
Abstract
Interventions to change health-related behaviours typically have modest effects and may be more effective if grounded in appropriate theory. Most theories applied to public health interventions tend to emphasise individual capabilities and motivation, with limited reference to context and social factors. Intervention effectiveness may be increased by drawing on a wider range of theories incorporating social, cultural and economic factors that influence behaviour. The primary aim of this paper is to identify theories of behaviour and behaviour change of potential relevance to public health interventions across four scientific disciplines: psychology, sociology, anthropology and economics. We report in detail the methodology of our scoping review used to identify these theories including which involved a systematic search of electronic databases, consultation with a multidisciplinary advisory group, web searching, searching of reference lists and hand searching of key behavioural science journals. Of secondary interest we developed a list of agreed criteria for judging the quality of the theories. We identified 82 theories and 9 criteria for assessing theory quality. The potential relevance of this wide-ranging number of theories to public health interventions and the ease and usefulness of evaluating the theories in terms of the quality criteria are however yet to be determined.
Introduction
Human behaviours, including tobacco and alcohol consumption, dietary behaviours, physical activity and sexual practices, play a key role in many of the leading causes of death in developing and developed countries (Aveyard & West, Citation2007; Danaei et al., Citation2009; Ezzati et al., Citation2002; Mokdad, Marks, Stroup, & Gerberding, Citation2004; Parkin, Boyd, & Walker, Citation2011; Solomon & Kington, Citation2002). Even small changes in such behaviours can have substantial effects on population health outcomes (Ezzati et al., Citation2002; Mokdad et al., Citation2004; National Institute for Health and Clinical Excellence (NICE), Citation2010; Solomon & Kington, Citation2002). Understanding these behaviours and the contexts in which they occur is essential for developing effective evidence-based health behaviour change interventions and policies and for reducing avoidable mobility and mortality (House of Lords, Citation2011; Office of Behavioural and Social Sciences Research, Citation2006).
Despite the relatively small investment in preventive health and behavioural science (Marteau, Dieppe, Foy, Kinmonth, & Schneiderman, Citation2006), there is evidence for the effectiveness of behaviour change interventions at individual, community and population levels (Abraham, Kelly, West, & Michie, Citation2009; Albarracin et al., Citation2005; Michie & West, Citation2013; National Institute for Health and Care Excellence, Citation2007; Nigg, Allegrante, & Ory, Citation2002). Interventions have been targeted at behavioural risk factors (e.g., smoking; Carr & Ebbert, Citation2012; Rice & Stead, Citation2008), encouraging protective behaviours (e.g., health screening; Brouwers et al., Citation2011; Everett et al., Citation2011), improving adaptation to chronic and acute illness (e.g., adherence to medical advice; Cutrona et al., Citation2010) and changing health professional behaviours to improve the quality and efficiency of services (e.g., hand hygiene compliance; Fuller et al., Citation2012). While there are many examples of successful interventions, there are also examples of ineffective interventions (e.g., Coleman, Citation2010; Summerbell et al., Citation2005); for those that are effective, the effects tend to be modest, with significant heterogeneity of short-term and long-term effects (Michie, Johnston, Francis, Hardeman, & Eccles, Citation2008).
To maximise the potential efficacy of interventions, it is necessary to understand behaviour and behaviour change: in other words, it is necessary to have a theoretical understanding of behaviour change. In this context, theory represents the accumulated knowledge of the mechanisms of action (mediators) and moderators of change as well as the a priori assumptions about what human behaviour is, and what the influences on it are. The application of theory is advocated as an integral step in intervention design and evaluation and in evidence synthesis, for example, by the UK Medical Research Council's guidance for developing and evaluating complex interventions (Campbell et al., Citation2000, Citation2007; Craig et al., Citation2008; Glanz & Bishop, Citation2010). This is for several reasons. First, the antecedents of behaviour and the causal determinants of change can be appropriately identified and targeted by the intervention (Hardeman et al., Citation2005; Michie & Abraham, Citation2004; Michie et al., Citation2008) and component behaviour change techniques can be selected and/or refined and tailored (Michie & Prestwich, Citation2010; Michie et al., Citation2008; Rothman, Citation2004). Second, theoretically identified mechanisms of action (i.e., mediators) can be investigated to gain further understanding as to how the intervention brings about its effects (Michie & Abraham, Citation2004; Rothman, Citation2004, Citation2009). This allows researchers to determine whether unsuccessful interventions have failed either because the intervention has had no effect upon the hypothesised mediator or because the hypothesised (and successfully influenced) mediator has had no effect upon behaviour (Michie & Abraham, Citation2004; Rothman, Citation2004, Citation2009), thus facilitating more efficient refinement of the intervention. Third, theory summarises the cumulative knowledge of how to change behaviour across different populations, behaviours and contexts. Finally, theory-based interventions provide an opportunity in which theory can be tested. This aids development of more useful theories which, in turn, supports intervention optimisation (Michie et al., Citation2008; Rothman, Citation2004).
The question as to whether interventions that are explicitly based on theory are more effective that those that are not is a complex one. Some reviews have found a positive association (Albada, Ausems, Bensing, & van Dulmen, Citation2009; Albarracin et al., Citation2005; Glanz & Bishop, Citation2010; Noar, Benac, & Harris, Citation2007; Swann, Bowe, Kosmin, & McCormick, Citation2003; Taylor, Conner, & Lawton, Citation2011), but others have found no association, or, even a negative association (Gardner, Wardle, Poston, & Croker, Citation2011; Roe, Hunt, Bradshaw, & Rayner, Citation1997; Stephenson, Imrie, & Sutton, Citation2000). Some reviews have reported a mixture depending on the measure of effectiveness (Ammerman, Lindquist, Lohr, & Hersey, Citation2002; Bhattarai et al., Citation2013; Kim, Stanton, Li, Dickersin, & Galbraith, Citation1997).
There are several factors that may explain this mixed picture. Theory is often poorly applied. A review investigating application of theory using the 19-item ‘Theory Coding Scheme’ (Michie & Prestwich, Citation2010), found that only 10% of studies of theory-based interventions reported links between behaviour change techniques and theoretical constructs and only 9% reported that all the constructs had been targeted by behaviour change techniques. Another explanation may be that the choice of theory may not have been appropriate. For example, if a behaviour is heavily influenced by habit or emotional states then a theory that focuses on beliefs and reflective thought processes may not be appropriate when informing intervention design.
The importance of understanding the theoretical underpinnings of behavioural interventions has been highlighted in previous research suggesting theoretical bases for combining behaviour change techniques within interventions to allow synergistic effects and enhance their effectiveness (Dombrowski et al., Citation2012; Michie, Abraham, Whittington, McAteer, & Gupta, Citation2009; Taylor et al., Citation2011; Webb, Joseph, Yardley, & Michie, Citation2010). Despite the advantages of theory, behaviour change interventions are often designed without reference to theory (Davies, Walker, & Grimshaw, Citation2010; Prestwich et al., Citation2013). For instance, a recent meta-analysis found that only 22.5% of 235 implementation studies explicitly used theories of behaviour change (Davies et al., Citation2010). Where theory is used, it is often only loosely referred to rather than rigorously applied to intervention design and evaluation (Painter, Borba, Hynes, Mays, & Glanz, Citation2008; Prestwich et al., Citation2013). In those situations where interventions are based on ‘explicit theory’, theory is often used sub-optimally to develop or evaluate the intervention (e.g., only a few of the theoretical constructs may be targeted and/or theory is not used to appropriately tailor the intervention).
Choosing a relevant theory can be a challenging task for intervention designers, especially given the large number of theories, many of which have the same or overlapping constructs, to choose from (Michie et al., Citation2005). There is a lack of guidance on how to select an appropriate theory for a particular purpose (Michie, Citation2008), with a predominance in published intervention evaluations of a small number of theories that have already gained recognition in the field (Painter et al., Citation2008). By using a ‘common’ or ‘favourite’ theory, rather than one that may be more suited to the particular characteristics of the target population, behaviour and context, the potential benefit of using theory is limited.
One approach to addressing the plethora of different, overlapping theories and lack of guidance as to how to choose between them was the development of the Theoretical Domains Framework (TDF; Cane, O'Connor, & Michie, Citation2012; Michie et al., Citation2005). Developed by psychologists and implementation researchers, the TDF provides a framework of theoretical domains to explain barriers and facilitators of behaviour in any particular situation. Informed by 128 explanatory constructs from 33 theories of behaviour, the TDF has been used in many contexts to understand behaviour and design theoretically informed interventions (Francis, O'Connor, & Curran, Citation2012; French et al., Citation2012). Another resource for theory-informed research is the US National Institute of Health's ‘Grid Enabled Measures’ (GEM) web-based database. GEM provides the descriptions of theoretical constructs and behavioural and social measures to assess these constructs (https://www.gem-beta.org/Public/Home.aspx). While both these approaches are of value, neither specifies relationships between theoretical domains and constructs in terms of the effect that one domain or construct may have on another. They deal with theoretical domains and constructs, not theories per se. One previous consensus exercise did generate a list of eight constructs thought to influence HIV-related behaviours, with the resulting framework specifying links between the constructs and behaviour (Fishbein et al., Citation2001). However, it is not clear how this consensus was reached and how relevant the included constructs are to other behaviours, given the focus on HIV-related behaviours. Researchers or interventions designers may want to select specific theories either at the beginning of the intervention design process or after conducting some preliminary research to indicate which theories are likely to be relevant and useful. In these situations there is a need for an accessible source of potentially useful theories, as well as a method for selecting amongst them.
At present, theories used in public health and behaviour change interventions more generally tend to emphasise individual and sometimes interpersonal rather than broader social and environmental variables (Glanz & Bishop, Citation2010). Capabilities and motivation (individual factors) are often targeted, but context (social and environmental variables) is far less likely to be considered. NICE's (Citation2007) behaviour change guidance concluded that interventions were more effective if they simultaneously targeted variables at different levels (e.g., individual, community and population; National Institute for Health and Care Excellence, Citation2007). Therefore, to maximise effectiveness, intervention designers are likely to benefit from drawing from a wider range of theories than currently used. Current resources on theories of behaviour change tend to reflect specific contexts and disciplines, and are thus inevitably limited in the range of theories considered (Agar, Citation2008; Conner & Norman, Citation2005; Glanz & Bishop, Citation2010; Glanz, Rimer, & Lewis, Citation2002).
To improve the selection and application of theory we need to consider, across relevant disciplines, those theories which may be of potential use in informing public health questions. By identifying a range of theories we can assess which theories may be of value given the behaviour, population and context in question. To this end, we conducted a scoping review and consensus exercise, informed by the disciplines of psychology, sociology, anthropology and economics. The scoping review and consensus exercise primarily aimed to address the question, ‘What theories exist across the disciplines of psychology, sociology, anthropology and economics that could be of value to guiding behaviour change interventions?’
To be as comprehensive as possible we focused on both theories of behaviour and behaviour change. Theories of behaviour tend to be linear, and explain the reasons why behaviour may occur by considering a number of predictors and their associations with one another and how these could influence the likelihood of a particular behaviour (Agar, Citation2008; Conner & Norman, Citation2005; Glanz & Rimer, Citation1997; Head & Noar, Citation2013). Theories of change tend to be more cyclical and identify interactional and dynamic behaviour change processes (Agar, Citation2008; Head & Noar, Citation2013). In practice, it is sometimes difficult to distinguish between the two and some theories could be viewed as both.
Of secondary interest we also addressed ‘What criteria should we consider when evaluating the quality and potential appropriateness of behaviour change theory?’ Finally, we assessed the extent to which the theories we identified had been applied within the behaviour change field.
The scope of the present paper is twofold: (i) to report in detail the methodology employed to identify relevant theories and to produce a compendium of these theories and (ii) to provide the list of agreed criteria for judging the quality of the theories. Ways in which some of the theories have been used to study behaviour change are also briefly summarised, though it is beyond the scope of this paper to discuss this in detail. Research examining how the theories have been operationalised and the quality of their empirical application (as measured by the quality criteria reported here) forms part of the future research programme.
Methods
Theories of behaviour and behaviour change were identified through five sources: expert consultation with a multidisciplinary project advisory group, electronic databases, web searching, forward and backward searching of reference lists and hand searching of key behavioural science journals. Empirical application of the theories was identified from electronic databases and searching the reference lists of retrieved articles. These, together with expert consultations with the advisory group, informed the development of the quality assessment criteria.
Expert advisory group
Twenty-four UK experts from the social and behavioural sciences and/or population health research formed the advisory group, which determined the scope, methods and conduct of the review. The group comprised four sociologists, five economists, five psychologists, four health service researchers, three anthropologists, two epidemiologists and one policy researcher.
Definition of key terms
One of the first tasks of the advisory group was to agree definitions of the terms ‘theory’ and ‘behaviour’. A shortlist of potentially relevant definitions of each term was compiled from peer-reviewed journals, reports and books, for example, the American Psychological Association Dictionary. In the first of two rounds of a Delphi process, advisory group members were asked to rate each definition and parts of the definition for potential use. When a definition (or a part of it) was rated as important by at least 50% of the group it was retained as relevant. In the second round, core concepts were extracted and synthesised by the authors and used to create working definitions which were then considered for refinement by the advisory group in order to create the final definitions:
The term theory was defined as: ‘a set of concepts and/or statements with specification of how phenomena relate to each other. Theory provides an organising description of a system that accounts for what is known, and explains and predicts phenomena’.
Behaviour was defined as: ‘anything a person does in response to internal or external events. Actions may be overt (motor or verbal) and directly measurable or, covert (activities not viewable but involving voluntary muscles) and indirectly measurable; behaviours are physical events that occur in the body and are controlled by the brain’.
Identification of relevant theories
To inform the literature search strategy, theories of behaviour and behaviour change were identified through expert consultation with the advisory group and an initial scoping of the literature using generic and discipline-specific terms related to behaviour and behaviour change theories. For example, the term ‘cultural change’ tended to be used by anthropologists, ‘action’ by sociologists and ‘behaviour’ by psychologists.
Literature search strategy
The literature search was conducted primarily to uncover theories of behaviour and behaviour change that were not identified through expert consultation with our advisory group. Secondary to this we identified the ways in which the theories we identified had been empirically applied. While we briefly report this, it was beyond the scope of the study to analyse this comprehensively and in detail. In order to retrieve relevant literature across different disciplines six databases were searched between 1 January 1960 and 11 September 2012: PsycINFO, Econlit, Cochrane Database of Systematic reviews, International Bibliography of Social Sciences, EMBASE and MEDLINE. Databases were chosen based on their coverage of discipline- and content-specific literature and on the volume of public health literature. Databases that did not allow the use of wildcards (to account for variations in spellings) or sets of search terms to be entered and combined through the use of Boolean operators, and/or databases that only retrieved titles of articles but not abstracts were not used (e.g., Anthropology Index Online). The final search was conducted on the 11 September 2012.
The search strategy included four sets of search terms: those that (i) apply theory to behaviour change (e.g., ‘behaviour change theory’); (ii) are relevant to behaviour change and also of relevance in understanding behaviour more generally [e.g., ‘Health Belief Model’ (HBM)]; (iii) are relevant to behaviour change but that do not mention theory (e.g., ‘behaviour modification’); and (iv) discipline-specific terms combined with the term behaviour change (e.g., ‘economics and behaviour change’). A list of the search terms together with how these terms were combined can be found in the online supplemental material (Supplemental Figure 1).
The search strategy was customised to each database. Standard filters were used to capture systematic reviews where applicable. A sensitivity analysis was performed to ensure that the search results included key articles on theories relevant to behaviour change (identified through the initial scoping of the literature). Given the complex body of evidence, in terms of cross-cutting disciplines and sheer breadth and volume of literature, the search was restricted to titles and abstracts to tighten the search specificity.
Additional potentially relevant theories were identified through expert consultation and web searching for key documents from organisations known for their interest in behaviour change. This included, from the USA, the National Institute of Health's Behaviour Change Consortium and, from the UK, the NICE, Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI Centre), Government Social Research Unit, House of Lords Science and Technology Select Committee Report on Behaviour Change and National Institute of Health Research's Health Technology Assessment.
Forward and backward citation searching, and hand searching of key behavioural science journals were performed to minimise the likelihood of relevant theories being missed. The journals hand searched were: Annals of Behavioural Medicine, BMC Health Services Research, British Journal of Health Psychology, Health Psychology, Health Psychology Review, Implementation Science, International Journal of Clinical and Health Psychology, Journal of Applied Behavioural Science and Social Science & Medicine.
Inclusion criteria for theories
Theories were included if they: (i) met our definition of theory and behaviour and (ii) considered individual behaviour as an outcome or part of the process leading to the outcome. Theories that considered group behaviour (e.g., ‘organisational behaviour’), without reference to individual behaviour were excluded. While we acknowledge that such theories are of interest to intervention designers who want to change group behaviour we decided to limit the scope of the review to theories concerned with individual behaviour change to keep it manageable. The inclusion of each theory was considered independently by at least two of the four authors and by members of the advisory group. Inter-rater reliability was assessed.
Theories that focused purely on cognition were not included. Examples of such theories include Social Comparison Theory (Festinger, Citation1954), which aims to explain how people's opinions are influenced within social groups and Cognitive Adaptation Theory (Taylor, Citation1983), which aims to explain how people cognitively adapt to threatening events. While these theories contribute to our understanding of knowledge, beliefs and intentions about behaviour there are often significant gaps between these and behaviour (Sheeran, Citation2002) and this project was about theories of behaviour and behaviour change.
We distinguished frameworks, which provide an organising structure, from theories which, in addition, offer explanations of how phenomena relate to each other and permit outcomes to be predicted. Thus, conceptual frameworks such as the TDF (Cane et al., Citation2012; Michie et al., Citation2005), or the Ecological Model (McLeroy, Bibeau, Steckler, & Glanz, Citation1988) that are commonly used to guide the design, implementation or evaluation of interventions were not included. While these frameworks have value in implementation and in public health research, policy and practice, this review was of specific theories.
Inclusion criteria for articles
Screening of articles was in two stages. The first stage (title and abstract) was intentionally inclusive, retaining articles if they mentioned: (i) theory in relation to behaviour or behaviour change or (ii) changing behaviour but made no reference to theory (the full text of the article was then checked to see if theory was used to inform the research). We considered all behaviour to be of relevance, not just health-related behaviours. At the second stage of screening (full-text) tighter restrictions applied and articles were included if: (i) theory and behaviour was defined as per our study definitions and (ii) they fell into one of four categories of article: descriptive, intervention, evaluative or review:
Descriptive articles were defined as those that contained the original description of a theory by the author/s who originally conceived of the theory (i.e., primary theory sources) or by an author/s who proposed advances in the theory by re-specification. Secondary theory sources (i.e., those that only provided an overview/description of the theory) were not included.
Intervention articles were defined as those that stated in their methods that they used theory to inform the development and/or evaluation of an intervention aimed at changing behaviour and that included a measure of behaviour as an outcome. We focused on behaviour as the end-point rather than the consequence of the behaviour (e.g., weight loss) because there are a number of factors further along the causal chain that could affect the link between behaviour and outcome (Hardeman et al., Citation2005).
Evaluative articles were defined as those reporting studies that empirically tested a theory longitudinally.
Review articles were defined as those that systematically reviewed a theory in relation to a change in behavioural outcomes. Narrative reviews or selective overviews of the literature (i.e., those without a description of a search strategy and no clear methodology that could be reproduced independently) were not included.
Articles were excluded if they: focused on cognition (e.g., intention to change behaviour) rather than actual behaviour; were restricted to research participation behaviours, animal studies, scale development, measurement or programme development, cost-effectiveness or single case studies; focused on mental health including therapeutic interventions where cognitive or emotional variables were the primary outcome. Dissertations and doctoral theses, books and book reviews, conference posters and presentations, editorials and commentaries were excluded for practical reasons to limit the volume of material to be retrieved and reviewed to manageable proportions. Articles that used multiple theories to inform their methodology were excluded because our review was of the empirical application of individual theories to changing behaviour.
We did not exclude articles based on their quality, since the methodology of applying these criteria has yet to be developed.
Inter-rater reliability
Articles were screened for relevance at abstract and full-text stage by the lead author (Rachel Davis). At both screening stages, 30% of the abstracts were independently screened by two other researchers (each of which screened 15%) and inter-rater reliability (calculated using percentage agreement) was assessed. Since the data constitute unbalanced cells, we have used percentage agreement as it provides a more transparent and more readily interpretable parameter than Cohen's kappa. As kappa corrects for chance agreement among multiple coders, use of kappa is likely to underestimate reliability (Steinijans, Diletti, Bomches, Greis, & Solleder, Citation1997). Differences of views about inclusion were resolved through discussion and consensus with the other authors.
Data extraction
Data were extracted on: (i) country where the research took place, (ii) theory used, (iii) type of article (descriptive, intervention, evaluative or review), (iv) design (quantitative, qualitative or mixed methods), (v) target behaviour (e.g., smoking, physical activity), (vi) target direction of behaviour [i.e., increase (which also included maintaining behaviour) or decrease in uptake] and (vii) measurement of behaviour (self-report, objective or both). Dual data extraction was conducted independently on 60% of the included papers by two researchers and inconsistencies resolved through joint discussion.
Quality assessment criteria
We reviewed key literature which synthesised scientific and philosophical perspectives on what makes a theory scientific and useful for the purpose of effecting healthy behaviour change in a target population (e.g., Glanz & Rimer, Citation1997; West, Citation2006) and used this to draft an initial list of quality criteria. These were considered by the advisory group in both a face-to-face discussion and a subsequent electronic Delphi-like consultation aimed at achieving consensus.
Results
We report the theories of behaviour and behaviour change identified in our review and the agreed criteria for assessing theory quality. A high-level summary of the key characteristics of the review articles is also provided.
Inter-rater reliability
A high level of agreement was observed for decisions on inclusion in relation to both the theories and the articles included in the review (>90%).
Theories identified
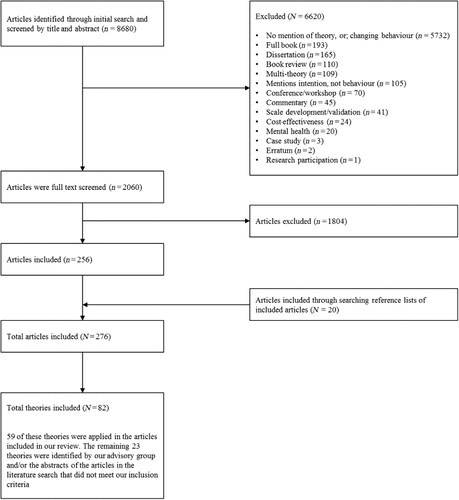
Eighty-two theories of behaviour and behaviour change were identified. These are listed in along with the lead author, date of the paper that originally described the theory and the number of articles that reported using the theory. Fifty-nine (out of the 82 theories) were applied in the articles included in our review. The remaining theories (N = 23) were identified by the advisory group and/or through abstracts of the articles retrieved in our literature search. In other words, these were theories that met our inclusion criteria but did not have relevant articles retrieved from our search strategy that met our article inclusion criteria, i.e., articles did not fall within one of our four categories (descriptive, intervention, evaluative, review). Theories identified through our search that were excluded, with reasons for exclusion, can be found in the online supplemental material (Supplemental Table 1).
Table 1. Theories identified, along with first author and date of the primary theory source and the number of articles reporting the theory.
It is important to note here that while our intention was to provide a list of potentially relevant theories across different disciplines, it was not possible to categorise the theories according to disciplines. Many of the theories had influences from more than one discipline and/or authors were from several disciplines or could not be categorised into any one discipline.
Quality assessment criteria
Nine defining features were identified as conceptually important for a good theory: (i) clarity of constructs – ‘Has the case been made for the independence of constructs from each other?’ (ii) clarity of relationships between constructs – ‘Are the relationships between constructs clearly specified?’ (iii) measurability – ‘Is an explicit methodology for measuring the constructs given?’ (iv) testability – ‘Has the theory been specified in such a way that it can be tested?’ (v) being explanatory – ‘Has the theory been used to explain/account for a set of observations? (statistically or logically)’; (vi) describing causality – ‘Has the theory been used to describe mechanisms of change?’ (vii) achieving parsimony – ‘Has the case for parsimony been made?’ (viii) generalisablity – ‘Have generalisations been investigated across’: (a) behaviours? (b) populations? (c) contexts?’ and (ix) having an evidence base.
Articles retrieved
In the results sections that follow we briefly summarise the main findings of the articles included in our review. Further examination of the empirical application of these theories using our quality assessment criteria is part of the future research programme.
Of 8680 articles retrieved through the database search, 6620 were excluded at the first stage of screening (title and abstract) and 1804 articles (out of the remaining 2060) were excluded after full-text screening, leaving 256 articles. To these a further 20 articles were added through searching the reference lists of the included articles, resulting in 276 articles. displays a flow chart of the search results.
Article characteristics
Articles were published between 1977 and 2012, with most of the research conducted in Europe and North America. Eighteen categories of behaviours were identified, with three accounting for 50% of the articles: increasing physical activity (N = 72; 26%), safe sex practices (N = 36; 13%) and smoking cessation (N = 30; 11%). Fifty-two (19%) articles addressed multiple health-related behaviours, with 17 (6%) of these targeting healthy eating and physical activity together. The remaining categories comprised behaviours relating to: healthy eating (N = 13), addictive behaviours including alcohol and drugs (N = 12), health examinations and tests (N = 11), environmental conservation (N = 10), violence and delinquency (N = 9), sun protection (N = 9), drug adherence (N = 5), job- or education-related activities (N = 4), Internet- or other technology-related behaviours (N = 4), health care professional adherence to health care guidelines (N = 3), financial-related activities (N = 2), speeding (N = 2) and 2 ‘others’ which were behaviours that did not fall into any of the above categories including pet removal from domestic residence (N = 1) and repairing mosquito nets (N = 1).
The majority of articles used quantitative methods (N = 243; 88%) and most reported interventions (N = 168; 61%) or were evaluative (N = 62; 35%). Thirty-one descriptive articles (either primary theory sources or extensions of a theory) were identified. Behaviour was most commonly measured by self-report methods (N = 194; 70%). For a high-level summary of these key characteristics, please refer to ; a more detailed account of each individual article can be found online in Supplemental Table 2.
Table 2. Characteristics of studies included in the systematic review (N = 276).
Papers published by the same first author and focused on the same theory were assessed to identify cases in which multiple articles based on the same intervention (i.e., intervention protocol and outcomes) or data-set had been published. This was found to be the case for 19 articles in total (covering 9 interventions/data-sets; see and ).
Frequency of use
Of the 82 theories identified, just 4 theories accounted for 174 (63%) of articles: the Transtheoretical Model of Change (TTM; N = 91; 33%), the Theory of Planned Behaviour (TPB; N = 36; 13%), Social Cognitive Theory (SCT; N = 29; 11%) and the Information-Motivation-Behavioural-Skills Model (IMB; N = 18; 7%). A further four theories accounted for an additional 32 (12%) of the included articles: the HBM (N = 9; 3%), Self-determination Theory (SDT; N = 9; 3%), Health Action Process Approach (HAPA; N = 8; 3%) and Social Learning Theory (SLT; N = 6; 2%; SLT is a precursor of SCT). The remaining theories (N = 70) were applied fewer than 6 times each in the literature that met our inclusion criteria, with most only being applied once or twice (see ).
Discussion
This scoping review of theories of behaviour/behaviour change of potential relevance to designing and evaluating public health interventions was informed by the disciplines of psychology, sociology, anthropology and economics. Eighty-two theories were identified that spanned a myriad of behaviours and could be applied to designing and evaluating interventions to improve public health, as well as tackle other social issues such as environmental sustainability and public safety.
It is important to note that the literature identified in the scoping review reflects the search strategy that aimed to identify theories rather than exhaustively review theoretically informed empirical studies. Therefore, whilst the review identified articles that use the theories in relation to our inclusion criteria, it does not reflect the wider application of these theories to public health-related research.
Scoping reviews are used to map or configure a body of evidence. They therefore tend to focus on breadth, including studies that are representative of the variation within the evidence base, rather than focusing on depth and assembling all the eligible material. It can also mean that establishing what the boundaries of the review are, and therefore what should be included or excluded, may be refined during the course of the review (Shemilt et al., Citation2013). Consensus methods can help with this process. While we intended to conduct this review in a systematic and reproducible way, as it was the first attempt that we were aware of to review a bodies of theory in this way, its purpose seemed more akin to that of a scoping than a systematic review. As Gough, Thomas, and Oliver (Citation2012) have suggested, there is a clear distinction between aggregative systematic reviews that are ‘about seeking evidence to inform decisions’ and configurative scoping reviews which are about ‘seeking concepts to provide enlightenment through new ways of understanding’. Arguably what we wanted to attempt was a combination of these two things but we have nevertheless labelled what we did a scoping review.
From the theories we identified, only a few were frequently applied in literature. While the purpose of our scoping review was not to uncover all the relevant literature on how these theories have been applied, the finding is of interest because it is consistent with other reviews and publications (e.g., Glanz & Bishop, Citation2010; Painter et al., Citation2008; Prestwich et al., Citation2013). Sixty-three per cent of the articles identified in the review related to just four theories: the TTM, TPB, SCT and the IMB Skills Model. While the literature we uncovered was limited by our inclusion criteria, and includes a small number cases in which authors have published more than one article applying the same theory to the same data-set or intervention, it indicates the very uneven distribution of frequency of theory use. This raises the question as to why many theories are so little used. One explanation may be that how often a theory is used, could in part, be confounded by the year in which the theory was introduced. Knowledge of a theory in terms of how much it is discussed in the public domain is also likely to play a role. Another explanation might be that those that are used more frequently are ‘better’ theories and selected for use because they have a stronger evidence base or meet other quality criteria. However, a couple of examples suggest that frequency does not necessarily follow quality. For example, the theory appearing most frequently in our review, the TTM, has been criticised on several grounds (West, Citation2005) and its empirical support has been questioned by systematic review findings (e.g., Cahill, Lancaster, & Green, Citation2010; Etter & Perneger, Citation1999; Littell & Girvin, Citation2002; Whitelaw, Baldwin, Bunton, & Flynn, Citation2000). On the other hand, recent meta-regression evidence has shown good support for Control Theory (Dombrowski et al., Citation2012; Ivers et al., Citation2012; Michie et al., Citation2009); however, this was identified in only one article in our review. Another explanation is that people are not aware of the full range of theories from which to choose and so instead opt for those most commonly applied in the literature. Frequency of use may not reflect perceived quality of the theory but instead, fashion, familiarity, prior training, exposure or incentivisation. We hope that this review will help to increase awareness among intervention designers and researchers about the range of theories available. We report nine criteria agreed as markers of theory quality that could aid selection of the most appropriate theory or theories.
Our decision to focus on theories of behaviour change at the level of the individual and exclude theories concerned with group behaviour is likely to be part of the explanation for the preponderance of psychological theories identified in the review, although even interventions at the community level tend to be informed by psychological or social–psychological theories (e.g., Bonell, Fletcher, et al., Citation2013; Bonell, Jamal, et al., Citation2013; Glanz & Bishop, Citation2010; National Institute for Health and Care Excellence, Citation2007). This, and the decision not to include books where sociological and anthropological theories are more likely to be found, may go some way to explaining why these types of theory are under-represented. In addition, Kelly et al. (Citation2010) found that sociological theories were missed in electronic searches, particularly if they were more than 25 years old. Given that interventions may be improved by drawing on theories specifically targeting group behaviours, this would be a useful focus for a future literature review as we are not aware of there being such a review.
This review raised the issues as to what constitutes ‘a theory’ and ‘a behaviour’. Theories, as conceptualised here, ranged from quite specific (e.g., to a particular behavioural domain or type of intervention) to very general, including multiple levels of influence. The cut-offs at either end of this spectrum were agreed by consensus but were inevitably arbitrary. A general observation was that more general theories may have greater face validity but be less useable in guiding research than more specific theories; choice of theory will therefore be partly guided by the purpose it is to be put to. Another observation was that there appeared to be no generally accepted use of terms such as theory, model, framework and orientation, with different uses by different authors. Increasing the precision of, and consensus on, use of terminology would be helpful for the field.
‘Behaviour’ also varies in level of specificity: for example, physical activity includes sports which includes volleyball which includes running. Behaviours are also part of sequences, often dependent on previous behaviours (e.g., carrying gym kit) and sometimes on other people's behaviours (e.g., others turning up for a team game). Just as the relevance of a particular theory may vary across type of behaviour, so it may vary according to the level of specificity.
The review also suggests that there are a large number of theories that are of potential use in designing public health interventions. The cataloguing of 83 theories of behaviour change is an important resource for researchers wishing to draw on theories beyond the few that currently dominate the literature. However, few of these theories have been subjected to wide-scale rigorous empirical evaluation. There have been calls for more operationalization, application, testing and refining of theories over many years (e.g., Michie & Johnston, Citation2012; Noar & Zimmerman, Citation2005; Rothman, Citation2004; Weinstein, Citation2007; Weinstein & Rothman, Citation2005), but advances are slow. We need more investment into methodological and substantive research in this area, for example, the use of fractionated factorial (Collins et al., Citation2011) and n-of-1 (Johnston, Jones, Charles, McCann, & McKee, Citation2013) designs to tease apart complex interventions and the extent to which theories can be generalised across populations, behaviours and contexts.
Identifying the theories in this review is just the first step in a much larger and ongoing programme of work aimed at improving the use of appropriate theory and the scientific rigour with which it is applied. Future work will investigate the ways in which theories have been operationalised and the extent to which different theories share constructs and can be seen as ‘families’ of theory. Transforming the nine quality criteria into forms, such as reliable scales or response options that can be used in evaluating theories is a complex task, and a study in its own right. The evolution of theories over time, including the issue of when a theory is considered a new theory, will also be examined. Many theories contained similar constructs or the same constructs but with slightly different names. Understanding these similarities and working towards a common set of terminology would facilitate the building of a cumulative understanding of mechanisms of action from both primary research and evidence syntheses. It would also further our understanding of the evolution of theories and how theories have been revised and/or integrated with other theories over time. Having said this, it is also important to recognise that not only language varies across and within disciplines but so do epistemological and ontological assumptions and preoccupations.
The next phase of the current research is to (i) investigate the connectedness of theories with each other and (ii) operationalize and demonstrate the application of the agreed quality criteria. These will both inform the understanding of theory and its development, and help guide researchers, policy-makers and interventions on the appropriate selection and application behaviour change theories to developing public health and other behaviour change interventions.
Supplemental material
Supplemental material for this article can be accessed here: http://dx.doi.org/10.1080/17437199.2014.941722.
Supplementary_material.pdf
Download PDF (399 KB)Acknowledgements
We are grateful to the study's advisory group for developing the literature search strategy, key definitions and the quality criteria for evaluating theory: Robert Aunger, Mary Barker, Mick Bloor, Heather Brown, Richard Cookson, Cyrus Cooper, Peter Craig, Paul Dieppe, Anna Dixon, Rachel Gooberman-Hill, Simon Griffin, Graham Hart, Kate Hunt, Susan Jebb, Marie Johnston, Mike Kelly, Steve Morris, Mark Petticrew, Paschal Sheeran, Mark Suhreke, Ivo Vlaev, Robert West, Daniel Wight, Daniel Zizzo. We are also grateful to Kate Sheals for invaluable help in the latter stages of manuscript preparation.
Funding
This project was funded by the Medical Research Council's Population Health Sciences Research Network [grant number PHSRN10]. The work was undertaken with the support of The Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer), a UKCRC Public Health Research: Centre of Excellence. Funding from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council [RES-590-28-0005], Medical Research Council, the Welsh Government and the Wellcome Trust [WT087640MA], under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged.
Additional information
Funding
References
- Abraham, C., Kelly, M. P., West, R., & Michie, S. (2009). The UK National Institute for Health and Clinical Excellence public health guidance on behaviour change: A brief introduction. Psychology, Health and Medicine, 14(1), 1–8. doi:10.1080/13548500802537903
- Agar, J. (2008). What happened in the sixties? British Journal for the History of Science, 41, 567–600. doi:10.1017/S0007087408001179
- Albada, A., Ausems, M. G. E. M., Bensing, J. M., & van Dulmen, S. (2009). Tailored information about cancer risk and screening: A systematic review. Patient Education and Counseling, 77, 155–171. doi:10.1016/j.pec.2009.03.005
- Albarracin, D., Gillette, J. C., Earl, A. N., Glasman, L. R., Durantini, M. R., & Ho, M. H. (2005). A test of major assumptions about behavior change: A comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychological Bulletin, 131, 856–897. doi:10.1037/0033-2909.131.6.856
- Ammerman, A. S., Lindquist, C. H., Lohr, K. N., & Hersey, J. (2002). The efficacy of behavioral interventions to modify dietary fat and fruit and vegetable intake: A review of the evidence. Preventive Medicine, 35(1), 25–41. doi:10.1006/pmed.2002.1028
- Aveyard, P., & West, R. (2007). Managing smoking cessation. BMJ, 335(7609), 37–41. doi:10.1136/bmj.39252.591806.47
- Bhattarai, N., Prevost, A., Wright, A., Charlton, J., Rudisill, C., & Gulliford, M. (2013). Effectiveness of interventions to promote healthy diet in primary care: Systematic review and meta-analysis of randomised controlled trials. BMC Public Health, 13(1), 1–14. doi:10.1186/1471-2458-13-1203
- Bonell, C. P., Fletcher, A., Jamal, F., Wells, H., Harden, A., Murphy, S., & Thomas, J. (2013). Theories of how the school environment impacts on student health: Systematic review and synthesis. Health & Place, 24, 242–249. doi:10.1016/j.healthplace.2013.09.014
- Bonell, C., Jamal, F., Harden, A., Wells, H., Parry, W., Fletcher, A., … Moore, L. (2013). Systematic review of the effects of schools and school environment interventions on health: Evidence mapping and synthesis. Public Health Research, 1(1). Retrieved from http://www.journalslibrary.nihr.ac.uk/__data/assets/pdf_file/0016/71161/FullReport-phr01010.pdf
- Brouwers, M. C., De Vito, C., Bahirathan, L., Carol, A., Carroll, J. C., Cotterchio, M., … Wathen, N. (2011). What implementation interventions increase cancer screening rates? A systematic review. Implementation Science, 6, 111. doi:10.1186/1748-5908-6-111
- Cahill, K., Lancaster, T., & Green, N. (2010). Stage-based interventions for smoking cessation. Cochrane Database of Systematic Reviews, (11), CD004492. doi:10.1002/14651858.CD004492.pub4
- Campbell, M., Fitzpatrick, R., Haines, A., Kinmonth, A. L., Sandercock, P., Spiegelhalter, D., & Tyrer, P. (2000). Framework for design and evaluation of complex interventions to improve health. BMJ, 321, 694–696. doi:10.1136/bmj.321.7262.694
- Campbell, N. C., Murray, E., Darbyshire, J., Emery, J., Farmer, A., Griffiths, F., … Kinmonth, A. L. (2007). Designing and evaluating complex interventions to improve health care. BMJ, 334, 455–459. doi:10.1136/bmj.39108.379965.BE
- Cane, J., O'Connor, D., & Michie, S. (2012). Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science, 7, 37. doi:10.1186/1748-5908-7-37
- Carr, A. B., & Ebbert, J. (2012). Interventions for tobacco cessation in the dental setting. Cochrane Database of Systematic Reviews, 6, CD005084. doi:10.1002/14651858.CD005084.pub3
- Coleman, T. (2010). Do financial incentives for delivering health promotion counselling work? Analysis of smoking cessation activities stimulated by the quality and outcomes framework. BMC Public Health, 10, 167. doi:10.1186/1471-2458-10-167
- Collins, L. M., Baker, T. B., Mermelstein, R. J., Piper, M. E., Jorenby, D. E., Smith, S. S., … Fiore, M. C. (2011). The multiphase optimization strategy for engineering effective tobacco use interventions. Annals of Behavioral Medicine, 41, 208–226. doi:10.1007/s12160-010-9253-x
- Conner, N., & Norman, P. (2005). Predicting health behaviour: Research and practice with social cognition models ( 2nd ed.). Buckingham: Open University Press.
- Craig, P., Dieppe, P., Macintyre, S., Michie, S., Nazareth, I., & Petticrew, M. (2008). Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ, 337, a1655. doi:10.1136/bmj.a1655
- Cutrona, S. L., Choudhry, N. K., Stedman, M., Servi, A., Liberman, J. N., Brennan, T., … Shrank, W. H. (2010). Physician effectiveness in interventions to improve cardiovascular medication adherence: A systematic review. Journal of General Internal Medicine, 25, 1090–1096. doi:10.1007/s11606-010-1387-9
- Danaei, G., Ding, E. L., Mozaffarian, D., Taylor, B., Rehm, J., Murray, C. J., & Ezzati, M. (2009). The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Medicine, 6(4), e1000058. doi:10.1371/journal.pmed.1000058
- Davies, P., Walker, A. E., & Grimshaw, J. M. (2010). A systematic review of the use of theory in the design of guideline dissemination and implementation strategies and interpretation of the results of rigorous evaluations. Implementation Science, 5, 14. doi:10.1186/1748-5908-5-14
- Dombrowski, S. U., Sniehotta, F. F., Avenell, A., Johnston, M., MacLennan, G., & Araujo-Soares, V. (2012). Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychology Review, 6, 7–32. doi:10.1080/17437199.2010.513298
- Etter, J. F., & Perneger, T. V. (1999). A comparison of two measures of stage of change for smoking cessation. Addiction, 94, 1881–1889. doi:10.1046/j.1360-0443.1999.9412188113.x
- Everett, T., Bryant, A., Griffin, M. F., Martin-Hirsch, P. P. L., Forbes, C. A., & Jepson, R. G. (2011). Interventions targeted at women to encourage the uptake of cervical screening. Cochrane Database of Systematic Reviews, (5), CD002834. doi:10.1002/14651858.Cd002834.Pub2
- Ezzati, M., Lopez, A. D., Rodgers, A., Vander Hoorn, S., Murray, C. J. L., & Coll, C. R. A. (2002). Selected major risk factors and global and regional burden of disease. Lancet, 360, 1347–1360. doi:10.1016/S0140-6736(02)11403-6
- Festinger, L. (1954). A theory of social comparison processes. Human Relations, 7, 117–140. doi:10.1177/001872675400700202
- Fishbein, M., Triandis, H. C., Kanfer, F. H., Becker, M., Middlestadt, S. E., & Eichler, A. (2001). Factors influencing behaviour and behaviour change. In A. Baum, T. A. Revenson, & J. E. Singer (Eds.), Handbook of health psychology (pp. 3–17). Mahwah, NJ: Lawrence Erlbaum Associates.
- Francis, J. J., O'Connor, D., & Curran, J. (2012). Theories of behaviour change synthesised into a set of theoretical groupings: Introducing a thematic series on the theoretical domains framework. Implementation Science, 7, 35. doi:10.1186/1748-5908-7-35
- French, S. D., Green, S. E., O'Connor, D. A., McKenzie, J. E., Francis, J. J., Michie, S., … Grimshaw, J. M. (2012). Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the theoretical domains framework. Implementation Science, 7, 38. doi:10.1186/1748-5908-7-38
- Fuller, C., Michie, S., Savage, J., McAteer, J., Besser, S., Charlett, A., … Stone, S. (2012). The feedback intervention trial (FIT) – improving hand-hygiene compliance in UK healthcare workers: A stepped wedge cluster randomised controlled trial. PLoS One, 7(10), e41617. doi:10.1371/journal.pone.0041617
- Gardner, B., Wardle, J., Poston, L., & Croker, H. (2011). Changing diet and physical activity to reduce gestational weight gain: A meta-analysis. Obesity Reviews, 12, e602–e620. doi:10.1111/j.1467-789X.2011.00884.x
- Glanz, K., & Bishop, D. B. (2010). The role of behavioral science theory in development and implementation of public health interventions. Annual Review of Public Health, 31, 399–418. doi:10.1146/annurev.publhealth.012809.103604
- Glanz, K., & Rimer, B. K. (1997). Theory at a glance: A guide for health promotion practice. Bethesda, MD: National Cancer Institute.
- Glanz, K., Rimer, B. K., & Lewis, F. M. (Eds.). (2002). Health behavior and health education. Theory, research and practice. San Francisco, CA: Jossey-Bass.
- Gough, D., Thomas, J., & Oliver, S. (2012). Clarifying differences between review designs and methods. Systematic Reviews, 1, 28. doi:10.1186/2046-4053-1-28
- Hardeman, W., Sutton, S., Griffin, S., Johnston, M., White, A., Wareham, N. J., & Kinmonth, A. L. (2005). A causal modelling approach to the development of theory-based behaviour change programmes for trial evaluation. Health Education Research, 20, 676–687. doi:10.1093/Her/Cyh022
- Head, K., & Noar, S. M. (2013). Facilitating progress in health behaviour theory development and modification: The reasoned action approach as a case study. Health Psychology Review, 8, 34–52.
- House of Lords. (2011). Behaviour change. Science and technology select committee, 2nd Report of Session 2010. London: The Stationery Office (on authority of the House of Lords).
- Ivers, N., Jamtvedt, G., Flottorp, S., Young, J. M., Odgaard-Jensen, J., French, S. D., … Oxman, A. D. (2012). Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database of Systematic Reviews, 6, CD000259. doi:10.1002/14651858.CD000259.pub3
- Johnston, D. W., Jones, M. C., Charles, K., McCann, S. K., & McKee, L. (2013). Stress in nurses: Stress-related affect and its determinants examined over the nursing day. Annals of Behavioral Medicine, 45, 348–356. doi:10.1007/s12160-012-9458-2
- Kelly, M., Morgan, A., Ellis, S., Younger, T., Huntley, J., & Swann, C. (2010). Evidence based public health: A review of the experience of the National Institute of Health and Clinical Excellence (NICE) of developing public health guidance in England. Social Science and Medicine, 71, 1056–1062. doi:10.1016/j.socscimed.2010.06.032
- Kim, N., Stanton, B., Li, X., Dickersin, K., & Galbraith, J. (1997). Effectiveness of the 40 adolescent AIDS-risk reduction interventions: A quantitative review. Journal of Adolescent Health, 20, 204–215. doi:10.1016/s1054-139x(96)00169-3
- Littell, J. H., & Girvin, H. (2002). Stages of change: A critique. Behavior Modification, 26, 223–273. doi:10.1177/0145445502026002006
- Marteau, T., Dieppe, P., Foy, R., Kinmonth, A. L., & Schneiderman, N. (2006). Behavioural medicine: Changing our behaviour – A growing body of evidence shows how to make behavioural interventions effective. British Medical Journal, 332, 437–438. doi:10.1136/bmj.332.7539.437
- McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Education and Behavior, 15, 351–377. doi:10.1177/109019818801500401
- Michie, S. (2008). Designing and implementing behaviour change interventions to improve population health. Journal of Health Services Research and Policy, 13(Suppl. 3), 64–69. doi:10.1258/jhsrp.2008.008014
- Michie, S., & Abraham, C. (2004). Interventions to change health behaviours: Evidence-based or evidence-inspired? Psychology & Health, 19(1), 29–49. doi:10.1080/0887044031000141199
- Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychology, 28, 690–701. doi:10.1037/a0016136
- Michie, S., & Johnston, M. (2012). Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychology Review, 6, 1–6. doi:10.1080/17437199.2012.654964
- Michie, S., Johnston, M., Abraham, C., Lawton, R., Parker, D., Walker, A., & Psychological Theory Group. (2005). Making psychological theory useful for implementing evidence based practice: A consensus approach. Quality & Safety in Health Care, 14(1), 26–33. doi:10.1136/qshc.2004.011155
- Michie, S., Johnston, M., Francis, J., Hardeman, W., & Eccles, M. (2008). From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Applied Psychology, 57, 660–680. doi:10.1111/j.1464-0597.2008.00341.x
- Michie, S., & Prestwich, A. (2010). Are interventions theory-based? Development of a theory coding scheme. Health Psychology, 29(1), 1–8. doi:10.1037/a0016939
- Michie, S., & West, R. (2013). Behaviour change theory and evidence: A presentation to government. Health Psychology Review, 7, 1–22. doi:10.1080/17437199.2011.649445
- Mokdad, A. H., Marks, J. S., Stroup, D. F., & Gerberding, J. L. (2004). Actual causes of death in the United States, 2000. JAMA, 291, 1238–1245. doi:10.1001/jama.291.10.1238
- National Institute for Health and Care Excellence. (2007). Behaviour change at population, community and individual levels [NICE public health guidance 6]. London: Author.
- National Institute for Health and Clinical Excellence. (2010). Health systems and health-related behaviour change – A review of primary and secondary evidence. London: Author.
- Nigg, C. R., Allegrante, J. P., & Ory, M. (2002). Theory-comparison and multiple-behavior research: Common themes advancing health behavior research. Health Education Research, 17, 670–679. doi:10.1093/Her/17.5.670
- Noar, S. M., Benac, C. N., & Harris, M. S. (2007). Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychological Bulletin, 133, 673–693. doi:10.1037/0033-2909.133.4.673
- Noar, S. M., & Zimmerman, R. S. (2005). Health behavior theory and cumulative knowledge regarding health behaviors: Are we moving in the right direction? Health Education Research, 20, 275–290. doi:10.1093/her/cyg113
- Office of Behavioural and Social Sciences Research. (2006). Healthier lives through behavioral and social science research. Bethesda, MD: Author.
- Painter, J. E., Borba, C. P. C., Hynes, M., Mays, D., & Glanz, K. (2008). The use of theory in health behavior research from 2000 to 2005: A systematic review. Annals of Behavioral Medicine, 35, 358–362. doi:10.1007/s12160-008-9042-y
- Parkin, D. M., Boyd, L., & Walker, L. C. (2011). The fraction of cancer attributable to lifestyle and environmental factors in the UK in 2010. British Journal of Cancer, 105(Suppl. 2), S77–S81. doi:10.1038/bjc.2011.489
- Prestwich, A., Sniehotta, F. F., Whittington, C., Dombrowski, S. U., Rogers, L., & Michie, S. (2013). Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychology, 33, 465–474. doi:10.1037/a0032853
- Rice, V. H., & Stead, L. F. (2008). Nursing interventions for smoking cessation. Cochrane Database of Systematic Reviews, (8), CD001188. doi:10.1002/14651858.Cd001188.Pub3
- Roe, L., Hunt, P., Bradshaw, H., & Rayner, M. (1997). Health promotion interventions to promote healthy eating in the general population: A review. London: Health Education Authority.
- Rothman, A. J. (2004). “Is there nothing more practical than a good theory?” Why innovations and advances in health behavior change will arise if interventions are used to test and refine theory. International Journal of Behavioral Nutrition and Physical Activity, 1, 11. doi:10.1186/1479-5868-1-11
- Rothman, A. J. (2009). Capitalizing on opportunities to refine health behavior theories. Health Education & Behavior, 36, 150s–155s. doi:10.1177/1090198109340514
- Sheeran, P. (2002). Intention-behaviour relations: A conceptual and empirical overview. European Review of Social Psychology, 12(1), 1–36. doi:10.1080/14792772143000003
- Shemilt, I., Simon, A., Hollands, G. J., Marteau, T. M., Ogilvie, D., O'Mara-Eves, A., … Thomas, J. (2013). Pinpointing needles in giant haystacks: Use of text mining to reduce impractical screening workload in extremely large scoping reviews. Research Synthesis Methods, 5(1), 31–49. doi:10.1002/jrsm.1093
- Solomon, S., & Kington, R. (2002). National efforts to promote behavior-change research: Views from the Office of Behavioral and Social Sciences Research. Health Education Research, 17, 495–499. doi:10.1093/her/17.5.495
- Steinijans, V. W., Diletti, E., Bomches, B., Greis, C., & Solleder, P. (1997). Interobserver agreement: Cohen's kappa coefficient does not necessarily reflect the percentage of patients with congruent classifications. International Journal of Clinical Pharmacology and Therapeutics, 35, 93–95.
- Stephenson, J. M., Imrie, J., & Sutton, S. R. (2000). Rigorous trials of sexual behaviour interventions in STD/HIV prevention: What can we learn from them? AIDS, 14(Suppl. 3), S115–S124.
- Summerbell, C. D., Waters, E., Edmunds, L. D., Kelly, S., Brown, T., & Campbell, K. J. (2005). Interventions for preventing obesity in children. Cochrane Database of Systematic Reviews, 2011(12), CD001871.
- Swann, C., Bowe, K., Kosmin, M., & McCormick, G. (2003). Teenage pregnancy and parenthood: A review of reviews. Evidence briefing. London: Health Development Agency.
- Taylor, N., Conner, M., & Lawton, R. (2011). The impact of theory on the effectiveness of worksite physical activity interventions: A meta-analysis and meta-regression. Health Psychology Review, 6, 33–73. doi:10.1080/17437199.2010.533441
- Taylor, S. E. (1983). Adjustment to threatening events: A theory of cognitive adaptation. American Psychologist, 38, 1161–1173. doi:10.1037/0003-066X.38.11.1161
- Webb, T. L., Joseph, J., Yardley, L., & Michie, S. (2010). Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. Journal of Medical Internet Research, 12(1), e4. doi:10.2196/jmir.1376
- Weinstein, N. D. (2007). Misleading tests of health behavior theories. Annals of Behavioral Medicine, 33(1), 1–10. doi:10.1207/s15324796abm3301_1
- Weinstein, N. D., & Rothman, A. J. (2005). Commentary: Revitalizing research on health behavior theories. Health Education Research, 20, 294–297. doi:10.1093/her/cyg125
- West, R. (2005). Time for a change: Putting the Transtheoretical (Stages of Change) Model to rest. Addiction, 100, 1036–1039. doi:10.1111/j.1360-0443.2004.00995.x
- West, R. (2006). Theory of addiction. Oxford: Blackwell.
- Whitelaw, S., Baldwin, S., Bunton, R., & Flynn, D. (2000). The status of evidence and outcomes in stages of change research. Health Education Research, 15, 707–718. doi:10.1093/her/15.6.707
