
ABSTRACT
Decisions involving two individuals (i.e., dyadic decision-making) have been increasingly studied in healthcare research. There is evidence of bi-directional influences in decision-making processes among spousal, provider-patient and parent–child dyads. Genetic information can directly impact biologically related individuals. Thus, it is important to understand dyadic decision-making about genetic health information among family members. This systematic literature review aimed to identify literature examining decision-making among family dyads. Peer-reviewed publications were included if they reported quantitative empirical research on dyadic decision-making about genetic information, published between January 1998 and August 2020 and written in English. The search was conducted in 6 databases and returned 3167 articles, of which 15 met the inclusion criteria. Most studies were in the context of cancer genetic testing (n = 8) or reproductive testing or screening (n = 5). Studies reported two broad categories of decisions with dyadic influence: undergoing screening or testing (n = 10) and sharing information with family (n = 5). Factors were correlated between dyads such as attitudes, knowledge, behaviors and psychological wellbeing. Emerging evidence shows that dyad members influence each other when making decisions about receiving or sharing genetic information. Our findings emphasize the importance of considering both members of a dyad in intervention design and clinical interactions.
Introduction
Individuals interact with a variety of people when faced with choices that impact their health. Empirical work has produced evidence of dyadic (between two individuals) interactions and influences in health decision-making including spousal, provider-patient, and parent–child dyads (Ferrer et al., Citation2017; Kenny et al., Citation2006; Monin et al., Citation2015). Frameworks such as the interdependence theory have been successfully applied to the study of health-related decisions, further demonstrating the importance of interacting with others in this context (Lewis et al., Citation2006; Monin et al., Citation2015). One health setting in which dyadic influences may be particularly relevant involves decisions related to genetic information.
Knowledge about genetic contributions to health is expanding with rapid advances in genetic technology (Green et al., Citation2020). More families than ever before are facing decisions about whether to undergo genetic testing and what do to with the information they receive. Patients are encouraged to critically engage in decisions about receiving and using genetic information, as these are often preference-sensitive decisions wherein a balance exists between harms and benefits of options with no clear superior choice (O’Connor et al., Citation2007; Paquin et al., Citation2018). Decisions about genetic information are preference-sensitive often because the clinical benefit of genetic information is not always clear; the interpretation of test results may be uncertain, or the options for medical intervention may be limited.
There are two predominant categories of decisions that patients and families engage within genetic healthcare: (1) the decision to undergoing testing and (2) decisions about what to do with the information gained from such tests. There are a variety of contexts in which these types of decisions occur, for example, genetic testing in a patient diagnosed with cancer to inform treatment options, pre-symptomatic testing in an individual with a family history of cardiac disease to inform preventative options, or prenatal testing to inform reproductive options of prospective parents.
Genetic information can directly impact both the person undergoing testing and their biological family members such as children, siblings, and other relatives. Given the relevance of genetic information to family members, it is important to understand dyadic decision-making among biologically related individuals. Understanding dyadic decision-making can inform strategies for enhancing patient and family engagement when making health decisions about genetic information.
The majority of inquiries into decision-making about genetic testing have been limited to the unit of the individual (Sweeny et al., Citation2014). With evidence from these studies, guidance and interventions have been developed that aid or support genetic testing decision-making (Dugas et al., Citation2012). Accordingly, these interventions and guidelines are generally focused on the individual or may aim to enhance shared decision-making between patient and provider (Dugas et al., Citation2012; Grimmett et al., Citation2018; Katapodi et al., Citation2018). A recent systematic review found that resources to support decision-making about cancer genetic testing have an over-emphasis on the cognitive aspects of making a decision (an individual-level factor), and lack tools that support patients through the decision-making process (Grimmett et al., Citation2018). Better understanding of dyadic decision-making between family dyads could enhance interventions that aim to holistically support patients’ decision-making about genetic information.
A recent systematic literature review investigated communication and decision-making between parents and their children regarding cancer susceptibility genetic testing and reproductive options (Dattilo et al., Citation2021). A key finding of this previous review was that while many parents believed they were responsible for communicating genetic test results to their children, communication may be complicated by factors such as their children’s age, developmental relevancy, and psychological concerns. The review did not explore dyadic decision-making between parents and children, such as whether decisions are correlated, or predictive factors. To date, there has not yet been a systematic review focusing on dyadic decision-making in genetics; there is a lack of understanding about the current evidence base, the methods and theories used, as well as what types of decisions are most relevant to the study of interdependence among dyads. The information gained through synthesizing literature about dyadic decision-making in genetics could be used to guide future research in terms of appropriate methods and theories and to promote the development of theory-informed interventions to enhance patient and family engagement in health decisions in genetics. Systematic review findings in this area may also have clinical relevance, for example, to inform clinical providers’ knowledge about which patient decisions are interdependent, thus allowing providers to tailor their interactions with patients to incorporate both members of a dyad. The aim of the current systematic literature review was to summarize evidence about dyadic decision-making in genetics, including identification of which decisions, and in what clinical genetics contexts, family dyads influence each other.
Methods
A systematic literature search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al., Citation2009). The protocol was registered with Prospero (ID: CRD42020166635). The scope of the review was determined using the PICOS (participants, interventions, comparisons, outcomes, and study design) tool (Methley et al., Citation2014). The PICOS selected for this study are outlined below and further detailed in the inclusion criteria section:
P: Biologically related or parent dyads in genetics (undergoing or already received genetic testing)
I: Interdependent decision-making process
C: Non-interdependent decision-making process
O: Decision outcome
S: Quantitative studies
Inclusion criteria
Peer-reviewed publications were included if they reported quantitative primary research about decision-making of biologically related dyads or parent dyads in genetics. We included parents as while they do not share genetic information with each other, they do share genetic information with their biological offspring. Only publications written in English and published between January 1998 and August 2020 were included. The lower date limit was selected as this coincides with a seminal publication outlining a transition to incorporate genetic information into healthcare (Collins et al., Citation1998). The date last searched was 29 August 2020. Publications were excluded if the influence of dyads was not accounted for in analyses (mostly due to a qualitative study design, see Supplemental Table for a list of qualitative studies), if dyadic relationships were not accounted for in quantitative analyses, or if decisions included many family members but did not include dyadic analyses; for example, publications reporting data from family network analyses were excluded.
Search strategy
Searches of the publications were conducted in the PubMed, PsycNET, PsycInfo, Scopus, Social Sciences Citation Index (SSCI) and Science Citation Index (SCI) via the Web of Science databases. These databases were selected due to their comprehensiveness and relevance to decision-making and genetic testing.
Search terms were derived from our primary keywords – ‘genetic testing’, ‘dyad’ and ‘decision-making’ and their synonyms. Search terms and the full electronic search strategy for one database are listed in supplementary information; these were adjusted for each database with the use of MeSH terms and Boolean logic by a librarian at the National Institutes of Health. Title and abstract, then full-text screens were conducted on publications identified by these search terms. Backward and forward reference searching of included publications was also conducted to identify additional publications not identified by our previous searches. The title and abstract of each publication was independently screened by two researchers (E.T. and H.E.Y.), meeting regularly to discuss the decisions (every 500 publications). Following this, each full-text article was independently screened by two researchers (E.T. and W.K.L.) meeting regularly to discuss the decisions (every 50 publications). Endnote software facilitated the search process (Bramer et al., Citation2017). Disagreements between researchers were resolved by consensus after discussion.
Data extraction
Coding of study data was independently conducted by two researchers (E.T. and W.K.L or E.R. and W.K.L.) using NVivo software. Disagreements between researchers were resolved by consensus after discussion. Data extracted included the name of the first author, year of publication, country in which the research was conducted, aim, sample characteristics and size, study design (including the statistical methods, whether the analysis accounted for related individuals, and any theories that were described/applied), participant demographics, measures of dyadic decision-making, and main findings.
Data synthesis
A meta-analysis or any type of quantitative synthesis was not performed in this systematic review because of high heterogeneity within the study data (Pai et al., Citation2004). We used a narrative synthesis approach to compare the studies and present findings (Popay et al., Citation2006). First, to identify the circumstances in which dyads influence each other’s decision-making, studies were grouped by categories of decisions (e.g., decision to take a test, decision to share test results), clinical context (e.g., cancer, pre-natal), and nature of dyadic relationship (e.g., parent–child, spousal). Content analysis was then performed whereby the findings of studies in each of the categories were compared and summarized, noting common themes where possible. Narrative descriptions of the themes were prepared and are presented in the Results. We also recorded and tabulated the variety of theories used across studies, as well as the methodological approach taken (e.g., descriptive statistics only vs. predictive models).
Quality of the studies was assessed using the QualSyst quality assessment (Kmet et al., Citation2004). The QualSyst tool includes ten questions scored from 0 to 2 where 0 = no (did not meet the quality criterion), 1 = partial (partially met the quality criterion), and 2 = yes (met the quality criterion). The summary quality score was calculated by summing scores for the ten questions and dividing by 20 (possible score range 0–2). Criteria includes aspects such as quality of description of study objective, appropriateness of study design, whether conclusions are supported by the available data, etc. In accordance with recommendations, we planned to exclude studies with QualSyst quality scores equal to or lower than 0.65; however, no studies with quality scores lower than 0.65 were identified. The influence of biases that may affect the cumulative evidence in this review (including publication and outcome-reporting bias) were not appropriate to assess as a meta-analysis was not performed and pre-published protocols were not available.
Results
Study characteristics
The systematic literature search resulted in 3167 articles, of which 15 articles describing data from 14 unique samples met the inclusion criteria (). Two articles (Hamilton et al., Citation2016; Mays et al., Citation2014) reported different analyses from the same respondents. Of the 15 eligible studies, 10 were of intimate couples, four of first- or second-degree relatives, and one of parent–child dyads. Overall, eight of the studies were related to cancer genetic testing, five focused on reproductive testing or screening, and two focused on genomic testing for multiple conditions. The majority of the studies were conducted in the USA (9/15). contains details of the study characteristics.
Figure 1. The PRISMA flow diagram (Moher et al., Citation2009).
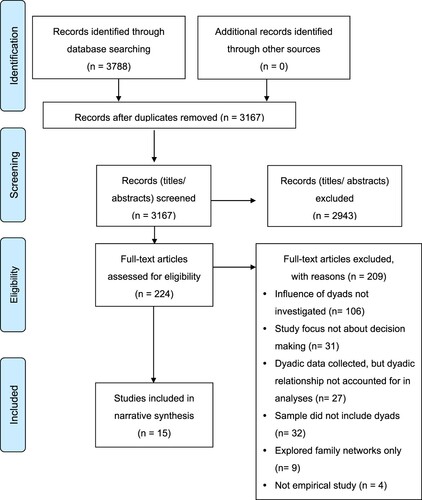
Table 1. Study characteristics.
Of the 10 studies with intimate couples, five were about reproductive testing or screening (Even-Zohar Gross et al., Citation2017; Henneman et al., Citation2001; Nazaré et al., Citation2011; Plantinga et al., Citation2019; Smith et al., Citation2014), three focused on sharing hereditary breast and ovarian cancer risk information with children (Hamilton et al., Citation2016; Mays et al., Citation2014; Sharff et al., Citation2012), one focused on deciding whether the female spouses should undergo hereditary breast and ovarian cancer genetic testing (Bluman et al., Citation2003) and one was about sharing genomic information about a range of genetic conditions with relatives (Turbitt et al., Citation2018). Among the four studies of first- or second-degree relatives’ decision-making, one was about undergoing hereditary breast and ovarian cancer genetic testing (Katapodi et al., Citation2013), two were about undergoing genetic testing for a range of cancers (Mellon et al., Citation2009; Shin et al., Citation2014) and one focused on decisions to share hereditary breast and ovarian cancer genetic information (Vos et al., Citation2011). The only study of parent–child dyads focused on decision-making about the child undergoing genomic testing for multiple conditions (Myers et al., Citation2020).
Quality assessment
The 15 studies were of relatively high quality with a minimum score of 0.75, a median score of 0.95 and an interquartile range of 0.85–1.00 ().
Table 2. Study quality using the QualSyst (Kmet et al., Citation2004).
Analytic methods for examining dyadic relationships and influences
All included studies accounted for the dyadic relationship in analyses. Six of the 15 studies used the Actor-Partner Interdependence Model (APIM) for statistical analyses, which allowed investigation of predictive dyadic effects (Hamilton et al., Citation2016; Mays et al., Citation2014; Mellon et al., Citation2009; Nazaré et al., Citation2011; Smith et al., Citation2014; Turbitt et al., Citation2018). Other analytic approaches used for dyadic data included the Stuart-Maxwell Test, correlation tests (including Intraclass correlation coefficient, Pearson’s, Spearman’s, and Cohen’s), and McNemar’s Test.
Theoretical frameworks guiding study design or data interpretation
Overall, eight studies described or applied theoretical models. This included family-based models such as the Family Communication Patterns Theory (Shin et al., Citation2014) and the Family Systems Theory (Katapodi et al., Citation2013; Turbitt et al., Citation2018), as well as individual-level models such as the Health Belief Model (Henneman et al., Citation2001) and the Transactional Model of Stress and Coping (Hamilton et al., Citation2016; Katapodi et al., Citation2013) ().
Table 3. Theoretical models in the included studies.
Decisions to undergo genetic testing: descriptive dyadic relationships
Of the 15 studies, 10 investigated decisions to undergo genetic testing (). Four studies were in the context of cancer, five focused on reproductive screening or testing, and one on genomic testing for a range of conditions. Three of these studies reported that decisions about undergoing testing are positively correlated among dyads, all of which were in the reproductive testing/screening context and dyads were all intimate couples (Henneman et al., Citation2001; Nazaré et al., Citation2011; Plantinga et al., Citation2019). These three studies reported that there was complete or a high degree of agreement between couples in the decision to undergo reproductive genetic testing or screening. Four studies did not report dyadic correlations in decisions to undergo testing; rather, they reported on attitudes or other variables predictive of a final decision (Even-Zohar Gross et al., Citation2017; Mellon et al., Citation2009; Myers et al., Citation2020; Smith et al., Citation2014).
One study reported correlations between cancer patients’ and their relatives’ decisions to learn cancer genetic test information (Shin et al., Citation2014). This study reported poor concordance between cancer patients’ decision to undergo, and their relatives’ decision to recommend, genetic testing for cancer. The remaining two studies investigating cancer genetic testing decisions did not report correlations between testing decisions (Bluman et al., Citation2003; Katapodi et al., Citation2013). One study investigated adolescents’ and their parents’ decisions to receive information about a range of genetic conditions from genome testing (Myers et al., Citation2020). This study did not report correlations between the decisions, though stated that adolescents were less likely to choose to receive all available results about themselves, compared to parents who were more likely to choose to receive all available results about the adolescent. Despite these differences, all dyads came to an agreement about receiving results after a joint discussion.
Some studies exploring decisions to undergo genetic testing reported on a variety of attitudinal and psychological variables that were correlated among dyads. Variables that were reported to be positively correlated included risk perceptions about genetic variant status (Bluman et al., Citation2003), potential advantages of genetic testing for cancer risk (Mellon et al., Citation2009), attitudes about reproductive testing (Even-Zohar Gross et al., Citation2017), genetic stigma beliefs, and affect relating to receiving test results (Smith et al., Citation2014).
Decisions to undergo genetic testing: predictive dyadic models
Some studies found predictive relationships among variables related to one member of the dyad, and subsequent decisions made by the other member of the dyad. One study explored the outcome ‘decisional balance’, made up of the perceived pros and cons of the decision to learn about genetic cancer risk (Mellon et al., Citation2009). Using the APIM, they explored actor and partner effects for women diagnosed with hereditary breast or ovarian cancer and their first- or second-degree relatives. They found that age and coping style of one member of the dyad was associated with the decision of the other dyad member (both for the person with a diagnosis and their relative). Specifically, an individual was more likely to indicate more pros than cons in the decision to receive genetic information when the partner was younger and had a monitoring coping style (i.e., information seekers). Partner’s family communication was negatively associated with an individual’s decision; when one member of the dyad reported high family communication, the other member of the dyad indicated more cons than pros in the decision to receive genetic information.
Two studies generated a concordance score between dyad predictor variables. These scores were used in models to test the dyadic predictors of the outcome of interest. One study found that agreement among dyads about perceptions of discomfort and barriers to reproductive screening was most strongly predictive of decisions to uptake screening (Henneman et al., Citation2001). Where both members of the dyad perceived low discomfort and low barriers, uptake of screening was high. One study found that dysfunctional communication between dyads was negatively associated with decisions to undergo genetic testing for cancer (Shin et al., Citation2014).
Decisions to share genetic information with family: descriptive dyadic relationships
Five studies investigated dyadic decision-making about sharing information with family members. Three included parents and the decision to share genetic information with biological children who may be at risk (Hamilton et al., Citation2016; Mays et al., Citation2014; Sharff et al., Citation2012). One included first- or second-degree relatives and explored sharing genetic information with these relatives (Vos et al., Citation2011). One study included intimate couples and decisions to share information with family members – the specific relationship of the family members was not specified (Turbitt et al., Citation2018). Most (four) of these studies were about sharing breast and ovarian cancer genetic risk information (Hamilton et al., Citation2016; Mays et al., Citation2014; Sharff et al., Citation2012; Vos et al., Citation2011). One study focused on sharing information on multiple conditions (Turbitt et al., Citation2018).
Partner reports of parent–child communication quality six months after genetic testing were correlated (Hamilton et al., Citation2016). Decisional conflict about communicating genetic test results to children was not correlated between parents (Mays et al., Citation2014). Intentions about sharing genomic results to family members was correlated between intimate couples (Turbitt et al., Citation2018). The two remaining studies did not report on dyadic correlations about family communication (Sharff et al., Citation2012; Vos et al., Citation2011).
Studies that investigated dyadic decision-making about family communication reported correlations between other attitudinal and psychological variables that are important in the decision-making process. Two studies reported positive correlations among parents in the quality of parent–child relationships (Hamilton et al., Citation2016; Mays et al., Citation2014). Level of worry about a genetic condition in the family was positively correlated among intimate couples (Turbitt et al., Citation2018). One study reported a weak positive correlation in resource needs for family communication decision support among mothers and their partners (Sharff et al., Citation2012). This same study reported poor agreement among dyads for motivations behind family communication.
Decisions to share genetic information with family: predictive dyadic models
Three studies reported variables related to one individual that predicted family communication decisions in the partner. Using the APIM, one study showed that partners’ parent–child communication quality prior to genetic testing predicted mothers’ parent–child communication quality after undergoing testing (Hamilton et al., Citation2016). The reverse effect was not present, in that mothers’ parent–child communication quality prior to genetic testing did not predict partners’ communication quality at follow up. Greater confidence in partner’s ability to cope with genetic test results and a stronger parenting alliance was associated with mothers’ communication with their child at follow up. Again, the reverse of these predictive effects were not present, suggesting that dyadic effects were present for mothers’ decisions about communicating genetic test results with their child, but not for partners’ communication decisions.
Another study that used the APIM showed that partner’s decisional conflict about communicating genetic test results to children was associated with an individual’s psychological distress (Mays et al., Citation2014). The predictive effects were present for both members of the dyad whether they were the mother at risk of cancer, or their partner. One study reported that the quality of the communication process by the relative was associated with an individual’s perception of the genetic test result, however, a lack of clarity in the analytic methods described limited understanding of how this conclusion was drawn (Vos et al., Citation2011). Of the other two studies that explored sharing genetic information, one did not detect partner effects associated with family communication (Turbitt et al., Citation2018) and the other did not report on partner effects (Sharff et al., Citation2012).
Discussion
The cumulative evidence synthesized in the current review suggests that genetic testing decisions are correlated within family dyads, and that dyad members influence each other when making decisions in some genetic-testing circumstances. There was greater evidence for correlated decisions between dyads undergoing reproductive genetic testing and less evidence for correlated decisions between dyads undergoing other types of genetic testing such as cancer risk screening, or decisions to communicate any type of genetic testing information to other family members.
Decisions in the context of reproductive genetic testing can refer to the choice to undergo reproductive genetic carrier screening – for prospective parents to find out if they are at a higher risk of passing a recessive or X-linked genetic condition to their children – as well as, the choice to undergo a variety of available genetic tests during pregnancy, such as aneuploidy screening. Our finding – that dyads (all intimate couples in this review) are correlated in their decisions about reproductive genetic testing – is not surprising given the consequences of these decisions will impact their shared offspring. Intimate couples think decisions about genetic testing during pregnancy should be joint decisions (Carroll et al., Citation2012, Citation2013). Indeed, most couples report they communicate with each other about the decision to undergo prenatal testing prior to making a choice (Kenen et al., Citation2000; Watanabe et al., Citation2017). Future research about decision-making in reproductive genetic testing should incorporate intimate couples as limiting studies to one individual could produce an incomplete understanding of this phenomenon.
This systematic review did not find strong evidence that decisions to undergo other types of genetic testing (such as to determine cancer risk) are correlated among individuals and their family members. We cannot definitively conclude that these decisions are not correlated between family members, as only one study reported that conclusion (Shin et al., Citation2014) – the remaining studies did not investigate correlations in family members’ decisions. It is possible that dyadic correlations are stronger in the context of reproductive genetic testing than in the context of other types of genetic testing due to the nature of the relationships under study (i.e., intimate couples vs. other relatives). Future research is needed to better understand the variation in the strength and direction of correlations in family members’ decisions to undergo genetic testing, particularly in contexts other than reproductive testing.
Only three of the included studies about receiving genetic information explored dyadic predictive models (Henneman et al., Citation2001; Mellon et al., Citation2009; Shin et al., Citation2014). The exploration of predictive models is critical in beginning to unpack the processes driving the observed correlations between dyad members. Combined, these studies suggest that individuals’ characteristics may predict partners’ decisions to undergo testing, including age, coping style (whether the individual is an information seeker), communication, and perceptions of discomfort and barriers to genetic testing. Of interest, communication skills were found to be associated with partners’ decisions to undergo testing in disparate ways. Our review found evidence that when one dyad member has strong family communication skills, their partner (women who may be at risk of hereditary cancer) is less likely to seek genetic testing for cancer risk (Mellon et al., Citation2009). However, our review also found evidence that dysfunctional communication between individuals at risk of hereditary cancer and their family members was negatively associated with uptake of genetic testing for cancer risk (Shin et al., Citation2014). It is important to note that the different contexts, variables, and analysis methods make direct comparisons of these two findings challenging. Further exploration is needed to understand how intimate couples and other family members can support individuals at risk of genetic conditions who are faced with decisions to undergo genetic testing.
Our synthesis showed that decisions about sharing genetic information with family members appear to be correlated between dyads (Hamilton et al., Citation2016; Turbitt et al., Citation2018). This finding was in the context of intimate couples sharing genetic information with family members (their children or other related individuals). Although these correlations were detected, few dyadic predictor variables were found to explain these correlations. Communication quality, confidence in partner’s ability to cope with genetic test results, and a stronger parenting alliance in a partner predicted mothers’ communication with their child about their genetic test results (Hamilton et al., Citation2016). This finding suggests that for individuals undergoing genetic testing, their parenting partner plays an important role in supporting communication of those test results with their child, which is paralleled by evidence from a qualitative study that partners often plan and discuss at length with each other how to communicate their genetic test results with their children (Patenaude et al., Citation2013). Individual-level beliefs and attitudes such as perceived value of results and worry about a genetic condition in the family were not predictive of partner communication (Turbitt et al., Citation2018).
Some studies in this review reported on beliefs and attitudes about genetic testing that are correlated between individuals. This included risk perceptions, attitudes, perceived advantages and affect about genetic information. All these variables were positively correlated in dyads regardless of dyad type or type of genetic testing for which beliefs, attitudes and perceptions were examined. Future research could explore mechanisms by which these attitudes and beliefs are formed (for example, through qualitative interviews). Such research could examine whether these attitudes and beliefs are formed independently, or through a process of communication and sharing of values between family members. If attitudes and beliefs are modified through dyadic influences, this could suggest potential targets for interventions aimed at supporting decision-making processes about genetic information.
Our review found that just over half of the studies reported the application of a theoretical framework and only 40% of studies used a family or interdependence-based theory. The application of theory is a key to exploring complex processes such as dyadic decision-making when selecting study variables, developing hypotheses, as well as, for interpretation of results. We strongly advocate for the use of theory in planning both observational and interventional studies in dyadic decision-making. For example, theoretical models of interdependence are relevant for dyadic enquiries and were used by two studies included in our review (Mays et al., Citation2014; Nazaré et al., Citation2011). An interdependence theory acknowledges both individual and partner level effects in decision-making and behavior (Lewis et al., Citation2006). A premise of interdependence theory is that the perspectives of both members of a dyad must be considered to understand the effects of couple interaction. There is some evidence that understanding and accounting for couple-level influences (for example, through application of an interdependence theory) when designing interventions to improve health outcomes is more successful compared to limiting the focus to the individual (Crepaz et al., Citation2015; Lassner, Citation1991).
Many of the studies in this review explored psychological constructs known to be important in decision-making processes and included in many health decision-making and behavior theories, such as attitudes and risk perceptions. Moreover, theoretical frameworks have been developed to examine the role of interpersonal (including dyadic) processes in health (Pietromonaco & Collins, Citation2017). However, studies identified for inclusion in this review did not explicitly report applying decision-making theories in their conceptualization, design, or analysis. The comprehensive body of work on the psychology of decision-making for other health decisions is relevant to decisions about genetic information. For example, there is evidence that emotions play a strong role in health decision-making. A small body of work suggests this is also true for genetic-testing related decisions, such as the finding that affective risk perceptions (for example, worry about experiencing a future health event) have more influence on genetic-testing decisions and behaviors compared to the influence of more conventional subjective risk perception measures (Ferrer et al., Citation2015; Taber et al., Citation2015); however, this remains an understudied area. One study in our review did measure worry about a genetic condition in the family (without applying a specific decision-making framework), but found it was unrelated to spouses’ family communication about genetic risk (Turbitt et al., Citation2018). There have been recent calls for multidisciplinary research that applies health judgement and decision-making expertise to the medical genetics’ context (Klein, Biesecker, et al., Citation2019; Klein, McBride, et al., Citation2019). Further exploration into how constructs from theoretical frameworks predict decisions about genetic testing information among dyads would advance understanding in this area and inform interventions to support dyads in these decision-making processes.
Through performing this systematic review, we found 27 studies that included dyads but did not account for interdependence in the analysis; these were excluded from our final dataset. When dyads are included in a study, accounting for non-independence is an essential step as non-independent data can result in underestimated standard errors and biased p-values, thus providing misleading results (Kenny, Citation1995). While studies included in our review did account for non-independence, few extended their analyses to explore predictive dyadic relationships. Although the complexity of dyadic analysis may deter some researchers without training in dyadic analysis methods, there have been recent advances to help the novice user, such as a user-friendly, freely available app to conduct dyadic data analyses (Stas et al., Citation2018). This app utilizes the Actor Partner Interdependence Model (APIM) which accounts for both one’s own (the actor) variables and the dyad’s (the partner) variables on the outcome. Our review found that the APIM was the most used analysis method to account for interdependence and explore dyadic predictive effects. In addition to the APIM, other popular analytic methods, such as multilevel modeling, can be used to successfully model non-independence among dyads, obtain unbiased results, and explore predictive relationships within and across dyads.
Approximately half of the studies in our review generated study-specific measures and used non-validated scales. In the context of genetics, where many conditions are rare and advances in genetic testing are rapid, it is often not possible to use previously validated measures to explore decision-making. However, for consistent, reliable, and replicable results, the use of previously validated measures is imperative (Cronbach & Meehl, Citation1955; Fried & Flake, Citation2018) and further psychometric studies to validate genetic testing decision-making scales are needed to advance research in this area (Gray et al., Citation2014). The absence of consistency in scales seen across studies in our review limited our ability to compare studies and provide a narrative synthesis, and a quantitative synthesis was not possible.
Implications for research
Our review highlights several important gaps in the dyadic decision-making literature in the context of genetic information, suggesting that future observational research is needed. We have indicated several directions for future research, including work to uncover when and among whom decisions about genetic testing are correlated and the factors and processes that drive those correlations.
Such observational research could guide the development of couple- or family-based interventions. An example of such intervention is a family-based intervention for women at risk of hereditary cancer faced with choices about genetic testing which was recently shown to be feasible and acceptable (Katapodi et al., Citation2018). This intervention was designed to target women genetically at high risk of hereditary cancer, and their biological relatives who may also be at risk. The intervention consists of two live webinars which are attended by both members of the dyad and a brief individual follow-up phone call. The webinars encourage interaction among family members with the support of expert clinicians. The effectiveness of this dyadic intervention on the decision-making process has not been studied. Efficacy of a dyadic intervention has been shown in the context of type 1 diabetes through a study that used decision coaching (non-directive guidance to support decision-making) with young people and their parents to support decisions about insulin delivery options (Lawson et al., Citation2020). The intervention was found to reduce decisional conflict and improve agreement between dyads about the preferred insulin delivery choice in a pre-/post-study. In summary, preliminary evidence suggests that interventions that incorporate both members of a dyad may be feasible and effective at modifying decision outcomes. Future research should continue to inform and expand upon such interventions.
Implications for clinical practice
The implications for clinical practice from our study are limited given the paucity of research we found. It is expected that the further research indicated in the previous section will have more direct clinical implications in guiding how best to approach decision-making where multiple individuals are involved. However, there are some potential recommendations that clinicians could consider. There is evidence that dyads interact and influence each other when making decisions about genetic information, and health providers such as genetic counselors may consider including family members in discussions when patients are faced with decisions about genetic information. Our study endorses models of shared decision-making that not only incorporate the health professional, but also other family members; for example, the TRIO Framework, a conceptual model depicting interaction between patients, health professionals and family caregivers when making cancer treatment decisions (Laidsaar-Powell et al., Citation2017). Aligned with our findings, the model demonstrates a diverse range of family involvement in decision-making including directly and indirectly, and the influence of family may change at various stages of the decision-making process. Clinicians could assess decision-making processes occurring at the family level, to understand how best to facilitate patient decision-making.
One study in the current review found that family communication deficits could negatively impact individuals’ decisions to undergo genetic testing, though another study contradicted these findings. Nonetheless, an exploration of family functioning, communication, and support systems during a clinical interaction may enhance decisional processes for individuals at risk of genetic conditions. Pre-existing family structures are a valuable source of support that could enhance decision-making processes and improve psychological outcomes (such as decisional conflict) for individuals faced with genetic testing decisions. Conversely, family structures could negatively impact or complicate the decision-making process, providing further rationale for the importance of clinician assessment of such structures.
Prior work has investigated strategies for managing conflict during prenatal genetic counseling sessions (Schoeffel et al., Citation2018). While we did not find evidence among the studies in our review of disagreement among intimate couples about reproductive testing, these guidelines may be useful to consider. Genetic counselors can increase partner participation and help couples to reach decision-making consensus, leading to informed decisions (Schoeffel et al., Citation2018). With the increasing use of genetic testing during pregnancy (made possible through non-invasive technologies), couples are more commonly offered testing through health professionals who do not have genetic counseling such as general practitioners and obstetricians (Allyse et al., Citation2015). The increased use of genetic testing outside the specialist genetic clinical context could reduce opportunities for decision-making to be facilitated by a trained genetic counselor, suggesting other health professionals will need to draw on such skills to enhance dyadic decision-making.
Limitations of the current systematic review
A small number of studies met the inclusion criteria and there was high heterogeneity across the included studies such that it was not possible to perform a quantitative data analysis. Studies that used a qualitative approach were excluded as the focus of this review was to explore quantitative dyadic influences and the use of statistical and theoretical models that account for interdependence. The excluded qualitative studies (see Supplemental Table) may provide further insight into dyadic decision-making processes in genetic testing and could be analyzed in future work. Our findings should be interpreted in light of the possibility for publication bias which may exclude studies reporting null findings (Ioannidis et al., Citation2014). Non-English journal articles were excluded due to resource limitations, so it is possible that relevant data not available in English was missed. Furthermore, the majority of studies were conducted in the USA and therefore findings may not be relevant to other countries. Previous studies have shown that the decision-making process for reproductive testing is influenced by individuals’ own sociocultural contexts (Haidar et al., Citation2018). Finally, although gender often plays an important role in health decision-making processes, the included studies did not include or examine gender in a way that made it possible to characterize the role of gender in dyadic decision-making regarding genetic testing.
Conclusions
The current systematic review identified limited published research into dyadic decision-making among family members about genetic information, suggesting many potential avenues for future work in this area. We did find some evidence of dyadic interactions and influences, in particular between intimate couples making decisions about reproductive genetic testing. This review found a variety of other circumstances and relationship where dyadic decision-making in genetics may be occurring. Future observational work is needed that could lead to intervention development to enhance patient and family engagement in decisions about genetic information. There is a need for such research to be theory informed and use methods that account for interdependence between dyads. Our findings are limited in their ability to provide clinical recommendations though providers should explore with patients the possibility that dyadic decision-making is occurring when engaging with decisions about genetic information.
Acknowledgements
Thank you to Nancy Terry, Biomedical Research Librarian, at the National Institutes of Health Library, Office of Research Services, US Department of Health and Human Services (HHS), Bethesda, MD. for her help conducting the database search.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Allyse, M., Minear, M. A., Berson, E., Sridhar, S., Rote, M., Hung, A., & Chandrasekharan, S. (2015). Non-invasive prenatal testing: A review of international implementation and challenges. International Journal of Women’s Health, 7, 113. https://doi.org/https://doi.org/10.2147/IJWH.S67124
- Bluman, L. G., Rimer, B. K., Regan Sterba, K., Lancaster, J., Clark, S., Borstelmann, N., Iglehart, J. D., & Winer, E. P. (2003). Attitudes, knowledge, risk perceptions and decision-making among women with breast and/or ovarian cancer considering testing for BRCA1 and BRCA2 and their spouses. Psychooncology, 12(5), 410–427. https://doi.org/https://doi.org/10.1002/pon.653
- Bramer, W. M., Milic, J., & Mast, F. (2017). Reviewing retrieved references for inclusion in systematic reviews using EndNote. Journal of the Medical Library Association: JMLA, 105(1), 84. https://doi.org/https://doi.org/10.5195/JMLA.2017.111
- Carroll, F. E., Al-Janabi, H., Flynn, T., & Montgomery, A. A. (2013). Women and their partners’ preferences for Down’s syndrome screening tests: A discrete choice experiment. Prenatal Diagnosis, 33(5), 449–456. https://doi.org/https://doi.org/10.1002/pd.4086
- Carroll, F. E., Owen-Smith, A., Shaw, A., & Montgomery, A. A. (2012). A qualitative investigation of the decision-making process of couples considering prenatal screening for Down syndrome. Prenatal Diagnosis, 32(1), 57–63. https://doi.org/https://doi.org/10.1002/pd.2901
- Collins, F. S., Patrinos, A., Jordan, E., Chakravarti, A., Gesteland, R., & Walters, L. (1998). New goals for the US human genome project: 1998–2003. Science, 282(5389), 682–689. https://doi.org/https://doi.org/10.1126/science.282.5389.682
- Crepaz, N., Tungol-Ashmon, M. V., Vosburgh, H. W., Baack, B. N., & Mullins, M. M. (2015). Are couple-based interventions more effective than interventions delivered to individuals in promoting HIV protective behaviors? A meta-analysis. AIDS Care, 27(11), 1361–1366. https://doi.org/https://doi.org/10.1080/09540121.2015.1112353
- Cronbach, L. J., & Meehl, P. E. (1955). Construct validity in psychological tests. Psychological Bulletin, 52(4), 281. https://doi.org/https://doi.org/10.1037/h0040957
- Dattilo, T. M., Lipak, K. G., Clark, O. E., Gehred, A., Sampson, A., Quinn, G., Zajo, K., Sutter, M. E., Bowman-Curci, M., & Gardner, M. (2021). Parent-child communication and reproductive considerations in families with genetic cancer predisposition syndromes: A systematic review. Journal of Adolescent and Young Adult Oncology, 10(1), 15–25. https://doi.org/https://doi.org/10.1089/jayao.2020.0084
- Dugas, M., Shorten, A., Dubé, E., Wassef, M., Bujold, E., & Chaillet, N. (2012). Decision aid tools to support women’s decision making in pregnancy and birth: A systematic review and meta-analysis. Social Science & Medicine, 74(12), 1968–1978. https://doi.org/https://doi.org/10.1016/j.socscimed.2012.01.041
- Even-Zohar Gross, N., Geva-Eldar, T., Pollak, Y., Hirsch, H. J., Gross, I., & Gross-Tsur, V. (2017). Attitudes toward prenatal genetic testing and therapeutic termination of pregnancy among parents of offspring with Prader-Willi syndrome. European Journal of Medical Genetics, 60(4), 205–211. https://doi.org/https://doi.org/10.1016/j.ejmg.2017.01.003
- Ferrer, R., Green, P., Oh, A., Hennessey, E., & Dwyer, L. (2017). Emotion suppression, emotional eating, and eating behavior among parent-adolescent dyads. Emotion, 17(7), 1052–1065. https://doi.org/https://doi.org/10.1037/emo0000295
- Ferrer, R. A., Taber, J., Klein, W., Harris, P., Lewis, K., & Biesecker, L. (2015). The role of current affect, anticipated affect and spontaneous self-affirmation in decisions to receive self-threatening genetic risk information. Cognition and Emotion, 29(8), 1456–1465. http://www.ncbi.nlm.nih.gov/pubmed/25482843, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4503523/pdf/nihms706113.pdf. https://doi.org/https://doi.org/10.1080/02699931.2014.985188
- Fried, E. I., & Flake, J. K. (2018). Measurement matters. APS Observer, 31, 3.
- Gray, S. W., Martins, Y., Feuerman, L. Z., Bernhardt, B. A., Biesecker, B. B., Christensen, K. D., Joffe, S., Rini, C., Veenstra, D., & McGuire, A. L. (2014). Social and behavioral research in genomic sequencing: Approaches from the clinical sequencing exploratory research consortium outcomes and measures working group. Genetics in Medicine, 16(10), 727–735. https://doi.org/https://doi.org/10.1038/gim.2014.26
- Green, E. D., Gunter, C., Biesecker, L. G., Di Francesco, V., Easter, C. L., Feingold, E. A., Felsenfeld, A. L., Kaufman, D. J., Ostrander, E. A., & Pavan, W. J. (2020). Strategic vision for improving human health at the forefront of genomics. Nature, 586(7831), 683–692. https://doi.org/https://doi.org/10.1038/s41586-020-2817-4
- Grimmett, C., Pickett, K., Shepherd, J., Welch, K., Recio-Saucedo, A., Streit, E., Seers, H., Armstrong, A., Cutress, R. I., & Evans, D. G. (2018). Systematic review of the empirical investigation of resources to support decision-making regarding BRCA1 and BRCA2 genetic testing in women with breast cancer. Patient Education and Counseling, 101(5), 779–788. https://doi.org/https://doi.org/10.1016/j.pec.2017.11.016
- Haidar, H., Vanstone, M., Laberge, A.-M., Bibeau, G., Ghulmiyyah, L., & Ravitsky, V. (2018). Cross-cultural perspectives on decision making regarding noninvasive prenatal testing: A comparative study of Lebanon and Quebec. AJOB Empirical Bioethics, 9(2), 99–111. https://doi.org/https://doi.org/10.1080/23294515.2018.1469551
- Hamilton, J. G., Mays, D., DeMarco, T., & Tercyak, K. P. (2016). Modeling the dyadic effects of parenting, stress, and coping on parent-child communication in families tested for hereditary breast-ovarian cancer risk. Familial Cancer, 15(4), 513–522. https://doi.org/https://doi.org/10.1007/s10689-016-9876-6
- Henneman, L., Bramsen, I., Van der Ploeg, H., Ader, H., Van der Horst, H., Gille, J., & Ten Kate, L. (2001). Participation in preconceptional carrier couple screening: Characteristics, attitudes, and knowledge of both partners. Journal of Medical Genetics, 38(10), 695–703. https://doi.org/https://doi.org/10.1136/jmg.38.10.695
- Ioannidis, J. P., Munafo, M. R., Fusar-Poli, P., Nosek, B. A., & David, S. P. (2014). Publication and other reporting biases in cognitive sciences: Detection, prevalence, and prevention. Trends in Cognitive Sciences, 18(5), 235–241. https://doi.org/https://doi.org/10.1016/j.tics.2014.02.010
- Katapodi, M. C., Jung, M., Schafenacker, A. M., Milliron, K. J., Mendelsohn-Victor, K. E., Merajver, S. D., & Northouse, L. L. (2018). Development of a Web-based family intervention for BRCA carriers and their biological relatives: Acceptability, feasibility, and usability study. JMIR Cancer, 4(1), e7. https://doi.org/https://doi.org/10.2196/cancer.9210
- Katapodi, M. C., Northouse, L. L., Milliron, K. J., Liu, G., & Merajver, S. D. (2013). Individual and family characteristics associated with BRCA1/2 genetic testing in high-risk families. Psychooncology, 22(6), 1336–1343. https://doi.org/https://doi.org/10.1002/pon.3139
- Kenen, R., Smith, A. C., Watkins, C., & Zuber-Pittore, C. (2000). To use or not to use: Male partners’ perspectives on decision making about prenatal diagnosis. Journal of Genetic Counseling, 9(1), 33–45. https://doi.org/https://doi.org/10.1023/A:1009429106757
- Kenny, D. A. (1995). The effect of nonindependence on significance testing in dyadic research. Personal Relationships, 2(1), 67–75. https://doi.org/https://doi.org/10.1111/j.1475-6811.1995.tb00078.x
- Kenny, D. A., Kashy, D., & Cook, W. (2006). Dyadic analysis. Guilford Press.
- Klein, W. M., Biesecker, B. B., & Turbitt, E. (2019). Judgment and decision making in genome sequencing. In A. Tibben & B. B. Biesecker (Eds.), Clinical genome sequencing (pp. 57–73). Elsevier.
- Klein, W. M., McBride, C. M., Allen, C. G., Arredondo, E. M., Bloss, C. S., Kaphingst, K. A., Sturm, A. C., & Wang, C. (2019). Optimal integration of behavioral medicine into clinical genetics and genomics. The American Journal of Human Genetics, 104(2), 193–196. https://doi.org/https://doi.org/10.1016/j.ajhg.2019.01.011
- Kmet, L. M., Lee, R. C., & Cook, L. S. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Alberta Heritage Foundation for Medical Research Edmonton.
- Laidsaar-Powell, R., Butow, P., Charles, C., Gafni, A., Entwistle, V., Epstein, R., & Juraskova, I. (2017). The TRIO framework: Conceptual insights into family caregiver involvement and influence throughout cancer treatment decision-making. Patient Education and Counseling, 100(11), 2035–2046. https://doi.org/https://doi.org/10.1016/j.pec.2017.05.014
- Lassner, J. B. (1991). Does social support aid in weight loss and smoking interventions? Reply from a family systems perspective. Annals of Behavioral Medicine, 13(2), 66–72. https://doi.org/https://doi.org/10.1093/abm/13.2.66
- Lawson, M. L., Shephard, A. L., Feenstra, B., Boland, L., Sourial, N., & Stacey, D. (2020). Decision coaching using a patient decision aid for youth and parents considering insulin delivery methods for type 1 diabetes: A pre/post study. BMC Pediatrics, 20(1), 1. https://doi.org/https://doi.org/10.1186/s12887-019-1898-4
- Lewis, M. A., McBride, C. M., Pollak, K. I., Puleo, E., Butterfield, R. M., & Emmons, K. M. (2006). Understanding health behavior change among couples: An interdependence and communal coping approach. Social Science & Medicine, 62(6), 1369–1380. https://doi.org/https://doi.org/10.1016/j.socscimed.2005.08.006
- Mays, D., DeMarco, T. A., Luta, G., Peshkin, B. N., Patenaude, A. F., Schneider, K. A., Garber, J. E., & Tercyak, K. P. (2014). Distress and the parenting dynamic among BRCA1/2 tested mothers and their partners. Health Psychology, 33(8), 765–773. https://doi.org/https://doi.org/10.1037/a0033418
- Mellon, S., Janisse, J., Gold, R., Cichon, M., Berry-Bobovski, L., Tainsky, M. A., & Simon, M. S. (2009). Predictors of decision making in families at risk for inherited breast/ovarian cancer. Health Psychology, 28(1), 38–47. https://doi.org/https://doi.org/10.1037/a0012714
- Methley, A. M., Campbell, S., Chew-Graham, C., McNally, R., & Cheraghi-Sohi, S. (2014). PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Services Research, 14(1), 1–10. https://doi.org/https://doi.org/10.1186/s12913-014-0579-0
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269. http://annals.org/data/Journals/AIM/20188/0000605-200908180-00008.pdf. https://doi.org/https://doi.org/10.7326/0003-4819-151-4-200908180-00135
- Monin, J. K., Levy, B., Chen, B., Fried, T., Stahl, S. T., Schulz, R., Doyle, M., & Kershaw, T. (2015). Husbands’ and wives’ physical activity and depressive symptoms: Longitudinal findings from the cardiovascular health study. Annals of Behavioral Medicine, 49(5), 704–714. https://doi.org/https://doi.org/10.1007/s12160-015-9705-4
- Myers, M. F., Martin, L. J., & Prows, C. A. (2020). Adolescents’ and parents’ genomic testing decisions: Associations with age, race, and sex. Journal of Adolescent Health, 66(3), 288–295. https://doi.org/https://doi.org/10.1016/j.jadohealth.2019.08.028
- Nazaré, B., Fonseca, A., Gameiro, S., Canavarro, M. C., & Dattilio, F. M. (2011). Amniocentesis due to advanced maternal age: The role of marital intimacy in couples’ decision-making process. Contemporary Family Therapy, 33(2), 128–142. https://doi.org/https://doi.org/10.1007/s10591-011-9151-9
- O’Connor, A. M., Wennberg, J. E., Legare, F., Llewellyn-Thomas, H. A., Moulton, B. W., Sepucha, K. R., Sodano, A. G., & King, J. S. (2007). Toward the ‘tipping point’: Decision aids and informed patient choice. Health Affairs, 26(3), 716–725. https://doi.org/https://doi.org/10.1377/hlthaff.26.3.716
- Pai, M., McCulloch, M., Gorman, J. D., Pai, N., Enanoria, W., Kennedy, G., Tharyan, P., & Colford Jr, J. M. (2004). Systematic reviews and meta-analyses: An illustrated, step-by-step guide. The National Medical Journal of India, 17(2), 86–95.
- Paquin, R. S., Peinado, S., Lewis, M. A., Biesecker, B. B., Rini, C., Roche, M., Butterfield, R. M., Powell, C. M., Berg, J. S., & Bailey, D. B. (2018). A behavior-theoretic evaluation of values clarification on parental beliefs and intentions toward genomic sequencing for newborns. Social Science & Medicine, 271, 112037 . https://doi.org/https://doi.org/10.1016/j.socscimed.2018.11.017
- Patenaude, A. F., DeMarco, T. A., Peshkin, B. N., Valdimarsdottir, H., Garber, J. E., Schneider, K. A., Hewitt, L., Hamilton, J., & Tercyak, K. P. (2013). Talking to children about maternal BRCA1/2 genetic test results: A qualitative study of parental perceptions and advice. Journal of Genetic Counseling, 22(3), 303–314. https://doi.org/https://doi.org/10.1007/s10897-012-9549-z
- Pietromonaco, P. R., & Collins, N. L. (2017). Interpersonal mechanisms linking close relationships to health. American Psychologist, 72(6), 531. https://doi.org/https://doi.org/10.1037/amp0000129
- Plantinga, M., Birnie, E., Schuurmans, J., Buitenhuis, A. H., Boersma, E., Lucassen, A. M., Verkerk, M. A., van Langen, I. M., & Ranchor, A. V. (2019). Expanded carrier screening for autosomal recessive conditions in health care: Arguments for a couple-based approach and examination of couples’ views. Prenatal Diagnosis, 39(5), 369–378. https://doi.org/https://doi.org/10.1002/pd.5437
- Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., Britten, N., Roen, K., & Duffy, S. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme Version, 1, b92.
- Schoeffel, K., Veach, P. M., Rubin, K., & LeRoy, B. (2018). Managing couple conflict during prenatal counseling sessions: An investigation of genetic counselor experiences and perceptions. Journal of Genetic Counseling, 27(5), 1275–1290. https://doi.org/https://doi.org/10.1007/s10897-018-0252-6
- Sharff, M. E., DeMarco, T. A., Mays, D., Peshkin, B. N., Valdimarsdottir, H. B., Garber, J. E., Schneider, K. A., Patenaude, A. F., & Tercyak, K. P. (2012). Parenting through genetic uncertainty: Themes in the disclosure of breast cancer risk information to children. Genetic Testing and Molecular Biomarkers, 16(5), 376–382. https://doi.org/https://doi.org/10.1089/gtmb.2011.0154
- Shin, D. W., Cho, J., Roter, D. L., Kim, S. Y., Park, J. H., Cho, B., Eom, H. S., Chung, J. S., Yang, H. K., & Park, J. H. (2014). Attitudinal concordance toward uptake and disclosure of genetic testing for cancer susceptibility in patient-family member dyads. Clinical Genetics, 86(2), 112–120. https://doi.org/https://doi.org/10.1111/cge.12343
- Smith, R. A., Wienke, S., & Coffman, D. L. (2014). Alpha-1 couples: Interpersonal and intrapersonal predictors of spousal communication and stress. Journal of Genetic Counseling, 23(2), 212–220. https://doi.org/https://doi.org/10.1007/s10897-013-9639-6
- Stas, L., Kenny, D. A., Mayer, A., & Loeys, T. (2018). Giving dyadic data analysis away: A user-friendly app for actor–partner interdependence models. Personal Relationships, 25(1), 103–119. https://doi.org/https://doi.org/10.1111/pere.12230
- Sweeny, K., Ghane, A., Legg, A. M., Huynh, H. P., & Andrews, S. E. (2014). Predictors of genetic testing decisions: A systematic review and critique of the literature. Journal of Genetic Counseling, 23(3), 263–288. https://doi.org/https://doi.org/10.1007/s10897-014-9712-9
- Taber, J. M., Klein, W. M., Ferrer, R. A., Lewis, K. L., Biesecker, L. G., & Biesecker, B. B. (2015). Dispositional optimism and perceived risk interact to predict intentions to learn genome sequencing results. Health Psychology, 34(7), 718–728. https://doi.org/https://doi.org/10.1037/hea0000159
- Turbitt, E., Roberts, M. C., Ferrer, R. A., Taber, J. M., Lewis, K. L., Biesecker, L. G., Biesecker, B. B., & Klein, W. M. (2018). Intentions to share exome sequencing results with family members: Exploring spousal beliefs and attitudes. European Journal of Human Genetics, 26(5), 735–739. https://doi.org/https://doi.org/10.1038/s41431-018-0118-2
- Vos, J., Jansen, A. M., Menko, F., Van Asperen, C. J., Stiggelbout, A. M., & Tibben, A. (2011). Family communication matters: The impact of telling relatives about unclassified variants and uninformative DNA-test results. Genetics in Medicine, 13(4), 333–341. https://doi.org/https://doi.org/10.1097/GIM.0b013e318204cfed
- Watanabe, M., Matsuo, M., Ogawa, M., Uchiyama, T., Shimizu, S., Iwasaki, N., Yamauchi, A., Urano, M., Numabe, H., & Saito, K. (2017). Genetic counseling for couples seeking noninvasive prenatal testing in Japan: Experiences of pregnant women and their partners. Journal of Genetic Counseling, 26(3), 628–639. https://doi.org/https://doi.org/10.1007/s10897-016-0038-7