
ABSTRACT
This qualitative study explored the experiences and perspectives of 16 clergy members from African Initiated Churches in Australia. Through Interpretative Phenomenological Analysis, data from semi-structured interviews was analyzed and found that mental health problems in the Zimbabwean-Australian community were attributed to both spiritual and psychological factors. Clergy play a crucial role as gatekeepers, often the initial point of contact for individuals experiencing mental distress. The study emphasizes the significance of spirituality and the critical role of clergy members in supporting individuals with mental health issues and connecting them to appropriate mental health services. Greater collaboration between clergy members and social work services is needed, and this research contributes to the mental health field and enhances social work understanding of the clergy’s role in addressing mental health issues in African communities.
Introduction
This qualitative study explored the experiences and perspectives of 16 clergy members from African Initiated Churches in Australia (AICs). This study examines the cultural connection of spirituality when addressing mental health issues in Indigenous communities (Calma et al., Citation2017; Dudgeon, Citation2017; Dudgeon & Walker, Citation2015). It demonstrates the need to reconcile the biomedical model with Indigenous perspectives as a way to protect diverse ways of understanding mental health, including spiritual and environmental understandings (Dudgeon, Citation2017; Watts & Hodgson, Citation2022). This study contributes to the broader field of mental health research by providing insights into the specific challenges encountered by Zimbabwean Australians, and the implications for mental health social work.
Zimbabwe is in Southern Africa, with borders shared by South Africa, Botswana, Zambia, and Mozambique. The country has a population of approximately 15.178979 million people (Zimbabwe National Statistical Agency, Citation2022). Despite its population size, Zimbabwe has experienced significant migration (of its citizens to the diaspora) since the turn of the century, coinciding with political and social upheaval. Zimbabwean migrants and their descendants, including both black and white Zimbabweans, have settled in various parts of the world, including Australia. As of 2021, Australian Census data show there were 39,714 Zimbabwean Australians, including individuals of both black and white ethnicities (Australian Bureau of Statistics, Citation2021). These Zimbabwean-Australians tend to seek Zimbabwean-Australian clergy for their mental health needs (Chaumba, Citation2016).
Migration from Zimbabwe to Australia by Zimbabweans is the result of a variety of interrelated motivations, including hopes for better educational and professional prospects as well as economic challenges and political unrest (Chaumba, Citation2016; Forrest et al., Citation2013). The migration process itself, however, introduces a myriad of challenges that extend beyond mere geographic relocation. Economic hardships and the pursuit of better prospects can contribute to a complex web of social and cultural dislocations, impacting the mental health and overall well-being of individuals in the diaspora. This challenges people to overcome their suffering and trauma with strength and resilience. In this context, pursuing well-being, mental health, and overall health is crucial. Overcoming these obstacles may provide serious problems for people who have suffered from mental distress. The clergy in Australia’s AICs may be of significant help in navigating the intricate processes of migration, economic hardship, and the challenges connected with integrating into a new cultural setting (Chaumba, Citation2016; Murambidzi, Citation2016). They may be of help in creating interventions that address the needs of the Australian-Zimbabwean community that necessitate knowledge of mental health and wellness with experiences of migration and diaspora.
The context of this study concerns Zimbabwean clergy’s understandings and responses to the mental health difficulties within their congregations. As discussed below, a mix of cultural and Christian knowledge intersects with Zimbabwean religious and spiritual beliefs and practices. During the colonial period, the spread of Christianity in Zimbabwe was closely linked to the political and economic interests of the European powers. Many Zimbabweans embraced Christianity to access education and other resources only available through the mission schools and hospitals established by the missionaries. According to Dudgeon (Citation2017) and Dudgeon and Walker (Citation2015), a similar pattern occurred in the context of the colonization, disempowerment, and resilience experienced by Indigenous Australians. Relatedly, non-Western cultures are required to address local issues in a way that respects the trauma and culture of Indigenous Australians (Calma et al., Citation2017; Dudgeon, Citation2017). Dudgeon (Citation2017) asserts that the colonization and disempowerment of Aboriginal Torres Strait Islanders inspired their resilience and tenacity to colonization. Human rights violations, discrimination, and environmental dilapidation are common for Zimbabweans who migrate to Australia (Chaumba, Citation2016; Forrest et al., Citation2013). Together with the difficulties faced by the transition to a new cultural setting, these difficulties may have a negative influence on migrants’ mental health (Chaumba, Citation2016; Dudgeon & Walker, Citation2015). Traumas encountered during the relocation process include losing identifiable cultural markers, upsetting social networks, and transitioning to a new healthcare system (Dudgeon & Walker, Citation2015; Krüger, Citation2020).
The social work role in mental health practice
Mental health social work occurs in contexts of cultural diversity, colonization, and in response to structural, interpersonal and intergenerational trauma. Each country has developed specific approaches to providing mental health services, depending on the cultural, social, and environmental histories of their respective societies. Bland et al. (Citation2021) suggest that one in six social workers in Australia identify as a mental health social worker and that social workers represent approximately 10% of the formal mental health workforce. The social work profession is one of five identified Allied Health professions that make up multidisciplinary teams in the mental health sector. As a result of sector reform nearly two decades ago, mental health curricula are part of the skills and knowledge for working in mental health services embedded in social work qualifying degrees (Australian Association of Social Workers, Citation2021).
Additionally, social workers contribute to mental health services both in, and beyond, hospitals, and in community treatment and recovery-oriented services (Bland et al., Citation2021) through the professions’ continuing emphasis on the social aspects of community life which contribute to good mental health and human flourishing. These social aspects include rights and social recognition, social justice, participation, family and social relationships, work and housing (Bland et al., Citation2021; Watts & Hodgson, Citation2022). Thus, social workers can play a role in connecting civil society organizations with the welfare and health sectors.
The social work engagement with religion and spirituality
Religious institutions and organizations are important to civil society in Australia. These institutions offer connections to the community, and many health and social welfare services and offer fellowship with others of similar faith. Faith-based organizations continue to comprise a large section of the delivery of social welfare in the Australian context (Howe & Howe, Citation2012). The origins of the social work profession in Australia and elsewhere are rooted in religious and spiritual foundations, with ties to charitable and philanthropic work led by religious institutions in the 15th and 16th centuries (Chenoweth & McAuliffe, Citation2017).
In Zimbabwe, social work maintains strong connections with religion. The School of Social Services, established in 1964, received support from the Jesuit Fathers of the Roman Catholic Church (Chogugudza, Citation2009). The United Methodist Church founded Africa University’s social work department. Ezekiel Guti University, affiliated with the ZAOGA Forward in Faith Church, offers a Bachelor of Arts Honours in Social Work. These examples highlight the enduring historical and ongoing relationship between social work and religion in Zimbabwe (Chogugudza, Citation2009). Understanding clergy responses to mental health problems will assist social workers who sit at the intersections of formal mental health and social welfare organizations and services in making connections to faith-based organizations.
Spirituality is thus a broad concept that encompasses various beliefs, practices, and experiences related to the human spirit or soul. In the context of social work, spirituality can be a valuable resource for individuals and communities facing challenges and seeking support (Dudgeon & Walker, Citation2015). However, there have also been criticisms of the integration of spirituality into social work practice. One criticism is that spirituality can be subjective and difficult to define, leading to potential inconsistencies in its application (Hodgson & Watts, Citation2017). Critics argue that the lack of a clear framework for incorporating spirituality into social work practice can result in varying interpretations and approaches among practitioners, which may impact the quality and effectiveness of services provided. Spirituality has also been at odds with evidence-based practice (Hodgson & Watts, Citation2017).
Furthermore, there have also been critiques on the lack of models and frameworks that guide spiritual interventions (Hodgson & Watts, Citation2017). For example, spirituality can be used as a form of cultural imposition, particularly when social workers’ personal beliefs or values influence their practice. There is widespread agreement that social workers should avoid imposing their spiritual views during social work practice (Crisp, Citation2010). Critics argue that social workers should be mindful of their own biases and avoid imposing their spiritual beliefs on clients, as this can undermine the principles of self-determination and respect for diversity.
In summary, a critical discussion of trauma and human rights in the context of mental health is essential for a comprehensive understanding of the complexities involved (Krüger, Citation2020). Clergy may be called upon to respond to the mental health needs of their congregants as it relates to trauma, human rights and racial issues (Dudgeon, Citation2017; Krüger, Citation2020). Trauma, both individual and collective, significantly influences mental health outcomes. Simultaneously, the consideration of human rights is crucial in ensuring that mental health interventions uphold principles of dignity, autonomy, and equality.
Mental health care, religion, and spirituality in Zimbabwe
In Zimbabwe, Christianity provided a sense of hope and belonging in a time of great social upheaval, as traditional Christianity is now the dominant religion in Zimbabwe, with over 85% of the population identifying as Christian (Zimbabwe National Statistics Agency, Citation2017). Most Zimbabwean Christians are members of Protestant denominations, with the largest being the Anglican, Methodist, and Presbyterian churches. There is also a significant Catholic population and a growing number of independent Pentecostal and charismatic churches. A significant population are members of the African Traditional Religion.
Early intervention and treatment of mental health problems (MHPs) are crucial, and clergy play a vital role in supporting individuals to seek appropriate help. MHPs pose a significant public health concern due to their impact on individuals, families, and societies (Vos et al., Citation2013). The term encompasses a range of issues, from complex familial and societal factors affecting mental health (Al Omari & Wynaden, Citation2014; Lawrence et al., Citation2015) to clinically diagnosed mental disorders and severe forms of mental distress, including suicidal ideation (AIHW, Citation2012; Vos et al., Citation2013).
Research by Shizha and Charema (Citation2012), Muchinako et al. (Citation2013) and Murambidzi (Citation2016) suggests that clergy serve as first responders to mental distress within their communities. They may also be the preferred source of assistance over mental health experts. Mandizadza and Chidarikire (Citation2016) argue that Zimbabweans experiencing mental health problems may seek social and emotional support from clergy before turning to professional health experts. Similar patterns were observed in the United States by Gatseva and Argirova (Citation2011), Hankerson et al. (Citation2013), and Griffith et al. (Citation2016) indicating that clergy are often approached for mental health-related issues, with congregants favoring church over mental health professionals. It is crucial to explore clergy beliefs, as they may align with those of their congregants, influencing long-term health trajectories and shaping the church’s response to individuals seeking assistance.
Zimbabwean conceptions of mental health
Most Zimbabweans understand mental health problems within their socio-cultural and holistic view (Mbiti, Citation1969), including their causes and etiology (Patel et al., Citation1995). Regardless of where they may be located globally, Zimbabweans living in the diaspora usually turn to clergy/pastors or traditional medical practitioners for their physical, emotional, political, and spiritual needs (Kajawu et al., Citation2016; Mangezi, Citation2020).
Zimbabweans believe in a Supreme Being known among the Shona people of Zimbabwe as Mwari (God) or Musiki (Creator) whilst among the Ndebele people, God is known as Umlimu (V. Mabvurira & Makhubele, Citation2018). There is a widespread belief among Zimbabweans that prayers are channeled to Mwari (God) through vadzimu (ancestral spirits) or amadhlozi in Ndebele, which are the family ancestors or spirits of dead relatives who care, protect and guide the living relatives who often invoke their intervention during times of crisis (V. Mabvurira, Citation2016). This view is supported in earlier studies by Bourdillon (Citation1987) and Taringa (Citation2006) who posit that vadzimu (ancestral spirits) are disembodied spirits of departed relatives who act as intermediaries between Mwari and the living watch over them and providing fortune and punishment accordingly.
Notably, despite the migration of many Zimbabweans to Australia, their cultural beliefs regarding the causes of MHPs have remained broadly consistent with those residing in Zimbabwe (Muchinako et al., Citation2013). In Zimbabwean society, mental health disorders, known as “chirwere chepfungwa,” are understood as conditions that impact the brain to the extent that the affected individual cannot function normally (Muchinako et al., Citation2013). This highlights the need to consider cultural perspectives in assessing, diagnosing, and treating mental health issues, especially for Zimbabwean migrants residing in Australia.
Generally, Zimbabweans are brought up to have cultural belief systems and faith in the supernatural which is different from the Western world (V. Mabvurira, Citation2016). Terms such as kupenga (mental disorders) and benzi (mad person) are used concerning mental disorders (V. Mabvurira, Citation2016). Studies indicate that many Zimbabweans believe that mental health problems are caused by social problems, drugs and alcohol, economic hardships, avenging spirits (ngozi), ancestral spirits (vadzimu), witchcraft (huroyi) and heredity (Mabvurira & Makhubele, Citation2018; Muchinako et al., Citation2013). According to witchcraft and avenging spirits are thought to be the leading causes of MHPs from an Afrocentric point of view. This view was confirmed in an earlier study by Bourdillon (Citation1987), in which he conducted an ethnographic inquiry of the Shona people with a particular reference to their religion. While people have settled in Australia, culture and cultural beliefs remain largely the same as those living in Zimbabwe, including the beliefs about the leading causes of MHPs. Early intervention and treatment of MHPs are essential, and clergy play a significant role in supporting people to seek appropriate help. Therefore, it is essential to explore the beliefs of Zimbabwean-Australian clergy as this may impact how they respond to congregants if they need assistance.
The belief systems of Zimbabwean-Australians are often underpinned by their cultural practices and by active participation in AICs, which are churches that independently began in Africa by Africans and without the influence of Western missionaries (Daneel, Citation1987; Ranger, Citation2007) they often looked up to as role models for their health choices and help-seeking behaviors (Heward-Mills et al., Citation2018; Murambidzi, Citation2016). According to Meyer-Weitz et al. (Citation1998) and (Verma et al., Citation2003), an individual’s belief system regarding the causes of health conditions informs their help-seeking behaviors.
The roles of the clergy in African-Initiated Churches in Australia
In general, the clergy members in these churches have a range of responsibilities, including 1). Providing spiritual guidance and counseling to congregants. 2). Conducting religious services and rituals, such as baptisms, weddings, and funerals. 3). Teaching and preaching the religious doctrine and scripture of the church. 4). Providing pastoral care and support to members of the community. 5). Advocating for social justice and human rights causes, such as the rights of refugees and asylum seekers or indigenous peoples. 6). Offering pastoral care and support to people facing challenging life transitions, such as illness, death, or relationship breakdowns. 7). Promoting the church’s values and teachings through public engagement and advocacy. 8). Serving as a liaison between the church and the broader community. 9). Leading and organizing community outreach programs and events. 10). In addition, the clergy members in African Initiated Churches in Australia may also play a significant role in addressing mental health issues, as highlighted by the study by Murambidzi (Citation2016). They may act as gatekeepers and provide support and referrals, connecting them with appropriate mental health services. Overall, the roles of the clergy in African Initiated Churches in Australia are diverse and multifaceted, reflecting the complex and evolving nature of these communities.
Research aim and objectives
The study explores the experiences and perspectives of Zimbabwean Australian clergy members concerning their response to their congregants and community members’ mental health needs. The objectives of this research are:
To investigate how Zimbabwean Australian clergy respond to the mental health needs of their congregants and community members.
To examine the understandings and perceptions of the mental health needs of congregants by their clergy from African Initiated Churches around Australia.
To contribute to the literature on the understanding and beliefs of the causes and their responses to mental health problems among Zimbabwean Australians.
To identify how Zimbabwean Australian clergy perceive their congregants’ and community members’ mental health needs and how they respond to them.
To examine how the clergy can work with other mental health agencies in their locations.
Significance
This study is significant as it represents one of the initial investigations into the experiences of the Zimbabwean-Australian clergy population in supporting individuals with mental health problems within their communities. Prior studies, such as those by Murambidzi (Citation2016), Bledsoe et al. (Citation2013) and Heward-Mills et al. (Citation2018) indicate that clergy members are often viewed as role models by their congregants, with many seeking their guidance during times of distress. It is worth noting that the role of clergy, regardless of their religious affiliation, in providing mental health support and care is an emerging field that remains largely under-researched. Therefore, the findings of this study have the potential to contribute significantly to the existing body of knowledge by filling this knowledge gap.
Theoretical framework
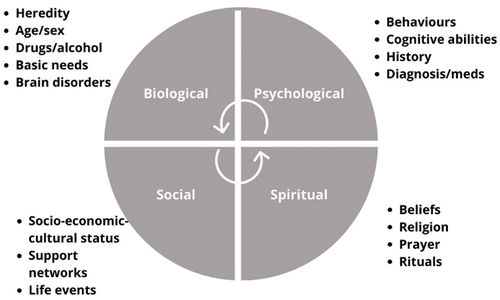
Dr George Engel proposed the biopsychosocial model (BPSM) in the 1970s as an alternative to the traditional biomedical model (Engel, Citation1977) According to Engel, health and illness result from complex biological, psychological, and social interactions (Engel, Citation1977). The model has been widely used in healthcare and is recognized as an essential framework for understanding health and illness (Leahy et al., Citation2020). The conventional BPSM posits that understanding an individual’s medical condition requires considering not only their biological factors but also their psychological and socio-economic, socio-environmental, and socio-cultural factors such as family, friends, financial difficulty, and beliefs (Papadimitriou, Citation2017).
Scholars such as King (Citation2000), McKee and Chappel (Citation1992) have advocated for the inclusion of spirituality, leading to the development of the “biopsychosocial-spiritual model” (BPSSM). This model emphasizes a holistic and comprehensive healthcare approach that considers various biological, psychological, social, and spiritual factors (Leahy et al., Citation2020). The spiritual dimension of the model is critical in recognizing the role of spirituality in promoting health and well-being (Leahy et al., Citation2020). The contrast between Indigenous spiritual values and the biomedical model of mental health emphasizes the importance of cultural and spiritual knowledge in addressing mental health needs (Dudgeon, Citation2017).
The BPSSM offers a contemporary framework suitable for investigating Zimbabwean-Australian Clergy’s understanding and experiences of responding to their communities’ mental health needs, addressing the gaps in the conventional BPSM (Murambidzi, Citation2016). The model was adopted in the current study because most Zimbabwean-Australian Congregants often rely on their spirituality for emotional and physical support (Mafuriranwa, Citation2021; Mangezi, Citation2020). By considering the spiritual dimension, the BPSSM provides a more comprehensive approach to healthcare that recognizes the role of spirituality in an individual’s well-being. This approach acknowledges that spirituality is a crucial component of human existence and can significantly impact an individual’s mental health (See ).
Figure 1. Biopsychosocial-spiritual model.
Methodology
This research employs a qualitative approach, specifically Interpretative Phenomenological Analysis (IPA) based on Smith’s work (J. A. Smith, Citation1996; J. Smith et al., Citation2009), to explore the mental health needs of Zimbabwean-Australian congregations led by the clergy (J. A. Smith & Osborn, Citation2003). IPA is considered suitable for examining how participants make sense of their personal and social worlds (J. A. Smith & Osborn, Citation2003). IPA focuses on understanding how individuals perceive psychological and social factors in their life experiences (Shaw et al., Citation2014; Tomkins, Citation2017). This approach recognizes the intersection of psychological and social factors (J. A. Smith, Citation2004), to uncover subjective perspectives on mental health within the context of migration, economic challenges, and cultural adaptation. IPA was selected as the most preferred technique for this study due to the complex and the little-studied nature of the clergy’s role in mental health (Al Omari & Wynaden, Citation2014; Eatough & Smith, Citation2008). This choice is consistent with IPA’s premise that participants have distinct perspectives and can offer detailed accounts of their lived experiences, making them authorities on their life narratives and experiences (J. A. Smith & Osborn, Citation2003).
Sampling
A non-probability purposive sampling method (Patton, Citation2015) was used to recruit sixteen participants who identified as Zimbabwean-Australian clergy (J. A. Smith & Osborn, Citation2003). Chairpersons of the Associations of the Zimbabwean Communities (in Western Australia, Victoria, New South Wales, Tasmania, and South Australia) assisted with recruitment across Australia (Patton, Citation2014). The various Chairpersons distributed information sheets to solicit participants willing to participate in the study.
Data collection and management
Demographic data collected by the research team included age, race, and ethnicity (J. A. Smith & Osborn, Citation2003). Data for this study was collected using in-depth semi-structured interviews with sixteen Zimbabwean-Australian clergy members (J. A. Smith & Osborn, Citation2003). The interviews aimed at exploring participants’ perspectives on their congregants’ or community members’ mental health problems (J. A. Smith & Osborn, Citation2003). Field notes and observations were recorded during the interviews, which were transcribed verbatim to maintain anonymity and confidentiality. Identifiers were assigned to the research participants to ensure privacy. The primary researcher (first author) conducted three of the interviews in person, and 13 were conducted online via WebEx, an online platform due to COVID-19 restrictions and the geographical location of participants. The interviews lasted 30 to 60 minutes, and responses were digitally recorded for later analysis.
Interviews explored participants’ views on the kinds of mental health problems that arise amongst the Zimbabwean-Australian Community and what they think causes mental health problems in this community. The interviews and questions asked focused on the personal life and background of participants. Examples of questions asked in this section were: 1). Can you tell me something about your experience as a member of the clergy? 2). How long have you been a clergy member, and what specific denomination is your congregation? The next set of questions focused on the conceptualization and experience of mental health problems disorders as a clinical phenomenon: Questions asked under this section included: 1). What do you understand about mental health disorders? 2). What can you tell me about your experience dealing with mental health disorders within the church congregation? The third area focused on the conceptualisation and experience of mental health disorders as a spiritual phenomenon. Questions asked in this section included: 1). How is mental illness different from demonic possession? 2). Do you think religion and spirituality is helpful in supporting the needs of individuals?
Being a cultural-insider researcher who shared the same language and cultural background with participants this may have contributed to the richness of the data obtained during the analysis, as Irvine et al. (Citation2008) suggested. Suwankhong and Liamputtong (Citation2015) assert that being a cultural insider gives a primary researcher an added advantage in gaining easy access to research participants. As a practising member of the clergy and social work practitioner, the primary investigator thus conceptualized clergy lived experiences from a cross-cultural perspective (Suwankhong & Liamputtong, Citation2015).
Ethical considerations
The study obtained ethical approval from the Curtin University Human Research Ethics Committee (Approval number: HRE2021–0037). Informed consent was obtained from the research participants. Additionally, standards for ethical conduct of research from the Australian Association of Social Workers (AASW) and the Council of Social Workers Zimbabwe (CSWZ) were examined, and all effort to ensure the study aligned with those standards was made. Permission to audio-record the interviews was sought from the participants. Only respondents who voluntarily agreed to be interviewees by signing the informed consent form were included in the study. The primary ethical consideration was the confidentiality and anonymity of participants, and to protect the privacy of participants and to safeguard the integrity of the research process, all identifying participants’ information was removed by assigning participant identifiers (Adu, Citation2019).
Data analysis
Interview recordings were transcribed verbatim before being thematically analyzed using the principles of IPA (J. A. Smith, Citation1996). In keeping with IPA protocols, the researchers had to “step into the participants’ shoes as far as possible” (Pietkiewicz & Smith, Citation2014, p. 11) to understand data from the participants’ point of view (Osborn & Smith, Citation1998). Transcripts were read several times, whilst taking note of emerging themes. Superordinate themes were developed from emergent themes and interrelated literature. The first stage comprised of initial coding of data followed by the refining of categories. Thereafter, analytical and dramaturgical analysis was done as suggested by (Saldaña, Citation2016).
Triangulation of data sources enabled the researchers to check the coding system (Patton, Citation2015) and to check the veracity and accuracy of the themes to ensure that they were derived and grounded in the data (Harding & Whitehead, Citation2013) and within IPA guidelines (J. A. Smith, Citation1996). To enable transparency and to allow themes to be drawn from data direct quotes from participants were embedded in the discussion and write up of the findings thus allowing participants’ voices to be heard (Pringle et al., Citation2011).
Results
Twelve participants from Pentecostal churches and three from mainstream churches were interviewed thus indicating a diverse representation of church traditions. Mainstream churches are typically large and well-established denominations within Christianity, with a hierarchical leadership structure and more traditional beliefs and practices (Sandal, Citation2011). On the other hand, Pentecostal churches are a group of protestant denominations that emphasize the role of the Holy Spirit in the lives of individual believers and speaking in tongues as evidence of the baptism in the Holy Spirit (Anim, Citation2020). Pentecostal Churches in the Zimbabwean-Australian community strongly emphasize speaking in tongues, working miracles, and the prosperity gospel as indicators of being born again (Harris, Citation2018; Togarasei, Citation2016). This brand of Pentecostalism is also reflected in the beliefs of Zimbabwean-Australian clergy who identify with the Pentecostal tradition. The term “Mainstream Churches” in this study refers to established denominations such as the Anglican Church, Roman Catholic Church, Methodist Church, and Uniting Church (Leavey, Citation2008; Tarusarira, Citation2020).
The participants were from Western Australia, Queensland, Australian Territory, Tasmania, New South Australia, and South Australia. Of the 16 participants, 11 were male (73%) and five were female (27%), with ages ranging from 30 to 60 years. Just over half of the participants reported receiving formal mental health training, while the rest indicated they had not received any formal mental health training. A small number were unsure of their training status.
Thematic analysis revealed three overarching themes illuminating Zimbabwean-Australian clergy explanations and understandings of mental health problems and their responses to congregants reporting MHPs: (1) spiritual explanations of mental health problems, (2) psychological explanations of mental health problems, and (3) clergy responses to mental health problems. The following is a summary of the breakdown of the main themes and sub-themes:
Spiritual explanations of mental health problems:
Evil spirits or demons
Witchcraft
Angry or unhappy ancestral spirits
Avenging or aggrieved spirits
Non-compliance to God or living in sin.
Psychological Explanations of mental health problems:
Psychological or biomedical causes.
Psychosocial explanations
Clergy responses to mental health problems:
Spiritual leadership
Health promotion and raising awareness.
Providing halfway and crisis support
Exorcism or deliverance
Prayer
Pastoral counseling
Preaching and teaching
Factors impacting on clergy response and preparedness to mental health problems:
Training
Lack of mental health information
Clergy conceptualized mental health problems as a multifaced phenomenon underpinned on spiritual and biomedical causes. The most common explanations of MHPs were evil spirits or demons known in the vernacular language as “mweya yakaipa/mweya yetsvina” or “madhimoni,” avenging or aggrieved spirits known as “ngozi” and ancestral spirits known as “midzimu.” In contrast, psychosocial and biological explanations dominated the biomedical explanations of mental health problems. Overall, the clergy’s response to mental health problems involves a combination of emotional, psychological, and spiritual support and collaboration with other professionals to ensure that people get the help they need.
Spiritual explanations of mental health problems
Evil spirits or demons
According to certain Pentecostal clergy members (Participants 1, 2, 3, 4, 6, 7, 8, 14), the primary cause of mental health problems lies in the belief in evil spirits or demons that necessitate spiritual interventions such as “deliverance” or “exorcism.” They believe that through these practices, they can forcefully “expel,” “drive out,” or “command” evil spirits to depart from those affected, resulting in freedom from physical or emotional distress for the victims (Participants 1, 2, 3, 4, 6, 14). Participant 14, for example mentioned that:
From my Afrocentric background, I think to a very large extent … evil spirits … cause mental health issues. Before I got some form of mental health training, I used to believe that spirits are the major cause of mental health issues which means to a very large extent, they cause mental health issues.
Participants (10, 12, 15) from mainstream churches reported that mental health problems were not always due to evil spirits but could also be due to biochemical and environmental factors. Although Participant 10, comes from a mainstream church, he acknowledged that evil spirits could sometimes cause mental health problems, though he admitted exorcism of evil spirits was not his area of ministry practice, he at times does conduct exorcisms.
Witchcraft
According to the clergy, mental health issues prevalent within the Zimbabwean-Australian community are primarily due to witchcraft, which uses spiritual forces to harm individuals. In the African worldview there is cultural connection to witchcraft and spirituality when addressing mental health issues in indigenous communities (Dudgeon & Walker, Citation2015; V. Mabvurira & Makhubele, Citation2018). Spiritual forces also known as poltergeist spirits can manifest themselves to their victims in various forms, such as goblins, witchcraft birds, bad airs, and poltergeist spirits. Participant 14, from an African perspective, believes that mental health problems can result from witchcraft, where evil spirits are released upon someone and cause mental health issues. Similarly, Participant 10 believes that mental health problems can result from believing in witchcraft and unhappy ancestral spirits, which afflict and torment individuals and families and adversely affect their lives and businesses.
Angry or unhappy ancestral spirits
The clergy also noted that mental health problems can be explained by believing in unhappy or angry ancestral spirits, known as “midzimu,” revered in Zimbabwean and African culture. If certain rituals are not performed, these spirits may cause misfortunes. One such ritual involves bringing the spirit of a deceased person back to their homestead, known as “kurova guva” (Rutsate, Citation2010; Vambe, Citation2009). According to Participant 10, many Zimbabwean Australians remain rooted in tradition, despite living in Australia, as if they have not entirely separated from their ancestral land.
Avenging or aggrieved spirits
Respondents reported that mental distress amongst the Zimbabwean-Community could also be attributed to spirits commonly known as avenging or aggrieved spirits (“ngozi”) in the Shona vernacular language:
If you killed someone who has not done anything wrong, it could come in that manner, avenging spirits. … it is not everything that is demonic, but this thing of avenging spirits needs something to appease, and I think if you look to Zimbabwe, you will know that … you do not just kill a person for no reason. If you have committed murder or suicide, you need to appease, which is why it can come up as an avenging spirit affecting the mental health of someone. (Participant 12)
Non-compliance to God or living in sin
Clergy also ascribed mental health problems to noncompliance with God or living in sin (“kuva nehukama hwakanaka naMwari kana kurarama muzvivi”). They reported that if one has a right relationship with God, he or she invokes God’s blessings and protection upon their life and likewise “if someone is not strong in worshiping God you can be disturbed mentally but still the hospital will be saying we cannot see any problem” (Participant 6).
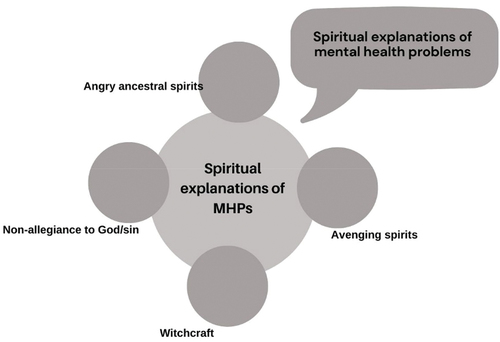
Similarly, Participant 10 reported of a church congregant who was refusing to take his medication and was suicidal. He reported that the individual appeared to have no “purpose … all he would talk about was ‘I am valueless, I have committed so much sin, I am going to go to hell, I do not deserve anything, I wasted myself during life’.” Participant 10 said all this congregant needed was counseling and someone who could assure him of his sense of purpose and God’s forgiveness. below depicts the spiritual explanations that clergy ascribed to mental health problems.
Figure 2. Spiritual explanations of mental health problems.
Psychological causes of mental health problems
Findings showed that the clergy participants drew from psychological understandings of mental health and distress, but these were largely centered on alcohol and other drugs as causative. Physical factors, such as heredity or genetics, were identified as potential biomedical contributors to mental health problems. Psychological factors extended beyond psychosocial aspects, encompassing both psychosocial and biomedical dimensions. For example, the recurrent mention of drugs and alcohol as contributing factors suggests a physiological dimension to these discussions. Participant 12’s view is that mental health problems can result from various causes, but with a specific emphasis on the impact of drug and alcohol abuse. Similarly, Participant 7’s recognition that excessive substance use, including involvement in drug pushing, can lead to mental health issues. The observations made by participants (1, 2, 3, 4, 5, 6, 8, 10, 12) mention alcohol and other drugs in the development or exacerbation of mental health issues particularly among the younger population. The inclusion of psychoactive substances like “smoking marijuana” and the view that the influence, wrong associations, and peer pressure highlight the social context in which mental health challenges may manifest among young people in the Zimbabwean-Australian community.
Psychosocial causes of mental health problems
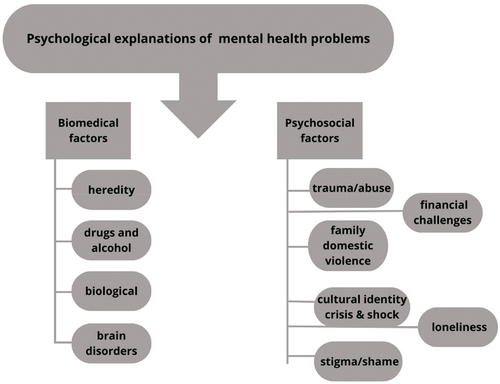
According to the clergy, the Zimbabwean-Australian community commonly experiences mental health problems from various psychosocial factors, including relationship breakdowns, domestic violence, abuse, childhood trauma, poverty, financial difficulties, and stressful life events such as loneliness and cultural identity crises (See ). Participant 4 summed the causes of mental health problems due to psychosocial factors as follows:
Loneliness and isolation can also lead someone to be depressed and then I think there is also cultural issues, cultural background, especially for the young generation because they are African by birth, but they are in a Western Culture. So, they do not really fit there, nor do they fit in the African community. So, they are kind of in between.
Figure 3. Psychological explanations of mental health problems.
Also, Participant 9 reported that migrating from Zimbabwe to Australia caused some mental health problems for some Zimbabweans:
Changing countries is a huge change and a lot of Zimbabweans have moved from overseas. They have been different roles in their society, in their community, and they come to this place and there is a role reversal of some sort. For example, back in Zimbabwe, traditionally, the men were the breadwinners. Then economically also and in terms of career wise, men tended to have better roles, better positions, better money compared to women.
Participant 10 also reported that some Zimbabwean Australians were experiencing intense feelings of isolation, loneliness, and financial difficulty due to the challenges of COVID-19 restrictions. Participant 10 reported that he had been presented with a case of “someone who had always been lonely, had lost all relatives and … felt better off dead than be alive.” He also reported of having counseled parishioners who had issues of “loneliness, … and being under … economic pressure.” Participant 9 described that some mental health problems in the Zimbabwean-Australian community were due to “traumatic situations” and “some traumatic backgrounds.” Participant 1 further confirmed that some mental health problems could be due to “trauma, … where people have experienced some adverse experiences in their lives, … which could include neglect, or abuse.”
The same view was also confirmed by Participant 7 who said that “childhood traumas can lead a person to develop mental health problems.” Likewise, Participant 15 also reported of the death by suicide of a Zimbabwean-Australian young man due to alleged homophobia and intolerance from his father toward his same-sex orientation. Participant 15 reported that there was a disagreement between the father and the young man as the father could not accept that his son was in a same-sex relationship:
In our culture [same sex relationships] is not acceptable … And there was [a] conflict between the parents and the child with the father not condoning it. And later that led the child … commit[ting] suicide and that was a very unfortunate situation, and it was a tragedy because really, we lost a life. And this was a mental challenge because the child could not accept what the father wanted, and neither could the father accept what the child wanted.
Participants (4, 5, 6, 10, 12, 13, 15) noted that the death by suicide of at least five young people within the Zimbabwean-Australian Community in the last five years was concerning, and clergy to come together to find ways of intervention and response to this problem. Figure three depicts how clergy understood mental health problems in terms of biomedical and psychological factors.
Clergy responses to mental health problems
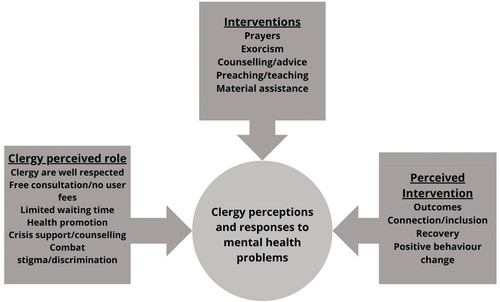
In their roles as first responders to people experiencing mental health problems, clergy mentioned pastoral interventions they employed when approached for help by their congregants and community members (See ). Data revealed by participants indicated that most clergy felt inadequately prepared to assist people with mental health problems. Interventions for mental health issues included a spectrum of clergy responses which included exorcism/deliverance, pastoral/biblical counseling, leadership, prayer, preaching/teaching, raising awareness of mental health problems, and problem-solving. However, material assistance was often given without understanding the underlying mental health problems.
Figure 4. Clergy perceptions and interventions for mental health problems.
Spiritual leadership
According to the interviewees, the Zimbabwean-Australian community holds clergy members in high regard as respected spiritual leaders. One of the interviewees, Participant 4, specifically mentioned that the clergy were perceived as spiritual leaders, and congregants believed their prayers could invoke divine intervention. As a result, clergy members were noted to have a significant influence on the health choices made by their parishioners. They were seen as promoting positive health and well-being by offering spiritual guidance and encouragement to their congregants.
Health promotion and raising awareness of mental health treatments
Participants reported that clergy were involved in promoting health and raising awareness on mental health treatments through health promotion programs, education and seminars on mental health and available resources and treatments. Participant 4 noted that in their church, they invite various speakers and experts who speak on various:
Areas of mental health, so they bring awareness to the community that there is mental health, it can be treated, you do not have to suffer by yourself. So, we have meetings among the ladies, … sometimes, we have combined sessions with the whole church.
Participant 4 further noted that other areas they teach to young people were “drug abuse, sexual abuse … alcoholism … bullying and peer pressure.”
Providing crisis support
Participants reported that due to multifaceted problems affecting the Zimbabwean-Australian community, clergy and the church were also perceived as important community resources that provided crisis support for individuals and families experiencing various problems, including family and domestic violence and various life challenges. Participant 13 reported that his church had opened “a halfway house or a transitional home” where women who are victims of domestic violence are offered temporary accommodation. It was reported that clergy were consulted on various life challenges such as marital issues, homelessness, trauma, abuse, financial difficulty, grief and loss, drugs and alcohol, and mental health problems. In this regard, most participants believed the church was better positioned to be the first point of contact for people in emotional and psychosocial distress.
Exorcism or deliverance
Clergy members reported using exorcism, also known as deliverance in certain Pentecostal churches, as an intervention for mental health problems. According to Participant 2, pastors conducted exorcism to cast out or expel evil spirits or demons. Participant 1 also acknowledged that demonic spirits can affect people, and that through prayer, demons can be expelled from a person’s life, leading to their recovery.
Prayer
According to the clergy interviewed, prayer was the most common response when congregants sought physical and emotional assistance. Congregants requested prayers for healing, deliverance, exorcism, and emotional support, perceiving pastors as possessing divine power to relieve their physical and emotional distress. As Participant 1 affirmed, prayer was often used to alleviate the distress caused by demonic spirits.
Pastoral or biblical counselling
According to the clergy interviewed, pastoral or biblical counseling was the second most common intervention for people with mental health problems. Pastoral and biblical counseling were reported to strengthen individuals and families and assist them in coping with life’s challenges through the word of God. Participant 4 mentioned that pastoral counseling and prayers for the sick were offered at no cost. Participant 4 stated that:
Freely we receive these gifts of helping people, and freely we give them; there is no cost whatsoever. We are willing to travel even to people’s houses or to where they are where they need help; we are willing to invite them over to our places to speak to them and to pray for them.
Preaching and teaching
Biblical preaching and teaching from the gospel pulpit were reported to be one of the key clergy interventions and contributions that enhanced positive and lifestyle behavior changes. According to the respondents, the clergy are involved in teachings that aim at changing unhealthy behaviors and lifestyles which either led to or were associated with many life problems including mental illness. Figure four illustrates clergy perceptions and perceived interventions for mental health problems.
Factors impacting on clergy response and preparedness for mental health problems
Training
Data collected suggest that clergy had a strong understanding of the spiritual explanation of mental health problems (Participants 1, 2, 3, 4, 6, 7, 11, 13) and clergy respond to these through biblical or scriptural counseling, exorcism, or practical deliverance. They are aware of the biomedical view of mental health problems, but they do not feel confident or well trained as their seminary or bible college training curriculum in Zimbabwe does not cover mental health issues. This is like findings by Murambidzi (Citation2016) who identified that the seminary and bible school training of pastors in Zimbabwe lacks components of mental health training. According to some respondents, mental health was partially covered in related topics and courses such as psychology, sociology and pastoral care and counseling as shown by Participant 15, who noted that mental health was not part of their clergy theological curriculum, hence, there should be “more training on mental health issues being afforded to the Clergy.”
There seemed to be a tendency to spiritualize and view presentations of mental health problems (especially by some Pentecostal preachers) as being demonic manifestations which required exorcism or practical deliverance where evil spirits were cast out. For instance, Participant 6 noted that pastors are better positioned and endowed “to help people with mental health problems … as they understand the spiritual and physical life all together.” Participant 6 who is a Pentecostal Pastor said:
In my understanding as a clergy … mental health problems … are more spiritual than … what people see on the physical. So, we look at it in the spiritual aspect that someone is affected in the spiritual side more than the physical that can be seen.
Lack of mental health information
The study findings show scarcity of mental health information and lack of awareness of mental health issues amongst clergy according to Participants (2, 10, 12, 15). Clergy reported lack of knowledge on available mental health services, and this impacted on their referral procedures between the church and the formal health system. Participant 1 who himself is a mental health professional cited that he provides contacts for mental health support services within his community through his church’s newsletters and church bulletins.
Discussion
This study aimed to explore the experiences and perspectives of African Initiated Church clergy members in Australia regarding mental health problems in the Zimbabwean-Australian community. The findings revealed that both spiritual and psychological factors were perceived to contribute to mental health problems in this community. The study also highlighted the significant role of clergy members as gatekeepers and initial points of contact for individuals experiencing mental distress (Heseltine-Carp & Hoskins, Citation2020). The study’s results suggest that the church can be crucial in supporting individuals with mental health issues and connecting them to appropriate mental health services (Heward-Mills et al., Citation2018).
The role of spirituality in mental health has been widely recognized and our study confirms that spirituality is a significant factor in the Zimbabwean-Australian community’s perception of mental health and is important to consider in contexts of Indigenous knowledge more widely (Dudgeon & Walker, Citation2015). Participants reported that mental health issues were sometimes attributed to spiritual factors, such as demonic possession or spiritual warfare. However, our study also found that clergy members often had a more holistic view of mental health that recognized spiritual and psychological dimensions. This finding highlights the importance of engaging with clergy members to provide culturally responsive and effective mental health support (Mandizadza & Chidarikire, Citation2016; Murambidzi, Citation2016).
This study also revealed the significant role of clergy members as gatekeepers and initial points of contact for individuals experiencing mental distress (Heseltine-Carp & Hoskins, Citation2020; Heward-Mills et al., Citation2018). Participants reported that clergy members were often the first people approached for help with mental health problems and were expected to provide emotional support, counseling, and spiritual guidance. This finding emphasizes the need for greater collaboration between clergy members and mental health organizations to ensure individuals receive appropriate care.
The outcomes of this research have significant implications for the instruction and preparation of religious leaders and mental health practitioners. The church can utilize these findings to develop its training and educational initiatives, which can improve the comprehension and recognition of mental health concerns among African communities. One approach could be for pastors to dedicate a week in their church programs to mental health awareness, inviting mental health professionals to provide additional support. Collaborating with mental health professionals may lead to early intervention and prevention of mental health problems.
Research has shown that clergy members can be crucial in identifying and addressing mental health problems in their congregations and communities. They are often the first point of contact for individuals experiencing mental health issues. They can help reduce stigma and increase awareness about mental health by providing education and outreach (Koenig, Citation2018). Clergy members often provide emotional support and a listening ear to those struggling with mental health problems. Through this type of counseling, clergy members can help individuals feel heard and understood, which can in turn promote healing and recovery. In addition to emotional support, clergy members can also provide spiritual support for those struggling with mental health issues. This may include prayer, meditation, or other religious practices that can help people feel more connected to a higher power or a sense of purpose (Dudgeon & Walker, Citation2015; Koenig, Citation2008). Research by has suggested that spirituality and religion can be protective factors for mental health, and incorporating these practices into treatment can benefit some individuals. This agrees with research by Dudgeon and Walker (Citation2015) and Grieves (Citation2009) who also posit that Aboriginal and Torres Strait Islander people have cultural worldviews and experiences that are rooted in religion and spirituality (Dudgeon & Walker, Citation2015; Grieves, Citation2009).
Clergy members may also refer congregants and community members to mental health professionals if they feel that more specialized support is needed. They can provide information about local resources for mental health care and offer support in finding the right therapist or treatment. In some cases, clergy members may also collaborate with mental health professionals to provide more comprehensive support. This may involve joint counseling sessions or workshops combining psychological and spiritual healing approaches (Toussaint et al., Citation2011).
Implications for social work collaborating with clergy working in mental health care
The role of clergy members in supporting mental health is not without its challenges. Clergy members may struggle to identify mental health issues and navigate the complexities of confidentiality and informed consent. They may also need to balance their role as a spiritual leader with that of a mental health advocate, which can require a delicate balancing act (Beaumont, Citation2011). Collaboration between social workers and clergy in mental health care can be beneficial in ensuring ethical and effective treatment for individuals. Clergy can provide spiritual and emotional support to individuals struggling with mental health issues, complementing traditional mental health treatment (Heward-Mills et al., Citation2018). On the other hand, clergy may not have the same level of training and expertise as mental health professionals, which could lead to inappropriate or harmful interventions (Heseltine-Carp & Hoskins, Citation2020).
Clergy members play a crucial role in providing support and guidance to individuals dealing with mental health challenges. In that regard, clergy may require training in mental health areas such as Mental Health First Aid (MHFA); Substance Abuse Counseling; Suicide Prevention; Trauma-Informed Care and Mental Health Awareness. The involvement of clergy in mental health care and the integration of religion/spirituality with social work can lead to more comprehensive and culturally sensitive support for individuals facing mental health challenges.
Social work collaboration with faith-based communities and churches involves a recognition that these organizations as important contributors to civil society and often act as crucial conduits to community participation for significant members of different ethnic and religious citizens. Social workers can collaborate with churches by developing partnerships with local religious leaders and congregations. This could involve providing mental health education and training to clergy and lay leaders and offering mental health services within the church setting. Social workers can also work with churches to develop outreach programs targeting underserved populations, such as the homeless or impoverished. Collaborating with ministers and church community leaders to build a more integrated mental health response can be a valuable way for social workers to address the mental health needs of these specific communities.
Limitations
Some limitations of this study should be acknowledged. Firstly, the sample size was relatively small, and participants were drawn from a single denomination, which may limit the generalizability of our findings. Secondly, the study relied on self-report data, which may be subject to social desirability bias. Finally, while Interpretive Phenomenological Analysis enabled exploration of participants’ experiences and perspectives in depth, applying the findings to other contexts may be challenging.
The principal researcher, interviewer and first author is a Zimbabwean Australian. This has allowed for a unique positioning as both a cultural insider and an objective researcher (Denzin & Lincoln, Citation2017; Fleming, Citation2018). Being a cultural insider allowed the first author to understand interviewees’ beliefs, values, customs, and norms in ways that an outsider might struggle to comprehend. It allowed for building rapport with the participants more efficiently, as they were often willing to explore in considerable depth their experiences (Suwankhong & Liamputtong, Citation2015). Preconceived notions about specific topics or assumptions about what the participants would say required recognition of biases and active mitigation of their impact on the research process (Fleming, Citation2018). Ongoing discussion with the research team (authors 2 and 3) assisted in maintaining and reflexive standpoint on the research, analysis, and reporting of findings.
Conclusion
This qualitative study has provided valuable insights into the experiences and perspectives of clergy members from African Initiated Churches in Australia and their role in addressing mental health issues in African communities. The findings emphasize the importance of understanding the cultural and spiritual factors that contribute to mental health issues in Zimbabwean-Australian communities and the critical role of clergy members in providing culturally responsive support and connecting individuals to appropriate mental health services.
This study contributes to the mental health field by enhancing our understanding of the clergy’s role in addressing mental health issues in African communities. Future research could build on these findings by exploring the experiences of individuals with mental health issues and mental health professionals in these communities and investigating effective interventions for promoting mental health and wellbeing in African communities. Ultimately, our study highlights the importance of culturally responsive mental health services that consider the unique cultural and spiritual beliefs and practices of individuals seeking help. Our study also highlights the challenges faced by African communities in accessing mental health services and the need for greater collaboration between clergy members and mental health organizations to promote mental health and well-being in these communities. We recommend using these findings to inform the development of culturally responsive mental health services and the training and education of clergy members to support individuals with mental health issues better.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Adu, P. (2019). A step-by-step guide to qualitative data coding. Routledge. http://ebookcentral.proquest.com/lib/curtin/detail.action?docID=5747025
- AIHW. (2012). Australia’s Health Series. Australian Institute of Health and Welfare.
- Al Omari, O., & Wynaden, D. (2014). Interpretative phenomenological analysis: The lived experience of adolescents with cancer. SAGE Publications, Ltd.
- Anim, E. K. (2020). An evaluation of Pentecostal Churches as agents of sustainable development in Africa: The case of the Church of Pentecost. In P. Öhlmann, W. Gräb, & M.L. Frost, African Initiated Christianity and the Decolonisation of Development (pp. 195–211). Routledge.
- Australian Association of Social Workers. (2021). Australian social work education and accreditation standards (ASWEAS) 2012: Guideline 1.1 guidance on essential core curriculum content. https://www.aasw.asn.au/document/item/3552
- Australian Bureau of Statistics. (2021). Census of population and housing: Cultural diversity data summary, 2021. Australian Bureau of Statistics Retrieved from. https://www.abs.gov.au/statistics/people/people-and-communities/cultural-diversitycensus/2021#data-download
- Beaumont, S. M. (2011). Pastoral counseling down under: A survey of Australian clergy. Pastoral Psychology, 60(1), 117–131. https://doi.org/10.1007/s11089-010-0289-4
- Bland, R., Drake, G., & Drayton, J. (2021). Social work practice in mental health: An introduction. Taylor & Francis Group.
- Bledsoe, T. S., Setterlund, K., Adams, C. J., Fok-Trela, A., & Connolly, M. (2013). Addressing pastoral knowledge and attitudes about clergy/mental health practitioner collaboration. Social Work & Christianity, 40(1), 23–45.
- Bourdillon, M. F. (1987). The Shona peoples: An ethnography of the contemporary Shona, with special reference to their religion (Vol. 1). Mambo Press.
- Calma, T., Dudgeon, P., & Bray, A. (2017). Aboriginal and Torres Strait Islander social and emotional wellbeing and mental health. Australian Psychologist, 52(4), 255–260. https://doi.org/10.1111/ap.12299
- Chaumba, J. (2016). Social capital and employment outcomes of Zimbabwean immigrants in the United States. Journal of International Migration and Integration, 17(2), 487–505. https://doi.org/10.1007/s12134-015-0419-z
- Chenoweth, L., & McAuliffe, D. (2017). The road to social work & human service practice. Cengage AU.
- Chogugudza, C. (2009). Social work education, training and employment in Africa: The case of Zimbabwe. Ufahamu: A Journal of African Studies, 35(1). https://doi.org/10.5070/F7351009559
- Crisp, B. R. (2010). Spirituality and social work. Ashgate Publishing Group.
- Daneel, M. L. (1987). Quest for belonging: Introduction to a study of African independent churches. Mambo Press.
- Denzin, N. K., & Lincoln, Y. S. (2017). The Sage Handbook of Qualitative Research. Sage Publications.
- Dudgeon, P. (2017). Australian indigenous psychology. Australian Psychologist, 52(4), 251–254. https://doi.org/10.1111/ap.12298
- Dudgeon, P., & Walker, R. (2015). Decolonising Australian psychology: Discourses, strategies, and practice. Journal of Social and Political Psychology, 3(1), 276–297. https://doi.org/10.5964/jspp.v3i1.126
- Eatough, V., & Smith, J. A. (2008). Interpretative Phenomenological Analysis (Vol. 179). Sage Publishing. https://doi.org/10.4135/9781848607927.n11
- Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196(4286), 129–136. https://doi.org/10.1126/science.847460
- Fleming, J. (2018). Recognizing and resolving the challenges of being an insider researcher in work-integrated learning. International Journal of Work-Integrated Learning, 19(3), 311–320.
- Forrest, J., Poulsen, M., & Johnston, R. (2013). Middle-class diaspora: Recent immigration to Australia from South Africa and Zimbabwe. South African Geographical Journal= Suid-Afrikaanse Geografiese Tydskrif, 95(1), 50–69. https://doi.org/10.1080/03736245.2013.806104
- Gatseva, P. D., & Argirova, M. (2011). Public health: The science of promoting health. Journal of Public Health, 19(3), 205–206. https://doi.org/10.1007/s10389-011-0412-8
- Grieves, V. (2009). Aboriginal spirituality: Aboriginal philosophy. The basis of aboriginal social and emotional wellbeing. Discussion Paper No. 9).
- Griffith, J. L., Myers, N., & Compton, M. T. (2016). How can community religious groups aid recovery for individuals with psychotic illnesses? Community Mental Health Journal, 52(7), 775–780. https://doi.org/10.1007/s10597-015-9974-1
- Hankerson, S. H., Watson, K. T., Lukachko, A., Fullilove, M. T., & Weissman, M. (2013). Ministers’ perceptions of church-based programs to provide depression care for African Americans. Journal of Urban Health, 90(4), 685–698. https://doi.org/10.1007/s11524-013-9794-y
- Harding, H., & Whitehead, D. (2013). Analysing data in qualitative research. In Z. Schneider, D. Whitehead, L.-W. G., & J. Haber (Eds.), Nursing and midwifery research: Methods and appraisal for evidence-based practice (5th ed., pp. 141–160). Elsevier.
- Harris, J. (2018). African American Pentecostal clergy members’ perceptions of mental health and their subsequent referral practices philadelphia college of osteopathic medicine. https://digitalcommons.pcom.edu/psychology_dissertations/460.
- Heseltine-Carp, W., & Hoskins, M. (2020). Clergy as a frontline mental health service: A UK survey of medical practitioners and clergy. General Psychiatry, 33(6), e100229. https://doi.org/10.1136/gpsych-2020-100229
- Heward-Mills, N. L., Atuhaire, C., Spoors, C., Pemunta, N. V., Priebe, G., & Cumber, S. N. (2018). The role of faith leaders in influencing health behaviour: A qualitative exploration on the views of Black African Christians in Leeds, United Kingdom. The Pan African Medical Journal, 30. https://doi.org/10.11604/pamj.2018.30.199.15656
- Hodgson, D., & Watts, L. (2017). Key concepts and theory in social work. Palgrave.
- Howe, B., & Howe, R. (2012). The influence of faith-based organisations on Australian social policy. Australian Journal of Social Issues, 47(3), 319–333. https://doi.org/10.1002/j.1839-4655.2012.tb00251.x
- Irvine, F., Roberts, G., & Bradbury-Jones, C. (2008). The researcher as insider versus the researcher as outsider: Enhancing rigour through language and cultural sensitivity. In P. Liamputtong (Ed.), Doing cross-cultural research (pp. 35–48). Springer.
- Kajawu, L. S. C., Jack, H., & Tonya, N. T. (2016). What do African traditional medical practitioners do in the treatment of mental disorders in Zimbabwe? International Journal of Culture and Mental Health, 1(1), 1–12. https://doi.org/10.1080/17542863.2015.1106568
- King, D. E. (2000). Faith, spirituality, and medicine: Toward the making of the healing practitioner. Psychology Press.
- Koenig, H. (2018). Spiritual care for allied health practice: A person-centered approach. Jessica Kingsley Publishers.
- Koenig, H. G. (2008). Medicine, religion, and health where science & spirituality meet. Templeton Foundation Press.
- Krüger, C. (2020). Culture, trauma and dissociation: A broadening perspective for our field. Journal of Trauma & Dissociation, 21(1), 1–13. https://doi.org/10.1080/15299732.2020.1675134
- Lawrence, D., Johnson, S., Hafekost, J., Boterhoven de Haan, K., Sawyer, M., Ainley, J., & Zubrick, S. R. (2015). The Mental Health of Children and Adolescents: Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing.
- Leahy, E., Chipchase, L., Calo, M., & Blackstock, F. C. (2020). Which learning activities enhance physical therapist practice? Part 1: Systematic review and meta-analysis of quantitative studies. Physical Therapy, 100(9), 1469–1483. https://doi.org/10.1093/ptj/pzaa107
- Leavey, G. (2008). U.K. clergy and people in mental distress: community and patterns of pastoral care. Transcultural Psychiatry, 45(1), 79–104. https://doi.org/10.1177/1363461507087999
- Mabvurira, V. (2016). Influence of African traditional religion and spirituality in understanding chronic illnesses and its implications for social work practice: A case of Chiweshe communal lands in Zimbabwe [ Doctoral diss.]. University of Limpopo. South Africa
- Mabvurira, V., & Makhubele, J. (2018). Influence of Shona beliefs in understanding illness: Implications for indigenous social work practice in Zimbabwe. Theologia Viatorum: Journal of Theology and Religion in Africa, 42(1), 77–99.
- Mafuriranwa, R. (2021). Interfacing religion, spirituality and social work. In V. Mabvurira (Ed.), Professional social work in Zimbabwe. Past, present and the future (p. 225). National Association of Social Workers of Zimbabwe. <https://lnkd.in/g9988gB>
- Mandizadza, E. J., & Chidarikire, S. (2016). A Phenomenological study into the role of spirituality and religiousness in the mental health of people with cancer in Zimbabwe. Journal of Spirituality in Mental Health, 18(2), 145–161. https://doi.org/10.1080/19349637.2015.1100972
- Mangezi, W. (2020). A letter from Zimbabwe. The Lancet Psychiatry, 7(5), 394. https://doi.org/10.1016/S2215-0366(20)30166-8
- Mbiti, J. (1969). African religions and philosophy. East African Educational Publishers Ltd.
- McKee, D. D., & Chappel, J. N. (1992). Spirituality and medical practice. Journal of Family Practice, 35(2), 201–205.
- Meyer-Weitz, A., Reddy, P., Weijts, W., Van den Borne, B., & Kok, G. (1998). The socio-cultural contexts of sexually transmitted diseases in South Africa: Implications for health education programmes. Aids Care-Psychological & Socio-Medical Aspects of Aids/hiv, 10(2), 39–55. https://doi.org/10.1080/09540129850124352
- Muchinako, G. A., Mabvurira, V., & Chinyenze, P. (2013). Mental illness and the Shona People. Advanced Research in Management and Social Sciences, 2(3), 160–172. https://garph.co.uk/IJARMSS/Mar2013/13.pdf
- Murambidzi, I. (2016). Conceptualisation of mental illness among Christian Clergy in Harare, Zimbabwe. University of Cape Town. Cape Town,sA. http://hdl.handle.net/11427/23421
- Osborn, M., & Smith, J. A. (1998). The personal experience of chronic benign lower back pain: An interpretative phenomenological analysis. British Journal of Health Psychology, 3(1), 65–83. https://doi.org/10.1111/j.2044-8287.1998.tb00556.x
- Papadimitriou, G. (2017). The “biopsychosocial Model”: 40 years of application in psychiatry. Psychiatrike= Psychiatriki, 28(2), 107–110. https://doi.org/10.22365/jpsych.2017.282.107
- Patel, V., Mutambirwa, J., & Nhiwatiwa, S. (1995). Stressed, depressed, or bewitched? Development in Practice, 5(3), 216–224. https://doi.org/10.1080/0961452951000157214
- Patton, M. (2015). Qualitative research & evaluation methods: Integrating theory and practice (4th ed.). SAGE Publications, Inc.
- Patton, M. Q. (2014). Qualitative research & evaluation methods: Integrating theory and practice. Sage publications.
- Pietkiewicz, I., & Smith, J. A. (2014). A practical guide to using interpretative phenomenological analysis in qualitative research psychology. Psychological Journal, 20(1), 7–14. https://doi.org/10.14691/cppj.20.1.7
- Pringle, J., Drummond, J., McLafferty, E., & Hendry, C. (2011). Interpretative phenomenological analysis: A discussion and critique. Nurse researcher, 18(3), 20–24. https://doi.org/10.7748/nr2011.04.18.3.20.c8459
- Ranger, T. (2007). African initiated churches. Transformation: An International Journal of Holistic Mission Studies, 24(2), 65–71. https://doi.org/10.1177/026537880702400201
- Rutsate, J. (2010). Mhande dance in the kurova guva ceremony: An enactment of Karanga spirituality. Yearbook for Traditional Music, 42, 81–99. https://doi.org/10.1017/S0740155800012674
- Saldaña, J. (2016). The coding manual for qualitative researchers. Sage.
- Sandal, N. A. (2011). Religious actors as epistemic communities in conflict transformation: The cases of South Africa and Northern Ireland. Review of International Studies, 37(3), 929–949. https://doi.org/10.1017/S0260210510001592
- Shaw, R., Burton, A., Xuereb, C. B., Gibson, J., & Lane, D. (2014). Interpretative phenomenological analysis in applied health research. SAGE Publications, Ltd. Springer.
- Shizha, E., & Charema, J. (2012). Health and wellness in Southern Africa: Incorporating indigenous and western healing practices. International Journal of Psychology and Counselling, 4(5), 59–67. https://doi.org/10.5897/IJPC10.030
- Smith, J. A. (1996). Beyond the divide between cognition and discourse: Using interpretative phenomenological analysis in health psychology. Psychology and Health, 11(2), 261–271. https://doi.org/10.1080/08870449608400256
- Smith, J. A. (2004). Reflecting on the development of interpretative phenomenological analysis and its contribution to qualitative research in psychology. Qualitative Research in Psychology, 1(1), 39–54.
- Smith, J., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis theory, method and research. Sage Publishing.
- Smith, J. A., & Osborn, M. (2003). Interpretative phenomenological analysis. In I. I. A. I. A. Smith (Ed.), Qualitative psychology: A practical guide to methods (p. 51–80). Sage.
- Suwankhong, D., & Liamputtong, P. (2015). Cultural insiders and research fieldwork: Case examples from cross-cultural research with Thai people. International Journal of Qualitative Methods, 14(5), 1609406915621404. https://doi.org/10.1177/1609406915621404
- Taringa, N. J. E. (2006). How environmental is African traditional religion? Exchange, 35(2), 191–214. https://doi.org/10.1163/157254306776525672
- Tarusarira, J. (2020). When piety is not enough: Religio-political organizations in pursuit of peace and reconciliation in Zimbabwe. Religions, 11(5), 235. https://doi.org/10.3390/rel11050235
- Togarasei, L. (2016). Historicising Pentecostal Christianity in Zimbabwe. Studia Historiae Ecclesiasticae, 42(1), 1–13. https://doi.org/10.25159/2412-4265/103
- Tomkins, L., Applied Qualitative Research in Psychology. (2017). Using interpretative phenomenological psychology in organisational research with working carers. In J. Brooks & N. King (Eds.), Applied Qualitative Research in Psychology (pp. 86–100). Palgrave Macmillan. https://doi.org/10.1057/978-1-137-35913-1_5
- Toussaint, L., Webb, J. R., & Keltner, W. (2011). Religion, spirituality and mental health. In J. Aten, K. O‘Grady, & E. Worthington (Eds.), The Psychology of Religion and Spirituality for Clinicians: Using Research in Your Practice (pp. 331–362). Taylor & Francis Group.
- Vambe, M. T. (2009). The function of songs in the Shona ritual-myth of Kurova Guva. Muziki, 6(1), 112–119. https://doi.org/10.1080/18125980903037393
- Verma, R. K., Sharma, S., Singh, R., Rangaiyan, G., & Pelto, P. J. (2003). Beliefs concerning sexual health problems and treatment seeking among men in an Indian slum community. Culture, Health & Sexuality, 5(3), 265–276. https://doi.org/10.1080/1369105011106356
- Vos, T., Barber, R. M., Bell, B., Bertozzi-Villa, A., Biryukov, S., Bolliger, I., Charlson, F., Davis, A., Degenhardt, L., Dicker, D., Duan, L., Erskine, H., Feigin, V. L., Ferrari, A. J., Fitzmaurice, C., Fleming, T., Graetz, N., Guinovart, C. … Salomon, J. A. (2013). Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. The Lancet, 386(9995), 743–800. https://doi.org/10.1016/S0140-6736(15)60692-4
- Watts, L., & Hodgson, D. (2022). A social justice perspective on the bio-psycho-social-spiritual dimensions of health. In M. Petrakis (Ed.), Social work practice in health: An introduction to contexts, theories and skills (pp. 14–24). Taylor & Francis Group.
- Zimbabwe National Statistical Agency. (2022). Census Preliminary Report – 2022, Zimbabwe. https://zimbabwe.opendataforafrica.org/anjlptc/2022-population-housing-census-preliminary.
- Zimbabwe National Statistics Agency. (2017). Inter-censal demographic survey. https://zimbabwe.unfpa.org/sites/default/files/pub-pdf/Inter%20Censal%20Demography%20Survey%202017%20Report.pdf
