
ABSTRACT
We present a methodological, theoretical, and technological outline of codesign principles for the effective development of digital heritage extended reality systems for health and care. The paper is based on two large-scale research projects involving ageing in rural and coastal communities, focused on the codesign of extended reality systems to stimulate new forms of access to local heritage sites with potential impact on health outcomes. Our approach stems from a multi-disciplinary collaboration between health, digital design, and heritage specialists, and suggests ways to reconcile diverging forms of knowledge production, such as our ‘researcher in residence’ methodology and the place-based complexities of codesigning such systems. Based on an analysis of fieldwork data and our own fieldwork experiences, the paper presents a roadmap for the codesign of digital heritage extended reality systems for health interventions that meet the needs of stakeholders and organisational implementation requirements, providing a useful tool in supporting the health and social care system for our ageing population.
1. Introduction
Following initial development, extended reality for health and care (we will denote these as XR-H throughout the paper) systems commonly undergo studies to assess their benefits. However, technical feasibility studies provide little insight into their effectiveness (Kim Citation2013), that is, the impact and adoption of the product in real-world settings. This leads to systems that, often, poorly match evidential and implementation requirements for successful delivery. Barriers that can be underappreciated without engaging stakeholders include realistic perceptions of price, digital health literacy of staff facilitating device use, or technical constraints such as connectivity infrastructure (Lucy et al. Citation2022). The high rate of development and obsolescence in the immersive sector exacerbates these implementation challenges (Sayma et al. Citation2020) with overworked healthcare staff unable to maintain pace with increasingly demanding digital skills, further emphasising digital health access inequalities (Yao et al. Citation2022). The effective development of XR-H systems is, then, a multidimensional challenge encompassing not only the creation of technologies, but broader organisational, technical, and social dynamics of institutions and communities of end users.
XR-H is, however, a broad innovation area which encompasses applications such as exposure therapies, surgical simulation, or pain management to name a few (Snoswell and Snoswell Citation2019). Within this emerging field, our paper focuses on interaction with heritage locations. Both heritage and healthcare organisations are increasingly addressing broader approaches to preventative medicine and multi-agency approaches to care and wellbeing (Reilly, Nolan, and Monckton Citation2018). Barton et al (Citation2009) report higher levels of mood and self-esteem (and lesser levels of fatigue or tension) in participants after accessing heritage sites. Furthermore, Price et al (Citation2020) indicate that heritage sites improve quality of life of visitors by providing opportunities for reminiscence with positive social and cognitive outcomes. Gallou (Citation2022) expands on this body of work by reviewing the notion of ‘wellbeing’ and proposing different pathways through which social wellbeing and heritage might be connected in ways not often considered in health literature, such as connectedness to place (and place-protective behaviour) and reduction of loneliness, and is aligned with Power and Smyth (Citation2016) who report positive feelings of belonging, engagement and place-based social wellbeing.
Despite this emerging body of evidence, research on the health outcomes from accessing heritage through digital platforms is limited. Older adults in particular are invested in heritage yet may face exclusion both through physical and digital media. Physical access to heritage sites is often limited due to site characteristics and conservation issues (e.g. uneven ground, or the inability to implement accessibility features) (Marasco and Balbi Citation2019). Digital heritage XR-H systems can therefore aid in inclusivity for those with physical and sensory barriers (Paladini et al. Citation2019) which are prevalent for older adults in care homes. We acronymise this approach as H-XR-H, and pose that H-XR-H interventions can provide a meaningful social activity for older adults, care home residents or patients, improving their quality of life and physical and mental health (Baker et al. Citation2020; Smith et al. Citation2018).
In this paper we identify three core areas to consider (methodological, place-based, and technological) for effective H-XR-H codesign with older adults, building upon a short paper published in the IEEE Conference on Virtual Reality and 3D User Interfaces (Veliz Reyes et al. Citation2023), fieldwork codesign data, and our own reflections arising from the planning and delivery of two large-scale research projects. After introducing our methodology, Section 3.1 discusses the methodological issues arising from multidisciplinarity in H-XR-H codesign. Here we review concepts such as ‘ill-defined problems’ originated in design research and the consideration of multidisciplinary work as an ‘information ecology’ (Nardi and O’Day Citation1999; Wang Citation2021) that ‘complexifies’ technological development. In Section 3.2 we discuss the contextualisation of place-based H-XR-H interventions and the fitness of a place-based paradigm within our research. Before a final discussion, Section 3.3 details experience design and technological considerations for H-XR-H codesign which facilitate embeddedness, participation, and access.
2. Methodology
2.1. Case studies
This paper emerges from two projects funded by UK Research and Innovation. Our research teams are working with older adults in local care homes and intergenerational groups on the codesign of H-XR-H systems stimulating new forms of access to and engagement with heritage sites. These projects are delivered by research staff representing the fields of health informatics, digital architectural design, heritage, smart cities and communities, sensing, and computing, to name a few, with participants from local care homes and community organisations comprising older adults and care home staff. Specifically, ‘Generating older active lives digitally’ (GOALD) focuses on XR-H for physical activity and sports reminiscence (delivered in partnership with the University of Stirling in Scotland), while ‘Intergenerational codesign of novel technologies in coastal communities’ (ICONIC) focuses on the intergenerational cocreation of digital technologies for H-XR-H, AI for voice recognition, telepresence, and social games. Prior work has demonstrated the importance of engaging end-users in design for other technologies aimed at health and care (H. L. Bradwell et al. Citation2019), and noted the importance of effectiveness (testing within real-world settings and contexts) rather than highly controlled trials demonstrating efficacy (H. Bradwell et al. Citation2022).
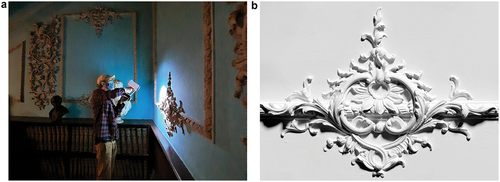
Throughout this paper, sections are illustrated by two case study historical locations in Southwest England: the Stair Hall at Powderham Castle (), and Higher Uppacott, a medieval longhouse in Dartmoor National Park (). Both sites have specific physical access issues that our heritage partners were keen to resolve through digital interpretation, and offer contrasts in terms of testing the potential of H-XR-H. The interior space at Powderham is tall, equivalent of four-stories, narrow and well-lit by roof-lights, including high walls, ceilings and ornamental details. The space at Higher Uppacott is single-storey, low and dark: lit-only by two small openings. The walls at Powderham are smooth but the extensive plasterwork is modelled in three dimensions and projects each object into the space; the interior surfaces at Higher Uppacott, by contrast, are simply-made, rough-textured and varied. Here, then, we not only address the technological specifications involved in the production of XR-H as ‘digital replicas’, but more broadly consider conditions of engagement, memory, material and place involved in the interpretation and interaction with our case study sites.
Figure 1. (Left): interior view of the stair all, Powderham Castle. figure 1b (right): interior view of the medieval longhouse in higher uppacott.

2.2. Participants
Throughout fieldwork, participant numbers ranged between 1 and 20 per activity. These activities comprised feedback, codesign or evaluation sessions involving H-XR-H, or sessions to familiarise participants with XR technology. Our researchers have facilitated evaluation and codesign sessions that are sensitive to different (and often, incremental) degrees of expertise throughout the project. GOALD fieldwork in England comprised 77 participants including 60 older adults, 5 young people, and 12 care home staff members. From this group, 35 engaged with H-XR-H systems, including 27 older adults, 2 young people, and 6 care home staff members. Their interactions with H-XR-H are a subset of a total of 870 recorded interactions with different forms of technology such as omnidirectional treadmills (H. Bradwell et al. Citation2023). All 35 participants interacted at least once with H-XR-H systems, but also interacted with other technologies which improved their overall digital literacy and expertise throughout the project, ranging from 3 to 20 interactions per participant. ICONIC comprises (to date) 16 participants engaging with H-XR-H systems, including 11 older adults and 5 young people. From this group, 3 older and 2 younger participants had used an XR system previously; all other participants were new to using XR technologies. Here we also identified an incremental digital expertise throughout the project, with participants taking part in 1 to 6 workshops each. As a result, this paper reports on mixed levels of expertise and an incremental digital literacy throughout these projects, with a substantial share (45%) of participants engaging in 5 or more activities (). Some people participated in both projects.
Figure 2. Recorded interactions with H-XR-H technology for both projects reported in this paper including young people (YP), older adults (OA) and care home staff members (staff). For ICONIC, this includes an initial session to familiarise participants with XR technologies. GOALD, this includes non-technology codesign and evaluation sessions.
2.3. Fieldwork and data analysis
The projects’ delivery plan comprises (to date) 93 fieldwork activities delivered by a team of research fellows and informed by broader research advisory teams from multiple disciplines. These activities include the testing, demonstration and codesign of technologies () with older adults, health and care staff, and intergenerational groups through a combination of on-site and on-line methods – all recorded through a range of media including transcribed interviews, video documentation, and photography. From these, 29 activities comprise H-XR-H systems. At the point of writing, GOALD fieldwork has been completed (9 months) with a focus on user-centred design activities such as usability testing and ergonomic evaluations. ICONIC is still delivering codesign activities over an extended 15-month period, including methods such as speculative and experience design workshops and low-fidelity prototyping (Tomisch and Borthwick Citation2021) with a stronger focus on ‘doing’ and ‘making’ as mechanisms to reach creative outcomes (Sanders and Jan Stappers Citation2014). The following sections of the paper include, for illustrative purposes, quotes and references to data captured from end users. Additionally, the codesign principles outlined in this paper have grown out of our research team’s lived experiences and reflections in the field through the planning, delivery and analysis of codesign activities. This interpretive approach (Thoresen and Öhlén Citation2015) allows us to balance the data captured from (and with) end users with the views, expectations and challenges faced by our research team throughout the delivery of these projects, linking their experiences with the way data is interpreted.
Figure 3. Schedule of codesign activities throughout the GOALD and ICONIC projects, highlighting activities specifically related to H-XR-H.
3. Codesign principles for the development of digital heritage XRH
3.1. Methodological considerations
In our research, H-XR-H development involves end users as well as specialists from healthcare, technology, and design fields. Here we recognise an initial point of contention – that of developing H-XR-H from diverging disciplinary spaces, epistemologies, and value systems. To facilitate a transdisciplinary dialogue, we see H-XR-H as an ‘information ecology’ (Nardi and O’Day Citation1999), a broader and inclusive space for exchange and cocreation not necessarily restricted by disciplinary boundaries and conventions. We present, then, the collaborative design of H-XR-H as a ‘complexified’ (Greenhalgh and Papoutsi Citation2018) synthesis across design, heritage theory and practice, and health disciplines and their corresponding analytical strengths (Pershina, Soppe, and Mari Thune Citation2019), mobilising them into boundary-spanning innovation which would not be otherwise available to any particular field of specialisation (Kaplan, Milde, and Schwartz Cowan Citation2016). Moreover, an ‘information ecologies’ approach responds to the need for broader conceptualisations of health and wellbeing including social wellbeing and place-based affects, aligned with the views of Nardi and O’Day (Citation1999) on promoting more informed, place-based approaches to study the interrelationships between people and technology. As argued by O’Day (Citation2000), thinking ecologically allows us to avoid common pitfalls of technology development and assessment such as the ‘rhetoric of inevitability’ in which technology is ‘either wonderful or awful’ and instead allowing us to look for more nuanced and critical spaces of acceptance, development and feedback leading onto innovation scenarios (Wang Citation2021). By looking at technology as a multi-disciplinary, context-informed subject, we also avoid ‘partial perspectives’ which can hide the contributions and roles of different fields of research and practice, let alone the voices of end users in the health and care sector. As such, to fully engage our chosen audience and to get the desired results in terms of health and wellbeing benefits, H-XR-H must be developed in collaboration with other fields such as practice-based heritage research using established methodologies for ‘heritage interpretation’ or storytelling: without the right story for the chosen ‘audience’ woven into the digital experience, a digital reconstruction of a heritage space is devoid of meaning and users will not have an associative framework of memory or curiosity through which to engage and respond (Blockley and Hems Citation2005).
A second element to consider is that of H-XR-H design itself. Wider participation often results in a complex set of constraints, expectations, and sometimes conflicting negotiations throughout design and development processes. As opposed to the more canonical ‘problem-solution’ development paradigm, then, H-XR-H design is an ‘ill-defined problem’ - that is, indetermined challenges ‘where the information is confusing, where there are many clients and decision makers with conflicting values’ (West Citation1967). Ill-defined problems are, however, common in the creative sector, and form the basis of institutionalised forms of education (design learning) and practice (design thinking) in creative professional spaces (Buchanan Citation1992; Coyne Citation2005). While detailed guidance on H-XR-H design is limited, a creativity-based approach can help reveal new opportunities arising from collaboratively imagining and designing H-XR-H products and experiences. For instance, Mejía et al. (Citation2022) indicate that future-making approaches in multidisciplinary collaboration enables the input from both reflective (focused on past and lived experiences) and projective (focused on speculative future visions and imaginaries) information. Although this distinction has been hardly explored within healthcare and design literature (see for instance Burke and Veliz-Reyes Citation2021), it gains relevance in the development of H-XR-H in the context of user groups in rural and coastal communities often deprived of the means of envisioning futures amid socioeconomic or accessibility challenges.
On engaging with those communities of end users, our third point of consideration is that of research ‘in residence’ (Marshall Citation2014). Research in residence facilitates the translation of coproduced research outputs into impactful interventions by embedding researchers into those communities and organisations, building relationships that facilitate the coproduction of digital solutions which are sensitive to those users and directly respond to their needs and expectations (Gradinger et al. Citation2019). Both projects reported in this paper follow a research in residence approach, with a team of research fellows building relationships on-site while negotiating technological and creative directions of H-XR-H codesign (). Here, we see the emergence of a novel research profile that bridges development with implementation, technological competence and creative thinking, managing uncertainty and conflicting expectations, doing research through codesign instead of about codesign (Phillips Citation2021; Vaughan Citation2017).
Figure 4. H-XR-H codesign session in Plymouth, UK.

3.2. Place-based considerations
Projects informing this paper are both focused on ageing users in rural and coastal communities, contextualising technology development within groups often out of reach from mainstream technological discourses and innovation policies. Our consideration of this geographic inequity follows a body of research stressing the place-based nature of codesign and social innovation, and the need to contextualise it within specific societal groups and geographies – particularly with marginalised and rural groups. Social innovation has thrown ‘light on complex processes of socioeconomic and spatial restructuring (…), especially as responses to the challenges confronting marginalised rural areas’ (Georgios and Barraí Citation2021). Locally in South West England, Willis (Citation2019) stresses the need to make a ‘place’ for information and communication technologies in rural communities, ‘both metaphorically in terms of the sense of community, and literally as a particular space’ in which information and communication technologies are developed, shared and taken care of. In social innovation for health technologies, Thompson (Citation2021) discusses the geographies of digital health, and claims that it is a ‘spatial artifact’ with impacts at home and domestic scales as well as in urban-rural divides. This is supported by Enrico et al. (Citation2022) who highlight the resulting ‘sense of relatedness to others and to the environment’ which ‘is particularly crucial for the health of older people, especially in contexts where people are typically isolated from mainstream society’. Our focus on rural and coastal communities (and more specifically on sites of natural and cultural significance) considers conditions of ‘place’ on the codesign of H-XR-H both metaphorically but also logistically: we need to address challenges such as limited connectivity, or lack of existing digital infrastructures to enable these user groups to engage with these sites. It is in these ‘places’ where end users have associations with heritage sites which are valuable for their communities (some of them, from past visits), and form the basis of desired outcomes of cultural significance such as ‘pride in place’ and ‘storytelling’ developed in these sites’ geographic vicinities. As a result, attempting to reach these outcomes requires pre-empting fieldwork challenges at research design and costing stages, ensuring an optimal research delivery infrastructure including the appointment of research staff able to facilitate codesign activities on-site, consideration of portable equipment specifications (including equipment for both technology codesign and data capture) and transport budgets to access locations marginalised from main transport links. These needs are increasingly acknowledged in national research funding programmes – for example, the recent Arts and Humanities Research Council’s Design Exchange Partnership scheme has been rolled out based on ‘designers in residence’ working directly alongside communities expected to benefit from design research outputs, further emphasised by a government-funded Place-Based Research Programme (Madgin and Robson Citation2023).
3.3. Experience design and technological considerations
Literature on XR-H often focuses on technological development and it rarely addresses them from an experiential perspective. Hodge et al (Citation2018) report 5 key aspects of XR-H design for people with dementia, namely ‘(1) careful physical design, (2) making room for sharing, (3) utilizing all senses, (4) personalization, and (5) ensuring the active inclusion of the person with dementia’. The focus on shareable, bespoke and inclusive experiences reveals the need to rethink the ‘extended’ in ‘extended reality’ and the appropriate technological approaches that can result in more compelling and engaging experiences with complex layers of interaction, physical activity and perception modalities (Moinnereau, de Oliveira, and Falk Citation2022). Data from GOALD on the use of an omnidirectional treadmill in care homes reference complex technological considerations in relation to place and plausibility illusions (Slater Citation2009), with end users referring to experiences of bodily telepresence and spatial awareness, such as ‘so that social contact there (…) they may as well be in my house’, or ‘I’m scared I’ll fall over the edge’. This confirms literature indicating that multimodal approaches impact the perceived quality of the experience in areas such as realism, presence and immersion (Gougeh et al. Citation2022). All these factors require consideration in the design process of H-XR-H as individuals have different tolerances and sensorial sensitivities – even more so for older adults who may have additional sensory challenges (Stevens and Choo Citation1996). The following sub-sections detail the experience design and technological considerations of our H-XR-H development pipeline, illustrated by excerpts of data collected from project participants during our fieldwork activities.
3.3.1. Site documentation
The documentation of heritage sites requires substantial planning in consideration to anticipated modes of H-XR-H navigation and interaction. Literature supports site-specific planning requirements, with a number of publications reporting on bespoke documentation techniques that respond to specific layout, spatial or lighting conditions in heritage locations. For example, Büyüksalih et al (Citation2020) report the mapping and modelling of complex cave geometry in Istanbul, with a detailed workflow involving laser scanning. They concurrently note the challenge of finding a balance between levels of detail and the system’s ability to render complex geometries to create a ‘sense of immersion’, which is echoed by data collected from our older research participants (‘I felt like I was in the room. It seems to be high up, the room, the staircase into the long pattern on the wall and ceiling’) as well as younger participants in intergenerational groups (‘I would like to feel immersed fully and be able to look at things as you would in real life’). Our projects have used long- and short-range laser 3D scanning. In both locations, we identified unique spatial characteristics (such as height or floor textures) that required the use of 360 long-range scanning, as well as detailed material and textural qualities documented via handheld scanners (). Due to conservation constraints, access was restricted and risk assessed, with limited opportunities to return and document missing elements. To ensure accuracy, multiple scans were conducted on each site creating purposefully redundant datasets for each site.
Figure 5. (Left): handheld 3D scanning of plaster ornaments in Powderham Castle. figure 5b (right): digital model of plaster ornaments built from 3D scanned data.
In addition to the documentation of material and geometric features, to become effective heritage interpretation tools digital models need a ‘story’. Whether text, audio, image or objects, they need additional content that brings the virtual space to life and makes it engaging. At Powderham Castle our postgraduate heritage researchers conducted extensive oral history interviews with members of the Courtenay family, including the earl of Devon, about their life at Powderham, their memories and what living meant to them. The intention for future development of the Stair Hall H-XR-H is to embed audio files of these site-specific family histories into the virtual experience. Similarly, at Higher Uppacott, we are currently working with the digital games design studio, Shadowtor Studios, to develop the virtual model of the interior into an interactive game that brings the space to life as it would have been used and experienced in the medieval period through interaction with objects to performing everyday activities such as preparing food. Data from codesign activities verifies the potential benefits of storytelling media: ‘I would’ve quite liked some audio with it and explaining, say, special parts in the room or the significance or whatever. That would be really nice. But it was very good for looking around the room and seeing all the small items’.
3.3.2. Lighting, textural and spatial design
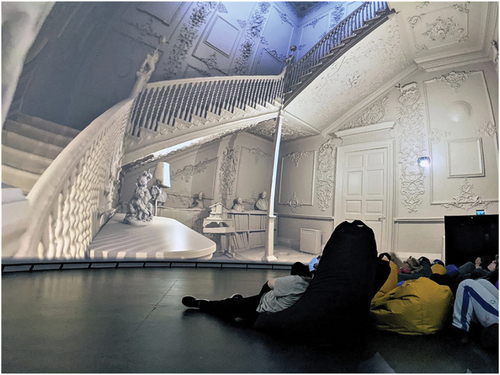
It has not been the intent to replicate these sites in virtual environments to a high degree of geometric fidelity (), but instead to create simulated spatial experiences that allow for a real-time compelling sense of presence and interaction with them (Champion Citation2021). This meant that despite inherent gaps in 3D scanned datasets (caused by hard-to-reach areas, for instance), we strived to develop an immersive experience through lighting design, textural and lighting considerations. This led to, often, a dissociation on the expected qualities of those spaces, with participants reporting (for example) that models ‘look artificial’ or ‘I tend to think that the walls cannot, in real life, be that shiny’. Moreover, these spatial qualities allowed our research team to extend the sites’ navigational opportunities through novel viewpoints and locomotion opportunities not previously anticipated, such as projection, fly-through and full-dome immersion tested with general public at the Devonport Market Hall 15 mt-diameter immersive dome as part of the research dissemination activities ().
Figure 6. Imposition of the digital model of Powderham Castle and surveying photography, showing geometric disparities.

Figure 7. Event for general audiences, showcasing the Powderham Castle inside a spherical 15 m-diameter immersive dome.
3.3.3. Locomotion
The disparity between physical spaces allocated for XR experiences and the virtual spaces, coupled with conflicting visual inputs for mobility-impaired users, such as virtual stairs, poses difficulties in implementing appropriate XR-H locomotion systems. As stated before, this is further emphasised by challenges inherent to ageing user groups which often present mobility restrictions (or are entirely restricted to care environments) and a lack of digital confidence due to self-perceived deteriorating memory. Here we have identified the creation of bespoke locomotion techniques as a key consideration for systems codesign with older adults, as well as an identifiable gap in the off-the-shelf market. This issue is exacerbated in H-XR-H, where the physical sites do not include accessibility features and adding them virtually can create authenticity conflicts. Standard controls and locomotion approaches such as teleportation were, for instance, disputed by ICONIC’s participants during the initial stages of the codesign process due to physical mobility constraints: ‘not being able to use the controls with confidence” or ‘the controls – they were not intuitive’, despite additional training and testing sessions dedicated to familiarising participants with locomotion control techniques. Although we have not identified a one-size-fits-all solution to this challenge, we have identified a gap in the market for more ergonomically adaptable control solutions for the locomotion of older adults in H-XR-H systems. This is reinforced by the recent development of a GOALD sub-study in an omnidirectional treadmill which confirms the unique ergonomic mobility requirements for older adults in a walk-on-site device, requiring further developments for deployability (H. Bradwell et al. Citation2023) that, in the voice of care home staff, can help address ‘reductions in mobility’ in older adults while ‘providing the opportunity to see the place that they love’.
3.3.4. Deployability
As indicated in the introduction, the challenges of XR-H design include a lack of consideration for external factors such as digital skills of staff operating the systems, or lack of local digital infrastructures such as connectivity. To facilitate this, our digital models are deployed via Oculus Quest 2 headsets with pre-loaded environments which, although this facilitates their use off-campus, have at times required creative solutions to bypass on-site deployability challenges such as the use of projectors on-site. To avoid these issues in future fieldwork, models have been adapted for successful real-time rendering including visualisation effects such as Bloom and Linear Fog in the Unity development platform. These techniques help mimic a sense of atmospheric ‘mood’ through visual techniques such as light glow, fog and atmospheric scattering. Furthermore, linear fog aids in providing depth perception cues, particularly in distant regions of the scene. This helps, overall, to enhance the overall sense of depth and spatial awareness in the virtual environment and helps create an impression of immersion as confirmed by our participants: ‘gave the impression of an actual visit’; ‘it does more remind me slightly about past visits’.
4. Discussion
In the United Kingdom, higher proportions of older people live in coastal regions (Stockton and Duke-Williams Citation2016). Asthana and Gibson (Citation2021) reported on the public health crisis for those communities, which can also face challenges associated with a lack of connectivity resulting in socio-economic, technological and geographic marginalisation. Additionally, the United Kingdom has complex development, testing and procurement pipelines to develop XR-H systems, with a fragmented National Health Service being the main factor limiting technology adoption and diffusion (Asthana, Jones, and Sheaff Citation2019). In that context, it is fundamental to explore ways to mobilise knowledge and coproduce technologies that work for the places and communities they are expected to benefit, while concurrently addressing challenges of marginalisation and equity.
This paper asserts that engaging and useful XR-H experiences for digital heritage, acronymised as H-XR-H, cannot be developed in isolation from the communities of users, health and care staff, and broader technological ecosystems they intend to support, and outlines a set of 10 methodological, place-based and technological considerations for H-XR-H codesign with older adults (). Among these, for example, we consider that effective H-XR-H systems must be developed within an appropriate interpretation framework, as well as in consideration to experiential aspects such as locomotion and navigational aids (where we have identified a gap in the hardware market).
Table 1. Summary of results.
More relevantly, we identify the opportunity to extrapolate these codesign principles towards broader spaces of technology development with, and for, marginalised communities. The relevance of place-based approaches, for example, has been highlighted across a range of rural and marginalised geographies which span beyond coastal communities only (Georgios and Barraí Citation2021), including contexts of global development and responsible innovation (Hartley et al. Citation2019) and emerging research agendas around placemaking and place-based feelings of pride-in-place and collective well-being (Madgin and Robson Citation2023). Similarly, a consideration of older adults in the development of technologies speaks to a more generalised need for inclusivity amid an ageing (65 or more) population expected to grow from 8% to 40.2% by 2037 in the United Kingdom (Stockton and Duke-Williams Citation2016). In the context of the South West of England, the climate emergency has been identified as an additional threat to heritage locations (Murphy, Thackray, and Wilson Citation2009), thus emphasising the need to protect, engage, and digitally archive those spaces to deliver positive health outcomes in the long-term.
To conclude, we expect this approach to help the academic community acknowledge the development opportunities of technological coproduction with marginalised communities, and emphasise the value and sense of pride that originates in places of natural and cultural significance (Svensson Citation2009). Although normally coastal communities and areas of cultural significance are marginalised from mainstream ‘levelling up’ discourses, our work indicates that place-based modes of social innovation can emerge from ‘the peripheries’ through codesigned, creative technological expressions.
Acknowledgements
This research is funded by the University of Plymouth Arts-Health Fund (2021) project “Digital asset archive of environmental models for use in navigational, VR and immersive arts and health research” and the UK Research & Innovation projects GOALD (ESRC Healthy Ageing Challenge: Social, Behavioural and Design Research Programme, grant no. ES/V016113/1), and ICONIC (EPSRC Digital Equity, grant no. EP/W024357/1). Ethical approval for these projects was secured following the University of Plymouth Research Ethics Policy, and the Faculty of Health Research Ethics and Integrity Committee. Our Arts-Health Fund project was delivered with the support from staff at Powderham Castle and Dartmoor National Park Authority, we are thankful to the Courtenay family and Emma Stockley for their support on accessing the sites. The project was delivered with assistantship from Matt Holmes, Thijs Mostert (3D scanning) and Musaab Garghouti (VR development).
On behalf of the GOALD project: University of Stirling: Catherine H. Hennessy, Alison Dawson, Gregory Mannion, Richard Haynes, Anna C. Whittaker, John Ritchie, Simone Tomaz, Karen Watchman. University of Plymouth: Sheena Asthana, Leonie Cooper, Katie Edwards, Tanja Krizaj, Alison Warren, Katherine Willis. Other co-investigators: Arunangsu Chatterjee (University of Leeds), Pete Coffee (Heriot-Watt University), Swen Gaudl (University of Gothenburg), Gemma Ryde (University of Glasgow). External partners: Active Stirling Ltd., Generations Working Together, Hearing Loss Cornwall, Nudge Community Builders, South Asian Society (Devon and Cornwall), Sporting Heritage, Sports Heritage Scotland, St. Breward Community, iSightCornwall, UKActive. On behalf of the ICONIC project: University of Plymouth: Amir Aly, Sheena Asthana, Dena Bazazian, Oksana Hagen, Kerry Howell, Emmanuel Ifeachor, Katherine Willis, Shang-Ming Zhou. External co-investigators: Arunangsu Chatterjee (University of Leeds), Swen Gaudl (University of Gothenburg), Chunxu Li (Hohai University). External partners: Centre of Pendeen, ClayTAWC, Cornwall Neighbourhoods 4 Change, Cornwall Rural Community Charity, Devon Communities Together, Geevor Tin Mine, Healthwatch Torbay, iSight Cornwall, Newquay Orchard, Nudge Community Builders, The Ocean Conservation Trust, Plymouth Community Homes, St Breward Community, and Torbay Community Development Trust.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Asthana, S., and A. Gibson. 2021. “Averting a Public Health Crisis in England’s Coastal Communities: A Call for Public Health Research and Policy.” Journal of Public Health 44 (3): 642–650. https://doi.org/10.1093/pubmed/fdab130.
- Asthana, S., R. Jones, and R. Sheaff. 2019. “Why Does the NHS Struggle to Adopt eHealth Innovations? A Review of Macro, Meso and Micro Factors.” BMC Health Services Research 19 (Article number 984). https://doi.org/10.1186/s12913-019-4790-x.
- Baker, S., J. Waycott, E. Robertson, R. Carrasco, B. Barbosa Neves, R. Hampson, and F. Vetere. 2020. “Evaluating the Use of Interactive Virtual Reality Technology with Older Adults Living in Residential Aged Care”. Information Processing & Management 57(3). Special Section on Marginalised Communities, Emerging Technologies, and Social Innovation in the Digital Age): Article 102105. https://doi.org/10.1016/j.ipm.2019.102105.
- Barton, J., R. Hine, and J. Pretty. 2009. “The Health Benefits of Walking in Greenspaces of High Natural and Heritage Value.” Journal of Integrative Environmental Sciences 6 (4): 261–278. https://doi.org/10.1080/19438150903378425.
- Blockley, M., and A. Hems. 2005. Heritage Interpretation. London: Routledge.
- Bradwell, H., L. Cooper, K. Edwards, R. Baxter, S. Tomaz, J. Ritchie, S. Gaudl, et al. 2023. “Staff Perceptions Towards Virtual Reality-Motivated Treadmill Exercise for Care Home Residents: A Qualitative Feedback Study with Key Stakeholders and Follow-Up Interview with Technology Developer.” BMJ Open 13:e073307. https://doi.org/10.1136/bmjopen-2023-073307.
- Bradwell, H., K. Jane Edwards, R. Winnington, S. Thill, V. Allgar, and R. B. Jones. 2022. “Implementing Affordable Socially Assistive Pet Robots in Care Homes Before and During the COVID-19 Pandemic: Stratified Cluster Randomized Controlled Trial and Mixed Methods Study.” JMIR Aging 5 (3): e38864. https://doi.org/10.2196/38864.
- Bradwell, H. L., K. Jane Edwards, R. Winnington, S. Thill, and R. B. Jones. 2019. “Companion Robots for Older People: Importance of User-Centred Design Demonstrated Through Observations and Focus Groups Comparing Preferences of Older People and Roboticists in South West England.” BMJ Open 9:e032468. https://doi.org/10.1136/bmjopen-2019-032468.
- Buchanan, R. 1992. “Wicked Problems in Design Thinking.” Design Issues 8 (2): 5–21. https://doi.org/10.2307/1511637.
- Burke, R. and A. Veliz Reyes. 2021. “Socio-Spatial Relationships in Design of Residential Care Homes for People Living with Dementia Diagnoses: A Grounded Theory Approach.” Architectural Science Review 66 ( 5: Design for Dementia): 391–405. https://doi.org/10.1080/00038628.2021.1941749
- Büyüksalih, G., T. Kan, G. Enç Özkan, M. Meriç, L. Isın, and T. P. Kersten. 2020. “Preserving the Knowledge of the Past Through Virtual Visits: From 3D Laser Scanning to Virtual Reality Visualisation at the Istanbul Çatalca İnceğiz Caves.” PFG – Journal of Photogrammetry, Remote Sensing and Geoinformation Science 88:133–146. https://doi.org/10.1007/s41064-020-00091-3.
- Champion, E. 2021. “Preserving Authenticity in Virtual Heritage.” In Virtual Heritage: A Guide, edited by E. Champion, 129–137. London: Ubiquity Press.
- Coyne, R. 2005. “Wicked Problems Revisited.” Design Studies 26 (1): 5–17. https://doi.org/10.1016/j.destud.2004.06.005.
- Enrico, B., S. Teasdale, O. Biosca, and D. A. Skelton. 2022. “The Health Impacts of Place-Based Creative Programmes on Older adults’ Health: A Critical Realist Review.” Health & Place 76:102839. July 2022. https://doi.org/10.1016/j.healthplace.2022.102839.
- Gallou, E. 2022. “Heritage and Pathways to Wellbeing: From Personal to Social Benefits, Between Experience Identity and Capability Shaping.” Wellbeing, Space and Society 3:100084. https://doi.org/10.1016/j.wss.2022.100084.
- Georgios, C., and H. Barraí. 2021. “Social Innovation in Rural Governance: A Comparative Case Study Across the Marginalised Rural EU.” Journal of Rural Studies 99:193–203. April 2023. https://doi.org/10.1016/j.jrurstud.2021.06.004.
- Gougeh, R. A., B. J. De Jesus, M. K. S. Lopes, M.-A. Moinnereau, W. Schubert, and T. H. Falk. 2022. “Quantifying User Behaviour in Multisensory Immersive Experiences.” IEEE International Conference on Metrology for Extended Reality, Artificial Intelligence and Neural Engineering (MetroXRAINE), Rome, Italy, 26-28 October 2022.
- Gradinger, F., J. Elston, S. Asthana, S. Martin, and R. Byng. 2019. “Reflections on the Researcher-In-Residence Model Co-Producing Knowledge for Action in an Integrated Care Organisation: A Mixed Methods Case Study Using an Impact Survey and Field Notes.” Evidence & Policy 15 (2): 197–215. https://doi.org/10.1332/174426419X15538508969850.
- Greenhalgh, T., and C. Papoutsi. 2018. “Studying Complexity in Health Services Research: Desperately Seeking an Overdue Paradigm Shift.” BMC Medicine 16 (95). https://doi.org/10.1186/s12916-018-1089-4.
- Hartley, S., C. McLeod, M. Clifford, S. Jewitt, and C. Ray. 2019. “A Retrospective Analysis of Responsible Innovation for Low-Technology Innovation in the Global South.” Journal of Responsible Innovation 6 (2): 143–162. https://doi.org/10.1080/23299460.2019.1575682.
- Hodge, J., M. Balaam, S. Hastings, and K. Morrissey. 2018. “Exploring the Design of Tailored Virtual Reality Experiences for People with Dementia.” CHI ’18: CHI Conference on Human Factors in Computing Systems, Montreal, Canada.
- Kaplan, S., J. Milde, and R. Schwartz Cowan. 2016. “Symbiont Practices in Boundary Spanning: Bridging the Cognitive and Political Divides in Interdisciplinary Research.” Academy of Management Journal 60 (4): 1387–1414. https://doi.org/10.5465/amj.2015.0809.
- Kim, S. Y. 2013. “Efficacy versus Effectiveness.” Korean Journal of Family Medicine 34 (4): 227. https://doi.org/10.4082/kjfm.2013.34.4.227.
- Lucy, J., H. Koikkalainen, L. Anderson, P. Lapok, A. Lawson, and S. D. Shenkin. 2022. “Foundation Level Barriers to the Widespread Adoption of Digital Solutions by Care Homes: Insights from Three Scottish Studies.” International Journal of Environmental Research and Public Health 19 (12): 7407. https://doi.org/10.3390/ijerph19127407.
- Madgin, R., and E. Robson. 2023. Developing a People-Centred, Place-Led Approach: The Value of the Arts and Humanities. Glasgow: University of Glasgow.
- Marasco, A., and B. Balbi. 2019. “Designing Accessible Experiences for Heritage Visitors Through Virtual Reality.” E-Review of Tourism Research 17 (3): 426–443.
- Marshall, M. 2014. “Researchers-In-Residence: A Solution to the Challenge of Evidence-Informed Improvement?” Primary Health Care Research & Development 15 (4): 337–338. https://doi.org/10.1017/S1463423614000310.
- Mejía, M., D. Henriksen, Y. Xie, A. García-Topete, R. F. Malina, and K. Jung. 2022. “From Researching to Making Futures: A Design Mindset for Transdisciplinary Collaboration.” Interdisciplinary Science Reviews 48 (1): 77–108. https://doi.org/10.1080/03080188.2022.2131086.
- Moinnereau, M.-A., A. A. de Oliveira Jr, and T. H. Falk. 2022. “Immersive Media Experience: A Survey of Existing Methods and Tools for Human Influential Factors Assessment.” Quality and User Experience 7. Article 5. https://doi.org/10.1007/s41233-022-00052-1.
- Murphy, P., D. Thackray, and E. Wilson. 2009. “Coastal Heritage and Climate Change in England: Assessing Threats and Priorities.” Conservation and Management of Archaeological Sites 11 (1): 9–15.
- Nardi, B. A., and V. L. O’Day. 1999. Information Ecologies: Using Technology with Heart. London: The MIT Press.
- O’Day, V. 2000. “Information ecologies.” The Serials Librarian 38 (1–2): 31–40. https://doi.org/10.1300/J123v38n01_05.
- Paladini, A., A. Dhanda, M. Reina Ortiz, A. Weigert, A. M. Eslam Nofal, M. Gyi, S. Su, K. Van Balen, and M. Santana Quintero. 2019. “Impact of Virtual Reality Experience on Accessibility of Cultural Heritage.” 2nd International Conference of Geomatics and Restoration (GEORES 2019), Milan, Italy.
- Pershina, R., B. Soppe, and T. Mari Thune. 2019. “Bridging Analog and Digital Expertise: Cross-Domain Collaboration and Boundary-Spanning Tools in the Creation of Digital Innovation.” Research Policy 48 (9): 103819. https://doi.org/10.1016/j.respol.2019.103819.
- Phillips, M. 2021. “The Academisation of Creativity and the Morphogenesis of the Practice-Based Researcher.” In The Routledge International Handbook of Practice-Based Research, edited by C. Vear, L. Candy, and E. Edmonds, 60–74. London: Routledge.
- Power, A., and K. Smyth. 2016. “Heritage, Health and Place: The Legacies of Local Community-Based Heritage Conservation on Social Wellbeing.” Health & Place 39:160–167. May 2016. https://doi.org/10.1016/j.healthplace.2016.04.005.
- Price, M., S. Keynes, and G. Woodhouse. 2020. Heritage, Health and Wellbeing. UK: The Heritage Alliance.
- Reilly, S., C. Nolan, and L. Monckton. 2018. Wellbeing and the Historic Environment: Threats, Issues and Opportunities for the Historic Environment. London: Historic England.
- Sanders, E. B. N., and P. Jan Stappers. 2014. “Probes, Toolkits and Prototypes: Three Approaches to Making in Codesigning.” CoDesign 10 (1): 5–14. ( CoDesigning through making). https://doi.org/10.1080/15710882.2014.888183.
- Sayma, M., R. Tuijt, C. Cooper, and K. Walters. 2020. “Are We There Yet? Immersive Virtual Reality to Improve Cognitive Function in Dementia and Mild Cognitive Impairment.” The Gerontologist 60 (7): e502–e512. https://doi.org/10.1093/geront/gnz132.
- Slater, M. 2009. “Place Illusion and Plausibility Can Lead to Realistic Behaviour in Immersive Virtual Environments.” Philosophical Transactions of the Royal Society B: Biological Sciences 364:3549–3557. https://doi.org/10.1098/rstb.2009.0138.
- Smith, N., A.-M. Towers, S. Palmer, J. Beecham, and E. Welch. 2018. “Being Occupied: Supporting ‘Meaningful Activity’ in Care Homes for Older People in England.” Ageing and Society 38 (11): 2218–2240. https://doi.org/10.1017/S0144686X17000678.
- Snoswell, A. J., and C. L. Snoswell. 2019. “Immersive Virtual Reality in Health Care: Systematic Review of Technology and Disease States.” JMIR Biomedical Engineering 4 (1): e15025. https://doi.org/10.2196/15025.
- Stevens, J. C., and K. K. Choo. 1996. “Spatial Acuity of the Body Surface Over the Life Span.” Somatosensory & Motor Research 13 (2): 153–166. https://doi.org/10.3109/08990229609051403.
- Stockton, J., and O. Duke-Williams. 2016. Geographical Maps Showing Characteristics Associated with the Ageing of the UK Population: A Report for the Government Office for Science Foresight ‘Future of an Ageing Population Project. Future of Ageing Collection. London: UK Government Office for Science.
- Svensson, E. 2009. “Consuming Nature-Producing Heritage: Aspects on Conservation, Economical Growth and Community Participation in a Forested, Sparsely Populated Area in Sweden.” International Journal of Heritage Studies 15 (6): 540–559. https://doi.org/10.1080/13527250903210837.
- Thompson, M. 2021. “The Geographies of Digital Health - Digital Therapeutic Landscapes and Mobilities.” Health & Place 70:102610. July 2021. https://doi.org/10.1016/j.healthplace.2021.102610.
- Thoresen, L., and J. Öhlén. 2015. “Lived Observations: Linking the researcher’s Personal Experiences to Knowledge Development.” Qualitative Health Research 25 (11): 1589–1598. https://doi.org/10.1177/1049732315573011.
- Tomisch, M., and M. Borthwick. 2021. Design.Think. Make. Break. Repeat. The Netherlands: BIS Publishers.
- Vaughan, L. 2017. Practice-Based Design Research. London & New York: Routledge.
- Veliz Reyes, A., M. Varga, H. Bradwell, and R. Baxter. 2023. “Unlocking Social Innovation in XR for Healthcare in Coastal Communities.” 30th IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops, Shanghai, 25-29 March.
- Wang, P. 2021. “Connecting the Parts with the Whole: Toward an Information Ecology Theory of Digital Innovation Ecosystems.” MIS Quarterly 45 (1): 397–422. https://doi.org/10.25300/MISQ/2021/15864. ( Special Issue ‘Next Generation IS Theories’)).
- West, C. 1967. “Wicked Problems.” Management Science 14 (4): B141–B142.
- Willis, K. S. 2019. “Making a ‘Place’ for ICTs in Rural Communities: The Role of Village Halls in Digital Inclusion.” C&T ’19: 9th International Conference on Communities & Technologies - Transforming Communities. Vienna, Austria. June 3–7, 2019.
- Yao, R., W. Zhang, R. Evans, G. Cao, T. Rui, and L. Shen. 2022. “Inequities in Health Care Services Caused by the Adoption of Digital Health Technologies: Scoping Review.” Journal of Medical Internet Research 24 (3): e34144. https://doi.org/10.2196/34144.