
ABSTRACT
Breastfeeding has many known benefits, but rates vary globally. We propose two main reasons why psychological theory and interventions have not been successful to date in explaining breastfeeding behaviours. Specifically, prior research underestimates the importance of (1) specific emotions and (2) wider injunctive influences (i.e., societal and moral norms about what women feel they ought to be doing) in the breastfeeding experience. Therefore, we conducted a systematic review of quantitative, qualitative, and mixed-methods studies that explored whether injunctive norms and/ or specific emotions are associated with breastfeeding behaviours (i.e., intentions, initiation and duration). Seventy-two papers were included in this review; data were extracted and quality appraisals conducted for all included studies. A meta-analysis of effect sizes was performed with the quantitative data. A convergent qualitative synthesis of the data was conducted, resulting in the following line of argument: Breastfeeding is a social behaviour and not a personal/individual behaviour. From this line of argument, three themes with associated sub-themes were developed, highlighting the importance of both specific emotions and injunctive norms on breastfeeding behaviours. These influences are discussed in relation to both theoretical and practical implications, as well as future research.
Breastfeeding has the potential to improve the health and wellbeing of parents and babies, as there are many known psychological, nutritional, and physical benefits. The World Health Organisation (WHO) recommends that women breastfeed their babies exclusivelyFootnote1 until six months of age, and continues beyond that alongside complementary feeding. However, breastfeeding rates globally are low, particularly in developed countries (Victora et al., Citation2016). For example, the UK initiation rate is 81% but only 34% of women are breastfeeding at six-months (1% exclusive breastfeeding; McAndrew et al., Citation2012). In order to improve breastfeeding behaviours, a range of different interventions have been implemented and evaluated, with mixed success. Prior research and reviews identified the following to be effective breastfeeding promotion techniques: peer support, father support, professional support (e.g., informational support from health professionals), education, such as antenatal classes (alone or in combination with peer/professional support), professional training (training about positioning and latching), hospital practices/initiatives, multi-sectorial initiatives, and media programmes (Dyson et al., Citation2006, Citation2010a).
One promising way to encourage breastfeeding behaviours is to use social psychological methods, such as focusing on social support and/or social cognitive variables (e.g., self-efficacy) when designing interventions. A recent meta-analysis has examined whether social psychological interventions impact (1) initiation of breastfeeding, (2) duration of any breastfeeding, and (3) exclusive breastfeeding (Davie et al., Citation2019). Firstly, it was found that social psychological interventions were successful at improving breastfeeding initiation; however, the quality of evidence was low. Secondly, focusing on breastfeeding duration, it was found that social psychological interventions did not encourage a longer duration of any breastfeeding. Finally, after controlling for publication biases, these interventions did not improve exclusive breastfeeding rates. Based on these results it can be concluded that social psychological interventions may not be as promising as hoped. Within the meta-analysis Davie et al. (Citation2019) identified that one of the problems with the social psychological studies included in their review, was that interventions were often not based on theoretical models, despite the recommendation of both the Medical Research Council (MRC) complex intervention framework (O’Cathain et al., Citation2019) and the National Institute for Health and Care Excellence (NICE) guidelines.
In terms of examining breastfeeding behaviours as an outcome, research has examined different forms of behaviours, including intentions, initiation, and duration (Bai et al., Citation2019; Davie et al., Citation2019). Additionally, some studies focus on exclusive breastfeeding (i.e., only breast milk directly from breast or expressed) and some studies focus on any breastfeeding. Therefore, in terms of studying breastfeeding there is a large range of possible outcomes, which makes it difficult to assess the evidence across multiple studies.
To complicate matters further it has been revealed that diverse psychological (e.g., mental health and self-views), contextual (e.g., country and regional level difference), and demographic factors (e.g., age, ethnicity, and socioeconomic status) influence breastfeeding rates, in terms of intentions, initiation, and duration (e.g., Dyson et al., Citation2006; Lawton et al., Citation2012; Lou et al., Citation2014; McMillan et al., Citation2008; Swanson et al., Citation2017). Prior research has identified many physical and practical barriers to successful breastfeeding, such as employment and maternity leave allowances, caring for older siblings, pain, low milk supply, and lack of access to professional support (see Patil et al., Citation2020 for a review). Additionally, there are mental health conditions, such as depression (Dennis & McQueen, Citation2009; Dias & Figueiredo, Citation2015) and anxiety (Hoff et al., Citation2019) which have been found to impact breastfeeding behaviours. Finally, social support (Raj & Plichta, Citation1998) and social cognitive factors (Lau et al., Citation2018), such as self-efficacy, are also known to impact breastfeeding outcomes.
We propose that there are two main reasons why psychological factors have been unable to fully explain breastfeeding behaviours. First, prior research underestimates the importance of specific emotions in the breastfeeding experience, focusing heavily on social cognitive components, such as self-efficacy and perceived behavioural control (see Bai et al., Citation2019; Lau et al., Citation2018), rather than emotional aspects. In the case of self-efficacy interventions these are primarily individualised rather than incorporating societal level influences (Bai et al., Citation2019). Second, prior research underestimates the importance of wider injunctive influences (i.e., social conventions and moral obligations about what women feel they ought to be doing), instead focusing heavily on subjective norms (i.e., what significant others think they should be doing or social pressure from significant others).
Therefore, to address this identified gap, we conducted a meta-analysis and systematic review of quantitative, qualitative, and mixed-methods studies that explored whether injunctive norms and/or emotions influence breastfeeding behaviours (i.e., intentions, initiation, and duration, including both any or exclusive breastfeeding behaviours).
Why examine specific emotions and wider injunctive norms?
The Theory of Planned Behaviour (TPB) posits that intentions are the most direct predictor of behaviour, and that intentions are predicted by attitudes, subjective norms, and perceived behavioural control (Ajzen, Citation1991). Whilst TPB can help explain some health behaviours, including breastfeeding behaviours (see Bai et al., Citation2019 for a review), there does appear to be some unexplained variance in predicting actual behaviours, rather than just intentions to perform a behaviour. Two variables, moral norms and anticipated affect, have been applied to help explain this variance in predicting health behaviours in general (Rivis et al., Citation2009), but not breastfeeding behaviours specifically.
Anticipated affect, the degree to which someone perceives that they will experience certain emotions if they either do or do not perform a behaviour, was incorporated because it was found that the original TPB model performed less well in predicting behaviours that had a strong emotional basis (see Rivis et al., Citation2009 for a review). Prior research has found that anticipated affect makes a unique contribution in predicting behavioural intentions above the other TPB factors (Rivis et al., Citation2009). In terms of affect or emotions in general, anticipated emotions have been found to be distinct from affective attitudes (Stevens et al., Citation2019). Affective attitudes (e.g., liking) are better predictors than cognitive attitudes of health behaviours, such as consuming fruit and vegetables or quitting smoking etc. (Lawton et al., Citation2009). However, affective attitudes normally focus on positive or negative evaluations, rather than specific emotions, which is problematic because specific emotions are often stronger predictors of distinct behaviours than global attitudes (Mackie & Smith, Citation2017). In terms of anticipated affect it should also be considered that people may feel different emotions in the moment, or when reflecting on past experiences, than they anticipate feeling in the future. Therefore, we propose that in understanding breastfeeding behaviours, it is not only important to examine affective attitudes and anticipated affect, but to also examine experienced or recalled emotions.
Previous research on the experienced emotions of women in relation to their breastfeeding behaviours indicates that self-conscious emotions (e.g., shame, guilt, embarrassment, and regret) play a role in breastfeeding experiences and infant feeding choice (e.g., Fallon et al., Citation2017; Komninou et al., Citation2017; Shepherd et al., Citation2017; Thomson et al., Citation2015). For example, Shepherd and colleagues reported that anticipated regret and anticipated pride positively predict exclusive breastfeeding duration (Shepherd et al., Citation2017). There is also evidence that mothers who give their baby formula milk experience feelings of guilt because of their feeding choice (Fallon et al., Citation2017; Komninou et al., Citation2017), and that embarrassment can be a perceived barrier to breastfeeding (e.g., Dyson et al., Citation2006). Finally, Thomson and colleagues found that both breastfeeding and non-breastfeeding mothers experienced shame because of their infant feeding choice (Thomson et al., Citation2015).
There has not, however, been a systematic investigation of which specific emotions (such as shame, guilt, or embarrassment) play a role in breastfeeding outcomes. Additionally, prior research has primarily focused on negative emotions rather than positive emotions, with the exception of Shepherd et al. (Citation2017), who examined anticipated pride. Therefore, in this systematic review and meta-analysis we aimed to identify which specific emotions play a role in breastfeeding, whether anticipated or experienced, and when they play a role, specifically whether this is in facilitating intentions, initiation, or breastfeeding duration.
In addition to anticipated affect, the extended TPB model also predicts that moral norms play a role in facilitating health behaviours (Rivis et al., Citation2009). A moral norm refers to the perceived moral obligation or moral correctness of performing a particular behaviour. Typically, TPB when applied to breastfeeding behaviours, has focused on subjective norms, specifically pressure from significant others, or knowledge of whether others think they should or should not breastfeed. Therefore, the subjective norms influence is from someone that is important to the individual engaging in the behaviour although subjective norms have not been found to consistently predict breastfeeding duration (Lau et al., Citation2018). However, it is possible that wider societal norms and moral norms also impact breastfeeding experiences and behaviours. Social domain theory (Turiel, Citation1983) distinguishes between two forms of social knowledge, social conventions and moral beliefs, with prior research indicating that people distinguish between these two types of norms/social knowledge (see Lourenço, Citation2014 for a review). According to domain theory, moral norms differ from social conventions in the assumption of universality; moral norms can also exist independent of social rules and authorities. In the context of breastfeeding, this means that if someone endorses a moral norm about breastfeeding, there is the belief that breastfeeding is morally correct and there is a moral obligation to breastfeed, not just a social obligation from significant others or wider society. As a result, it can be argued that although subjective norms, societal norms, and moral norms are all similar, being types of injunctive normative influence, (i.e., they all focus on what people think they ought to be doing), they nonetheless differ in focus. Therefore, we aimed to go beyond subjective norms and identify wider injunctive norms (societal and moral) that may be important in breastfeeding experiences and behaviour.
In summary, this mixed studies systematic review and meta-analysis aimed to explore the role of specific emotions and injunctive norms in breastfeeding behaviours (i.e., intentions, initiation, and duration). We include studies with a mix of research designs (qualitative, quantitative, and mixed-methods) to address the complex research questions and behaviours and to allow the qualitative findings to further explain the quantitative findings. We assess how specific emotions (positive versus negative) and different forms of injunctive influences (subjective versus societal versus moral) are associated with breastfeeding outcomes (intentions, initiation, and duration) by performing meta-analyses for the different quantitative relationships. Additionally, through an exploration of qualitative findings, we highlight other factors and complexities that will not be evident through the quantitative results.
Methods
Design
We conducted a systematic search of qualitative, quantitative, and mixed-methods studies that explored the role of injunctive norms and/or emotions on breastfeeding behaviours (intention, initiation, and/or duration). Qualitative, quantitative, and mixed-methods data were included in the synthesis; the quantitative data (including relevant data from mixed-methods studies) extracted for meta-analysis. The review was registered on the PROSPERO database (registration number CRD42018112720) and has been reported in line with the PRISMA (Preferred Reporting for Systematic Reviews and Meta-Analyses) checklist.
Inclusion criteria
Inclusion criteria for studies were developed based on the PICOCS (Participants, Intervention, Comparator, Outcome, Context, Study Design) acronym (Petticrew & Roberts, Citation2006), as recommended by The Centre for Research and Dissemination (Citation2009). As the review was not restricted to intervention studies that elicited either injunctive norms or emotions, the ‘Intervention’ element of PICOCS was combined with ‘Comparator’ and adapted to ‘Influences’, as the constructs of interest were either injunctive norms about breastfeeding or breastfeeding-related emotions. Only studies published in peer-reviewed journals in English were included. No date restrictions were set.
Participants. We included studies in which women with children, or expectant women were the participants. Studies that focused on the attitudes or intentions of groups, such as high-school students or doctors, were excluded, unless they were specifically targeting parents or parents-to-be within these groups.
Influences. We examined two types of influencing factors: injunctive norms and specific emotions related to breastfeeding. We focused on two different types of injunctive norms: (1) moral norms, defined as breastfeeding being perceived as a moral issue (i.e., moral correctness, moral obligation), and (2) social norms, defined as a perception that others think they should or should not breastfeed (i.e., social pressure, social obligation). The social norm factor was split into subjective norms (i.e., from significant others) and societal norms (i.e., from wider society). Emotion was defined as state emotions/affect related specifically to breastfeeding (e.g., guilt, shame, or joy about breastfeeding); therefore, emotion/affect in included studies could be either positive or negative and either anticipated or experienced. Studies that explored trait low-mood or parental mood more broadly (e.g., post-natal depression or mood disorders) were excluded, as these do not focus on the experience of specific state emotions.
Outcomes. The outcomes were breastfeeding behaviours, including intentions, initiation, and duration. We included exclusive breastfeeding and breastfeeding of any kind, as previous definitions of exclusive breastfeeding are mixed.
Context. No restrictions were set with regards to the context, setting, or location of included studies.
Study design. All study designs were included in order to better understand these complex behaviours and influences.
Search strategy and screening
The following databases were searched by SG during October and November 2018, (with the searches repeated in November 2019): CINAHL, Cochrane Database of Systematic Reviews, Embase, ProQuest Dissertations and Theses Global (doctoral dissertations only), Psychology Cross Search, and PubMed.
Search terms were developed based on those used in two previous reviews, (Lau et al., Citation2018; Rivis et al., Citation2009), plus the emotion terms covered in two recent surveys of mothers (Russell, Birtel, Smith, Hart, & Newman, under review; Shepherd et al., Citation2017). Search terms and the search strategy were piloted in one database to ensure relevant studies were being returned and to test the effects of including different terms relating to parents and parents-to-be. The search terms can be found in ; additionally the basic search strategy and an example of a final search are reported in Appendix A.
Table 1. Keywords for search terms.
For the original searches, titles and abstracts of articles retrieved from databases were screened by SG against the inclusion criteria. Any studies that appeared to include at least one measure of a construct of interest (emotions, moral norms, societal norms, subjective norms) and at least one outcome measure of interest (breastfeeding intentions, initiation, or duration) were marked for full-text review, regardless of study design. A random 10% sample of screened abstracts (n = 442) was reviewed by SR; agreement rate regarding inclusion/exclusion between SG and SR was initially 81.7%. Discussion revealed that SG had been over-inclusive of abstracts that referred to variables in vague terms, such as ‘maternal characteristics’; further investigation of a sample of 19 papers demonstrated that abstracts with these terms did not include any of the psychosocial variables of interest and were only reporting demographic information about participants. It was agreed that abstracts that did not explicitly refer to psychosocial terms (e.g., attitudes, intentions, emotions) should therefore be excluded. After amending SG's screening to exclude such abstracts, the agreement rate on the 10% sample of abstracts was 99.1%.
After abstract screening, hand-searching was performed by SG on relevant systematic reviews identified from the database searching and on the final set of papers that were included in the review after full-text screening was completed. Full-text review was then conducted by SR and DS (both authors reviewed all of the papers independently). Agreement was satisfactory (Kappa = .67; Frequencies: Agree = 85.8%, Disagree = 14.2%); where there was disagreement a third reviewer (MB or KH) made an independent decision to resolve the disagreement.
The original searches were repeated to see if any additional papers were published between November 2018 and November 2019. SR did both the abstract/title screening and the full text review for these updated searches.
Data extraction and quality appraisal
Data were extracted according to pre-defined criteria (see Appendix B). Each paper was evaluated using the QATSDD 16 item quality assessment tool (Sirriyeh et al., Citation2012), as there were quantitative, qualitative, and mixed-method studies. Fourteen criteria are applicable to quantitative studies, 14 to qualitative and 16 to mixed-methods studies; each criterion requires the assessor to rate the paper on a score from 0 Not at all to 3 Complete. The sum of each criterion, and then a percentage of the total score are calculated. Before completing the data extraction and quality appraisals, SR and DS reviewed four papers to trial both the data extraction and quality appraisal methods. Data extraction and quality assessments were then completed by SR and DS. Due to methodological expertise SR reviewed quantitative papers and DS reviewed qualitative and mixed-methods papers. Twenty papers were checked for consistency and application by KH and MB, which revealed very minor differences in the quality appraisals for four papers; these differences did not substantively affect the ratings given in the appraisals. No differences were identified in the data extraction.
Data analysis: Quantitative Findings only
For studies that included quantitative results we extracted effect sizes for the relationship between breastfeeding outcomes (intentions, initiation, and duration) and either positive emotions, negative emotions, subjective norms, societal norms, or moral norms. Effect sizes (e.g., correlations) were transformed using Comprehensive Meta-Analysis (CMA) Software. Some studies only reported regressions, so regression coefficients were first transformed into correlations using Peterson and Brown's (Citation2005) formula, before computing overall effect sizes in CMA. For our analysis we used random effects models.
Data synthesis: qualitative, mixed-methods, and quantitative findings
A convergent qualitative synthesis was conducted following data extraction and quality assessment (Gough, Citation2015; Pluye & Hong, Citation2014). Taking this approach allows an interpretative angle to be applied to the papers providing an amalgamated interpretation of complex behaviours through an inductive thematic synthesis (Thomas & Harden, Citation2008). The findings from all the papers (mixed-methods, qualitative and quantitative studies) were included in the synthesis; this included all themes, concepts, and quotes (raw data) stated in the results, findings or discussion sections. Once these data were extracted, the six steps of thematic analysis as proposed by Braun and Clarke (Citation2006) were followed. Two reviewers (DS and SR) independently familiarised themselves with the extracted textual data and descriptive themes based on the themes presented in each paper were developed (stages 1 & 2). These themes were then discussed between both reviewers by returning to the extracted data and in relation to the literature, study characteristics, and the review research question (stage 3 and 4); these were then presented as interpretative themes of the review papers (stage 5) and writing (stage 6). During this process of synthesis, it became evident that the themes constructed from the data were naturally explained by one statement. Thus, a line of argument as traditionally developed when following a meta-ethnographic approach to synthesis (Noblit & Hare, Citation1988) was used.
Results
Studies included in the review
The PRISMA flowchart and study screening details are shown in . A total of 5,596 titles were identified from the database searches, of which 1,193 were duplicates. This left 4,403 abstracts to be screened, of which 4,121 were excluded, leaving 282 records for full-text review from the database searches. During database screening, 31 potentially relevant literature reviews were identified; the reference lists of which were screened, identifying a further three literature reviews. From the screening of these reviews’ reference lists, an additional 68 articles were retrieved for full-text review.
Figure 1. PRISMA flowchart.
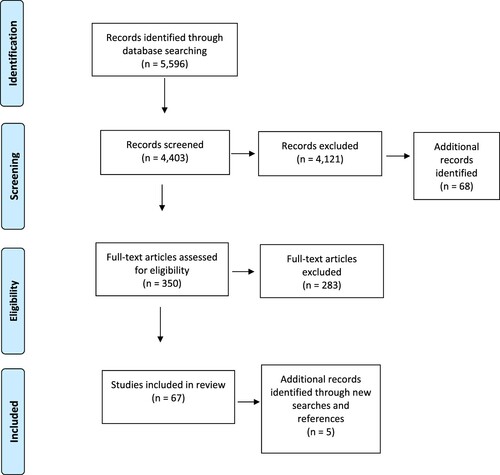
After sourcing these 350 [282 + 68] articles for full-text review, 52 articles were excluded from the review as the full-texts could not be sourced. We also decided to exclude the 62 doctoral theses as there were issues in terms of both quality and accessibility. One hundred and sixty nine articles were excluded during full-text review as they did not meet the inclusion criteria for the following reasons: Not published in English (1), Duplicate (2), Not empirical research (21), Wrong sample or Collapses across parent with other sample (e.g., clinicians, general population) (8), Outcome(s) not relevant/do not fit with search terms (3), Influences(s) not relevant/do not fit with search terms (55), Influence(s) and Outcome(s) not relevant/do not fit with search terms (41), Outcome(s) not clearly measured/ discussed, so cannot tell how predictors relate to outcomes (38).
This left an initial total of 67 articles that met the inclusion criteria and explored the impact of injunctive norms (subjective, societal, or moral), and/or emotions on breastfeeding intentions, initiation, or duration. The reference lists of these 67 articles were then reviewed to identify additional potentially relevant articles; this process was repeated until no new articles were identified and resulted in one additional reference being found.
The searches were repeated in November 2019, in which a total of 627 titles were identified from the database searches, of which 139 were duplicates. This left 488 abstracts to be screened, of which 481 were excluded, leaving seven records for full-text review from the database searches. Three articles were excluded as they did not meet the inclusion criteria (one could not be accessed, one did not include relevant outcomes, one was not empirical research). Therefore, four papers were identified from these additional searches, resulting in a total of 72 papers included in the review.
Quality assessment
For the quantitative papers, the quality assessment scores ranged from 31% to 91% (average 61%). Most studies outlined details about the research setting and methods of recruitment, while very few provided clear justification of sample size or had user involvement. For the qualitative papers, the quality assessment scores ranged from 24% to 57% (average 36%). For the mixed-method papers, the quality assessment scores ranged from 23% to 54% (average 34%). Like the quantitative papers it was fairly common that recruitment methods were detailed for qualitative and mixed-method papers; however, details about analytical methods or user involvement were sparse. Overall the quality assessments for the qualitative and mixed methods papers were far lower than for the quantitative approaches; therefore, results from these papers need to be interpreted cautiously. Quality appraisals for all papers can be found on the Open Science Framework OSF (https://osf.io/zqdum/?view_only=c9f5419b295245398241dab3232ca9b2).
Study characteristics
The full data extraction table can be found in the above OSF link; however, a summary of the main study characteristics can be found below.
Design and method of analysis. The majority of the articles were quantitative (45 papers), primarily cross-sectional surveys (Cross-sectional Survey = 28, Cohort = 6, Longitudinal = 6, Trial/Experimental = 5). Of these quantitative papers, 34 used regression analyses to test the main hypothesis, eight papers examined differences across conditions or groups (e.g., via ANOVAs or frequencies), and 3 papers used modelling (e.g., SEM). There were 17 qualitative and 10 mixed-methods papers, using the following methods of analysis: Framework analysis = 2, Grounded theory = 1, Thematic analysis = 4, Interpretative phenomenological analysis = 4, Content analysis/coding = 8, Unclear = 8.
Sample. Sample sizes ranged from 6 to 10,834 (Qualitative 6–36, Mixed 25–900, Quantitative 50–10,834). As highlighted by the quality assessment, sample size was frequently not justified in detail. There was a wide range of participant ages, from 15 to 55 years, with most samples having a mean age from the late 20s to mid-30s. A large proportion of studies did not report ethnicity; however, those that did had diverse samples. Of the studies that reported marital status, the percentage of married or committed couples ranged from 24% to 99%. Not all the studies reported parity; the lowest proportion of prima-parous was 33%, whilst some studies aimed to recruit only prima-parous mothers.
Time period. Nearly half the studies collected data at more than one time point (33 papers, 46%). Some started recruitment antenatally and continued for up to 2 years (over 2 years was the largest range, though most samples included babies younger than 6 months, i.e.,). Some studies involved recalling previous experience.
Country. There was a large range of countries sampled (n=20). Studies were primarily from the USA or the UK; however, some can be considered under-represented samples (e.g., Vietnam and Turkey). The following countries were sampled: UK (21, nearly half were from England), USA (20), China (4), Ireland (3), Iran (3), Australia (2), Canada (2), Malaysia (2), Netherlands (2), Unclear (2), Finland (1), Ghana (1), Indonesia (1), Israel (1), Korea (1), Mexico (1), Puerto Rico (1), Spain (1), Thailand (1), Turkey (1), Vietnam (1).
Outcome measures. Only five papers measured intentions, initiation, and duration together. Most studies included a measure of breastfeeding duration (n = 54). Over half of the papers included a measure of breastfeeding intentions (n = 40). There were fewer studies that included a measure of breastfeeding initiation (n = 26). For all of the outcome measures there was a large range in terms of breastfeeding definitions (i.e., exclusive, any, or not specified). Most papers used self-report measures for assessing breastfeeding behaviours. There were no differences in the frequency of studies measuring norms or emotions based on breastfeeding outcome measure.
Emotions and injunctive norms identified. Specific emotions were commonly identified as impacting the breastfeeding experience and actual behaviour (n = 42). Differing from the extended TPB, most research focused on emotions experienced during breastfeeding or when reflecting on one's breastfeeding experience, with very few studies including a measure of anticipated emotion. A large proportion of the papers measured some form of injunctive norms (n = 56), with most of these including perceived subjective norms.
Meta-analysis of effect sizes
We aimed to examine how much specific emotions (e.g., shame, guilt, embarrassment, enjoyment) and injunctive norms (subjective, societal, and moral) were associated with the different breastfeeding outcomes (intention, initiation, and duration). However, findings were lacking in some areas, so it was deemed necessary to collapse across breastfeeding outcomes, and to treat positive and negative emotions as separate factors, but not to look at specific emotions. We ran five separate meta-analyses to examine these relationships, the overall effect size statistics for which can be found in . Additionally, individual effect size and forest plots can be found in the OSF link.
Table 2. Overall effect sizes for each influencing factor.
Four papers reported an effect size for the relationship between positive emotions and breastfeeding outcomes (5 individual effect sizes); the overall correlation was significant, and suggested there was a positive relationship, r = 0.24, p =.007, 95% CI [0.07, 0.040]. When focusing on negative emotions, four individual effect sizes were included from two papers; however, the overall effect was not found to be significant, r = 0.50, p = 0.12, 95% CI [0.21, 1.19]. It is important to note that eighteen studies which focused on negative emotions did not include a relevant effect size for the relationship between negative emotions and breastfeeding outcomes. Of these, fifteen were focusing on embarrassment, and these studies only indicated that embarrassment was present, not how much it is associated with breastfeeding outcomes.
In terms of the injunctive norms, 47 effect sizes for subjective norms were included, 7 effect sizes for societal norms, and 9 effect sizes for moral norms. For the subjective norms, the majority of studies included intentions as an outcome (24 individual effects for intentions; 19 for duration, and 4 for initiation). The overall relationship between subjective norms and all breastfeeding outcomes (intentions, initiation, and duration) was significant, r = 0.26, p <.001, 95% CI [0.19, 0.319]. The overall analyses of subjective norms were followed up with three additional analyses of the relationship between subjective norms and specific behaviours. It was found that the relationship between subjective norms and intentions, r = 0.39, p <.001, 95% CI [0.314, 0.454] was stronger than that between subjective norms and duration r = 0.18, p <.001, 95% CI [0.113, 0.25]. The relationship between subjective norms and initiation was not significant, r = 0.11, p = 0.42, 95% CI [−0.15, 0.35].
Looking at the wider injunctive norms, the overall relationship between societal norms and all breastfeeding behaviours was not significant, r = 0.24, p =.23, 95% CI [−0.149, 0.562]. However, the relationship between moral norms and breastfeeding outcomes was significant, r = 0.28, p=0.048, 95% CI [0.003, 0.516]. Therefore, based on the results of the meta-analysis, there is evidence that positive emotions, subjective norms, and moral norms are associated with breastfeeding outcomes; there is, however, a current lack of quantitative evidence for any association between breastfeeding outcome and negative emotions or societal norms. Additionally, it should be noted that effect sizes were heterogenous across studies for each of the five analyses (see ), which suggests substantial differences across studies.
Synthesis of findings
Taking a convergent qualitative synthesis approach to understanding the qualitative data, we generated three themes and developed a line of argument to address our research question. As stated above, the reporting of injunctive norms or emotions based on one type of breastfeeding behaviour alone was not evident in the findings. Thus, the line of argument and the themes cover all breastfeeding behaviours from intentions through to duration and have not been split according to breastfeeding behaviour unless useful. The line of argument and three themes with associated sub-themes are outlined in turn and where possible (see ) data from the included 72 papers are used to demonstrate the themes. Due to the data being presented in the original papers in a number of ways (e.g., with and without participant details), no participant demographics are presented with quotes.
Figure 2. Overview of themes and subthemes.
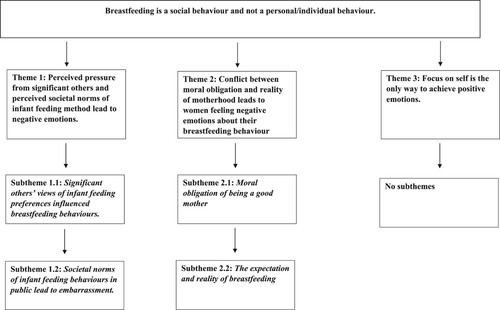
Line of argument: Breastfeeding is a social behaviour and not a personal/individual behaviour.
Underpinning the infant feeding behaviour of some women in the included studies was the view that breastfeeding was a social behaviour rather than an individual behaviour, due to the strong effect of social (societal and subjective) and moral norms, which influenced the emotions they felt. Societal norms of breastfeeding were found to be reflective of society's image of a good mother and sometimes impacted on women's perceived expectations of becoming a breastfeeding mother, which created a moral norm around breastfeeding being a moral obligation of a mother rather than a personal choice. When breastfeeding behaviours did not follow women's expectations, this was related to the expression of several negative emotional responses. Societal norms of infant feeding choices being linked to the image of a good mother and pressure from significant others led to many women reporting feeling pressure to breastfeed, in turn resulting in negative emotions, such as guilt and embarrassment, based on their infant feeding preferences. In particular, women reported feeling embarrassed to breastfeed in front of others (including friends and family). The disconnect between the expectation of being a mother who is morally obligated to breastfeed and the reality of breastfeeding, sometimes resulted in feeling like a failure and experiencing associated negative emotions, i.e., guilt. Positive emotions were only reported when women put aside these social pressures and moral obligations to focus purely on their own beliefs and desires around infant feeding. In these instances, positive emotions such as satisfaction and emotional bonding were felt by women. However, because so many of the studies had research questions that focused on the barriers to breastfeeding, rather than what encourages breastfeeding, there was far less focus on positive emotions in the questions being asked. The three themes presented below further demonstrate the interplay between injunctive norms (subjective, societal, and moral norms) and women's emotions regarding their infant feeding behaviours.
Theme 1: Perceived pressure from significant others and perceived societal norms of infant feeding method lead to negative emotions.
Negative emotions, namely embarrassment, were found to result from some women reporting feeling external pressure regarding their infant feeding choice from significant others (friends and family) and perceived societal norms. The perceived societal and subjective norms were, in most cases, highlighting the importance of breastfeeding but in a few instances norms demonstrated a preference for formula feeding. This theme was supported by 59 of the 72 studies, with data to support this theme identified across 40 quantitative studies, 10 qualitative, and 9 mixed-methods studies. Two subthemes further explain this process from social norms (societal and subjective) to negative emotions and the impact on breastfeeding behaviour. For this theme, there was some difference regarding breastfeeding behaviour.
I’d also try to keep my awareness of how other people feel because I know that some people find it really embarrassing. (in Murphy, Citation1999)
'There's a lot there's still a lot of negative attitudes out there that you see in the media with people especially with public breastfeeding. (in Newman & Williamson, Citation2018)
Subtheme 1.1: Significant others’ views of infant feeding preferences influenced breastfeeding behaviours.
Some women perceived pressure from friends and family to feed according to their friends’ and families’ preferences (i.e., subjective norms), which often undermined the breastfeeding experience for women (Nuampa et al., Citation2018; Took et al., Citation2009; Rempel, Citation2004). In most instances, breastfeeding was favoured but, in some cases, breastfeeding was not approved of (Bai et al., Citation2009). The norms of certain individuals were highlighted as particularly important to the women, such as partners (Natan et al., Citation2016; Tarkka et al., Citation1999) and midwives/nurses (Swanson & Power, Citation2005). Subjective norms impacted breastfeeding intentions (Bartle & Harvey, Citation2017; Dodgson et al., Citation2003; Ismail et al., Citation2014; McMillan et al., Citation2009; Mitra et al., Citation2004; Natan et al., Citation2016; Saunders-Goldson & Edwards, Citation2004; Swanson & Power, Citation2005) and breastfeeding duration (Bajoulvand et al., Citation2019; Brown & Jordan, Citation2013; Hauff et al., Citation2014; O’Campo et al., Citation1992; Tuan et al., Citation2014; Zhang et al., Citation2018). However, subjective norms were at times a weak predictor of their intentions to breastfeed (Avery et al., Citation1998; Bajoulvand et al., Citation2019; Manstead et al., Citation1983; Stockdale, Citation2001; Tengku Ismail et al., Citation2016) and did not always predict breastfeeding behaviours (Forster et al., Citation2006; Gijsbers et al., Citation2006; Johnson-Young, Citation2018; Lawton et al., Citation2012; McMillan et al., Citation2008; Shepherd et al., Citation2017; Wambach, Citation1997). In some instances, it was unclear as to the contribution of subjective norms as a TPB-variable in the analysis (Donnan et al., Citation2013; Duckett et al., Citation1998; Masoumi et al., Citation2017; Saffari et al., Citation2017). Moreover, the influence of subjective norms on breastfeeding intentions was found by some authors to be dependent on socio-cultural factors, i.e., age (Dyson et al., Citation2010b), social class (Tarrant et al., Citation2004), ethnicity (Bai et al., Citation2011), country of residence (Fabiyi et al., Citation2016), body mass index classification (Hauff et al., Citation2014), marital status (Bai et al., Citation2010), and the presence of social support (Goksen, Citation2002). Finally, subjective norms had an impact on women's breastfeeding initiation (Khoury et al., Citation2005; Kools et al., Citation2005) but evidence was limited.
I do [want to bottle feed]. I’m not getting myself out in front of everyone. (in Dyson et al., Citation2010b)
'The mindset here is that people think that only those mothers who have low educational background will breastfeed their babies … . (in Tarrant et al., Citation2004)
Subtheme 1.2: Societal norms of infant feeding behaviours in public lead to embarrassment.
Breastfeeding in public was viewed as not being socially or morally acceptable by some women (Scott & Mostyn, Citation2003). There was an experience of conflict for some women, where they felt that they should not breastfeed because of a formula feeding culture (Scott & Mostyn, Citation2003; Shortt et al., Citation2013; Tarrant et al., Citation2004), but at the same time they felt a social expectation to breastfeed (Andrew & Harvey, Citation2011; Cortes-Rua & Diaz-Gravalos, Citation2019; Rehayem et al., Citation2019; Symon et al., Citation2013; Tarkka et al., Citation1999). Societal norms impacted their decision to initiate breastfeeding (Kong & Lee, Citation2004). Feeling like others would disapprove (Bai et al., Citation2009), perceived social stigma (Kendall-Tackett & Sugarman, Citation1995; Newman & Williamson, Citation2018), and views that breastfeeding was not normal (Bailey et al., Citation2004) all impacted whether or not women continued to breastfeed.
'There is a taboo around it. Ah look at her with her diddy [breast] out feeding the baby. (in Shortt et al., Citation2013)
My mother-in-law and sister-in-law while I was still in hospital bought three tins of milk in case I gave up breastfeeding. Family are so negative, everyone is just so negative … . (in Scott & Mostyn, Citation2003)
A major barrier to breastfeeding was embarrassment of breastfeeding in public and in social situations, with embarrassment about feeding in public impacting the breastfeeding experience in general (Hannon et al., Citation2000; Shortt et al., Citation2013; Stockdale, Citation2001). Embarrassment was a reason that expectant mothers did not form intentions to breastfeed in the first place, as they anticipated that they would experience embarrassment and discomfort if they had to breastfeed in front of others (Dyson et al., Citation2010; Humphreys et al., Citation1998; Mitra et al., Citation2004; Murphy, Citation1999). This discomfort was felt by some due to the sexualisation of breasts (Dyson et al., Citation2010b). Embarrassment also impacted breastfeeding initiation, as those who perceived breastfeeding as embarrassing were less likely to start breastfeeding than those who did not see it as embarrassing (Fein & Roe, Citation1998; Khoury et al., Citation2005; Kong & Lee, Citation2004; Matthews et al., Citation1998; McMillan et al., Citation2009; Perez-Escamilla et al., Citation1998; Riscia et al. Citation2017; Tarrant et al., Citation2010). Embarrassment, particularly about feeding in public, also impacted how long women continued to breastfeed; it was listed as a reason why people switched feeding method and discontinued breastfeeding (Avery et al., Citation1998; Brown & Jordan, Citation2013; Brownell et al., Citation2002; Fein & Roe, Citation1998; Guerrero et al., Citation1999; Rempel, Citation2004; Scott & Mostyn, Citation2003). Alongside the embarrassment for breastfeeding in public was a fear of disapproval in public if they formula-fed their baby (Andrew & Harvey, Citation2011). The impact of embarrassment on breastfeeding behaviour was not always clear in analysis (e.g., Dungy et al., Citation2008).
Embarrassing isn't it? Just slap-ping it out and slapping it out … sat with all your mates and everybody's round, and like, oh, I couldn't do it me. (in Dyson et al., Citation2010)
Most people don't breastfeed beyond six months so they just assume it's a kind of a tiny child thing rather than actually a toddler thing. Because my daughter is that little bit older … that's when you tend you get more dirty looks the older your child gets so if they can walk like that's really a nono, if they can ask for it that's also a bit of a stigma. (in Newman & Williamson, Citation2018)
Theme 2: Conflict between moral obligation and reality of motherhood leads to women feeling negative emotions about their breastfeeding behaviour.
Guilt, shame, and regret were negative emotions sometimes reported as resulting from the strong obligation felt by women during pregnancy and after birth to breastfeed their baby to give it the best start in life and to fit with the social norm around infant feeding. These negative emotions arose as the reality of motherhood was not as expected in relation to breastfeeding behaviour and thus initiation and maintenance did not happen as planned. This theme was evidenced in 15 of the 72 included papers (10 qualitative studies, 4 quantitative studies, and 1 mixed-methods study). Two subthemes help to explain this theme further and outline the processes leading to these negative emotions.
Breastfeeding […] is pushed down your throat and out of guilt you are made to feel if you don't do it, you are doing your child a mis-justice. Everybody everywhere pushes breastfeeding, and [I] feel they look down your nose at you if you don't. (in Thomson et al., Citation2015)
It isn't how motherhood is supposed to be. (in Spencer et al., Citation2014).
Subtheme 2.1: Moral obligation of being a good mother.
Breastfeeding was sometimes perceived as a moral choice or obligation, as it is doing what is best and morally right for the baby (Murphy, Citation1999). Not fulfilling this moral obligation made some women feel inadequate as a mother and thus they experienced feelings of shame (Thomson et al., Citation2015). This feeling of moral obligation impacted on intentions to breastfeed (Lawton et al., Citation2012; McMillan et al., Citation2008), initiation of breastfeeding (Spencer et al., Citation2015), and breastfeeding duration (Bailey et al., Citation2004; McMillan et al., Citation2008; Saffari et al., Citation2017). For some, the moral obligation to breastfeed was so strong that they expressed a fear of failure of not being able to achieve any breastfeeding behaviour; for many this resulted in a shorter period of breastfeeding than intended (Spencer et al., Citation2015) and they feared not being able to breastfeed properly (McMillan et al., Citation2008). Religious obligations to breastfeed were mentioned in one paper; for the women in this study, they also feared failure and criticism from others within their religious community, so felt they had no choice other than to breastfeed and felt personal guilt in anticipation of their breastfeeding behaviours (Rehayem et al., Citation2019). In one study moral norms and self-identity were also found to be particularly important for women of a low socio-economic status (McMillan et al., Citation2008).
… we come with this intention of ‘we must breastfeed, we want to breastfeed, that's the only option we want’. If we can't ultimately, we’ll formula feed, but formula-feeding, especially from a Muslim background if you fail to breastfeed it's almost you feel like you’ve failed in a sense. (*other mothers agree*). And so you really want to try every single option to breastfeed your child … . (in Rehayem et al., Citation2019)
Subtheme 2.2: The expectation and reality of breastfeeding.
Mothers experienced feelings of guilt, regret, and disappointment because of the perceived difference between their expectation of motherhood, which for many involved breastfeeding, and the reality of being a mother and actually breastfeeding. The disconnect between expectations and reality led to shorter duration of breastfeeding than intended and feelings of guilt (Cortes-Rua & Diaz-Gravalos, Citation2019; Guyer et al., Citation2012; Spencer et al., Citation2014). Mothers also experienced self-conscious emotions, such as shame, disappointment, and guilt, when they stopped exclusive breastfeeding (Bailey et al., Citation2004), did not achieve their breastfeeding goals (Asiodu et al., Citation2017), or anticipated that they would feel these negative emotions (Shepherd et al., Citation2017). Anxiety and fear about physical aspects of breastfeeding were also reported as barriers to actual breastfeeding behaviour (i.e., pain whilst breastfeeding, Hannon et al., Citation2000; not having enough milk, Fabiyi et al., Citation2016). These emotions, from both physical and psychological attributes, impacted how long they continued to breastfeed (Bailey et al., Citation2004; Cortes-Rua & Diaz-Gravalos, Citation2019; Otoo et al., Citation2009; Shepherd et al., Citation2017). These feelings of disconnect and of the barriers to breastfeeding led to women initially feeling ‘disappointed’ and ‘vulnerable’ at the start of their breastfeeding journey in terms of support from health care professionals and feeling devalued by other mothers who were breastfeeding (Guyer et al., Citation2012).
I mean it was relief to put her on the bottle but guilt, the guilt [here Yasmin is visibly upset]. It was unreal, it was just unreal. I wanted to [breast feed] so much as well you know but I couldn't. (in Bailey et al., Citation2004)
I just thought that the breastfeeding would happen and it was a natural thing that would happen and my body would do what it was supposed to do. (in Guyer et al., Citation2012)
Theme 3: Focus on self is the only way to achieve positive emotions.
Positive emotions were only expressed when women appeared to not be influenced by the social norms and instead held a personal desire to breastfeed for their own benefit. This theme was present in 12 of the 72 papers (6 quantitative studies, 3 qualitative studies and 3 mixed-methods studies), but as stated above, most papers focused on barriers to breastfeeding behaviour and thus did not measure positive emotions, which does not mean they were not present. When positive emotions were reported/measured, women were more likely to have initiated breastfeeding and have a longer duration of breastfeeding behaviour. Mothers experienced the highest personal satisfaction when their current feeding method aligned with their infant feeding intentions (Symon et al., Citation2013) and when they felt happiness and enjoyment regarding their breastfeeding behaviour (Nuampa et al., Citation2018). For those who intended to breastfeed and then initiated breastfeeding, perseverance was reported as being key.
Kept persevering, did everything I could. (in Symon et al., Citation2013)
I wouldn't trade breastfeeding my children for anything. It is one of the most satisfying experiences I have ever had … The closeness I feel for my kids because of breastfeeding is wonderful. (in Kendall-Tackett & Sugarman, Citation1995)
Bonding is a reason I want to breastfeed. I want my baby to know me when I’m away at school. I don't want my baby to call my mother her mother. (in Hannon et al., Citation2000)
I didn't even feel as if it was a bonding time with him, I just felt, because it was painful and urm he wasn't being satisfied by it, I just, it was, I suppose I was anxious which didn't help, so I never quite felt that it was our time to connect with each other. It was a nightmare … It was a nightmare to be honest. (in Spencer et al., Citation2014)
Discussion
This systematic review and meta-analysis has synthesised qualitative, quantitative, and mixed-methods data from seventy-two papers examining the role of emotions and injunctive norms in breastfeeding intentions, initiation, and duration. The meta-analysis of the quantitative data, from quantitative and mixed-methods studies, indicates that positive emotions are associated with increased breastfeeding behaviours. The overall relationship between negative emotions and breastfeeding outcomes in this meta-analysis is not significant; arguably, however, this can be attributed to the lack of reported effect sizes between embarrassment and breastfeeding outcomes in the studies reviewed. Prior research identifies embarrassment as a commonly experienced emotion but has yet to quantify how much embarrassment contributes to breastfeeding success or discontinuation of breastfeeding. Although the meta-analysis did not provide evidence of a relationship between negative emotions and breastfeeding outcomes, embarrassment is further identified as important in our qualitative synthesis. This highlights the importance of understanding the experience of embarrassment in greater depth and future research should quantitatively examine what role this emotion plays in women's breastfeeding behaviours.
In terms of the injunctive norms, subjective norms (i.e., knowledge of what significant others think women should do) were significantly associated with breastfeeding behaviours in this meta-analysis, and this is particularly the case for breastfeeding intentions. The overall relationship between broader societal norms and breastfeeding is not significant, but as with negative emotions, this is most likely due to a lack of prior research that has focused on this type of injunctive norm. Finally, in this meta-analysis, moral norms (i.e., perceived moral obligation to breastfeed) are related to breastfeeding outcomes. This suggests that in addition to subjective norms, moral norms are important influences on breastfeeding outcomes. However, these positive relationships (i.e., correlations) were not always evident in the qualitative findings.
The themes and subthemes generated in the synthesis also identified the importance of both emotions and injunctive norms on breastfeeding behaviours. Specifically, both social norms and feelings of obligation (whether from significant others, wider society, or moral considerations) resulted in the experience of negative self-conscious emotions (particularly embarrassment and guilt), which undermined breastfeeding behaviours. When women focused on their individual needs and reported feeling positive emotions this resulted in more breastfeeding success and wellbeing. Overall, the current findings suggest that in terms of the extended TPB (Rivis et al., Citation2009), which adds moral norms and anticipated affect, it is important to consider these variables. However, we should also incorporate experienced emotions in general, both positive and negative, when understanding breastfeeding behaviours, and should consider the influence of wider injunctive norms, including both wider societal norms and moral norms.
When reflecting on the implications of these findings it is important to consider some of our assumptions from prior literature. For example, from the literature it appeared as if the presence of injunctive norms is what led to negative emotions resulting in less breastfeeding success; however, the other directional relationship is also plausible, as according to the affect-as-information theory (Shwarz & Clore, Citation1983) and the social intuitionist model (Haidt, Citation2001), emotions are a major determinant of our attitudes and behaviours. Nevertheless, what is apparent from the literature is that there is clear intertwinement between negative emotions and injunctive norms, which impacts breastfeeding behaviours. This again has implications for the extended TPB (Rivis et al., Citation2009), as it may be less useful to consider the sequential relationships between these variables but rather that they are cyclical and/or intertwined.
There are also positions and biases of the research team that should be acknowledged. The first author (SR) is a social psychologist who primarily conducts quantitative research, and her prior research focuses on the importance of emotions and morality in societal issues, which may have impacted the interpretation of literature. Additionally, the first author breastfed both of her babies. The second author (DS) is a qualitative researcher and health psychologist who has two children (one was exclusively breastfed and one was fed through a combination of methods including expressed breast milk). The third author (MB) is a social psychologist with expertise in intergroup relations and mental health stigma, she does not have any children. The fourth author (KH) is a research dietitian whose work focuses on nutrition in early life, including the role of breastfeeding in infant and maternal health. She breastfed both of her children. The fifth author (SG) is a mixed-methods researcher and health psychologist, who mostly conducts research in the area of public health; she does not have any children and has not previously conducted any research in infant feeding. Therefore, the research team has a range of expertise, research interests, and prior experience with infant feeding, which we acknowledge here in the interest of transparency.
Additionally, it is important to acknowledge limitations and differences of studies included within the review and meta-analysis, which may limit the conclusions that can be drawn. One issue in the literature is that most studies focus their research questions and sample selection on understanding barriers to breastfeeding, rather than on what encourages breastfeeding. Therefore, there is a negativity bias within research conducted, in which it seems as if the expectation is that women will fail in achieving their breastfeeding goals. Also, in terms of research focus, there is a bias towards studying negative emotions over positive emotions, even though our results (from both the meta-analysis and synthesis) suggest that positive emotions are associated with breastfeeding outcomes and wellbeing. Based on the current results there seems to be a strong need for researchers to focus on the positive aspects of breastfeeding as well. For example, Lyons et al. (Citation2019) explored what encourages and discourages obese women from breastfeeding by sampling women who successfully breastfed. The literature reviewed here suggests that women experienced the most positive emotions when their initial intentions translated into breastfeeding initiation, which also resulted in women breastfeeding for longer and feeling better about themselves. Therefore, further research is needed to understand how to help women form positive intentions and how to make them a reality. In particular, it is important that women are supported to form intentions based on their own personal reasons and positive emotions rather than based on any perceived obligation or pressure to breastfeed.
Another issue in the existing literature is the predominant focus on cognitive elements (e.g., TPB factors and beliefs, such as perceived behavioural control or self-efficacy) over emotions, which needs to be remedied. The majority of studies were cross-sectional and applied TPB to understand breastfeeding intentions (and sometimes duration). However, future research should focus on emotions, for example directly comparing the role of positive versus negative emotions, or reflective, anticipated, or actual emotions. Future research should also endeavour to use different approaches and methods to study emotions, for example in-depth diary studies could be used. At face value this seems quite time consuming; however, diary studies in other domains have been found to have a positive impact on wellbeing (Pennebaker, Citation1997).
It is also seemingly difficult to compare across studies because there are many different operationalisations and measures of emotions, injunctive norms, and breastfeeding behaviours. For example, breastfeeding as an outcome measure differed greatly between studies in this review, with the outcomes ranging from initiation of breastfeeding as being placed on the breast once (Brownell et al., Citation2002) to exclusive breastfeeding at six-months (e.g., Nguyen et al., Citation2014). There was also great variability in terms of what type of breastfeeding outcome was measured: intention, initiation, or duration. On a positive note, there were far more studies that included multiple time points and measures. Conversely, it was problematic that there were far fewer studies that included a measure of breastfeeding initiation, or some objective measure, likely due to the difficulty associated with obtaining these measures. Comparing studies with classifications of breastfeeding as diverse as ‘any’ versus ‘exclusive’ is challenging in general; additionally the operationalisation of breastfeeding outcomes was not always clear, which limits our ability to synthesize and draw conclusions.
A final issue was the variability in terms of sample characteristics and recruitment methods. It was beneficial that there was a wide range of countries sampled, but the populations subsequently differed on many characteristics (e.g., variability in age, Hannon et al. (Citation2000) – teens in USA compared to most studies which included mothers in their late twenties and early thirties), again making it difficult to compare findings, and other studies were missing crucial demographic information. Researchers should consider this point when designing and reporting future studies given that breastfeeding behaviour is known to vary by context and demographics (e.g., Lawton et al., Citation2012; Lou et al., Citation2014; McMillan et al., Citation2008; Swanson et al., Citation2017). Additionally, very few studies incorporated a priori information about their determination of sample size. Samples were recruited through varied means, and participants’ judgements relied on either current breastfeeding experiences or on retrospective memory, again complicating any comparisons and potentially introducing error due to the questionable accuracy of retrospective memory. Nevertheless, despite the shortcomings in the studies reviewed, there is a wide range of evidence supporting the idea that both emotions and injunctive influences play a role in breastfeeding behaviours.
In terms of the practical implications of these findings, firstly, we can suggest that pregnant women need better information concerning the realities of breastfeeding earlier in their journey to motherhood, and that they need long term support. The reality of breastfeeding needs to be addressed in antenatal classes, as many women do not have a realistic view or any knowledge of the barriers to breastfeeding. Also, since societal expectations shift as the babies become older, it is important that women receive continued support. Recommendations surrounding the length of time that women breastfeed for must not be viewed as end points, as many women continue past these and may require extra support, should they wish to continue feeding, due to increased stigma as the infant ages. Second, as mentioned previously, we need to encourage women to focus on breastfeeding as an individual behaviour, from which they can get individual enjoyment, rather than just feeling like they have a social obligation to breastfeed. Seeing a behaviour as a personal choice can empower women to make a decision about infant feeding that suits them and their baby, rather than making a decision that is influenced by external pressures (such as social stigma). This may reduce the guilt felt by women who decide the best choice for them and baby is not to breastfeed. Third, interventions need to target the specific emotions that women experience, such as aiming to reduce feelings of embarrassment that women anticipate (or experience) feeling when feeding in public. It is also important to reduce feelings of shame, guilt, and regret that women may experience when they feel they are not achieving their breastfeeding goals, and to overcome these feelings in order to achieve their long-term breastfeeding aspirations, or, if they discontinue breastfeeding, to experience fewer negative emotions as a result of this. One way to do this is to elicit positive emotions, as these have been shown to counteract negative emotions (Fredrickson, Citation2001), even when elicited from an outside source (Lai et al., Citation2014). Similarly, according to self-affirmation theory, if we affirm our self-concept in another domain this can foster positive outcomes, behaviour change, and wellbeing (Epton et al., Citation2015). Therefore, based on these two theoretical standpoints and the current findings, we would encourage future interventions that look to targeting positive feelings and self-views from other sources to increase breastfeeding behaviours.
Acknowledgements
The current research was funded by the University of Surrey VICI Returner Grant.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 Exclusive breastfeeding defined as giving breastmilk directly from breast or expressed, not supplementing with any other liquids (e.g., formula milk or water).
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. https://doi.org/https://doi.org/10.1016/0749-5978(91)90020-T.
- Andrew, N., & Harvey, K. (2011). Infant feeding choices: Experience, self-identity and lifestyle. Maternal & Child Nutrition, 7(1), 48–60. https://doi.org/https://doi.org/10.1111/j.1740-8709.2009.00222.x
- Asiodu, I., Waters, C., Dailey, D., & Lyndon, A. (2017). Infant feeding decision-making and the influences of social support persons among first-time African American mothers. Maternal & Child Health Journal, 21(4), 863–872. https://doi.org/https://doi.org/10.1007/s10995-016-2167-x
- Avery, M., Duckett, L., Dodgson, J., Savik, K., & Henly, S. J. (1998). Factors associated with very early weaning among primiparas intending to breastfeed. Maternal & Child Health Journal, 2(3), 167–179. https://doi.org/https://doi.org/10.1023/A:1021879227044
- Bai, Y. K., Lee, S., & Overgaard, K. (2019). Critical review of theory use in breastfeeding interventions. Journal of Human Lactation, 0890334419850822(3). https://doi.org/https://doi.org/10.1177/0890334419850822.
- Bai, Y. K., Middlestadt, S. E., Joanne Peng, C. Y., & Fly, A. D. (2009). Psychosocial factors underlying the mother’s decision to continue exclusive breastfeeding for 6 months: An elicitation study. Journal of Human Nutrition and Dietetics, 22(2), 134–140. https://doi.org/https://doi.org/10.1111/j.1365-277X.2009.00950.x
- Bai, Y., Middlestadt, S. E., Peng, C., & Fly, A. D. (2010). Predictors of continuation of exclusive breastfeeding for the first six months of life. Journal of Human Lactation, 26(1), 26–34. https://doi.org/https://doi.org/10.1177/0890334409350168
- Bai, Y., Wunderlich, S. M., & Fly, A. D. (2011). Predicting intentions to continue exclusive breastfeeding for 6 months: A comparison among racial/ethnic groups. Maternal and Child Health Journal, 15(8), 1257–1264. https://doi.org/https://doi.org/10.1007/s10995-010-0703-7
- Bailey, C., Pain, R. H., & Aarvold, J. E. (2004). A ‘give it a go’ breast-feeding culture and early cessation among low-income mothers. Midwifery, 20(3), 240–250. https://doi.org/https://doi.org/10.1016/j.midw.2003.12.003
- Bajoulvand, R., Gonzalez-Jimenez, E., Imani-Nasab, M. H., & Ebrahimzadeh, F. (2019). Predicting exclusive breastfeeding among Iranian mothers: Application of the theory of planned behavior using structural equation modeling. Iranian Journal of Nursing and Midwifery Research, 24(5), 323–329. https://doi.org/https://doi.org/10.4103/ijnmr.IJNMR_164_18
- Bartle, N. C., & Harvey, K. (2017). Explaining infant feeding: The role of previous personal and vicarious experience on attitudes, subjective norms, self-efficacy, and breastfeeding outcomes. British Journal of Health Psychology, 22(4), 763–785. https://doi.org/https://doi.org/10.1111/bjhp.12254
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/https://doi.org/10.1191/1478088706qp063oa
- Brown, A., & Jordan, S. (2013). Impact of birth complications on breastfeeding duration: An internet survey. Journal of Advanced Nursing, 69(4), 828–839. https://doi.org/https://doi.org/10.1111/j.1365-2648.2012.06067.x
- Brownell, K., Hutton, L., Hartman, J., & Dabrow, S. (2002). Barriers to breastfeeding Among African American Adolescent mothers. Clinical Pediatrics, 41(9), 669–673. https://doi.org/https://doi.org/10.1177/000992280204100905
- Centre for Research and Dissemination. (2009). Systematic reviews: CRD’s guidance for undertaking systematic reviews in health care. http://www.york.ac.uk/inst/crd/pdf/Systematic_Reviews.pdf
- Cortes-Rua, L., & Diaz-Gravalos, G. J. (2019). Early interruption of breastfeeding. A qualitative study. Enfermería Clínica, 29(4), 207–215. https://doi.org/https://doi.org/10.1016/j.enfcli.2018.11.003
- Davie, P., Chilcot, J., Chang, Y.-S., Norton, S., Hughes, L. D., & Bick, D. (2019). Effectiveness of social-psychological interventions at promoting breastfeeding initiation, duration and exclusivity: A systematic review and meta-analysis. Health Psychology Review, 14(4), 449–485. https://doi.org/https://doi.org/10.1080/17437199.2019.1630293
- Dennis, C. L., & McQueen, K. (2009). The relationship between infant-feeding outcomes and postpartum depression: A qualitative systematic review. Pediatrics, 123(4), e736–e751. https://doi.org/https://doi.org/10.1542/peds.2008-1629
- Dias, C. C., & Figueiredo, B. (2015). Breastfeeding and depression: A systematic review of the literature. Journal of Affective Disorders, 171, 142–154. https://doi.org/https://doi.org/10.1016/j.jad.2014.09.022
- Dodgson, J. E., Henly, S. J., Duckett, L., & Tarrant, M. (2003). Theory of planned behavior-based models for breastfeeding duration among Hong Kong mothers. Nursing Research, 52(3), 148–158. https://doi.org/https://doi.org/10.1097/00006199-200305000-00004
- Donnan, P. T., Dalzell, J., Symon, A., Rauchhaus, P., Monteith-Hodge, E., Kellett, G., Wyatt, J. C., & Whitford, H. M. (2013). Prediction of initiation and cessation of breastfeeding from late pregnancy to 16 weeks: The Feeding Your Baby (FYB) cohort study. BMJ Open, 3(8), e003274. https://doi.org/https://doi.org/10.1136/bmjopen-2013-003274
- Duckett, L., Henly, S., Avery, M., Potter, S., Hills-Bonczyk, S., Hulden, R., & Savik, K. (1998). A theory of planned behavior-based structural model for breast-feeding. Nursing Research, 47(6), 325–336. https://doi.org/https://doi.org/10.1097/00006199-199811000-00006
- Dungy, C. I., McInnes, R. J., Tappin, D. M., Wallis, A. B., & Oprescu, F. (2008). Infant feeding attitudes and knowledge among socioeconomically disadvantaged women in Glasgow. Maternal & Child Health Journal, 12(3), 313–322. https://doi.org/https://doi.org/10.1007/s10995-007-0253-9
- Dyson, L., Renfrew, M., McFadden, A., McCormick, F., Herbert, G., & Thomas, J. (2010a). Policy and public health recommendations to promote the initiation and duration of breast-feeding in developed country settings. Public Health Nutrition, 13(1), 137–144. https://doi.org/https://doi.org/10.1017/S136898000999067X
- Dyson, L., Green, J. M., Renfrew, M. J., Mcmillan, B, & Woolridge, M. (2010). Factors influencing the infant feeding decision for socioeconomically deprived pregnant teenagers: The moral dimension. Birth: Issues in Perinatal Care, 37(2), 141–149. https://doi.org/https://doi.org/10.1111/j.1523-536X.2010.00394.x
- Dyson, L., Green, J. M., Renfrew, M. J., McMillan, B., & Woolridge, M. (2010b). Factors influencing the infant feeding decision for socioeconomically deprived pregnant teenagers: The moral dimension. Birth: Issues in Perinatal Care, 37(2), 141–149. https://doi.org/https://doi.org/10.1111/j.1523-536X.2010.00394.x
- Dyson, L., Renfrew, M., McFadden, A., McCormick, F., Herbert, G., & Thomas, J. (2006). Promotion of breastfeeding initiation and duration: Evidence into practice briefing. NICE.
- Epton, T., Harris, P. R., Kane, R., van Koningsbruggen, G. M., & Sheeran, P. (2015). The impact of self-affirmation on health-behavior change: A meta-analysis. Health Psychology, 34(3), 187–196. https://doi.org/https://doi.org/10.1037/hea0000116
- Fabiyi, C., Peacock, N., Hebert-Beirne, J., & Handler, A. (2016). A qualitative study to understand nativity differences in breastfeeding Behaviors Among middle-class African American and African-born women. Maternal & Child Health Journal, 20(10), 2100–2111. https://doi.org/https://doi.org/10.1007/s10995-016-2029-6
- Fallon, V., Komninou, S., Bennett, K. M., Halford, J. C. G., & Harrold, J. A. (2017). The emotional and practical experiences of formula-feeding mothers. Maternal & Child Nutrition, 13(4), 1–14. https://doi.org/https://doi.org/10.1111/mcn.12392
- Fein, S. B., & Roe, B. (1998). The effect of work status on initiation and duration of breast-feeding. American Journal of Public Health, 88(7), 1042–1046. https://doi.org/https://doi.org/10.2105/AJPH.88.7.1042
- Forster, D. A., McLachlan, H. L., & Lumley, J. (2006). Factors associated with breastfeeding at six months postpartum in a group of Australian women. International Breastfeeding Journal, 1(1), 1–18. https://doi.org/https://doi.org/10.1186/1746-4358-1-18
- Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. American Psychologist, 56(3), 218–226. https://doi.org/https://doi.org/10.1037/0003-066X.56.3.218
- Gijsbers, B., Mesters, I., Knottnerus, J. A., & van Schayck, C. P. (2006). Factors associated with the initiation of breastfeeding in asthmatic families: The attitude-social influence-self-efficacy model. Breastfeeding Medicine, 1(4), 236–246. https://doi.org/https://doi.org/10.1089/bfm.2006.1.236
- Goksen, F. (2002). Normative vs. Attitudinal considerations in breastfeeding behavior: Multifaceted social influences in a developing country context. Social Science & Medicine, 54(12), 1743–1753. https://doi.org/https://doi.org/10.1016/S0277-9536(01)00145-9
- Gough, D. (2015). Qualitative and mixed methods in systematic reviews. Systematic Reviews, 4(1), 1–3. https://doi.org/https://doi.org/10.1186/s13643-015-0151-y
- Guerrero, M. L., Morrow, R. C., Calva, J. J., Ortega-Gallegos, H., Weller, S. C., Ruiz-Palacios, G. M., & Morrow, A. L. (1999). Rapid ethnographic assessment of breastfeeding practices in periurban Mexico City. Bulletin of the World Health Organization, 77(4), 323–330.
- Guyer, J., Millward, L., & Berger, I. (2012). Mothers’ breastfeeding experiences and implications for professionals. British Journal of Midwifery, 20(10), 724–733. https://doi.org/https://doi.org/10.12968/bjom.2012.20.10.724
- Haidt, J. (2001). The emotional dog and its rational tail: A social intuitionist approach to moral judgment. Psychological Review, 4, 814–834.
- Hannon, P. R., Willis, S. K., Bishop-Townsend, V., Martinez, I. M., & Scrimshaw, S. C. (2000). African-American and Latina adolescent mothers’ infant feeding decisions and breastfeeding practices: A qualitative study. Journal of Adolescent Health, 26(6), 399–407. https://doi.org/https://doi.org/10.1016/S1054-139X(99)00076-2
- Hauff, L. E., Leonard, S. A., & Rasmussen, K. M. (2014). Associations of maternal obesity and psychosocial factors with breastfeeding intention, initiation, and duration. American Journal of Clinical Nutrition, 99(3), 524–534. https://doi.org/https://doi.org/10.3945/ajcn.113.071191
- Hoff, C. E., Movva, N., Vollmar, A. K. R., & Pérez-Escamilla, R. (2019). Impact of maternal anxiety on breastfeeding outcomes: A systematic review. Advances in Nutrition, 10(5), 816–826. https://doi.org/https://doi.org/10.1093/advances/nmy132
- Humphreys, A. S., Thompson, N. J., & Miner, K. R. (1998). Assessment of breastfeeding intention using the transtheoretical model and the theory of reasoned action. Health Education Research, 13(3), 331–341. https://doi.org/https://doi.org/10.1093/her/13.3.331
- Ismail, T. A., Muda, W. M., & Bakar, M. I. (2014). Intention of pregnant women to exclusively breastfeed their infants: The role of beliefs in the theory of planned behaviour. Journal of Child Health Care, 18(2), 123–132. https://doi.org/https://doi.org/10.1177/1367493512473857
- Johnson-Young, E. A. (2018). Predicting intentions to breastfeed for three months, six months, and one year using the theory of planned behavior and body satisfaction. Health Communication, 34(7), 1–12. doi:https://doi.org/10.1080/10410236.2018.1437523.
- Kang, N. M., Choi, Y. J., Hyun, T., & Lee, J. E. (2015). Associations of breastfeeding knowledge, attitude and interest with breastfeeding duration: A cross-sectional web-based study. Journal of Korean Academy of Nursing, 45(3), 449–458. https://doi.org/https://doi.org/10.4040/jkan.2015.45.3.449
- Kendall-Tackett, K. A., & Sugarman, M. (1995). The social consequences of long-term breastfeeding. Journal of Human Lactation, 11(3), 179–183. https://doi.org/https://doi.org/10.1177/089033449501100316
- Khoury, A. J., Moazzem, S. W., Jarjoura, C. M., Carothers, C., & Hinton, A. (2005). Breast-feeding initiation in Low-income women: Role of attitudes, support, and perceived control. Women’s Health Issues, 15(2), 64–72. https://doi.org/https://doi.org/10.1016/j.whi.2004.09.003
- Komninou, S., Fallon, V., Halford, J. C. G., & Harrold, J. A. (2017). Differences in the emotional and practical experiences of exclusively breastfeeding and combination feeding mothers. Maternal & Child Nutrition, 13(3), 1–11. https://doi.org/https://doi.org/10.1111/mcn.12364
- Kong, S. K. F., & Lee, D. T. F. (2004). Factors influencing decision to breastfeed. Journal of Advanced Nursing, 46(4), 369–379. https://doi.org/https://doi.org/10.1111/j.1365-2648.2004.03003.x
- Kools, E. J., Thijs, C., & de Vries, H. (2005). The behavioral determinants of breast-feeding in the Netherlands: Predictors for the initiation of breast-feeding. Health Education & Behavior, 32(6), 809–824. https://doi.org/https://doi.org/10.1177/1090198105277327
- Lai, C. K., Haidt, J., & Nosek, B. A. (2014). Moral elevation reduces prejudice against gay men. Cognition & Emotion, 28(5), 781–794. https://doi.org/https://doi.org/10.1080/02699931.2013.861342
- Lau, C. Y. K., Lok, K. Y. W., & Tarrant, M. (2018). Breastfeeding duration and the theory of planned behavior and breastfeeding self-efficacy framework: A systematic review of observational studies. Maternal and Child Health Journal, 22(3), 327–342. https://doi.org/https://doi.org/10.1007/s10995-018-2453-x
- Lawton, R., Ashley, L., Dawson, S., Waiblinger, D., & Conner, M. (2012). Employing an extended theory of planned behaviour to predict breastfeeding intention, initiation, and maintenance in White British and South-Asian mothers living in Bradford. British Journal of Health Psychology, 17(4), 854–871. https://doi.org/https://doi.org/10.1111/j.2044-8287.2012.02083.x
- Lawton, R., Conner, M., & Mceachan, R. (2009). Desire or reason: Predicting health behaviors from affective and cognitive attitudes. Health Psychology, 28(1), 56–65. https://doi.org/https://doi.org/10.1037/a0013424
- Lou, Z., Zeng, G., Orme, J. G., Huang, L., Liu, F., Pang, X., & Kavanagh, K. F. (2014). Breastfeeding knowledge, attitudes, and intention in a sample of undergraduate students in mainland China. Journal of Human Lactation, 30(3), 331–339. https://doi.org/https://doi.org/10.1177/0890334414526058
- Lourenço, O. (2014). Domain theory: A critical review. New Ideas in Psychology, 32, 1–17. https://doi.org/https://doi.org/10.1016/j.newideapsych.2013.08.001
- Lyons, S., Currie, S., & Smith, D. M. (2019). Learning from women with a body mass index (Bmi) ≥ 30 kg/m2 who have breastfed and/or are breastfeeding: A qualitative interview study. Maternal Child Health, 23(5), 648–656. https://doi.org/https://doi.org/10.1007/s10995-018-2679-7
- Mackie, D. M., & Smith, E. R. (2017). Group-based emotion in group processes and intergroup relations. Group Processes & Intergroup Relations, 20(5), 658–668. https://doi.org/https://doi.org/10.1177/1368430217702725
- Manstead, A. S., Proffitt, C., & Smart, J. L. (1983). Predicting and understanding mothers’ infant-feeding intentions and behavior: Testing the theory of reasoned action. Journal of Personality and Social Psychology, 44(4), 657–671. https://doi.org/https://doi.org/10.1037/0022-3514.44.4.657
- Masoumi, S. Z., Kazemi, F., & Ahmadi, S. (2017). Investigating the effects of instructing mothers using BASNEF model on continuing exclusive breastfeeding of late-preterm infants. Journal of Comprehensive Pediatrics, 8(2), doi:https://doi.org/10.5812/compreped.59243
- Matthews, K., Webber, K., McKim, E., Banoub-Baddour, S., & Laryea, M. (1998). Maternal infant-feeding decisions: Reasons and influences. Canadian Journal of Nursing Research, 30(2), 177–198.
- McAndrew, F., Thompson, J., Fellows, L., Large, A., Speed, M., & Renfrew, M. J. (2012). Infant feeding survey 2010. Health and Social Care Information Centre.
- McKinley, N. M., & Hyde, J. S. (2004). Personal attitudes or structural factors? A contextual analysis of breastfeeding duration. Psychology of Women Quarterly, 28(4), 388–399. https://doi.org/https://doi.org/10.1111/j.1471-6402.2004.00156.x
- McMillan, B., Conner, M., Green, J., Dyson, L., Renfrew, M., & Woolridge, M. (2009). Using an extended theory of planned behaviour to inform interventions aimed at increasing breastfeeding uptake in primiparas experiencing material deprivation. British Journal of Health Psychology, 14(2), 379–403. https://doi.org/https://doi.org/10.1348/135910708X336112
- McMillan, B., Conner, M., Woolridge, M., Dyson, L., Green, J., Renfrew, M., Bharj, K., & Clarke G. (2008). Predicting breastfeeding in women living in areas of economic hardship: Explanatory role of the theory of planned behaviour. Psychology & Health, 23(7), 767–788. https://doi.org/https://doi.org/10.1080/08870440701615260
- Mitra, A. K., Khoury, A. J., Hinton, A. W., & Carothers, C. (2004). Predictors of breastfeeding intention among low-income women. Maternal & Child Health Journal, 8(2), 65–70. https://doi.org/https://doi.org/10.1023/B:MACI.0000025728.54271.27
- Murphy, E. (1999). ‘Breast is best’: Infant feeding decisions and maternal deviance. Sociology of Health & Illness, 21(2), 187–208. https://doi.org/https://doi.org/10.1111/1467-9566.00149
- Natan, M. B., Wiener, A., & Haim, Y. B. (2016). Women’s intention to exclusively breast feed: The Israeli perspective. Midwifery, 34, 173–177. https://doi.org/https://doi.org/10.1016/j.midw.2015.11.013
- Newman, K. L., & Williamson, I. R. (2018). Why aren’t you stopping now?!’ Exploring accounts of white women breastfeeding beyond six months in the east of england. Appetite, 129, 228–235. https://doi.org/https://doi.org/10.1016/j.appet.2018.06.018
- Noblit, G., & Hare, R. D. (1988). Meta-ethnography: Synthesizing qualitative studies. Sage.
- Nuampa, S., Tilokskulchai, F., Patil, C. L., Sinsuksai, N., & Phahuwatanakorn, W. (2018). Factors related to exclusive breastfeeding at Six months in Thai adolescent mothers: An application of concept mapping. Maternal & Child Nutrition, 2, e12714. doi:https://doi.org/10.1111/mcn.12714.
- O’Campo, P., Faden, R. R., Gielen, A. C., & Wang, M. C. (1992). Prenatal factors associated with breastfeeding duration: Recommendations for prenatal interventions. Birth: Issues in Perinatal Care, 19(4), 195–201. https://doi.org/https://doi.org/10.1111/j.1523-536X.1992.tb00402.x
- O’Cathain, A., Croot, L., Duncan, E., Rousseau, N., Sworn, K., Turner, K. M., Yardley, L., & Hoddinott, P. (2019). Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open, 9, e029954. https://doi.org/https://doi.org/10.1136/bmjopen-2019-029954
- Otoo, G. E., Lartey, A. A., & Perez-Escamilla, R. (2009). Perceived incentives and barriers to exclusive breastfeeding among periurban Ghanaian women. Journal of Human Lactation, 25(1), 34–41. https://doi.org/https://doi.org/10.1177/0890334408325072
- Patil, D. S., Pundir, P., Dhyani, V. S., Krishnan, J. B., Parsekar, S. S., Merlin D’Souza, S., Ravishankar, N., Renjith, V. (2020). A mixed-methods systematic review on barriers to exclusive breastfeeding. Nutrition and Health, 26(4), 323–346. https://doi.org/https://doi.org/10.1177/0260106020942967
- Pennebaker, J. W. (1997). Writing about emotional experiences as a therapeutic process. Psychological Science, 8(3), 162–166. https://doi.org/https://doi.org/10.1111/j.1467-9280.1997.tb00403.x
- Perez-Escamilla, R., Himmelgreen, D., Segura-Millan, S., Gonzalez, A., Ferris, A. M., Damio, G., & Bermudez-Vega, A. (1998). Prenatal and perinatal factors associated with breast-feeding initiation among inner-city Puerto Rican women. Journal of the American Dietetic Association, 98(6), 657–663. https://doi.org/https://doi.org/10.1016/S0002-8223(98)00150-3
- Peterson, R. A., & Brown, S. P. (2005). On the use of beta coefficients in meta-analysis. The Journal of Applied Psychology, 90, 175–181. https://doi.org/https://doi.org/10.1037/0021-9010.90.1.175
- Petticrew, M., & Roberts, H. (2006). Systematic reviews in the social sciences: A practical guide. Oxford: Blackwell. http://capitadiscovery.co.uk/surrey-ac/items/797907
- Pluye, P., & Hong, Q. N. (2014). Combining the power of stories and the power of numbers: Mixed methods research and mixed studies reviews. Annual Review of Public Health, 35(1), 29–45. https://doi.org/https://doi.org/10.1146/annurev-publhealth-032013-182440
- Raj, V. K., & Plichta, S. B. (1998). The role of social support in breastfeeding promotion: A literature review. Journal of Human Lactation, 14(1), 41–45. https://doi.org/https://doi.org/10.1177/089033449801400114
- Rehayem, A., Taki, S., Brown, N., & Denney-Wilson, E. (2019). Infant feeding beliefs and practices of Arabic mothers in Australia. Women and Birth, 33(4), e391–e399. https://doi.org/https://doi.org/10.1016/j.wombi.2019.07.004
- Rempel, L. A. (2004). Factors influencing the breastfeeding decisions of long-term breastfeeders. Journal of Human Lactation, 20(3), 306–318. https://doi.org/https://doi.org/10.1177/0890334404266969
- Risica, P. M., & McCausland, K. (2017). Infant feeding decisions and behaviours among low-income smoke-exposed women: Timing and change during pregnancy. Public Health Nutrition, 20(15), 2796–2805. https://doi.org/https://doi.org/10.1017/S1368980017001690
- Rivis, A., Sheeran, P., & Armitage, C. J. (2009). Expanding the affective and normative components of the theory of planned behavior: A meta-analysis of anticipated affect and moral norms. Journal of Applied Social Psychology, 39(12), 2985–3019. https://doi.org/https://doi.org/10.1111/j.1559-1816.2009.00558.x
- Saffari, M., Pakpour, A. H., & Chen, H. (2017). Factors influencing exclusive breastfeeding among Iranian mothers: A longitudinal population-based study. Health Promotion Perspectives, 7(1), 34–41. https://doi.org/https://doi.org/10.15171/hpp.2017.07
- Saunders-Goldson, S., & Edwards, Q. T. (2004). Factors associated with breastfeeding intentions of African-American women at military health care facilities. Military Medicine, 169(2), 111–116. https://doi.org/https://doi.org/10.7205/MILMED.169.2.111
- Schwarz, N., & Clore, G. L. (1983). Mood, misattribution, and judgements of well-being: Informative and directive functions of affective states. Journal of Personality and Social Psychology, 45, 513–523.
- Scott, J. A., & Mostyn, T. (2003). Women’s experiences of breastfeeding in a bottle-feeding culture. Journal of Human Lactation, 19(3), 270–277. https://doi.org/https://doi.org/10.1177/0890334403255225
- Shepherd, L., Walbey, C., & Lovell, B. (2017). The role of social-cognitive and emotional factors on exclusive breastfeeding duration. Journal of Human Lactation, 33(3), 606–613. https://doi.org/https://doi.org/10.1177/0890334417708187
- Shortt, E., McGorrian, C., & Kelleher, C. (2013). A qualitative study of infant feeding decisions among low-income women in the Republic of Ireland. Midwifery, 29(5), 453–460. https://doi.org/https://doi.org/10.1016/j.midw.2012.03.001
- Sirriyeh, R., Lawton, R., Gardner, P., & Armitage, G. (2012). Reviewing studies with diverse designs: The development and evaluation of a new tool. Journal of Evaluation in Clinical Practice, 18(4), 746–752. https://doi.org/https://doi.org/10.1111/j.1365-2753.2011.01662.x
- Spencer, R., Greatrex-White, S., & Fraser, D. M. (2014). ‘I was meant to be able to do this’: A phenomenological study of women’s experiences of breastfeeding. Evidence Based Midwifery, 12(3), 83–88.
- Spencer, R. L., Greatrex-White, S., & Fraser, D. M. (2015). I thought it would keep them all quiet’. Women’s experiences of breastfeeding as illusions of compliance: An interpretive phenomenological study. Journal of Advanced Nursing, 71(5), 1076–1086. https://doi.org/https://doi.org/10.1111/jan.12592
- Stevens, C. J., Gillman, A. S., Gardiner, C. K., Montanaro, E. A., Bryan, A. D., & Conner, M. (2019). Feel good now or regret it later? The respective roles of affective attitudes and anticipated affective reactions for explaining health-promoting and health risk behavioral intentions. Journal of Applied Social Psychology, 49(6), 331–348. https://doi.org/https://doi.org/10.1111/jasp.12584
- Stockdale, J. (2001). A measure of intention: The theory of planned behaviour applied to breastfeeding. RCM Midwives Journal, 4(10), 330–333.
- Susiloretni, K. A., Hadi, H., Blakstad, M. M., Smith, E. R., & Shankar, A. H. (2019). Does exclusive breastfeeding relate to the longer duration of breastfeeding? A prospective cohort study. Midwifery, 69, 163–171. https://doi.org/https://doi.org/10.1016/j.midw.2018.11.008
- Swanson, V., Keely, A., & Denison, F. C. (2017). Does body image influence the relationship between body weight and breastfeeding maintenance in new mothers? British Journal of Health Psychology, 22(3), 557–576. https://doi.org/https://doi.org/10.1111/bjhp.12246
- Swanson, V., & Power, K. G. (2005). Initiation and continuation of breastfeeding: Theory of planned behaviour. Journal of Advanced Nursing, 50(3), 272–282. https://doi.org/https://doi.org/10.1111/j.1365-2648.2005.03390.x
- Symon, A. G., Whitford, H., & Dalzell, J. (2013). Infant feeding in Eastern Scotland: A longitudinal mixed methods evaluation of antenatal intentions and postnatal satisfaction--The Feeding Your Baby study. Midwifery, 29(7), e49–e56. https://doi.org/https://doi.org/10.1016/j.midw.2012.06.017
- Tarkka, M. T., Paunonen, M., & Laippala, P. (1999). Factors related to successful breast feeding by first-time mothers when the child is 3 months old. Journal of Advanced Nursing, 29(1), 113–118. https://doi.org/https://doi.org/10.1046/j.1365-2648.1999.00868.x
- Tarrant, M., Dodgson, J. E., & Choi, V. W. (2004). Becoming a role model: The breastfeeding trajectory of Hong Kong women breastfeeding longer than 6 months. International Journal of Nursing Studies, 41(5), 535–546. https://doi.org/https://doi.org/10.1016/j.ijnurstu.2003.12.007
- Tarrant, R. C., Younger, K. M., Sheridan-Pereira, M., White, M. J., & Kearney, J. M. (2010). The prevalence and determinants of breast-feeding initiation and duration in a sample of women in Ireland. Public Health Nutrition, 13(6), 760–770. https://doi.org/https://doi.org/10.1017/S1368980009991522
- Tengku Ismail, T. A., Wan Muda, W. A., & Bakar, M. I. (2016). The extended theory of planned behavior in explaining exclusive breastfeeding intention and behavior among women in Kelantan, Malaysia. Nutrition Research and Practice, 10(1), 49–55. https://doi.org/https://doi.org/10.4162/nrp.2016.10.1.49
- Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology, 8(1), 1–10. https://doi.org/https://doi.org/10.1186/1471-2288-8-45
- Thomson, G., Ebisch-Burton, K., & Flacking, R. (2015). Shame if you do--shame if you don’t: Women’s experiences of infant feeding. Maternal & Child Nutrition, 11(1), 33–46. https://doi.org/https://doi.org/10.1111/mcn.12148
- Tuan, N. T., Nguyen, P. H., Hajeebhoy, N., & Frongillo, E. A. (2014). Gaps between breastfeeding awareness and practices in Vietnamese mothers result from inadequate support in health facilities and social norms. The Journal of Nutrition, 144(11), 1811–1817. https://doi.org/https://doi.org/10.3945/jn.114.198226
- Tuan, N. T., Nguyen, P. H., Hajeebhoy, N., & Frongillo, E. A. (2014). Gaps between breastfeeding awareness and practices in Vietnamese mothers result from inadequate support in health facilities and social norms. Journal of Nutrition, 144(11), 1811–1817. https://doi.org/https://doi.org/10.3945/jn.114.198226
- Turiel, E. (1983). The development of social knowledge: Morality and convention. Cambridge University Press.
- Victora, C. G., Bahl, R., Barros, A. J. D., França, G. V. A., Horton, S., Krasevec, J., Murch, S., Sankar, M. J., Walker, N., & Rollins, N. C. (2016). Breastfeeding in the twenty-first century: Epidemiology, mechanisms, and lifelong effect. The Lancet, 387(10017), 475–490. https://doi.org/https://doi.org/10.1016/S0140-6736(15)01024-7
- Wambach, K. A. (1997). Breastfeeding intention and outcome: A test of the theory of planned behavior. Research in Nursing & Health, 20(1), 51–59. https://doi.org/https://doi.org/10.1002/(SICI)1098-240X(199702)20:1<51::AID-NUR6>3.0.CO;2-T
- Worobey, J. (2011). Why some mothers stop breast-feeding: Self-reported reasons for switching to formula. Topics in Clinical Nutrition, 26(3), 229–233. https://doi.org/https://doi.org/10.1097/TIN.0b013e3182260d9b
- Zhang, Z., Zhu, Y., Zhang, L., & Wan, H. (2018). What factors influence exclusive breastfeeding based on the theory of planned behaviour. Midwifery, 62, 177–182. doi:https://doi.org/10.1016/j.midw.2018.04.006