
ABSTRACT
Recent studies suggest that the lived environment can affect cognition across the lifespan. We examined, in a large cohort of older adults (n = 3447), whether susceptibility to a multisensory illusion, the Sound-Induced Flash Illusion (SIFI), was influenced by the reported urbanity of current and childhood (at age 14 years) residence. If urban environments help to shape healthy perceptual function, we predicted reduced SIFI susceptibility in urban dwellers. Participants reporting urban, compared with rural, childhood residence were less susceptible to SIFI at longer Stimulus-Onset Asynchronies (SOAs). Those currently residing in urban environments were more susceptible to SIFI at longer SOAs, particularly if they scored low on general cognitive function. These findings held even when controlling for a several covariates, such as age, sex, education, social participation and cognitive ability. Exposure to urban environments in childhood may influence individual differences in perception and offer a multisensory perceptual benefit in older age.
Introduction
Our world is becoming more urbanized and, simultaneously, the average age of the population is increasing. Understanding the impact of urbanization upon physical and cognitive health across the lifespan is therefore critical to public health and is of global interest.
Exposure to urban environments may confer some cognitive benefits across the life-course. Dementia and cognitive impairment in aging are more frequent in rural than in urban dwellers, even when lifestyle and accessibility of services are taken into account (for review see Cassarino & Setti, Citation2015). Proposed accounts for these differences include education (Contador et al., Citation2015; Jia et al., Citation2014; Weden et al., Citation2018), social participation (Vogelsang, Citation2016) and socioeconomic factors (Nunes et al., Citation2010). However, Cassarino and Setti (Citation2015) proposed that exposure to a multiplicity of sensory stimulation might serve to “train the brain”. Living in areas with a mix of residential and land-use services has been associated with better cognitive performance in aging (Wu et al., Citation2016), which has been ascribed to the opportunities for cognitive stimulation offered by a more complex environment (Cassarino & Setti, Citation2016; Wu et al., Citation2015).
One aspect of the environment that might have an impact with regards to brain training is that it is multisensory in nature, and the multisensory properties of our environment may differ depending on urbanity level. Urban environments present an abundance of sensory input; the sounds of pedestrian crossings, the sirens and flashing lights of emergency vehicles, competing smells from restaurants, the touch of colliding passersby. The urban world is a multisensory metropolis. Whilst rural environments also include multisensory cues, the nature of these cues differ from those in the urban world. For example, the urban world contains more visual “clutter” (Linnell et al., Citation2013), “man-made” sounds and higher auditory noise levels (European Environment Agency, Citation2020), whilst rural landscapes, which contain more open spaces and sounds associated with nature, can pose lower sensory and cognitive demands (see Cassarino & Setti, Citation2016). Given the differences in these sensory environments it might be expected that multisensory perception is differentially shaped by urbanity.
The ability to coordinate and integrate several senses appears to be fundamental to healthy cognition across the lifespan. For example, children (Denervaud et al., Citation2020) and older adults (Murray et al., Citation2018) who show faster response times for multisensory relative to unisensory stimuli also show better cognitive performance. Following this, inefficient patterns of multisensory integration have been associated with Mild Cognitive Impairment (Chan et al., Citation2015), falls and balance (Setti et al., Citation2011; Stapleton et al., Citation2014) and poorer global cognitive performance (Hernández et al., Citation2019) in older adults. Furthermore, working memory load has also been shown to affect multisensory integration in young adults (Michail & Keil, Citation2018). There are therefore evident links between multisensory perception and cognition as well as urbanization and cognition. However, whether urbanization and multisensory perception are related remains, to our knowledge, unexplored. In this study, we therefore investigated the impact of the lived environment on multisensory perception in aging.
In a study of 3765 older adults from 'The Irish Longitudinal Study on Ageing' (TILDA), Cassarino et al. (Citation2016) reported that older adults currently dwelling in urban environments showed better general cognitive and executive function compared with their rural counterparts. When population density was considered as a proxy for urbanization, the effect of urbanization on cognitive function was modulated by the presence of functional limitations (i.e. physical disabilities and difficulties experienced with activities in daily living, Cassarino et al., Citation2018). In Cassarino et al.’s 2016 study, the greatest benefits to cognitive function were observed in rural-living participants reporting an urban compared with a rural childhood. These participants showed cognitive performance similar to those reporting an urban residence currently as well as in childhood (i.e. their performance was better than those reporting childhood-rural and current-rural residence). Thus, it is possible that urban environments provide the necessary cognitive stimulation during childhood that might serve to benefit cognitive aging (White & Shah, Citation2019).
Living in the urban world requires a different approach to monitoring the environment for interesting or dangerous objects or situations. Urban dwellers tend to prioritize divided (or exploratory) over focused attention (Linnell et al., Citation2013), and this might be driven by differences in attention mechanisms that are influenced by arousal (Linnell & Caparos, Citation2020; Linnell et al., Citation2014). The environment currently lived in also appears to influence perception, as urban dwellers manifest global processing biases, utilizing irrelevant contextual information to guide perceptual judgments (see White & Shah, Citation2019 for discussion). For example, urban dwellers are more susceptible to the Ebbinghaus illusion, in which size estimates for a central circle are influenced by the size of surrounding irrelevant circles (Caparos et al., Citation2012; De Fockert et al., Citation2007). This effect of urbanity emerges in childhood (Bremner et al., Citation2016). However, Caparos et al. (Citation2012) also found that even brief exposure to urban environments was sufficient to induce global biases in rural dwellers. If urban exposure in childhood does serve to change perception, it is therefore possible that these perceptual changes remain malleable in adulthood depending on the characteristics of the lived environment.
It is possible that processing information at a global level poses an adaptive advantage in the urban world. For example, whilst crossing the road, several signals may need to be processed in order to cross safely; a person might want to focus on the pedestrian crossing signal (the red/green person), but might also want to be aware of an approaching cyclist or a bump in the pavement that could cause a trip (White & Shah, Citation2019). Although one might encounter these situations in both urban and rural contexts, such perceptually complex situations might be expected to occur more frequently in the urban world. Thus, processing global context information might be relatively beneficial when navigating urban areas.
Despite the multisensory nature of the environment, it has yet to be determined whether urban dwellers manifest global biases in multisensory contexts. For example, it is unclear whether urban residents are more likely to integrate multiple sensory signals separated in space and/or time. Based on existing evidence, it might be expected that perception in urban dwellers would also be more affected by irrelevant cross-sensory information, but this has not yet been tested.
A well-established paradigm in which irrelevant information influences perception across the senses is the Sound-Induced Flash Illusion (SIFI) (Shams et al., Citation2000, Citation2002; for reviews see Hirst et al., Citation2020; Keil, Citation2020). In this illusion presenting one visual “flash” with two sequential “beeps” results in the perception of two flashes, even though only one was physically presented. Critically, in this illusion, perception is influenced by learned “rules of thumb” regarding how the world ought to appear. In Bayesian terms, these rules of thumb are termed “priors”, and these priors are used to guide quick and optimal perceptual judgments (for an outline as to how priors are implemented in audiovisual perception at the neurocomputational level see Ursino et al., Citation2019). Susceptibility to the SIFI appears to arise from such Bayesian optimal inference, combined with the reliability of the information encoded by each sense (Shams, Ma et al., Citation2005). Thus, if an individual’s perceptual system expects discontinuous visual input (multiple flashes) and audition is relatively more reliable than vision (perhaps due to better temporal acuity, e.g., Welch et al., Citation1986), it is likely that participants will report that they saw two flashes when one flash was paired with two beeps. In line with this, Wang et al. (Citation2019) showed that if participants were informed that multiple flashes would occur on a higher proportion of trials, illusory responses were more likely to occur.
Age-related change in vision and hearing has been shown to account for some, but not all, age-related change in SIFI susceptibility (Hirst et al., Citation2020, Citation2019). Thus, it is important to consider the broad range of factors giving rise to individual differences in perception. It has been suggested that exposure to natural versus urban scenes can influence temporal perception (Berry et al., Citation2015). Given the role of perceptual priors in SIFI susceptibility, it would be expected that susceptibility to this illusion might differ between individuals who have been exposed to urban versus rural environments, in which the temporal statistics of the environment may differ in terms of the amount and type of multisensory exposure.
In 2014, The 'Irish Longitudinal Study on Ageing' (TILDA) became the first large-scale study on aging globally to integrate a measure of multisensory function (a task based on the SIFI) into its healthcare assessment. As TILDA also includes data on childhood and current exposure to urban and rural environments (Cassarino et al., Citation2016, Citation2018), this affords us, for the first time, the opportunity to investigate the impact of urban environments on multisensory perception. This is a critical question if we are to understand how urbanization shapes the ability to deal with multiple sensory inputs in our ever-aging population, particularly in light of the close link between unisensory (Dupuis et al., Citation2015; F. R. Lin et al., Citation2013; M. Y. Lin et al., Citation2004; Loughrey et al., Citation2018; See et al., Citation2011) and multisensory function (Chan et al., Citation2015; Hernández et al., Citation2019) and cognition in aging.
On the one hand, if perception in urban dwellers is more refined due to repeated exposure to congruous and incongruous multisensory stimuli then it might be expected that those participants should be less susceptible to the SIFI, particularly when temporal discrepancy between multisensory stimuli (i.e. Stimulus Onset Asynchrony, SOA) is large. Consistent with this, increased SIFI susceptibility has been linked with poorer cognitive function in older adults (Chan et al., Citation2015) including the TILDA cohort (Hernández et al., Citation2019) and it has been argued that urban environments have a benefit on cognitive function (Cassarino et al., Citation2016, Citation2018). Thus, we might expect participants exposed to urban environments to show patterns of multisensory performance consistent with healthier cognitive profiles (e.g., be less susceptible to the SIFI). On the other hand, if urban dwellers have a global processing bias, and this extends to multisensory contexts (and the temporal domain), we would expect urbanites to be more influenced by irrelevant auditory information when making visual judgments (e.g., be more susceptible to the SIFI). Critically, we examined the role of both current and childhood environments in shaping multisensory perception, thus we can consider the impact of urbanization upon future generations growing up in the urbanized world.
Methods
Participants
Participants were drawn from wave 3 of the 'Irish Longitudinal Study on Ageing' (TILDA), a population representative sample of individuals over 50 years of age from across the Republic of Ireland (for details of the sampling design see Whelan and Savva, Citation2013). Participants completed a Computer Assisted Personal Interview (CAPI) carried out by a trained interviewer as well as a comprehensive clinic-based health assessment, in which the SIFI was administered. The study was approved by the Trinity College Faculty of Health Sciences Ethics Committee. Testing protocols conformed to the Declaration of Helsinki and data collection and storage complied with European GDPR. All participants provided written, informed consent when they first participated in the study and consent was repeated at wave 3 (the focus of this study). Nurses performing the healthcare assessment were informed that participants who were deaf and/or blind would not be eligible to partake in the SIFI test. outlines the operationalization of variables included in the models and outlines sample selection protocol. As shown in the final sample consisted of mainly female participants and ranged 50 to 93 years of age. Most participants reported obtaining a minimum of secondary school education. General cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), and data from participants obtaining a score below 23, indicating possible mild cognitive impairment, were excluded (Carson et al., Citation2018).
Table 1. Variables included in the model and operationalization of each measure. LogMAR = acuity score for the better eye the visual acuity score (VAS) inverts the LogMAR scale such that a score of 100 represents a logMAR score of 0 or 20/20 vision and lower scores indicate poorer vision, 2B0F = accuracy for judging 2 Beeps presented with no Flashes with 70 ms SOA, 0B2F = accuracy for judging 2 Flashes presented with no Beeps with 70 ms SOA 1B1F = accuracy for judging 1 Flash presented with 1 Beep. SOA = Stimulus Onset Asynchrony, MoCA = Montreal Cognitive Assessment, NART = National Adult Reading Test, TIA = Transient Ischemic Attack
Table 2. Demographic information for participants reporting childhood and current urban/rural residence. Categorical variables are shown as count (%). MoCA = Montreal Cognitive Assessment, NART = National Adult Reading Test, VAS = Visual Acuity Score
Figure 1. Sampling selection procedure. MoCA = Montreal Cognitive Assessment, NART = National Adult Reading Test.
Procedure
Residence
The geographical location of residence of the respondent at the time of the interview was assessed by the interviewer according to three categories: (a) urban, (b) other settlements, (c) rural areas. These categories were assessed based on the Irish Census, 2011 (www.cso.ie), such that the “urban” category refers to the Dublin area, which is the only urban settlement with more than one million inhabitants in the Republic of Ireland, “other settlements” included five cities, five boroughs, and 75 towns with a population ranging from 1,500 to less than 200,000 inhabitants, rural areas were settlements with a population of less than 1,500. Childhood residence was assessed via self-report, when participants first took part in the TILDA study, they were asked “Were you living in a rural area when you were about age 14?”, participants responding “yes” and “no” to this question were characterized as having rural and urban childhood residence respectively (see for characteristics of each group).
Sound-induced flash illusion
The specific task based on the Sound-Induced Flash Illusion (SIFI) used in TILDA has been described elsewhere (see Hernández et al., Citation2019; Hirst et al., Citation2019). Testing took place in a dimly lit testing room with the nurse who conducted the healthcare assessment. Participants were seated in front of a computer (Dell Latitude E6400 with Intel Core 2 Duo CPU, 2Gb RAM, using Windows 7 Professional OS, 60 Hz refresh rate) and instructed to look at the fixation cross at the center of the screen. If the participant usually wore glasses or hearing aids they also wore them during the assessment. A fixation cross marked the start of each trial and appeared for 1000 ms. The visual and/or auditory stimuli were then presented. The visual stimulus comprised a white disc (1.5° visual angle, 32fl luminance approximately), projected onto a black background positioned 5 cm below the central fixation (4.77° visual angle) cross for 16 ms. Viewing distance was approximately 60 cm. Auditory beeps were brief bursts of 3500 Hz sounds (10 ms, 1 ms ramp), presented aloud at approximately 80 dB via the inbuilt speakers in the laptop.
The main testing block contained multisensory illusory trials (2B1F) multisensory non-illusory trials (2B2F, 1B1F) and unisensory visual trials (0B2F, 0B1F).Footnote1 Illusory trials (2B1F) were presented at one of six SOAs, −230 ms, −150 ms, −70 ms, 70 ms, 150 ms, 230 ms, where negative values indicate that the second beep was presented before the flash-beep pair (which we refer to as “Pre” in our analysis, as opposed to “Post” where the second beep followed the flash). Congruent 2B2F trials were presented at three SOAs, 70 ms, 150 ms, 230 ms. Unisensory 0B2F trials were presented at one SOA, 70 ms. Each trial type was presented twice within a block and in random order across participants. Before the main testing block, a practice phase was presented comprising one trial from each of the following conditions: illusory 2B1F (SOAs of 70, 150, and 230), non-illusory 2B2F and 1B1F, and unisensory visual 0B2F 70 ms. Participants were asked to report the number of visual flashes perceived. Once a response was provided, the nurse, who sat near the participant, recorded the participant’s vocal responses by pressing the corresponding number key on a laptop. The nurse then pressed the space bar to continue to the next trial. A separate block of unisensory auditory trials was then presented. In this block, either 1 beep or 2 beeps were presented in the absence of any flash (1B0F, 2B0F). In the unisensory 2B0F condition, the two beeps were presented at three SOAs, 70 ms, 150 ms, and 230 ms. Participants were asked to identify the number of beeps they heard. As in the main block, the nurse pressed the corresponding key once a verbal response was given. Two trials per condition were presented in this block.
Data analysis
Statistical analyses were performed in the R statistical programming environment (R studio version 3.6.1; R CoreTeam, Citation2018). Our dependent variable was accuracy for judging the number of flashes. This score represented the proportion correct (0, 0.5 or 1) for each participant. We therefore implemented generalized logistic mixed-effect models using “glmer” in the “lme4” package (family = “binomial”) (Bates et al., Citation2015).
Our fixed effects of interest were Stimulus Onset Asynchrony (SOA), childhood residence (rural or urban), and current residence (Dublin city/county, another city or town, rural). To assess if residence moderated the pattern of performance on the SIFI we included three interactions terms: SOA x childhood residence, SOA x current residence, and SOA x childhood residence x current residence. The significance of SOA and the interaction terms were assessed using likelihood ratio tests (comparing the fit of each model with and without that term, whilst considering covariates). A list of all covariates included in the model and their operationalization are shown in , the formulae of all models are shown in supplementary material. We report four models:
Model 1 included all terms and is non-adjusted;
Model 2 included all terms and is adjusted for relevant covariates;
Model 3 included only interaction terms that significantly improved model fit and is adjusted for relevant covariates (i.e. Model 2 without the three-way interaction between SOA, current residence and childhood residence);
Finally, Model 4 included additional interaction terms to, firstly, assess whether the observed effects withstood the inclusion of previously reported interactions (SOA x MoCA and SOA x sex; Hernández et al., Citation2019) and, secondly, to further assess the relationship between general cognition (MoCA), residence, and SOA.
For completion, we conducted supplementary analyses, which indicated that the urbanity of childhood and/or current residence did not influence unisensory performance (see Supplementary section S4).
Results
As shown in , the odds of making a correct response in the 2B1F illusory condition were significantly lower at both 150 ms and 230 ms SOA relative to the 70 ms SOA reference condition for both groups. A likelihood ratio test showed that including the factor “SOA” significantly improved the fit of the model (χ2(2) = 2252.3, p <.001).
Figure 2. A) Odds ratio for making a correct response on illusory 2B1F trials (i.e. a “one flash” response) based on predictors included for models 1, 3 and 4. For complete results see Supplementary Table S1. Lower panels show the predicted probability of accuracy at each SOA for participants grouped on childhood residence at around age 14 years (panel b) and current residence (panel c). 95% confidence intervals are shown. SOA = Stimulus Onset Asynchrony, MoCA = Montreal Cognitive Assessment, Curr. = Current.
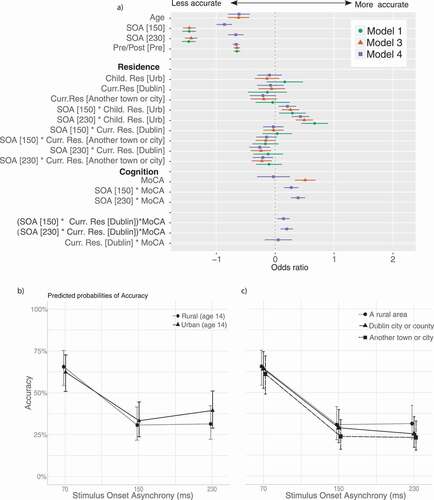
Childhood residence interacted with SOA. Considering reference performance at 70 ms, participants reporting an urban childhood residence were less susceptible to the illusion (i.e. more accurate) at longer SOAs compared with those reporting a rural childhood residence, this comparison reached significance at both 150 and 230 ms SOA (see ). The childhood residence by SOA interaction term significantly improved the model fit (χ2(2) = 43.59, p < .001).
A likelihood ratio test showed that the three-way interaction between childhood residence, current residence, and SOA did not significantly improve the model fit (χ2(6) = 7.48, p = .279). As such, although the interaction between current residence and SOA did significantly improve the fit of the model containing all terms (χ2(4) = 13.13, p = .011), this effect was seen only when the three-way interaction was dropped from the model. Dropping the three-way interaction from the model showed that participants reporting a current urban residence were more susceptible to the illusion at the longest SOA of 230 ms, considering performance in the reference condition (70 ms) relative to rural dwellers (, model 3 and ).
As previously reported (Hernández et al., Citation2019), those with higher MoCA scores were less susceptible to the SIFI at longer SOAs and females were more susceptible to the SIFI at longer SOAs. Both interaction terms (MoCAx SOA and sex x SOA) significantly improved model fit (χ2(2) = 164.66, p < .001 and χ2(2) = 409.6, p < .001 respectively). To assess whether the relationships between residency and SIFI performance at longer SOAs could be linked to cognitive function, we included two additional three-way interaction terms, Childhood residence x SOA x MoCA and Current residence x SOA x MoCA, the three-way interaction with current, but not childhood, residence improved model fit (χ2(6) = 14.142, p = .028 and χ2(3) = 6.332, p = .097 respectively). For those currently living in the most urban areas (i.e. Dublin), lower general cognition coincided with less efficient multisensory processing (i.e. greater SIFI susceptibility; see Supplemental figure, section S3).
Discussion
In this study, we examined the effect of urban compared with rural residence, both currently and in childhood, upon multisensory perception in aging. The findings showed that, relative to those reporting a rural childhood, participants reporting an urban childhood environment were less susceptible to the Sound-Induced Flash Illusion (SIFI) at longer Stimulus-Onset Asynchronies (SOAs); a pattern consistent with performance in younger compared with older adults (e.g., McGovern et al., Citation2014) and termed “efficient” multisensory integration based on associated clinical outcomes (Setti et al., Citation2011, Citation2014). Notably, an effect of residence was not observed at shorter SOAs. Given that reduced temporal acuity rather than differences in multisensory perception per se are associated with performance at short SOAs (Hirst et al., Citation2020), and given the adverse outcomes that have been associated with sustained SIFI susceptibility at longer SOAs (e.g., Chan et al., Citation2015; Setti et al., Citation2011) we focus our discussion on the effects we observed in this study at longer SOAs. It has already been proposed that urban childhood residence may positively affect cognitive function in aging (Cassarino et al., Citation2016, Citation2018), and that urban environments can “train” the brain (Cassarino & Setti, Citation2015). Our results extend these findings to the realm of multisensory perception.
In contrast to the results based on childhood residence, we observed that participants currently residing in urban, rather than rural, environments were more susceptible to the SIFI at long SOAs, and this was most prominent in those with lower scores on general cognitive function (MoCA).Footnote2 This result appears consistent with findings in the spatial domain (e.g., the Ebbinghaus illusion), showing that visual perception in urban dwellers is influenced by irrelevant information separated in space, reflecting a global processing bias (Bremner et al., Citation2016; Caparos et al., Citation2012). Our findings may suggest this may extend to the temporal domain, as those currently living in urban environments were more likely to process irrelevant information separated in time. Furthermore, our findings imply that the effect of current residence, but not childhood residence, appears more associated with general cognitive function. Since the majority of the global processing literature has focused on the visual, spatial domain, an interesting direction for multisensory research would be to explore if the lived environment influences the integration of multisensory information separated in space, such as in the ventriloquist illusion (Howard & Templeton, Citation1966) or in terms of integration “capacity” (Van der Burg et al., Citation2013; Wilbiks & Dyson, Citation2018).
The effect of urbanity on global versus local processing biases has been shown to shift depending on the current lived-in environment (Caparos et al., Citation2012), and our findings of differing effects of childhood and current residence are consistent with this. It is possible that the effect of current lived-in environment is linked to higher level processing, as suggested by the interaction with the MoCA. Converging neuroimaging evidence shows that the SIFI results from early, direct modulation of visual cortex by auditory inputs (Shams, Iwaki et al., Citation2005; Watkins et al., Citation2007, Citation2006). The mechanisms by which SIFI is mediated by cognitive functions appear less clear. Whilst the SIFI has been found to be moderated by memory load (Michail & Keil, Citation2018) and cognitive expectation (Wang et al., Citation2019) other cognitive manipulations such as attentional orienting do not appear to moderate the illusion. For example, explicitly instructing participants to attend to one or the other modality (Odegaard et al., Citation2016) and explicit feedback training does not appear to modulate illusion perception (Rosenthal et al., Citation2009). The relationship between the current lived environment, cognitive function and multisensory perception in aging therefore requires further empirical investigation, beyond what can be determined from associative studies.
In sum, whilst cognitively demanding urban environments in childhood appear to pose benefits for perceptual efficiency, exposure to these same environments in later life may have a differing effect on perception (increasing SIFI susceptibility), particularly in those with lower cognitive scores. However, as the effect of current residence was less prominent than the effect of childhood residence (see ), our conclusion is offered cautiously, with further empirical work required to fully elucidate the impact of current urban versus rural residence on perceptual function in later life.
It is notable that the SIFI is temporal in nature, and it would be expected that perceptual priors influencing the SIFI should be fundamentally shaped by the temporal statistics of the environment. Whilst we do not have a thorough mapping of the temporal regularities for each environment in the current analysis, it might be expected that temporal discontinuity would be expected to be more frequent in urban environments, thus shaping perception (see Hirst et al., Citation2020; Shams et al., Citation2000, for descriptions of a discontinuity hypothesis in SIFI). One possibility is that, urban environments shape priors in a way that reduce the likelihood of coupling auditory and visual information i.e. a reduced common source prior (Ernst, Citation2010; Shams & Beierholm, Citation2010), possibly because these individuals are exposed to an abundance of sensory cues that do not originate from a common source. However, without an empirical assessment of the temporal visual and auditory environment in rural and urban settings we cannot be sure that an imbalance of temporal regularities exists in the current study. This reflects a limitation of the current study, and a direction for future investigation. There are, of course, additional limitations that should be considered. For example, although TILDA provides a wealth of data by which to control for confounding factors, participants’ data were not tested for neurodevelopmental disorders which might influence perceptual function (e.g., ASD, Schizophrenia, etc). Secondly, the categorization of urban vs. rural environments we implemented may be too broad. Although this approach remains informative, it is possible that a more fine-grained analysis of environmental exposure and the temporal statistics of the environment, would allow more precise insight regarding this question. The current findings provide clear justification to further investigate the impact that an increasingly urban and multisensory world may have upon perceptual and cognitive function across the life-course.
Conclusions
We show for the first time that susceptibility to the Sound-Induced Flash Illusion (SIFI) at long Stimulus Onset Asynchronies (SOAs) is reduced in older adults reporting urban, versus rural, childhood residence. Furthermore, we found that those reporting current urban residence were more susceptible to the illusion at longer SOAs and that this was strongest in those with lower scores on general cognitive function. These findings support the conclusion that cognitively and perceptually demanding urban environments in childhood may pose advantages for perceptual function in aging (e.g., more “efficient” multisensory integration). However, critical remaining questions are whether this benefit might be mitigated by current residence, and how this relates to cognitive function in later life.
Author contribution statement
The Irish Longitudinal Study on Ageing (TILDA) is an interdisciplinary project coordinated by R.A.K. A.S and F.N.N designed the protocol for the Sound-Induced Flash Illusion incorporated into TILDA. R.J.H., A.S. M.C. and F.N.N developed the analysis plan and R.J.H. conducted the analysis and prepared the manuscript for publication for which F.N.N., M.C. and A.S. provided feedback and revisions. All authors approved the final version of the manuscript for submission.
Ethics approval
The study was approved by the Trinity College Faculty of Health Sciences Ethics Committee.
Consent to participate
All participants provided written, informed consent when they first participated in the study and consent was repeated at wave 3 (the focus of this study).
Consent for publication
No identifying participant information is published in the current manuscript.
Code availability
The code used for this analysis is available upon reasonable request from the author.
ANC-OA_20-75-File004.docx
Download MS Word (82.3 KB)Acknowledgments
This work was supported by the Health Research Board (HRB); Grant reference ILP-PHR-2017-014.
Declarations Disclosure statement
The authors have no conflicts of interest to declare.
Data availability
TILDA has a public database that includes unisensory and cognitive measures included in the current analysis available at https://tilda.tcd.ie/data/accessing-data/a list of studies using data from this database can be found at https://tilda.tcd.ie/publications/papers/. The SIFI data is planned to be included in future releases of the TILDA dataset, subject to General Data Protection Regulation. For information on hot desk applications see https://tilda.tcd.ie/data/accessing-data/hotdesk/.
Supplementary material
Supplemental data for this article can be accessed here
Additional information
Funding
Notes
1. “B” and “F” indicate the number of Beeps and Flashes, respectively.
2. Although beyond the scope of the current study, it is important to note that the MoCA reflects a general diagnostic tool for cognitive impairment, and all participants in our selected sample scored above the cutoff for mild cognitive impairment.
References
- Bates, D., Maechler, M., Bolker, B., & Steve, W. (2015). Fitting linear mixed-effects models using lme4. Journal of Statistical Software, 67(1), 1–48. https://doi.org/10.18637/jss.v067.i01
- Berry, M. S., Repke, M. A., Nickerson, N. P., Conway, L. G., Odum, A. L., & Jordan, K. E. (2015). Making time for nature: Visual exposure to natural environments lengthens subjective time perception and reduces impulsivity. PLoS ONE, 10(11), 1–16. https://doi.org/https://doi.org/10.1371/journal.pone.0141030
- Bremner, A. J., Doherty, M. J., Caparos, S., de Fockert, J., Linnell, K. J., & Davidoff, J. (2016). Effects of culture and the Urban environment on the development of the ebbinghaus illusion. Child Development, 87(3), 962–981. https://doi.org/https://doi.org/10.1111/cdev.12511
- Caparos, S., Ahmed, L., Bremner, A. J., de Fockert, J., Linnell, K. J., & Davidoff, J. (2012). Exposure to an urban environment alters the local bias of a remote culture. Cognition, 122(1), 80–85. https://doi.org/https://doi.org/10.1016/j.cognition.2011.08.013
- Carson, N., Leach, L., & Murphy, K. J. (2018). A re-examination of montreal cognitive assessment (MoCA) cutoff scores. International Journal of Geriatric Psychiatry, 33(2), 379–388. https://doi.org/https://doi.org/10.1002/gps.4756
- Cassarino, M., O’Sullivan, V., Kenny, R. A., & Setti, A. (2016). Environment and cognitive aging: A cross-sectional study of place of residence and cognitive performance in the Irish Longitudinal Study on Aging. Neuropsychology, 30(5), 543–557. https://doi.org/https://doi.org/10.1037/neu0000253
- Cassarino, M., O’Sullivan, V., Kenny, R. A., & Setti, A. (2018). Disabilities moderate the association between neighbourhood urbanity and cognitive health: Results from the Irish longitudinal study on ageing. Disability and Health Journal, 11(3), 359–366. https://doi.org/https://doi.org/10.1016/j.dhjo.2017.12.002
- Cassarino, M., & Setti, A. (2015). Environment as “brain training”: A review of geographical and physical environmental influences on cognitive ageing. Ageing Research Reviews, 23, 167–182. https://doi.org/https://doi.org/10.1016/j.arr.2015.06.003
- Cassarino, M., & Setti, A. (2016). Complexity as key to designing cognitive-friendly environments for older people. Frontiers in Psychology, 7(AUG), 1–12. https://doi.org/https://doi.org/10.3389/fpsyg.2016.01329
- Chan, J. S., Kaiser, J., Brandl, M., Matura, S., Prvulovic, D., Hogan, M., & Naumer, M. (2015). Expanded temporal binding windows in people with mild cognitive impairment. Current Alzheimer Research, 12(1), 61–68. https://doi.org/https://doi.org/10.2174/1567205012666141218124744
- Contador, I., Bermejo-Pareja, F., Puertas-Martin, V., & Benito-Leon, J. (2015). Childhood and adulthood rural residence increases the risk of Dementia: NEDICES study. Current Alzheimer Research, 12(4), 350–357. https://doi.org/https://doi.org/10.2174/1567205012666150324181327
- de Fockert, J., Davidoff, J., Fagot, J., Parron, C., & Goldstein, J. (2007). More accurate size contrast judgments in the ebbinghaus illusion by a remote culture. Journal of Experimental Psychology: Human Perception and Performance, 33(3), 738–742. https://doi.org/https://doi.org/10.1037/0096-1523.33.3.738
- Denervaud, S., Genatz, E., Matusz, P. J., & Murray, M. M. (2020). Multisensory gains in simple detection predict global cognition in schoolchildren. Scientific Reports, 10, 1394. https://doi.org/https://doi.org/10.1038/s41598-020-58329-4
- Dupuis, K., Pichora-Fuller, M. K., Chasteen, A. L., Marchuk, V., Singh, G., & Smith, S. L. (2015). Effects of hearing and vision impairments on the montreal cognitive assessment. Aging, Neuropsychology, and Cognition, 22(4), 413–437. https://doi.org/https://doi.org/10.1080/13825585.2014.968084
- Ernst, M. O. (2010). From independence to fusion: A comprehensive model for multisensory integration. Journal of Vision. 5 8 650 https://doi.org/https://doi.org/10.1167/5.8.650
- European Environment Agency. (2020). Potential quiet areas in Europe based upon the quietness suitability index (QSI), European Environment Agency, 2020. https://www.eea.europa.eu/data-and-maps/figures/quietness-suitability-index-qsi-1
- Hernández, B., Setti, A., Kenny, R. A., & Newell, F. N. (2019). Individual differences in ageing, cognitive status, and sex on susceptibility to the sound-induced flash illusion: A large-scale study. Psychology and Aging, 34(7), 978–990. https://doi.org/https://doi.org/10.1037/pag0000396
- Hirst, R. J., McGovern, D. P., Setti, A., Shams, L., & Newell, F. N. (2020). What you see is what you hear: Twenty years of research using the Sound-Induced Flash Illusion. Neuroscience & Biobehavioral Reviews, 118, 759–774. https://doi.org/https://doi.org/10.1016/j.neubiorev.2020.09.006
- Hirst, R. J., Setti, A., Kenny, R., & Newell, F. N. (2019). Age-related sensory decline mediates the Sound-Induced Flash Illusion: Evidence for reliability weighting models of multisensory perception. Scientific Reports, 9(19347). https://doi.org/https://doi.org/10.1038/s41598-019-55901-5
- Howard, I., & Templeton, W. B. (1966). Human spatial orientation. Wiley.
- Jia, J., Wang, F., Wei, C., Zhou, A., Jia, X., Li, F., Tang, M., Chu, L., Zhou, Y., Zhou, C., Cui, Y., Wang, Q., Wang, W., Yin, P., Hu, N., Zuo, X., Song, H., Qin, W., Wu, L., Jia, L., … Dong, X. (2014). The prevalence of dementia in urban and rural areas of China. Alzheimer’s and Dementia, 10(1), 1–9. https://doi.org/https://doi.org/10.1016/j.jalz.2013.01.012
- Keil, J. (2020). Double flash illusions: Current findings and future directions. Frontiers in Neuroscience, 14, 298. https://doi.org/https://doi.org/10.3389/fnins.2020.00298
- Lin, F. R., Yaffe, K., Xia, J., Xue, Q. L., Harris, T. B., Purchase-Helzner, E., Satterfield, S., Ayonayon, H. N., Ferrucci, L., & Simonsick, E. M. (2013). Hearing loss and cognitive decline in older adults. JAMA Internal Medicine, 173(4), 293–299. https://doi.org/https://doi.org/10.1001/jamainternmed.2013.1868
- Lin, M. Y., Gutierrez, P. R., Stone, K. L., Yaffe, K., Ensrud, K. E., Fink, H. A., Sarkisian, C. A., Coleman, A. L., & Mangione, C. M. (2004). Vision impairment and combined vision and hearing impairment predict cognitive and functional decline in older women. Journal of the American Geriatrics Society, 52(12), 1996–2002. https://doi.org/https://doi.org/10.1111/j.1532-5415.2004.52554.x
- Linnell KJ, Caparos S. Urbanisation, the arousal system, and covert and overt attentional selection. Curr Opin Psychol. 2020 Apr;32:100-104. doi:https://doi.org/10.1016/j.copsyc.2019.07.030. Epub 2019 Jul 21. PMID: 31430648. https://doi.org/https://doi.org/10.1016/j.copsyc.2019.07.030
- Linnell, K. J., Caparos, S., & Davidoff, J. (2014). Urbanization increases left-bias in line-bisection: an expression of elevated levels of intrinsic alertness?. Frontiers in psychology, 5, 1127. https://doi.org/https://doi.org/10.3389/fpsyg.2014.01127
- Linnell, K. J., Caparos, S., de Fockert, J. W., & Davidoff, J. (2013). Urbanization decreases attentional engagement. Journal of Experimental Psychology: Human Perception and Performance, 39(5), 1232–1247. https://doi.org/https://doi.org/10.1037/a0031139
- Loughrey, D. G., Kelly, M. E., Kelley, G. A., Brennan, S., & Lawlor, B. A. (2018). Association of age-related hearing loss with cognitive function, cognitive impairment, and dementia a systematic review and meta-analysis. JAMA Otolaryngology - Head and Neck Surgery, 144(2), 115–126. https://doi.org/https://doi.org/10.1001/jamaoto.2017.2513
- McGovern, D. P., Roudaia, E., Stapleton, J., McGinnity, T. M., & Newell, F. N. (2014). The sound-induced flash illusion reveals dissociable age-related effects in multisensory integration. Frontiers in Aging Neuroscience, 6(250), 1–9. https://doi.org/https://doi.org/10.3389/fnagi.2014.00250
- Michail, G., & Keil, J. (2018). High cognitive load enhances the susceptibility to non-speech audiovisual illusions. Scientific Reports, 8(1), 1–11. https://doi.org/https://doi.org/10.1038/s41598-018-30007-6
- Murray, M. M., Eardley, A. F., Edginton, T., Oyekan, R., Smyth, E., & Matusz, P. J. (2018). Sensory dominance and multisensory integration as screening tools in aging. Scientific Reports, 8(1), 8901. https://doi.org/https://doi.org/10.1038/s41598-018-27288-2
- Nunes, B., Silva, R. D., Cruz, V. T., Roriz, J. M., Pais, J., & Silva, M. C. (2010). Prevalence and pattern of cognitive impairment in rural and urban populations from Northern portugal. BMC Neurology, 10, 42. http://www.biomedcentral.com/1471-2377/10/42%5Cnhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed9&NEWS=N&AN=2010401561
- Odegaard, B., Wozny, D. R., & Shams, L. (2016). The effects of selective and divided attention on sensory precision and integration. Neuroscience Letters, 614, 24–28. https://doi.org/https://doi.org/10.1016/j.neulet.2015.12.039
- R CoreTeam. (2018). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. http://www.r-project.org/
- Rosenthal, O., Shimojo, S., & Shams, L. (2009). Sound-induced flash illusion is resistant to feedback training. Brain Topography, 21(3–4), 185–192. https://doi.org/https://doi.org/10.1007/s10548-009-0090-9
- See, A. Y., Anstey, K. J., & Wood, J. M. (2011). Simulated cataract and low contrast stimuli impair cognitive performance in older adults: Implications for neuropsychological assessment and everyday function. Aging, Neuropsychology, and Cognition, 18(1), 1–21. https://doi.org/https://doi.org/10.1080/13825585.2010.501404
- Setti, A., Burke, K. E., Kenny, R. A., & Newell, F. N. (2011). Is inefficient multisensory processing associated with falls in older people? Experimental Brain Research, 209(3), 375–384. https://doi.org/https://doi.org/10.1007/s00221-011-2560-z
- Setti, A., Stapleton, J., Leahy, D., Walsh, C., Kenny, R. A., & Newell, F. N. (2014). Improving the efficiency of multisensory integration in older adults: Audio-visual temporal discrimination training reduces susceptibility to the sound-induced flash illusion. Neuropsychologia, 61(1), 259–268. https://doi.org/https://doi.org/10.1016/j.neuropsychologia.2014.06.027
- Shams, L., & Beierholm, U. R. (2010). Causal inference in perception. Trends in Cognitive Sciences, 14(9), 425–432. https://doi.org/https://doi.org/10.1016/j.tics.2010.07.001
- Shams, L., Iwaki, S., Chawla, A., & Bhattacharya, J. (2005). Early modulation of visual cortex by sound: An MEG study. Neuroscience Letters, 378, 76–81. https://doi.org/https://doi.org/10.1016/j.neulet.2004.12.035
- Shams, L., Kamitani, Y., & Shimojo, S. (2000). What you see is what you hear. Nature, 408(6814), 788. https://doi.org/https://doi.org/10.1038/35048669
- Shams, L., Kamitani, Y., & Shimojo, S. (2002). Visual illusion induced by sound. Cognitive Brain Research, 14(1), 147–152. https://doi.org/https://doi.org/10.1016/S0926-6410(02)00069-1
- Shams, L., Ma, W. J., & Beierholm, U. (2005). Sound-induced flash illusion as an optimal percept. NeuroReport, 16(17), 1923–1927. https://doi.org/https://doi.org/10.1097/01.wnr.0000187634.68504.bb
- Stapleton, J., Setti, A., Doheny, E. P., Kenny, R. A., & Newell, F. N. (2014). A standing posture is associated with increased susceptibility to the sound-induced flash illusion in fall-prone older adults. Experimental Brain Research, 232(2), 423–434. https://doi.org/https://doi.org/10.1007/s00221-013-3750-7
- Ursino, M., Cuppini, C., Magosso, E., Beierholm, U., & Shams, L. (2019). Explaining the effect of likelihood manipulation and prior through a neural network of the audiovisual perception of space. Multisensory Research, 32(2), 87–109. https://doi.org/https://doi.org/10.1163/22134808-20191324
- van der Burg, E., Awh, E., & Olivers, C. N. L. (2013). The capacity of audiovisual integration is limited to one item. Psychological Science, 24(3), 345–351. https://doi.org/https://doi.org/10.1177/0956797612452865
- Vogelsang, E. M. (2016). Older adult social participation and its relationship with health: Rural-urban differences. Health and Place, 42(September), 111–119. https://doi.org/https://doi.org/10.1016/j.healthplace.2016.09.010
- Wang, A., Sang, H., He, J., Sava-Segal, C., Tang, X., & Zhang, M. (2019). Effects of cognitive expectation on sound-induced flash illusion. Perception, 48(12), 1214–1234. https://doi.org/https://doi.org/10.1177/0301006619885796
- Watkins, S., Shams, L., Josephs, O., & Rees, G. (2007). Activity in human V1 follows multisensory perception. NeuroImage, 37(2), 572–578. https://doi.org/https://doi.org/10.1016/j.neuroimage.2007.05.027
- Watkins, S., Shams, L., Tanaka, S., Haynes, J. D., & Rees, G. (2006). Sound alters activity in human V1 in association with illusory visual perception. NeuroImage, 31(3), 1247–1256. https://doi.org/https://doi.org/10.1016/j.neuroimage.2006.01.016
- Weden, M. M., Shih, R. A., Kabeto, M. U., & Langa, K. M. (2018). Secular trends in dementia and cognitive impairment of U.S. rural and urban older adults. American Journal of Preventive Medicine, 54(2), 164–172. https://doi.org/https://doi.org/10.1016/j.amepre.2017.10.021
- Welch, R. B., DutionHurt, L. D., & Warren, D. H. (1986). Contributions of audition and vision to temporal rate perception. Perception & Psychophysics, 39(4), 294–300. https://doi.org/https://doi.org/10.3758/BF03204939
- Whelan, B. J., Savva, G. M., 2013. Design and methodology of the Irish Longitudinal Study on Ageing. J. Am. Geriatr. Soc. 61, 265–268. https://doi.org/https://doi.org/10.1111/jgs.12199 61.
- White, H., & Shah, P. (2019). Attention in urban and natural environments. Yale Journal of Biology and Medicine, 92(1), 115–120. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6430180/thepubmedIDis30923478.
- Wilbiks, J. M. P., & Dyson, B. J. (2018). The contribution of perceptual factors and training on varying audiovisual integration capacity. Journal of Experimental Psychology: Human Perception and Performance, 44(6), 871–884. https://doi.org/https://doi.org/10.1037/xhp0000503
- Wu, Y. T., Prina, A. M., & Brayne, C. (2015). The association between community environment and cognitive function: a systematic review. Social Psychiatry and Psychiatric Epidemiology, 50(3), 351–362. https://doi.org/https://doi.org/10.1007/s00127-014-0945-6
- Wu, Y. T., Prina, A. M., Jones, A., Barnes, L. E., Matthews, F. E., Brayne, C., & CFAS, M. R. C. (2016). Land use mix and five-year mortality in later life: Results from the cognitive function and ageing study. Health and Place, 38, 54–60. https://doi.org/https://doi.org/10.1016/j.healthplace.2015.12.002