

ABSTRACT
Tensioning techniqueswere the first neurodynamic techniques used therapeutically in the management of people with neuropathies. This article aims to provide a balanced evidence-informed view on the effects of optimal tensile loading on peripheral nerves and the use of tensioning techniques. Whilst the early use of neurodynamics was centered within a mechanical paradigm, research into the working mechanisms of tensioning techniques revealed neuroimmune, neurophysiological, and neurochemical effects. In-vitro and ex-vivo research confirms that tensile loading is required for mechanical adaptation of healthy and healing neurons and nerves. Moreover, elimination of tensile load can have detrimental effects on the nervous system. Beneficial effects of tensile loading and tensioning techniques, contributing to restored homeostasis at the entrapment site, dorsal root ganglia and spinal cord, include neuronal cell differentiation, neurite outgrowth and orientation, increased endogenous opioid receptors, reduced fibrosis and intraneural scar formation, improved nerve regeneration and remyelination, increased muscle power and locomotion, less mechanical and thermal hyperalgesia and allodynia, and improved conditioned pain modulation. However, animal and cellular models also show that ‘excessive’ tensile forces have negative effects on the nervous system. Although robust and designed to withstand mechanical load, the nervous system is equally a delicate system. Mechanical loads that can be easily handled by a healthy nervous system, may be sufficient to aggravate clinical symptoms in patients. This paper aims to contribute to a more balanced view regarding the use of neurodynamics and more specifically tensioning techniques.
Introduction
Neurodynamic techniques are commonly utilized with either an assessment focus (i.e. to assess the mechanosensitivity of the nervous system) or treatment focus. Within a treatment paradigm, neurodynamic techniques refer to therapeutic methods (manual techniques or exercises) which (1) facilitate movement between the nervous system and its interfacing tissues (e.g. by mobilizing the nervous system itself, including the internal neural connective tissue layers, or the structures that surround the nervous system) or (2) reduce the mechanical loading on the nervous system (e.g. adopting a posture or joint position that unloads the nervous system). The aim of these therapeutic techniques is to restore the altered homeostasis in and around the nervous system [Citation1].
When considering techniques that are aimed at mobilizing the nervous system itself, a biomechanical distinction can be made between ‘tensioning techniques’ and ‘sliding techniques’ [Citation2]. Both aim to mobilize the nervous system [Citation3,Citation4], but tensioning techniques are associated with a considerable increase in nerve strain, whereas with sliding techniques the nervous system can be mobilized without substantial increases in strain [Citation2,Citation5,Citation6].
Historically, tensioning techniques were the first described neurodynamic treatment techniques. They were derived from the neurodynamic tests (previously called neural tension tests). Because tensioning techniques use elements of neurodynamic tests that are aimed to reproduce or provoke the patient’s symptoms [Citation7], they may be contraindicated. In order to mobilize the nervous system, but without provoking or exacerbating symptoms, sliding techniques were developed [Citation5]. A sliding technique consists of two or more joint movements whereby movements which load the nervous system are simultaneously counterbalanced by movements that unload the nervous system. For example, throwing a dart can be considered a sliding technique for the median nerve (and a tensioning technique for the ulnar nerve). A backhand frisbee throw can be considered a tensioning technique for the median nerve (and a sliding technique for the ulnar nerve) ().
Figure 1. Examples of functional sliding and tensioning techniques. Throwing a dart is a sliding technique for the median nerve (A: wrist extension loads the median nerve; elbow flexion simultaneously unloads the median nerve; B: Elbow extension loads the median nerve; wrist flexion simultaneously unloads the median nerve), but a tensioning technique for the ulnar nerve (A: wrist extension and elbow flexion both load the ulnar nerve; B: elbow extension and wrist flexion both unload the ulnar nerve). Conversely, a frisbee backhand throw is a sliding technique for the ulnar nerve (C: elbow flexion loads the ulnar nerve and wrist flexion simultaneously unloads the ulnar nerve; D: wrist extension loads the ulnar nerve; elbow extension simultaneously unloads the ulnar nerve), but a tensioning technique for the median nerve (C: wrist and elbow flexion both unload the median nerve; D: wrist and elbow extension both load the median nerve).
Because sliding techniques are associated with greater nerve excursion with less strain [Citation2–4,Citation8], a common misconception is that sliding techniques are clinically superior to tensioning techniques. They are indeed biomechanically different, but there is no clinical evidence that one type of technique is more effective than another. Each type of technique most likely has its place depending on the stages of tissue healing and aims of the intervention.
Traditionally, neural mobilization has been based within a mechanical paradigm. This is not surprising, as ‘entrapment’ neuropathy suggests a mechanical cause, and longitudinal and transverse nerve movement is reduced in conditions, such as carpal tunnel syndrome [Citation9] and cervical radiculopathy [Citation10]. However, there is now a greater understanding that the effects of neural mobilization are also – and perhaps predominantly – neurophysiological, neurochemical and neuroimmune.
Interestingly, the beneficial effects of neurodynamic techniques in animal models of nerve injury have all been demonstrated following tensioning techniques [Citation11–16]. The aim of this article is therefore to provide a re-appraisal of neurodynamic tensioning techniques. We will focus on the effects of tensile loading on neurons and nerves in-vitro and ex-vivo, from animal models and human trials, to highlight beneficial effects of moderate nerve tension. We already want to emphasize that by no means are we advocating a re-introduction of nerve stretching or vigorous neurodynamic techniques. We always have and will continue to advocate to err on the side of caution in the management of people with neuropathies and to base treatment and technique selection on sound clinical reasoning. We hope this paper will provide important context for this clinical reasoning process for clinicians who use (or do not use) neurodynamic techniques in their clinical practice.
A structure designed to handle tension
During functional activities, the peripheral nervous system needs to be able to accommodate substantial amounts of nerve tension and elongation. Composite limb movements typically expose peripheral nerves to approximately 5 to 10% strain [Citation17], although some authors report much higher increases up to 20% strain [Citation18–20]. Because form and function follow each other, the nervous system is structurally designed to handle nerve strain well.
Peripheral nerves are heterogeneous structures. They exhibit non-linear viscoelastic responses to tensile loading [Citation21,Citation22]. Furthermore, although the well-organized, multilayered structure of the extracellular matrix bears considerable mechanical loads, the response of peripheral nerves to mechanical load is also characterized by their ability to glide, bend and twist [Citation22]. Neuroprotective architectural features, such as their unique undulating pattern, may also offer additional protective strength [Citation23]. In addition, mechanical properties of peripheral nerves are not equal along their length [Citation24], revealing a complex tissue ultrastructure [Citation25]. A recent model of nerve layer connections has been proposed to explain the complex (whole) nerve response to stretch [Citation26]. This model suggests that the mesoneurium, epineurium, and perineurium are coupled via viscoelastic physical connections and interact with a loosely coupled perineurium and endoneurium, allowing axons to glide and unravel throughout the length of the nerve. Collectively, these mechanical features allow nerves to straighten without bearing significant stresses while maintaining functional and structural integrity of the delicate axons within [Citation26].
Beneficial effects of tensile loading
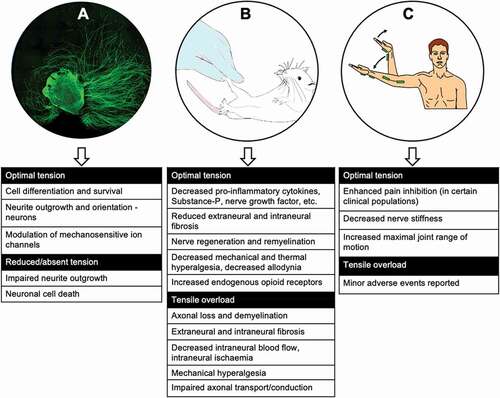
The following sections present findings from in-vitro, ex-vivo (including cadaveric), and animal and human in-vivo research which has assessed the effects of tensile loading on nerves (.).
Figure 2. The effects of tensile loading of the nervous system from (A) evidence from the Petri dish, (B) evidence from animal models, and (C) evidence from human trials.
1. Evidence from the Petri dish
Mechanical stimuli are fundamental for tissue healing since they affect cell differentiation and tissue renewal in physiological and pathological conditions, from embryo development to wound healing [Citation27–29]. Mechanical load applied directly to nerves can activate intracellular processes responsible for nerve myelination and nerve homeostasis. In-vitro experiments performed on human and rodent neurons have shown that stretch promotes cell differentiation (a process in which immature neurons acquire an adult phenotype with neurites connecting to other surrounding neurons, via neurites outgrowth). This process is fundamental in nerve repair following injury. For example, 7 days of intermittent mechanical stretch (10% strain at 0.25 Hz, for 120 minutes/day), applied to sensory neurons maintained in culture for an extended period of time (human neuroblastoma cell line; SH-SY5Y)), promoted processes linked to nerve regeneration (i.e. neurite outgrowth and cell differentiation) [Citation30]. A study examining sensory and motor neurons demonstrated that repeated application of tensile load (between 0.1–1% strain) resulted in dose-dependent neurite outgrowth, cell differentiation, and modulation of mechanosensitive ion channel expression with a plausible anti-nociceptive effect [Citation31,Citation32].
Progressive uniaxial tension for 14 days applied to ex-vivo DRG explants from rats significantly enhanced the outgrowth and orientation of neurites [Citation33–35]. A tailored mechanical stretch (with a strain of 0.1–1% for cultured neurons and up to 10% for DRG explants) had positive effects on neurite outgrowth and pain modulation [Citation27,Citation30,Citation36,Citation37]. Higher levels of stretch had negative effects on neurons, such as impaired neurite regeneration and increased neuronal death [Citation27,Citation33,Citation34,Citation36–38].
2. Evidence from animal models
Following a peripheral nerve injury, a cascade of neuro-immune responses occurs resulting in neuroinflammation and neuromodulation [Citation39]. In severe nerve injuries, this occurs not only at the injury site, but also more proximal along the neuraxis: at the corresponding DRG [Citation40], the dorsal horn of the spinal cord [Citation41] and higher brain centers, such as in the midbrain [Citation42], thalamus [Citation43], nucleus accumbens, and prefrontal cortex [Citation44]. Neuro-immune responses are defined as substances or processes (such as neuropeptides, cytokines, hormones and altered gene expression) involved in interactions between the immune system and the nervous system [Citation45]. These neuro-immune responses play an important role in the generation and maintenance of neuropathic pain following a nerve injury. Most of these insights originate from animal models of peripheral nerve injuries associated with severe axonal damage. More recently however, local and remote neuro-immune responses (e.g. in the DRG and spinal cord) have been demonstrated in people with lumbar radiculopathy [Citation46].
A recent literature review [Citation47] revealed that neural mobilization positively influenced various neuro-immune responses at the peripheral nerve injury site, but also at the corresponding DRG, spinal cord and higher brain centers. Interestingly, the type of treatment techniques used in these animal studies all mimicked tensioning techniques, with remarkable results. For example, in rats with induced painful diabetic neuropathy, tensioning techniques alleviated mechanical hypersensitivity on the paw of the treated side compared to the untreated side or compared to animals who did not receive neural mobilization [Citation13]. This improvement correlated with lower concentrations of pro-inflammatory cytokines (IL-1β and TNF-α) in the sciatic nerve and its branches only on the treated side.
At the level of the DRG, tensioning techniques resulted in a decrease of Substance-P and transient receptor potential vanilloid 1 (TRPV1) expression, and an increase in m-opioid receptor expression in rats with a sciatic nerve injury [Citation12]. These are relevant changes, as TRPV1 upregulation contributes to mechanical allodynia and thermal hyperalgesia; Substance-P plays an important role in the development of chronic pain [Citation48] and is responsible for the development of hyperalgesia in rats [Citation49]. Another study revealed that tensioning techniques were associated with a decrease in nerve growth factor (NGF) and glial fibrillary acidic protein (GFAP) in the DRG [Citation12]. Suppression of NGF overproduction in the DRG has shown to be related to neuropathic pain attenuation following a chronic constriction injury to the sciatic nerve [Citation50]. GFAP is a molecular marker for glial cell activity (astrocytes) and glial cell activation is a phenomenon linked to neuropathic pain [Citation51]. A decrease in GFAP expression following tensioning techniques was also observed in the lumbar spinal cord, associated with a reduction in mechanical and thermal hyperalgesia and allodynia [Citation12].
Glial cells and brain-derived neurotrophic factor (BDNF) expression are increased in the midbrain following a sciatic nerve injury causing neuropathic pain in rats [Citation14]. Glial cells are implicated in the development of persistent pain and BDNF released from activated microglia contributes to the nociceptive transmission. Remarkably, tensioning techniques resulted in a normalization of glial cells and BDNF expression [Citation14]. Also in the midbrain, tensioning techniques resulted in an increase in endogenous opioid receptors (Kappa-opioid receptors) in the periaqueductal gray [Citation16]. Furthermore, the rats who received tensioning techniques had increased tibialis anterior muscle strength and better locomotion compared to injured rats who did not receive neural mobilization [Citation16].
Tensioning techniques following a sciatic nerve crush injury or a chronic constriction injury in rats resulted in reduced intraneural scar formation [Citation15], anti-allodynic and neurotrophic effects able to speed up the nerve regeneration processes [Citation11,Citation12]. A severe sciatic nerve constriction injury can cause significant axonal loss (i.e. Wallerian degeneration) distal to the injury site. Increased numbers of axons with myelin sheaths of normal thickness and less inter-axonal fibrosis after treatment (tensioning techniques) have been shown in rats compared to controls with the same sciatic nerve injury who did not receive the intervention [Citation11]. In contrast, when injured nerves are not exposed to mechanical stimuli, nerve regeneration diminishes due to increased intraneural scar tissue formation, leading to mechanical allodynia and hyperalgesia [Citation11,Citation12,Citation15].
3. Evidence from human trials
In larger human clinical trials, neural mobilization is typically part of a multimodal intervention [Citation52–55]. If neural mobilization is evaluated as a unimodal intervention, different neurodynamic techniques are often combined [Citation52,Citation53], making it impossible to isolate the effects of tensioning techniques. A few smaller studies that evaluate the immediate effects of tensioning techniques are, however, available. Tensioning techniques enhanced conditioned pain modulation in people with chronic neck pain [Citation56]. Tensioning techniques had no effect on pain intensity in people with chronic neck pain [Citation56], and decreased pain intensity in computer users with elbow pain [Citation57].
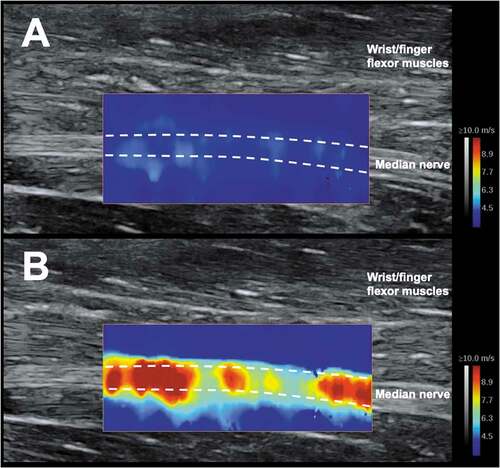
Ultrasound shear wave elastography investigations in healthy young adults revealed that nerve stiffness adapts to both short and long-term tensile mechanical stimuli [Citation58,Citation59] (). For example, sciatic nerve stiffness at the onset of stretch pain decreased following maintaining a nerve tension position (long-sitting, maintained twice for 3 minutes) [Citation58]. Similarly, a randomized controlled trial revealed a decrease in sciatic and tibial nerves’ stiffness following a neural tensioning style regime (total loading stimuli of 7.5 hours over 12 weeks), compared to a muscle stretching style regime [Citation59].
Figure 3. The median nerve, imaged using shear wave elastography, at the level of the mid-forearm when (A) relaxed and (B) when on stretch. Note: colored elastogram presents nerve shear wave velocity (metres/sec) (an index of nerve stiffness).
There is a growing body of evidence of in-vivo studies supporting that mechanical properties of human peripheral nerves are altered in various peripheral neuropathies, such as those associated with nerve compression [Citation60], metabolic syndrome [Citation61], and radiculopathies [Citation62–64]. Interestingly, a preliminary study reported that a 3-min slump (static) stretch resulted in an immediate decrease in sciatic nerve stiffness in people with unilateral sciatica [Citation65].
Too much of a good thing?
As described above, mechanical loading, including tensile forces, is fundamental to maintain the homeostasis in the nervous system. However, the response is influenced by the characteristics of tensile loading, such as the magnitude, duration, rate of loading and frequency [Citation66]. For example, 8% nerve strain exposed to an animal nerve [Citation67,Citation68] caused immediate reduction of intraneural blood flow, with total occlusion (leading to ischemia) at 15% strain (if sustained for up to one hour) [Citation68–70]. Nerve conduction becomes impaired from 8% strain of an animal nerve [Citation67] with conduction block from 10% to 12% strain, sustained (sustained for up to one hour) [Citation70]. Furthermore, as little as 3–5% strain of experimentally inflamed animal nerve resulted in increased neural mechanosensitivity [Citation71]. Nerve elongation has also been shown to decrease the cross-sectional area of a peripheral nerve [Citation72], a phenomenon believed to result in increased intraneural pressure with associated adverse effects [Citation22,Citation68,Citation73]. To the authors’ knowledge, there are no studies that have investigated the effect of ‘excessive’ tensile forces on neuroimmune responses both locally and at remote sites along the neuraxis, but it is likely that symptom flare following too much tensile loading, which often has a delayed onset, is also related to an increase in neuroinflammation.
Clinical reflections
From the research described above, what do these values of nerve tension and strain mean for clinical practice? During forward-bending in standing, sciatic nerve strain has been reported to reach 10.5% strain [Citation74], whilst composite movements of the upper limb expose the median [Citation20], radial [Citation19] and ulnar [Citation18] nerves to 18%, 12% and 10% strain respectively. During neurodynamic testing, it has been reported that the straight-leg raise test increased tibial nerve strain to 12.5%, whilst the median nerve neurodynamic test exposed the distal median nerve (proximal to the wrist) to 4% strain [Citation17]. However, some care is required when interpreting these values. Comparison of nerve strain between and within different methods (i.e. cadaver versus animal) is difficult as strain calculations require an accurate measure of nerve length at rest, and this is different between studies, which may explain the sometimes vastly different strain values reported in the literature.
Systematic reviews with and without meta-analyses reveal the clinical efficacy of neurodynamic techniques (which typically combine sliding and tensioning exercises, and techniques to mobilize the structures that surround the nervous system) for various conditions [Citation75–79]. Basic science studies revealed the potential working mechanisms of neurodynamic techniques (see above). However, the translation of these findings to clinical recommendations remains challenging, if not impossible. For example, all studies that used animal models to document the effects of tensioning techniques used nerve injury models that are much more severe than the neuropathies patients who seek physiotherapy care present with. The nerve injuries are also uniformly the same for all animals, with a selective lesion to the nerve without damage to joints or intervertebral discs, and animals are typically young without comorbidities.
It has also been difficult to directly determine nerve strain from human research, which presents a significant limitation (to date) when interpreting the effects of tensile forces upon the nervous system. In-vivo, human studies have examined shear-strain at the nerve-muscle interface [Citation80], ultrasound shear wave elastography to measure nerve shear wave velocity (an index of nerve stiffness) [Citation59,Citation81] (), and indirect measures of nerve strain calculated from excursion values [Citation74]. Future technologies that allow direct quantification of nerve strain through human research will be of great interest to this field.
The rate of tension application is important to consider also. It is believed that sudden stretching trauma has the potential to be more damaging compared to more gradual tension applied within appropriate limits [Citation67]. For example, fast eccentric muscle contractions have been shown to induce functional and structural damage in interfacing animal [Citation82,Citation83] and human [Citation84] nerves. Clinically, neurodynamic techniques are typically promoted to be performed as dynamic techniques rather than sustained or static holds [Citation85,Citation86]. Furthermore, tensioning techniques are promoted within limits of perceived passive resistance [Citation53,Citation87], a feature that has been adopted also in animal models with beneficial results [Citation27,Citation34]. Making evidence-based recommendations regarding the precise frequency and number of repetitions of neurodynamic techniques, including tensioning techniques, is problematic given the large variability reported in the literature [Citation85,Citation88]. For example, a systematic review of lower-limb neural mobilization techniques for healthy people and people with low back pain revealed technique application duration between 60 and 300 seconds with repetitions ranging between 1 and 45 [Citation88].
As mentioned earlier, tensioning techniques are considered more biomechanically challenging than sliding techniques, and as such careful clinical reasoning is essential when using and prescribing them, particularly in regard to mitigating symptom flare and/or clinical deterioration [Citation79]. Although there are many benefits of tensile loading to the nervous system, there is also a risk that movement-based techniques, in particular tensioning techniques, may be temporarily aggravating peripheral neuropathic pain [Citation89].
Conclusion
The studies summarized within this article illustrate the beneficial effects of optimal mechanical load to healthy and pathological nerves. The research shows that repeated mechanical tension on animal peripheral nerves applied by tensioning techniques has positive effects on nerve biomechanics, nerve repair and nerve regeneration processes, promoting multi-level changes in the peripheral and central nervous systems. Notably, these changes are induced in the cells of the peripheral and central nervous system and are linked to pain modulation and normal nerve function restoration. However, the optimal tension dosage to apply in clinical conditions remains the challenge. Not enough tension may result in little effects, whereas too much tension will undoubtedly exacerbate symptoms. It should be noted, that the optimal dosage for applying nerve tension in people with neuropathies has not been established and is unlikely to be established any time soon. A dosage that works well in one patient, may be too much or too little for another person. Therefore, judicious use of neurodynamic techniques, including tensioning techniques, should always consider multiple aspects and how they interact, such as the clinical presentation, nature of the symptoms, levels of irritability, pathophysiology, stages of healing, beliefs of the patient. Frequent re-assessments continue to play an important role.
Acknowledgments
Our thanks to Lilah Ellis for the provision of illustrations for .
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Richard Ellis
Richard is an Associate Professor in the Department of Physiotherapy at Auckland University of Technology (AUT) in New Zealand. He teaches on both the undergraduate and postgraduate programmes in the fields of musculoskeletal physiotherapy, manual and manipulative therapy, ultrasound imaging and research. Richard is also a Co-Director of the Health and Rehabilitation Research Institute (HRRI) at AUT, leading the Active Living and Rehabilitation: Aotearoa New Zealand (ALARA, https://hrri.aut.ac.nz/research-activities/active-living-and-rehabilitation) research group within HRRI. External to AUT, Richard is the Treasurer and an Executive Committee member of the International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT). Richard is a Senior Tutor with the New Zealand Manipulative Physiotherapists Association (NZMPA). He is also an Associate Editor for the New Zealand Journal of Physiotherapy.
Giacomo Carta
Ricardo is a Griffith University Postdoctoral Research Fellow at Menzies Health Institute Queensland and a member of Griffith Centre of Biomedical and Rehabilitation Engineering (GCORE) in Australia. Ricardo’s personal research interests are in understanding the integrated contributions of structure and biomechanics of peripheral nerves to neural function, dysfunction, and regeneration. His research expertise spans neuromusculoskeletal biomechanics, advanced neuroimaging methods, and clinical neurophysiology. Ricardo’s current research focuses on understanding the mechanisms underlying nerve damage in various peripheral neuropathies, with a particular focus on chemotherapy-induced peripheral neuropathy, and seeks to enhance the early diagnosis and management of peripheral neuropathies and chronic neuropathic pain.
Ricardo J. Andrade
Giacomo is a final-year Ph.D. student in Experimental Medicine and Therapy at the Stefano Geuna & Stefania Raimondo lab (Human Anatomy Department) at the University of Turin and Cavalieri Ottolenghi Neuroscience Institute, Italy (https://bit.ly/3kn81iD). Giacomo’s research interests are in understanding the pro-regenerative and pain modulation mechanisms of manual therapy and in particular neurodynamic treatment of somatic and autonomic nerves. His research expertise spans neuronal culture (in vivo and ex vivo), in vivo animal experiments with behavioral, histochemical, and molecular analyses, and neuropathic pain patient assessment. Giacomo’s current research focuses on understanding markers in the peripheral nerves responsible for pain modulation and nerve regeneration that are shared between humans and other mammals and seeks to implement clinical treatments for pain and neurodegenerative diseases. He also teaches in both the undergraduate and postgraduate programs in the fields of general neuroscience and neuropathic patient management.
Michel W. Coppieters
Michel is Menzies Foundation Professor of Health Research at Griffith University in Brisbane (Australia), where he directs the Musculoskeletal Health and Persistent Pain Research Group (https://mskhealthlab.com.au). The Group’s state-of-the-art research facility has quickly become one of the best pain labs in Australia and beyond. Although the focus has traditionally been on common musculoskeletal conditions, such as back pain and neck pain, we also research important conditions and side-effects that affect the musculoskeletal system, such as diabetic neuropathy, spinal cord injury and chemotherapy-induced peripheral neuropathy. We conduct lab-based research, as well as clinical research in the community, primary care, and hospital settings. Our research aims to (1) better understand the pathobiology of musculoskeletal and neurological conditions, (2) improve diagnostic procedures, (3) develop and evaluate biologically plausible interventions and (4) assess whether success of these interventions can be explained by reversal of the original pathobiological processes. Michel has successfully supervised many national and international PhD students. He has an excellent track record in mentoring early and mid-career researchers and clinicians, and is well-respected nationally and internationally.
References
- Coppieters M, and Nee RJ. Neurodynamic management of the peripheral nervous system. In:Jull G, Moore A, and Falla D, et al. editors. Grieve’s Modern Musculoskeletal Physiotherapy. 4th ed Elsevier:2015; 287–297 .
- Coppieters MW, Butler DS. Do ‘sliders’ slide and ‘tensioners’ tension? An analysis of neurodynamic techniques and considerations regarding their application. Manual Ther. 2008;13(3):213–221.
- Coppieters MW, Andersen LS, Johansen R, et al. Excursion of the sciatic nerve during nerve mobilization exercises: an in vivo cross-sectional study using dynamic ultrasound imaging. J Orthop Sports Phys Ther. 2015;45(10):731–737.
- Ellis RF, Hing WA, McNair PJ. Comparison of longitudinal sciatic nerve movement with different mobilization exercises: an in vivo study utilizing ultrasound imaging. J Orthop Sports Phys Ther. 2012;42(8):667–675.
- Coppieters MW, Alshami AM. Longitudinal excursion and strain in the median nerve during novel nerve gliding exercises for carpal tunnel syndrome. J Orthop Res. 2007;25(7):972–980.
- Coppieters MW, Alshami AM, Babri AS, et al. Strain and excursion of the sciatic, tibial, and plantar nerves during a modified straight leg raising test. J Orthop Res. 2006;24(9):1883–1889.
- Nee RJ, Jull GA, Vicenzino B, et al. The validity of upper-limb neurodynamic tests for detecting peripheral neuropathic pain. J Orthop Sports Phys Ther. 2012;42(5):413–424.
- Coppieters MW, Hough AD, Dilley A. Different nerve-gliding exercises induce different magnitudes of median nerve longitudinal excursion: an in vivo study using dynamic ultrasound imaging. J Orthop Sports Phys Ther. 2009;39(3):164–171.
- Ellis R, Blyth R, Arnold N, et al. Is there a relationship between impaired median nerve excursion and carpal tunnel syndrome? A systematic review. J Hand Ther. 2017;30(1):3–12.
- Thoomes E, Ellis R, Dilley A, et al. Excursion of the median nerve during a contra-lateral cervical lateral glide movement in people with and without cervical radiculopathy. Musculoskelet Sci Pract. 2021;52. DOI:https://doi.org/10.1016/j.msksp.2021.102349.
- Da Silva JT, Dos Santos FM, Giardini AC, et al. Neural mobilization promotes nerve regeneration by nerve growth factor and myelin protein zero increased after sciatic nerve injury. Growth Factors. 2015;33(1):8–13.
- Santos FM, Silva JT, Giardini AC, et al. Neural mobilization reverses behavioral and cellular changes that characterize neuropathic pain in rats. Mol Pain. 2012;8. DOI:https://doi.org/10.1186/1744-8069-8-57.
- Zhu GC, Tsai KL, Chen YW, et al. Neural mobilization attenuates mechanical allodynia and decreases proinflammatory cytokine concentrations in rats with painful diabetic neuropathy. Phys Ther. 2018;98(4):214–222.
- Giardini AC, Santos FMD, Da Silva JT, et al. Neural mobilization treatment decreases glial cells and brain-derived neurotrophic factor expression in the central nervous system in rats with neuropathic pain induced by CCI in rats. Pain Res Manag. 2017;2017. DOI:https://doi.org/10.1155/2017/7429761.
- Ê L, Santana H, Medrado A, et al. Neurodynamic mobilization reduces intraneural fibrosis after sciatic crush lesion in rats. Braz J Med Human Health. 2017;5(2):54–62.
- Santos FM, Grecco LH, Pereira MG, et al. The neural mobilization technique modulates the expression of endogenous opioids in the periaqueductal gray and improves muscle strength and mobility in rats with neuropathic pain. Behav Brain Funct. 2014;10(1):1.
- Nee RJ, Yang CH, Liang CC, et al. Impact of order of movement on nerve strain and longitudinal excursion: abiomechanical study with implications for neurodynamic test sequencing. Manual Ther. 2010;15(4):376–381.
- Wright TW, Glowczewskie F, Cowin D, et al. Ulnar nerve excursion and strain at the elbow and wrist associated with upper extremity motion. J Hand Surg Am. 2001;26A(4):655–662.
- Wright TW, Glowczewskie F, Cowin D, et al. Radial nerve excursion and strain at the elbow and wrist associated with upper-extremity motion. J Hand Surg Am. 2005;30(5):990–996.
- Wright TW, Glowczewskie F, Wheeler D, et al. Excursion and strain of the median nerve. J Bone Joint Surg Am. 1996;78(12):1897–1903.
- Ma Z, Hu S, Tan JS, et al. In vitro and in vivo mechanical properties of human ulnar and median nerves. J Biomed Mater Res A. 2013;101(9):2718–2725.
- Topp KS, Boyd BS. Structure and biomechanics of peripheral nerves: nerve responses to physical stresses and implications for physical therapist practice. Phys Ther. 2006;86(1):92–109.
- Shah SB. Tissue biomechanics: whales have some nerve. Curr Biol. 2017 Mar 06;27(5):R177–R179.
- Phillips JB, Smit X, De Zoysa N, et al. Peripheral nerves in the rat exhibit localized heterogeneity of tensile properties during limb movement. J Physiol. 2004;557(3):879–887.
- Mason S, Phillips JB. An ultrastructural and biochemical analysis of collagen in rat peripheral nerves: the relationship between fibril diameter and mechanical properties. J Peripher Nerv Syst. 2011;16(3):261–269.
- Sung J, Sikora-Klak J, Adachi SY, et al. Decoupled epineurial and axonal deformation in mouse median and ulnar nerves. Muscle Nerve. 2019;59(5):619–628.
- Carta G, Gambarotta G, Fornasari BE, et al. The neurodynamic treatment induces biological changes in sensory and motor neurons in vitro. Sci Rep. 2021;11. DOI:https://doi.org/10.1038/s41598-021-92682-2.
- Panciera T, Azzolin L, Cordenonsi M, et al. Mechanobiology of YAP and TAZ in physiology and disease. Nat Rev Mol Cell Biol. 2017;18(12):758–770.
- Passini FS, Jaeger PK, Saab AS, et al. Shear-stress sensing by PIEZO1 regulates tendon stiffness in rodents and influences jumping performance in humans. Nat Biomed Eng. 2021. DOI:https://doi.org/10.1038/s41551-021-00716-x.
- Higgins S, Lee JS, Ha L, et al. Inducing neurite outgrowth by mechanical cell stretch. Biores Open Access. 2013;2(3):212–216.
- van Wilgen CP, Testa M. Giving insight in pain research of tomorrow! Pain Rep. 2019;4(3):e753.
- Zhang M, Wang Y, Geng J, et al. Mechanically activated piezo channels mediate touch and suppress acute mechanical pain response in mice. Cell Rep. 2019;26(6):1419–1431.e4.
- Loverde JR, Ozoka VC, Aquino R, et al. Live imaging of axon stretch growth in embryonic and adult neurons. J Neurotrauma. 2011;28(11):2389–2403.
- Loverde JR, Pfister BJ. Developmental axon stretch stimulates neuron growth while maintaining normal electrical activity, intracellular calcium flux, and somatic morphology. Front Cell Neurosci. 2015;9. DOI:https://doi.org/10.3389/fncel.2015.00308
- Pfister BJ, Iwata A, Taylor AG, et al. Development of transplantable nervous tissue constructs comprised of stretch-grown axons. J Neurosci Meth. 2006;153(1):95–103.
- Gladman SJ, Ward RE, Michael-Titus AT, et al. The effect of mechanical strain or hypoxia on cell death in subpopulations of rat dorsal root ganglion neurons in vitro. Neuroscience. 2010;171(2):577–587.
- Zhou M, Hu M, He S, et al. Effects of RSC96 schwann cell-derived exosomes on proliferation, senescence, and apoptosis of dorsal root ganglion cells in Vitro. Med Sci Monit. 2018;24:7841–7849.
- Kampanis V, Tolou-Dabbaghian B, Zhou L, et al. Cyclic stretch of either PNS or CNS located nerves can stimulate neurite outgrowth. Cells. 2020;10(1):1.
- Calvo M, Bennett DLH. The mechanisms of microgliosis and pain following peripheral nerve injury. Exp Neurol. 2012;234(2):271–282.
- Hu P, McLachlan EM. Macrophage and lymphocyte invasion of dorsal root ganglia after peripheral nerve lesions in the rat. Neuroscience. 2002;112(1):23–38.
- Watkins LR, Maier SF. Beyond neurons: evidence that immune and glial cells contribute to pathological pain states. Physiol Rev. 2002;82(4):981–1011.
- Mor D, Bembrick AL, Austin PJ, et al. Anatomically specific patterns of glial activation in the periaqueductal gray of the sub-population of rats showing pain and disability following chronic constriction injury of the sciatic nerve. Neuroscience. 2010;166(4):1167–1184.
- Schmid AB, Nee RJ, Coppieters MW. Reappraising entrapment neuropathies-Mechanisms, diagnosis and management. Manual Ther. 2013;18(6):449–457.
- Fiore NT, Austin PJ. Are the emergence of affective disturbances in neuropathic pain states contingent on supraspinal neuroinflammation? Brain Behav Immun. 2016;56:397–411.
- Chapman CR, Tuckett RP, Song CW. Pain and stress in a systems perspective: reciprocal neural, endocrine, and immune interactions. J Pain. 2008;9(2):122–145.
- Albrecht DS, Ahmed SU, Kettner NW, et al. Neuroinflammation of the spinal cord and nerve roots in chronic radicular pain patients. Pain. 2018;159(5):968–977.
- Lutke Schipholt I, Coppieters M, Meijer O, et al. Effects of joint and nerve mobilisation on neuroimmune responses in animals and humans with neuromusculoskeletal conditions: a systematic review and meta-analysis. Pain Rep. 2021;6(2):e927.
- Gao YJ, Zhang YQ, Zhao ZQ. Involvement of spinal neurokinin-1 receptors in the maintenance but not induction of carrageenan-induced thermal hyperalgesia in the rat. Brain Res Bull. 2003;61(6):587–593.
- Hoot MR, Sim-Selley LJ, Selley DE, et al. Chronic neuropathic pain in mice reduces μ-opioid receptor-mediated G-protein activity in the thalamus. Brain Res. 2011;1406:1–7.
- Dai WL, Yan B, Bao YN, et al. Suppression of peripheral NGF attenuates neuropathic pain induced by chronic constriction injury through the TAK1-MAPK/NF-κB signaling pathways. Cell Commun Signal. 2020;18(1):1.
- Dubový P, Klusáková I, Hradilová-Svíženská I, et al. Activation of astrocytes and microglial cells and CCL2/CCR2 upregulation in the dorsolateral and ventrolateral nuclei of periaqueductal gray and rostral ventromedial medulla following different types of sciatic nerve injury. Front Cell Neurosci. 2018;12. DOI:https://doi.org/10.3389/fncel.2018.00040.
- Ferreira G, Stieven F, Araujo F, et al. Neurodynamic treatment did not improve pain and disability at two weeks in patients with chronic nerve-related leg pain: a randomised trial. J Physiother. 2016;62(4):197–202.
- Nee RJ, Vicenzino B, Jull GA, et al. Neural tissue management provides immediate clinically relevant benefits without harmful effects for patients with nerve-related neck and arm pain: a randomised trial. J Physiother. 2012;58(1):23–31.
- Wolny T, Linek P. Long-term patient observation after conservative treatment of carpal tunnel syndrome: a summary of two randomised controlled trials. PeerJ. 2019;2019:11.
- Ayub A, Osama M, Shakil UR, et al. Effects of active versus passive upper extremity neural mobilization combined with mechanical traction and joint mobilization in females with cervical radiculopathy: a randomized controlled trial. J Back Musculoskelet Rehabil. 2019;32(5):725–730.
- Fernandez-Carnero J, Sierra-Silvestre E, Beltran-Alacreu H, et al. Neural tension technique improves immediate conditioned pain modulation in patients with chronic neck pain: a randomized clinical trial. Pain Med. 2019;20(6):1227–1235.
- Arumugam V, Selvam S, MacDermid JC. Radial nerve mobilization reduces lateral elbow pain and provides short-term relief in computer users. Open Orthop J. 2014;17(8):368–371.
- Andrade RJ, Freitas SR, Hug F, et al. The potential role of sciatic nerve stiffness in the limitation of maximal ankle range of motion. Sci Rep. 2018;8(1):14532.
- Andrade RJ, Freitas SR, Hug F, et al. Chronic effects of muscle and nerve-directed stretching on tissue mechanics. J Appl Physiol. 2020;129(5):1011–1023.
- Kantarci F, Ustabasioglu FE, Delil S, et al. Median nerve stiffness measurement by shear wave elastography: a potential sonographic method in the diagnosis of carpal tunnel syndrome. Eur Radiol. 2014;24(2):434–440.
- Dikici AS, Ustabasioglu FE, Delil S, et al. Evaluation of the tibial nerve with shear-wave elastography: a potential sonographic method for the diagnosis of diabetic peripheral neuropathy. Radiology. 2017;282(2):494–501.
- Celebi UO, Burulday V, Ozveren MF, et al. Sonoelastographic evaluation of the sciatic nerve in patients with unilateral lumbar disc herniation. Skeletal Radiol. 2019;48(1):129–136.
- Neto T, Freitas SR, Andrade RJ, et al. Noninvasive measurement of sciatic nerve stiffness in patients with chronic low back related leg pain using shear wave elastography. J Ultrasound Med. 2019;38(1):157–164.
- Wang Q, Zhang H, Zhang J, et al. The relationship of the shear wave elastography findings of patients with unilateral lumbar disc herniation and clinical characteristics. BMC Musculoskelet Disord. 2019;20(1):438.
- Neto T, Freitas SR, Andrade RJ, et al. Shear wave elastographic investigation of the immediate effects of slump neurodynamics in people with sciatica. J Ultrasound Med. 2020;39(4):675–681.
- Bueno FR, Shah SB. Implications of tensile loading for the tissue engineering of nerves. Tissue Eng Part B Rev. 2008;14(3):219–233.
- Driscoll PJ, Glasby MA, Lawson GM. An in vivo study of peripheral nerves in continuity: biomechanical and physiological responses to elongation. J Orthop Res. 2002;20(2):370–375.
- Lundborg G, Rydevik B. Effects of stretching the tibial nerve of the rabbit. A preliminary study of the intraneural circulation and the barrier function of the perineurium. J Bone Joint Surg Br. 1973;55(2):390–401.
- Ogata K, Naito M. Blood flow of peripheral nerve effects of dissection, stretching and compression. J Hand Surg. 1986;11B(1):10–14.
- Wall EJ, Massie JB, Kwan MK, et al. Experimental stretch neuropathy. Changes in nerve conduction under tension. J Bone Joint Surg Br. 1992;74-B(1):126–129.
- Dilley A, Lynn B, Pang SJ. Pressure and stretch mechanosensitivity of peripheral nerve fibres following local inflammation of the nerve trunk. Pain. 2005;117(3):462–472.
- Pagnez MAM, Corrêa LA, Almeida RS, et al. The variation of cross-sectional area of the sciatic nerve in flexion-distraction technique: a cross-sectional study. J Manipulative Physiol Ther. 2019;42(2):108–116.
- Millesi H, Zoch G, and Reihsner R. Mechanical properties of peripheral nerves. Clin Orthop Relat Res. 1995; 5(314):76–83.
- Ellis R, Richards N, Archer L, et al. Assessing sciatic nerve excursion and strain with ultrasound imaging during forward bending. Ultrasound Med Biol. 2021;47(9):2560–2569.
- Basson A, Olivier B, Ellis R, et al. The effectiveness of neural mobilization for neuromusculoskeletal conditions: a systematic review and meta-Analysis. J Orthop Sports Phys Ther. 2017;47(9):593–615.
- Ellis RF, Hing WA. Neural mobilization: a systematic review of randomized controlled trials with an analysis of therapeutic efficacy. J Man Manip Ther. 2008;16(1):8–22.
- Lim YH, Chee DY, Girdler S, et al. Median nerve mobilization techniques in the treatment of carpal tunnel syndrome: a systematic review. J Hand Ther. 2017;30(4):397–406.
- Neto T, Freitas SR, Andrade RJ, et al. Sciatic nerve stiffness is not changed immediately after a slump neurodynamics technique. Muscles Ligaments Tendons J. 2017;7(3):583–589.
- Su Y, Lim ECW. Does evidence support the use of neural tissue management to reduce pain and disability in nerve-related chronic musculoskeletal pain? A systematic review with meta-analysis. Clin J Pain. 2016;32(11):991–1104.
- Ellis R, Rohan M, Hitt JR, et al. Ultrasound elastography measurement of sciatic nerve displacement and shear strain during active and passive knee extension. J Ultrasound Med. 2018;37(8):2091–2103.
- Andrade RJ, Nordez A, Hug F, et al. Non-invasive assessment of sciatic nerve stiffness during human ankle motion using ultrasound shear wave elastography. J Biomech. 2016;49(3):326–331.
- Kouzaki K, Kobayashi M, Nakamura KI, et al. Repeated bouts of fast eccentric contraction produce sciatic nerve damage in rats. Muscle Nerve. 2016;54(5):936–942.
- Lee K, Kouzaki K, Ochi E, et al. Eccentric contractions of gastrocnemius muscle-induced nerve damage in rats. Muscle Nerve. 2014;50(1):87–94.
- Ochi E, Ueda H, Tsuchiya Y, et al. Eccentric contraction–induced muscle damage in human flexor pollicis brevis is accompanied by impairment of motor nerve. Scand J Med Sci Sports. 2020;30(3):462–471.
- Ridehalgh C, Barnard K. Principles of nerve treatment. In: Petty NJ, Barnard K, editors. Principles of musculoskeletal treatment and management: a handbook for therapists. 3rd ed ed. Edinburgh: Elsevier; 2018. p. 180–194.
- Shacklock MO. Clinical neurodynamics: a new system of neuromusculoskeletal treatment. Oxford: Butterworth Heinemann; 2005.
- Rodríguez-Sanz D, López-López D, Unda-Solano F, et al. Effects of median nerve neural mobilization in treating cervicobrachial pain: a randomized waiting list–controlled clinical trial. Pain Pract. 2018;18(4):431–442.
- Neto T, Freitas SR, Marques M, et al. Effects of lower body quadrant neural mobilization in healthy and low back pain populations: a systematic review and meta-analysis. Musculoskelet Sci Pract. 2017;27:14–22.
- Zusman M. Mechanisms of peripheral neuropathic pain: implications for musculoskeletal physiotherapy. Phys Ther Rev. 2008;13(5):313–323.