
ABSTRACT
Web-based interventions can be effective in treating depressive symptoms. Patients with risk not responding to treatment have been identified by early change patterns. This study aims to examine whether early changes are superior to baseline parameters in predicting long-term outcome. In a randomized clinical trial with 409 individuals experiencing mild to moderate depressive symptoms using the web-based intervention deprexis, three latent classes were identified (early response after registration, early response after screening and early deterioration) based on early change in the first four weeks of the intervention. Baseline variables and these classes were included in a Stepwise Cox Proportional Hazard Multiple Regression to identify predictors associated with the onset of remission over 36-months. Early change class was a significant predictor of remission over 36 months. Compared to early deterioration after screening, both early response after registration and after screening were associated with a higher likelihood of remission. In sensitivity and secondary analyses, only change class consistently emerged as a predictor of long-term outcome. Early improvement in depression symptoms predicted long-term outcome and those showing early improvement had a higher likelihood of long-term remission. These findings suggest that early changes might be a robust predictor for long-term outcome beyond baseline parameters.
Introduction
Mental disorders, especially depression, have increased considerably in recent years, with a growing number of patients registering for treatment (World Health Organization, Citation2022). Overall, there are many studies on the effectiveness of psychotherapy for depression for both face-to-face (e.g. Munder et al., Citation2019) and remote therapy, such as video therapy (Berryhill et al., Citation2019) or web-based program deprexis (Twomey et al., Citation2020). In recent years, research has increasingly focused on how therapy works and the processes of change and their relationship to outcome (e.g. Lutz, de Jong et al., Citation2021; Lutz, Deisenhofer et al., Citation2023).
One potential predictor of treatment outcome is early treatment response. Early response is defined as statistically and/or clinically significant improvements in symptoms during the initial phase of psychotherapy (Beard & Delgadillo, Citation2019). Previous studies have shown that most patient symptom change occurs in an early phase of psychotherapy (Rubel et al., Citation2015) and that early patterns of change are an important predictor of treatment outcome in face-to-face psychotherapy (Beard & Delgadillo, Citation2019; Lutz et al., Citation2014; Nordberg et al., Citation2014). Preliminary evidence also indicates the potential of early change patterns to predict outcomes in web-based interventions. For example, Schibbye et al. (Citation2014) concluded that the outcome of a CBT-oriented web-based intervention may be predicted by the assessment of early change. The studies conducted by Lutz et al. (Citation2017, Citation2019). further demonstrated that patterns of early change can predict treatment outcomes and adherence to web-based interventions. Also, in a study of the web-based self-management intervention deprexis, results indicated that patients who had a high level of initial impairment and deteriorated in the early phase of the intervention had a high likelihood of dropout (Arndt et al., Citation2020). However, a study by Fuhr et al. (Citation2022) was unable to find an impact of early change on treatment outcome. Fuhr et al. (Citation2022) examined RCT data from n = 152 patients with mild to moderate major depression, assessed weekly over a treatment period of 20 weeks. The authors noted a slow decline in symptoms after sessions four, five, six and seven until the end of treatment. However, adding early change to the model had no further effect on symptom prediction. A significant distinction between this study and the previously mentioned studies lies in the limited sample size, preventing the application of latent class analysis, as undertaken in the studies conducted by Lutz et al. (Citation2017, Citation2019). Therefore, the authors noted that it cannot be ruled out that differing symptom trajectories might have influenced later symptom change (Fuhr et al., Citation2022). Information about early change is clinically relevant to therapists as it can be used to better understand patient progress early in treatment, make treatment planning decisions and adjust the treatment strategy when deterioration occurs (Lutz et al., Citation2019, Lutz, Schwartz et al., Citation2022).
In summary, early change is a predictor of treatment outcome at treatment termination across different treatment modalities. In addition, further studies have also shown that early change is a predictor of long-term follow-up in face-to-face psychotherapy. In a sample of depressed adolescents, Renaud et al. (Citation1998) reported that individuals who had an early response to therapy had better outcomes at termination of treatment and at 1- and 2-year follow-up periods than those whose scores remained unchanged or deteriorated within the first 2 weeks of treatment. Similarly, another study by Schlagert and Hiller (Citation2017) demonstrated that early responders had significantly lower BDI scores at treatment termination and during follow-up periods after 6 and 12 months. In addition, a study conducted by Lutz et al. (Citation2009) on a sample of depressed patients showed that early change predicted outcomes at treatment termination and one and a half years after treatment ended (follow-up).
Randomized controlled trials have demonstrated the efficacy of the web-based self-management intervention deprexis (Beevers et al., Citation2017; Berger et al., Citation2011, Citation2018; Bücker et al., Citation2018; Fischer et al., Citation2015; Fuhr et al., Citation2018; Gräfe et al., Citation2020; Klein et al., Citation2016, Citation2020; Lopes et al., Citation2023; Meyer et al., Citation2009, Citation2015; Moritz et al., Citation2012; Richter et al., Citation2022; Schröder et al., Citation2014; Zwerenz et al., Citation2017, Citation2019). A meta-analysis conducted on the program showed that the intervention achieves a moderate effects size, on average (g = 0.51; Twomey et al., Citation2020). Studies also showed significant symptomatic improvements over three months (and to a lesser extent over six months) in adults with initially severe depressive symptoms (Meyer et al., Citation2015). Further studies found that deprexis was effective in the long-term up to 36 months (Humer et al., Citation2020; Kaiser et al., Citation2021). In their study on the effects of deprexis in early change on treatment outcome Lutz et al. (Citation2017) identified a total of three latent classes: Two classes of early response (n = 158, n = 185) and one class of early deterioration (n = 66). The three classes differed significantly in outcome. 62% participants of the early response after registration and 56% of the early response after screening class showed reliable change at the end of treatment, while only 27% participants of the early deterioration class showed reliable improvement. Class membership also significantly improved outcome prediction by 24.8% compared to patient intake characteristics.
To our knowledge, there are no studies that have used early change patterns to predict long-term outcome in web-based interventions. Further, there are no studies of web-based interventions with a 3-year follow-up period. Hence, this study aims to explore whether in patients with an affective disorder, long-term treatment outcome (up to 3 years after treatment) can be better predicted by early patterns of change than by baseline characteristics. Considering the summarized findings on web-based interventions and early patterns of change, we hypothesized that participants with early improvements show less severe depressive symptoms in the long term.
Methods
Study design
This study was conducted using data from the EVIDENT study, a multicenter randomized controlled trial (RCT). The trial was approved by the Ethics Committee of the German Psychological Association (DGPs SM 04_2012) and was registered with ClinicalTrials.gov (NCT01636752). For the full study protocol, see Klein et al. (Citation2013). Recruitment began in August 2012 and ended in December 2013. The last 36 months follow-up assessment was collected in December 2016. Diagnostic interviews were conducted via telephone in five centers in Germany (screening). The diagnostic interviews were conducted by trained raters. Raters were advanced university students or had a degree in psychology or medicine. The raters had received training and at least one of their audiotaped interviews and the ratings were monitored by an experienced rater (Klein et al., Citation2013). All participants were allowed to receive any form of treatment, including antidepressant medication and psychotherapy. Participants in the intervention group received access to the web-based intervention in addition to care as usual (CAU). Participants in the control group received CAU only. Based on a pragmatic design approach, CAU was not influenced by investigators. After the last follow-up, participants in the control group were offered access to the web-based intervention.
Treatment
After the screening participants had to register on the study website (registration). Participants in the intervention group were then given access to the web-based intervention deprexis (Meyer et al., Citation2009) for a period of 12 weeks. Deprexis consists of 10 modules based on a cognitive-behavioral therapy (CBT) approach with the modules presented in the form of a dialogue or chat. The content is consistent with a broadly defined CBT framework but also include elements that go beyond narrowly defined CBT (e.g. interpersonal therapy elements, positive psychology). Examples of the deprexis modules are behavioral activation, cognitive restructuring, acceptance and mindfulness, and problem-solving techniques. Each module is designed to engage users in an interactive “simulated dialogue” and provides exercises and suggestions on how to apply the strategies in everyday life. The modules include text, illustrations, and audio-based exercises. A detailed description of the program can be found in Meyer et al. (Citation2009) as well as Beevers et al. (Citation2017). In the EVIDENT study, participants with mild depression symptoms (scores between 5 and 9 on the Patient Health Questionnaire-9 [PHQ-9]; Kroenke et al., Citation2001) received deprexis without guidance, and participants with moderate depression symptoms (PHQ-9 scores between 10 and 14) received weekly email support. An e-mail program was integrated into the platform for the guided version. Participants were informed that they could write an e-mail at any time. Once a week, participants received a generic e-mail about their program usage in the previous week, the mood measurement was acknowledged, but there was no feedback about the responses made in the program by the participants or the specific therapeutic strategies they used. Therapists who provided email support were advanced university students or had a degree in psychology or medicine, received training before the start of the intervention, were supervised during the intervention, and received support with email correspondence from the supervisor when needed. No differences in outcome were found between the guided vs. non-guided version of deprexis (Berger et al., Citation2011). This is consistent with a recent trial of a modified version of deprexis, in which an unguided version was at least as effective as a therapist-supported version of the same treatment program (Gold et al., Citation2023).
Inclusion and exclusion criteria
Inclusion criteria were internet access, age between 18 and 65 years, ability to read German, willingness to participate in a diagnostic interview via telephone, a score of 5–14 on the PHQ-9 in the initial screening and written informed consent. Exclusion criteria were a lifetime diagnosis of schizophrenia or bipolar disorder or current suicidality, which were determined in the diagnostic interview. A total of n = 2020 potential participants were screened for the EVIDENT study, recruited from a variety of settings, including inpatient and outpatient medical and psychological clinics, depression internet forums, health insurance companies and the media. Participants included in the EVIDENT study (n = 1013) were randomly assigned to the intervention or the control group. For the analysis presented in this paper, only participants from the intervention group who completed at least one PHQ-9 in the first four weeks (either at week two or week four) were included, as our main focus was whether early change predicted long-term treatment outcome. Participants in the control group only completed the PHQ-9 at pre and post measurement time points and not every two weeks as the intervention group (see section below for measurement time points), therefore the control group was not included in the analyses. N = 26 of the n = 509 participants assigned to the treatment group did not register to access the intervention and n = 74 did not complete any measurements during the first four weeks. After the application of the inclusion and exclusion criteria, the final sample consisted of n = 409 participants, which is the same sample as the one used in Lutz et al. (Citation2017). For full participant flow, see .
Figure 1. Flowchart of participants.
Measurement time points
Depression symptoms and overall impairment were measured before the start of the study at screening and registration (baseline, start of treatment), every second week during 12 weeks of treatment, immediately after the study (post-treatment) and during the follow-up period (see below). The average duration between the telephone screening and registration on the deprexis website by participants was M = 10.21 (SD = 9.3) days. Full assessments were conducted at three, 6 and 12 months after randomization. In addition, monthly assessments of depressive symptoms were conducted between post-treatment and 12-month follow-up. Participants were then invited to extended follow-up assessments at 18, 24, 30 and 36 months.
Outcome measures
Demographic variables (age, gender, marital status, educational status, employment status) were recorded with non-standardized questionnaires at baseline. To assess further predictor variables and outcome, the following instruments were used.
Patient health questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., Citation2001) is a widely used, reliable and valid self-report instrument for assessing the severity of depressive symptoms. It consists of nine items which are rated on a 4-point Likert scale from 0 (“not at all”) to 3 (“almost every day”), resulting in a total severity score between 0 and 27. The internal reliability of the PHQ-9 has been found to be α = .89, and its validity has been shown in a variety of settings and populations (Kroenke et al., Citation2001).The PHQ-9 was used to measure outcome in terms of remission defined as a total score below the threshold for mild depressive symptoms (PHQ-9 < 5; Nierenberg & DeCecco, Citation2001).
Mini international neuropsychiatric interview
The Mini International Neuropsychiatric Interview (MINI; Sheehan et al., Citation1998) is a brief diagnostic interview developed for DSM-IV and ICD-10 psychiatric diagnoses. It was used to determine whether a depressive disorder was present as a predictor variable and to rule out a lifetime diagnosis of schizophrenia, bipolar disorder, and acute suicidality as exclusion criteria.
Web Screening Questionnaire
The Web Screening Questionnaire (WSQ; Donker et al., Citation2009) is a 15-item self-report instrument for disorders, particularly mood, anxiety, and alcohol problems, and was used to determine the presence of panic attacks. The WSQ has overall acceptable specificity (.44−.77) for the subscales of the respective diagnoses, good external validity, and good sensitivity (.72−1.00; Donker et al., Citation2009).
Number of sessions and total usage time
The number of sessions was defined by summing up all separate sessions of at least 10 minutes duration. Total usage time was defined as the total duration in minutes spent online using the intervention.
Statistical analysis
Analyses were conducted using IBM SPSS Statistics (Version 28.0; IBM Corp., Citation2021). Patterns of early change in depressive symptoms, measured by the PHQ-9 over the first 4 weeks of deprexis, were identified using piecewise growth mixture modeling (PGMM) using MPlus (Version 7.4; Muthén & Muthén, Citation2014). The individual variation of intercepts (initial scores) and slopes (changes) are captured using a latent class variable that is added to the growth model. This enables the identification of subpopulations of participants with similar growth curves. Cases with missing data in the PHQ-9 within the first 4 weeks were not excluded. Instead, all available data was used to estimate the growth curves within clusters. To identify patterns of early change, growth mixture models are widely used (e.g. Beard & Delgadillo, Citation2019). The applied PGMM modelled two distinct phases of change patterns, one prior to the intervention (phase 1; time between screening and registration) as well as during the intervention (phase 2; time between registration and the assessment in the fourth week after registration). A model with three latent growth factors was used: with one intercept (initial impairment) and two slopes (phase 1 and 2). The first slope loadings (change in phase 1) were fixed to 0 at screening and 1 at registration and later assessments to model the change before the intervention (phase 1). The second slope loadings (change in phase 2) were fixed to 0 for screening and registration and to the log-linear transformation (base 10) of 2 and 3 for the two following assessments to model the change in phase 2. The log-linear transformation of the factor loadings for the second slope was used as this improved the model fit compared to the linear transformation in the Bayesian information criterion (BIC; Schwarz, Citation1978; linear: 6826.981, log-linear: 6820.196). To identify the optimal number of latent trajectory classes, the BIC and the bootstrapped likelihood ratio test (BLRT; Nylund et al., Citation2007) were applied. In the first step, the model with the lowest BIC value was determined starting with a one-class model and in subsequent runs an additional class was added step by step. In the second step, the BLTR was used as an additional criterion to reduce possible overextraction of classes. From the stage where the BIC value did not decrease any further from a model with k classes to a model with k + 1 classes, this solution was tested against a solution with k-1 classes using the BLRT. If the BLRT was significant (p < .05), the model was selected as the best solution. However, if the p-value of the BLRT was not significant, the model was rejected and the solution with one class less (k-1) was tested against a model with two classes less (k-2). This process was repeated until the BLRT was significant. For the final analysis, the variances around the class-specific slopes were fixed to 0 in both phases, while the intercept variances were freely estimated but had to be constant between the classes. Hence, the heterogeneity in change had to be accounted completely by the difference in the mean slopes of the different latent classes. This forced the estimation procedure to be more sensitive to patterns of change over time than to differences in the initial level of impairment. For more details see also Lutz et al. (Citation2017).
Primary outcome
The primary analysis for the outcome reported (i.e. remission on PHQ-9) was an intention-to-treat analysis (ITT analysis), including all randomized participants (Fisher et al., Citation1990). A time-to-event analysis was conducted with the primary outcome (onset of remission) as the dependent variable and the following predictor variables: age, sex, marital status, educational status, employment status, recruitment source, baseline severity of depression (binary variable with 0 = mild versus 1 = moderate on the PHQ-9), baseline diagnosis of depression (MINI), baseline diagnosis of dysthymia (MINI), self-reported number of previous depressive episodes, self-reported presence of panic attacks (WSQ), concurrent psychiatric care, concurrent psychotherapy, number of sessions, total usage time, and early change latent class. Class membership was included in the analyses as a categorical variable with three categories. Participants who did not achieve remission within 36 months or dropped out were censored. Stepwise Cox Proportional Hazards Multiple Regression was used to determine which set of predictor variables was statistically associated with the onset of remission over 36 months (Cox, Citation1972). Tolerance levels of .25 and higher indicated that none of the predictors was too highly correlated with the other predictors to be entered into the multiple regression. Hazard ratios were calculated for each predictor that was retained in the final model.
Sensitivity analyses
Sensitivity analyses were conducted to determine the robustness of our results. In the first sensitivity analysis, all above-described variables were entered into the Cox Regression simultaneously instead of stepwise. Our second sensitivity analysis examined the impact of missing data. We used imputation to estimate missing scores by evaluating the relationships between observed and missing scores as well as baseline scores. Missing monthly rating scores were imputed via the R package missForst version 1.4 (Stekhoven & Bühlmann, Citation2012). MissForest uses random forest to impute missing values and can handle continuous and categorial data in addition to nonlinear associations and interactions.
Secondary analysis
We used Linear Mixed Models (LMM) with an autoregressive heterogeneous covariance structure (AR1) adjusted for baseline severity to analyze the association of the above-mentioned predictors with PHQ-9 change from baseline to 36 months follow-up. In the LMMs, time (level 1) was nested in patients (level 2). Time in months was used as a within-group factor on level 1, with the early deterioration class as the reference group to model change in PHQ-9. All variables that served as predictors in the Stepwise Cox Proportional Hazards Multiple Regression described above were entered into the model as fixed effects on level 2.
Results
Participant characteristics
Participants were on average M = 43.15 (SD = 11.10, Range = 18 − 65) years old and 70.2% (n = 287) were female. 49.9% (n = 204) of participants had a high school diploma that would allow them to study at a university. 62.1% (n = 254) of participants were married or in a stable partnership and 23.72% (n = 97) were in employment. 68.22% (n = 279) met the criteria for panic attacks in the WSQ. 70.66% (n = 289) of participants reported not having received psychiatric treatment and 62.35% (n = 255) reported not having received psychotherapeutic treatment. Most participants (47.4%; n = 194) were recruited through the internet or other media, 26.2% (n = 107) through insurance companies, 15.2% (n = 62) through internet forums and 11.2% (n = 46) through clinics. 19.3% (n = 79) of participants reported having had one depressive episode to their lifetime, 40.6% (n = 166) reported having had between two and five episodes to their lifetime, and 40.1% (n = 164) had more than six depressive episodes in their lifetime. Interviewed via the MINI, 69.4% (n = 284) met the criteria for current major depression and 63.4% (n = 260) for dysthymia. On average, participants used deprexis for M = 473.12 (SD = 288.62, Range = 60−2510) minutes and the average number of deprexis sessions was M = 9.1 (SD = 4.38, Range = 1 − 30). 64.5% (n = 264) of participants suffered from moderate depression (PHQ ≥10) and received weekly brief email support in addition to the web-intervention. The number of participants who received email support during the web-based intervention differed significantly between the classes (p < .001). In the early response after registration 96.2% (152/158), in the early response after screening 31% (57/185) and in the early deterioration class 83% (55/66) scored above the cut-off at 10 on the PHQ-9 at screening.
Patterns of early change
The three-class solution showed the best model fit as suggested by the BIC and BLTR (for 2 classes BIC = 6782.91, BLTR < .001; for 3 classes BIC = 6773.41 BLTR < .001; 4 classes BIC = 6777.33 BLTR < .001).
The first subgroup (early response after registration; n = 158), had a rapid early decrease in depressive symptoms after registration (phase 2). The effect size of the early change during phase 1 and 2 was d = 1.35. In the second subgroup (early response after screening; n = 185) depressive symptoms decreased significantly in phase 1 and 2. The early response effect size within this latent class was d = 0.98. The third subgroup (early deterioration; n = 66) showed a significant increase in depressive symptoms in phase 1 and phase 2 with a negative effect size for early change d = −1.78. For a graphical visualization of the latent classes, see .
Figure 2. Latent classes for the mean latent growth curves of the piecewise growth mixture modeling (PGMM).
Primary outcome
In the Stepwise Cox Proportional Hazards Multiple Regression, the early change class was entered first (χ22 = 59.053; p < .001), and number of sessions was entered next (χ23 = 77.787 p < .001). In the second and final model, a higher number of sessions was associated with a higher likelihood of remission (HR = 1.065; 95% CI 1.036–1.095; p < .001). Compared to those belonging to the “early deterioration” latent class, membership in the “early response after registration” and “early response after screening” classes was associated with a higher likelihood of remission over 36 months (HR = 2.013; 95% CI 1.149–3.527; p = .015 for “early response after registration” and HR = 5.131; 95% CI 2.993–8.797; p < .001 for “early response after screening”). For detailed remission rates, see and for a graphical visualization, see .
Figure 3. Kaplan-Meier estimates of the duration of depressive symptoms until first remission.
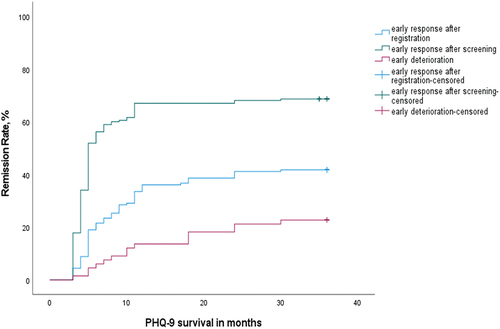
Table 1. Cumulated remission rates in the PHQ-9 over the long-term symptom course in months for the latent classes.
Sensitivity analyses
We performed sensitivity analyses to determine the robustness of our primary outcome results. Firstly, when entering all variables into the Cox Regression simultaneously instead of stepwise as in the main analysis, the same pattern of results emerged. Secondly, we reran the Stepwise Cox Proportional Hazards Multiple Regression after replacing the missing values using imputation. In this model, concurrent psychotherapy (HR = 1.365; 95% CI 1.027–1.814; p = .032) and a greater number of sessions were associated with a higher likelihood of remission (HR = 1.053; 95% CI 1.026–1.081; p < .001); and again, compared to those belonging to the “early deterioration” latent class, membership in the “early response after registration” and “early response after screening” classes was associated with a higher likelihood of remission over 36 months (HR = 2.139; 95% CI 1.223–3.739; p = .008 for “early response after registration” and HR = 5.074; 95% CI 2.963–8.689; p < .001 for “early response after screening”).
Secondary outcome
Based on the LMM analysis, the following variables had a significant effect on PHQ-9 change over 36 months: baseline severity of depressive symptoms (F1,116 = 11.12, p < .001), comorbid panic attacks (F1,124 = 5.76, p = .018) and early change class (F2,122 = 15.05, p < .001). Higher baseline severity, the absence of comorbid panic attacks, and belonging to the early deterioration class were each associated with a smaller decrease in depressive symptoms. All other variables had no significant effects on PHQ-9 change over time. For detailed information on the significant variables, see .
Table 2. Variables with a significant effect on PHQ-9 change over 36 months.
Discussion
The present study investigated whether early changes in depression symptoms predicted long-term treatment outcomes for individuals receiving a web-based cognitive-behavioral intervention for depression (deprexis). Early change was identified as a significant predictor of long-term outcome beyond various baseline parameters. Specifically, individuals who experienced early improvements of depression symptoms were more likely to achieve and remain in remission for up to 36 months after treatment. In contrast, individuals who experienced early deterioration of depression symptoms were less likely to achieve remission. This study’s findings are consistent with previous research that has highlighted the importance of early changes in depression symptoms for predicting treatment outcomes (Lutz, de Jong et al., Citation2021). Early improvements in depression symptoms have been found to be associated with better treatment outcomes across web-based interventions (Lutz et al., Citation2017) and face-to-face psychotherapy (Beard & Delgadillo, Citation2019). Furthermore, early changes have already been identified as factors that account for variances in treatment outcome, surpassing the influence of baseline parameters (Lutz et al., Citation2017). The present study extends this research by demonstrating that early changes in depression symptoms are also predictive of long-term outcomes for individuals receiving web-based cognitive-behavioral interventions for depression. The remission rates over three years, when compared across the three latent classes, indicate that only 22.7% of patients with early deterioration after screening showed remission. This means that only one out of five people showed remission after three years. In comparison, twice as many people in the early response after registration class (41.8%) and three times as many people in the early response after screening class (68.6%) showed remission three years after the web-based self-management intervention. But in the pattern of patients who showed improvement after screening, meaning prior to the intervention, it may also be possible that the observed effect is based in part on hope and positive treatment expectations, which may also have a positive effect on treatment outcome. The therapeutic contact made during screening might already be relieving and lead to further positive treatment expectations (Constantino, Citation2012; Swift & Derthick, Citation2013). This would not limit the significance of early changes for treatment outcomes in follow-up assessments, but could indicate that web-based interventions such as deprexis can induce hope and positive treatment expectations too and patients undergoing web-based treatments can also maintain these early changes throughout treatment and even until the follow-up assessment.
In addition, these results suggest that early changes may be robust predictors of long-term outcome beyond baseline characteristics and support the findings of Hammelrath et al. (Citation2023), who showed in their study that therapeutic alliance and early symptom change constituted the most important predictors, whereas in comparison, models trained on baseline data were not significantly better. The authors concluded that fair accuracies could only be achieved by including information from early treatment phases.
Overall, early feedback on progress or deterioration during the treatment process is clinically important, as this information allows decisions to be made about further treatment planning or the adaptation of interventions (e.g. Lutz, Schwartz, et al., Citation2022). However, we must also consider that while psychotherapy is effective in treating depression compared to a control group, still about more than 50% of patients who receive therapy do not respond to it (Cuijpers et al., Citation2021). Therefore, the authors argue that more effective treatment strategies such as sequencing and combining treatments are needed (Cuijpers et al., Citation2021). Lutz et al. (Citation2015) also argue that the identification of early deterioration and outcome measures during the course of treatment can be used as an indicator if treatment needs to be adapted or the treatment dosage should be increased. Regarding web-based programs, patients who deteriorate early in these programs could be offered further treatment following the web-based intervention as these patients had significantly lower long-term remission rates than those who improved early during the web-based self-management intervention. These patients also had a worse treatment outcome at termination than patients with early response and in addition showed no improvement in depressive symptoms at the end of treatment (Lutz et al., Citation2017). Therefore, patients who show early deterioration or no improvement may benefit from longer and/or more intensive treatment beyond the web-based intervention, whereas for patients who show early improvement, the self-help program may be sufficient. However, it is also possible that a web-based intervention was not the appropriate modality for the patients who deteriorated early in the intervention. Furthermore, individuals who did not show early improvement may not have responded to other interventions, regardless of type or dosage (e.g. never responders). The significant difference in long-term remission rates between the three change classes underlines the potential of basing personalized treatment plans on early response patterns. Thus, given the increasing integration of technology into psychotherapeutic care, i.e. feedback systems (Barkham et al., Citation2023) or remote therapy (Lutz, Edelbluth, et al., Citation2021), it is important to understand how web-based interventions such as deprexis can potentially be used to extend traditional psychotherapy, thus either reducing the demands on healthcare systems or bridging waiting periods for face-to-face psychotherapy. Investigating whether early change or early deterioration in a prior web-based intervention predicts the outcome of subsequent face-to-face therapy could serve as the basis for a stepped care model. Such an approach could enhance personalized treatment planning by integrating different psychotherapy modalities.
Strengths, limitations, and future directions
This study has notable strengths, but also several limitations. One of the strengths of the present study is its large sample size, which increases the generalizability of the findings. Additionally, the inclusion criteria of the study were broad and the recruitment of participants in clinical as well as community settings allows for better generalizability of the results. Another major strength of the study is the long follow-up period of three years. However, the study is not without limitations. One limitation is that it only included individuals who completed at least one PHQ-9 in the first four weeks of treatment, which may have introduced selection bias. Additionally, the study did not assess the quality or adherence to the web-based cognitive-behavioral intervention, which may have influenced treatment outcomes. Also, the study only included individuals who were able to read German, which may limit the generalizability of the findings. Another limitation regarding the generalizability is that only participants with mild to moderate depression severity were included, therefore the results may not be valid for individuals with severe depressive symptoms. An additional limitation that was not considered in the analyses is the level of the institution, as we only considered the 2-level structure of time points nested in patients. In recent studies, there is evidence that there is an institution effect of approximately 2% (Firth et al., Citation2019). Since the therapeutic contact in web-based interventions is none to low and the contact in our study (telephone screening and email contact for the patients with moderate depression scores at screening) was done by trained research team members, the impact on the treatment outcome, especially on the long-term outcome, should be very low, since there was no “therapeutic contact” after the intervention ended and this contact beforehand has been very general and has not addressed specific interventions. Furthermore, as no control group was included in the analyses, it is unknown whether the observed effects might have occurred similarly if there had been no or a different treatment. Moreover, it is important to mention that over the course of the very long follow-up phase of three years, there were decreasing numbers of respondents completing assessments. Due to the missing values, we performed a sensitivity analysis with multiple imputations and showed that early change was a robust predictor of long-term treatment outcome. Lastly, it is important to consider the use of latent class analyses for assessing early change patterns with caution, as it represents a simplification of a more complex reality and comes with potential drawbacks, such as the risk of specification errors (e.g. Bauer, Citation2008, Citation2011; Nagin & Odgers, Citation2010). However, early patterns of change may also be the result of regression to the mean. The inclusion of the pre-treatment phase should be investigated in further studies. Despite these limitations, the present study has important clinical implications. The findings suggest that early changes in depression symptoms can be used to identify individuals who are at risk for poor treatment outcomes and who may require additional or alternative interventions. Future research could examine patient and process variables that are associated with early response. For face-to-face therapy, the attunement between patient and therapist seems to be indicative of early improvements in severely impaired patients (Schwartz et al., Citation2022). However, as patient-therapist attunement plays no role in web-based self-help programs, other variables relevant to such programs and associated with early changes should be identified. Additionally, more research on the long-term effectiveness of web-based interventions is necessary to consolidate and replicate this study’s findings and identify further predictors beyond early response.
Conclusions
The present study provides further support for the importance of early changes in depression symptoms for the prediction of long-term treatment outcomes for individuals receiving web-based cognitive-behavioral interventions for depression. Therefore, this study contributes to the existing literature and extends its findings by demonstrating that early change not only serves as a reliable predictor of treatment outcomes but can also predict long-term treatment effects. If replicated, such findings could be used to provide feedback to therapists for the purpose of tailoring treatments and monitoring therapeutic processes (Lutz, Deisenhofer, et al., Citation2022).
Acknowledgments
The authors wish to thank GAIA AG (Hamburg, Germany), which provided technical support and made the internet intervention (deprexis) available at no cost to participants in the trial. The complete list study team members includes: Sandra Nolte, Matthias Rose (local principal investigator), Anna Paulitschek, Leonie Gmöhling, Leonie Schickedanz; Berlin. Thomas Berger, Bern. Viola Gräfe, Wolfgang Greiner (local principal investigator); Bielefeld. Mirja Behrens, Cecile Hoermann, Anna J. Katharina Jahns, Thies Lüdke, Björn Meyer, Steffen Moritz (local principal investigator), Johanna Schröder, Amit Gulati, Eik Vettorazzi; Hamburg. Carla Gamon, Fritz Hogan, Martin Kolbe, Jan Philipp Klein (local principal investigator), Antje Roniger, Christina Späth; Lübeck. Alice Arndt, Liv Glindemann, Wolfgang Lutz (local principal investigator), David Rosenbaum, Kathinka Wolter; Trier. Flora Bach, Elisabeth Beck, Kristina Fuhr, Martin Hautzinger (local principal investigator), Katharina Krisch, Melanie Wahl; Tübingen.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Arndt, A., Lutz, W., Rubel, J., Berger, T., Meyer, B., Schröder, J., Späth, C., Hautzinger, M., Fuhr, K., Rose, M., Hohagen, F., Klein, J. P., & Moritz, S. (2020). Identifying change-dropout patterns during an internet-based intervention for depression by applying the Muthen-Roy model. Cognitive Behaviour Therapy, 49(1), 22–40. https://doi.org/10.1080/16506073.2018.1556331
- Barkham, M., de Jong, K., Delgadillo, J., & Lutz, W. (2023). Routine outcome monitoring (ROM) and feedback: Research review and recommendations. Psychotherapy Research, 33(7), 841–855. https://doi.org/10.1080/10503307.2023.2181114
- Bauer, D. J. (2008). Observations on the use of growth mixture models in psychological research. Multivariate Behavioral Research, 42(4), 757–786. https://doi.org/10.1080/00273170701710338
- Bauer, D. J. (2011). Evaluating individual differences in psychological processes. Current Directions in Psychological Science, 20(2), 115–118. https://doi.org/10.1177/0963721411402670
- Beard, J. I. L., & Delgadillo, J. (2019). Early response to psychological therapy as a predictor of depression and anxiety treatment outcomes: A systematic review and meta-analysis. Depression and Anxiety, 36(9), 866–878. https://doi.org/10.1002/da.22931
- Beevers, C. G., Pearson, R., Hoffman, J. S., Foulser, A. A., Shumake, J., & Meyer, B. (2017). Effectiveness of an internet intervention (deprexis) for depression in a united states adult sample: A parallel-group pragmatic randomized controlled trial. Journal of Consulting and Clinical Psychology, 85(4), 367–380. https://doi.org/10.1037/ccp0000171
- Berger, T., Hämmerli, K., Gubser, N., Andersson, G., & Caspar, F. (2011). Internet-based treatment of depression: A randomized controlled trial comparing guided with unguided self-help. Cognitive Behaviour Therapy, 40(4), 251–266. https://doi.org/10.1080/16506073.2011.616531
- Berger, T., Krieger, T., Sude, K., Meyer, B., & Maercker, A. (2018). Evaluating an e-mental health program (“deprexis”) as adjunctive treatment tool in psychotherapy for depression: Results of a pragmatic randomized controlled trial. Journal of Affective Disorders, 227, 455–462. https://doi.org/10.1016/j.jad.2017.11.021
- Berryhill, M. B., Culmer, N., Williams, N., Halli-Tierney, A., Betancourt, A., Roberts, H., & King, M. (2019). Videoconferencing psychotherapy and depression: A systematic review. Telemedicine and E-Health, 25(6), 435–446. https://doi.org/10.1089/tmj.2018.0058
- Bücker, L., Bierbrodt, J., Hand, I., Wittekind, C., Moritz, S., & van Wouwe, J. P. (2018). Effects of a depression-focused internet intervention in slot machine gamblers: A randomized controlled trial. Public Library of Science ONE, 13(6), e0198859. https://doi.org/10.1371/journal.pone.0198859
- Constantino, M. J. (2012). Believing is seeing: An evolving research program on patients’ psychotherapy expectations. Psychotherapy Research, 22(2), 127–138. https://doi.org/10.1080/10503307.2012.663512
- Cox, D. R. (1972). Regression models and life‐tables (with discussion). Journal of the Royal Statistical Society: Series B (Methodological), 34(2), 187–202. https://doi.org/10.1111/j.2517-6161.1972.tb00899.x
- Cuijpers, P., Karyotaki, E., Ciharova, M., Miguel, C., Noma, H., & Furukawa, T. A. (2021). The effects of psychotherapies for depression on response, remission, reliable change, and deterioration: A meta‐analysis. Acta Psychiatrica Scandinavica, 144(3), 288–299. https://doi.org/10.1111/acps.13335
- Donker, T., van Straten, A., Marks, I., & Cuijpers, P. (2009). A brief web-based screening questionnaire for common mental disorders: Development and validation. Journal of Medical Internet Research, 11(3), e19. https://doi.org/10.2196/jmir.1134
- Firth, N., Saxon, D., Stiles, W. B., & Barkham, M. (2019). Therapist and clinic effects in psychotherapy: A three-level model of outcome variability. Journal of Consulting and Clinical Psychology, 87(4), 345–356. https://doi.org/10.1037/ccp0000388
- Fischer, A., Schröder, J., Vettorazzi, E., Wolf, O. T., Pöttgen, J., Lau, S., Heesen, C., Moritz, S., & Gold, S. M. (2015). An online programme to reduce depression in patients with multiple sclerosis: A randomised controlled trial. The Lancet Psychiatry, 2(3), 217–223. https://doi.org/10.1016/S2215-0366(14)00049-2
- Fisher, L. D., Dixon, D. O., Herson, J., Frankowski, R. K., Hearron, M. S., & Peace, K. E. (1990). Intention to treat in clinical trials. In K. E. Peace (Ed.), Statistical issues in drug research and development (pp. 331–350). Marcel Dekker.
- Fuhr, K., Schröder, J., Berger, T., Moritz, S., Meyer, B., Lutz, W., Hohagen, F., Hautzinger, M., & Klein, J. P. (2018). The association between adherence and outcome in an internet intervention for depression. Journal of Affective Disorders, 229, 443–449. https://doi.org/10.1016/j.jad.2017.12.028
- Fuhr, K., Werle, D., & Batra, A. (2022). How does early symptom change predict subsequent course of depressive symptoms during psychotherapy? Psychology and Psychotherapy, 95(1), 137–154. https://doi.org/10.1111/papt.12370
- Gold, S. M., Friede, T., Meyer, B., Moss-Morris, R., Hudson, J., Asseyer, S., Bellmann-Strobl, J., Leisdon, A., Ißels, L., Ritter, K., Schymainski, D., Pomeroy, H., Lynch, S. G., Cozart, J. S., Thelen, J., Román, C. A. F., Cadden, M., Guty, E., Lau, S., Pöttgen, J., et al. (2023). Internet-delivered cognitive behavioural therapy programme to reduce depressive symptoms in patients with multiple sclerosis: A multicentre, randomised, controlled, phase 3 trial. Lancet Digital Health, 5(10), e668–e678. https://doi.org/10.1016/S2589-7500(23)00109-7
- Gräfe, V., Moritz, S., & Greiner, W. (2020). Health economic evaluation of an internet intervention for depression (deprexis), a randomized controlled trial. Health Economics Review, 10(1), 1–11. https://doi.org/10.1186/s13561-020-00273-0
- Hammelrath, L., Hilbert, K., Heinrich, M., Zagorscak, P., & Knaevelsrud, C. (2023). Select or adjust? How information from early treatment stages boosts the prediction of non-response in internet-based depression treatment. Psychological Medicine, 54(8), 1641–1650. https://doi.org/10.1017/S0033291723003537
- Humer, E., Kocsis-Bogar, K., Berger, T., Schröder, J., Späth, C., Meyer, B., Moritz, S., Lutz, W., Probst, T., & Klein, J. P. (2020). A comparison of the three year course between chronic depression and depression with multiple vs. few prior episodes. Psychiatry Research, 291, 113235. https://doi.org/10.1016/j.psychres.2020.113235
- IBM Corp. (2021). IBM SPSS statistics for windows (Version 28.0) [ Computer software]. IBM Corp.
- Kaiser, T., Boschloo, L., Berger, T., Meyer, B., Späth-Nellissen, C., Schröder, J., Hohagen, F., Moritz, S., & Klein, J. P. (2021). Maintaining outcomes of internet-delivered cognitive-behavioral therapy for depression: A network analysis of follow-up effects. Frontiers in Psychiatry, 12, 598317. https://doi.org/10.3389/fpsyt.2021.598317
- Klein, J. P., Barthel, B., Berger, T., & Moritz, S. (2020). Feasibility, effectiveness and safety of the self-management intervention deprexis in routine medical care: Results of an uncontrolled observational study. Internet Interventions, 22, 100341. https://doi.org/10.1016/j.invent.2020.100341
- Klein, J. P., Berger, T., Schröder, J., Späth, C., Meyer, B., Caspar, F., Lutz, W., Arndt, A., Greiner, W., Gräfe, V., Hautzinger, M., Fuhr, K., Rose, M., Nolte, S., Löwe, B., Anderssoni, G., Vettorazzi, E., Moritz, S., & Hohagen, F. (2016). Effects of a psychological internet intervention in the treatment of mild to moderate depressive symptoms: Results of the EVIDENT study, a randomized controlled trial. Psychotherapy and Psychosomatics, 85(4), 218–228. https://doi.org/10.1159/000445355
- Klein, J. P., Berger, T., Schröder, J., Späth, C., Meyer, M., Caspar, F., Lutz, W., Greiner, W., Hautzinger, M., Rose, M., Gräfe, V., Hohagen, F., Andersson, G., Vettorazzi, E., & Moritz, S. (2013). The EVIDENT-trial: Protocol and rationale of a multicenter randomized controlled trial testing the effectiveness of an online-based psychological intervention. BMC Psychiatry, 13(1), 239. https://doi.org/10.1186/1471-244X-13-239
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
- Lopes, R. T., da Rocha, G. C., Svacina, M. A., Meyer, B., Šipka, D., & Berger, T. (2023). Effectiveness of an internet-based self-guided program to treat depression in a sample of Brazilian users: Randomized controlled trial. JMIR Formative Research, 7(1), e46326. https://doi.org/10.2196/46326
- Lutz, W., Arndt, A., Rubel, J., Berger, T., Schröder, J., Späth, C., Meyer, B., Greiner, W., Gräfe, V., Hautzinger, M., Fuhr, K., Rose, M., Nolte, S., Löwe, B., Hohagen, F., Klein, J. P., & Moritz, S. (2017). Defining and predicting patterns of early response in a web-based intervention for depression. Journal of Medical Internet Research, 19(6), e206. https://doi.org/10.2196/jmir.7367
- Lutz, W., Deisenhofer, A. K., Rubel, J., Bennemann, B., Giesemann, J., Poster, K., & Schwartz, B. (2022). Prospective evaluation of a clinical decision support system in psychological therapy. Journal of Consulting and Clinical Psychology, 90(1), 90. https://doi.org/10.1037/ccp0000642
- Lutz, W., Deisenhofer, A.-K., Weinmann-Lutz, B., & Barkham, M. (2023). Data-informed clinical training and practice. In L. G. Castonguay & C. E. Hill (Eds.), Training in psychotherapy: Learning, improving, and supervising therapeutic skills (pp. 191–213). American Psychological Association. https://doi.org/10.1037/0000364-010
- Lutz, W., de Jong, K., & Rubel, J. (2015). Patient-focused and feedback research in psychotherapy: Where are we and where do we want to go? Psychotherapy Research, 25(6), 625–632. https://doi.org/10.1080/10503307.2015.1079661
- Lutz, W., de Jong, K., Rubel, J. A., & Delgadillo, J. (2021). Measuring, predicting, and tracking change in psychotherapy. In M. Barkham, W. Lutz, & L. G. Castonguay (Eds.), Bergin and Garfield’s handbook of psychotherapy and behavior change: 50th anniversary edition (pp. 89–133). John Wiley & Sons, Inc.
- Lutz, W., Edelbluth, S., Deisenhofer, A.-K., Delgadillo, J., Moggia, D., Prinz, J., & Schwartz, B. (2021). The impact of switching from face-to-face to remote psychological therapy during the COVID-19 pandemic. Psychotherapy and Psychosomatics, 90(4), 285–286. https://doi.org/10.1159/000515543
- Lutz, W., Hofmann, S. G., Rubel, J., Boswell, J. F., Shear, M. K., Gorman, J. M., Woods, S. W., & Barlow, D. H. (2014). Patterns of early change and their relationship to outcome and early treatment termination in patients with panic disorder. Journal of Consulting and Clinical Psychology, 82(2), 287–297. https://doi.org/10.1037/a0035535
- Lutz, W., Rubel, J., Schwartz, B., Schilling, V., & Deisenhofer, A. (2019). Towards integrating personalized feedback research into clinical practice: Development of the Trier Treatment Navigator (TTN). Behaviour Research and Therapy, 120, 103438. https://doi.org/10.2016/j.brat.2019.103438
- Lutz, W., Schwartz, B., & Delgadillo, J. (2022). Measurement-based and data-informed psychological therapy. Annual Review of Clinical Psychology, 18(1), 71–98. https://doi.org/10.1146/annurev-clinpsy-071720-014821
- Lutz, W., Stulz, N., & Köck, K. (2009). Patterns of early change and their relationship to outcome and follow-up among patients with major depressive disorders. Journal of Affective Disorders, 118(1–3), 60–68. https://doi.org/10.1016/j.jad.2009.01.019
- Meyer, B., Berger, T., Caspar, F., Beevers, C. G., Andersson, G., & Weiss, M. (2009). Effectiveness of a novel integrative online treatment for depression (deprexis): Randomized controlled trial. Journal of Medical Internet Research, 11(2), e15. https://doi.org/10.2196/jmir.1151
- Meyer, B., Bierbrodt, J., Schröder, J., Berger, T., Beevers, C. G., Weiss, M., Jacob, G., Späth, C., Andersson, G., Lutz, W., Hautzinger, M., Löwe, B., Rose, M., Hohagen, F., Caspar, F., Greiner, W., Moritz, S., & Klein, J. P. (2015). Effects of an internet intervention (deprexis) on severe depression symptoms: Randomized controlled trial. Internet Interventions, 2(1), 48–59. https://doi.org/10.1016/j.invent.2014.12.003
- Moritz, S., Schilling, L., Hauschildt, M., Schröder, J., & Treszl, A. (2012). A randomized controlled trial of internet-based therapy in depression. Behaviour Research and Therapy, 50(7–8), 513–521. https://doi.org/10.1016/j.brat.2012.04.006
- Munder, T., Flückiger, C., Leichsenring, F., Abbass, A. A., Hilsenroth, M. J., Luyten, P., Rabung, S., Steinert, C., & Wampold, B. E. (2019). Is psychotherapy effective? A re-analysis of treatments for depression. Epidemiology and Psychiatric Sciences, 28(3), 268–274. https://doi.org/10.1017/S2045796018000355
- Muthén, L. K., & Muthén, B. O. (2014). MPLUS (Version 7.4.) [ Computer software]. Muthén & Muthén.
- Nagin, D. S., & Odgers, C. L. (2010). Group-based trajectory modeling in clinical research. Annual Review of Clinical Psychology, 6(1), 109–138. https://doi.org/10.1146/annurev.clinpsy.121208.131413
- Nierenberg, A. A., & DeCecco, L. M. (2001). Definitions of antidepressant treatment response, remission, nonresponse, partial response, and other relevant outcomes: A focus on treatment-resistant depression. The Journal of Clinical Psychiatry, 62 Suppl 16, 5–9.
- Nordberg, S. S., Castonguay, L. G., Fisher, A. J., Boswell, J. F., & Kraus, D. (2014). Validating the rapid responder construct within a practice research network. Journal of Clinical Psychology, 70(9), 886–903. https://doi.org/10.1002/jclp.22077
- Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A monte carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569. https://doi.org/10.1080/10705510701575396
- Renaud, J., Brent, D. A., Baugher, M., Birmaher, B., Kolko, D. J., & Bridge, J. (1998). Rapid response to psychosocial treatment for adolescent depression: A two-year follow-up. Journal of the American Academy of Child & Adolescent Psychiatry, 37(11), 1184–1190. https://doi.org/10.1097/00004583-199811000-00019
- Richter, L. E., Machleit-Ebner, A., Scherbaum, N., & Bonnet, U. (2022). How effective is a web-based mental health intervention (Deprexis) in the treatment of moderate and major depressive disorders when started during routine psychiatric inpatient treatment as an adjunct therapy? A pragmatic parallel-group randomized controlled trial. Fortschritte der Neurologie· Psychiatrie. https://doi.org/10.1055/a-1826-2888
- Rubel J, Lutz W, Kopta S Mark, Köck K, Minami T, Zimmermann D and Saunders S M. (2015). Defining early positive response to psychotherapy: An empirical comparison between clinically significant change criteria and growth mixture modeling. Psychological Assessment, 27(2), 478–488. 10.1037/pas0000060
- Schibbye, P., Ghaderi, A., Ljótsson, B., Hedman, E., Lindefors, N., Rück, C., Kaldo, V., & Chen, K. (2014). Using early change to predict outcome in cognitive behaviour therapy: Exploring timeframe, calculation method, and differences of disorder-specific versus general measures. Public Library of Science ONE, 9(6), e100614. https://doi.org/10.1371/journal.pone.0100614
- Schlagert, H. S., & Hiller, W. (2017). The predictive value of early response in patients with depressive disorders. Psychotherapy Research, 27(4), 488–500. https://doi.org/10.1080/10503307.2015.1119329
- Schröder, J., Brückner, K., Fischer, A., Lindenau, M., Köther, U., Vettorazzi, E., & Moritz, S. (2014). Efficacy of a psychological online intervention for depression in people with epilepsy: A randomized controlled trial. Epilepsia, 55(12), 2069–2076. https://doi.org/10.1111/epi.12833
- Schwartz, B., Rubel, J. A., Deisenhofer, A.-K., & Lutz, W. (2022). Movement-based patient-therapist attunement in psychological therapy and its association with early change. Digital Health, 8, 205520762211290. https://doi.org/10.1177/20552076221129098
- Schwarz, G. (1978). Estimating the dimension of a model. The Annals of Statistics, 6(2), 461–464. https://doi.org/10.1214/aos/1176344136
- Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R., & Dunbar, G. C. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59 Suppl 20, 22–57.
- Stekhoven, D. J., & Bühlmann, P. (2012). Missforest–non-parametric missing value imputation for mixed-type data. Bioinformatics (Oxford, England), 28(1), 112–118. https://doi.org/10.1093/bioinformatics/btr597
- Swift, J. K., & Derthick, A. O. (2013). Increasing hope by addressing clients’ outcome expectations. Psychotherapy Theory, Research, Practice, Training, 50(3), 284. https://doi.org/10.1037/a0031941
- Twomey, C., O’Reilly, G., Bültmann, O., Meyer, B., & Vigo, D. (2020). Effectiveness of a tailored, integrative internet intervention (deprexis) for depression: Updated meta-analysis. Public Library of Science ONE, 15(1), e0228100. https://doi.org/10.1371/journal.pone.0228100
- World Health Organization. (2022). World mental health report: Transforming mental health for all.
- Zwerenz, R., Baumgarten, C., Becker, J., Tibubos, A., Siepmann, M., Knickenberg, R. J., & Beutel, M. E. (2019). Improving the course of depressive symptoms after inpatient psychotherapy using adjunct web-based self-help: Follow-up results of a randomized controlled trial. Journal of Medical Internet Research, 21(10), e13655. https://doi.org/10.2196/13655
- Zwerenz, R., Becker, J., Knickenberg, R. J., Siepmann, M., Hagen, K., & Beutel, M. E. (2017). Online self-help as an add-on to inpatient psychotherapy: Efficacy of a new blended treatment approach. Psychotherapy and Psychosomatics, 86(6), 341–350. https://doi.org/10.1159/000481177