
Abstract
Objectives: Everyday technologies (ETs) can be challenging to use, particularly for older adults with cognitive impairments. This study evaluated the relationship between the self-perceived ability to use ET and observable performance of self-chosen and familiar, but challenging ETs in people with mild cognitive impairment (MCI) or dementia.
Method: A self-perceived report, the Everyday Technology Use Questionnaire (S-ETUQ), and a structured observational tool, the Management of Everyday Technology Assessment (META), assessing the perceived and observed ability to use ET, were used in 41 people with MCI and 38 people with dementia. Correlations were investigated with non-parametric statistical tests.
Results: In the dementia group, self-perceived report and observational scores correlated on a significant medium level (Rs=0.44, p = 0.006). In the MCI group, no significant correlation was found.
Conclusion: The findings of this study suggest the ability of older adults with cognitive impairments to use ETs can be depicted with self-perceived reports as well as with observations. However, the combination of both approaches is recommended to get a comprehensive picture. While the S-ETUQ provides a broad picture of the use, presence and relevance of technologies in an individual’s life, the META describes a specific human-technology interaction in detail. Furthermore, the results suggest people with early dementia retain the ability and insight to accurately reflect on their own ability to use ET, emphasizing the need to include their experiences in research and clinical work.
Introduction
As technological development continues to further influence everyday life (Bates & Bitton, Citation2010; Coughlin, Pope, & Leedle, Citation2006; Hedman, Lindqvist, & Nygård, Citation2016), it is important to evaluate the ability to use technology and the effects this human-technology interaction can have on the elderly (Keningsberg et al., Citation2017). Technologies supporting older adults with and without disabilities have been reported to maintain or improve cognitive functioning, promote feelings of independence and safety, support social connectivity or increase well-being (Coorey, Neubeck, Mulley, & Redfern, Citation2018; Forsman et al., Citation2017; Khosravi, Rezvani, & Wiewiora, Citation2016; McDougall & House, Citation2012). In contrast, the involvement of technology in daily activities has been described as potentially demotivating or misleading in the elderly population (Kottorp et al., Citation2016; Schulz et al., Citation2015), pointing out that technology can also complicate everyday life. A meta-analysis showed that age is negatively related to perceived ease of technology use (Hauk, Hüffmeier, & Krumm, Citation2018) and technologies with greater complexity are more demanding for older compared to younger adults (Ziefle & Bay, Citation2005), which might indicate a greater challenge for elderly with cognitive impairments.
Structured self-reports are a common method to gain insight into individuals’ self-perceived abilities. Various tools have been developed specifically for older adults and assessed with proven psychometrics for example instrumental activities of daily living (Pfeffer, Kurosaki, Harrah, Chance, & Filos, Citation1982). The Everyday Technology Use Questionnaire (ETUQ) was developed to assess the ability of older adults to use everyday technology (ET). ET is here defined as all electronic, technological or mechanical equipment that exist in the everyday life of the individual, for example, smartphones, online banking, or remote controls (Nygård, Citation2008). ET thus describes a wide range of objects/services with a variety of complexity. The ETUQ structured interview evaluates the relevance of and perceived ability to use various technologies in an individuals’ everyday life. The tool has been repeatedly used in older adults with and without cognitive impairment (Fallahpour, Kottorp, Nygård, & Lund, Citation2014; Fallahpour, Kottorp, Nygård, & Lund, Citation2015; Hedman, Nygård, Malinowsky, Almkvist, & Kottorp, Citation2016; Ryd, Nygård, Malinowsky, Öhman, & Kottorp, Citation2017). Guided by the ETUQ, participants are asked to reflect upon their use of ETs from various areas of everyday life such as home maintenance (e.g. coffee machine) or purchasing (e.g. ATM).
The ETUQ has shown to have a person reliability of 0.81 suggesting a high replicability in the generated measures (Rosenberg, Nygård, & Kottorp, Citation2009). Furthermore, the ability to use ETs seems to highly correlate with activities of daily living (Ryd, Nygård, Malinowsky, Öhman, & Kottorp, Citation2015). This highlights the necessity to take the ability to use ET into account when focusing on participation in everyday life. In the worst case, the inability to manage ETs could result, for example, in problems paying for services (e.g. transport) and resources (e.g. food) that influence well-being and health. In 2011, a short version of this assessment tool, the S-ETUQ, was developed reducing the amount of items from 90+ to 33 to provide a more convenient, cost- and time-effective tool to investigate the ability to use ET in clinical practice with equally reliable person measures of perceived abilities (Kottorp & Nygård, Citation2011).
In addition to self-reports, observations can be performed to evaluate an individuals’ performance or ability. This might be particularly important when investigating people with MCI and dementia, as a lack of certain dimensions of insight has been described as increasing with disease severity (Mak, Chin, Ng, Yeo, & Hameed, Citation2015). The evaluation of own memory function and problems in activities of daily living seem particularly difficult for people with amnestic dysfunctions (Leicht, Berwig, & Gertz, Citation2010), which might affect the outcome of self-reports. However, to this point it is unclear how accurate the insight of people with MCI or dementia is when reflecting on their own ability to use ET, which can be investigated through comparing the self-report to an observation.
The management of everyday technology assessment (META) is a performance-based observational tool measuring an individual’s ability to use ET at home or in society (Malinowsky, Citation2011). The subjects’ management of self-chosen ETs that are perceived as relevant, well-known and to a certain degree challenging, is observed and rated by a health professional such as an occupational therapist or psychologist. The META has been used in elderly with and without cognitive impairment (Malinowsky, Almkvist, Kottorp, & Nygård, Citation2011; Malinowsky & Larsson-Lund, Citation2014) and it reports a person reliability of 0.74 (Malinowsky, Almkvist, Nygård, & Kottorp, Citation2011).
It is recommended to combine self-reports with observational assessments to get a comprehensive overview of a person’s abilities (Fearing, Law, & Clark, Citation1997; Fisher, Citation2009; Kielhofer, Citation2008; Nygård, Citation2006). This can be challenging in clinical settings due to organizational limitations or persons’ endurance. Therefore, it seems necessary to investigate the relation between information gathered with a self-perceived report and observation. This would allow for recommendations to researchers and clinicians on how to best gain knowledge of or support a person’s ability to use ET.
The present study aims to evaluate the relationship between (1) the self-perceived ability to use relevant ETs assessed by the S-ETUQ and (2) the observable performance of self-chosen and familiar, but challenging ETs evaluated by the META. To get insight into the distinctions and similarities of ET use in people with various stages of cognitive impairments, people with MCI and dementia were included. We hypothesize that the tools assessing perceived and observed abilities of ET use correlate and complement each other. Group differences between people with MCI and early dementia are expected. However, due to limited correlation studies between observations and self-perceived reports in these populations, concrete expectations cannot be formulated and this study represents an exploration in this topic. Finally, the relevance of technological items and level of challenge posed by the technologies within the self-perceived reports and observations will be described in detail. The focus of the descriptive analysis will lie on group trends to describe the composition and specific benefits of each instrument.
Methods
Study design and ethics
A cross-sectional, non-experimental design was used. The present study was approved by the Regional Ethical Committee (Registration Number 2013/5:1). Potential participants were provided with oral and written information about the study. Written informed consent was obtained from all subjects and subjects had the right to withdraw from participation at any point without giving reasons.
Participants
Participants were recruited in Sweden through memory investigation clinics, a Traffic Medicine Center and activity groups offered by municipalities within the Stockholm area. The inclusion criteria for all participants were: (1) age >55, (2) active users of ET, (3) compensation for visual and hearing difficulties (if applicable; e.g. glasses/hearing aids), (4) ability to conduct the interview in Swedish or English and (5) being diagnosed with mild-stage dementia or MCI. The age restriction was chosen to focus on an aging population, but also to involve individuals with early cognitive decline. The diagnosis of mild stage dementia was given by a physician according to the standardized DSM-IV criteria (American Psychiatric Association, Citation2000) or as major neurocognitive disorder in the mild stage according to the DSM-5 (American Psychiatric Association, Citation2013). MCI was defined as (i) neither cognitively normal nor fulfilling the criteria of dementia, (ii) evidence of cognitive deterioration shown by either objectively measured decline over time and/or subjective report of decline via self-report and/or informant in conjunction with objective cognitive deficits, and (iii) preserved activities of daily living and complex instrumental functions (Winblad et al., Citation2004). Therefore, participants of the MCI group were included if they did not have a dementia diagnosis and fell into one of the following categories: (1) a clinical diagnose of Mild Cognitive Impairment, (2) subjective memory impairment of memory dysfunction verified by clinical tests, (3) mild cognitive dysfunction due to other diagnoses, for example Parkinson’s disease, Multiple Sclerosis or stroke, and (4) cognitive impairments with a (consequential) depression as long as the depression was medically treated. Participants were excluded if they experienced temporary confusion or episodes of a (major) depression resulting in cognitive impairments. The sample size was orientated on the principles of Walter, Eliasziw, and Donner (Citation1998) in combination with a power analysis with a power of 0.8 and p < 0.05. This resulted in the aim to include at least 33 participants in each group.
Instruments
Socio-demographics and descriptive instruments
Information about the participants’ gender, age, living situation, years of education and level of participating in activities (Frenchay activity index (FAI) (Holbrook & Skilbeck, Citation1983) were gathered in an interview. The FAI captures the level of perceived activity involvement and reflects on the frequency of performing everyday activities during the past three or six months. Furthermore, cognitive abilities were measured with the Mini Mental State Examination (MMSE) (Folstein, Folstein, & McHugh, Citation1975). Using clinical judgement and based on all available information collected in contact with the client, including the META observations and the S-ETUQ interview, the final non-standard assessment related to overall functional level and the need for assistance to live in the community was performed. This was done by the interviewer against a set of given criteria for overall functional level and independence related to the participant’s requirements for living in the community using a four-graded scale; 1) independent, 2) minimal assistance or supervision, 3) moderate assistance, 4) maximum assistance. All above mentioned information were used to describe the sample.
The everyday technology use questionnaire: the self-perceived report
The short-form version of the Everyday Technology Use Questionnaire, S-ETUQ, was used in this study. The aim of the questionnaire is to identify relevance of different ETs as well as perceptions of ability to use ET. The S-ETUQ contains 33 items representing a variety of ETs and derived via item reduction guided by assertions of a Rasch model (Bond & Fox, Citation2007). Relevance of ET is defined in the user manual as ‘technology that is available to the person, has earlier been used, is currently used or intended to be used by the person’ (p.13) (Nygård, Rosenberg, & Kottorp, Citation2015) and only ETs relevant to the individual are included in the scoring. illustrates the scale. The S-ETUQ requires 15-20 minutes and has been used in various populations of older adults with and without cognitive impairments, demonstrating high levels of internal scale validity, uni-dimensionality, acceptable precision in the generated measures, and evidence of validity in relation to external variables (Kottorp & Nygård, Citation2011).
Table 4. S-ETUQ descriptive data.
Management of everyday technology assessment: the observational tool
The Management of Everyday Technology Assessment (META) is an observation-based assessment of the ability to manage ET (Malinowsky, Citation2011). The tool was developed to evaluate the ability to manage ET for older adults via a proxy rating in order to facilitate provision of individual support in ET management and to gain information useful for design and adaption of ETs. In total, the META consist of 17 items. In the present study, only the n = 11 ‘Observed Performance Skills’ were used (see ). During the assessment, the individual is observed using ETs of their own possession and choice that are relevant, currently in use and somewhat challenging for that person. To learn and practice the scoring, the observer/rater receive training (see “Data collection process” Section). Previous META studies proved acceptable person response validity and technology goodness-of-fit (Kassberg, Malinowsky, Jacobsson, & Lund, Citation2013; Malinowsky, Almkvist, Kottorp, et al., Citation2011). Furthermore, the tool is sensitive to group differences between elderly without known cognitive impairment, MCI and Alzheimer’s disease, and those with different severities of acquired brain injury (Malinowsky, Almkvist, Kottorp, et al., Citation2011).
Table 1. META observable performance skills.
Table 2. Sociodemographic characteristics, MMSE scoring, general ability measure and FAI.
Data collection process
Data was collected between 2014 and 2016 by four experienced occupational therapists (OTs). All OTs completed a one-day ETUQ and a two-day META training course which included assessment of live- or video-taped cases prior to data collection. The training consisted of studying the manual, instructions for administration, definitions of the items and the scoring criteria. Participants’ appointments were scheduled in their own home at a mutually convenient time. The OTs collected the socio-demographic information and conducted the META and S-ETUQ on the same occasion. As the order of the tools was not expected to influence the outcome, this was not further specified. A minimum of two technological artefacts or services were assessed with the META for each participant. Additionally, the MMSE evaluations were undertaken either during the assessment occasion or the score was collected from the medical records of the participant if documented within six months.
Data preparation analysis
First, the ordinal raw score data from the assessments with the S-ETUQ and the 11 performance skill items of the META were separately transformed into abstract interval-like measures, i.e. person ability measures expressed in log-odd probability units (logits) using computer software applications of a Rasch rating scale model (Bond & Fox, Citation2007). These analyses are able to take the different facets into account, e.g. variations in level of challenge in the items and the ETs chosen, adjusting the final personal ability measure to these facets. The S-ETUQ assesses two facets (person and ET) and thus, the software WINSTEPS (Linacre, Citation2017b) was applied. The META includes four different facets (person, rater, item and ET) and thus a many-faceted analysis was required and the software program FACETS was used (Linacre, Citation2017a). The analyses resulted in estimated measures of each person’s observed (META) and perceived ability (S-ETUQ) to use ET. The use of Rasch models to develop valid and reliable measures from the META and S-ETUQ are described in detail elsewhere (Kottorp & Nygård, Citation2011; Malinowsky, Citation2011). Since the raters were not linked by assessing the same participants, they were assumed as equally severe and rater leniency was anchored at the same severity in the analysis. Raters’ acceptable goodness-of-fit was set as outfit MnSq > 0.6 and ˂1.5 (Engelhard, Citation1994). It is commonly accepted that 5% of the responses (i.e., person, technology, performance skill item and rater) are expected to be misfits by chance with z-values less than 2. In the present study, therefore, 95% of the responses were supposed to demonstrate acceptable goodness-of-fit to the Rasch measurement model and not to be a threat to validity (Bond & Fox, Citation2007).
Statistical main analysis
For the main analysis, the Statistical Package for Social Science (SPSS) was used (IBM Corp. Released 2016. IBM SPSS Statistics for Macintosh, Version 24.0. Armonk, NY: IBM Corp.). Demographic group differences were calculated with t-tests or Chi-square test. Since the S-ETUQ and META data showed non-normal distribution, the relationship between the personal ability measures of the S-ETUQ and META were explored with Spearman’s rho coefficient (Rs) for the whole group as well as for the MCI group and dementia group. To control for significant group differences in sociodemographic information (years of education), and age as it might influence the ability to use ET, Spearman’s partial correlation was additionally conducted by computing the specific syntax in SPSS. The strength of the association was determined through Cohen’s guidelines for social sciences: 0.1–0.3 = small, 0.3–0.5 medium, and 0.5–1.0 = large effect (Cohen, Citation1988). To analyse the group differences regarding the S-ETUQ and META person ability measures, the Mann-Whitney test was used. Furthermore, the data was tested for outliers with the outlier labelling rule and a factor of 2.2 (Hoaglin, Iglewicz, & Tukey, Citation1986) and the Grubbs outlier test (Grubbs & Beck, Citation1972). Descriptive statistics were used to give further insight into the different ETs used and performance skills reported by the S-ETUQ and META. The alpha level was set to 0.05 throughout all analysis.
Results
Participants
N = 38 people with dementia and n = 41 people with MCI participated in the study (total sample n = 79). There were no significant differences in the socio-demographics (gender, living condition and age) between the groups. The MCI group had significantly more years of education than the dementia group (p < 0.05). The MMSE (p < 0.01) and FAI (p < 0.01) scores of the MCI group were significantly higher compared to the dementia group. For details see .
Group differences and correlations between S-ETUQ and META
Across the total sample, a small significant correlation (Rs=0.25, p = 0.024) was found between META and S-ETUQ. When controlling for years of education, the correlation stayed stable (Rs=0.27, p = 0.017). The correlation was non-significant when controlling for age in the total sample (Rs=.21, p=.06). The correlation between the S-ETUQ and META in the dementia group was of significant medium size (Rs=0.44, p = 0.006; controlled for years of education: Rs=.42, p=.009; controlled for age: Rs=.50, p=.002), while no significant correlation was found in the MCI group (Rs=.06, p=.71; controlled for years of education: Rs=.03, p=.85; controlled for age: Rs= −.09, p=.57).
The data was examined visually and statistically tested for outliers. Two outliers were identified (see ), hence, the correlation analysis was repeated without the outliers. The result showed small variations compared to the first correlation test () in each groups. In the total sample, the correlation was non-significant (Rs=.22, p=.052) without the outliers, however, significant when controlling for years of education (Rs=.24, p=.04).
Figure 1. Scatter-Plot visualizing the relationship between measures of perceived and observed ability to use ET over the whole group, the MCI group and the dementia group. Note: higher scores indicate greater ability. Individual A: observed ability (META)=4.26 logits, perceived ability (S-ETUQ)=63.36 logits. Individual B: observed ability (META)=1.61 logits, perceived ability (S-ETUQ)=70.89 logits.
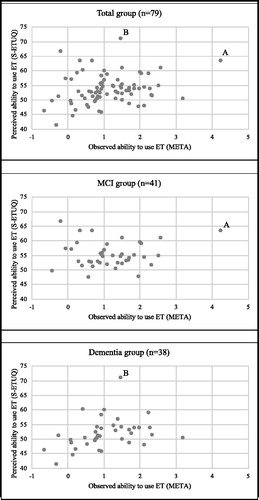
Table 3. Means of S-ETUQ and META, correlations.
When comparing the S-ETUQ and META scores between the groups, a significant group difference was found for the S-ETUQ scores (p < 0.001), while no significant differences could be reported between groups for the META scores (p=.54).
Descriptive results of the S-ETUQ and META
The descriptive analysis of the S-ETUQ showed the relevance and self-perceived level of ability to use various technological items ().
A couple of technologies are highlighted to demonstrate the insight gained from descriptive S-ETUQ results: the TV with remote control is relevant for 100% of the people in both groups, however, one person with dementia reports not being able to use it anymore. In the MCI group, the debit card was reported as relevant by 95.1% of the group, but caused minor problems in usage for 35.9%. In the dementia group, 10.7% were not able to use the debit card anymore. 16.1% stopped using the ATM even though both technologies were perceived as relevant. Within highly relevant technologies, the individuals in the dementia group showed a tendency to need more assistance to use the ETs or stopped using them even though they were relevant. The biggest difference in relevance between the groups was described for ‘cell phone, text’, where 75.6% of people with MCI and only 21.1% of people with dementia named this technology as important. The video player, even if available and perceived as relevant, was not used anymore by 61.9% of individuals in the MCI and 83.3% in the dementia group.
With the META, n = 237 performances were observed (MCI: n = 121; Dementia: n = 116). In the MCI group, the computer (n = 29), the TV (n = 25), smartphone (n = 19) and mobile phone (n = 17) were chosen most. In the dementia group, the most common choices were the TV (n = 33), mobile phone (n = 17), computer (n = 9), and music player (n = 9). While people with MCI had a tendency to choose information and communication technologies such as the smartphone, computer and digital camera, people with dementia chose more often household technologies like the washing machine, power tools or coffee machine when asked to perform a challenging ET ().
Table 5. Descriptive results META observations.
Intra-rater reliability of the META
Raters’ demonstrated a goodness-of-fit with outfit MnSq between 0.97 and 1.34, which indicates an acceptable consistency (intra-rater reliability).
Discussion
This study evaluated the relationship between the self-perceived ability to use ET and the observable performance of self-chosen and familiar, but challenging ETs in people with MCI or dementia. In the total sample, a small significant correlation was found between the self-reported perceived abilities and observed performance skills (Rs=0.25, p = 0.024). When excluding two outliers, the correlation became non-significant (p = 0.052). In the dementia group only, the correlation between the S-ETUQ and META showed a significant medium size (with and without outliers, and when controlling for years of education and age) suggesting a connection between information gathered with both tools. This finding might further indicate that people with mild dementia retain the ability to accurately describe their ability to use ETs and therefore, attention needs to be paid to their self-perceptions regarding technology relevance and use (see “Disadvantages and advantages of self-perceived reports to evaluate ET use”section). This personal insight can inform researchers, clinicians and relatives about problems in everyday life and potential need for support in human-technology interactions.
In the MCI group, no significant correlation was found neither with nor without the outlier, which was unexpected. Generally, the tendency of a stronger association between perceived and observed abilities to use ET in people with greater cognitive impairments was in line with previous research. In a study of people with acquired brain injury, the subsample with severe disabilities had a strong significant correlation between perceived and observed abilities to use ET, while no significant correlation could be reported in the recovery group (Malinowsky & Larsson-Lund, Citation2014). A number of studies in aging research compared self-perceptions and other methods and found non-significant correlations (Magaziner, Zimmerman, Gruber-Baldini, Hebel, & Fox, Citation1997; Ready, Ott, & Grace, Citation2004; Schmitter-Edgecombe, Parsey, & Cook, Citation2011; Schmitter-Edgecombe & Parsey, Citation2014). Ready et al. (Citation2004) pointed out that neither of these sources have been established to be superior and Schmitter-Edgecombe et al. (Citation2011) concluded that tests need to be cautious in predicting functions as they might be tapping into different aspects of the same construct. However, these studies did not focus on technology use and this difference needs to be kept in mind.
In the present study, the non-significant correlation in the MCI group could be explained by the self-chosen ETs being too challenging during the observation. This could result in a lower META person ability measure, which then did not correlate with the S-ETUQ perceived ability measure. Furthermore, the mean ability measures for the META were quite similar in the MCI and dementia group. This differs from an earlier META study, where the means showed to be significantly different between these groups (Malinowsky, Almkvist, Kottorp, et al., Citation2011). The data collection of Malinowsky, Almkvist, Kottorp, et al. (Citation2011), however, took place about six years prior to the studied data set. Technology develops rapidly and seems to increase in complexity, which might be a possible explanation for this MCI sample to experience difficulties equal to those experienced by the dementia sample. There are many different types of technologies, various brands and technological items, and in this study each participant only performed about three self-chosen ETs. A previous study ranking the level of challenge of ETs (Malinowsky, Kottorp, Patomella, Rosenberg, & Nygård, Citation2015) identified, for example, the use of a microwave to be less complex than actions performed on a cell phone. In the present META assessment, people with dementia tended to manage less complex technologies (e.g. TV) during the observation while people with MCI managed more complex technologies (e.g. smartphone).
Therefore, the perceived ability to use ET does not always appear related to observed ability and vice versa, specifically for individuals with MCI. Perceived and observed ability should be described as two different but corresponding aspects of evaluations of ET use.
Furthermore, certain technologies seem to be slightly less relevant for people with dementia than for individuals with MCI, for example sending texts with a cell phone. When aiming to introduce new technological objects to the elderly, perceived relevance should be taken into account.
Combining the S-ETUQ and META
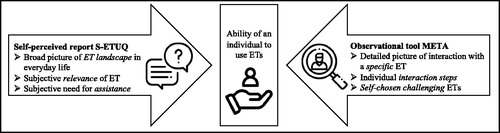
The S-ETUQ and META both describe the construct of technology use in older adults with cognitive impairments well. The information gathered by each instrument, however, is complementary (). While the S-ETUQ reports on a broader range of technologies, their relevance, needed assistance, and self-perceived ability to use them, the META reveals the level of complexity the individual associates with technological item. Additionally, the META can depict the detailed performance skills during the human-technology-interaction. Health professionals could choose one or the other to investigate a specific question. However, combined, the S-ETUQ and META provide a comprehensive view of the person’s ability to perform ET. This can be an advantage in the clinical setting, where the health professional might want to gain a broader understanding of the person’s situation regarding their ability to use ET.
Figure 2. Unique characteristics of the S-ETUQ and META.
Disadvantages and advantages of self-perceived reports to evaluate ET use
Generally, self-perceived reports capture the conscious perceptions of an individual’s perspective and require the control of higher mental processes (Hadjistavropoulos & Craig, Citation2002) such as memory recall. In healthy individuals, a summarized self-perceived report can be memory biased (Hassan, Citation2005) and furthermore describes a temporal picture of a perception with a limited amount of fluctuation. To get a more detailed picture, the experience sampling method (ESM) could be of help to describe abilities, activities and pattern in everyday life (Shiffman, Stone, & Hufford, Citation2008). The ESM is a data collection method where individuals repeatedly fill in short (digital) diaries reflecting on behaviour, emotion, and social context right in the moment (Csikszentmihalyi & Larson, Citation1987). The upcoming ‘Monitor-Mi’ study will evaluate the feasibility and validity of the ESM incorporated in a smartphone app in an MCI population. The ESM has not yet been used to focus on the ability to use ET. However, it might have the potential to provide a new perspective on ET use.
Additionally, even if remembered, admitting problems in everyday life after a diagnosis of cognitive impairments can be accompanied with a feeling of shame or discomfort (Garand, Lingler, Conner, & Dew, Citation2009) potentially leading to a downplay of difficulties. Problems with handling everyday information or activities might be seen as an obvious sign of cognitive decline. In the specific case of the technology use described in the present study, however, it might have been easier for the individuals to admit difficulties, for example getting frustrated with using smartphone apps/functions, as many technological devices and services are relatively new for older people. It might be seen as ‘normal’ to struggle with ET such as a smartphone – even for an older person without cognitive impairment. The complex technology can be made responsible for the inaccurate interaction rather than the person’s inability. It is not possible to differentiate this with the S-ETUQ as the self-perceived ability refers to the person-technology interaction. Generally, the S-ETUQ might describe an especially just picture of abilities in people with MCI and dementia and could help health professionals to get an idea of realistic problems in everyday life, as ET is intertwined in many daily activities (Nygård, Kottorp, & Rosenberg, Citation2015).
Disadvantages and advantages of observations to evaluate ET use
In some situations, when self-perceived reports cannot be obtained such as in people with severe dementia due to limited cognitive abilities to reflect or speak (Zwakhalen, Hamers, Abu-Saad, & Berger, Citation2006), observations might be the only way to assess a person’s functional ability. In the present study, the participants had mild dementia and were thus able to communicate experiences. Nevertheless, the META observation was of value as a human-technology interaction with a specific self-chosen ET could be described. The person with MCI or dementia choses at least three relevant but challenging ETs themselves, giving the individual high independence of choice. The choice can inform the researcher or clinicians about level of technological complexity the person wants to take on. As pointed out before, the participants with dementia in this study seem to have an ultimately conscious tendency for easier technologies (e.g. TV or microwave), while the participants with MCI tend to choose more complex technologies such as a computer or a smartphone. During observations, this particular complexity can be a challenge for the investigator when observing ET use, as many steps are performed to produce an action (e.g. turn buttons, use appropriate force, perform steps in a certain action). When used in its intended way, the META adds information about the performance that a self-perceived report cannot provide, hence, completes the view of a person’s ET use.
Limitations
The S-ETUQ and META represent two different data-collection modes, however, both tools focus on the same construct and therefore the results could be influenced by the amount of overlap between the tools rather than pure differences of abilities. Technology develops rapidly and despite the fact that the S-ETUQ includes a range of items/services from various domains and the participants chose currently-available ETs during the META observation, the latest innovations might not have been evaluated in this study. Tablets, for example, seem to be becoming more interesting for older adults (Fernández, Hernández, Gutiérrez, Escuela, & Fino, Citation2017). In the S-ETUQ and META, the participants could chose to include additional technologies perceived as relevant, but tablets were not named by this sample. Future research should pay special attention to include newly developed ETs when assessing technology use in people with MCI and dementia. The ETUQ gets regularly updated and will prospectively contribute to this question. Furthermore, during the observation, participants with dementia might have chosen technologies that were relatively easy to perform in order to not be confronted with their own impairments in that moment. It is possible that greater difficulties experienced in everyday life with ETs were not described in this study. Other limitations include the time-consuming S-ETUQ and META training, as well as the data processing procedure. This includes the Rasch analysis via additional software (WINSTEPS/FACETS), which makes the use of the instruments more complex. It is not uncommon, however, for extensive instruments to require training and supervision during examination as well as data processing. In the case of the S-ETUQ and META, online courses are currently in development, including support during the data processing. Finally, the MCI group had milder cognitive impairments and greater abilities to perform everyday activities than the dementia group. However, individuals with MCI from various origins were included and the abilities to perform complex activities in daily life may vary by MCI subtype (Bangen et al., Citation2010). Future studies might want take the different MCI aetiologies into account. However, in this study it was not possible due to the small sample size and the cross-sectional design. A longitudinal approach would be beneficial to get further insight, potentially also including a control group with no cognitive impairment. A control group could display the full range of abilities to perform ET in older adults with and without cognitive impairments.
Conclusions
It is important for clinicians to have valid assessment tools that can provide information on the difficulties people with cognitive impairments might have when using ET. This study emphasises the benefits of combining the S-ETUQ and META to gain knowledge about the individual’s situation. While the self-perceived report describes a broad picture of the technological landscape, including perceived relevance of technological items and the need for assistance to use them correctly, the observational tool illustrates the detailed steps of a specific human-technology interaction. The latter can be used to provide information on concrete technological features that might need adjustment to improve usability. The findings indicate that people with mild dementia have an accurate insight into their own abilities to use ETs, hence, emphasising the need for clinicians and researchers to pay attention to their expressed experiences.
Acknowledgement
First of all, the authors would like to thank the participants who generously shared their use of everyday technology for us. We also want to thank the professionals who helped us to recruit participants. Furthermore, thanks go to Cecilia Bråkenhielm, Monica Pantzar and Annika Persson Vasiliou for data collection and management. Finally, the authors wish to acknowledge the support from the Swedish Council for Health, Working Life and Welfare (FORTE) as the funder. The icons in are made by freepik from www.flaticon.com.
Disclosure statement
None of the authors have any disclosure of interest to report.
Additional information
Funding
Notes on contributors
S. L. Bartels
Sara L. Bartels was involved in the analysis, interpretation of the results and writing of the article.
S. Assander
Susanne Assander was involved in the preliminary analysis, interpretation and writing of the manuscript.
A.-H. Patomella
Ann-Helen Patomella assisted with the design and writing of the manuscript.
J. Jamnadas-Khoda
Jenny Jamnadas-Khoda was involved in the analysis and interpretation of the results, and drafting the manuscript.
C. Malinowsky
Camilla Malinowsky was involved in the design, analysis, interpretation and writing of the manuscript.
Related Research Data
References
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders. Washington, DC: American Psychiatric Association.
- American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.) Washington, DC: American Psychiatric Association.
- Bangen, K. J., Jak, A. J., Schiehser, D. M., Delano-Wood, L., Tuminello, E., Han, S. D., … Bondi, M. W. (2010). Complex activities of daily living vary by mild cognitive impairment subtype. Journal of the International Neuropsychological Society, 16(04), 630–639. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2891154/
- Bates, D. W., & Bitton, A. (2010). The future of health information technology in the patient-centered medical home. Health Affairs, 29(4), 614–621.
- Bond, T. G., & Fox, C. M. (2007). Applying the Rasch model: Fundamental measurement in the human sciences. Mahwah, NJ: Lawrence Erlbaum Associates Publishers.
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences Hillsdale, NJ: Erlbaum.
- Coorey, G. M., Neubeck, L., Mulley, J., & Redfern, J. (2018). Effectiveness, acceptability and usefulness of mobile applications for cardiovascular disease self-management: Systematic review with meta-synthesis of quantitative and qualitative data. European Journal of Preventive Cardiology, 25, 505–521.
- Coughlin, J. F., Pope, J. E., & Leedle, B. R. (2006). Old age, new technology, and future innovations in disease management and home health care. Home Health Care Management & Practice, 18(3), 196–207.
- Csikszentmihalyi, M., & Larson, R. (1987). Validity and reliability of the experience sampling method. Journal of Nervous and Mental Disease, 175(9), 526–536.
- Engelhard, G. (1994). Examining rater errors in the assessment of written composition with a many‐faceted Rasch model. Journal of Educational Measurement, 31(2), 93–112.
- Fallahpour, M., Kottorp, A., Nygård, L., & Lund, M. (2014). Perceived difficulty in use of everyday technology in persons with acquired brain injury of different severity: A comparison with controls. Journal of Rehabilitation Medicine, 46(7), 635–641.
- Fallahpour, M., Kottorp, A., Nygård, L., & Lund, M. L. (2015). Participation after acquired brain injury: Associations with everyday technology and activities in daily life. Scandinavian Journal of Occupational Therapy, 22(5), 366–376.
- Fearing, V., Law, M., & Clark, J. (1997). An occupational performance process model: Fostering client and therapist alliances. Canadian Journal of Occupational Therapy, 64(1), 7–15.
- Fernández, M. D. M., Hernández, J. D. S., Gutiérrez, J. M., Escuela, M. R. H., & Fino, E. R. (2017). Using communication and visualization technologies with senior citizens to facilitate cultural access and self-improvement. Computers in Human Behavior, 66, 329–344.
- Fisher, A. G. (2009). Occupational Therapy Intervention Process Model: A model for planning and implementing top–down, client-centered, and occupation-based interventions. Ft. Collins, CO: Three Star Press.
- Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-Mental State": A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12(3), 189–198.
- Forsman, A. K., Nordmyr, J., Matosevic, T., Park, A.-L., Wahlbeck, K., & McDaid, D. (2017). Promoting mental wellbeing among older people: technology-based interventions. Health Promotion International, 33, 1042–1054. doi:
- Garand, L., Lingler, J. H., Conner, K. O., & Dew, M. A. (2009). Diagnostic labels, stigma, and participation in research related to dementia and mild cognitive impairment. Research in Gerontological Nursing, 2(2), 112–121.
- Grubbs, F. E., & Beck, G. (1972). Extension of sample sizes and percentage points for significance tests of outlying observations. Technometrics, 14(4), 847–854.
- Hadjistavropoulos, T., & Craig, K. D. (2002). A theoretical framework for understanding self-report and observational measures of pain: A communications model. Behaviour Research and Therapy, 40(5), 551–570.
- Hassan, E. (2005). Recall bias can be a threat to retrospective and prospective research designs. The Internet Journal of Epidemiology, 3(2), 339–412.
- Hauk, N., Hüffmeier, J., & Krumm, S. (2018). Ready to be a silver surfer? A meta-analysis on the relationship between chronological age and technology acceptance. Computers in Human Behavior, 84, 304–319.
- Hedman, A., Lindqvist, E., & Nygård, L. (2016). How older adults with mild cognitive impairment relate to technology as part of present and future everyday life: A qualitative study. BMC Geriatrics, 16, 73. doi:
- Hedman, A., Nygård, L., Malinowsky, C., Almkvist, O., & Kottorp, A. (2016). Changing everyday activities and technology use in mild cognitive impairment. British Journal of Occupational Therapy, 79(2), 111–119.
- Hoaglin, D. C., Iglewicz, B., & Tukey, J. W. (1986). Performance of some resistant rules for outlier labeling. Journal of American Statistical Association, 81(396), 991–999.
- Holbrook, M., & Skilbeck, C. E. (1983). An activity index for use with stroke patients. Age and Ageing, 12(2), 166–170.
- Kassberg, A.-C., Malinowsky, C., Jacobsson, L., & Lund, M. L. (2013). Ability to manage everyday technology after acquired brain injury. Brain Injury, 27(13-14), 1583–1588.
- Keningsberg, P.-A., Aquino, J.-P., Bérard, A., Brémond, F., Charras, K., Dening, T., … & Nguyen, M. (2017). Assistive technologies to address capabilities of people with dementia: From research to practice. doi:10.1177/1471301217714093
- Khosravi, P., Rezvani, A., & Wiewiora, A. (2016). The impact of technology on older adults’ social isolation. Computers in Human Behavior, 63, 594–603.
- Kielhofer, G. (2008). Model of human occupation: Theory and application (4th ed.) Baltimore: Wolters Kluwer/Lippincott Williams & Wilkins.
- Kottorp, A., & Nygård, L. (2011). Development of a short-form assessment for detection of subtle activity limitations: Can use of everyday technology distinguish between MCI and Alzheimer’s disease?. Expert Review of Neurotherapeutics, 11(5), 647–655.
- Kottorp, A., Nygård, L., Hedman, A., ÖHman, A., Malinoswky, C., Rosenberg, L., … Ryd, C. (2016). Access to and use of everyday technology among older people: A occupational justice issue - but for whom?. Journal of Occupational Science, 23, 382–388.
- Leicht, H., Berwig, M., & Gertz, H. J. (2010). Anosognosia in Alzheimer's disease: the role of impairment levels in assessment of insight across domains. Journal of the International Neuropsychological Society, 16(03), 463–473.
- Linacre, J. M. (2017a). FACETS: Many-Faceted Rasch Measurement Computer Program. Chicago: MESA Press.
- Linacre, J. M. (2017b). Winsteps-Rasch Measurement Computer Program. Chicago: MESA Press.
- Magaziner, J., Zimmerman, S. I., Gruber-Baldini, A. L., Hebel, J. R., & Fox, K. M. (1997). Proxy reporting in five areas of functional status: comparison with self-reports and observations of performance. American Journal of Epidemiology, 146(5), 418–428.
- Mak, E., Chin, R., Ng, L. T., Yeo, D., & Hameed, S. (2015). Clinical associations of anosognosia in mild cognitive impairment and Alzheimer's disease. International Journal of Geriatric Psychiatry, 30(12), 1207–1214.
- Malinowsky, C. (2011). Managing Technology in Everyday Activities: A study of older adults with dementia, MCI and no cognitive impairment. Stockholm.
- Malinowsky, C., Almkvist, O., Kottorp, A., & Nygård, L. (2011). Ability to manage everyday technology: A comparison of persons with dementia or mild cognitive impairment and older adults without cognitive impairment. Disability and Rehabilitation: Assistive Technology, 5, 462–469. doi:
- Malinowsky, C., Almkvist, O., Nygård, L., & Kottorp, A. (2011). Psychometric evaluation of a new assessment of the ability to manage technology in everyday life. Scandinavian Journal of Occupational Therapy, 18, 26–35. doi:
- Malinowsky, C., Kottorp, A., Patomella, A.-H., Rosenberg, L., & Nygård, L. (2015). Changes in the technological landscape over time: Relevance and difficulty levels of everyday technologies as perceived by older adults with and without cognitive impairment. Technology and Disability, 27(3), 91–101.
- Malinowsky, C., & Larsson-Lund, M. (2014). The association between perceived and observed abilities to use everyday technology in people of working age with ABI. Scandinavian Journal of Occupational Therapy, 21, 465–472.
- McDougall, S., & House, B. (2012). Brain training in older adults: Evidence of transfer to memory span performanceand pseudo-Matthew effects. Ageing, Neuropsychology & Cognition, 19(1-2), 195–221.
- Nygård, L. (2006). How can we get access to the experiences of people with dementia?. Scandinavian Journal of Occupational Therapy, 13(2), 101–112.
- Nygård, L. (2008). The meaning of everyday technology as experienced by people with dementia who live alone. Dementia, 7(4), 481–502.
- Nygård, L., Kottorp, A., & Rosenberg, L. (2015). Making use of research: Clinical views on an evaluation of everyday technology use. Scandinavian Journal of Occupational Therapy, 22(1), 24–32.
- Nygård, L., Rosenberg, L., & Kottorp, A. (2015). Manual Everyday Technology Use Questionnaire: ETUQ Everyday technology in activities at home and society. Stockholm.
- Pfeffer, R. I., Kurosaki, T. T., Harrah, C. H. J., Chance, J. M., & Filos, S. (1982). Measurement of functional activities in older adults in the community. Journal of Gerontology, 37(3), 323–329.
- Ready, R. E., Ott, B. R., & Grace, J. (2004). Patient versus informant perspectives of quality of life in mild cognitive impairment and Alzheimer's disease. International Journal of Geriatric Psychiatry, 19(3), 256–265.
- Rosenberg, L., Nygård, L., & Kottorp, A. (2009). Everyday technology use questionnaire: psychometric evaluation of new assessment of competence in technology use. OTJR: Occuation. Participation, Health, 29(2), 52–62.
- Ryd, C., Nygård, L., Malinowsky, C., Öhman, A., & Kottorp, A. (2015). Associations between performance of activities of daily living and everyday technology use among older adults with mild stage Alzheimer’s disease or mild cognitive impairment. Scandinavian Journal of Occupational Therapy, 22(1), 33–42.
- Ryd, C., Nygård, L., Malinowsky, C., Öhman, A., & Kottorp, A. (2017). Can the everyday technology use questionnaire predict overall functional level among older adults with mild cognitive impairment or mild-stage alzheimer's disease? - A pilot study. Scandinavian Journal of Caring Sciences, 31(1), 201–209.
- Schmitter-Edgecombe, M., Parsey, C., & Cook, D. J. (2011). Cognitive correlates of functional performance in older adults: Comparison of self-report, direct observation, and performance-based measures. Journal of the International Neuropsychological Society, 17(05), 853–864.
- Schmitter-Edgecombe, M., & Parsey, C. M. (2014). Cognitive correlates of functional abilities in individuals with mild cognitive impairment: Comparison of questionnaire, direct observation, and performance-based measures. The Clinical Neuropsychologist, 28(5), 726–746.
- Schulz, E., Wahl, H.-W., Matthews, J. T., De Vito Dabbs, A., Beach, S. R., & Czaja, S. J. (2015). Advancing the aging and technology agenda in gerontology. The Gerontologist, 55(5), 724–734.
- Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment The Annual Review of Clinical Psychology, 4(1), 1–32.
- Walter, S. D., Eliasziw, M., & Donner, A. (1998). Sample size and optimal design for reliability studies. Statistics in Medicine, 17(1), 101–110.
- Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L.-O., … Petersen, R. C. (2004). Mild cognitive impairment–beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. Journal of Internal Medicine, 256(3), 240–246.
- Ziefle, M., & Bay, S. (2005). How older adults meet complexity: Aging effects on the usability of different mobile phones. Behaviour & Information Technology, 24(5), 375–389.
- Zwakhalen, S. M., Hamers, J. P., Abu-Saad, H. H., & Berger, M. P. (2006). Pain in elderly people with severe dementia: A systematic review of behavioural pain assessment tools. BMC Geriatrics, 6(1), 3.