a research assistant attached electrodes for collection of heart rate and then asked the participant to rest while watching an art video to acclimate to the laboratory. After 20 min of acclimation, the participant was shown to the TSST room, where two judges (one male and one female) sat at a table. The judges played taped instructions for the speech and arithmetic tasks, and then, asked the participant to leave the room. The research assistant accompanied the participant back to the acclimation room, and then, provided her with paper and pencil to prepare a speech describing a recent experience of discrimination. After 5 min, the research assistant accompanied the participant back to the TSST room, where the speaking judge asked her to begin her speech. The speech and arithmetic tasks were delivered in front of a video camera. The speaking judge was instructed to prompt the participant after 20 s of no response: “You still have time. Please continue.” If necessary, prompts continued every 20 s until the end of the 5-min speech period. The participant then returned to the acclimation room for a 60-min recovery period.
Research assistants who were not informed of participant sexual orientation coded the videotapes of the TSST for source of unfair treatment, including race, sexual identity, age, sex, physical attribute, education, income, and family status (e.g. single parent). These categories were not mutually exclusive, as participants could describe multiple sources of unfair treatment for a single event. The most common sources identified were race (46.4%), sex (42.6%), sexual orientation (14.1%), age (11.4%). About a quarter of LGB women described an experience with discrimination based on sexual orientation.
Salivary cortisol
Saliva samples for the assessment of cortisol were collected at 8 time points: 10, 5, and 0 min pre-TSST, and 20, 40, 50, and 60 min post-TSST. In order to control for the circadian rhythm of cortisol, the laboratory visit took place at approximately 2:00 pm. Saliva samples were collected using standard salivettes and were stored in the laboratory at −80 °C until assayed. Samples were thawed, centrifuged at 3000 rpm for 10 min, and pipetted into test wells. All samples from each subject were assayed in the same batch to minimize variability and with reagents from the same lot. Samples were assayed in duplicate using the Salimetrics HS Salivary Cortisol EIA Kit for unbound cortisol. This assay has a lower limit of sensitivity from 0.007 to 1.2 ug/dL. The average inter-assay variance is 3.9% and 7.1%, and the average intra-assay variance is 6.7% and 6.9% for high and low concentrations, respectively.
Participants reported on waking time; whether they had napped that day; and consumption of oral medications, caffeine, nicotine, and any illicit substances in the past 12 h. None of these factors were associated with cortisol response to the TSST.
Heart rate variability
Participants were asked to clean the areas of skin where the electrodes would be placed with alcohol wipes. ECG data were collected via a MindWare mobile data collection device with a standard three-sensor configuration. ECG sensors were affixed (right and left clavicle and left lower rib) and leads from the mobile device were attached and fed underneath the participants’ clothes. Participants had been informed prior to arrival to wear loose-fitting clothing.
Heart rate was monitored continuously throughout the study visit. The digitalized ECG signals were examined in MindWare HRV 3.2.0, and detections of artifact R-wave occurrences corrected. HRV was measured from a continuous time series of inter-beat intervals measured using Mindware software. The root mean square of successive differences (RMSSD) in inter-beat intervals was used as a time-domain estimate of HRV. To examine changes in HRV across the protocol, mean RMSSD was generated for 8 separate epochs: the first and second 10 min prior to the stressor; 5 min of speech preparation; 7 min of stressor, including the speech delivery and mental arithmetic; and four 10-min periods during recovery. Inter-rater reliability for the editing of artifacts was established using 40 × 5 min epochs (10 per participant for 4 randomly selected participants). Coefficients of agreement across the primary HRV outcome measures ranged from 0.93 to 1.0.
Negative mood
Acute emotional responses to the task were assessed using the International Short Form of the Positive and Negative Affect Scale (PANAS) (Thompson, Citation2007). Originally developed by Watson et al. (Citation1988), this abbreviated 10-item version of the PANAS was developed for use with diverse populations by excluding items that were more difficult to define. Participants completed the PANAS at 8 time points: 10, 5, and 0 min pre-TSST, and 20, 40, 50, and 60 min post-TSST. The average alpha coefficient for the 5-item PANAS-Negative scale was 0.68.
Analytic plan
We compared reactivity and recovery of stress response among four groups: Black and White LGB and Black and White heterosexuals. Reactivity was defined as the change from pre-TSST to 20 min post- for cortisol and negative mood, and from the preparation period to the delivery of the speech and mental arithmetic for HRV. Recovery was defined as the change from 20 min post- to 40 min post-TSST for cortisol and negative mood, and from the TSST to 10 min post-TSST for HRV. In addition, we examined whether source of discrimination described during the TSST was associated with magnitude of reactivity and recovery. The data used for the present study are available on request from the corresponding author, [KK].
Results
Among the 150 LGB participants, 41 (27.3%) identified as lesbian or gay and 109 (72.7%) as bisexual. Race (65.6% Black American), age (mean = 24.2), wake time (mean = 8:09), and time of day of assessment (mean = 13:42) did not significantly vary across sexual orientation groups. Participants who identified as Native American, Multiracial, or refused to report a racial identity (n = 17) and participants who did not identify as female (n = 8) were not included in the present analyses.
We first plotted cortisol, HRV, and negative mood before, during, and after the TSST to determine whether reactivity and recovery could be captured using standard time intervals for the four groups: Black and White LGB and Black and White heterosexuals. As shown in , the point of inflection for the three indices largely corresponded to the typical peak response at 20 min post-TSST for cortisol and mood and during the TSST for HRV. We then compared the four groups on magnitude of reactivity and recovery separately for each of the three indices: cortisol, HRV, and negative mood. Results for the six ANOVAS with post hoc contrasts are presented in .
Figure 1. Cortisol levels before and after the Trier Social Stress Test (TSST) as a function of sexual orientation and race. Cortisol reactivity to the TSST (change from pre- to 20 min post) significantly varied by group (F [3,258] = 3.67, p =.013, eta = 0.20). Greater increases in cortisol following the TSST were observed for White LGB women (mean change score = 0.06) compared to Black LGB women (mean change score = 0.00). No effect was observed for the effect of group on cortisol recovery.
![Figure 1. Cortisol levels before and after the Trier Social Stress Test (TSST) as a function of sexual orientation and race. Cortisol reactivity to the TSST (change from pre- to 20 min post) significantly varied by group (F [3,258] = 3.67, p =.013, eta = 0.20). Greater increases in cortisol following the TSST were observed for White LGB women (mean change score = 0.06) compared to Black LGB women (mean change score = 0.00). No effect was observed for the effect of group on cortisol recovery.](/cms/asset/14d852e5-be6e-4b63-b47b-84d2c4605823/ists_a_1741545_f0001_c.jpg)
Figure 2. Heart rate variability (HRV) before and after the TSST as a function of sexual orientation and race. HRV reactivity to the TSST (prep to TSST) significantly varied by group (F [3,244] = 3.86, p =.010, eta = 0.21). The decrease in HRV during the TSST was smaller in magnitude for White LGB women (mean change score = –10.49) compared to Black LGB women (mean change score = –25.25). There was a significant effect of group on recovery of HRV (F [3,244] = 3.19, p =.024, eta = 0.19); and a trend toward statistical significance for LGB Black women to show a greater increase in HRV following the TSST compared to White heterosexual women.
![Figure 2. Heart rate variability (HRV) before and after the TSST as a function of sexual orientation and race. HRV reactivity to the TSST (prep to TSST) significantly varied by group (F [3,244] = 3.86, p =.010, eta = 0.21). The decrease in HRV during the TSST was smaller in magnitude for White LGB women (mean change score = –10.49) compared to Black LGB women (mean change score = –25.25). There was a significant effect of group on recovery of HRV (F [3,244] = 3.19, p =.024, eta = 0.19); and a trend toward statistical significance for LGB Black women to show a greater increase in HRV following the TSST compared to White heterosexual women.](/cms/asset/6b217bf9-11da-4a40-89c2-d5131a1ced01/ists_a_1741545_f0002_c.jpg)
Figure 3. Negative mood before and after the TSST as a function of sexual orientation and race. No statistically significant effect of group of Negative mood score on the Short Form of the Positive and Negative Affect Scale.
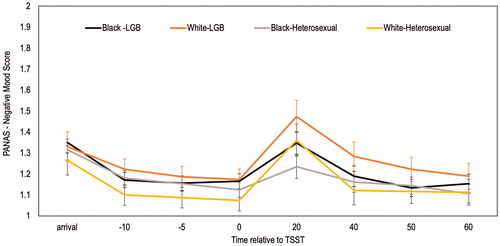
Table 1. Comparison of reactivity indices by race and sexual orientation.
Cortisol reactivity to the TSST significantly varied by group (F [3,258] = 3.67, p = .013, eta = 0.20) (). Greater increases in cortisol following the TSST were observed for White LGB women (mean change score = 0.06) compared to Black LGB women (mean change score = 0.00). Reactivity to the TSST as measured by HRV also significantly varied by group (F [3,244] = 3.86, p = .010, eta = 0.21) (). The decrease in HRV during the TSST was smaller in magnitude for White LGB women (mean change score = −10.49) compared to Black LGB women (mean change score = −25.25). There was a significant effect of group on recovery of HRV (F [3,244] = 3.19, p = .024, eta = 0.19); post hoc comparisons showed only a trend toward statistical significance for LGB Black women to show a greater increase in HRV following the TSST compared to White heterosexual women. There was no statistically significant effect of group on reactivity or recovery of negative mood ().
We, then, explored whether source of discrimination described during the TSST was associated with magnitude of reactivity and recovery for the three indices. Topics that focused on race, age, and sex were not significantly associated with reactivity or recovery to the TSST. Increases in cortisol following the TSST were significantly higher for women who described unfair treatment attributed to sexual orientation (mean change score = 0.06) compared to those who did not (mean change score = 0.01) (F [1, 245] = 6.76 p = .010, eta = 0.16). Changes in negative mood following the TSST were twice as high for women who described unfair treatment attributed to sexual orientation (mean = 0.34) compared to women who did not (mean = 0.17) (F [1, 253] = 4.38, p = .037, eta = 0.13).
Discussion
The TSST is the most widely used laboratory-based social evaluative stressor and has evidence of ecological validity (e.g. Henze et al., Citation2017). In the present study, the primary aim was to modify the speech task in way that would increase the motivation and relevance of the stressor without changing the validity of the task. Importantly, given the gap in understanding of health disparities for sexual minority women, we aimed for a modification that would yield typical responses on average for both sexual minority and heterosexual women, including an increase in cortisol and negative mood and a decrease in HRV. This modification worked equally well regardless of sexual minority status. Having a probe to measure individual differences in stress reactivity that is valid for sexual minority and heterosexual women provides the opportunity to further identify individual-level social stressors and perceived discrimination, as well as other factors, that may lead to hyper- or hypo-responsiveness of systems involved in stress regulation and general health. These factors may serve as targets of preventive interventions, the efficacy of which could be measured in part by reactivity to controlled laboratory stressors such as the TSST.
Our findings are consistent with prior studies that have successfully adapted the TSST to increase the salience and relevance of the stressor across diverse populations. Kim et al. (Citation2018), modified the speech task to a language brokering task for Mexican American adolescents; the 46 youth were required to translate medical instructions from English to Spanish prior to the oral arithmetic task. Typical increases in cortisol were found for the sample on average. Phan et al. (Citation2017) tested the impact of the addition of verbal feedback during the standard speech task, aiming to intensify the social evaluative component, and observed a change in the magnitude of hormonal response as a function of the modification. In our own work, we addressed task relevance by instructing adolescents to prepare a response to being treated unfairly such as being told that they were not allowed to do something or being blamed for something they felt was not their fault (Hipwell et al., Citation2009). Finally, Hatzenbuehler and McLaughlin (Citation2014) tested HPA-axis activity in response to discussing an experience in which the participant had been rejected based on sexual orientation in a sample of LGB young adults.
The current study had several notable strengths. First, the study recruited a large, diverse sample of participants drawn from a population-representative cohort study. This design facilitated greater statistical power to examine between-group differences and bolster confidence in the external validity of findings. Second, we examined acute stress reactivity. Prior studies focused on more global assessments that characterize relatively baseline levels of biological systems and have found mixed results regarding the presence and direction of between-group differences. In the context of a laboratory stressor, we are able to characterize patterns of reactivity in stress response systems that may be more proximally related to health disparities outcomes than baseline functioning. Third, this study examined both objective and self-report measures of reactivity. This approach provides a more rigorous test of hypotheses by allowing us to examine response concordance across indices.
The results of this study should be interpreted within the context of its limitations. The cross-sectional design of this study precludes inferences about how stress reactivity may change over time. Although, Black and White American women were well represented, other racial and ethnic minorities and men were not, limiting the generalizability of the results. Minority stress is associated with a broad range of health disparities, which are associated with stress reactivity, but were not examined here. Additionally, we did not examine factors that could modulate stress response (e.g. social support). Although, these factors were beyond the scope of the present study, they do represent important future directions. In particular, future studies should examine reciprocal relationships between social determinants of health, acute stress responses, and health outcomes over time.
This study provided an objective test of prior theoretical models, proposing that individual differences in stress reactivity represent a pathway by which minority stress influences health disparities. In support of this model, we found that an adaptation of the TSST elicits generalized stress responses in cortisol, HRV, and negative affect that are consistent with the original and adapted versions of the TSST. Further, by providing a more open-ended prompt, participants provided responses that were more personally salient. This approach balances retaining the social evaluative aspects of the TSST with the need to identify idiographic stress response and provides an additional approach that can be leveraged in future studies to characterize biomarkers of stress reactivity across diverse samples.
Notes on contributors
Dr. Keenan is a Professor and Dr. Berona a post-doctoral fellow in the Department of Psychiatry and Behavioral Neuroscience at the University of Chicago. Dr. Hipwell is a Professor, Dr. Stepp an Associate Professor, and Ms. Romito a Research Associate in the Department of Psychiatry at the University of Pittsburgh.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Austin, S. B., Rosario, M., McLaughlin, K. A., Roberts, A. L., Gordon, A. R., Sarda, V., Missmer, S., Anatale-Tardiff, L., & Scherer, E. A. (2016). Sexual orientation and diurnal cortisol patterns in a cohort of U.S. young adults. Psychoneuroendocrinology, 69, 197–208.
- Austin, S. B., Rosario, M., McLaughlin, K. A., Roberts, A. L., Sarda, V., Yu, K., Missmer, S., Anatale-Tardiff, L., & Scherer, E. A. (2018). Sexual orientation and salivary alpha-amylase diurnal rhythms in a cohort of U.S. young adults. Psychoneuroendocrinology, 97, 78–85.
- Beatty, D. L., & Matthews, K. A. (2009). Unfair treatment and trait anger in relation to nighttime ambulatory blood pressure in African American and white adolescents. Psychosomatic Medicine, 71(8), 813–820.https://doi.org/https://doi.org/10.1097/PSY.0b013e3181b3b6f8
- Buske-Kirschbaum, A., Jobst, S., Wustmans, A., Kirschbaum, C., Rauh, W., & Hellhammer, D. (1997). Attenuated free cortisol response to psychosocial stress in children with atopic dermatitis. Psychosomatic Medicine, 59(4), 419–426.https://doi.org/https://doi.org/10.1097/00006842-199707000-00012
- Cavigelli, S. A., & Caruso, M. J. (2015). Sex, social status and physiological stress in primates: The importance of social and glucocorticoid dynamics. Philosophical Transactions of the Royal Society B, 26, 370.
- Cochran, S. D., & Mays, V. M. (2007). Physical health complaints among lesbians, gay men, and bisexual and homosexually experienced heterosexual individuals: Results from the California Quality of Life Survey. American Journal of Public Health, 97(11), 2048–2055.https://doi.org/https://doi.org/10.2105/AJPH.2006.087254
- Cook, S. H., Juster, R.-P., Calebs, B. J., Heinze, J., & Miller, A. L. (2017). Cortisol profiles differ by race/ethnicity among young sexual minority men. Psychoneuroendocrinology, 75, 1–4.
- Diez Roux, A. V., Jacobs, D. R., Kiefe, C. I.,; Coronary Artery Risk Development in Young Adults (CARDIA) Study (2002). Neighborhood characteristics and components of the insulin resistance syndrome in young adults: The Coronary Artery Risk Development in Young Adults (CARDIA) study. Diabetes Care, 25(11), 1976–1982.https://doi.org/https://doi.org/10.2337/diacare.25.11.1976
- Dowd, J. B., Palermo, T., Chyu, L., Adam, E., & McDade, T. W. (2014). Race/ethnic and socioeconomic differences in stress and immune function in The National Longitudinal Study of Adolescent Health. Social Science & Medicine, 115, 49–55.https://doi.org/https://doi.org/10.1016/j.socscimed.2014.06.011
- Flentje, A., Heck, N. C., Brennan, J. M., & Meyer, I. H. (2020). The relationship between minority stress and biological outcomes: A systematic review. Journal of Behavioral Medicine.
- Goodman, W. K., Janson, J., & Wolf, J. M. (2017). Meta-analytical assessment of the effects of protocol variations on cortisol responses to the Trier Social Stress Test. Psychoneuroendocrinology, 80, 26–35.https://doi.org/https://doi.org/10.1016/j.psyneuen.2017.02.030
- Hatzenbuehler, M. L., & McLaughlin, K. A. (2014). Structural stigma and hypothalamic-pituitary-adrenocortical axis reactivity in lesbian, gay, and bisexual young adults. Annals of Behavioral Medicine, 47(1), 39–47.https://doi.org/https://doi.org/10.1007/s12160-013-9556-9
- Henze, G. I., Zänkert, S., Urschler, D. F., Hiltl, T. J., Kudielka, B. M., Pruessner, J. C., & Wüst, S. (2017). Testing the ecological validity of the Trier Social Stress Test: Association with real-life exam stress. Psychoneuroendocrinology, 75, 52–55.https://doi.org/https://doi.org/10.1016/j.psyneuen.2016.10.002
- Hipwell, A. E., Keenan, K., & Marsland, A. (2009). Exploring psychophysiological markers of vulnerability to somatic illnesses in females. Journal of Pediatric Psychology, 34(9), 1030–1283.https://doi.org/https://doi.org/10.1093/jpepsy/jsp010
- Jamieson, J. P., Nock, M. K., & Mendes, W. B. (2012). Mind over matter: Reappraising arousal improves cardiovascular and cognitive responses to stress. Journal of Experimental Psychology: General, 141(3), 417–422.
- Juster, R. P., Doyle, D. M., Hatzenbuehler, M. L., Everett, B. G., DuBois, L. Z., & McGrath, J. J. (2019). Sexual orientation, disclosure, and cardiovascular stress reactivity. Stress, 22(3), 321–331.
- Juster, R. P., Hatzenbuehler, M. L., Mendrek, A., Pfaus, J. G., Smith, N. G., Johnson, P. J., Lefebvre-Louis, J. P., Raymond, C., Marin, M. F., Sindi, S., Lupien, S. J., & Pruessner, J. C. (2015). Sexual orientation modulates endocrine stress reactivity. Biological Psychiatry, 77(7), 668–676.
- Juster, R. P., Raymond, C., Desrochers, A. B., Bourdon, O., Durand, N., Wan, N., Pruessner, J. C., & Lupien, S. J. (2016). Sex hormones adjust "sex-specific" reactive and diurnal cortisol profiles. Psychoneuroendocrinology, 63, 282–290.
- Juster, R.-P., Smith, N. G., Ouellet, É., Sindi, S., & Lupien, S. J. (2013). Sexual orientation and disclosure in relation to psychiatric symptoms, diurnal cortisol, and allostatic load. Psychosomatic Medicine, 75, 103–116.
- Karlén, J., Ludvigsson, J., Hedmark, M., Faresjö, Å., Theodorsson, E., & Faresjö, T. (2015). Early psychosocial exposures, hair cortisol levels, and disease risk. Pediatrics, 135, 1450–1457.https://doi.org/https://doi.org/10.1542/peds.2014-2561
- Keenan, K., Hipwell, A. E., Chung, T., Stepp, S., Loeber, R., Stouthamer-Loeber, M., & McTigue, K. (2010). The Pittsburgh Girls Studies: Overview and initial findings. Journal of Clinical Child & Adolescent Psychology, 39(4), 506–521.https://doi.org/https://doi.org/10.1080/15374416.2010.486320
- Kim, S. Y., Zhang, M., Zeiders, K. H., Sim, L., & Gleason, M. E. J. (2018). Acute salivary cortisol response among Mexican American adolescents in immigrant families. Cultural Diversity and Ethnic Minority Psychology, 24(4), 510–520.https://doi.org/https://doi.org/10.1037/cdp0000218
- Kirschbaum, C., Wüst, S., Faig, H. G., & Hellhammer, D. H. (1992). Heritability of cortisol responses to huma corticotropin-releasing hormone, ergometry, and psychological stress in humans. The Journal of Clinical Endocrinology & Metabolism, 75, 1526–1530.https://doi.org/https://doi.org/10.1210/jcem.75.6.1464659
- Lande, M. B., Pearson, T. A., Vermilion, R. P., Auinger, P., & Fernandez, I. D. (2008). Elevated blood pressure, race/ethnicity, and C-reactive protein levels in children and adolescents. Pediatrics, 122(6), 1252–1257.https://doi.org/https://doi.org/10.1542/peds.2007-3162
- Lehavot, K., & Simoni, J. M. (2011). The impact of minority stress on mental health and substance use among sexual minority women. Journal of Consulting and Clinical Psychology, 79(2), 159–170.https://doi.org/https://doi.org/10.1037/a0022839
- Matthews, K. A., & Gallo, L. C. (2011). Psychological perspectives on pathways linking socioeconomic status and physical health. Annual Review of Psychology, 62(1), 501–530.https://doi.org/https://doi.org/10.1146/annurev.psych.031809.130711
- McLaughlin, K. A., Sheridan, M. A., Tibu, F., Fox, N. A., Zeanah, C. H., & Nelson, C. A. (2015). Causal effects of the early caregiving environment on development of stress response systems in children. Proceedings of the National Academy of Sciences, 112(18), 5637–5642.
- Meyer, I. H. (2015). Resilience in the study of minority stress and health of sexual and gender minorities. Psychology of Sexual Orientation and Gender Diversity, 2(3), 209–213.
- Meyer, I. H., Schwartz, S., & Frost, D. M. (2008). Social patterning of stress and coping: Does disadvantaged social statuses confer more stress and fewer coping resources? Social Science & Medicine, 67(3), 368–379.https://doi.org/https://doi.org/10.1016/j.socscimed.2008.03.012
- Phan, J. M., Schneider, E., Peres, J., Miocevic, O., Meyer, V., & Shirtcliff, E. A. (2017). Social evaluative threat with verbal performance feedback alters neuroendocrine response to stress. Hormones and Behavior, 96, 104–115.https://doi.org/https://doi.org/10.1016/j.yhbeh.2017.09.007
- Slopen, N., & Williams, D. R. (2014). Discrimination, other psychosocial stressors, and self-reported sleep duration and difficulties. Sleep, 37(1), 147–156.https://doi.org/https://doi.org/10.5665/sleep.3326
- Thompson, E. R. (2007). Development and validation of an internationally reliable short-form of the Positive and Negative Affect Schedule (PANAS). Journal of Cross-Cultural Psychology, 38(2), 227–242.https://doi.org/https://doi.org/10.1177/0022022106297301
- Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070.https://doi.org/https://doi.org/10.1037/0022-3514.54.6.1063