
ABSTRACT
Physical activity (PA) is recommended for childhood cancer survivors (CCSs). However, many CCSs have low levels of activity. This review aimed to systematically identify, appraise and synthesise qualitative research evidence on the barriers and facilitators to PA from the perspective of CCSs. Six databases (MEDLINE, Embase, PsycINFO, CINAHL, SPORTDiscus, and Scopus) were searched to identify qualitative data on PA gathered from CCSs diagnosed ≤18 years of age and who had completed active treatment. An inductive thematic synthesis was undertaken to identify descriptive themes relating to barriers and facilitators to PA, before mapping these onto the Theoretical Domains Framework (TDF). Methodological quality was assessed using CASP, and confidence in review findings was assessed using the GRADE-CERQual approach. Eight original studies were eligible. A total of 45 descriptive themes (29 facilitators and 16 barriers) were mapped onto nine domains of the TDF; they were most commonly mapped onto the Environmental Context and Resources (n = 13 descriptive themes) and the Social Influences (n = 13) domains. Study quality was variable and overall confidence in review findings was low. Conclusive/strong evidence for the barriers and facilitators to PA is lacking, highlighting the need for further research on the perceived influences on PA in CCSs. PROSPERO Registration: CRD42019147829.
Introduction
There are almost 500,000 childhood cancer survivors (CCSs) in the United States (Howlader et al., Citation2021), and a similar number across Europe (Vassal et al., Citation2016). Improved cancer therapies have increased both survival rates and life expectancy for CCSs (Yeh et al., Citation2020); therefore, this expanding survivor population is also ageing. By early-to-mid adulthood, the majority of CCSs will develop at least one chronic health condition (known as late effects) related to their cancer treatment (Geenen et al., Citation2007; Hudson et al., Citation2013; Phillips et al., Citation2015). In this population, cardiovascular disease (CVD) is the leading cause of non-cancer mortality; survivors are up to 7-times more likely to die from CVD than the general population (Armstrong et al., Citation2009; Fidler et al., Citation2017; Winther et al., Citation2018). Although this increased risk is primarily due cardio-toxic therapies (e.g., anthracycline, radiotherapy to fields exposing the heart), traditional risk factors, including obesity, dyslipidemia, and hypertension, further increase CCSs’ risk of developing, and dying from, CVD (Armstrong et al., Citation2013; Winther et al., Citation2018).
Physical activity (PA) is defined as any bodily movement produced by skeletal muscles that requires energy expenditure and encompasses exercise and movement for leisure, transport, work and play (World Health Organization, Citation2020). In adults, PA has been negatively correlated with the risk of cardiovascular mortality (Cheng et al., Citation2018) and, in children, is strongly related to indicators of physical health, including cardio-metabolic markers such as cholesterol and blood pressure (Poitras et al., Citation2016). Among CCSs, being less physically active has been associated with metabolic syndrome, cardio-metabolic risk factors (e.g., larger waist circumference), and cardiovascular events (Jones et al., Citation2014; Slater et al., Citation2015; Smith et al., Citation2014). In addition, in those who have received cardio-toxic therapies, better physical fitness has been associated with the presence of fewer cardio-metabolic risk factors (Schindera et al., Citation2021).
However, CCSs are often stated to be insufficiently active. A large proportion do not meet national physical activity recommendations (Mizrahi et al., Citation2019; Zhang et al., Citation2012). They also engage in less PA (Antwi et al., Citation2019; Zhang et al., Citation2012) and have lower levels of physical fitness than non-cancer controls (Antwi et al., Citation2019; Kabak et al., Citation2019). CCSs report a decline in activity and fitness during treatment and a significant proportion do not return to their pre-diagnosis level of PA post-treatment (Keats et al., Citation2006; Stössel et al., Citation2020).
Modification of health behaviours such as PA offer a preventative strategy to the increased cardio-metabolic risk in CCSs, and there is growing interest in developing and testing PA interventions for these survivors. A critical step in developing behaviour change interventions is to identify factors that the user group (in this case CCSs post-treatment) perceive to make it more likely that they will carry out the behaviour (facilitators), or which hinder their performance of the behaviour (barriers) (Bartholomew Eldredge et al., Citation2016; O'Cathain et al., Citation2019). Qualitative methods such as interviews and focus groups are of particular value in developing an understanding of the influences on behaviour (Atkins et al., Citation2017). Synthesising existing research is a key step in intervention design (Bartholomew Eldredge et al., Citation2016; O'Cathain et al., Citation2019), and bringing together the findings from qualitative research can assist in arriving at new or enhanced understandings in order to inform decisions on health interventions (Flemming & Noyes, Citation2021).
To our knowledge, no such review exists that brings together qualitative evidence from studies with CCSs regarding their views of PA. Therefore, to inform the development of future PA interventions in CCSs, we aimed to systematically identify, appraise and synthesise qualitative research evidence regarding the barriers and facilitators to PA as reported by CCSs who have completed active treatment. In line with recommendations for interventions to be theoretically informed (Bartholomew Eldredge et al., Citation2016; Michie et al., Citation2011; O'Cathain et al., Citation2019), we mapped barriers and facilitators onto the Theoretical Domains Framework (TDF) – a comprehensive framework synthesised from 128 theoretical constructs from 33 theories – which can guide the identification of theoretical constructs which influence behaviour (Cane et al., Citation2012; Michie et al., Citation2005). The TDF consists of 14 domains (examples of domains include knowledge, skills, beliefs about capabilities) and has been used to inform intervention design in various healthcare settings and target populations (Cheung et al., Citation2019; Flannery et al., Citation2018; Kolehmainen et al., Citation2011; Nicholson et al., Citation2014), but as yet has not been used to explore PA behaviours in CCSs.
Methods
The review was prospectively registered with PROSPERO, the international prospective register of systematic reviews (registration number CRD42019147829).
Design
A thematic synthesis of qualitative studies was undertaken following the steps of Thomas and Harden (Citation2008). The review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statements (Page et al., Citation2021; Tong et al., Citation2012) (see Supplementary Materials 1 and 2).
Search strategy
A search of the following six electronic databases was conducted to identify relevant published studies: MEDLINE, Embase, PsycINFO, CINAHL, SPORTDiscus, and Scopus. With assistance from a medical librarian, a comprehensive search strategy based on the five components of the PICOS search strategy tool for qualitative research was designed, adapted for use with specific databases, and piloted (Methley et al., Citation2014). The PICOS components and the accompanying searches are presented in Supplementary Materials 3 and 4. The searches were run from database inception until 1 February 2021 and limited to articles published in English. Reference lists of systematic reviews identified in database searches were screened. Forward and backward citation searches were conducted for all included studies.
Article selection criteria
To be included, studies had to include qualitative data pertaining to PA, as defined above (World Health Organization, Citation2020), in CCSs (). This could be either wholly qualitative studies or mixed-method studies with a distinct qualitative component (e.g., a survey followed by an interview). Studies that presented only quantitative data from structured interviews, and studies that used surveys with open-ended questions, were not included due to a lack of depth and detail. Studies had to explore PA from the perspective of CCSs themselves. Although the views of others (e.g., family members, healthcare professionals) may have been contained within the papers, these data were not extracted for this review.
Table 1. Inclusion and exclusion criteria for systematic review.
For this review, we defined CCSs to be individuals currently of any age who had received a diagnosis of any cancer or a brain tumour in childhood (aged ≤18 years old) and who had completed active hospital-based cancer treatment. Studies which included individuals on maintenance therapy were eligible since these patients are treated as outpatients and are typically able to return to normal activities, such as PA (AboutKidsHealth, Citation2018). It was anticipated that relevant studies may include heterogeneous samples in terms of age at diagnosis and phase of cancer continuum. Therefore, it was stipulated that to be eligible, at least half (50% or more) of the participants should be aged ≤18 years at diagnosis and at least half should have completed active treatment.
Screening process and study selection
Following deduplication, references were imported into Rayyan software (Ouzzani et al., Citation2016) and two reviewers (MB and MP or LS) independently screened titles and abstracts to identify potentially eligible studies. To maximise sensitivity, any article considered potentially relevant by either reviewer was obtained in full-text before being independently assessed by two reviewers. Any discrepancy between reviewers was resolved in discussion with a third reviewer. Where required, the authors of papers were contacted to provide further details about their study sample to confirm eligibility.
Data extraction and synthesis
Data extraction was carried out by MP and cross-checked by MB. Characteristics of the study design and the participants were extracted. Findings were extracted from the results sections but also the abstract and discussion where these findings had not been presented elsewhere in the paper. Data to be synthesised included direct quotes from participants, and the primary study authors’ interpretations of the findings regarding CCSs’ perspectives on PA. Where studies included data on multiple health behaviours (e.g., diet, PA), only that relating specifically to PA was extracted. The PDFs of included papers were imported into NVivo 12 software to facilitate analysis (QSR International Pty Ltd, Citation2018).
Qualitative data synthesis
The three steps of thematic synthesis as described by Thomas and Harden (Citation2008) were followed. First, inductive line-by-line coding was carried out by MP during which ‘free’ codes were assigned, which described the meaning and content of each line of text. Codes and the accompanying text were second-checked by MB (an experienced qualitative researcher) and reviewed with MP to ensure consistency. Next, the two reviewers organised and grouped the initial codes based on similarities and differences, to create descriptive themes. Descriptive themes were labelled based on the data and codes they were describing, thus remaining ‘close’ to the data (Thomas & Harden, Citation2008), and were at the level which reflected whether the theme was identified as a barrier or facilitator of PA. Lastly, to generate analytical themes which went ‘beyond’ the data (Thomas & Harden, Citation2008), we used the TDF, which consists of 14 domains of theoretical constructs which can influence behaviour (Cane et al., Citation2012; Michie et al., Citation2005). MB and MP organised and mapped the descriptive themes onto the TDF domains, before discussing with LS and VA-S (both experienced in using the TDF) to reach a consensus on the categorisation of the themes within the framework.
Quality assessment and transparency of reporting
The methodological quality of the included studies was assessed using the Critical Appraisal Skills Programme (CASP) Qualitative Checklist, which consists of 10 items assessing rigour, credibility and relevance (Critical Appraisal Skills Programme. CASP Qualitative Checklist, Citation2018). MB and MP independently appraised each study and any discordance was resolved through discussion.
An important determinant of any assessment of study quality is the quality of reporting (Carroll et al., Citation2012); therefore, the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) checklist was also completed by MB to provide a comprehensive assessment of the transparency of reporting for each study (Tong et al., Citation2007). COREQ details 32 components of study design that should be included in reports of qualitative research. As per established guidance (Noyes et al., Citation2018), no study was excluded on the basis of poor quality or reporting. Rather the results of CASP and COREQ were used to inform our assessment of confidence in each of the review findings.
Assessing confidence in the review findings
The GRADE-CERQual (Confidence in the Evidence from Reviews of Qualitative Research) approach was used to assess confidence in each of the findings of the review (Lewin et al., Citation2015), these being the barriers and facilitators (descriptive themes) which had been categorised to a TDF Domain. Assessment of the four components of methodological limitations; coherence; adequacy of data; and relevance informs an overall judgement of confidence in each finding – that is, the extent to which the finding is a reasonable representation of the phenomenon of interest (Lewin et al., Citation2015). As per CERQual guidance, the confidence level for all findings began at high and was downgraded to moderate, low or very low based on the assessment of each of the four components (Lewin et al., Citation2018).
Results
A total of 1729 hits were returned from the database searches. After screening by title and abstract, 61 full-text papers were reviewed, resulting in 8 eligible studies (). A summary of the included studies is presented in . The studies were published between 2013 and 2021, with five originating from the United States of America (USA) (Kuntz et al., Citation2019; Lowe et al., Citation2016; Rokitka et al., Citation2021; Santa Maria et al., Citation2014; Wu et al., Citation2015), two from Canada (Price et al., Citation2020; Wright et al., Citation2013) and one from the United Kingdom (UK) (Burke et al., Citation2017). Only five of the eight studies focused specifically on PA (Burke et al., Citation2017; Price et al., Citation2020; Rokitka et al., Citation2021; Wright et al., Citation2013; Wu et al., Citation2015).
Figure 1. PRISMA flow diagram of study selection.
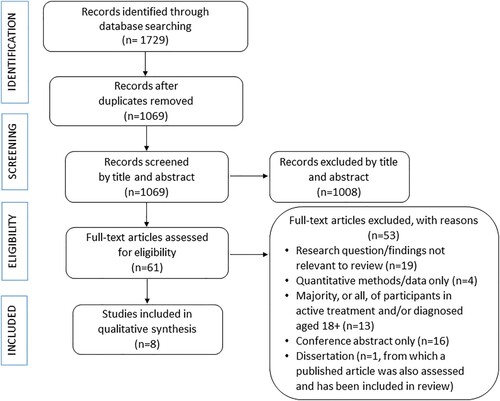
Table 2. Key characteristics of included studies.
Five studies adopted a purely qualitative approach (Burke et al., Citation2017; Kuntz et al., Citation2019; Price et al., Citation2020; Santa Maria et al., Citation2014; Wu et al., Citation2015), whilst three reported qualitative data as part of a mixed-methods study (Lowe et al., Citation2016; Rokitka et al., Citation2021; Wright et al., Citation2013). Six collected data via one-to-one interviews (Burke et al., Citation2017; Kuntz et al., Citation2019; Lowe et al., Citation2016; Price et al., Citation2020; Rokitka et al., Citation2021; Wright et al., Citation2013). All studies were cross-sectional, apart from Burke et al. (Citation2017), who interviewed their participants three times over a three-month period.
Included sample sizes varied from three participants to 30, and data were reported from a total of 126 participants. Studies included participants as young as eight years old (Burke et al., Citation2017), and as old as 52 years (Rokitka et al., Citation2021). One study included only survivors of central nervous system tumours (Santa Maria et al., Citation2014), whilst the remainder recruited patients with a range of diagnoses. Only four studies included samples in which all participants had been diagnosed aged 18 years and under (Burke et al., Citation2017; Lowe et al., Citation2016; Santa Maria et al., Citation2014; Wright et al., Citation2013). Although seven studies focused their recruitment on survivors who had completed active cancer treatment (Burke et al., Citation2017; Lowe et al., Citation2016; Price et al., Citation2020; Rokitka et al., Citation2021; Santa Maria et al., Citation2014; Wright et al., Citation2013; Wu et al., Citation2015), two of these also included survivors on maintenance therapy (Burke et al., Citation2017; Price et al., Citation2020). Whilst two studies did not state the time since completion of treatment for their sample (Wright et al., Citation2013; Wu et al., Citation2015), the remaining studies were split as to whether they included survivors nearer to the completion of their treatment, (Burke et al., Citation2017; Kuntz et al., Citation2019; Price et al., Citation2020) or longer-term survivors (those ≥5 years post-treatment) (Lowe et al., Citation2016; Rokitka et al., Citation2021; Santa Maria et al., Citation2014).
Quality assessment and transparency of reporting
Studies scored between four and eight (out of nine) on the CASP checklist. Several studies presented limited details regarding the recruitment strategy, data collection, relationship between researcher and participant, and data analysis. Transparency of reporting was variable, with studies reporting between seven and 25 of the 32 items in the COREQ checklist. Components relating to the personal characteristics of researcher, relationship with participants, data collection and data analysis were often not reported. Full details of the CASP and COREQ assessments can be found in Supplementary Materials 5 and 6.
Synthesis of findings
Inductive coding identified 45 descriptive themes which described individual barriers (n = 16) and facilitators (n = 29) to PA as perceived by CCSs. These descriptive themes mapped onto nine TDF domains (). The results are presented by TDF domain, with one or two quotes from participants or study authors’ interpretations for illustrative purposes in the text. Further example quotes are presented in Supplementary Material 7.
Table 3. Summary of qualitative findings regarding the barriers and facilitators to physical activity identified in included studies.
Based on judgements of the four CERQual components, the majority of descriptive themes were assessed as being of low confidence (n = 30 descriptive themes), suggesting that it is only possible that they are a reasonable representation of the barriers and facilitators to PA in CCSs. The remainder of descriptive themes (n = 15) were judged as being of very low confidence, indicating that it is not clear whether the finding is a reasonable representation of the barriers and facilitators to PA in CCSs. This was mainly due to lack of adequacy as findings were not supported by sufficiently rich data or a sufficient number of participants or studies. There was also a lack of studies that were deemed directly relevant to the review question (e.g., study did not focus on survivors views of barriers and facilitators to PA; inclusion of survivors on active treatment; inclusion of survivors aged >18 years at diagnosis). Methodological concerns were also common. Definitions of both the CERQual components, and the levels of confidence are given in Supplementary Material 8. A summary of the CERQual confidence levels for each of the barriers and facilitators is summarised in , with the full CERQual evidence profile available in Supplementary Material 9.
TDF domain: skills
A loss of their physical skills due to the effects of cancer and its treatment was reported by survivors to be a barrier to PA in four studies (Burke et al., Citation2017; Kuntz et al., Citation2019; Lowe et al., Citation2016; Rokitka et al., Citation2021). Survivors reported a loss of strength, stamina, speed, flexibility and movement skills, which had affected their ability to do certain types of PA such as walking, running and jumping. This loss of skills had also affected their ability to re-engage in PA such as sports (particularly school-based) and leisure activities:
At the time when I had cancer, I had lost all of my muscle. I had to learn how to run again because I had been in bed a lot and couldn’t do that. (Lowe et al., Citation2016; participant quote)
It [biking] is quite good because it’s also benefitting me in football because I can now kick it quite hard and far. (Burke et al., Citation2017; participant quote)
TDF domain: beliefs about capabilities
Two descriptive themes relating to survivors’ beliefs about their perceived ability to be physically active were identified across five studies (Burke et al., Citation2017; Kuntz et al., Citation2019; Lowe et al., Citation2016; Rokitka et al., Citation2021; Wu et al., Citation2015). Regarding barriers to PA, all five studies reported that survivors perceived the cancer to have adversely affected their overall ability to be physically active. This was a result of: inactivity due to cancer and its treatment; treatment side-effects (e.g., fatigue); the presence of late effects; adverse health conditions; and not being their ‘old physical self’. Survivors reported this prevented exercising and participating in activities such as dancing, walking or running longer distances. Others reported they could no longer do particular activities to the same level, or with the same ease, as they had before their cancer:
But the thing is, I had osteosarcoma so my leg can’t stand a lot of … can’t run, because it’s like, a lot of pounding and stuff like that. (Rokitka et al., Citation2021; participant quote)
Obviously [I am] a bit nervous because there’s always that feeling that you’re going to fall off, but it’s slowly getting better and I’m getting a bit more confident and stuff. (Burke et al., Citation2017; participant quote)
TDF domain: beliefs about consequences
Two themes (both facilitators) were evidenced in four studies relating to survivors’ perceptions of the beneficial effects of PA on their health (Burke et al., Citation2017; Lowe et al., Citation2016; Rokitka et al., Citation2021; Wright et al., Citation2013). All four studies reported the belief among participants that being physically active, and increasing PA levels, was beneficial to their physical health by maintaining (e.g., maintaining weight), improving (e.g., getting stronger) and protecting their health (e.g., reducing the risk of poor health and cancer in future):
I think having a past of being sick and knowing that exercise helps is definitely a major motivator. (Rokitka et al., Citation2021; participant quote)
I think [physical activity] gives me a brighter outlook … like wanting me to be better … (Wright et al., Citation2013; participant quote)
TDF domain: intentions
Two themes relating to intentions for PA were identified across three studies (Lowe et al., Citation2016; Rokitka et al., Citation2021; Wu et al., Citation2015). A lack of motivation to do exercise was reported by a survivor in one study (Wu et al., Citation2015), whilst in two studies, motivation to exercise came from a feeling of responsibility to others:
I think about the kids who are just lying in bed, getting all that medicine and they can’t go exercise. It’s kind of like motivation, and I feel like I’m doing it for them. (Lowe et al., Citation2016; participant quote)
TDF domain: goals
Three goal-oriented themes were identified across four studies (Lowe et al., Citation2016; Price et al., Citation2020; Wright et al., Citation2013; Wu et al., Citation2015). In terms of facilitators, one study reported that survivors stated that having goals helped to maintain PA:
Participants reported that having a goal and routine helped survivors sustain healthy habits. For instance, one survivor registered for a running race, which encouraged him to run regularly. (Wu et al., Citation2015; authors’ interpretation)
Everything proves that it is good for you. There is no reason not to do it, but I think there […] are other priorities in life. (Price et al., Citation2020; participant quote)
TDF domain: environmental context and resources
All eight studies contributed to aspects of environmental context and the availability of resources. The value of being able to access facilities and resources for PA was found across three studies (Burke et al., Citation2017; Lowe et al., Citation2016; Wu et al., Citation2015). Memberships of gyms and wellness centres and having equipment were noted to increase motivation, improve accessibility to, and facilitate, exercise. However, in one study survivors expressed feeling embarrassed in gym environments (Wu et al., Citation2015). This stemmed from an awareness of their physical limitations due to cancer and its treatment.
Two studies reported that survivors expressed an interest in facilities or experiences that were specifically tailored to cancer survivors (Kuntz et al., Citation2019; Wu et al., Citation2015). Such programs would provide an environment where survivors would feel more comfortable and equipment would be suitable for all physical abilities. In addition, such opportunities would enable survivors to interact with other young adult survivors through group exercises or providing activities which facilitate PA whilst also allowing survivors to meet and talk:
Even do a gym that would cater to different physical abilities and make it more comfortable for them, because it could be intimidating to go to a normal gym so maybe a cancer survivor only gym that does have all the different levels of weights for them. (Wu et al., Citation2015; participant quote)
Introducing people to new sports or activities that they maybe haven’t done before and then helping them get ready for, ‘Hey, want to do a triathlon? Great, here’s some information. Here’s what you need to do to do that’. (Wu et al., Citation2015; participant quote)
Having a resource, whether it’s a person on an online community, to help me make informed decisions and follow good practices for managing my health, like knowing good ways to exercise and use my time effectively to exercise, and exercise right so I don’t hurt myself or do something stupid like that. (Lowe et al., Citation2016; participant quote)
Eight participants (40%) reported that it was difficult to regularly find time to exercise, usually because of work schedules. (Rokitka et al., Citation2021; authors’ interpretation)
Money wise, my mom sends me money […] and I like exclusively keep the money she sends me for like yoga and the gym and things like that which is a huge help. (Price et al., Citation2020; participant quote)
I think they think it is important, but we don’t as a family go out and go out for a run or a walk or a bike, I mean we try but it is not a routine. (Price et al., Citation2020; participant quote)
[I’ve heard nothing about health-risk behaviors, physical activity or nutrition], and of course, there hasn’t really been much of a context for that to come up because I haven’t seen a doctor regularly in a while, and I didn’t go through any exit counselling. (Lowe et al., Citation2016 participant quote)
TDF domain: social influences
Six studies provided data on how others were perceived to help or hinder survivors’ engagement with PA (Burke et al., Citation2017; Kuntz et al., Citation2019; Lowe et al., Citation2016; Price et al., Citation2020; Santa Maria et al., Citation2014; Wright et al., Citation2013). For example, keeping up with the PA level of peers was suggested to be a facilitator by a survivor in one study (Wright et al., Citation2013) and friendships were stated to provide an opportunity for PA in another (Lowe et al., Citation2016). A survivor in the same study also reported that having no one else to engage in exercise was a barrier to PA:
I think I would have been in better shape … if I would have had somebody to exercise with me when I was younger after I had cancer. (Lowe et al., Citation2016; participant quote)
Positive parental modelling of PA behaviours was an important influence on the PA of children in the two studies which focused on the influence of parents (Price et al., Citation2020; Santa Maria et al., Citation2014). However, an additional nuance suggested by survivors in the study by Price and colleagues was that parental modelling was more complex in that survivors whose parents took part in PA for recreation and enjoyment purposes appeared to be more active than those survivors who described their parents’ motivations to be active were more centred on health and appearance reasons:
Adolescent and young adult cancer survivors who described their parents’ physical activity as high but externally motivated (e.g., to reduce morbidity, enhance physical appearance) seemed to be less involved in physical activity themselves. (Price et al., Citation2020; authors’ interpretation)
My mom talks to me about losing weight. She’s like, you need to get up and exercise. Thing is, she weighs more than me. (Santa Maria et al., Citation2014; participant quote)
Parental encouragement for PA was reported in three studies (Burke et al., Citation2017; Price et al., Citation2020; Wright et al., Citation2013). This included providing prompts and reminders, encouragement to continue or increase PA levels, support to try out new activities and parents also engaging in PA alongside their children. However, the study by Price and colleagues found that whilst this encouragement could be viewed as positive and supportive, some survivors felt it could be negative and controlling, particularly if the activities were not chosen by the child:
Adolescent and young adult cancer survivors felt this type of support was negative when they perceived their parents as “pushing” or “urging” them to participate in physical activities that they did not choose or find enjoyable. (Price et al., Citation2020; authors’ interpretation)
Through cycling, they were able to build meaningful friendships and foster relationships with their parents, which made them feel supported. (Burke et al., Citation2017; authors’ interpretation)
At first it limited my physical activities because at first my parents didn’t want me to do things. I went to a private high school and because the administration viewed my health history, I don’t think they really wanted me to be involved with sports, so I gravitated towards music and had fun with that. (Lowe et al., Citation2016; participant quote)
They talk about that and how important it is to stay healthy. Right when I finished treatment, they were telling me that my bones were probably really weak and that it would be important to do weight bearing activities, so I run a lot. (Lowe et al., Citation2016; participant quote)
TDF domain: emotion
Three studies provided information on the role emotions play in PA (Burke et al., Citation2017; Wright et al., Citation2013; Wu et al., Citation2015). In two, survivors commented that feelings of stress, depression, embarrassment and frustration could prevent PA (Wright et al., Citation2013; Wu et al., Citation2015). However, in one study, there was evidence that experiencing negative emotions such as stress and fear about one’s health could also play a part in motivating a return to PA:
I was like, man, I’m going to die of a heart attack or something, and for me that thought was frightening enough that I was like I need to do something … I think that’s what sparked me to start working out again, and hit the gym. (Wu et al., Citation2015; participant quote)
makes me feel better about myself and makes me feel good after I’m done. (Wright et al., Citation2013; participant quote)
TDF domain: behavioural regulation
Three studies contributed to four themes of facilitators of PA concerning behavioural regulation (Price et al., Citation2020; Wright et al., Citation2013; Wu et al., Citation2015). In one study, a survivor expressed that slowly building up PA levels after treatment could help facilitate PA, whilst another participant suggested that it was adapting and changing activities after treatment that helped to maintain PA (Wright et al., Citation2013). In one study, survivors suggested that introducing new activities either maintained their interest in PA, or could help to stimulate interest in others:
Similarly, introducing interesting activities, such as video games involving physical activities, can motivate survivors, particularly young ones, to do exercise. (Wu et al., Citation2015; participant quote)
In two studies (Price et al., Citation2020; Wu et al., Citation2015), the routine was acknowledged as being potentially beneficial to maintaining PA:
… and if we had a schedule, I think it would be easier to do something as a whole family or at least my mom, my dad, and me. (Price et al., Citation2020; participant quote)
Discussion
This systematic review and qualitative evidence synthesis have systematically identified, appraised and synthesised qualitative research evidence on the barriers and facilitators to PA, as perceived by CCSs. To our knowledge, this is the first review to summarise qualitative evidence of these issues in CCSs. By bringing together existing qualitative evidence on the topic and by using a theoretically driven synthesis to map the review findings, it has enabled a systematic way to view insights into the factors which CCSs perceive to help or hinder their PA behaviours, whilst including studies that were not necessarily targeting this research question.
By synthesising published data, we have highlighted that CCSs who have completed hospital-based treatment still continue to face a variety of complex influences on their behaviour. Data mapped onto nine of the TDF domains. By far, the majority of descriptive themes (both barriers and facilitators) mapped onto the domains of Environmental Context and Resources and Social Influences, with many of these themes relating to the influence of parents. Although parental influence and support is recognised as a key factor in the PA of children and adolescents (Biddle et al., Citation2011; Martins et al., Citation2015), including those with physical disabilities (McKenzie et al., Citation2021), the weighting of these issues in the review findings could be due to parental factors being the main focus of two of the included studies (Price et al., Citation2020; Santa Maria et al., Citation2014). Nevertheless, this highlights the potentially important role that parents may have in both the development and the implementation of PA interventions for CCSs. However, parental engagement and involvement in such interventions for CCSs are noted to be rare (Brown et al., Citation2020; Raber et al., Citation2016).
Our synthesis also identified other influential factors previously reported in young people without a history of cancer, such as the availability of social support, access to facilities, issues relating to time and money, as well as perceived competence and self-consciousness about appearance (Biddle et al., Citation2011; Brunton et al., Citation2003). However, this review helps to bring together evidence of how these factors influence PA in the context of childhood cancer survivorship such as how survivors perceive the cancer and treatment to have impacted on their physical skills and capability; how survivors may feel uncomfortable in typical exercise environments; the potential need for resources and advice tailored to survivors; and the role healthcare professionals may play in encouraging PA. These findings not only help to illuminate the challenges CCSs face, but also the ways in which interventions could begin to support CCSs to be more physically active.
The use of the TDF provided a ‘theoretical lens’ through which the likely influences on PA could be viewed to identify what personal, social and environmental changes need to occur in order to improve PA in CCSs (Atkins et al., Citation2017). These results when used in conjunction with the Behaviour Change Wheel (BCW) (Michie et al., Citation2014), a framework developed for characterising and designing behaviour change interventions, will help to inform important decisions, including what intervention functions and behaviour change techniques are likely to be effective in bringing about a change in the PA behaviour of CCSs. For example, for barriers identified in the TDF domains of Environmental Context and Resources and Social Influences, intervention functions suggested by the BCW include environmental restructuring and modelling. Behaviour change techniques associated with these intervention functions include the demonstration of the behaviour, social support, and restructuring the physical environment.
The GRADE-CERQual approach was used to assess the confidence of the review findings and the extent to which they were a reasonable representation of the perceived influences on PA behaviours of CCSs. In doing so, the majority of review findings were found to be of low confidence. This was mainly due to a paucity of data in terms of its richness, the small number of primary studies (and participants) which contributed to each review finding, and the lack of studies that focused on PA (as opposed to health behaviours in general), as well as the inclusion of heterogeneous samples. Taken together, these issues highlight the lack of research that has been undertaken to explore PA behaviours in CCSs, and specifically research to understand the barriers and facilitators to PA. Therefore, although this review offers a valuable first step in the development of an evidence-based and theoretically informed intervention, further primary research is needed.
Strength and limitations
The review was carried out according to the methodological and reporting standards set out by both PRISMA and ENTREQ. A rigorous and reproducible search strategy of multiple data sources was utilised and at least two independent reviewers carried out screening, data checking and quality assessment. In addition, backward and forward citation searching was used to avoid missing studies, and where necessary, authors of potentially eligible studies were contacted to clarify study details to confirm inclusion/exclusion.
Although a theoretical framework was utilised to categorise the perceived influences on PA behaviours in CCSs, initial inductive coding ensured that any data that potentially did not fit within the TDF domains would still be captured by the synthesis. However, all data did in fact map onto the TDF domains. Additionally, the GRADE-CERQual approach was used to assess how much confidence could be placed on each of our review findings.
The eligibility criteria was restricted to enable the identification of issues pertinent to survivors of childhood cancer who had completed active cancer treatment. However, in doing so, only eight papers were eligible and half of the included studies contained a minority of patients who were diagnosed older than 18 years. Additionally studies included participants currently aged 8–52 years old, making it difficult to identify how the influences of PA may differ across age groups. The majority of papers originated from the USA, with the remainder from Canada and the UK, thus limiting the generalisability of findings.
Conclusion
Sub-optimal levels of PA are a well-documented issue in CCSs. This review is the first to systematically identify, appraise and synthesise qualitative evidence regarding the barriers and facilitators to PA, as perceived by CCSs no longer on active hospital-based treatment. Few studies were eligible and although multiple influences on the PA behaviour of CCSs were identified, confidence in the review findings was low. Therefore, this highlights that further in-depth qualitative research is needed in this area to strengthen the evidence-base, and to further inform intervention development.
Supplemental Material
Download PDF (575.8 KB)Acknowledgements
MB, LS, RS and VA-S conceived the review. MB and LS secured funding to support MP. MB and MP conducted the searches, screened for eligibility, extracted and analysed the data (supported by LS and VA-S). All authors contributed to the interpretation of the data. MB drafted the manuscript, and all authors provided revisions, comments and approved the final manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- AboutKidsHealth. (2018). Acute lymphoblastic leukemia: Chemotherapy phases. Retrieved July 23, 2021, from https://www.aboutkidshealth.ca/article?contentid=2846&language=english
- Antwi, G. O., Jayawardene, W., Lohrmann, D. K., & Mueller, E. L. (2019). Physical activity and fitness among pediatric cancer survivors: A meta-analysis of observational studies. Supportive Care in Cancer, 27(9), 3183–3194. https://doi.org/10.1007/s00520-019-04788-z
- Armstrong, G. T., Liu, Q., Yasui, Y., Neglia, J. P., Leisenring, W., Robison, L. L., & Mertens, A. C. (2009). Late mortality among 5-year survivors of childhood cancer: A summary from the childhood cancer survivor study. Journal of Clinical Oncology, 27(14), 2328–2338. https://doi.org/10.1200/JCO.2008.21.1425
- Armstrong, G. T., Oeffinger, K. C., Chen, Y., Kawashima, T., Yasui, Y., Leisenring, W., Stovall, M., Chow, E. J., Sklar, C. A., Mulrooney, D. A., Mertens, A. C., Border, W., Durand, J.-B., Robison, L. L., & Meacham, L. R. (2013). Modifiable risk factors and major cardiac events among adult survivors of childhood cancer. Journal of Clinical Oncology, 31(29), 3673–3680. https://doi.org/10.1200/JCO.2013.49.3205
- Atkins, L., Francis, J., Islam, R., O’Connor, D., Patey, A., Ivers, N., Foy, R., Duncan, E. M., Colquhoun, H., Grimshaw, J. M., Lawton, R., & Michie, S. (2017). A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science, 12(1), 77. https://doi.org/10.1186/s13012-017-0605-9
- Bartholomew Eldredge, L. K., Markham, C. M., Ruiter, R. A. C., Fernandez, M. E., Kok, G., & Parcel, G. S. (2016). Planning health promotion programs: An intervention mapping approach (4th ed.). Jossey-Bass.
- Biddle, S. J. H., Atkin, A. J., Cavill, N., & Foster, C. (2011). Correlates of physical activity in youth: A review of quantitative systematic reviews. International Review of Sport and Exercise Psychology, 4(1), 25–49. https://doi.org/10.1080/1750984X.2010.548528
- Brown, M. C., Sharp, L., Sniehotta, F. F., Skinner, R., & Araújo-Soares, V. (2020). The development of health behaviour change interventions for childhood cancer survivors: The need for a behavioural science approach. Pediatric Blood & Cancer, 67, e28500. https://doi.org/10.1002/pbc.28500
- Brunton, G. H. A., Rees, R., Kavanagh, J., Oliver, S., & Oakley, A. (2003). Children and physical activity: A systematic review of barriers and facilitators. EPPI-Centre, Social Science Research Unit, Insitute of Education, University of London. Retrieved February 2021, from http://eppi.ioe.ac.uk/cms/Portals/0/PDF%20reviews%20and%20summaries/Children_PA.pdf?ver=2006-03-02-124608-950
- Burke, S. M., Brunet, J., Wurz, A., Butler, C., & Utley, A. (2017). Cycling through cancer: Exploring childhood cancer survivors’ experiences of well- and ill-being. Adapted Physical Activity Quarterly, 34(4), 345–361. https://doi.org/10.1123/apaq.2016-0011
- Cane, J., O’Connor, D., & Michie, S. (2012). Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science, 7(1), 37. https://doi.org/10.1186/1748-5908-7-37
- Carroll, C., Booth, A., & Lloyd-Jones, M. (2012). Should we exclude inadequately reported studies from qualitative systematic reviews? An evaluation of sensitivity analyses in two case study reviews. Qualitative Health Research, 22(10), 1425–1434. https://doi.org/10.1177/1049732312452937
- Cheng, W., Zhang, Z., Cheng, W., Yang, C., Diao, L., & Liu, W. (2018). Associations of leisure-time physical activity with cardiovascular mortality: A systematic review and meta-analysis of 44 prospective cohort studies. European Journal of Preventive Cardiology, 25(17), 1864–1872. https://doi.org/10.1177/2047487318795194
- Cheung, W. J., Patey, A. M., Frank, J. R., Mackay, M., & Boet, S. (2019). Barriers and Enablers to direct observation of trainees’ Clinical performance: A qualitative study using the theoretical domains framework. Academic Medicine, 94(1), 101–114. https://doi.org/10.1097/ACM.0000000000002396
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. (2018). Retrieved September 2019, from https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf
- Fidler, M. M., Reulen, R. C., Henson, K., Kelly, J., Cutter, D., Levitt, G. A., Frobisher, C., Winter, D. L., & Hawkins, M. M. (2017). Population-based long-term cardiac-specific mortality among 34 489 five-year survivors of childhood cancer in Great Britain. Circulation, 135(10), 951–963. https://doi.org/10.1161/CIRCULATIONAHA.116.024811
- Flannery C., McHugh S., Anaba A. E., Clifford E., O’Riordan M., Kenny L. C., McAuliffe F. M., Kearney P. M., Byrne M. (2018). Enablers and barriers to physical activity in overweight and obese pregnant women: An analysis informed by the theoretical domains framework and COM-B model. BMC Pregnancy and Childbirth, 18(1), 178. https://doi.org/10.1186/s12884-018-1816-z
- Flemming, K., & Noyes, J. (2021). Qualitative evidence synthesis: Where are we at? International Journal of Qualitative Methods, 20, 1609406921993276. https://doi.org/10.1177/1609406921993276
- Geenen, M. M., Cardous-Ubbink, M. C., Kremer, L. C. M., van den Bos, C., van der Pal, H. J. H., Heinen, R. C., Jaspers, M. W. M., Koning, C. C. E., Oldenburger, F., Langeveld, N. E., Hart, A. A. M., Bakker, P. J. M., Caron, H. N., & van Leeuwen, F. E. (2007). Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. JAMA, 297(24), 2705–2715. https://doi.org/10.1001/jama.297.24.2705
- Howlader, N., Noone, A. M., Krapcho, M., Miller, D., Brest, A., Yu, M., Ruhl, J., Tatalovich, Z., Mariotto, A., Lewis, D. R., Chen, H. S., Feuer, E. J., & Cronin, K. A. (Eds.). (2021). SEER cancer statistics review, 1975-2018. National Cancer Institute. Retrieved November 15, 2021, from https://seer.cancer.gov/csr/1975_2018/
- Hudson, M. M., Ness, K. K., Gurney, J. G., Mulrooney, D. A., Chemaitilly, W., Krull, K. R., Green, D. M., Armstrong, G. T., Nottage, K. A., Jones, K. E., Sklar, C. A., Srivastava, D. K., & Robison, L. L. (2013). Clinical ascertainment of health outcomes among adults treated for childhood cancer. JAMA, 309(22), 2371–2381. https://doi.org/10.1001/jama.2013.6296
- Jones, L. W., Liu, Q., Armstrong, G. T., Ness, K. K., Yasui, Y., Devine, K., Tonorezos, E., Soares-Miranda, L., Sklar, C. A., Douglas, P. S., Robison, L. L., & Oeffinger, K. C. (2014). Exercise and risk of major cardiovascular events in adult survivors of childhood Hodgkin lymphoma: A report from the childhood cancer survivor study. Journal of Clinical Oncology, 32(32), 3643–3650. https://doi.org/10.1200/JCO.2014.56.7511
- Kabak, V. Y., Calders, P., Duger, T., Mohammed, J., & van Breda, E. (2019). Short and long-term impairments of cardiopulmonary fitness level in previous childhood cancer cases: A systematic review. Supportive Care in Cancer, 27(1), 69–86. https://doi.org/10.1007/s00520-018-4483-8
- Keats, M. R., Culos-Reed, S. N., Courneya, K. S., & McBride, M. (2006). An examination of physical activity behaviors in a sample of Adolescent cancer survivors. Journal of Pediatric Oncology Nursing, 23(3), 135–142. https://doi.org/10.1177/1043454206287304
- Kolehmainen, N., Francis, J. J., Ramsay, C. R., Owen, C., McKee, L., Ketelaar, M., & Rosenbaum, P. (2011). Participation in physical play and leisure: Developing a theory- and evidence-based intervention for children with motor impairments. BMC Pediatrics, 11(1), 100. https://doi.org/10.1186/1471-2431-11-100
- Kuntz, N., Anazodo, A., Bowden, V., Sender, L., & Morgan, H. (2019). Pediatric cancer patients’ treatment journey: Child, adolescent, and young adult cancer narratives. Journal of Pediatric Nursing, 48, 42–48. https://doi.org/10.1016/j.pedn.2019.06.003
- Lewin, S., Bohren, M., Rashidian, A., Munthe-Kaas, H., Glenton, C., Colvin, C. J., Garside, R., Noyes, J., Booth, A., Tunçalp, Ö., Wainwright, M., Flottorp, S., Tucker, J. D., & Carlsen, B. (2018). Applying GRADE-CERQual to qualitative evidence synthesis findings—paper 2: How to make an overall CERQual assessment of confidence and create a summary of qualitative findings table. Implementation Science, 13(1), 10. https://doi.org/10.1186/s13012-017-0689-2
- Lewin, S., Glenton, C., Munthe-Kaas, H., Carlsen, B., Colvin, C. J., Gülmezoglu, M., Noyes, J., Booth, A., Garside, R., & Rashidian, A. (2015). Using qualitative evidence in decision making for health and Social interventions: An approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLOS Medicine, 12(10), e1001895. https://doi.org/10.1371/journal.pmed.1001895
- Lowe, K., Escoffery, C., Mertens, A. C., & Berg, C. J. (2016). Distinct health behavior and psychosocial profiles of young adult survivors of childhood cancers: A mixed methods study. Journal of Cancer Survivorship, 10(4), 619–632. https://doi.org/10.1007/s11764-015-0508-1
- Martins, J., Marques, A., Sarmento, H., & Carreiro da Costa, F. (2015). Adolescents’ perspectives on the barriers and facilitators of physical activity: A systematic review of qualitative studies. Health Education Research, 30(5), 742–755. https://doi.org/10.1093/her/cyv042
- McKenzie, G., Willis, C., & Shields, N. (2021). Barriers and facilitators of physical activity participation for young people and adults with childhood-onset physical disability: A mixed methods systematic review. Developmental Medicine & Child Neurology, 63(8), 914–924. https://doi.org/10.1111/dmcn.14830
- Methley, A. M., Campbell, S., Chew-Graham, C., McNally, R., & Cheraghi-Sohi, S. P. I. C. O. (2014). PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Services Research, 14(1), 579. https://doi.org/10.1186/s12913-014-0579-0
- Michie, S., Atkins, L., & West, R. (2014). The Behaviour Change Wheel: a guide to designing interventions. Silverback Publishing.
- Michie, S., Johnston, M., Abraham, C., Lawton, R., Parker, D., & Walker, A. (2005). Making psychological theory useful for implementing evidence based practice: A consensus approach. Quality and Safety in Health Care, 14(1), 26–33. https://doi.org/10.1136/qshc.2004.011155
- Michie, S., van Stralen, M., & West, R. (2011). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 6, 42. https://doi.org/10.1186/1748-5908-6-42
- Mizrahi, D., Fardell, J. E., Wakefield, C. E., Simar, D., Maguire, A. M., Hubbard, G., & Cohn, R. J. (2019). How physically active do Australian and New Zealander childhood cancer survivors perceive themselves? A report from the ANZCHOG survivorship study. Complementary Therapies in Medicine, 44, 196–203. https://doi.org/10.1016/j.ctim.2019.04.020
- Nicholson, S. L., Donaghy, M., Johnston, M., Sniehotta, F. F., van Wijck, F., Johnston, D., Greig, C., McMurdo, M. E. T., & Mead, G. (2014). A qualitative theory guided analysis of stroke survivors’ perceived barriers and facilitators to physical activity. Disability and Rehabilitation, 36(22), 1857–1868. https://doi.org/10.3109/09638288.2013.874506
- Noyes, J., Booth, A., Flemming, K., Garside, R., Harden, A., Lewin, S., Pantoja, T., Hannes, K., Cargo, M., Thomas, J. (2018). Cochrane qualitative and implementation methods group guidance series-paper 3: Methods for assessing methodological limitations, data extraction and synthesis, and confidence in synthesized qualitative findings. Journal of Clinical Epidemiology, 97, 49–58. https://doi.org/10.1016/j.jclinepi.2017.06.020
- O'Cathain, A., Croot, L., Duncan, E., Rousseau, N., Sworn, K., Turner, K. M., Yardley, L., & Hoddinott, P. (2019). Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open, 9(8), e029954. https://doi.org/10.1136/bmjopen-2019-029954
- Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan – a web and mobile app for systematic reviews. Systematic Reviews, 5(1), 210. https://doi.org/10.1186/s13643-016-0384-4
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
- Phillips, S. M., Padgett, L. S., Leisenring, W. M., Stratton, K. K., Bishop, K., Krull, K. R., Alfano, C. M., Gibson, T. M., de Moor, J. S., Hartigan, D. B., Armstrong, G. T., Robison, L. L., Rowland, J. H., Oeffinger, K. C., & Mariotto, A. B. (2015). Survivors of childhood cancer in the United States: Prevalence and burden of morbidity. Cancer Epidemiology Biomarkers & Prevention, 24(4), 653–663. https://doi.org/10.1158/1055-9965.EPI-14-1418
- Poitras, V. J., Gray, C. E., Borghese, M. M., Carson, V., Chaput, J.-P., Janssen, I., Katzmarzyk, P. T., Pate, R. R., Connor Gorber, S., Kho, M. E., Sampson, M., & Tremblay, M. S. (2016). Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Applied Physiology, Nutrition, and Metabolism, 41(6 (Suppl. 3)), S197–S239. https://doi.org/10.1139/apnm-2015-0663
- Price, J., Wurz, A., Ramphal, R., Wilson, K., & Brunet, J. (2020). Using a dyadic approach to explore parental support for physical activity among young cancer survivors. Disability and Rehabilitation, 43(19), 2704–2712. https://doi.org/10.1080/09638288.2020.1712621
- QSR International Pty Ltd. (2018). NVivo (Version 12). https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
- Raber, M., Swartz, M. C., Santa Maria, D., O’Connor, T., Baranowski, T., Li, R., & Chandra, J. (2016). Parental involvement in exercise and diet interventions for childhood cancer survivors: A systematic review. Pediatric Research, 80(3), 338–346. https://doi.org/10.1038/pr.2016.84
- Rokitka, D., Heffler, J., Zevon, M., Kitcho, C., Schweitzer, J., Rodriguez, E. M., & Mahoney, M. C. (2021). Designing an exercise intervention for adult survivors of childhood cancers. BMC Cancer, 21(1), 1. https://doi.org/10.1186/s12885-020-07763-8
- Santa Maria, D., Swartz, M. C., Markham, C., Chandra, J., McCurdy, S., & Basen-Engquist, K. (2014). Exploring parental factors related to weight management in survivors of childhood central nervous system tumors. Journal of Pediatric Oncology Nursing, 31(2), 84–94. https://doi.org/10.1177/1043454213518112
- Schindera, C., Zürcher, S. J., Jung, R., Boehringer, S., Balder, J. W., Rueegg, C. S., Kriemler, S., & Weid, N. X. (2021). Physical fitness and modifiable cardiovascular disease risk factors in survivors of childhood cancer: A report from the SURfit study. Cancer, 127(10), 1690–1698. https://doi.org/10.1002/cncr.33351
- Slater, M. E., Steinberger, J., Ross, J. A., Kelly, A. S., Chow, E. J., Koves, I. H., Hoffmeister, P., Sinaiko, A. R., Petryk, A., Moran, A., Lee, J., Chow, L. S., & Baker, K. S. (2015). Physical activity, fitness, and cardiometabolic risk factors in adult survivors of childhood cancer with a history of hematopoietic cell transplantation. Biology of Blood and Marrow Transplantation, 21(7), 1278–1283. https://doi.org/10.1016/j.bbmt.2015.04.007
- Smith, W. A., Li, C., Nottage, K. A., Mulrooney, D. A., Armstrong, G. T., Lanctot, J. Q., Chemaitilly, W., Laver, J. H., Srivastava, D. K., Robison, L. L., Hudson, M. M., & Ness, K. K. (2014). Lifestyle and metabolic syndrome in adult survivors of childhood cancer: A report from the St. Jude lifetime cohort study. Cancer, 120(17), 2742–2750. https://doi.org/10.1002/cncr.28670
- Stössel, S., Neu, M. A., Oschwald, V., Söntgerath, R., Däggelmann, J., Eckert, K., Hamacher, V., Baumann, F. T., Bloch, W., & Faber, J. (2020). Physical activity behaviour in children and adolescents before, during and after cancer treatment. Sport Sciences for Health, 16(2), 347–353. https://doi.org/10.1007/s11332-019-00612-7
- Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology, 8(1), 45. https://doi.org/10.1186/1471-2288-8-45
- Tong, A., Flemming, K., McInnes, E., Oliver, S., & Craig, J. (2012). Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Medical Research Methodology, 12(1), 181. https://doi.org/10.1186/1471-2288-12-181
- Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042
- Vassal, G., Schrappe, M., Pritchard-Jones, K., Arnold, F., Basset, L., Biondi, A., Bode, G., Eggert, A., Hjorth, L., Kamerić, L., Kamerić, N., Karner, S., Kearns, P., Kienesberger, A., Kowalczyk, J., Lack, P., Perilongo, G., Sullivan, R., Tsirou, A., … Ladenstein, R. (2016). The SIOPE strategic plan: A European cancer plan for children and adolescents. Journal of Cancer Policy, 8, 17–32. https://doi.org/10.1016/j.jcpo.2016.03.007
- Winther, J. F., Bhatia, S., Cederkvist, L., Gudmundsdottir, T., Madanat-Harjuoja, L., Tryggvadottir, L., Wesenberg, F., Hasle, H., & Sällfors Holmqvist, A. (2018). Risk of cardiovascular disease among Nordic childhood cancer survivors with diabetes mellitus: A report from adult life after childhood cancer in Scandinavia. Cancer, 124(22), 4393–4400. https://doi.org/10.1002/cncr.31696
- World Health Organization. (2020). Physical activity. Retrieved June 16, 2020, from https://www.who.int/news-room/fact-sheets/detail/physical-activity
- Wright, M., Bryans, A., Gray, K., Skinner, L., & Verhoeve, A. (2013). Physical activity in adolescents following treatment for cancer: Influencing factors. Leukemia Research and Treatment, 2013, 592395. https://doi.org/10.1155/2013/592395
- Wu, Y. P., Yi, J., McClellan, J., Kim, J., Tian, T., Grahmann, B., Kirchhoff, A. C., Holton, A., & Wright, J. (2015). Barriers and facilitators of healthy diet and exercise among adolescent and young adult cancer survivors: Implications for behavioral interventions. Journal of Adolescent and Young Adult Oncology, 4(4), 184–191. https://doi.org/10.1089/jayao.2015.0028
- Yeh, J. M., Ward, Z. J., Chaudhry, A., Liu, Q., Yasui, Y., Armstrong, G. T., Gibson, T. M., Howell, R., Hudson, M. M., Krull, K. R., Leisenring, W. M., Oeffinger, K. C., & Diller, L. (2020). Life expectancy of adult survivors of childhood cancer over 3 decades. JAMA Oncology, 6(3), 350–357. https://doi.org/10.1001/jamaoncol.2019.5582
- Zhang, F. F., Saltzman, E., Must, A., & Parsons, S. K. (2012). Do childhood cancer survivors meet the diet and physical activity guidelines? A review of guidelines and literature. International Journal of Child Health and Nutrition, 1(1), 44–58. https://doi.org/10.6000/1929-4247.2012.01.01.06