
ABSTRACT
Cultures could influence parents in the way they perceive adverse situations and in how external factors influence resilience, which in turn, may differentially affect the quality of life of a child. The present study aimed to examine the associations between different dimensions of parental resilience and the quality of life of children in Indonesia. The samples consisted of 497 families. This study used the Parenting Resilience Elements and the Quality of Life Questionnaire. Parental resilience consists of three dimensions, knowledge of child’s characteristics, positive perception of parenting, and perceived social support. Knowledge of child’s characteristics, one of the parental resilience dimensions, significantly related to the Quality of Life dimensions of communication and influence, and development. Positive perceptions of parenting related to socio-emotional well-being. Perceived social support related to material well-being, activity, and socio-emotional well-being. We found that the parental resilience related to Quality of Life of children with developmental disabilities. Some findings could be unique for a collectivist culture and highlight the complexities of the association between different factors of parent resilience and Quality of Life of children with developmental disabilities in Indonesia.
Introduction
Developmental disabilities include severe delays in cognition, communication, social abilities, or motor abilities (Odom, Horner, & Snell, Citation2007) that usually emerge before the age of 22. A plethora of studies have demonstrated that having a developmental disability can have serious consequences for children’s quality of life (Odom et al., Citation2007; Sasson, Citation2000; Townsend-White, Pham, & Vassos, Citation2012; Wong et al., Citation2016). Whereas developmental disabilities are likely to affect children’s quality of life negatively, there are also factors that have protective effects. High levels of parental resilience have been found to have a positive effect on the quality of life of children with developmental disabilities (Migerode, Maes, Buysse, & Brondeel, Citation2012; Orbuch, Parry, Chesler, Fritz, & Repetto, Citation2005). Most studies on the role of parental resilience of a child with a developmental disability included families from Western societies. Little is known about the role of parental resilience in the quality of life of children with developmental disabilities living in non-Western cultures. This is important because parents in non-Western cultures may differ significantly from those in Western cultures in the way they perceive adverse situations and in how external factors influence resilience (Garcia-Dia, DiNapoli, Garcia-Ona, Jakubowski, & O’Flaherty, Citation2013; Ungar, Citation2006, Citation2011), which in turn, may differentially affect the quality of life of children. In the present study, the association between parental resilience and the quality of life of children was examined using a sample of Indonesian parents of children with a developmental disability.
Children with a developmental disability experience severe limitations in various dimensions of their daily activities (Dunst, Citation2007; Odom et al., Citation2007). To minimise these limitations, interventions often target at improving children’s quality of life (Chow, Lo, & Cummins, Citation2005). Quality of life can be defined as one’s satisfaction of life, consisting of different but related constructs, such as material well-being, socio-emotional well-being, communication and influence, development (optimising potential and independence), and activities that allow people to broaden their life experience (Felce & Perry, Citation1995).
Parents of children with developmental disabilities face different challenges. For instance, they show higher levels of stress compared to parents of children without developmental disabilities (Gupta, Citation2007). Furthermore, from time to time, parents of children with a developmental disability are confronted with adverse situations, as their children have specific psychological and physical needs (King et al., Citation2003; Suzuki, Kobayashi, Moriyama, Kaga, & Inagaki, Citation2013). Compared to typically developing children, parents of children with autism spectrum disorder find it more challenging to raise their children. They also have difficulties in finding an appropriate school. Moreover, they are often expected to participate in home exercise programs which often result in stressful situations (Santoso, Ito, Ohshima, Hidaka, & Bontje, Citation2015; Schieve, Blumberg, Rice, Visser, & Boyle, Citation2007; Suzuki et al., Citation2013). Children whose parents can adapt well to such adverse situations have been found to experience a better quality of life than children with parents who are less capable of adapting (Cappe, Wolff, Bobet, & Adrien, Citation2011).
Previous research indicates that children’s quality of life largely depends on family support, family health and happiness (Burgess & Gutstein, Citation2007; Frain et al., Citation2007). When parents are able to adapt and deal with those situations, this may, in turn, positively affect the quality of life of the child (Cappe et al., Citation2011; Migerode et al., Citation2012; Suzuki et al., Citation2013). Suzuki et al. (Citation2013) define resilience in parents with a child with a developmental disability as an adaptation process in the challenge of an adverse situation of their children behaviour problems that include both internal and external factors, such as positive perceptions, skills, coping styles, efficacies, and social supports.
Previous studies have also shown that the concept of parental resilience can be further categorised into three different but related constructs. The first construct refers to knowledge of the child’s characteristics (Suzuki et al., Citation2015), which concerns the way parents perceive their child’s behaviour. Parents with better knowledge of their child’s behaviour are more likely to experience perceived control which may lead to less parental stress (Harrison & Sofronoff, Citation2002; Singer, Ethridge, & Aldana, Citation2007). The second construct is the perceived social support by parents. Parents with higher levels of perceived social support show more emotional well-being and optimism, whereas parents who perceive low levels of support are more likely to develop depression and anxiety (Boyd, Citation2002; Ekas, Lickenbrock, & Whitman, Citation2010; Smith, Greenberg, & Seltzer, Citation2012). The final dimension of parental resilience refers to the positive perception of parenting itself, which can be defined as the ‘pleasure and happiness in rearing the child and the acceptance of the parental role’ (Suzuki et al., Citation2015, p. 8). Mother’s perceptions of the child are positively associated with reframing coping strategies and positive reframing of potentially traumatic and stressful events (Hastings & Taunt, Citation2002).
Although the significant role of parental resilience in the quality of life of children with developmental disabilities is well-established, most studies have been conducted in Western societies. This is an important limitation as the perceived quality of life has been shown to be culturally dependent (Neely-Barnes & Dia, Citation2008). Moreover, findings from existing studies in Western cultures might not be generalised to other cultures, such as the Asian culture. Many people in Indonesia, for instance, believe that children’s disabilities are related to problems during pregnancy, and developmental disability is perceived as something that cannot and should not be influenced, due to karmic influences (Riany, Cuskelly, & Meredith, Citation2016). Such cultural beliefs may cause stigma and limit the possibilities for families to find professional support (Kusumastuti, Pradanasari, & Ratnawati, Citation2014).
As a consequence, parents are more likely to take the burden by themselves (Kusumastuti et al., Citation2014). This also means that they have to make other family members (e.g. grandparents) understand their child’s condition and accept the limitations caused by the child’s disability as well (Santoso et al., Citation2015). In Indonesia, such cultural beliefs may prevent children from enrolling appropriate intervention programmes and participating in community activities (Kusumastuti et al., Citation2014; Riany, Cuskelly, & Meredith, Citation2016). This may negatively affect the quality of life of the children. However, research in this field in non-Western contexts is still scarce.
This study aimed to examine the associations between parental resilience and the quality of life of children with developmental disabilities using some samples from Indonesian families. More specifically, the importance of each of the three dimensions of parental resilience (i.e. knowledge of child’s characteristic, perceived social support, and positive perceptions of parenting) was examined. Regarding the quality of life, we looked at the dimensions of physical well-being, material well-being, communication and influence, socio-emotional well-being, development, and activity. Based on previous studies (Greeff & Van der Walt, Citation2010; Migerode et al., Citation2012; Openshaw, Citation2011; Orbuch et al., Citation2005), the present study hypothesised that each of the dimensions of parental resilience would be associated with each of the dimensions of quality of life.
Materials and Methods
Participants
Questionnaires were sent to 822 families. Five hundred families returned the questionnaires, resulting in the participation rate of 61%. Three families were excluded because their children were older than 22. Therefore, the final samples consisted of 497 families. All families live in Java Island, the most populated island of Indonesia. The largest proportion of children with disabilities in Indonesia are in Java Island as more people in Indonesia live on this Island (Diono, Mujaddid, & Budijanto, Citation2014).
Parents who were included in the present study have at least one child diagnosed as a child with a developmental disability. More specifically, 32% (n = 160) of the parents have a child with autism spectrum disorder, 23% (n= 113) of the parents have a child with an intellectual disability, 10%t (n= 49) of the parents have a child with ADHD, 7% (n= 36) of the parents have a child with Down syndrome, and 28% (n = 139) of the parents have a child with a learning disability, speech or hearing disorder, physical, and visual impairment (see ).
Children who were included had a mean age of 11 years (SD = 4.36 years), most of them were the eldest child in the family (48.1%). The average educational levels of the parents were between senior high school and undergraduate, while the average family incomes were under the regional minimum wage (see ). The average educational levels and incomes suggested an overrepresentation of families with a relatively low socio-economic status. Socio-economic status was included as a latent score based on father’s education level, mother’s educational level (7 levels ranging from no education to post graduate), and family monthly income in Indonesian Rupiah (see ).
Measures
The parental resilience and child’s quality of life scale were translated into the Indonesian language by two Indonesian experts in both linguistics and psychology. The translation process was completed by three other experts who gave ratings for the Indonesian version compared to the original English version. All professionals involved in the translations discussed the translation and reached consensus on the final content. The researcher decided one of two translations and gave it to parents for readability check.
Parental Resilience
Parental resilience was measured using the Parenting Resilience Elements Questionnaire (PREQ) developed by Suzuki et al. (Citation2015), consisting of 13 items, divided over three subscales. On each item, a statement was presented, and the parents were asked to indicate the extent to which they agreed with this statement. The questionnaire included the following subscales: Knowledge of the Child’s Characteristics (5 items; e.g.e.g. I can figure out the reason behind my child’s trouble), Perceived Social Support (4 items; e.g. I have someone whom I can trust my child with.), and Positive Perceptions of Parenting (4 items; e.g. My child makes me feel energised.). The items were rated on a seven-point Likert scale, ranging from strongly disagree (1), disagree (2), disagree somewhat (3), undecided (4), agree somewhat (5), agree (6) to strongly agree (7). Each subscale had sufficient internal consistency. Items 2, 9 and 11 of this scale were excluded (see , the explanation is below the table). One item, item 2, was deleted from the factor of knowledge of the child’s characteristic. Parents of a child with a developmental disability questioned how their child’s future such as their physical independence, education, and financial independence (Heiman, Citation2002). Items 9 and 11, from the factor of perceived social supports, were excluded because the Indonesian culture is characterised by high levels of interdependence when it comes to family. Extended family is a strong source of support (Riany, Cuskelly, & Meredith, Citation2017). Parents are also likely to learn from other parents’ experience about raising children with a developmental disability (Santoso et al., Citation2015).
Table 1. Demographic characteristics of participants.
Table 2. Parental resilience subscales and items.
Child’s Quality of Life
Child’s quality of life was measured with the Quality of Life Questionnaire developed by Petry, Maes, and Vlaskamp (Citation2009), consisting of a total of 54 items, divided into six subscales (Petry et al., Citation2009). This questionnaire was developed to evaluate people’s quality of life with profound multiple disabilities (Petry et al., Citation2009). Parents were asked to indicate the extent to which they agree with given statements. The questionnaire included the following subscales: Physical Well-being (8 items; e.g. the person has seldom pain); Material Well-being (9 items; e.g. The person has at his/her disposal all technical aids and adaptations that he/she needs regarding activities and leisure); Socio-emotional Well-being (6 items; e.g. the person expresses affection towards people in his/her direct environment), Communication and Influence (9 items; e.g. the person expresses his/her preferences with regard to activities and actions (e.g. personal care, nourishment), Development (9 items; e.g. the person receives schooling/education or developmental stimulation), and Activities (9 items; e.g. the person participates in activities that interest him/her). Response options ranged from strongly disagree (1), disagree (2), agree (3), and strongly agree (4). Each subscale showed sufficient internal consistency, with the exception of the subscale measuring physical well-being consisting of eight items (internal consistency = 0.37; e.g. the person has seldom pain). This subscale was excluded because the items were not suitable for this research population as most of the children in those families did not have a physical disability. Some other items that did not apply to this sample were also excluded (see ). Items were excluded because most of the families in this study did not hire special support for their children. It was also because, in Indonesia, some public services were not designed to be accessible for all children. Most of the children in this population were still depend on other adults (parents, teachers, or therapists) for activity.
Procedure
Participating parents were recruited via inclusive schools, special schools for disabled children, therapy centres, and personal referral. At each institution, initial contact was made with the person in charge (i.e. headmasters, coordinators, or owner of the therapy centre). Subsequently, a letter with detailed information about the study was sent. Once they gave permission, they listed the entire eligible parents. Finally, questionnaires were sent to the homes of the parents or were handed over personally. Data collectors had no control over how the parents filled in the questionnaires, whether by both of the parents or by the parent (father or mother). Informed consent about the research and data collection was included in the first page, and parents who agreed to participate needed to sign it in.
Statistical Analysis
Using Mplus version 7.4 (Muthén), we employed structural equation modelling to test the structural relationship between measured variables and latent constructs. Mplus allows the integrative test of different associations with multiple dependent variables, as well as the use of latent constructs. In the model of the present study, family resilience consisted of three independent factors (i.e. Knowledge of child characteristics, Perception of positive parenting, and Perceived social support). These three factors were related to the five qualities of life outcome measures (i.e. material well-being, social well-being, communication and influence, development, and activities). Finally, we controlled for the confounding effects of child’s age, gender, and type of disability, as well as for the socio-economic status (i.e. SES) of the family. The latter was assessed by a latent construct of father and mother education level and monthly income in Indonesian Rupiah. To determine model fit, we used the Comparative Fit Index (CFI) (Bentler, Citation1990), the Tucker-Lewis Index (TLI); (Kline & Santor, Citation1999), and the Root Mean Squared Estimate of Approximation (RMSEA) (Steiger, Citation1990).
Results
Factor Loadings of Latent Variables
Factor loadings for Parental Resilience ranged from 0.42 to 0.86. Quality of Life factor loadings of the five factors ranged from 0.43 to 0.68. Loadings for SES were >.70.
Findings of Correlation and Comparison Analysis
Prior to the test of the structural equation model that we used to answer the main research question, we computed Pearson correlations between the main study variables, including demographic variables, parental resilience, and quality of life. presents the bivariate correlations between the study variables. What stands out are the strong significant correlations between family resilience and the quality of life dimensions.
Table 3. Quality of life subscales and items.
Table 4. Pearson correlation among measures.
Furthermore, we analysed associations between parents’ education level and family income and children’s quality of life and parental resilience factors. A one-way ANOVA showed that higher levels of fathers’ education were related to Material well-being (F(6, 425) = 6.248, p < 0.000), and Perceived social support (F(6, 407) = 3.015, p= 0.007). Higher levels of mother’s education were related with Material well-being (F(6, 437) = 7.174, p < 0.000) and Activity (F(6, 436) = 2.155, p= 0.046). Bivariate correlations showed positive associations between Family income and Material well-being (r = 0.354, p = 0.000), Socio-emotional well-being (r = 0.195, p = 0.000), Activity (r = 0.176, p = 0.000), Perceived social support (r = 0.174, p = 0.000), and Positive perception of parenting (r = 0.157, p = 0.001).
In addition, a one-way between-subjects ANOVA was conducted to compare the different child’s age groups (i.e. infant and toddler, early childhood, middle childhood, late childhood, adolescent) on child’s quality of life. Results showed a statistically significant difference between child’s age groups on Material well-being F(4, 383) = 2.5, p = 0.042. More specifically, material well-being in late childhood children (M = 2.63, SD = 0.390) was significantly lower than in the adolescent age group (M = 2.76, SD = 0.393). However, other age groups did not differ. There was also a significant difference between child’s age groups on Communication and influence F(4, 369) = 3.33, p = 0.011. Post hoc group comparisons indicated that the mean score of Communication and Influence in early childhood (M = 2.57, SD = 0.498) was significantly different than that in the middle childhood age group (M = 2.82, SD = 0.405) and the adolescent age group (M = 2.85, SD = 0.391).
Finally, we conducted a one-way ANOVA to test for differences among children with various developmental disabilities. The results indicated significant differences between the types of disability in Material well-being F(8,442) = 2.4, p = 0.015, Communication and Influence F(8,428) = 3.69, p < .001, Socio-emotional well-being F(8,454) = 3.34, p < .001, Development F(8,437) = 3.64, p < .000, and Activity F(8,445) = 3.7, p < .000. However, no significant differences were found for parent resilience. A Tukey post hoc test showed that Communication and influence showed lower levels in families with a child with an Autism spectrum disorder (M = 2.69, SD = 0.516) than in families with a child with an Intellectual disability (M = 2.88, SD = 0.322), ADHD (M = 2.91, SD = 0.516), or a Learning disability (M = 3.01, SD = 0.279). Furthermore, families with a child with an Autism spectrum disorder (M = 2.79, SD = 0.374) also showed lower levels of Socio-emotional well-being as compared to families with a child with an Intellectual disability (M = 2.97, SD = 0.424), and ADHD (M = 3.01, SD = 0.525). In addition, families with a child with Autism (M = 2.74, SD = 0.374) also showed lower levels of Development than families with a child with ADHD (M = 2.99, SD = 0.374), and a Learning Disability (M = 3.03, SD = 0.3640). Finally, lower levels of Activity were found in families with a child with Autism (M = 2.7, SD = 0.405) than in families with a child with ADHD (M = 2.92, SD = 0.483).
Findings of the Structural Equation Model
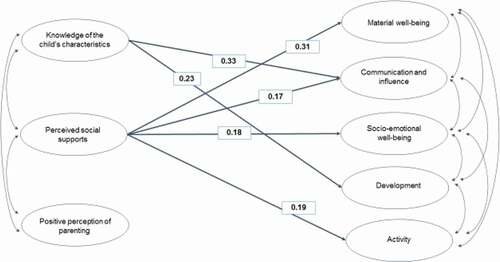
Findings of the structural model while controlling for the effects of child’s age, gender, type of disability, and socioeconomic status (father’s and mother’s education and family monthly income) are presented in . Model fit was acceptable which is RMSEA = 0.052, CFI = 0.80, and TLI = 0.78. Knowledge of the child’s characteristics significantly related to Quality of Life dimensions of Communication and Influence (B = .33, p < .01) and Development (B = .23, p < .05). Perceived social support related significantly to the Quality of Life dimensions of Material well-being (B = .31, p < .001), Activity (B = .19, p < .01), Socio-emotional well-being (B = .18, p< .01), and Communication and Influence (B = .17, p< .05).
Figure 1. The associations between parental resilience and the quality of life.
Discussion
This study aimed to examine the associations of three dimensions of parental resilience with five dimensions of the quality of life of children with developmental disabilities using a sample of families from Indonesia. Studies in other countries have shown that different dimensions of parental resilience are associated with dimensions of the quality of life. This is the first study with a similar focus in Indonesia. Findings showed significant associations between knowledge of child’s characteristics on the one hand and quality of life dimensions of communication and influence and development on the other hand. This is consistent with previous studies showing that parents who have a realistic image of their child’s abilities are more capable in understanding the needs of their child, and are more likely to let their child develop optimally, given its developmental disability (Suzuki et al., Citation2015).
Furthermore, the parental resilience dimension of perceived social support positively related to material well-being, communication and influence, socio-emotional well-being, and activity. More specifically, parents who experience high levels of social support were more capable of encouraging their child to participate in outdoor and social activities (Anaby et al., Citation2013; Anderson, Citation2009; Bois, Sarrazin, Brustad, Trouilloud, & Cury, Citation2005; Boyd, Citation2002; Ekas et al., Citation2010; Santoso et al., Citation2015; Schippers, Citation2010; Siperstein, Glick, & Parker, Citation2009; Smith et al., Citation2012).
The results of the present study shed light on the specific role of parental resilience on the quality of life in Indonesian families. In contrast to more individualistic western cultures, the Indonesian culture has a more collectivistic nature, which means that it is a culture that relies heavily on the family system, including spouse and grandparents who understand the child’s condition (Santoso et al., Citation2015). With respect to this specific study, the family system, who understand the child condition, can contribute significantly to the socio-emotional and material well-being of the child because they provide support which tightens the family bond, sense of mutual sharing in an emotional, and material sense as well (Santoso et al., Citation2015; Yeh, Arora, & Wu, Citation2006). Support from the family system may contribute significantly to parental resilience if family members accept the child condition, provide practical and emotional support in daily child’s care, and understand the child’s condition (Greeff & Van der Walt, Citation2010; Luong, Yoder, & Canham, Citation2009; Santoso et al., Citation2015).
In a collectivistic culture, however, it is more uncommon to discuss family problems with health care professionals. Parents of children with developmental disabilities tend to discuss their discomforts with family members or friends only; to a lesser extent with professionals such as a doctor, psychologist, or counsellor (Yeh et al., Citation2006). Becoming a part of members of the community who experience a similar situation is thus an important coping strategy for parents with a disabled child (Santoso et al., Citation2015; Yeh et al., Citation2006). For parents of children with developmental disabilities, however, the exclusive reliance on their own families may be a risk factor regarding their material and socio-emotional well-being. The previous research has indicated that it is especially important for parents with a developmentally disabled child to be involved in public groups’ advocacies or parents’ organisations to have better material and socio-emotional resources to draw strength from in adverse situations (Schippers, Citation2010).
In contrast to what was expected, we did not find any association between material well-being on the one hand and knowledge of the child’s characteristics and positive perception on the other hand. One can only speculate about the reasons why we did not find these associations, but in the present study it is likely to be caused by the overall overrepresentation of parents with low social economic status (i.e. low income and low completed education). For such parents, it has been found that external factors, such as perceived social support, significantly relate to material well-being as it facilitates access for various fulfilment of their children’s needs and themselves, that they cannot afford themselves (Henly, Danziger, & Offer, Citation2005; Magnuson & Duncan, Citation2002; Orthner, Jones-Sanpei, & Williamson, Citation2004). In low-middle and developing countries, such as Indonesia, support is available and accessible for those who have a high income since the government still provides only limited services for the low SES (Riany et al., Citation2017; Sidjaja, Newcombe, & Sofronoff, Citation2017).
There was also a non-significant relation between Communication and Influence and Positive perception of parenting. Communication and Influence refers to how children with developmental disabilities are able to express themselves, to be understood, to make choices, and to know what they want (Petry et al., Citation2009). The absence of the association could be explained by the fact that Indonesia, as a collectivist–culture country, has different ideas of what positive parenting refers to as compared to more individualistic cultures. In more collectivistic cultures, parents emphasise interdependency and control on child behaviour (Chao & Tseng, Citation2002; Keshavarz & Baharudin, Citation2009; Riany, Meredith, & Cuskelly, Citation2017; Sorkhabi, Citation2005). Parents in Indonesia believe that good parenting stems from parental control so that children should be obedient and comply with their parents (Chao & Tseng, Citation2002). This was also found in parents of children with developmental disabilities. One study showed that parents of children with Autism Spectrum Disorder (ASD) had an even more authoritarian parenting style than parents of children without ASD (Riany et al., Citation2017).
Socio-emotional well-being and activity, as the quality of life dimensions, were not related to the knowledge of parents. These two qualities of life dimensions refer to the social relationship, social participation, and involvement in social activities. Participation in society in a collectivist culture depends highly on other people and the extent to which there is community acceptance. Other people’s thought and perception are important in their social life (Chao & Tseng, Citation2002; Yeh et al., Citation2006). Support, acceptance, and flexibility from the society are perceived as highly important dimensions determining the extent to which children with disabilities are involved in social life (Maulidia, Kinanthi, Permata, & Fitria, Citation2017). Parents may keep their children from seeing other people than their own family. Some parents may be ashamed and feel stigmatised by the society, and as a consequence, they may keep their children within their own family life (Chiang & Hadadian, Citation2007; Riany et al., Citation2016). This also relates to the absent association between the dimensions of development (of Quality of life) and perceived social support and positive perception, as the dimensions of parental resilience.
Conclusions
The findings of this study highlight the complexities of the association between different dimensions of parent resilience and the quality of life of children with developmental disabilities in Indonesia. Some findings of our study are in line with the existing research in Western cultures. However, some findings found seem unique for collectivistic cultures.
For practical implications, service providers need to recognise this cultural context. This study showed that perceived social support needs to be available for parents of disabled children, specifically for parents with low social economic status. Professionals should assist parents in their attempt to understand their children’s characteristics to have a sense of control about children’s behaviours difficulties. This could be reached through a training program for parents aimed at providing further information about children’s characteristics. It is also important to improve parents’ positive perception of their parenting. Professional support together with parents support groups may provide some approaches for parents about concrete parenting practices or coping strategies. Another important factor that should be taken into consideration is social acceptance towards children with developmental disabilities.
Limitation and Future Research
Although this study can be seen as an important first step in understanding the role of parental resilience towards the quality of life in Indonesian families of disabled children, some limitations should be acknowledged. Firstly, this study uses a cross-sectional design. As a consequence, we cannot draw any conclusions about causality. Theoretically, parental resilience may indeed predict children’s quality of life. However, the quality of life may also function as a precedent for parental resilience. Future research should obtain longitudinal data as this study only uses data from Indonesian parents. In order to be able to say something about the specificity of the Indonesian situation and context, the inclusion of other nationalities is warranted. Another limitation comes from the measure of general perception of social support. Based on this measure, it is hard to conclude whether or not potential stigma of having a child with disabilities prevents families from socialising with extended family members. Future research should include questions that may help to gain insight into this specific matter. Type of disability was included in the SEM model, however small sample sizes in some of the cells withheld us from statements about how the model would fit different types of disability. Future research should focus on different types of disabilities as it is conceivable that the links that we found in our study do differ in different sub-populations. Finally, it is worth noting that results may be biased because not all parents of disabled children could be reached and included in the present study. Only parents who bring their children to school or therapy centres were included in this study. Therefore, the results of the present study could not be generalised to all Indonesian parents of children with developmental disabilities. This is only the case for parents with middle or high socio-economic status. Given the fact that most parents of children with developmental disabilities in the present study have relatively low socio-economic status, the future study needs to include more variation in parents’ demographics.
Disclosure Statement
The named authors have no conflict of interest, financial or otherwise.
Additional information
Funding
References
- Anaby, D., Hand, C., Bradley, L., DiRezze, B., Forhan, M., DiGiacomo, A., & Law, M. (2013). The effect of the environment on participation of children and youth with disabilities: A scoping review. Disability and Rehabilitation, 35(19), 1589–1598.
- Anderson, D. (2009). Adolescent girls’ involvement in disability sport: Implications for identity development. Journal of Sport and Social Issues, 33(4), 427–449.
- Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238–246. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/2320703.
- Bois, J. E., Sarrazin, P. G., Brustad, R. J., Trouilloud, D. O., & Cury, F. (2005). Elementary schoolchildren’s perceived competence and physical activity involvement: The influence of parents‘ role modelling behaviours and perceptions of their child’s competence. Psychology of Sport and Exercise, 6(4), 381–397.
- Boyd, B. A. (2002). Examining the relationship between stress and lack of social support in mothers of children with autism. Focus on Autism and Other Developmental Disabilities, 17(4), 208–215.
- Burgess, A. F., & Gutstein, S. E. (2007). Quality of life for people with Autism: Raising the standard for evaluating successful outcomes. Child and Adolescent Mental Health, 12(2), 80–86. Retrieved from: https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1475-3588.2006.00432.x.
- Cappe, E., Wolff, M., Bobet, R., & Adrien, J.-L. (2011). Quality of life: A key variable to consider in the evaluation of adjustment in parents of children with autism spectrum disorders and in the development of relevant support and assistance programmes. Quality of Life Research, 20(8), 1279–1294. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/21312064 https://link.springer.com/content/pdf/10.1007%2Fs11136-011-9861-3.pdf.
- Chao, R., & Tseng, V. (2002). Parenting of Asians. In M. H. Bornstein (Ed.), Handbook of parenting: Social Conditions and applied parenting (Vol. 4, pp. 59–93). Mahwah, NJ, US: Lawrence Erlbaum Associates Publisher.
- Chiang, L. H., & Hadadian, A. (2007). Chinese and Chinese-American families of children with disabilities. International Journal of Special Education, 22(2), 19–23.
- Chow, S. M. K., Lo, S. K., & Cummins, R. A. (2005). Self-perceived quality of life of children and adolescents with physical disabilities in Hong Kong. Quality of Life Research, 14(2), 415–423. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/15892430.
- Diono, A., Mujaddid, F. A. P., & Budijanto, D. (2014). Situasi Penyandang Disabilitas. Retrieved from http://www.pusdatin.kemkes.go.id/resources/download/pusdatin/buletin/buletin-disabilitas.pdf.
- Dunst, C. J. (2007). Early intervention for infants and toddlers with developmental disabilities. Handbook of Developmental Disabilities, 161–180.
- Ekas, N. V., Lickenbrock, D. M., & Whitman, T. L. (2010). Optimism, social support, and well-being in mothers of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40(10), 1274–1284. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/20195734.
- Felce, D., & Perry, J. (1995). Quality of life: Its definition and measurement. Research in Developmental Disabilities, 16(1), 51–74. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/7701092.
- Frain, M. P., Berven, N. L., Tschopp, M. K., Lee, G. K., Tansey, T., & Chronister, J. (2007). Use of the resiliency model of family stress, adjustment and adaptation by rehabilitation counselors. Journal of Rehabilitation, 73(3), 18–25. Retrieved from <Go to ISI>://WOS:000250016600003
- Garcia-Dia, M. J., DiNapoli, J. M., Garcia-Ona, L., Jakubowski, R., & O’Flaherty, D. (2013). Concept analysis: Resilience. Archives of Psychiatric Nursing, 27(6), 264–270. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/24238005 https://www.sciencedirect.com/science/article/pii/S0883941713000927?via%3Dihub.
- Greeff, A. P., & Van der Walt, K. J. (2010). Resilience in families with an autistic child. Education and Training in Autism and Developmental Disabilities, 45(3), 347–355.
- Gupta, V. B. (2007). Comparison of parenting stress in different developmental disabilities. Journal of Developmental and Physical Disabilities, 19(4), 417–425.
- Harrison, C., & Sofronoff, K. (2002). ADHD and parental psychological distress: Role of demographics, child behavioral characteristics, and parental cognitions. Journal of the American Academy of Child & Adolescent Psychiatry, 41(6), 703–711. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/12049445.
- Hastings, R. P., & Taunt, H. M. (2002). Positive perceptions in families of children with developmental disabilities. American Journal on Mental Retardation, 107(2), 116–127. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/11853529.
- Heiman, T. (2002). Parents of children with disabilities: Resilience, coping, and future expectations. Journal of Developmental and Physical Disabilities, 14(2), 159–171.
- Henly, J. R., Danziger, S. K., & Offer, S. (2005). The contribution of social support to the material well-being of low-income families. Journal of Marriage and Family, 67(1), 122–140. Retrieved from: https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.0022-2445.2005.00010.x.
- Keshavarz, S., & Baharudin, R. (2009). Parenting style in a collectivist culture of Malaysia. European Journal of Social Sciences, 10(1), 66–73.
- King, G., Lawm, M., King, S., Rosenbaum, P., Kertoy, M. K., & Young, N. L. (2003). A conceptual model of the factors affecting the recreation and leisure participation of children with disabilities. Physical and Occupational Therapy in Pediatrics, 23(1), 63–90. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/12703385 https://www.tandfonline.com/doi/pdf/10.1080/J006v23n01_05?needAccess=true.
- Kline, R. B., & Santor, D. A. (1999). Principles and practice of structural equation modelling. Canadian Psychology, 40(4), 381.
- Kusumastuti, P., Pradanasari, R., & Ratnawati, A. (2014). The problems of people with disability in Indonesia and what is being learned from the world report on disability. American Journal of Physical Medicine and Rehabilitation, 93(1Suppl 1), S63–67. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/24356085.
- Luong, J., Yoder, M. K., & Canham, D. (2009). Southeast Asian parents raising a child with autism: A qualitative investigation of coping styles. The Journal of School Nursing, 25(3), 222–229. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/19364878.
- Magnuson, K. A., & Duncan, G. J. (2002). Parents in poverty. Handbook of Parenting, 4, 95–121.
- Maulidia, F. N., Kinanthi, M. R., Permata, A. S., & Fitria, N. (2017). Family resilience pada keluarga yang memiliki anak dengan spektrum Autistik–ditinjau dari Perspektif Ibu [Family resilience in the family with Autistic Spectrum Disorder child - mother’s perspective]. Intuisi: Jurnal Psikologi Ilmiah, 9(1), 47–56.
- Migerode, F., Maes, B., Buysse, A., & Brondeel, R. (2012). Quality of life in adolescents with a disability and their parents: The mediating role of social support and resilience. Journal of Developmental and Physical Disabilities, 24(5), 487–503. Retrieved from <Go to ISI>://WOS:000308345700005: https://link.springer.com/content/pdf/10.1007%2Fs10882-012-9285-1.pdf.
- Neely-Barnes, S. L., & Dia, D. A. (2008). Families of children with disabilities: A review of literature and recommendations for interventions. Journal of Early and Intensive Behavior Intervention, 5(3), 93–107.
- Odom, S. L., Horner, R. H., & Snell, M. E. (2007). Handbook of developmental disability. Retrieved from https://www.researchgate.net/profile/Rutger_Gaag/publication/225798847_Handbook_of_developmental_disabilities/links/55144a760cf283ee08351252/Handbook-of-developmental-disabilities.pdf
- Openshaw, K. P. (2011). The relationship between family functioning, family resilience, and quality of life among vocational rehabilitation clients [Doctoral dissertation]. Utah State University. Retrieved from https://digitalcommons.usu.edu/cgi/viewcontent.cgi?article=2084&context=etd
- Orbuch, T. L., Parry, C., Chesler, M., Fritz, J., & Repetto, P. (2005). Parent-child relationships and quality of life: Resilience among childhood cancer survivors. Family Relations, 54(2), 171–183. Retrieved from: https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.0197-6664.2005.00014.x.
- Orthner, D. K., Jones-Sanpei, H., & Williamson, S. (2004). The resilience and strengths of low-income families. Family Relations, 53(2), 159–167. Retrieved from: https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.0022-2445.2004.00006.x.
- Petry, K., Maes, B., & Vlaskamp, C. (2009). Measuring the quality of life of people with profound multiple disabilities using the QOL-PMD: First results. Research in Developmental Disabilities, 30(6), 1394–1405. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/19595562.
- Riany, Y. E., Meredith, P., & Cuskelly, M. (2017). Understanding the influence of traditional cultural values on Indonesian parenting. Marriage and Family Review, 53(2), 207–226. Retrieved from <Go to ISI>://WOS:000424607800001: https://www.tandfonline.com/doi/pdf/10.1080/01494929.2016.1157561?needAccess=true.
- Riany, Y. E., Cuskelly, M., & Meredith, P. (2016). Cultural beliefs about autism in Indonesia. International Journal of Disability, Development and Education, 63(6), 623–640.
- Riany, Y. E., Cuskelly, M., & Meredith, P. (2017). Parenting style and parent–child relationship: A comparative study of Indonesian parents of children with and without Autism Spectrum Disorder (ASD). Journal of Child and Family Studies, 26(12), 3559–3571.
- Santoso, T. B., Ito, Y., Ohshima, N., Hidaka, M., & Bontje, P. (2015). Resilience in daily occupations of Indonesian mothers of children with Autism Spectrum Disorder. American Journal of Occupational Therapy, 69(5), 6905185020p6905185021–6905185028. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/26356659http://ajot.aota.org/article.aspx?articleid=2436690.
- Sasson, S. (2000). Beneficence versus respect for autonomy: An ethical dilemma in social work practice. Journal of Gerontological Social Work, 33(1), 5–16. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/14628757 https://www.tandfonline.com/doi/pdf/10.1300/J083v33n04_02?needAccess=true.
- Schieve, L. A., Blumberg, S. J., Rice, C., Visser, S. N., & Boyle, C. (2007). The relationship between autism and parenting stress. Pediatrics, Suppl 119(Supplement 1), S114–121. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/17272578.
- Schippers, A. (2010). Quality of life in disability studies. Medische Antropologie, 22(2), 277.
- Sidjaja, F. F., Newcombe, P. A., & Sofronoff, K. (2017). The diagnosis of autism spectrum disorder in urban Indonesia: A brief report. International Journal of Disability, Development and Education, 64(1), 33–44. Retrieved from <Go to ISI>://WOS:000392844200003: https://www.tandfonline.com/doi/pdf/10.1080/1034912X.2016.1162768?needAccess=true.
- Singer, G. H. S., Ethridge, B. L., & Aldana, S. I. (2007). Primary and secondary effects of parenting and stress management interventions for parents of children with developmental disabilities: A meta-analysis. Mental Retardation and Developmental Disabilities Research Reviews, 13(4), 357–369. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/17979202.
- Siperstein, G. N., Glick, G. C., & Parker, R. C. (2009). Social inclusion of children with intellectual disabilities in a recreational setting. Intellectual and Developmental Disabilities, 47(2), 97–107. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/19368488 https://aaiddjournals.org/doi/pdf/10.1352/1934-9556-47.2.97.
- Smith, L. E., Greenberg, J. S., & Seltzer, M. M. (2012). Social support and well-being at mid-life among mothers of adolescents and adults with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders, 42(9), 1818–1826. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/22160348 https://link.springer.com/content/pdf/10.1007%2Fs10803-011-1420-9.pdf.
- Sorkhabi, N. (2005). Applicability of Baumrind’s parent typology to collective cultures: Analysis of cultural explanations of parent socialization effects. International Journal of Behavioral Development, 29(6), 552–563. Retrieved from <Go to ISI>://WOS:000233474900010: https://www.tandfonline.com/doi/pdf/10.1080/01650250500172640?needAccess=true.
- Steiger, J. H. (1990). Structural model evaluation and modification: An interval estimation approach. Multivariate Behavioral Research, 25(2), 173–180. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/26794479 https://www.tandfonline.com/doi/pdf/10.1207/s15327906mbr2502_4?needAccess=true.
- Suzuki, K., Kobayashi, T., Moriyama, K., Kaga, M., Hiratani, M., Watanabe, K., … Yamashita. (2015). Development and evaluation of a Parenting Resilience Elements Questionnaire (PREQ) measuring resiliency in rearing children with developmental disorders. PLoS One, 10(12), p e0143946. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/26633810.
- Suzuki, K., Kobayashi, T., Moriyama, K., Kaga, M., & Inagaki, M. (2013). A framework for resilience research in parents of children with developmental disorders. Asian Journal of Human Services, 5(0), 104–111. Retrieved from https://www.jstage.jst.go.jp/article/ajhs/5/0/5_104/_pdf.
- Townsend-White, C., Pham, A. N. T., & Vassos, M. V. (2012). Review: A systematic review of quality of life measures for people with intellectual disabilities and challenging behaviours. Journal of Intellectual Disability Research, 56(3), 270–284. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/21679329.
- Ungar, M. (2006). Resilience across cultures. British Journal of Social Work, 38(2), 218–235.
- Ungar, M. (2011). Community resilience for youth and families: Facilitative physical and social capital in contexts of adversity. Children and Youth Services Review, 33(9), 1742–1748. Retrieved from <Go to ISI>://WOS:000294147600031: https://www.sciencedirect.com/science/article/pii/S0190740911001496?via%3Dihub.
- Wong, S. Y., Wong, T. K., Martinson, I., Lai, A. C., Chen, W. J., & He, Y. S. (2016). Needs of Chinese parents of children with developmental disability. Journal of Learning Disabilities, 8(2), 141–158.
- Yeh, C. J., Arora, A. K., & Wu, K. A. (2006). A new theoretical model of collectivistic coping Handbook of multicultural perspectives on stress and coping (pp. 55–72). Boston, MA: Springer.