
ABSTRACT
This study investigates intergenerational relationships between the father’s personality disorder (PD) traits and the PD traits of his male and female offspring. We examine whether the intergenerational transmission of PD is due to the father transmitting a general vulnerability to all PDs, or whether the transmission is more specific to particular PDs. Structural Equation Modelling techniques are used to investigate a hypothesised model, based on Livesley’s [(2007). A framework for integrating dimensional and categorical classifications of personality disorder. Journal of Personality Disorders, 21(2), 199–224. https://doi.org/10.1521/pedi.2007.21.2.199] conceptualisation, which reorganises the DSM PD traits into four dimensions: Emotional Dysregulation, Dissocial Behaviour, Inhibitedness, and Compulsivity. General and specific transmission effects are examined for each model. The data comes from the Cambridge Study in Delinquent Development, a large-scale prospective longitudinal survey of 411 males and their biological offspring. Findings revealed that the intergenerational transmission of PD traits from fathers to female offspring appeared to be both general and disorder-specific. Firm conclusions could not be drawn about the intergenerational transmission of PD traits from fathers to male offspring, as the data did not fit the hypothesised model.
Introduction
Little is known about the intergenerational transmission of personality disorders (PDs) in community samples. The majority of studies focus on high-risk samples, and their findings may not be generalisable. However, it is known that, despite the low prevalence of PD in community samples, cases reaching clinical thresholds are still to be found. It has often been suggested that PDs should be viewed as dimensional rather than categorical constructs (Edens et al., Citation2006; Guay et al., Citation2007; Hare & Neumann, Citation2008), providing further rationale for examining their presence in community samples. To this end, this study analyses data from the Cambridge Study in Delinquent Development (CSDD), a prospective longitudinal study of the development of delinquent behaviour in a community sample of 411 males originally from south London. This article also presents findings from the most recently completed interview phase of the study, which involved tracing and interviewing biological children of the original study males.
We present analyses of the PD data collected from the third generation of the study (G3) and aim to build on previous analyses that examined the intergenerational transmission of criminal offending (see Auty et al., Citation2017; Farrington et al., Citation2009a; Farrington et al., Citation2017) and psychopathy (see Auty et al., Citation2015). The CSDD attempted to interview every biological child (aged 18 or over) of the original male cohort, so statistical techniques to take account of the non-independence of observations (children from the same family) are used throughout. This analysis looks at the influence of the father’s PD traits on those of his offspring. Male and female offspring are analysed separately, so that gender differences can also be explored. Only transmission to adult biological offspring is analysed, so that PD traits should be relatively stable.
Previous studies examining the impact of parental personality pathology on offspring have focused on the two broad domains of internalising and externalising disorders. Intergenerational associations for externalising psychopathology, such as offending, antisocial behaviour and conduct disorder, are well recognised (Besemer et al., Citation2017; Farrington et al., Citation1996; Frick & Loney, Citation2002; Rowe & Farrington, Citation1997; Thornberry et al., Citation2003). Internalising disorders have also demonstrated intergenerational relationships (Kim et al., Citation2009; Pettit et al., Citation2008). Less, however, is known about the intergenerational relationships of PDs, and no studies have examined intergenerational continuities of PD traits in a large community sample.
Mechanisms of intergenerational transmission
Three main mechanisms have been proposed to explain the intergenerational transmission of specific forms of psychopathology, such as depression (see Goodman & Gotlib, Citation1999), and these can be applied more generally to personality disorders. Firstly, the relationship between the personality disorder of parents and their offspring could be explained by genetic transmission. Results from numerous twin studies show that personality disorders are moderately heritable (Bouchard, Citation2004; Gjerde et al., Citation2012; Kendler & Prescott, Citation2006; Plomin et al., Citation2001)
Secondly, environmental risk factors specific to the mother, such as stress smoking or substance abuse, could have an effect on the prenatal development of the child (Wakschlag et al., Citation2002; Ward, Citation1991). Adverse prenatal conditions, such as maternal depression, have been linked to lower activity levels and limited response to social stimulation in the child (Field, Citation1992). Antenatal maternal stress and anxiety have been linked to pregnancy complications, lower gestational age and low birth weight (Glover, Citation1997), with one study finding that stress had a similar effect size as smoking and had significant relationship with head circumference and predicted poorer scores on a neurological examination, suggesting effects on brain development (Lou et al., Citation1994). Developmental problems thought to be consequences of prenatal exposure to drugs or alcohol have been well documented. As well as effects on the foetus’ growth and physical wellbeing (Coles et al., Citation1992), a recent review of current scientific literature on the impact of maternal cocaine and opioid use on children up to three years old, found their use to be related to infants’ growth, and behaviour, such as irritability, alertness, excitability and behaviour regulation, and cognitive and language development (Bandstra et al., Citation2010).
A third mechanism proposes that children are exposed to their parents’ maladaptive behaviour, which Johnson et al. (Citation2001) has shown mediates the relationship between parental and offspring psychiatric symptoms, whilst controlling for the effects of the offspring’s temperament and psychiatric disorders in adolescence. An important moderator of the effects of the parent’s behaviour is the amount of time the child is exposed to the parent. For example, Jaffee et al. (Citation2003) found that, for the offspring of fathers who engaged in low levels of antisocial behaviour, the less time he lived in the family home, the more conduct problems the offspring had. However, fathers with high levels of antisocial behaviour, who resided in the family home, predict poor behavioural outcomes for their children. The children suffer two disadvantages; increased genetic risk of antisocial personality disorder (PD) and being raised in a home environment unsuitable for successful child rearing. Similarly, Lamb (Citation1997) has argued that the amount of time fathers invest in child care is less closely associated with child outcomes than the quality of fathers’ involvement with their children. Furthermore, intergenerational relationships may be closer among same-sex pairs, as offspring may be more strongly influenced by the parent that is most similar to themselves, and several studies have found that parents have the greatest impact on same-sex children through their negative parenting (Deater-Deckard & Dodge, Citation1997; Koestner et al., Citation1991). Although internalising disorders and externalising disorders are known to be highly familial, the transmission of increased risk for offspring psychopathology is likely to be mediated by the interaction of genetic and psychosocial risk factors (Kramer, Citation2005; Rutter, Citation2005).
General or disorder-specific transmission of personality disorders
Studies of the familial nature of externalising and internalising disorders have suggested that the intergenerational transmission of these problem behaviours tends to be general rather than disorder-specific. Parents seem to pass on ‘a vulnerability to a spectrum of disorders’ (Hicks et al., Citation2004, p. 926) to their offspring, rather than an increased risk for a particular disorder. Hicks et al.’s (Citation2004) genetically informative twin study examined whether the transmission of externalising disorders (conduct disorder, antisocial PD, and drug and alcohol dependence) was due to a transmission of general or disorder-specific vulnerability. In their sample of 542 families, they found that general transmission and not disorder-specific transmission accounted for intergenerational similarities. This general vulnerability to externalising disorders was highly heritable, according to their estimates. However, they did find disorder-specific effects between siblings (for conduct disorder, and drug and alcohol dependence). They hypothesised that this indicated the effect of environmental factors that were independent of the parents’ externalising disorders, for example the role of peers.
Some studies focusing on the transmission of externalising disorders have revealed inconsistent findings. Hicks (Citation2004) notes that family and adoption studies found evidence of specific transmission effects for externalising disorders, yet twin studies reported considerable overlap of externalising syndromes, leading Hicks to conclude that the aetiology of externalising disorders was due to a general externalising (EXT) factor that was highly heritable. Few studies have considered both general and specific transmission at the same time, and even fewer have examined the transmission of internalising disorders as well. Some of these studies are reviewed below.
In an adoption study of 785 adolescents from 402 families, Keyes et al. (Citation2008) examined the effects of parental smoking on the disinhibited behaviour of offspring. Their statistical analyses found several significant interactions between adoption status and the disinhibited behaviour of offspring, for example that the effect of being exposed to parental smoking was greater for offspring in biological families, compared to those in adoptive families. An increased non-specific genetic risk for several disinhibited behaviours was transmitted in biologically-related families, increasing the offspring’s risk for a wide range of externalising behaviours including tobacco and marijuana use, alcohol use, disruptive behaviour disorder, delinquency, antisocial attitudes and low harm avoidance.
In their analyses of data from the Minnesota Twin Family Study, Bornovalova et al. (Citation2010) tested general and specific transmission effects of four parental externalising disorders (conduct disorder, antisocial behaviour, alcohol dependence and drug dependence) on three childhood disruptive disorders (attention deficit hyperactivity disorder, conduct disorder and oppositional defiant disorder). Similar to Hicks et al. (Citation2004), they did not find any specific transmission effects from parents to their 11-year old offspring, but they did find specific transmission effects between siblings for each of the childhood disruptive disorders. Similarly, Grove et al. (Citation1991) studied schizotypy traits in the first-degree relatives of schizophrenics. They observed that schizophrenia is, in general, not highly concentrated within families, but they found that many of the general schizotypy traits were. They concluded that familial transmission was explained by a single factor that predisposed individuals to schizotypy traits and an elevated risk for schizophrenia.
There is some evidence that different types of parental PD do contribute to specific problems in their offspring. In a study of the children of mothers with borderline PD, higher scores on the temperament dimension of harm avoidance were demonstrated by their children. Moreover, the children tended to perceive their mothers as being overly protective. These children also exhibited a higher prevalence of emotional and behavioural problems than comparison groups and described themselves as having very low self-esteem (Barnow et al., Citation2006). Narcissistic PD is also thought to show strong intergenerational relationships. Rappoport (Citation2005) argues that narcissistic parents often have offspring who are either narcissistic or co-dependent, because of the parents’ inability to engage emotionally with their children's needs.
Gender
Studies examining the effects of gender on intergenerational transmission of personality pathology have produced mixed results and the role of the offspring’s gender remains unclear. A study of broad internalising and externalising disorders in a three-generation community sample by Kim et al. (Citation2009) found some quite complex gender-specific pathways. The analysis indicated that men’s and women’s internalising and externalising traits were associated with the traits of their offspring, in both the same PD domain and the opposite PD domain. For example, mothers’ internalising behaviour had a strong relationship with the internalising traits of both their male and female offspring, but the son’s externalising behaviour was predicted by their mother’s internalising and externalising behaviour. Generally, they found that the influence of fathers was limited.
Thomas et al. (Citation1995) reported some gender effects of parental depression on children’s development. That is, maternal depressive traits were significantly related to daughters’ internalising behaviour, whereas paternal depressive traits were significantly related to sons’ internalising behaviour. Ge et al. (Citation1995) found that paternal depression was significantly related to daughters’ depression, whereas maternal depression was predictive of sons’ depression only.
Studies examining the influence of parental psychopathology on the development of problem behaviours has traditionally focussed on mothers, possibly due to the high prevalence of absent fathers. This has meant that the impact of fathers’ behaviour is less well understood (Phares, Citation1992). More recently, Connell and Goodman (Citation2002) examined the growing body of research on both maternal and paternal factors associated with internalising and externalising problems in children. Their meta-analysis of 134 independent samples included many more recent studies. When comparing the strength of association between psychopathology in mothers and fathers and internalising and externalising disorders in their children, they found that associations were stronger for maternal rather than paternal psychopathology and for internalising rather than externalising problems in children (Connell & Goodman, Citation2002). Therefore, further examination of intergenerational associations for PDs is needed in order to clarify the impact of the personality pathology of the father on their offspring.
DSM personality disorders
Many empirical studies have failed to replicate the 10 DSM diagnostic categories, revealing that PDs are not distinct from each other and that there is substantial overlap of diagnostic criteria (Eaton et al., Citation2011). The DSM classification system assumes that the features of PDs are organised into 10 separate diagnostic entities, and this system has been criticised for inadequate structural validity: ‘the universe of personality disorder constructs is not accurately parsed as 10 latent categories’ (Krueger et al., Citation2011, p. 186). The overlap of diagnostic criteria means that discriminant validity is also low (Widiger & Clark, Citation2000). The diagnostic concepts bear little resemblance to typical clinical presentations and a meta-analysis revealed that personality disorder not otherwise specified (PDNOS) was the third most frequently used diagnosis in structured interview studies and the most frequently used personality diagnosis in nonstructured interview studies (Verheul & Widiger, Citation2004). In the case of broad diagnoses such as borderline PD and antisocial PD, the diagnostic criteria identify a group of individuals who are so heterogeneous that the value of the category has been questioned by Stone (Citation1980), who wondered whether borderline PD was a diagnosis worth retaining. Lykken (Citation1995) made similar remarks with regard to antisocial PD. In short, studies have shown that there are large differences between clinical concepts and models based on empirical data. Studies have failed to find discrete categories; PDs are continuously distributed in the population (Benjamin, Citation1996). The current DSM classification does not ‘carve nature at its joints’ (McCullagh, Citation1980, p. 200).
The empirical evidence seems to suggest that four major dimensions underlie the domain of PD (Hart, Citation1998; Millon & Davis, Citation1996). An ICD-11 literature review also drew similar conclusions (Anthony & Cohler, Citation1987), finding four dimensions; asocial / schizoid; dissocial/antisocial; obsessional/anankastic; and anxious/dependent. Livesley (Citation2007) developed an evidence-based dimensional classification and identified four domains of PD; emotional dysregulation, socially avoidant, dissocial and compulsive. There is further evidence for the four-factor structure from behavioural genetic studies, which suggest firstly that the four-factor structure reflects the genetic architecture of PD traits (Capaldi et al., Citation2012) and secondly, that there is genetic continuity between normal and disordered personality traits (Kendler et al., Citation2013).
The current study
This study investigates the intergenerational transmission of PD traits (as measured using the SCID-II: First et al., Citation1997) to discover whether a general vulnerability is transmitted from fathers to offspring or whether an increased risk for a specific PD is transmitted. The proposed model involves the alternative four-factor model of PD developed by Livesley (Citation1986).
Materials and methods
Participants
The Cambridge Study in Delinquent Development (CSDD) is a prospective longitudinal survey of the origins of offending and antisocial behaviour, based on an original sample of 411 males from south London. The study began in 1961–62 when the participants were selected by taking all the boys (aged 8–9) from the registers of six state primary schools that were within a one-mile radius of the study’s office. The socioeconomic background of the sample was predominantly white (87% white, British origin) and working class (94% had a father with a skilled, semi-skilled or manual occupation, compared to the national figure at that time, which was 78%). The original male participants are referred to as G2 (generation two) and their biological children as G3 (generation three). Analyses of the information collected from the original study males and their parents (generation one – G1) can be found in six books (Farrington et al., Citation2013; Piquero et al., Citation2007; West, Citation1969; West, Citation1982; West & Farrington, Citation1973; West & Farrington, Citation1977) and in seven summary articles (Farrington, Citation1995, Citation2003, Citation2019, Citation2021b; Farrington et al., Citation2009b; Farrington & West, Citation1981; Farrington & West, Citation1990).
The G2 males were last contacted during the period 1999–2004 for a social and medical interviews: 365 of 394 men who were still alive were interviewed (93%). Of 343 who completed the social interview face-to-face (others who were abroad had a telephone or postal interview), 304 (89%) also completed the face-to-face medical interview. This included an assessment of the traits of the 10 DSM PDs using the screening questionnaire of the Structured Clinical Interview for Axis II Personality Disorders (SCID-II; First et al., Citation1997). The medical interview was administered to the G2 males by a qualified and trained forensic psychiatrist.
From 2004 to 2011, 518 (82.2% of the 630 eligible children born up to 1992) of their biological offspring (G3) were interviewed and assessed for PD using the paper-and-pencil version of the SCID II. The data from the 518 offspring interviews was then matched with their fathers’ data. 48 offspring could not be matched as their father had not taken part in the medical interview: seven others had fathers who had died before the medical interview, 17 offspring could not complete the SCID-II assessment as they lived abroad and their interview was conducted over the telephone and one G3 individual did not complete the assessment due to the interview being curtailed. This resulted in a sample of 452 man and child pairs (230 fathers and sons, 222 fathers and daughters) on which the current analysis is based.
The G3 offspring were only contacted for interview if their father had been interviewed previously. We were required to seek his (or his female partner’s) agreement to interviewing his child in order to meet the ethical standards of the South East England Regional Medical Ethics Committee. At each interview, written informed consent was obtained from all participants.
Measures
SCID-II screening questionnaire
PD traits were measured using the screening questionnaire of the Structured Clinical Interview for DSM-IV Personality Disorders (SCID-II: Spitzer et al., Citation1990). The SCID-II is a well-established measure that has demonstrated acceptable sensitivity and specificity (Ekselius et al., Citation1994). The G3 participants completed a paper-based, self-administered questionnaire containing 116 questions and were asked to respond either ‘yes’, ‘no’ or ‘don’t know’ to each one. Each question assessed one of the 10 Axis II PDs (avoidant, dependent, obsessive-compulsive, paranoid, schizotypal, schizoid, histrionic, narcissistic, borderline, and antisocial) of the DSM-IV (American Psychiatric Association, Citation1994). The diagnostic criteria for schizotypal and histrionic PD include several items that can only be rated by an observer (for example: ‘displays rapidly shifting and shallow expression of emotions’). These items were rated as part of the medical questionnaire and were added to supplement the data from the screening questionnaire.
Analytical approach
Variables were created to indicate the number of traits of each PD that each respondent endorsed. Counts were used to increase statistical power as the number of participants reaching diagnostic thresholds in community samples is considerably lower than in clinical samples. Also, PD traits can still cause significant impairment to an individual even when they are below a diagnostic cut-point (Gotlib et al., Citation1995). It has also been argued that dimensional rather than categorical representations of PDs are a more accurate reflection of clinical reality (Clark, Citation2007; Widiger & Simonsen, Citation2005), and that they better capture the true nature of PDs (Hopwood et al., Citation2011; Oldham & Skodol, Citation2000; Skodol et al., Citation2005; Widiger & Samuel, Citation2005).
Structural equation modelling was used to investigate whether the transmission of domains of PD from fathers to their offspring was general or disorder-specific. Structural equation modelling (SEM) tests hypotheses about causal relationships between variables, and models are often depicted pictorially to aid understanding. The transmission of PD traits was investigated by testing a model that reorganises the PD traits into four domains, and therefore has four observed variables.
The PD trait counts were positively skewed, as is often the case in community samples. This means that if the maximum likelihood (ML) method is used, standard errors and chi-squares may be incorrect. Using weighted least-squares (WLS) would be an alternative solution to this problem, but this method requires a very large sample, so normal scores were calculated in PRELIS, the preprocessor for LISREL (Du Toit et al., Citation2001, p. 143).
Given the non-independence of our observed variables (the PD trait counts from individuals, some of whom were from the same family), multilevel confirmatory factor models (structural equation models) were specified in LISREL (version 9.1). Therefore, the multi-group ‘$CLUSTER’ option was used to obtain a robust variance estimate that adjusts for within-cluster correlation. The multi-group analysis creates models for two groups, one for ‘within families’ and a second one for ‘between families’. This approach to multilevel structural equation modelling was developed by Muthen (Citation1994). Two covariance matrices are produced (a between groups covariance matrix and a within groups covariance matrix) and analysed by LISREL.
Cases with missing data are dealt with in LISREL by listwise deletion. This resulted in the removal of one father and son dyad. The final sample for the SEM analysis was therefore 229 father and son dyads and 222 father and daughter dyads. In order for the model to be identified, the factor loading of one of the observed variables for every latent variable needs to be set to 1.0.
The fit of models was evaluated using several fit indices. Firstly, the X² fit statistic provides an overall estimate of model fit. In this instance we wish to retain our null hypothesis (that the proposed model fits the data), so a good fit is indicated by a nonsignificant chi-square value, or a chi-square value that is less than two times the degrees of freedom. Secondly, the root-mean-square error of approximation (RMSEA) provides an estimate of discrepancy in model fit per one degree of freedom; values less than 0.08 indicate a good fit to the data, and values less than 0.05 indicate a very good fit to the data. Thirdly, other fit indices such as a goodness-of-fit Index (GFI) and a comparative fit index (CFI), compare our model to the null or independence model. Values between 0.90 and 1.00 indicate a good fit to the data.
Model: based on Livesley’s four dimensions of personality disorder
To test Livesley’s (Citation2007) model of PD, the DSM-IV diagnostic criteria that were used to define and assess every PD were reorganised into 30 primary traits (see Livesley, Citation2007). The 30 primary traits were then organised into the four proposed domains of PD; emotional dysregulation, dissocial behaviour, inhibitedness and compulsivity (see ).
Table 1. Domains of personality disorder.
The proposed model () has two latent PD (G2PD & G3PD) variables. Each has the same four observed variables (EmDys = emotional dysregulation, Disso = dissocial behaviour, Inhib = inhibitedness, Compu = compulsivity), according to Livesley’s (Citation2007) representation. These are the normalised trait count variables for each dimension. The latent variables represent the features common to their observed variables. The latent error variables (the small circular variables to the left of each observed variable) represent the variances not explained by the latent variable that are specific to each observed variable. The unidirectional arrows that link the latent variables (from G2PD to G3PD) represent the general transmission effect, and this covariance is tested first. The two latent factors (G2PD and G3PD) are regressed on the observed variables. These arrows (on the right-hand side of the model) test the hypothesis that a general vulnerability to PD is transmitted from fathers to their offspring.
Figure 1. Hypothesised two factor model of the intergenerational transmission of the four domains of personality disorder. Note: Fathers’ PD dimension variables: G2EmDys = Emotional Dysregulation, G2Disso = Dissocial Behaviour, G2Inhib = Inhibitedness, G2Compu = Compulsivity. Offspring’s PD dimension variables: G3EmDys = Emotional Dysregulation, G3Disso = Dissocial Behaviour, G3Inhib = Inhibitedness, G3Compu = Compulsivity.
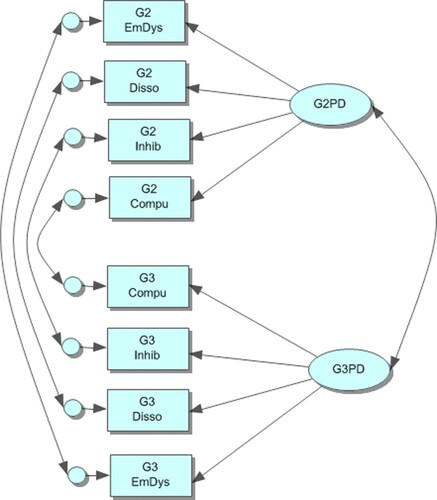
Modification Indices in the LISREL output can then be inspected to see if the model can be improved by adding an error covariance, shown by the bidirectional arrows on the left hand side of . These arrows link the residuals (or latent error terms) for each observed variable. They represent disorder-specific transmission that increases the similarity between the father and the offspring that is independent of the latent variable. Therefore, if the Modification Indices suggest that the model will be substantially improved by adding an error covariance between a specific fathers’ PD domain and the same domain in their offspring, this would suggest evidence of disorder-specific transmission, as the observed PD domain variables in each generation both have something in common that is not explained by their latent variable. The four error covariances are added to the model one at a time, to test for specific transmission effects.
Results
General and specific transmission of personality disorder domains
Male offspring
The intergenerational transmission of PD traits was explored using the four dimensions model (). Results of the model fitting are provided in . The first model tested allowed for only general transmission between the two latent variables; G2PD and G3PD. Although it provided quite a poor fit to the data (χ2 = 99.16, df = 38, p ≤ 0.001; RMSEA = 0.084, GFI = 0.949, CFI = 0.951), the modification indices suggested that the fit of the model would be improved if some specific transmission effects were included into the model. Therefore, residual covariances were added one at a time to test for disorder-specific transmission effects. Results of these tests are given in under ‘Specific transmission effects’. We did not detect any form of disorder-specific transmission from fathers to male offspring for the inhibitedness and emotional dysregulation dimensions. Very weak disorder-specific transmission effects were detected for the dissocial behaviour and compulsivity dimensions. The inclusion of these effects into the model did improve model fit slightly, but generally the overall fit of even the best fitting model, which included both of these effects, was quite poor (χ2 = 66.89, df = 35, p = <0.001; RMSEA = 0.063, GFI = 0.965, CFI = 1.00; see ). The final path diagram for this model is shown in . The path diagram shows that the general transmission effect between the two latent variables ‘G2PD’ and ‘G3PD’ is very small (0.05) and not statistically significant. The specific transmission effect between ‘G2 Compulsivity’ and ‘G3 Compulsivity’ is also quite small (0.303) and not statistically significant. The specific transmission effect between ‘G2 Dissocial Behaviour’ and ‘G3 Dissocial Behaviour’ is also small (0.172) and also not significant.
Figure 2. Intergenerational transmission of Livesley’s (Citation2007) four domains of personality disorder from G2 fathers to G3 male offspring.
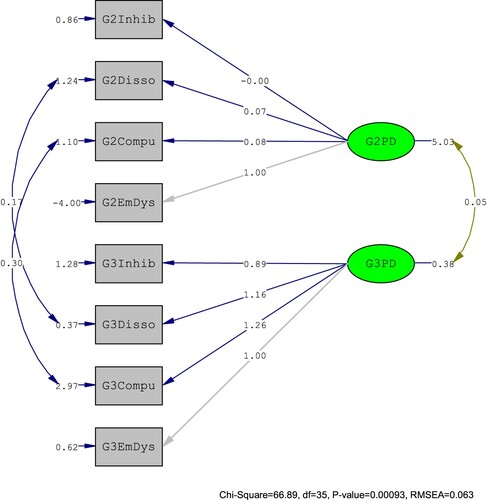
Table 2. Indices of fit for alternative models for the intergenerational transmission of personality disorder.
The path diagram also reveals that the estimated factor loadings are all positive, except one. The loadings represent the size of the expected change in the observed variable for a one unit increase in its latent variable. The largest of these is 1.26, and this is the coefficient for the regression of G3 Dissocial Behaviour on the latent variable G3PD. We can also see that the estimated factor loadings for the fathers’ PD domains are somewhat smaller than those for their male offspring. Inspecting the output for this model reveals that all parameter estimates for the G3 males are statistically significant (p < 0.05), but those for the G2 males are not significant. The output for this model also reveals a Heywood case.Footnote1 In this model, the error variance for the observed variable ‘G2EmDys’ (G2 emotional dysregulation) is negative. This is most likely to be caused by very low prevalence of traits of this domain amongst the G2 males.
Female offspring
The intergenerational transmission of PD traits was then explored with the female sample. The results of the model fitting process are shown in the bottom panel of . The first model, which allowed for only a general transmission, provided an inadequate fit to the data (χ2 = 68.97, df = 38, p = 0.00156; RMSEA = 0.061, GFI = 0.962, CFI = 0.328). The modification indices suggested that the inclusion of some disorder-specific transmission effects would greatly increase the fit of the model. Specific transmission effects were examined one at a time for each dimension, as shown in . The addition of specific transmission effects for the Dissocial Behaviour and Compulsivity dimensions greatly increased the fit of the model. The final model is shown in . It included the general transmission effect, and two specific effects, providing an acceptable fit to the data (χ2 = 44.84, df = 35, p = 0.12316; RMSEA = 0.036, GFI = 0.975, CFI = 1.000). The χ2 value roughly approximates the number of degrees of freedom. The fit of the final model is discussed in more detail below.
Figure 3. Intergenerational transmission of Livesley’s (Citation2007) four domains of personality disorder from G2 fathers to G3 female offspring.
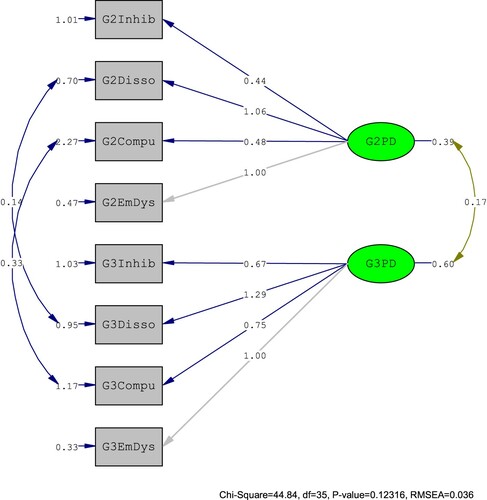
The path diagram in reveals that the estimated factor loadings are all positive and the LISREL output revealed that they all had small standard errors. The loadings represent the size of the expected change in the observed variable (the PD trait count variable) for a one unit increase in its latent variable. The largest of these for the G2 PD dimensions is 1.06, which is the coefficient for the regression of ‘G2 Dissocial Behaviour’ on the latent variable ‘G2 PD’. The largest loading for the G3 PD dimensions is also for G3 ‘Dissocial Behaviour’ (1.29). All parameter estimates are statistically significant (p < 0.05).
The path diagram also shows that the general transmission effect between the two latent variables ‘G2PD’ and ‘G3PD’ is somewhat larger than in the male model (0.17), and the output revealed that it is also statistically significant (p = 0.037). The specific transmission effect between ‘G2 Compulsivity’ and ‘G3 Compulsivity’ is quite small (0.330) and not statistically significant. The specific transmission effect between ‘G2 Dissocial Behaviour’ and ‘G3 Dissocial Behaviour’ is also small (0.137) and almost significant (p = 0.0753). Therefore, weak dimension-specific transmission effects for fathers and their female offspring were detected, particularly for the Dissocial Behaviour dimension, and for the Compulsivity dimension.
The R2 values tell us how well our observed variables measure the underlying construct of PD. In our model the R2 values show a mixture of weak and strong measures, with the strongest measure of G2 PD being the indicator G2 Emotional Dysfunction, indicating that 45.5% of its variance can be explained by G2 PD. The weakest measure is G2 Compulsivity, indicating that only 3.9% of its variance can be explained by its latent variable G2 PD. The strongest measure of G3 PD is also the G3 Emotional Dysfunction observed variable, indicating that 64.2% of its variance can be explained by the latent variable G3 PD. The weakest measure is G3 Inhibitedness, indicating that 20.5% of its variance can be explained by its latent variable G3 PD.
Examining the fit statistics for the model as a whole provides further evidence that the model provides a good fit to the data. The Root Mean Square Error of Approximation (RMSEA) value for our model is 0.036 (values less than 0.05 are thought to indicate good fit). The Goodness-of-Fit Index (GFI) for our model is 0.98 indicating a good fit (a value close to 1.00). Finally, the Comparative Fit Index (CFI) for our model was 1.00 indicating a good fit to the data.
Discussion
This analysis provided some of the first evidence of the intergenerational transmission of PD traits in a large community sample. We looked at whether the transmission of personality disorder traits was general or disorder-specific. The model reorganised the DSM PD traits into four domains; Emotional Dysregulation, Dissocial Behaviour, Inhibitedness, and Compulsivity. The model for males suggested that there were some disorder-specific transmission effects, so two error covariances were added to the model, but neither were found to be statistically significant and the output revealed another Heywood case affecting the G2 Emotional Dysregulation variable, again probably caused by low prevalences of PD traits in the G2 male sample. The model for females fitted the data quite well. A non-significant general transmission effect was found, and the female model was improved by adding specific transmission effects, for both Compulsivity (largest transmission effect) and Dissocial Behaviour (second largest specific transmission effect). The specific transmission effect for Dissocial Behaviour was found to be almost significant.
Both the male and the female models were improved by adding specific transmission effects, both for Compulsivity (largest transmission effect) and Dissocial Behaviour (the second largest specific transmission effects). These two are probably most closely related to externalising behaviours, although it is interesting that a specific transmission effect was not found for disinhibited behaviour.
The results suggest that a model organised around four domains of personality fits the structure of PD traits in this community sample. The four-factor model fitted well for females. The specific transmission effects found in the structural equation models in this article in contrast to the other studies that found quite different results and little evidence of specific transmission effects, probably reflects the fact that we have looked at a much broader range of psychopathology than the previous studies reviewed earlier, particularly Hicks et al. (Citation2004), who only looked at externalising disorders.
There are some important limitations to the study. Firstly, the screening instrument has been shown by several studies to inflate the diagnoses of PDs by approximately 20%, compared to the full SCID-II interview (Ekselius et al., Citation1994). However, this is a limitation with all screening instruments, and studies often have to make compromises due to time and funding constraints, yet still achieve a sample size large enough for statistical analyses. Although several studies have shown that manipulating diagnostic thresholds leads to improvements in sensitivity and specificity, most studies have only found acceptable levels of concordance between data from screening questionnaires and clinician ratings (Ekselius et al., Citation1994; Ullrich et al., Citation2008). Because of these concerns, PD traits were analysed as dimensional constructs, but problems surrounding over-diagnosis with screening instruments still apply to some extent.
The mode of administration of the SCID-II screening questionnaire also needs to be mentioned briefly, as it could be a further limitation. The SCID-II screening questionnaire was the final section of the G3 social interview that lasted, on average, one hour and 41 min. It is possible that interviewees were tired by this stage; many interviewees complained about the length of the questionnaire. The G2 males’ SCID-II was completed in a separate medical interview and was not part of the social interview. This difference in method could be responsible for some of the differences in PD traits in the two generations.
Criticisms of the use of self-completion questionnaires are often made. It is suggested that they are inappropriate to assess certain types of PD where lack of personal insight or dishonesty are features of the disorder. They also receive further criticism because some PDs, particularly schizotypal PD, involve traits which ideally need to be observed by a clinician, such as ‘odd thinking and speech’ and ‘inappropriate or constricted affect’ (two of the traits for schizotypal PD). The present analysis attempted to compensate for this by using data from the Screening Version of the Hare Psychopathy Checklist (PCL: SV; Hart et al., Citation1995), because these observed items had been rated as part of the PCL: SV assessment.
Secondly, structural equation modelling (SEM) has several limitations as a data analytic technique. Some relevant general concerns are described below, but much more detailed criticisms can be found in Tomarken and Waller (Citation2004), Barrett (Citation2007), Bentler (Citation2007), and Steiger (Citation2007). SEM models are approximations, and the technique cannot be used to definitely establish that any particular model is correct. Furthermore, even SEM models that appear to fit the data well can have additional problems; one of the most common criticisms of SEM is that important variables may have been omitted from the model. Therefore we cannot assume that a model that fits the data well includes all the key influencing variables. Tomarken and Waller (Citation2003) have cautioned that the indices that are commonly used to evaluate the fit of a model can often be too lenient. They refer to several simulation studies that have provided some evidence that statistics used to assess fit are dependent on many other different factors, including the size of the sample, the number of parameters in the model and the method used to estimate the model, and are not sufficiently sensitive to misspecified models. Ultimately, determining model fit can be quite subjective (Marsh et al., Citation2004), so caution is advisable when interpreting results.
Livesley’s (Citation2007) model could also be criticised for the way traits are allocated to each of the four domains (see ); some traits are assigned to one domain, yet could arguably belong to another, for example, the oppositional trait forms part of the Emotional Dysregulation trait, yet may be more conceptually related to the Dissocial Behaviour domain. The same argument may also apply to some of the other primary traits.
Finally, the extent to which PD traits are stable across the life course is a matter of debate. The G2 males were approximately 48 years old when they completed the SCID-II questionnaire, but the average age of the G3 offspring when they completed the assessment was 25 years old. It is probable that the PD traits in the G2 male sample have declined as they have got older and therefore differences in prevalences are explained by age. Several studies have shown that normal personality traits display high levels of stability, often for periods as long as 30 years (Cadoret et al., Citation1995; Jaffee et al., Citation2003; Livesley et al., Citation1993). However, Bierut et al. (Citation1999) have provided evidence to suggest that the severity of PD traits declines with age.
Despite these problems, we would argue that we have demonstrated a plausible model of the intergenerational transmission of PDs from fathers to female offspring. More research is needed to investigate this transmission for male offspring.
Implications
The challenge is to translate research findings into effective policy interventions. It is essential that empirical findings are useable.
Policy interventions can be made at two levels to prevent intergenerational continuities in personality difficulties: Firstly, preventative programmes can be targeted at young children who are at high risk of negative outcomes, because of their exposure to environmental risk factors. Secondly, programmes can be targeted at parents who have personality difficulties. These interventions are valuable as both the parent and their children will benefit. For reviews of intervention programmes, see Farrington (Citation2021a)
Parent training programmes have been developed as response to research evidence that deficiencies in the parenting of antisocial parents have a causal role in the development of antisocial and possibly later criminal behaviour in their offspring. Several approaches to parent training have been developed, most notably by Patterson (Citation1982) and Webster-Stratton (Citation2000). Parent training programmes teach parents to implement a structured approach of rewards, appropriate punishments, active engagement and supervision with their child. Evidence suggests that this approach will improve the behaviour of their child (and the parent–child relationship) in the short term and reduce future negative outcomes for children, such as becoming involved in antisocial or criminal behaviour. Parent training progrmmeams have been the subject of several systematic reviews and meta-analyses, which provide results highlighting their effectiveness. For example, in a recent systematic review and meta-analysis of 28 Randomized controlled trials Michelson et al. (Citation2013) found that parent management training had significant benefits for the treatment of children with disruptive behaviour. A Cochrane review (Barlow et al., Citation2014) has shown that parenting programmes can also have positive benefits for parental psychosocial wellbeing. They reviewed 48 studies and found that attendance at group-based parenting programmes led to significant reductions in parental depression, anxiety, stress, anger, guilt and improvements in confidence and levels of satisfaction with their partner relationship in the short-term. Effects on stress and confidence were still significant after six months.
Research has shown that those with antisocial PD and severe mental illness often have comorbid substance misuse disorders. These individuals also have higher prevalence rates of substance misuse; they start using substances at an early age and become addicted more quickly. There are substantial costs associated with their health and also for their family. They also frequently involved with the criminal justice system. Clearly, effective interventions are needed. Often there is a very strong family history of substance misuse which contributes to a more stressful family home life. Mueser (Citation2003) suggests that as those with severe personality disorders and substance misuse disorders would benefit from intensive community-based treatment approaches. He advocates an Assertive Community Treatment (ACT) model which is an intensive programme, which engages the whole family, who become part of the treatment programme. It and is provided in settings that are familiar to the client. Mueser (Citation2003) has also suggested that those with antisocial PD and substance misuse disorders respond well to ‘contingent reinforcement’ as family members offer to lend money to substance dependent family members, and this both worsens their addiction and causes arguments in the family home. Interventions based on this problem solving approach have shown initial promising results with reductions in substance misuse up to two years after treatment.
Whether the intergenerational transmission of PD is general or specific has important implications for interventions. For example, it is desirable to identify factors that mediate PD transmission. In previous research (Auty et al., Citation2015), the father’s employment problems was identified as an important mediator of PD transmission. This suggests that, in order to reduce PD transmission, it would be advantageous to try to improve the father’s employment history, for example in a programme such as the National Supported Work Demonstration Project (Uggen, Citation2000). However, if PD transmission is specific, it would be desirable to (a) identify persons who are most at risk of a particular type of PD transmission (e.g. those who have emotional dysregulation), and (b) identify the specific mediators of this specific type of PD transmission that should then be targeted in intervention programmes. This surely would prove to be a beneficial research agenda for the future.
Acknowledgements
The authors wish to thank all the families involved in the CSDD.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 The APA Dictionary of Psychology defines a Heywood case as ‘any correlation coefficient, regression coefficient, factor loading, or similar parameter estimate having a value that is impossible or very rare (e.g., a negative error variance estimate). Heywood cases may indicate any of the following: a sample that is too small to adequately estimate the parameters; data that do not have a normal distribution or that contain outliers; a misspecified model that is not appropriate for the data; or a parameter whose true value is so close to a boundary (e.g., 1 or 0) in the population that its estimate exceeded this limit due to sampling fluctuation’ (VandenBos, Citation2015). See also Heywood and Filon (Citation1931).
References
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). APA Press.
- Anthony, E. J., & Cohler, B. J. (1987). The invulnerable child. Guilford Press.
- Auty, K. M., Farrington, D. P., & Coid, J. W. (2015). Intergenerational transmission of psychopathy and mediation via psychosocial risk factors. The British Journal of Psychiatry, 206(1), 26–31. https://doi.org/https://doi.org/10.1192/bjp.bp.114.151050
- Auty, K. M., Farrington, D. P., & Coid, J. W. (2017). The intergenerational transmission of criminal offending: Exploring gender-specific mechanisms. British Journal of Criminology, 57(1), 215–237. https://doi.org/https://doi.org/10.1093/bjc/azv115
- Bandstra, E. S., Morrow, C. E., Mansoor, E., & Accornero, V. H. (2010). Prenatal drug exposure: Infant and toddler outcomes. Journal of Addictive Diseases, 29(2), 245–258. https://doi.org/https://doi.org/10.1080/10550881003684871
- Barlow, J., Smailagic, N., Huband, N., Roloff, V., & Bennett, C. (2014). Group-based parent training programmes for improving parental psychosocial health. Cochrane Database Syst Rev, 5, CD002020. https://doi.org/https://doi.org/10.1002/14651858.CD002020
- Barnow, S., Spitzer, C., Grabe, H. J., Kessler, C., & Freyberger, H. J. (2006). Individual characteristics, familial experience, and psychopathology in children of mothers with borderline personality disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 45(8), 965–972. https://doi.org/https://doi.org/10.1097/01.chi.0000222790.41853.b9
- Barrett, P. (2007). Structural equation modelling: Adjudging model fit. Personality and Individual Differences, 42(5), 815–824. https://doi.org/https://doi.org/10.1016/j.paid.2006.09.018
- Benjamin, L. S. (1996). Interpersonal diagnosis and treatment of personality disorders (2nd ed.). Guilford.
- Bentler, P. M. (2007). On tests and indices for evaluating structural models. Personality and Individual Differences, 42(5), 825–829. https://doi.org/https://doi.org/10.1016/j.paid.2006.09.024
- Besemer, S., Ahmad, S. I., Hinshaw, S. P., & Farrington, D. P. (2017). A systematic review and meta-analysis of the intergenerational transmission of criminal behavior. Aggression and Violent Behavior, 37, 161–178. https://doi.org/https://doi.org/10.1016/j.avb.2017.10.004
- Bierut, L. J., Heath, A. C., Bucholz, K. K., Dinwiddie, S. H., Madden, P. A. F., Statham, D. J., Dunne, M. P., & Martin, N. G. (1999). Major depressive disorder in a community-based twin sample. Are there different genetic and environmental contributions for men and women? Archives of General Psychiatry, 56(6), 557–563. https://doi.org/https://doi.org/10.1001/archpsyc.56.6.557
- Bornovalova, M. A., Hicks, B. M., Iacono, W. G., & McGue, M. (2010). Familial transmission and heritability of childhood disruptive disorders. American Journal of Psychiatry, 167(9), 1066–1074. https://doi.org/https://doi.org/10.1176/appi.ajp.2010.09091272
- Bouchard, T. J. (2004). Genetic influence on human psychological traits. Current Directions in Psychological Science, 13(4), 148–151. https://doi.org/https://doi.org/10.1111/j.0963-7214.2004.00295.x
- Cadoret, R. J., Yates, W. R., Troughton, E., Woodworth, G., & Stewart, M. A. (1995). Genetic-environmental interaction in the genesis of aggressivity and conduct disorders. Archives of General Psychiatry, 52(11), 916–924. https://doi.org/https://doi.org/10.1001/archpsyc.1995.03950230030006
- Capaldi, D. M., Pears, K. C., Kerr, D. C. R., Owen, L. D., & Kim, H. K. (2012). Growth in externalizing and internalizing problems in childhood: A prospective study of psychopathology across three generations. Child Development, 83(6), 1945–1959. https://doi.org/https://doi.org/10.1111/j.1467-8624.2012.01821.x
- Clark, L. A. (2007). Assessment and diagnosis of personality disorder: Perennial issues and an emerging reconceptualization. Annual Review of Psychology, 58(1), 227–257. https://doi.org/https://doi.org/10.1146/annurev.psych.57.102904.190200
- Coles, C. D., Platzman, K. A., Smith, I., James, M. E., & Falek, A. (1992). Effects of cocaine and alcohol use in pregnancy on neonatal growth and neurobehavioral status. Neurotoxicology and Teratology, 14(1), 23–33. https://doi.org/https://doi.org/10.1016/0892-0362(92)90025-6
- Connell, A. M., & Goodman, S. H. (2002). The association between psychopathology in fathers versus mothers and children's internalizing and externalizing behavior problems: A meta-analysis. Psychological Bulletin, 128(5), 746–773. https://doi.org/https://doi.org/10.1037/0033-2909.128.5.746
- Deater-Deckard, K., & Dodge, K. (1997). Externalizing behavior problems and discipline revisited: Nonlinear effects and variation by culture, context, and gender. Psychological Inquiry, 8(3), 161–175. https://doi.org/https://doi.org/10.1207/s15327965pli0803_1
- Du Toit, M., Du Toit, S., & Hawkins, D. M. (2001). Interactive LISREL: User's guide. Scientific Software International. Incorporated.
- Eaton, N. R., Krueger, R. F., South, S. C., Simms, L. J., & Clark, L. A. (2011). Contrasting prototypes and dimensions in the classification of personality pathology: Evidence that dimensions, but not prototypes, are robust. Psychological Medicine, 41(6), 1151–1163. https://doi.org/https://doi.org/10.1017/S0033291710001650
- Edens, J. F., Marcus, D. K., Lilienfeld, S. O., & Poythress Jr., N. G. (2006). Psychopathic, not psychopath: Taxometric evidence for the dimensional structure of psychopathy. Journal of Abnormal Psychology, 115(1), 131–144. http://ovidsp.ovid.com/athens/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=ovfth&AN=00004468-200602000-00015http://sfx.library.qmul.ac.uk/qmsfx?sid=OVID&isbn=&issn=0021-843X&volume=115&issue=1&date=2006&title=Journal+of+Abnormal+Psychology&atitle=Psychopathic%2C+Not+Psychopath%3A+Taxometric+Evidence+for+the+Dimensional+Structure+of+Psychopathy.&aulast=Edens%2C+John&spage=131 https://doi.org/https://doi.org/10.1037/0021-843X.115.1.131
- Ekselius, L., Lindström, E., von Knorring, L., Bodlund, O., & Kullgren, G. (1994). SCID II interviews and the SCID screen questionnaire as diagnostic tools for personality disorders in DSM-III-R. Acta Psychiatrica Scandinavica, 90(2), 120–123. https://doi.org/https://doi.org/10.1111/j.1600-0447.1994.tb01566.x
- Farrington, D. P. (1995). The development of offending and antisocial behaviour from childhood: Key findings from the Cambridge study in delinquent development. Journal of Child Psychology and Psychiatry, 36(6), 929–964. https://doi.org/https://doi.org/10.1111/j.1469-7610.1995.tb01342.x
- Farrington, D. P. (2003). Key results from the first 40 years of the Cambridge study in delinquent development. In T. P. Thornberry, & M. D. Krohn (Eds.), Taking stock of delinquency: An overview of findings from contemporary longitudinal studies (pp. 137–183). Kluwer/Plenum.
- Farrington, D. P. (2019). The Cambridge study in delinquent development. In D. Eaves, C. D. Webster, Q. Haque, & J. Eaves-Thalken (Eds.), Risk rules: A practical guide to structured professional judgement and violence prevention (pp. 225–233). Pavilon Publishing.
- Farrington, D. P. (2021a). The developmental evidence base: Prevention. In D. A. Crighton, & G. J. Towl (Eds.), Forensic psychology (3rd ed., pp. 263–293). Wiley.
- Farrington, D. P. (2021b). New findings in the Cambridge study in delinquent development. In J. C. Barnes, & D. R. Forde (Eds.), The encyclopedia of research methods in criminology and criminal justice. Hoboken: Wiley. In Press.
- Farrington, D. P., Barnes, G. C., & Lambert, S. (1996). The concentration of offending in families. Legal and Criminological Psychology, 1(1), 47–63. https://doi.org/https://doi.org/10.1111/j.2044-8333.1996.tb00306.x
- Farrington, D. P., Coid, J. W., & Murray, J. (2009a). Family factors in the intergenerational transmission of offending. Criminal Behaviour and Mental Health, 19(2), 109–124. https://doi.org/https://doi.org/10.1002/cbm.717
- Farrington, D. P., Coid, J. W., & West, D. J. (2009b). The development of offending from age 8 to age 50: Recent results from the Cambridge study in delinquent development. Monatsschrift fur Kriminologie und Strafrechtsreform (Journal of Criminology and Penal Reform), 92(2), 160–173. https://doi.org/https://doi.org/10.1515/mks-2009-922-306
- Farrington, D. P., Piquero, A. R., & Jennings, W. G. (2013). Offending from childhood to late middle age: Recent results from the Cambridge study in delinquent development. Springer.
- Farrington, D. P., Ttofi, M. M., & Crago, R. V. (2017). Intergenerational transmission of convictions for different types of offenses. Victims & Offenders, 12(1), 1–20. https://doi.org/https://doi.org/10.1080/15564886.2016.1187693
- Farrington, D. P., & West, D. J. (1981). The Cambridge study in Delinquent development. In S. A. Mednick, & A. E. Baert (Eds.), Prospective longitudinal research: An empirical basis for the primary prevention of psychosocial disorders (pp. 137–145). Oxford University Press.
- Farrington, D. P., & West, D. J. (1990). The Cambridge study in delinquent development: A long-term follow-up of 411 London males. In H. J. Kerner, & G. Kaiser (Eds.), Kriminalitat: Personlichkeit, Lebensgeschichte und Verhalten (Criminality: Personality, behaviour and life history) (pp. 115–138). Springer-Verlag.
- Field, T. (1992). Infants of depressed mothers. Development and Psychopathology, 4(01), 49–66. https://doi.org/https://doi.org/10.1017/S0954579400005551
- First, M. B., Gibbon, M., Spitzer, R. L., Benjamin, L. S., & Williams, J. B. (1997). Structured clinical interview for DSM-IV Axis-II personality disorders. Washington, D.C: American Psychiatric Press.
- Frick, P. J., & Loney, B. R. (2002). Understanding the association between parents and child antisocial behavior. In R. J. McMahon, & R. D. Peters (Eds.), The effects of parental dysfunction on children (pp. 105–126). Kluwer Academic/Plenum Publishers.
- Ge, X., Conger, R. D., Lorenz, F. O., Shanahan, M., & Elder Jr., G. H. (1995). Mutual influences in parent and adolescent psychological distress. Developmental Psychology, 31(3), 406–419. https://doi.org/https://doi.org/10.1037/0012-1649.31.3.406
- Gjerde, L. C., Czajkowski, N., Røysamb, E., Ørstavik, R. E., Knudsen, G. P., Østby, K., Torgersen, S., Myers, J., Kendler, K. S., & Reichborn-Kjennerud, T. (2012). The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire. Acta Psychiatrica Scandinavica, 126(6), 448–457. https://doi.org/https://doi.org/10.1111/j.1600-0447.2012.01862.x
- Glover, V. (1997). Maternal stress or anxiety in pregnancy and emotional development of the child. The British Journal of Psychiatry, 171(2), 105–106. https://doi.org/https://doi.org/10.1192/bjp.171.2.105
- Goodman, S. H., & Gotlib, I. H. (1999). Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review, 106(3), 458–490. https://doi.org/https://doi.org/10.1037/0033-295x.106.3.458
- Gotlib, I. H., Lewinsohn, P. M., & Seeley, J. R. (1995). Symptoms versus a diagnosis of depression: Differences in psychosocial functioning. Journal of Consulting and Clinical Psychology, 63(1), 90–100. https://doi.org/https://doi.org/10.1037/0022-006x.63.1.90
- Grove, W. M., Lebow, B. S., Clementz, B. A., Cerri, A., Medus, C., & Iacono, W. G. (1991). Familial prevalence and coaggregation of schizotypy indicators: A multitrait family study. Journal of Abnormal Psychology, 100(2), 115–121. https://doi.org/https://doi.org/10.1037/0021-843x.100.2.115
- Guay, J.-P., Ruscio, J., Knight, R. A., & Hare, R. D. (2007). A taxometric analysis of the latent structure of psychopathy: Evidence for dimensionality. Journal of Abnormal Psychology, 116(4), 701–716. https://doi.org/https://doi.org/10.1037/0021-843x.116.4.701
- Hare, R. D., & Neumann, C. S.. (2008). Psychopathy as a clinical and empirical construct. Annual Review of Clinical Psychology, 4(1), 217–246. https://doi.org/https://doi.org/10.1146/annurev.clinpsy.3.022806.091452
- Hart, S. D. (1998). Psychopathy and risk for violence. In D. J. Cooke, A. Forth, & R. D. Hare (Eds.), Psychopathy: Theory, Research and Implications for society (pp. 355–373). Kluwer Academic Publishers.
- Hart, S. D., Cox, D. J., & Hare, R. D. (1995). Manual for the Psychopathy Checklist: Screening Version (PCL:SV). Multi-Health Systems.
- Heywood, H. B., & Filon, L. N. G. (1931). On finite sequences of real numbers. Proceedings of the Royal Society of London. Series A, Containing Papers of a Mathematical and Physical Character, 134(824), 486–501. https://doi.org/https://doi.org/10.1098/rspa.1931.0209
- Hicks, B .M., Krueger, R. F., & Iacono, W. G. (2004). Family transmission and heritability of externalizing disorders: A twin-family study. Archives of General Psychiatry, 61, 922–928.
- Hicks, B. M., Krueger, R. F., Iacono, W. G., McGue, M., & Patrick, C. J. (2004). Family transmission and heritability of externalizing disorders: A twin-family study. Archives of General Psychiatry, 61(9), 922–928. https://doi.org/https://doi.org/10.1001/archpsyc.61.9.922
- Hopwood, C. J., Malone, J. C., Ansell, E. B., Sanislow, C. A., Gill, C. M., McGlashan, T. H., Pinto, A., Markowitz, J. C., Shea, M. T., Skodol, A. E., Gunderson, J. G., Zanarini, M. C., & Morey, L. C. (2011). Personality assessment in DSM-5: Empirical support for rating severity, style and traits. Journal of Personality Disorders, 25(3), 305–320. <Go to ISI>://WOS:000291369900003. https://doi.org/https://doi.org/10.1521/pedi.2011.25.3.305.
- Jaffee, S. R., Moffitt, T. E., Caspi, A., & Taylor, A. (2003). Life with (or without) father: The benefits of living with two biological parents depend on the father's antisocial behavior. Child Development, 74(1), 109–126. https://doi.org/https://doi.org/10.1111/1467-8624.t01-1-00524
- Johnson, J. G., Cohen, P., Kasen, S., Smailes, E., & Brook, J. S. (2001). Association of maladaptive parental behavior with psychiatric disorder among parents and their offspring. Archives of General Psychiatry, 58(5), 453–460. https://doi.org/https://doi.org/10.1001/archpsyc.58.5.453
- Kendler, K. S., Aggen, S. H., & Patrick, C. J. (2013). Familial influences on conduct disorder reflect two genetic factors and one shared environmental factor. Archives of General Psychiatry, 70(1), 78–86. https://doi.org/https://doi.org/10.1001/jamapsychiatry.2013.267
- Kendler, K. S., & Prescott, C. A. (2006). Genes, environment, and psychopathology: Understanding the causes of psychiatric and substance use disorders. Guilford Press.
- Keyes, P. D. M., Legrand, P. D. L., Iacono, P. D. W., & McGue, P. D. M. (2008). Parental smoking and adolescent problem behavior: An adoption study of general and specific effects. American Journal of Psychiatry, 165(10), 1338–1344. https://doi.org/https://doi.org/10.1176/appi.ajp.2008.08010125
- Kim, H. K., Capaldi, D. M., Pears, K. C., Kerr, D. C. R., & Owen, L. D. (2009). Intergenerational transmission of internalising and externalising behaviours across three generations: Gender-specific pathways. Criminal Behaviour and Mental Health, 19(2), 125–141. https://doi.org/https://doi.org/10.1002/cbm.708
- Koestner, R., Zuroff, D., & Powers, T. (1991). Family origins of adolescent self-criticism and its continuity into adulthood. Journal of Abnormal Psychology, 100(2), 191–197. https://doi.org/https://doi.org/10.1037/0021-843X.100.2.191
- Kramer, D. A. (2005). Commentary: Gene-environment interplay in the context of genetics, epigenetics, and gene expression. Journal of the American Academy of Child & Adolescent Psychiatry, 44(1), 19–27. http://ovidsp.ovid.com/athens/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=ovftg&AN=00004583-200501000-00004; http://sfx.library.qmul.ac.uk/qmsfx?sid=OVID&isbn=&issn=0890-8567&volume=44&issue=1&date=2005&title=Journal+of+the+American+Academy+of+Child+%26+Adolescent+Psychiatry&atitle=Commentary%3A+Gene-Environment+Interplay+in+the+Context+of+Genetics%2C+Epigenetics%2C+and+Gene+Expression.&aulast=KRAMER%2C+DOUGLAS&spage=19 https://doi.org/https://doi.org/10.1097/01.chi.0000145804.30112.6b
- Krueger, R. F., Eaton, N. R., Clark, L. A., Watson, D., Markon, K. E., Derringer, J., Skodol, A., & Livesley, W. J. (2011). Deriving an empirical structure of personality pathology for DSM-5. Journal of Personality Disorders, 25(2), 170–191. https://doi.org/https://doi.org/10.1521/pedi.2011.25.2.170
- Lamb, M. E. (1997). Fathers and child development: An introductory overview and guide. In M. E. Lamb (Ed.), The role of the father in child development (3rd ed., pp. 1–18). Wiley.
- Livesley, W. J. (2007). A framework for integrating dimensional and categorical classifications of personality disorder. Journal of Personality Disorders, 21(2), 199–224. https://doi.org/https://doi.org/10.1521/pedi.2007.21.2.199
- Livesley, W .J. (1986). Trait and behavioral prototypes of personality disorder. American Journal of Psychiatry, 143, 728–732.
- Livesley, W. J., Jang, K. L., Jackson, D. N., & Venon, P. A. (1993). Genetic and environmental contributions to dimensions of personality disorder. American Journal of Psychiatry, 150(12), 1826–1831. https://doi.org/https://doi.org/10.1176/ajp.150.12.1826
- Lou, H. C., Hansen, D., Nordentoft, M., Pryds, O., Jensen, F., Nim, J., & Hetnmingsen, R. (1994). Prenatal stressors of human life affect fetal brain development. Developmental Medicine & Child Neurology, 36(9), 826–832. https://doi.org/https://doi.org/10.1111/j.1469-8749.1994.tb08192.x
- Lykken, D. T. (1995). The Antisocial Personalities. Hillsdale, NJ: Erlbaum.
- Marsh, H. W., Hau, K.-T., & Wen, Z. (2004). In search of golden rules: Comment on hypothesis-testing approaches to setting cut-off values for fit indexes and dangers in overgeneralizing Hu and Bentler's (1999) findings. Structural Equation Modeling: A Multidisciplinary Journal, 11(3), 320–341. https://doi.org/https://doi.org/10.1207/s15328007sem1103_2
- McCullagh, P. (1980). Regression models for ordinal data. Journal of the Royal Statistical Society. Series B (Methodological), 42(2), 109–142. https://doi.org/https://doi.org/10.1111/j.2517-6161.1980.tb01109.x
- Michelson, D., Davenport, C., Dretzke, J., Barlow, J., & Day, C. (2013). Do evidence-based interventions work when tested in the “real world?” A systematic review and meta-analysis of parent management training for the treatment of child disruptive behavior. Clinical Child and Family Psychology Review, 16(1), 18–34. https://doi.org/https://doi.org/10.1007/s10567-013-0128-0
- Millon, T., & Davis, R. D. (1996). Disorders of personality: DSM-IV and beyond. J. Wiley.
- Mueser, K. T. (2003). Integrated treatment for dual disorders: A guide to effective practice. Guilford Press.
- Muthen, B. O. (1994). Multilevel covariance structure analysis. Sociological Methods & Research, 22(3), 376–398. https://doi.org/https://doi.org/10.1177/0049124194022003006
- Oldham, J. M., & Skodol, A. E. (2000). Charting the future of Axis II. Journal of Personality Disorders, 14(1), 17–29. https://doi.org/https://doi.org/10.1521/pedi.2000.14.1.17
- Patterson, G. R. (1982). Coercive family process. Castalia.
- Pettit, J. W., Olino, T. M., Roberts, R. E., Seeley, J. R., & Lewinsohn, P. M. (2008). Intergenerational transmission of internalizing problems: Effects of parental and grandparental major depressive disorder on child behavior. Journal of Clinical Child and Adolescent Psychology, 37(3), 640–650. https://doi.org/https://doi.org/10.1080/15374410802148129
- Phares, V. (1992). Where's poppa? The relative lack of attention to the role of fathers in child and adolescent psychopathology. American Psychologist, 47(5), 656–664. https://doi.org/https://doi.org/10.1037/0003-066x.47.5.656
- Piquero, A. R., Farrington, D. P., & Blumstein, A. (2007). Key issues in criminal career research: New analyses of the Cambridge study in delinquent development. Cambridge University Press.
- Plomin, R., Defries, J. D., Mcclearn, G. E., & Mcguffin, P. (2001). Behavioral genetics (4th ed.). Worth Publishers.
- Rappoport, A. (2005). Co-narcissism: How we accommodate to narcissistic parents. The Therapist, 16(2), 36–48.
- Rowe, D. C., & Farrington, D. P. (1997). The familial transmission of criminal convictions. Criminology; An interdisciplinary Journal, 35(1), 177–202. https://doi.org/https://doi.org/10.1111/j.1745-9125.1997.tb00874.x
- Rutter, M. (2005). Environmentally mediated risks for psychopathology: Research strategies and findings. Journal of the American Academy of Child & Adolescent Psychiatry, 44(1), 3–18. http://ovidsp.ovid.com/athens/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=ovftg&AN=00004583-200501000-00003http://sfx.library.qmul.ac.uk/qmsfx?sid=OVID&isbn=&issn=0890-8567&volume=44&issue=1&date=2005&title=Journal+of+the+American+Academy+of+Child+%26+Adolescent+Psychiatry&atitle=Environmentally+Mediated+Risks+for+Psychopathology%3A+Research+Strategies+and+Findings.&aulast=RUTTER%2C+MICHAEL&spage=3 https://doi.org/https://doi.org/10.1097/01.chi.0000145374.45992.c9
- Skodol, A. E., Oldham, J. M., Bender, D. S., Dyck, I. R., Stout, R. L., Morey, L. C., Shea, M. T., Zanarini, M. C., Sanislow, C. A., Grilo, C. M., McGlashan, T. H., & Gunderson, J. G. (2005). Dimensional representations of DSM-IV personality disorders: Relationships to functional impairment. American Journal of Psychiatry, 162(10), 1919–1925. https://doi.org/https://doi.org/10.1176/appi.ajp.162.10.1919
- Spitzer, R. L., Williams, J. B. W., Gibbon, M., & First, M. B. (1990). The structured clinical interview for DSM-II Axis II (SCID-II). American Psychiatric Press.
- Steiger, J. H. (2007). Understanding the limitations of global fit assessment in structural equation modeling. Personality and Individual Differences, 42(5), 893–898. https://doi.org/https://doi.org/10.1016/j.paid.2006.09.017
- Stone, M. H. (1980). The borderline syndromes: Constitution, personality, and adaptation. Tata McGraw-Hill Education.
- Thomas, A. M., Forehand, R., & Neighbours, B. (1995). Changes in maternal depressive mood: Unique contribution to adolescent functioning over time. Adolescence, 30(117), 43–52.
- Thornberry, T. P., Freeman-Gallant, A., Lizotte, A. J., Krohn, M. D., & Smith, C. A. (2003). Linked lives: The intergenerational transmission of antisocial behavior. Journal of Abnormal Child Psychology, 31(2), 171–184. https://doi.org/https://doi.org/10.1023/a:1022574208366
- Tomarken, A. J., & Waller, N. G. (2003). Potential problems with ‘well fitting’ models. Journal of Abnormal Psychology, 112(4), 578–598. https://doi.org/https://doi.org/10.1037/0021-843x.112.4.578
- Tomarken, A. J., & Waller, N. G. (2004). Structural equation modeling: Strengths, limitations, and misconceptions. Annual Review of Clinical Psychology, 1(1), 31–65. https://doi.org/https://doi.org/10.1146/annurev.clinpsy.1.102803.144239
- Uggen, C. (2000). Work as a turning point in the life course of criminals: A duration model of age, employment, and recidivism. American Sociological Review, 65(4), 529–546. https://doi.org/https://doi.org/10.2307/2657381
- Ullrich, S., Deasy, D., Smith, J., Johnson, B., Clarke, M., Broughton, N., & Coid, J. (2008). Detecting personality disorders in the prison population of England and Wales: Comparing case identification using the SCID-II screen and the SCID-II clinical interview. Journal of Forensic Psychiatry & Psychology, 19(3), 301–322. https://doi.org/https://doi.org/10.1080/14789940802045182
- VandenBos, G. R. (2015). APA dictionary of psychology. American Psychological Association.
- Verheul, R., & Widiger, T. A. (2004). A meta-analysis of the prevalence and usage of the personality disorder not otherwise specified (PDNOS) diagnosis. Journal of Personality Disorders, 18(4), 309–319. https://doi.org/https://doi.org/10.1521/pedi.2004.18.4.309
- Wakschlag, L. S., Pickett, K. E., Cook, E., Benowitz, N. L., & Leventhal, B. L. (2002). Maternal smoking during pregnancy and severe antisocial behavior in offspring: A review. American Journal of Public Health, 92(6), 966–974. https://doi.org/https://doi.org/10.2105/AJPH.92.6.966
- Ward, A. J. (1991). Prenatal stress and childhood psychopathology. Child Psychiatry & Human Development, 22(2), 97–110. https://doi.org/https://doi.org/10.1007/BF00707788
- Webster-Stratton, C. (2000). Incredible years trouble shooting guide. Umbrella Press.
- West, D. J. (1969). Present conduct and future delinquency. Heinemann.
- West, D. J. (1982). Delinquency: Its roots, careers and prospects. Heinemann.
- West, D. J., & Farrington, D. P. (1973). Who becomes delinquent? Heinemann.
- West, D. J., & Farrington, D. P. (1977). The delinquent way of life. Heinemann.
- Widiger, T. A., & Clark, L. A. (2000). Toward DSM—V and the classification of psychopathology. Psychological Bulletin, 126(6), 946–963. https://doi.org/https://doi.org/10.1037/0033-2909.126.6.946
- Widiger, T. A., & Samuel, D. B. (2005). Diagnostic categories or dimensions? A question for the diagnostic and statistical manual of mental disorders-fifth edition. Journal of Abnormal Psychology, 114(4), 494–504. https://doi.org/https://doi.org/10.1037/0021-843x.114.4.494
- Widiger, T. A., & Simonsen, E. (2005). Alternative dimensional models of personality disorder: Finding a common ground. Journal of Personality Disorders, 19(2), 110–130. https://doi.org/https://doi.org/10.1521/pedi.19.2.110.62628