
ABSTRACT
Using the UK as an example, students attending higher education providers (HEPs) increasingly suffer mental ill-health due to new stress factors. Relationships between stress, frequently co-occurring chronic medically unexplained symptoms (MUS) and mental health are explored as the basis for proposing The BodyMind Approach® (TBMA) as an innovative intervention, addressing the body and mind experience of MUS. Excessive stress can lead to/exacerbate, mental health difficulties and/or MUS (such as fibromyalgia, chronic fatigue/pain for which tests and scans are normal). MUS mostly affects women, non-native speakers and young people, all high numbers at HEPs. Students resist mental health services, and half in need do not disclose or seek help. TBMA, as an evidence-based, research-informed intervention, tested in the health service, is more accessible when framed as learning to self-manage symptom distress. Policymakers might consider this intervention to help improve student mental health as part of an institution-wide approach.
Introduction
This article proposes that The BodyMind Approach® (TBMA) (Payne, Citation2009) can be employed as an innovative psychoeducational intervention targeting the many students in universities with medically unexplained symptoms (MUS) (such as chronic pain/fatigue, fibromyalgia, headache or backache for which tests/scans return normal), often with co-occurring anxiety/depression. It provides a rationale for TBMA by exploring benefits in the context of the relationships between student stress, MUS and the substantial increase in mental ill-health in higher education provider (HEP) settings. By contributing to the discussion on how to enhance student help-seeking behaviour for chronic stress/mental health difficulties, TBMA has the potential to advance knowledge and facilitate theory development in mental health within HEPs. Although not reporting the research here, TBMA has shown encouraging outcomes in the UK National Health Service (Payne & Brooks, Citation2017, Citation2018, Citation2020).
TBMA emphasises the cultivation of good mental health and sustained resilience through participants learning to self-manage stress, associated with MUS, by integrating body with mind. Previous studies on body-oriented approaches for MUS (Papadopoulos et al., Citation2017; Röhricht et al., Citation2019) showed positive results. Students may be more able to live well with their bodily distress by learning to self-manage rather than experiencing consequences such as reduced emotional resilience, and/or mental health conditions due to overwhelming stress. TBMA could contribute to overall mental health and wellbeing by, for example, increasing early help-seeking behaviour and academic outcomes, and reducing referrals to oversubscribed counselling services and/or withdrawals from studies. It is hoped this discourse will help inform organisational practices and educational policies aimed at supporting student mental health and wellbeing.
The BodyMind Approach®
Current HEPs’ interventions address solely the psychological elements of MUS. This, despite almost half of students feeling unable to access such services due to stigma, defensive verbal communication to avoid emotion, their explanatory model being solely physical, or if non-native speakers, for example. Medication/pain management treat these bodily symptoms but neglect the associated stress/anxiety/depression. No current intervention caters for both the emotional and bodily distress, attracts less stigma, reduces avoidance behaviour and employs nonverbal, embodied methods rather than verbal language alone. Since many students do not disclose/seek help for chronic stress/mental health difficulties, a psychoeducational intervention targeting students with MUS may be more acceptable, reducing fear of judgement thus increasing numbers benefiting from support.
TBMA is designed for students not coping with their MUS to learn to self-manage both symptoms, and the emotional counterpart, to improve and sustain good mental health. The conceptual framework proposed highlights how an innovative, holistic TBMA learning and teaching programme, addressing the inter-relationship of body with mind, might contribute to an integrated, whole-university approach towards student mental health.
Derived from the arts therapies, TBMA is research-informed, employing findings from adult and experiential learning, mindfulness, groupwork, emotional regulation, neuroscience, embodied social cognition, attachment, self-management and MUS (Payne et al., Citation2019, Citation2019) ().
Figure 1. TBMA model.
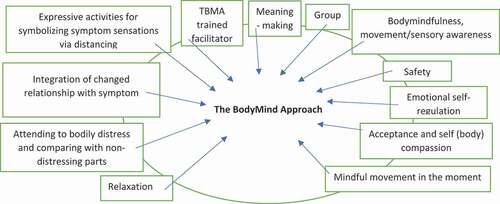
TBMA groups comprise 12 two-hourly sessions over 10 weeks. Pre and post monitoring, and formulation of a tailor-made action plan for embedment over the subsequent 6 months are included. From piloting TBMA training online delivery of TBMA online for students is possible.
TBMA employs embodied, enactive practices such as bodymindfulness, movement, writing, mark-making or collage to help make meaning from sensory experiencing in the body. By exploring symptoms, and associated emotions, and practicing tracking these, ‘signals’, sent by the body about emotions, the relationship with symptoms can change. For example, learning to notice subtle tightening or retreating in the body is a response to a possible threatening situation (Craig, Citation2002; Dael et al., Citation2012). Becoming conscious of, and receptive to, this interoceptive response can lead to feelings of control, agency and emotional resilience. TBMA promotes kind attention to bodily sensations, monitoring signals from interoceptive awareness, with an exploratory interest, rather than emotional reactivity and negative appraisal. Attention towards interaction between sensation, emotions, images and thoughts, supports body with mind connectivity. Movement is an innate mechanism for auto/self-regulation (Shafir, Citation2015). An increased awareness of movement can support emotional regulation towards internal/external stimuli, giving more choice and skills to adapt, so needs are met.
TBMA appears acceptable and more accessible to people experiencing MUS than psychological therapy (Payne & Brooks, Citation2020). Research (N = 90) shows TBMA can sustain engagement (97%); reliably reduce symptom distress (63%), anxiety (42%), and depression (35%); and increase overall activity (58%), wellbeing (55%), and functioning (35%) (Payne, Citation2014; Payne & Stott, Citation2010), sustained over 6 months (Payne & Brooks, Citation2017). Approaches that integrate practices to promote multiple dimensions of students’ wellbeing, such as the bidirectionality of body with mind, are limited (Moses et al., Citation2016). Stress reduction, counselling or mindfulness focus on reducing anxiety/depression (Church et al., Citation2012; Deckro et al., Citation2002; Regehr et al., Citation2013), ignore chronic symptoms and are usually conducted individually, whereas group support focussing on both symptom- and emotional-distress, found in TBMA, helps reverse isolation. Interventions targeting pain, self-help/social support, wellbeing, academic performance, resilience, persistence and retention, ignore psychological aspects (Mattanah et al., Citation2012; Robbins et al., Citation2009). TBMA addresses both physical and emotional health simultaneously by firstly working with the bodily distress, subsequently, leading to self-management of the symptom (dis)stress-response.
TBMA, endorsed as a class for learning to manage symptoms, might be more appealing to students than counselling/psychological approaches. TBMA, promoted as supporting sustained wellbeing in body and mind, helping the learning process, improving grades, preventing excessive stress, may increase help-seeking behaviour. Classes might prevent any associated mental health difficulties from escalating, or even occurring since MUS can be a precursor.
The advantages of TBMA include reducing a) the possibility of new conditions, b) exacerbation of existing concerns, c) isolation d) anxiety/depression, and increasing a) activity, b) wellbeing, and c) feelings of control when living with uncertainty. Wordage is insufficient to describe TBMA, but details are available (Payne et al., Citation2019).
Stress and its relationship to student mental health
Whilst stress is part of life people respond, and experience it, differently. Any threat towards something cared about, such as employment, results in stress. Threats are due to demands exceeding the capacity to cope. The initial stress reaction is helpful – alerting us to what matters, find our comfort-zone or change our lives to cope. When stressors are excessive, multiple, and sustained, they can reduce mental health and cause bodily symptoms (Clarke, Citation2016). Vulnerability to excessive stress can result in poor emotional self-regulation, reduced resilience to manage, and/or MUS/mental health difficulties.
A history of trauma can lead to a pre-disposition for stress overflowing. When potential threats are perceived, such as students feeling out of control due to academic demands, transition, uncertainty or isolation, the stress response kicks-in. When that threat feels bigger than the capacity to cope, the stress response gets stuck in the body. The unconscious body-brain wants to avoid that situation repeating, so, if a similar situation/or felt-experience to past trauma is involved the reptilian brain responds in that same way.
Targeting vulnerable student groups may help to prevent high-stress levels to avoid mental ill-health (Universities UK, Citation2019) and/or MUS (Kroenke & Price, Citation1993). TBMA, by supporting students to learn to manage stress through managing their MUS (via self/body compassion), and emotional regulation may improve students’ resilience and ability to cope with threats (De la Fuente et al., Citation2008). Some new factors involved in these higher student stress levels leading to increased mental health concerns, and/or MUS, are presented as a context and rationale for delivering TBMA in HEPs.
New factors affecting student stress levels
Students have always experienced stress, but in the UK nowadays there is more due to new, complex, and multi-faceted factors, leading to, or exacerbating, mental health conditions, or impacting students vulnerable to stress.
The rise in the percentage of children and young people with mental health difficulties in England, together with the widening participation government policy for HEPs, has resulted in more students entering with a diagnosis, or with fragile mental health. Consequently, any increase in stressors may have a knock-on effect on already delicate mental health.
The government’s policy of 50% of all young people entering HEPs led to growing numbers from disadvantaged backgrounds. This policy is measured by the Higher Education Statistics Authority/HESA (Higher Education Statistics Agency, Citation2018) using indicators of: a) low neighbourhood HEP participation, b) parents not having attended HEPs, and, c) increased enrolment from state schools/colleges. Poor mental health in disadvantaged populations (social, economic, cultural or political) is higher (Meyer et al., Citation2008), and associated with substantially greater risks of common mental health conditions (House of Commons Education Committee and Health and Social Care Committee, Citation2018), and MUS (Kroenke & Price, Citation1993). These students experience more stressors, such as likely feeling more isolated, increased pressure to succeed, less support, and poorer financial security (Williams et al., Citation2015), exposing them to stress overflowing resulting in mental ill-health and/or MUS. Indeed, reports from this policy anticipated increased mental health difficulties (Department for Business Innovation & Skills, Citation2013).
Early research suggests change and transition are stressful (Hobfoll & Walfisch, Citation1986). Students have always had to adjust to substantial change transitioning to unfamiliar HEPs when growing from adolescence to adulthood, dependence to independence, acclimatising to changes in lifestyle and increased study demands. Since greater numbers now are fragile to mental health difficulties, change/transitions can be more problematic. Leaving supportive family, friends, school, usually going to a strange city with unknown people, can tip the balance for students who previously managed. When transitioning to HEPs, returning from vacation or going on placement, stress will be experienced positively or negatively depending on mental health history.
Economic factors can be a stressor, for example, where a full-time student is having to work due lack of parental financial contribution to the maintenance loan. The rise in tuition fees (covered by a student loan viewed as debt) results in partial increases in undergraduates’ mental health difficulties (Richardson et al., Citation2015), and debt links to poorer psychological functioning and students considering withdrawing (Cooke et al., Citation2004; Walsemann et al., Citation2015).
The competitive employment market pressurises students to gain the highest degree level. An increase of only 10% of graduate jobs occurred since 2001, and, in the third quarter of 2017 49% of all recent graduates worked in non-graduate roles (Office of National Statistics, Citation2017). This shortfall will likely increase substantially in forthcoming years.
Any combination of these factors can be additional stressors contributing to increased student mental ill-health, especially hard to cope with if feeling unsupported, already fragile to excessive stress, and with a diagnosed/undiagnosed mental health concern and/or MUS. TBMA, in supporting students to self-manage MUS, may not only decrease excessive stress, but sustain robust, emotional health and wellbeing and increase connection with the collective.
Student stress and medically unexplained symptoms
Just as MUS can lead to, and is associated with, excessive stress (Mobini, Citation2015), high-stress levels can result in MUS, and mental, and/or physical illnesses (Schneiderman et al., Citation2005). In a University College London (UCL) Union survey students complained of anxiety, depression, physical pain and insomnia, in that order (University College London Union, Citation2019). If students complain of the physical symptoms of excessive stress almost as much as the emotional ones, then TBMA can effectively support both. Physical symptoms (for example, pain, insomnia, eye twitching, fatigue) alert us to the effects of a threat/pressure i.e. a stress response in the body. TBMA can educate students to notice and understand these signals to learn how to self-manage stress, hopefully before symptoms (another stress) overflow to trigger mental health difficulties and/or develop into chronic MUS.
One in six GP consultations are for MUS (Rosendal et al., Citation2015; Steinbrecher et al., Citation2011). MUS mostly affects women, young people (Nimnuan et al., Citation2001; Reid et al., Citation2002; Steinbrecher et al., Citation2011) and non-native speakers (Verhaak et al., Citation2006), all of which number highly in the student population. There is a high prevalence of MUS in students, often with co-occurring anxiety, depression, and chronic stress (Henningsen et al., Citation2003). Consequently, MUS it is an important area of concern related to improving student mental health/wellbeing.
MUS treatment is normally via mental health services but for only the most severe presentations of IBS with anxiety/depression (Laird et al., Citation2016), except for graded exercise for chronic fatigue (Cochrane Database of Systematic Reviews, Citation2008). Most MUS sufferers find mental health routes unacceptable due to their explanatory model as physical, rather than psychological (Heijmans et al., Citation2011). TBMA focusses on the stress-experience of the symptoms firstly, it is attractive, fitting with this mindset.
When adaptive stress responses kick-in, previous unresolved threats to survival, safety or wellbeing are stimulated, and unwanted stress pours into the ‘stress bucket’. The result can be a chronic stress state, often manifesting as MUS, causing even more stress (as the threat is in the body) in a downward spiral if interruption to the iterative cycle is unforthcoming (Mobini, Citation2015). TBMA is designed to interfere with this cycle, realigning body with mind for healthier functioning, and overall wellbeing. Symptom distress can be the tipping point for future deterioration and complex mental health conditions if not addressed early (Chew-Graham et al., Citation2017). Yet, so far, there is no early pathway for learning self-management of MUS in HEPs. TBMA can fill this gap. In the context of student mental health, an understanding of the ramifications of excessive stress in student life is important when considering how to address this critical issue. Excessive stress, MUS and mental health are inextricably related. To stem the substantial rise in student mental health concerns, undue stress, and associated MUS, HEPs need appropriate interventions.
Student mental health
Student mental health difficulties have grown immensely, mirroring the rise in the diagnosis of children and young people (NHS Digital, Citation2018). From 2,169 applicants, and 6,504 current students, 12% reported mental health difficulties, 32% ‘often/always’ felt down/depressed in the previous 4 weeks, and 30% ‘often/always’ felt isolated/lonely (Unite, Citation2016). Over the last ten years the number of student suicides rose (Office of National Statistics, Citation2018), and attrition rates grew due to mental ill-health (Marsh, Citation2017). One in four students reported mental health problems (YouGov, Citation2016), and nearly five times as many as 10 years ago disclosed a mental health condition (Thorley, Citation2017).
Mental health difficulties peak between 16 and 24 years, overlapping the median age of students. Kessler et al. (Citation2005) found 64% of students (and 83% of undergraduates) are between 16 and 24 years, as today, with 75% of mental health problems established by age 25. The increased numbers in this age range results in more mental health difficulties, driven by women who are almost three times more likely to experience mental ill-health than men. The proportion of 16–24-year-old women students with mental health difficulties increased by 38% from 1993 to 2014, whereas it decreased by 3% for 16–24-year-old men (NHS Digital, Citation2014). Since 2015, more women than men have consistently entered UK universities (Higher Education Statistics Agency (Higher Education Statistics Agency, Citation2018). Consequently, with widening participation, more women than men are entering HEPs with a diagnosed/undiagnosed mental health condition. Mostly women participated in TBMA health-service deliveries so TBMA could contribute to improving the mental health/MUS conditions of women students.
The increase in student mental ill-health is not solely in the UK. In the USA, Soet and Sevig (Citation2006) explored the history, coping and mental health distress levels in one university, and provided recommendations for research, policy and practice. Kitzrow (Citation2009) acknowledged the needs and challenges posed by the increase in students with serious psychological problems seeking counselling onsite. Iarovici (Citation2014) raised concerns that student mental health was becoming a crisis for HEPs.
The UK media highlighted the increase in undergraduate mental health difficulties (Marsh, Citation2017), although students always had mental health difficulties. As far back as Roberts et al. (Citation1999) student mental health in two London universities was substantially lower than in the general population, supported later by Stallman (Citation2010). Cooke et al. (Citation2006) found mental health levels never returned to those of pre-enrolment in 4,699 students. Webb et al. (Citation1996) reported student anxiety at 54%, and depression at 13%; and Bewick et al. (Citation2008) also found anxiety higher than depression for 1,129 students. Andrews and Wilding (Citation2004) surveyed 351 students one month before starting university and at mid-course. Nine percent of those with no symptoms before university had depression, and 20% had clinically significant anxiety by mid-course. In a year, a quarter of students reported psychological distress associated with increased risk of anxiety, depression, substance abuse and personality disorders (Verger et al., Citation2009). Anxiety, associated with excessive stress, appears to be a major concern for students.
Only 27% of students thought their university provided adequate mental health support (NatWest, Citation2020). The Equality Challenge Unit (Citation2014) found half experiencing mental health difficulties had not received support, and that almost half with difficulties were unwilling to disclose/seek treatment fearing other students thinking less of them or of receiving unfair treatment from their institution. The biggest challenges for students with mental health difficulties seeking help were fearing judgements and being shown as weak (Byrom, Citation2014). TBMA circumnavigates these barriers since it engages students based on their MUS, rather than their mental health/stress presentation. There is safety in self-referring to an intervention for overtly presenting physical symptoms, rather than for mental health, and when perceived as a class for learning, rather than as psychological therapy for mental health concerns. The fears evaporate, so participants can sustain involvement over 12 sessions.
Conclusion
Mental health difficulties will continue to increase for students (NHS Digital, Citation2018). Higher education policies and wellbeing services have a long way to go in their legal duty of care to avoid harm, support, and co-produce strategies to support mental health. There is an opportunity now to consider joined up approaches to transform cultures and embed initiatives beyond wellbeing services, to improve help-seeking, decrease isolation, and promote a shared purpose for good mental health. Leaving students to struggle may result in more mental health difficulties, increased distress for those already diagnosed, and the onset of more chronic, debilitating MUS.
Stones and Glazzard (Citation2019) recommend an institution-wide approach to eradicate stigma, enabling students to be mentally healthy, and extending beyond provisions targeting solely mental ill-health. TBMA fits into this extended provision. There are overlaps between the body, mind and aspects of wellbeing (Checkoway, Citation2011) and these overlaps could be captured by TBMA at times of increased stress such as induction, before/after transitions, placements, examinations and deadlines. TBMA may support help-seeking, reduce stigma and attend to students’ physical (and emotional) distress as part of an overall mental health and wellbeing strategy based in student services/faculties/schools. It will be crucial to research TBMA as context; referral system and population all differ from those in the health service.
There are unique opportunities now with the UK University Mental Health Charter (Hughes & Spanner, Citation2019) to review the way student mental health is regarded, and which evidence-based interventions are accessible and acceptable to all students, not only those able to engage with student wellbeing services.
Disclosure statement
The author confirms there is no conflict of interest.
Additional information
Notes on contributors
Helen Payne
Professor Helen Payne, PhD., holds a Chair in Psychotherapy at the University of Hertfordshire. She conducts research, examines and supervises doctoral candidates globally. Her background is in embodied learning and is founding editor-in-chief for the international journal ‘Body, Movement and Dance in Psychotherapy’ www.tandfonline.com/toc/tbmd20/current. She developed TBMA to support people in the NHS with persistent bodily symptoms for which tests and scans return as normal, and in which she trains facilitators. Publications include: ‘A qualitative study of the views of patients with medically unexplained symptoms on The BodyMind Approach®: Employing embodied methods and arts practices for self-management’ (Open Access). http://journal.frontiersin.org/article/10.3389/fpsyg.2020.554566/full?&utm_source=Email_to_authors_&utm_medium=Email&utm_content=T1_11.5e1_author&utm_campaign=Email_publication&field=&journalName=Frontiers_in_Psychology&id=554566
References
- Andrews, B., & Wilding, J. M. (2004). The relation of depression and anxiety to life-stress and achievement in students. British Journal of Psychology, 95(Pt4), 509–521. https://doi.org/10.1348/0007126042369802
- Bewick, B. M., Gill, J., & Mulhern, B. (2008). Using electronic surveying to assess psychological distress within the UK university student population: A multi-site pilot investigation. E-Journal of Applied Psychology, 4(2), 1–5. https://doi.org/10.7790/ejap.v4i2.120
- Byrom, N. (2014). Grand challenges in student mental health report. Student Minds. http://www.studentminds.org.uk/uploads/3/7/8/4/3784584/grand_challenges_report_for_public.pdf
- Checkoway, B. (2011). New perspectives on civic engagement and psychosocial well-being. Liberal Education, 97(2), 6–11.
- Chew-Graham, C. A., Heyland, S., Kingstone, T., Shepherd, T., Buszewicz, M., Burroughs, H., & Sumathipala, A. (2017). Medically unexplained symptoms: Continuing challenges for primary care. British Journal of General Practice, 67(656), 106–107. https://doi.org/10.3399/bjgp17X689473
- Church, D., De Asis, M. A., & Brooks, A. J. (2012). Brief group intervention using emotional freedom techniques for depression in college students: A randomized controlled trial. Depression Research and Treatment, 2012, 1–7. Article ID 257172 https://www.hindawi.com/journals/drt/2012/257172/
- Clarke, D. D. (2016, September 1). Solving medical mysteries: Hidden stresses and unexplained symptoms. Slovenian Journal of Public Health, 55(3), 152–154. https://doi.org/10.1515/sjph-2016-0029
- Cochrane Database of Systematic Reviews. (2008). Cognitive behaviour therapy for chronic fatigue syndrome. First published: July 16, 2008 by Cochrane Publications.
- Cooke, R., Barkham, B. M., Audin, K., Bradley, M., & Davy, J. (2004). Student debt and its relation to student mental health. Journal of Further and Higher Education, 28(1), 53–66. https://doi.org/10.1080/0309877032000161814
- Cooke, R., Bewick, B. M., Barkham, M., Bradley, M., & Audin, K. (2006). Measuring, monitoring and managing the psychological well-being of first year university students. British Journal of Guidance & Counselling, 34(4), 505–517. https://doi.org/10.1080/03069880600942624
- Craig, A. D. (2002). How do you feel? Interoception: The sense of the physiological condition of the body. Nature Reviews Neuroscience, 3(8), 655–666. https://doi.org/10.1038/nrn894
- Dael, N., Mortillaro, M., & Scherer, K. R. (2012). Emotion expression in body action and posture. Emotion, 12(5), 1085–1101. https://doi.org/10.1037/a0025737
- De la Fuente, J., Fernández-Cabezas, M., & Mattila, P. (2008). Evaluations of an organisational stress management program in a municipal public works’ organisations. Journal of Occupational Health Psychology, 13(1), 10–23. https://doi.org/10.1037/1076-8998.13.1.10
- Deckro, G. R., Ballinger, K. M., Hoyt, M., Wilcher, M., Dusek, J., Myers, P., Greenberg, B., Rosenthal, D. S., & Benson, H. (2002). The evaluation of a mind/body intervention to reduce psychological distress and perceived stress in college students. Journal of American College Health, 50(6), 281–287. https://doi.org/10.1080/07448480209603446
- Department for Business Innovation & Skills. (2013). Widening participation in higher education. https://www.gov.uk/government/collections/widening-participation-in-higher-education
- Equality Challenge Unit. (2014). Understanding adjustments: Supporting staff and students who are experiencing mental health difficulties. https://www.ecu.ac.uk/publications/understanding-adjustments-mental-health/
- Heijmans, M., Olde Hartman, T. C., van Weel, C., Dowrick, C., Lucassen, P. L. B. J., & van Weel, C. (2011). Experts’ opinions on the management of medically unexplained symptoms in primary care. A qualitative analysis of narrative reviews and scientific editorials. Family Practice, 28(4), 444–455. https://doi.org/10.1093/fampra/cmr004
- Henningsen, P., Zimmermann, T., & Sattel, H. (2003). Medically unexplained physical symptoms, anxiety, and depression: A meta-analytic review. Psychosomatic Medicine, 65(4), 528–533. https://doi.org/10.1097/01.PSY.0000075977.90337.E7
- Higher Education Statistics Agency. (2018). Table 15 - UK domiciled student enrolments by disability and sex 2016/17. https://www.hesa.ac.uk/data-and-analysis/students/table-15
- Hobfoll, S. E., & Walfisch, S. (1986). Stressful event, mastery and depression: A review of crisis theory. Journal of Community Psychology, 14(2), 183–195. https://doi.org/10.1002/1520-6629(198604)14:2<183::AID-JCOP2290140209>3.0.CO;2-Q
- House of Commons Education Committee and Health and Social Care Committee. (2018). The government’s green paper on mental health: Failing a generation.Publications Parliament, UK. https://publications.parliament.uk/pa/cm201719/cmselect/cmhealth/642/64207.html
- Hughes, G., & Spanner, L. (2019). The University mental health charter. Student Minds.
- Iarovici, D. (2014). Mental health issues and the university student. Johns Hopkins University Press.
- Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
- Kitzrow, M. A. (2009). The mental health needs of today’s college students: Challenges and recommendations. NASP, 46(4), 646–660. https://doi.org/10.2202/1949-6605.5037
- Kroenke, K., & Price, P. K. (1993). Symptoms in the community. Archives of International Medicine, 153(21), 2474–2480. http://dx.doi.org/10.1001/archinte.1993.00410210102011
- Laird, K. T., Tanner-Smith, E. E., Russell, A. C., Hollon, S. D., & Walker, L. S. (2016). Short-term and long-term efficacy of psychological therapies for irritable bowel syndrome: A systematic review and meta-analysis. Clinical Gastroenterology and Hepatology, 14(7), 937–947. https://doi.org/10.1016/j.cgh.2015.11.020
- Marsh, S. (2017). Number of university dropouts due to mental health problems trebles. The Guardian Newspaper. https://www.theguardian.com/society/2017/may/23/number-university-dropouts-due-to-mental-health-problems-trebles#img-1
- Mattanah, J. F., Brooks, L. J., Brand, B. L., Quimby, J. L., & Ayers, J. F. (2012). A social support intervention and academic achievement in college: Does perceived loneliness mediate the relationship? Journal of College Counseling, 15(1), 22–36. https://doi.org/10.1002/jocc.2012.15.issue-1
- Meyer, I. H., Schwartz, S., & Frost, D. M. (2008). Social patterning of stress and coping: Does disadvantaged social status confer more stress and fewer coping resources? Social Science & Medicine, 67(3), 368–379. https://doi.org/10.1016/j.socscimed.2008.03.012
- Mobini, S. (2015). Psychology of medically unexplained symptoms: A practical review. Cogent Psychology, 2(1), 1033876. https://doi.org/10.1080/23311908.2015.1033876
- Moses, J., Bradley, G. L., & O’Callaghan, F. V. (2016). When college students look after themselves: Self-care practices and well-being. Student Affairs Research and Practice, 53(3), 345–359. https://doi.org/10.1080/19496591.2016.1157488
- NatWest. (2020). NatWest student living index 2020. NatWest Bank. https://personal.natwest.com/personal/life-moments/students-and-graduates/student-living-index.html
- NHS Digital. (2014). Adult psychiatric morbidity survey. https://files.digital.nhs.uk/pdf/q/3/mental_health_and_wellbeing_in_england_full_report.pdf
- NHS Digital. (2018). Mental health of children and young people in England, 2017 [PAS]. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2017/2017
- Nimnuan, C., Hotopf, M., & Wessely, S. (2001). Medically unexplained symptoms. An epidemiological study in seven specialities. Journal of Psychosomatic Research, 51(1), 361–367. https://doi.org/10.1016/s0022-3999(01)00223-9
- Office of National Statistics. (2017). Graduates in the UK labour market. https://www.gov.uk/government/statistics/graduates-in-the-uk-labour-market-2017
- Office of National Statistics. (2018). Estimating suicide among higher education students, England and Wales. https://www.ons.gov.uk/releases/estimatingsuicideamonghighereducationstudentsenglandandwales
- Papadopoulos, N., Burrell, C., Smith, L., & Röhricht, F. (2017). Therapeutic processes and personalised care in body-oriented psychological therapy for patients with medically unexplained symptoms (MUS). European Journal for Person Centered Healthcare, 5(4), 449–453. https://doi.org/10.5750/ejpch.v5i4.1356
- Payne, H. (2009). Pilot study to evaluate dance movement psychotherapy (the BodyMind Approach) with patients with medically unexplained symptoms: Participant and facilitator perceptions and a summary discussion. Body, Movement & Dance in Psychotherapy, 5(2), 95–106. doi: 10.1080/174329709029/8008
- Payne, H. (2014). Patient experience: Push past symptom mysteries. The Health Service Journal, 124(6390), 26–27.
- Payne, H., & Brooks, S. (2017). Moving on: The bodymind approach™ for medically unexplained symptoms (outcomes). Public Mental Health, 16, 2, 63–71. https://doi.org/10.1108/JPMH-10-2016-0052
- Payne, H., & Brooks, S. (2018). Different strokes for different folks: The bodymind approach as a learning tool for patients with medically unexplained symptoms to self-manage. Frontiers in Psychology, 9, 2222. https://doi.org/10.3389/fpsyg.2018.02222
- Payne, H., & Brooks, S. (2020). A qualitative study of the views of patients with medically unexplained symptoms on the bodymind Approach®: Employing embodied methods and arts practices for self-management. Frontiers in Psychology, 11, 3223. https://doi.org/10.3389/fpsyg.2020.554566
- Payne, H., Roberts, A., & Roberts, A. (2019). The bodymind Approach® as transformative learning to promote self-management for patients with medically unexplained symptoms. Journal of Transformative Education, 18(2), 114–147. https://doi.org/10.1177/1541344619883892
- Payne, H., & Stott, D. (2010). Change in the moving bodymind: Quantitative results from a pilot study on the bodymind approach (BMA) as groupwork for patients with medically unexplained symptoms (MUS). Counselling and Psychotherapy Research, 10(4), 295–307. https://doi.org/10.1080/14733140903551645
- Regehr, C., Glancy, D., & Pitts, A. (2013). Interventions to reduce stress in university students: A review and meta-analysis. Journal of Affective Disorders, 148(1), 1–11. https://doi.org/10.1016/j.jad.2012.11.026
- Reid, S., Wessely, S., Crayford, T., & Hotopf, M. (2002). Frequent attenders with medically unexplained symptoms: Service use and costs in secondary care. British Journal of Psychiatry, 180(3), 248–253. https://doi.org/10.1192/bjp.180.3.248
- Richardson, T., Elliott, P., & Roberts, R. (2015). The impact of tuition fees’ amount on mental health over time in British students. Journal of Public Health, 37(3), 412–418. https://doi.org/10.1093/pubmed/fdv003
- Robbins, S. B., Oh, I., Le, H., & Button, C. (2009). Intervention effects on college performance and retention as mediated by motivational, emotional, and social control factors: Integrated meta-analytic path analyses. Applied Psychology, 94(5), 1163–1184. https://doi.org/10.1037/a0015738
- Roberts, R., Golding, J., Towell, T., & Weinreb, I. (1999). The effects of economic circumstances on British students’ mental health. Journal of American College Health, 48(3), 103–109. https://doi.org/10.1080/07448489909595681
- Röhricht, F., Sattel, H., Kuhn, C., & Lahmann, C. (2019). Group body psychotherapy for the treatment of somatoform disorder: A partly randomised controlled feasibility pilot study. BMC Psychiatry, 19(1), 120. https://doi.org/10.1186/s12888-019-2095-6
- Rosendal, M., Carlsen, A. H., Rask, M. T., & Moth, G. (2015). Symptoms as the main problem in primary care: A cross-sectional study of frequency and characteristics. Scandinavian Journal of Primary Health Care, 33(2), 91–99. https://doi.org/10.3109/02813432.2015.1030166
- Schneiderman, N., Ironson, G., & Siegel, S. D. (2005). Stress and health: Psychological, behavioural, and biological determinants. Annual Review of Clinical Psychology, 1(1), 607–628. https://doi.org/10.1146/annurev.clinpsy.1.102803.144141
- Shafir, T. (2015). Movement based strategies for emotion regulation. In M. L. Bryant (Ed.), Handbook on emotion regulation: Processes, cognitive effects and social consequences (pp. 231–249). Nova Science Publishers.
- Soet, J., & Sevig, T. (2006). Mental health issues facing a diverse sample of college students: Results from the college student mental health survey. NASPA, 43(3), 410–431. https://doi.org/10.2202/1949-6605.1676
- Stallman, H. M. (2010). Psychological distress in university students: A comparison with general population data. Australian Psychologist, 45(4), 249–257. https://doi.org/10.1080/00050067.2010.482109
- Steinbrecher, N., Koerber, S., Frieser, D., & Hiller, W. (2011). The prevalence of medically explained symptoms in primary care. Psychosomatics, 52(3), 263–271. https://doi.org/10.1016/j.psym.2011.01.007
- Stones, S., & Glazzard, J. (2019). Supporting student mental health in higher education. Critical Publishing.
- Thorley, C. (2017). Not by degrees: Improving student health in the UK’s universities. Institute for Public Policy Research. www.ippr.org/publications/not-by-degrees
- Unite. (2016). Student resilience: Unite students insight report. Retrieved 14 Jan, 2021, from https://www.unite-group.co.uk/sites/default/files/2017-03/student-insight-report-2016.pdf
- Universities UK (2019) Step change. https://universitiesuk.ac.uk/policy-and-analysis/stepchange/Pages/framework.aspx
- University College London Union. (2019). Heads up: Reporting on mental health. https://studentsunionucl.org/sites/uclu.org/files/u198046/documents/heads_up_-_reporting_on_mental_health_online_final.pdf
- Verger, P., Combes, J. B., & Perettti-Wattel, P. (2009). Psychological distress in first year university students: Socioeconomic, academic stressors, mastery and social support in young men and women. Social Psychiatry and Psychiatric Epidemiology, 44(8), 643–650. https://doi.org/10.1007/s00127-008-0486-y
- Verhaak, P. F., Meijer, S. A., Visser, A. P., & Wolters, G. (2006). Persistent presentation of medically unexplained symptoms in general practice. Family Practice, 23 (4), 14–20. Epub 2006 Apr 21. PMID: 16632487. https://doi.org/10.1093/fampra/cml016
- Walsemann, K. M., Gee, G. C., & Gentile, D. (2015). Sick of our loans: Student borrowing and the mental health of young adults in the United States. Social Science & Medicine, 124, 85–93. https://doi.org/10.1016/j.socscimed.2014.11.027
- Webb, E., Ashton, C. H., Kelly, P., & Kamali, F. (1996). Alcohol and drug use in UK university students. Lancet, 348(9032), 922–925. https://doi.org/10.1016/S0140-6736(96)03410-1
- Williams, M., Coare, P., & Anderson, J. (2015). Higher Education Funding Council for England (HEFCE). https://www.employment-studies.co.uk/resource/understanding-provision-students-mental-health-problems-and-intensive-support-needs
- YouGov. (2016). One in four students suffer from mental health problems. YouGov, UK. https://yougov.co.uk/news/2016/08/09/quarter-britains-students-are-afflicted-mentalhea/

