
Abstract
Previous tailoring research has traditionally studied effects of system-initiated message content to match individual characteristics. Recently scholars have explored how tailoring health information to individual modality preferences and processing styles can increase message effectiveness. Using a web-based experiment among a representative sample of Internet users (N = 392; 25–86 years), this study investigated the underlying mechanisms that might explain the effects of mode tailoring on website attitudes and recall of online health information. Results from structural equation modeling showed that mode tailoring – enabling users to self-customize a health website’s presentation mode (via textual, visual, audiovisual information) – increased users’ perceived active control, which in turn contributed to higher perceived relevance and website engagement, and reduced cognitive load. Positive indirect effects of mode tailoring (vs. no tailoring) through these mechanisms were found for both website attitude and information recall. The findings suggest that perceived active control is the key driver of mode tailoring effects. Mode tailoring can be a promising and novel strategy to maximize the effectiveness of tailored health communications. The authors discuss the implications for theory and design of digital health information.
Online health information, such as health websites and patient portals, is increasingly used to supplement traditional methods of health education (e.g., doctor-patient communication, brochures). One of the relative advantages of web-based approaches for communicating health information is the ability to tailor content, structure and presentation to match individual information needs and preferences. Tailoring the content of health messages has shown to be more effective in influencing attitudes and behavior change compared to providing non-tailored information although effect sizes often remain small (Lustria et al., Citation2013; Noar, Benac, & Harris, Citation2007). As such, scholars have urged the importance of exploring novel ways of tailoring to maximize message effectiveness, such as tailoring the presentation mode to individual information modality preferences and processing styles (Smit, Linn, & Weert, Citation2015).
One assumption supporting the use of mode tailoring is that the way in which information is being delivered may affect how information is evaluated, processed, and remembered (Kreuter, Citation2000; Lang, Citation2006). The literature shows that individuals vary in their information mode preferences (e.g., textual vs. audiovisual online information), processing styles (e.g., verbal vs. visual learners), and cognitive motivations (e.g., low vs. high need for cognition; Bakker, Citation1999; Heo & Cho, Citation2009; Mayer & Massa, Citation2003). Moreover, recent studies examining different mode tailoring strategies – based on preference for charts and graphs versus illustrated visuals, and textual versus (audio)visual information – have shown favorable cognitive, evaluative and behavioral outcomes (Jensen, King, Carcioppolo, & Davis, Citation2012; Linn, Alblas, Van Weert, & Bol, Citation2015; Nguyen, Smets, Bol, Loos, & Van Weert, Citation2018; Nguyen et al., Citation2017).
Traditionally, tailoring starts with an assessment of individual characteristics, preferences and/or theoretical constructs related to the intended behavioral outcome, which is then used to design health messages that are deemed more personally relevant. An expert system collects user data, generates tailored messages based on an analysis of individual data, and delivers this information in a preplanned format. A different approach is to let the user initiate the tailoring process and customize information by selecting personally relevant elements. This is particularly suitable for online environments, and has shown promising effects on user evaluations and information processing in various contexts (e.g., Chung & Nah, Citation2009; Nguyen et al., Citation2017; Sundar & Marathe, Citation2010). With respect to mode tailoring, Nguyen et al. (Citation2017), (Citation2018) found that self-tailoring the mode of information presentation on a health website led to greater website satisfaction, increased attention, and better information recall. What remains relatively unclear, however, is what underlying processes drive the effects of user-initiated mode tailoring. Is mode-tailored information more effective because users have active control over the website, are able to engage with the content, select personally relevant information elements, and process information more easily?
This study sets out to understand why mode tailoring – i.e., adjusting information to individual preferences for presentation modality, using textual, visual, and/or audiovisual information – is effective. Specifically, we investigate which underlying mechanisms help explain the effects of mode tailoring on attitudinal (i.e., website attitude) and cognitive outcomes (i.e., information recall) regarding online health information. Gaining a better understanding of these underlying processes will enhance our understanding of why user-initiated mode tailoring (from now on ‘mode tailoring’) is effective. Ultimately, we aim to extend the existing theoretical models of tailoring and contribute to the literature on effective design of online health information.
Theoretical Approaches to Understand Mode Tailoring Effects
Both the elaboration likelihood model (ELM) and the limited capacity model of motivated mediated message processing (LC4MP) suggest that message processing is dependent on the ability and the motivation to process information (Lang, Citation2006; Petty, Barden, & Wheeler, Citation2002). According to the ELM, several factors may influence the ability to process information – the cognitive resources available to the individual, relevant knowledge and individual differences in need for cognition. Motivation to engage in an activity (e.g., attend to a message) also influences message processing. The ELM posits that when individuals perceive messages to be personally relevant, they are more likely to be motivated to process information more deeply (i.e., ‘central route’ processing) instead of superficially (i.e., ‘peripheral route’ processing), and consequently form more robust attitudes toward the message. Similarly, the LC4MP suggests that when individuals are motivated and are able to allocate sufficient cognitive resources to a message, the message will be successfully processed, stored in memory, and can be easily retrieved from memory (i.e., recalled) later. Together, the ELM and LC4MP suggest that for information to be evaluated more rigorously (i.e., website attitude) and processed adequately (i.e., information recall), designers should develop messages that may increase individuals’ motivation and ability to process information. In the following sections, we will elaborate on the mechanisms that play a role in optimizing processing conditions as afforded by mode tailoring.
The Facilitating Role of Perceived Active Control
User control theory suggests that providing people with control over the pace, order and content provided in online contexts (i.e., hypermedia) can increase the motivation to process information and improve learning ability, given individual differences in processing styles (Dillon & Jobst, Citation2005; Eveland & Dunwoody, Citation2001). As such, mode tailoring can enhance information processing in two ways. First, providing the option to toggle between presentation modes may increase feelings of active control over the information environment, which consequently enhances the motivation to attend to the message. Similarly, the option to choose the presentation mode and sense of active control may enhance the ability to process information by considering potential differences in cognitive abilities such as learning styles. As such, we expect perceived active control to be the main driver of mode tailoring effects by facilitating the motivation and ability to process information.
Moreover, perceived active control is recognized as an important sub-dimension of website interactivity (Liu & Shrum, Citation2002; McMillan & Hwang, Citation2002). In the context of online communications, Liu and Shrum (Citation2002) identified three dimensions – active control, two-way communication and synchronicity – that contribute to the overall perception of interactivity. In turn, research has underlined the positive effects of interactivity on improving engagement with, comprehension and processing of online health information; in promoting more positive attitudes toward health websites; and in creating more conducive environments for persuasion and behavior change (e.g., Kim & Stout, Citation2010; Lustria, Citation2007; Oh & Sundar, Citation2015). One study, where users were able to adapt the message sequence of an online intervention, highlighted the importance of perceived active control for information processing and persuasion outcomes (Kim & Stout, 2010). In line with these findings, user-initiated mode tailoring is likely to heighten perceived active control, consequently enhancing evaluative and cognitive responses. We focus on perceived active control, as research has shown that this is more predictive of outcomes than actual control (Voorveld, Neijens, & Smit, Citation2011).
H1: Mode tailoring will contribute to greater perceived active control, which will enhance (a) website attitude and (b) information recall.
Increasing Motivation: Perceived Relevance and Website Engagement
Several studies have shown that tailoring health messages to personal values, beliefs, preferences and characteristics increases the perceived relevance of the information, thereby increasing the motivation to attend to the information (Jensen et al., Citation2012; Kreuter & Wray, Citation2003; Lustria et al., Citation2016). Mode tailoring can also increase the perceived relevance of health information by giving users the ability to decide for themselves what information to consult and how to consult it. This sense of active control creates a situation in which the resulting information – the product of one’s own customization efforts – is personally relevant to the user (e.g., Kalyanaraman & Sundar, Citation2006; Marathe & Sundar, Citation2011). This, in turn, can lead to more positive website attitudes and better information recall.
H2: Mode tailoring contributes to greater perceived active control, which in turn heightens perceived relevance, consequently enhancing (a) website attitude and (b) information recall.
Tailored health information generally receives more attention and is processed more deeply than non-tailored information (e.g., Kreuter & Wray, Citation2003; Lustria et al., Citation2016). Previous research showed that tailored websites (vs. standard websites) are visited longer, revisited more often, and evaluated more positively by users (Crutzen et al., Citation2011; Danaher, Boles, Akers, Gordon, & Severson, Citation2006; Severson, Gordon, Danaher, & Akers, Citation2008). Such website engagement is an important prerequisite for information recall. The more users are engaged in organizing, encoding, and storing information at a self-paced rate, the more likely this information can be recalled correctly (Bol et al., Citation2016; Lang, Citation2006; Nguyen et al., Citation2017). Mode tailoring allows users to customize presentation formats, increasing perceptions of active control that may consequently increase users’ engagement in the website. This, in turn, is expected to lead to more positive website evaluations and higher information recall.
H3: Mode tailoring contributes to greater perceived active control, which in turn increases website engagement, consequently enhancing (a) website attitude and (b) information recall.
Increasing Ability: Perceived Cognitive Load
Until now, little is known about whether mode tailoring reduces the cognitive resources needed to process information. One idea is that mode tailoring facilitates information processing by adapting to individual cognitive abilities and processing styles. Overall, cognitive learning theories such as LC4MP (Lang, Citation2006) and cognitive theory of multimedia learning (CTML; Mayer, Citation2002) suggest that: (1) individuals have limited and vary in their capacity to process information, so multimodal presentations can aid information processing by reducing cognitive load, and (2) individuals automatically select, organize, and integrate content that makes sense to their unique situation (i.e., motivationally relevant message features). Following these principles, LC4MP and CTML lend support for mode tailoring, as the purpose of mode tailoring is for users to find an optimal fit between their individual information preferences, cognitive needs and processing styles on the one hand, and the mode(s) of information presentation on the other hand. In essence, enabling the ability to tailor the mode of presentation may help optimize processing conditions by reducing the cognitive load, thereby positively affecting website evaluations and information processing outcomes.
H4: Mode tailoring contributes to greater perceived active control, which in turn reduces cognitive load, consequently increasing (a) website attitude and (b) information recall.
Method
The current study explores the underlying mechanisms that explain the effects of mode tailoring on website attitudes and recall of online health information. To test the hypotheses, we conducted a between-subjects (condition: mode-tailored vs. standardized website) online experiment whereby study participants were exposed to a health-related website. The institutional review board from the Amsterdam School of Communication Research gave ethical approval for this study.
Procedure
We collected data through an online research panel of the ISO-certified research company Flycatcher (for other studies using Flycatcher’s research panel, see: Bol, Linn, Smets, Verdam, & Van Weert, Citation2020; Stanczyk, Crutzen, Bolman, Muris, & de Vries, Citation2013). From this panel, a representative sample of the Dutch general population were invited to participate in the study through an e-mail with a link to the online questionnaire. We created a stratified sample based on gender, level of education, and geographical distribution to create a sample representative of the Dutch population. Individuals under the age of 25 were not approached for participation, as colorectal cancer rarely affects those younger than 25 years (American Cancer Dutch Comprehensive Cancer Organisation, Citation2017; Society, Citation2017).
We informed participants that the study was about online health information. After a baseline survey for background information, participants were given a hypothetical scenario in which they had to visit a medical clinic in the near future to confirm a possible diagnosis of colorectal cancer. To prepare for this hypothetical visit, they were instructed to explore a website that contained information about their appointment and cancer diagnostics (see ‘Stimulus Materials’). Participants were randomly assigned to view either a mode-tailored or standardized version of the website. In the mode-tailored condition, participants were directed to a website where all the modes were switched off to ensure that they were able to select their own preferred mode(s). Participants could view the website as long as they wanted. Upon completing this task, we assessed mediating and outcome variables. Participants received a small financial incentive upon study completion.
Participants
Of the 515 Dutch adults who completed the questionnaire, 392 participants were included in the sample for analysis. Participants were excluded if they: (1) selected no presentation mode in the tailored condition (n = 31; see ‘Procedure’), or (2) did not view the website for ≥ 30 seconds, which was the minimum time needed to view the information (n = 24). We also excluded participants if they: (1) ignored the instructions by not closing the website before continuing with the questionnaire, interfering with our measurement of recall (n = 26); (2) ignored the instructions and did not open at least one of two webpages in addition to the homepage (n = 21); or (3) had technical problems during the study (n = 1). We also excluded participants for which we could not track website use data because they turned on private browsing (n = 71). As participants could meet more than one exclusion criterion, the numbers do not add up to the total number of participants excluded (n = 123).
The average age of our sample was 55 years (SD = 14.50), with a range from 25 to 86 years. About half of participants were male (52.8%). The sample consisted of people with varying levels of education (28.6% low education, 42.9% middle-high education, 28.6% high education). Participants reported an average Internet use of 20 hours per week (SD = 13.63, range 1–115), and had varying levels of Internet efficacy (M = 5.58, SD = 1.34, range 1–7).
Stimulus Materials
The study websites were based on an existing website of a multidisciplinary outpatient clinic in The Netherlands (from now on referred to as ‘the clinic’). The clinic is a highly specialized center that provides fast diagnostics in complex cases of colorectal cancer. Through this fast diagnosis procedure, patients are able to receive their diagnosis and treatment plan within one day. Given the intensity of fast diagnosis and the multiple consultations scheduled with different doctors (e.g., gastroenterologist, surgeon, oncologist), patients are strongly advised to read about various aspects of the procedure prior to their appointments. These materials are provided on their website. For the current study, we developed a website consisting of three webpages: a homepage, one webpage with general information about the clinic (e.g., the fast diagnostics procedure, which doctors they would meet), and one webpage with information on how patients could prepare for consultations (e.g., information about symptoms, what to bring to the appointment).
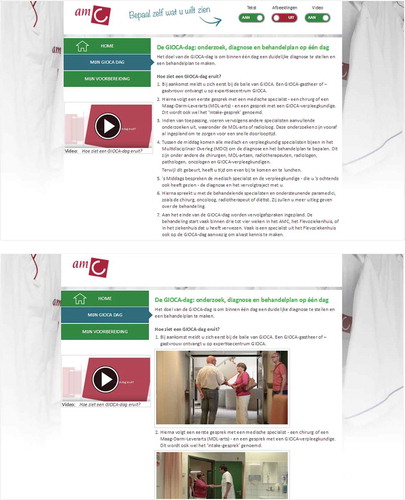
Both versions of the website (for experimental and control conditions) contained exactly the same health content including text, visuals and videos. The only difference was that participants assigned to the mode-tailored website could self-select their preferred modes of information presentation, while participants assigned to the control condition viewed the same content but did not have the ability to tailor presentation modes. On the mode-tailored website, tailoring was operationalized through an interactive built-in tool, enabling users to self-select whether online information would be presented through verbal (text), visual (pictures and illustrations), and/or audiovisual (videos) information in real-time (see for examples of the websites).
Figure 1. Mode-tailored website with text and video selected (top) and non-tailored standardized website with text, visuals and video (bottom).
Measures
Outcome Variables
Website attitude was measured with nine items (the website is creative, well developed, well organized, enjoyable, sophisticated, user-friendly, confusing [reverse coded], coherent, and the website looks nice) on a 7-point agreement scale (M = 5.13, SD = 1.06; α =.92). Items were based on the Website Satisfaction Scale (Bol et al., Citation2015; Van Weert et al., Citation2011) and previous research assessing website attitudes (Sundar & Marathe, Citation2010). We measured information recall with seven open-ended questions based on the website content (e.g., Which topics will be discussed with the healthcare providers?), using the method of the Netherlands Patient Information Recall Questionnaire (Jansen et al., Citation2008). We developed a codebook beforehand to allocate recall scores (0 = incorrect, 1 = partially correct, 2 = correct), which was converted to percentage correctly recalled (M = 25.82, SD = 22.07). Blinded double coding 19% of the recall answers (n = 74), showed good intercoder reliability (mean κ = .925, p < .001).
Mediating Variables
Perceived active control over the website was assessed with four items “I felt that I had a great deal of control over my visiting experience at this website” (M = 5.55, SD = 1.19; α = .92; Voorveld et al., Citation2011). Perceived relevance of the website was measured with three items, e.g. “the website seemed personally made for me” (M = 4.68, SD = 1.43; α = .87; Jensen et al., Citation2012; Lustria et al., Citation2016). We measured cognitive load with two items based on the Paas cognitive load scale, e.g. “viewing the information on the website took me a lot of effort” (reversely coded; M = 2.28, SD = 1.33; Pearson’s r = .77; Paas, Citation1992). We used 7-point agreement scales. Website engagement was measured by the time spent on the website in seconds (M = 361.27, SD = 424.82).
Manipulation Check
To check whether participants took note of the mode tailoring manipulation, they rated the statement “I could decide how the information was presented on the website” on a 7-point agreement scale (M = 5.21, SD = 1.70).
Background Variables
We measured socio-demographic information (i.e., age, gender and education level), participants’ experience with cancer (i.e., being diagnosed with cancer themselves and knowing someone being diagnosed with cancer), and Internet use in hours per week. Internet efficacy was measured with three items, e.g., “in general, I find websites easy to use” (Cronbach’s α = .94; Ajzen, Citation1991). We tracked participants’ website use with a built-in tracking system.
Statistical Analyses
Pearson’s correlations for all variables are reported in for the full sample (N = 392). We conducted t tests and Chi-square tests to test for successful manipulation and randomization. We tested the hypothesized model (H1–H4) with structural equation modeling (SEM) in AMOS version 22. Before model testing, we performed two steps to ensure multivariate normality for accurate maximum likelihood estimation. First, as distributions of the time variable ‘website engagement’ were skewed right, we log-transformed the data. Second, we used Mahalanobis distance method to identify outliers (n = 29) that exceeded the critical value at p < .05 (Kline, Citation2011). After log transformation and omission of outliers, multivariate normality assumptions were met (Multivariate kurtosis = 1.66, c.r. = 1.62; Kline, Citation2011).Footnote1 Model fit based on N = 363 was assessed with Chi-square, the root mean squared error of approximation (RMSEA), the standardized root mean square residual (SRMR), the Tucker-Lewis Index (TLI), the comparative fit index (CFI). To the model paths, bootstrapping was performed to obtain 95% bias-corrected confidence intervals based on 5,000 bootstrap iterations (Bollen & Stine, Citation1992). In the figures presenting the SEM analysis, measured/observed and latent variables are denoted with rectangles and circles, respectively.
Table 1. Descriptive statistics and correlation matrix of study variables (N = 392)
Results
Manipulation and Randomization Check
The manipulation of mode tailoring succeeded. Participants in the mode-tailored condition had higher perceptions of being able to decide how the website information was presented (M = 5.99, SD = 1.25) than those in the standardized condition (M = 4.54, SD = 1.76), t(390) = −9.32, p < .001. The randomization was successful. The conditions did not differ in any of the background variables.
Website Use Patterns
shows the website use patterns by condition. Participants (N = 392) spent 361 seconds on average on the website (about 6 minutes), with no difference between conditions, t(390) = 1.18, p = .237. Most participants visited all three pages (M = 2.87, SD = 0.34), with no difference between conditions, t(390) = 0.81, p = .417. Participants made on average nine (re)visits to these pages (M = 8.71, SD = 5.62). However, participants in the mode-tailored condition did this more often (M = 11.31) than those in the standardized condition (M = 6.43), t(336) = −9.34, p < .001. Furthermore, participants viewed on average one out of three videos (M = 0.91, SD = 0.99), playing 22.7% of the entire video (SD = 13.1%). Interestingly, participants on the mode-tailored website viewed on average less videos (M = 0.80) than those on the standardized website (M = 1.00), t(390) = 2.03, p = .043.
Table 2. Website use patterns of the mode-tailored and standardized website (N = 392)
With regard to mode actions on the mode-tailored website, participants made on average 5 clicks to (de)select the text, visuals, or video mode (M = 4.87, SD = 3.01). Most people started with text (76.0%), whereas a smaller number of people selected visuals (13.7%) or video (10.4%) as their first mode. The first mode selection was on average made around 18 seconds (SD = 15). During the entire website visit, the majority of the participants selected multimodal information (i.e., text, visuals and video: 84.7%; text and visuals: 8.7%; text + video: 0.5%; visuals and video: 0.5%) over unimodal information (i.e., text-only: 4.4%; visuals-only: 0.5%; video-only: 0.5%).
Model Testing
The hypothesized model (N = 363) showed a good fit to the data, χ2(9) = 18.11, p = .034, CMIN/DF = 2.012, TLI = .971, CFI = .987, RMSEA = .053, SRMR = .040 (Hooper, Coughlan, & Mullen, Citation2008).Footnote2 shows the standardized path coefficients and statistical significance for individual pathways in the hypothesized model. shows the estimates and confidence intervals of the direct, indirect effects and total effects of mode tailoring on website attitude and information recall.
Table 3. Standardized direct and indirect effects of mode tailoring on website attitude and information recall (N = 363)
Figure 2. Hypothesized model. Model fit (N = 363): χ2 (9) = 18.11, p =.034, CMIN/DF = 2.012, TLI = 0.971, CFI = 0.987, RMSEA =.053, SRMR =.040, ECVI = 0.155. Website attitude: R2 =.573; Recall of information: R2 =.274. Estimates presented are standardized path estimates. Including the background variables as control (i.e., age, gender, education, cancer experience, Internet experience) in the model did not change the significance levels of the estimated paths.
We first hypothesized that mode tailoring would contribute to greater perceived active control, which in turn would enhance (a) website attitudes and (b) information recall. Compared to the standardized website, the mode-tailored website significantly increased participants’ perceived active control (β = .11, p = .034), which in turn led to a more favorable website attitudes (β = .44, p = .001). Perceived active control did not directly associate with information recall (β = .08, p = .170). Thus, only hypothesis 1a was confirmed.
Furthermore, we hypothesized that greater perceived active control – as afforded by mode tailoring – would increase perceived relevance (H2) and website engagement (H3), and reduce cognitive load (H4), ultimately enhancing (a) website attitudes and (b) information recall. The results showed that perceived active control heightened perceived relevance (β = .61, p < .001), increased website engagement (β = .22, p < .001), and reduced cognitive load (β = .51, p < .001). Serial indirect effects of mode tailoring on website attitude (β = .08, 95% CI [0.01, 0.15], p = .033) and information recall (β = .03, 95% CI [0.01, 07], p = .026) were both significant. However, only perceived relevance influenced website attitude (β = .38, p < .001), confirming hypothesis 2a. Furthermore, only website engagement (β = .38, p = .001) and cognitive load (β = −.26, p < .001) predicted information recall, confirming hypothesis 3b and 4b.
Discussion
Tailoring scholars continuously explore novel ways to design more effective health information. This study investigated what mechanisms explain the effects of user-initiated mode tailoring on a health website – i.e., enabling users to adjust the mode of information presentation via textual, visual and/or audiovisual information – on attitudinal and cognitive outcomes in a representative sample of Internet users (25–86 years). The results from a structural equation model (SEM) show that specific theory-based mechanisms explain the effects of mode tailoring on website attitude and information recall, but they do so via distinct pathways. While all indirect effects were facilitated by higher perceived active control by the mode-tailored website, perceived relevance explained effects on website attitudes, while website engagement and cognitive load explained effects on information recall. We discuss the implications of our results for theory and effective design of online health information below.
Theoretical Implications
Overall, our study contributes to tailoring research by exploring a different approach to tailoring. Traditional tailoring research has mainly focused on content, and has thus attempted to find explanations for the effectiveness of this tailoring strategy. In doing so, Lustria et al.’s (Lustria et al., Citation2016) model of tailoring effects focused on explaining content tailoring effects from a system-initiated approach. In our user-initiated mode-tailoring model, we confirmed the importance of several mediators proposed by Lustria et al.’s (Lustria et al., Citation2016) model of tailoring effects, such as perceived relevance and website engagement. We also extend this model by specifying mechanisms relevant for user-initiated mode tailoring, such as perceived active control and cognitive load. Moreover, by testing these mechanisms in a single SEM, we find that these mechanisms explain significant variance in the effects of mode tailoring on website attitude and information recall.
Our results demonstrate that perceived active control serves as a key driver in explaining the effects of mode tailoring. While the relationships between tailoring, perceived active control and outcomes have been widely assumed in the customization literature (see also Kalyanaraman & Sundar, Citation2006; Marathe & Sundar, Citation2011), this study is novel in that it considers the role of cognitive processing load in this context, and that it tests this set of mechanisms in a single model. Our finding corroborates with one of the key assumptions in self-determination theory that everyone has a basic need for autonomy, driving people to seek control over different situations one encounters in life (Ryan & Deci, Citation2000). In the context of health behaviors, Smit and Bol (Citation2019) recently found that individuals with high need for autonomy prefer to exert control over how to reach their health-related goals, suggesting they may benefit more from customizable health information. As such, it is likely that the perception of being in control over the presentation format fulfilled people’s need for autonomy, explaining the favorable effects of mode tailoring in this study. Furthermore, our study also confirms previous work focusing on the role of website interactivity in improving engagement with and processing and comprehension of health websites (e.g., Kim & Stout, 2010; Lustria, Citation2007; Oh & Sundar, Citation2015). The notion that perceived active control functions as a key driver of user-initiated mode tailoring, facilitating other message processing mechanisms, is a fruitful area for future health communication and tailoring research, and a valuable insight for eHealth intervention designers.
Interestingly, the results specified mechanisms (i.e., perceived relevance) responsible for enhancing website attitudes and other mechanisms (i.e., website engagement and cognitive load) that explained improved recall of information. These different pathways substantiate current theoretical and empirical research by providing a better understanding of why mode tailoring is effective (i.e., mechanisms of motivation vs. ability) and for which outcomes mode tailoring is valuable (i.e., attitudinal vs. cognitive). Altogether, our findings support arguments from educational science that providing users with control over the information structure can increase the motivation (i.e., through perceived relevance and website engagement) and ability (i.e., by freeing up cognitive resources) to process information, consequently enhancing attitudinal and cognitive learning outcomes (Dillon & Jobst, Citation2005; Eveland & Dunwoody, Citation2001). Researchers and professionals can use these insights as practical guidelines to design effective health messages.
Practical Implications
Overall, developing system-driven tailored communication interventions is a costly process, especially as tailoring of intervention materials become more sophisticated (Lairson et al., Citation2008). Typically, content tailoring requires a lot more development work that involves the development of content, creation of a message library, and formulation of tailoring criteria and algorithms. One argument in favor of a user-initiated approach, such as the way mode tailoring was operationalized in this study, is that it can offset some of the development costs by allowing users to tailor the information themselves. Given that no complex algorithms are needed, mode tailoring can be considered a relatively simple and cost-friendly tool to enhance users’ engagement with online information. One issue is that mode tailoring (be it system-or user-initiated) requires all materials to be covered in textual, visual, and audiovisual formats. This involves different areas of expertise (e.g., researchers, graphic designers, clinicians) and potentially a financial investment to develop these materials if they are not readily available. Designers of online health information should consider this trade-off.
Study Limitations and Future Research Directions
It is worth noting that the effect of mode tailoring on perceived active control, as well as indirect effects on outcomes, were relatively small. A possible explanation is that requiring the user to tailor information might demand more cognitive effort for some (or because it was a novel task), thus attenuating perceptions of perceived active control and cognitive load levels at the point of measurement in our study – which was after a one-time exposure. The benefits of control over the information may be more likely to become prominent after repeated exposure, when people become more familiar with the digital interface (Ariely Citation2000). Follow-up studies should explore whether repeated use of mode-tailored websites will further heighten perceived active control and reduce cognitive load. Moreover, as mode tailoring alone only slightly increased perceptions of active control, health websites might aim to include other interactive features such as customization options that allow for control over the content, sequence and amount of information (Kim & Stout, 2010). Besides customization options, clear navigational tools such as hyperlinks and search functions can also facilitate perceptions of active control (Lustria, 2007; Voorveld et al., Citation2011), and could be meaningful in improving other information processing mechanisms, as well as website attitudes and information recall.
It is important to discuss the extent to which our findings are generalizable to clinical populations. First, because our sample was recruited from an online research panel, participants might have had more experience with using the Internet than the average person or patient. However, our stratification procedure ensured that the sample composition reflected those of the Dutch population as accurately as possible, and thus our sample included participants with varying Internet experiences. Second, the current study applied a scenario-based study procedure. Participants could have imagined themselves in this scenario in different ways, possibly influencing their use, processing and evaluation of the information. However, the randomization procedure in this study likely reduced the potential confounding role of such difference. Moreover, scenario-based studies are common in experimental research to mimic responses from clinical patients, and have deemed valid for various outcomes important for health communication (Van Vliet et al., Citation2012). This is further supported by a recent study that showed that web-based mode tailoring can benefit cancer patients in clinical settings (Nguyen et al., Citation2019), which suggests that the findings from the current study can be extended to clinical populations.
This study examined the underlying mechanisms of mode tailoring in explaining improvements in website attitudes and information recall. Such information processing outcomes are important prerequisites for health outcomes overall. For instance, greater knowledge or information recall is an important precondition for effective disease-management (Linn, van Dijk, Smit, Jansen, & van Weert, Citation2013), informed decision-making (Fagerlin et al., Citation2006), cancer screening (Shim, Kelly, & Hornik, Citation2006), and health behavior change (De Melo Ghisi, Abdallah, Grace, Thomas, & Oh, Citation2014). While recent work has shown that mode-tailored health information can benefit patients’ website evaluations and reduce their anxiety (Nguyen et al., Citation2019), future research is warranted to see if other health outcomes can be improved by tailoring the presentation mode of online health information.
Future studies could examine additional mediators relevant within the context of tailored digital information. As the effect of user-initiated mode tailoring on perceived active control in our study was only small, it could be that other relevant mechanisms are at play (e.g., perceived autonomy support; Smit & Bol, Citation2019; Sundar, Bellur, & Jia, Citation2012). Including additional measures of attention and elaboration besides website engagement (here operationalized by time spent on the website) might also be valuable. Eye-tracking research, for example, could give a more objective measure of which content and information modes people attend to, while self-report measures of attention, elaboration, and engagement can give us insight into how recipients process the information (e.g., Craig Lefebvre, Tada, Hilfiker, & Baur, Citation2010). Considering that attention and elaboration are proposed as key mechanisms that explain effects of tailored communications (Lustria et al., Citation2016), future research should explore these message processing variables more comprehensively.
Overall, to gain a richer and more comprehensive understanding of effective tailoring, we highly encourage future research to disentangle mechanisms and effects of both mode tailoring and content tailoring, and system-initiated and user-initiated tailoring. Studies that compare the relative effectiveness of content and mode tailoring, or examine possible synergy effects of combining different tailoring strategies, are also worthwhile. Typical tailoring strategies usually employ a more involved message design process (using different tailoring tactics like behavioral construct tailoring) – this takes more time and may be costlier (Lairson et al., Citation2008). If comparative studies can prove that user-initiated approaches, like mode tailoring, are just as or more effective than traditional tailoring strategies, then it may be a more cost-effective approach. Further research on different dimensions of tailoring web-based information, as well as replication studies in other samples and contexts, may also provide insight into when and for whom which different tailoring approaches are effective.
Conclusions
The central question tailoring scholars often examine is: How do we develop effective messages, that will be perceived as personally relevant, can engage recipients, and can be adequately processed? Various studies have shown that message tailoring – often employing a system-initiated approach based on complex algorithms – increases perceived relevance which then enhances attention, elaboration, and behavioral outcomes (Jensen et al., Citation2012; Lustria et al., Citation2016). Our study sought to answer the question: Can user-initiated tailoring strategies such as mode tailoring evoke the same tailored experience that is considered important for message processing, elaboration and behavioral outcomes? The current study suggests that this is the case. Our results show that increasing active control on a health website – by enabling users to tailor the mode of information presentation – facilitates information processing by heightening the perceived relevance, enhancing engagement, and reducing cognitive load, which consequently benefits website attitude and information recall. This suggests that mode tailoring is a promising strategy to maximize the effectiveness of tailored health communications. Overall, this study provides a first insight into the specific mechanisms that explain mode tailoring effects on attitudinal and cognitive outcomes, confirms existing theoretical models of tailoring effects, and proposes a novel approach to, and extension of, traditional tailoring research in today’s digital environment. Future research will have to examine this further and guide us to a deeper and comprehensive understanding of various tailoring strategies, mechanisms, and effects.
Acknowledgments
We wish to thank Prof dr. Julia C. M. van Weert for the critical feedback on earlier versions of this manuscript, and dr. Rachid Azrout for assisting with data analysis. This study was conducted when Minh Hao Nguyen and Nadine Bol were working at the Amsterdam School of Communication Research/ASCoR, University of Amsterdam. This study was funded by the Dutch Cancer Society (KWF), grant numbers UvA 2014-6700 and UvA 2014-7288. KWF was not involved in the study design, data collection, data analysis and report writing.
Additional information
Funding
Notes
1 Log-transforming our data and/or excluding outliers yielded the similar results, demonstrating the robustness of our model. However, preference was given to removing outliers from the sample for model testing (N = 363) to ensure multivariate normality, because model fit indices, parameter estimates, and significance tests are then considered more reliable (Lei & Lomax, Citation2005).
2 We also estimated a saturated SEM with all possible paths between variables, in which insignificant paths were removed from the model one by one (i.e., constrained to zero). This resulted in a similar final model.
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. doi:10.1016/0749-5978(91)90020-T
- Ariely, D. (2000). Controlling the information flow: Effects on consumers’ decision making and preferences. Journal of Consumer Research, 27(2), 233–248. doi:10.1086/314322
- Bakker, A. B. (1999). Persuasive communication about AIDS prevention: Need for cognition determines the impact of message format. AIDS Education and Prevention, 11, 150.
- Bol, N., Linn, A. J., Smets, E. M., Verdam, M. G., & Van Weert, J. C. (2020). Tailored communication for older patients with cancer: Using cluster analysis to identify patient profiles based on information needs. Journal of Geriatric Oncology. Ahead of print. doi: 10.1016/j.jgo.2020.01.004.
- Bol, N., Smets, E., Eddes, E., de Haes, J., Loos, E., & Van Weert, J. (2015). Illustrations enhance older colorectal cancer patients’ website satisfaction and recall of online cancer information. European Journal of Cancer Care, 24(2), 213–223. doi:10.1111/ecc.12283
- Bol, N., Van Weert, J., Loos, E., Romano Bergstrom, J., Bolle, S., & Smets, E. (2016). How are online health messages processed? using eye tracking to predict recall of information in younger and older adults. Journal of Health Communication, 21(4), 387–396. doi:10.1080/10810730.2015.1080327
- Bollen, K. A., & Stine, R. A. (1992). Bootstrapping goodness-of-fit measures in structural equation models. Sociological Methods & Research, 21(2), 205–229. doi:10.1177/0049124192021002004
- Chung, D. S., & Nah, S. (2009). The effects of interactive news presentation on perceived user satisfaction of online community newspapers. Journal of Computer-Mediated Communication, 14(4), 855–874. doi:10.1111/j.1083-6101.2009.01473.x
- Craig Lefebvre, R., Tada, Y., Hilfiker, S. W., & Baur, C. (2010). The assessment of user engagement with eHealth content: The eHealth engagement scale. Journal of Computer-Mediated Communication, 15(4), 666–681. doi:10.1111/j.1083-6101.2009.01514.x
- Crutzen, R., de Nooijer, J., Brouwer, W., Oenema, A., Brug, J., & de Vries, N. K. (2011). Strategies to facilitate exposure to internet-delivered health behavior change interventions aimed at adolescents or young adults: A systematic review. Health Education & Behavior, 38(1), 49–62. doi:10.1177/1090198110372878
- Danaher, B. G., Boles, S. M., Akers, L., Gordon, J. S., & Severson, H. H. (2006). Defining participant exposure measures in web-based health behavior change programs. Journal of Medical Internet Research, 8(3), e15. doi:10.2196/jmir.8.3.e15
- De Melo Ghisi, G. L., Abdallah, F., Grace, S. L., Thomas, S., & Oh, P. (2014). A systematic review of patient education in cardiac patients: Do they increase knowledge and promote health behavior change? Patient Education and Counseling, 95(2), 160–174. doi:10.1016/j.pec.2014.01.012
- Dillon, A., & Jobst, J. (2005). Multimedia learning with hypermedia. In R. Mayer (Ed.), The Cambridge handbook of multimedia learning (pp. 569–588). New York, USA: Cambridge University Press.
- Dutch Comprehensive Cancer Organisation. (2017, September 2). Cijfers over kanker. Updated. Retrieved from http://www.cijfersoverkanker.nl/selecties/dataset_2/img5a268d84bf985
- Eveland, W., & Dunwoody, S. (2001). User control and structural isomorphism or disorientation and cognitive load? learning from the web versus print. Communication Research, 28(1), 48–78. doi:10.1177/009365001028001002
- Fagerlin, A., Lakhani, I., Lantz, P. M., Janz, N. K., Morrow, M., Schwartz, K., … Katz, S. J. (2006). An informed decision? Breast cancer patients and their knowledge about treatment. Patient Education and Counseling, 64(1–3), 303–312. doi:10.1016/j.pec.2006.03.010
- Heo, J., & Cho, C. (2009). A new approach to target segmentation: Media-usage segmentation in the multi-media environment. Journal of Targeting, Measurement and Analysis for Marketing, 17(3), 145–155. doi:10.1057/jt.2009.12
- Hooper, D., Coughlan, J., & Mullen, M. (2008). Structural equation modelling: Guidelines for determining model fit. Electronic Journal of Business Research Methods, 6, 53–60.
- Jansen, J., Van Weert, J., Van der Meulen, N., Van Dulmen, S., Heeren, T., & Bensing, J. (2008). Recall in older cancer patients: Measuring memory for medical information. The Gerontologist, 48(2), 149–157. doi:10.1093/geront/48.2.149
- Jensen, J. D., King, A. J., Carcioppolo, N., & Davis, L. (2012). Why are tailored messages more effective? A multiple mediation analysis of a breast cancer screening intervention. Journal of Communication, 62(5), 851–868. doi:10.1111/j.1460-2466.2012.01668.x
- Kalyanaraman, S., & Sundar, S. (2006). The psychological appeal of personalized content in web portals: Does customization affect attitudes and behavior? Journal of Communication, 56(1), 110–132. doi:10.1111/j.1460-2466.2006.00006.x
- Kim, H., & Stout, P. A. (2010). The effects of interactivity on information processing and attitude change: Implications for mental health stigma. Health Communication, 25(2), 142–154. doi: 10.1080/10410230903544936
- Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York: The Guilford Press.
- Kreuter, M. W. (2000). Are tailored health education materials always more effective than non-tailored materials? Health Education Research, 15(3), 305–315. doi:10.1093/her/15.3.305
- Kreuter, M. W., & Wray, R. J. (2003). Tailored and targeted health communication: Strategies for enhancing information relevance. American Journal of Health Behavior, 27(1), 227–232. doi:10.5993/ajhb.27.1.s3.6
- Lairson, D. R., DiCarlo, M., Myers, R. E., Wolf, T., Cocroft, J., Sifri, R., … Wender, R. (2008). Cost‐effectiveness of targeted and tailored interventions on colorectal cancer screening use. Cancer, 112(4), 779–788. doi:10.1002/cncr.23232
- Lang, A. (2006). Using the limited capacity model of motivated mediated message processing to design effective cancer communication messages. Journal of Communication, 56(suppl_1), S57–S80. doi:10.1111/j.1460-2466.2006.00283.x
- Lei, M., & Lomax, R. G. (2005). The effect of varying degrees of nonnormality in structural equation modeling. Structural Equation Modeling: A Multidisciplinary Journal, 12(1), 1–27. doi:10.1207/s15328007sem1201_1
- Linn, A. J., Alblas, M., Van Weert, J. C. M., & Bol, N. (2015). Een kwestie van voorkeur? een experimentele studie naar het aanpassen van gezondheidsinstructies aan de voorkeur voor modaliteit van de ontvanger. Tijdschrift Voor Communicatiewetenschap, 43(4), 362–377. doi:10.5553/TCW/138469302015043004004
- Linn, A. J., Van Dijk, L., Smit, E. G., Jansen, J., & Van Weert, J. C. M. (2013). May you never forget what is worth remembering: The relation between recall of medical information and medication adherence in patients with inflammatory bowel disease. Journal of Crohn’s and Colitis, 7(11), e543–e550. doi:10.1016/j.crohns.2013.04.001
- Liu, Y. P., & Shrum, L. J. (2002). What is interactivity and is it always such a good thing? Implications of definition, person, and situation for the influence of interactivity on advertising effectiveness. Journal of Advertising, 31(4), 53–64. doi:10.1080/00913367.2002.10673685
- Lustria, M. L. A. (2007). Can interactivity make a difference? Effects of interactivity on the comprehension of and attitudes toward online health content. Journal of the American Society for Information Science and Technology, 58(6), 766–776. doi: 10.1002/(ISSN)1532-2890
- Lustria, M. L. A., Cortese, J., Gerend, M. A., Schmitt, K., Kung, Y. M., & McLaughlin, C. (2016). A model of tailoring effects: A randomized controlled trial examining the mechanisms of tailoring in a web-based STD screening intervention. Health Psychology, 35(11), 1214–1224. doi:10.1037/hea0000399
- Lustria, M. L. A., Noar, S. M., Cortese, J., Van Stee, S. K., Glueckauf, R. L., & Lee, J. (2013). A meta-analysis of web-delivered tailored health behavior change interventions. Journal of Health Communication, 18(9), 1039–1069. doi:10.1080/10810730.2013.768727
- Marathe, S., & Sundar, S. S. (2011). What drives customization? Control or identity? Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Vancouver, Canada, 781–790. doi:10.1145/1978942.1979056
- Mayer, R. E. (2002). Multimedia learning. Psychology of Learning and Motivation, 41, 85–139. doi:10.1016/S0079-7421(02)80005-6
- Mayer, R. E., & Massa, L. J. (2003). Three facets of visual and verbal learners: Cognitive ability, cognitive style, and learning preference. Journal of Educational Psychology, 95(4), 833–846. doi:10.1037/0022-0663.95.4.833
- McMillan, S. J., & Hwang, J.-S. (2002). Measures of perceived interactivity: An exploration of the role of direction of communication, user control, and time in shaping perceptions of interactivity. Journal of Advertising, 31(3), 29–42. doi:10.1080/00913367.2002.10673674
- Nguyen, M. H., Smets, E. M. A., Bol, N., Loos, E. F., Van Laarhoven, H. W. M., Geijsen, E. D., … Van Weert, J. C. M. (2019). Tailored Web-based information for younger and older patients with cancer: Randomized controlled trial of a preparatory educational intervention on patient outcomes. Journal of Medical Internet Research, 21(10), e14407. doi:10.2196/14407
- Nguyen, M. H., Smets, E. M. A., Bol, N., Loos, E. F., & Van Weert, J. C. M. (2018). How tailoring the mode of information presentation influences younger and older adults’ satisfaction with health websites. Journal of Health Communication, 23(2), 170–180. doi:10.1080/10810730.2017.1421729
- Nguyen, M. H., Van Weert, J. C. M., Bol, N., Loos, E. F., Tytgat, K. M. A. J., Van de Ven, A. W. H., & Smets, E. M. A. (2017). Tailoring the mode of information presentation: Effects on younger and older adults’ attention and recall of online information. Human Communication Research, 43(1), 102–126. doi:10.1111/hcre.12097
- Noar, S. M., Benac, C. N., & Harris, M. S. (2007). Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychological Bulletin, 133(4), 673–693. doi:10.1037/0033-2909.133.4.673
- Oh, J., & Sundar, S. S. (2015). How does interactivity persuade? An experimental test of interactivity on cognitive absorption, elaboration, and attitudes. Journal of Communication, 65(2), 213–236. doi: 10.1111/jcom.2015.65.issue-2
- Paas, F. (1992). Training strategies for attaining transfer of problem-solving skill in statistics: A cognitive-load approach. Journal of Educational Psychology, 84(4), 429–434. doi:10.1037/0022-0663.84.4.429
- Petty, R., Barden, J., & Wheeler, S. (2002). The elaboration likelihood model of persuasion: Health promotions that yield sustained behavior change. In R. DiClemente, R. Crosby, & M. Kegler (Eds.), Emerging theories in health promotion practice and research (pp. 71–99). San Fransisco, CA: Jossey-Bass.
- Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1), 68–78. doi:10.1037/0003-066X.55.1.68
- Severson, H. H., Gordon, J. S., Danaher, B. G., & Akers, L. (2008). ChewFree.com: Evaluation of a web-based cessation program for smokeless tobacco users. Nicotine & Tobacco Research, 10(2), 381–391. doi:10.1080/14622200701824984
- Shim, M., Kelly, B., & Hornik, R. (2006). Cancer information scanning and seeking behavior is associated with knowledge, lifestyle choices, and screening. Journal of Health Communication, 11(sup001), 157–172. doi:10.1080/10810730600637475
- Smit, E., Linn, A., & Weert, J. (2015). Taking online computer-tailoring forward: The potential of tailoring the message frame and delivery mode of online health behaviour change interventions. The European Health Psychologist, 17, 25–31.
- Smit, E. S., & Bol, N. (2019). From self-reliers to expert-dependents: Identifying classes based on health-related need for autonomy and need for external control among mobile users. Media Psychology, 1–24. Advanced online publication, doi:10.1080/15213269.2019.1604235.
- Society, A. C. (2017). Colorectal cancer facts and figures 2017-2019. Atlanta, Georgia: American Cancer Society.
- Stanczyk, N. E., Crutzen, R., Bolman, C., Muris, J., & de Vries, H. (2013). Influence of delivery strategy on message-processing mechanisms and future adherence to a Dutch computer-tailored smoking cessation intervention. Journal of Medical Internet Research, 15(2), e28. doi:10.2196/jmir.2153
- Sundar, S., & Marathe, S. (2010). Personalization versus customization: The importance of agency, privacy, and power usage. Human Communication Research, 36(3), 298–322. doi:10.1111/j.1468-2958.2010.01377.x
- Sundar, S. S., Bellur, S., & Jia, H. (2012). Motivational technologies: A theoretical framework for designing preventive health applications. In M. Bang & E. L. Ragnemalm (Eds..), Persuasive technology. Design for health and safety (Persuasive 2012. Lecture Notes in Computer Science, Vol. 7284, pp. 112–122). Berlin, Heidelberg: Springer. doi:10.1007/978-3-642-31037-9_10.
- Van Vliet, L. M., Van der Wall, E., Albada, A., Spreeuwenberg, P. M., Verheul, W., & Bensing, J. M. (2012). The validity of using analogue patients in practitioner–patient communication research: Systematic review and meta-analysis. Journal of General Internal Medicine, 27(11), 1528–1543. doi:10.1007/s11606-012-2111-8
- Van Weert, J., Van Noort, G., Bol, N., Van Dijk, L., Tates, K., & Jansen, J. (2011). Tailored information for cancer patients on the internet: Effects of visual cues and language complexity on information recall and satisfaction. Patient Education and Counseling, 84(3), 368–378. doi:10.1016/j.pec.2011.04.006
- Voorveld, H., Neijens, P., & Smit, E. (2011). The relation between actual and perceived interactivity. Journal of Advertising, 40(2), 77–92. doi:10.2753/JOA0091-3367400206