
ABSTRACT
Cash transfer programmes have recently emerged as promising interventions for HIV prevention among adolescents in Africa. However, the pathways through which risk reduction occurs are not well understood. We examine data on 1429 adolescents and youth from the Kenya Cash Transfer for Orphans and Vulnerable Children, which has been shown to result in delayed sexual debut among adolescents. We explored three potential mediating pathways: schooling, socio-economic status and psycho-social status. None of these hypothesised mediators greatly altered the main effect. However, school attendance had a larger protective effect on sexual debut among females but was only increased by the programme among males. This gendered pattern of effects may explain why we did not see a mediating effect of the cash transfer through schooling, despite schooling's protective effects against early sexual debut. Results also suggest that cash transfer programmes in Africa can contribute to the reduction of HIV related risk behaviours.
KEYWORDS:
Introduction
Cash transfer programmes have become an important policy instrument in low-income countries for alleviating short-term poverty and facilitating human capital formation. Since the World Bank conducted a review in 2009 on more than 2 dozen developing countries implementing conditional cash transfers (CCT) (World Bank, Citation2009), there has been a rapid increase in cash transfer programmes in sub-Saharan Africa (SSA), with 14 government-run programmes in operation in Eastern and Southern Africa (ESA) alone. The ‘African model’ of cash transfer programmes differs from the well-known Latin American programmes such as Oportunidades (Mexico) and Bolsa Familia (Brazil), which condition payments on children being enrolled in school and select beneficiaries using complex proxy means tests. In contrast, the national programmes in SSA tend to be unconditional, employ community-based or categorical approaches to selecting eligible households, and target on poverty and vulnerability (e.g. families with orphans) rather than on poverty alone (Davis, Gaarder, Handa, & Yablonski, Citation2012; Niño-Zarazúa, Barrientos, Hickey, & Hulme, Citation2012).
Several of the Latin American CCT programmes have undergone social experiments to measure programme impacts, and significant effects have been observed on a range of welfare and human capital outcomes including consumption (Hoddinott & Skoufias, Citation2004), school enrollment (Paul Schultz, Citation2004), child nutritional status (Behrman & Hoddinott, Citation2005), and child development (Fernald, Gertler, & Neufeld, Citation2008; Paxson & Schady, Citation2007). A similar evidence base using social experiments is emerging from the unconditional SSA programmes and the results to date are equally impressive. Impacts on school attendance, for example, mirror those from Latin America (The Kenya CT-OVC Evaluation Team, Citation2012a), and strong effects on productive activity (Covarrubias, Davis, & Winters, Citation2012) and consumption (The Kenya CT-OVC Evaluation Team, Citation2012b) have also been reported.
More recently, given the generalised prevalence of HIV in ESA and the idea that poverty may be an important structural determinant of HIV risk, researchers have sought to examine the ability of cash transfers to reduce HIV risk (Heise, Lutz, Ranganathan, & Watts, Citation2013; Pettifor, MacPhail, Nguyen, & Rosenberg, Citation2012; Wamoyi et al., Citation2014). One line of inquiry examines the potential for monetary incentives to influence HIV related risk behaviour, and a conceptual framework for this link is offered in Medlin and De Walque (Citation2008). A second line of inquiry examines the ability of cash transfers to more broadly address structural drivers of HIV, including poverty and low levels of schooling.
In testing the former, the evidence that monetary incentives directly linked to sexually-transmitted infections (STI) testing can reduce risky sexual behaviours is limited (Bjorkman Nyqvist, Corno, De Walque, & Jakob, Citation2015; De Walque et al., Citation2012; Kohler & Thornton, Citation2012). In a randomised-control trial (RCT) among individuals aged 18–30 in rural Tanzania, limited evidence was found that a cash transfer conditional on testing negative for four sexually transmitted infections reduced the prevalence of testing positive for their combined prevalence. However, the relationship between cash transfers and STIs was driven not by the STIs conditioned on at baseline. Rather, a significant relationship between cash transfers and STIs was only found in an aggregate measure of STI prevalence, which included a lesser known STI not tested at baseline, and for which there is no rapid test available and treatment guidelines are unclear. Slightly higher payments were associated with larger effects (De Walque et al., Citation2012). In contrast, Kohler and Thornton (Citation2012) report no impact on maintaining HIV-negative status from an experimental CCT in Malawi (Kohler & Thornton, Citation2012). Finally, a lottery experiment in Lesotho with eligibility for pay-outs in the treatment arm tied to testing negative for two STIs found that the intervention reduced HIV incidence over two years; however this impact was driven by the sub-sample of risk-loving individuals (Bjorkman Nyqvist et al., Citation2015).
In the second line of inquiry examining cash transfers (either unconditional or conditional on schooling attendance), which more broadly address structural drivers of HIV, there is growing evidence that cash transfers can reduce sexual debut, pregnancy, and HIV prevalence. A cash transfer to young women in Malawi that was conditional on school enrollment decreased the prevalence of HIV and herpes simplex 2 (Baird, Garfein, McIntosh, & Ozler, Citation2012), and reduced sexual debut among girls who were not attending school at baseline (Baird, Chirwa, McIntosh, & Ozler, Citation2010). Further, a three-year RCT of a school-based CCT in rural Zimbabwe found that comprehensive school support is effective in reducing early marriage among orphan girls (one or both parents deceased) who were in grade six at study entry (Hallfors et al., Citation2011). In South Africa, an evaluation of a fully scaled up, unconditional cash transfer programme, the Child Support Grant (CSG), found that the programme decreased adolescent sexual activity and pregnancy (Heinrich et al., Citation2012). Another analysis of impacts of the CSG found reductions in transactional and age-disparate sex among female adolescents (Cluver et al., Citation2013). Finally, the Kenya Cash Transfer for Orphans and Vulnerable Children (CT-OVC) has been previously shown to have had a significant effect in delaying sexual debut among young people aged 15–25 in intervention households (Handa, Halpern, Pettifor, & Thirumurthy, Citation2014), as well as pregnancy among female adolescents aged 15–24 (Handa et al., Citation2015).
Although the aforementioned evidence suggests that cash transfer programmes can influence HIV risk-related outcomes in some target groups, the precise mechanisms for the observed impacts are unclear. Our main objective in this article is to understand how the CT-OVC has achieved this reduction in sexual debut among youth in intervention households by exploring the three mediators described above: schooling, household economic status, and youth mental health. This study fills an important gap in our knowledge about cash transfers and HIV risk by providing evidence on the potential mechanisms within the context of a national social protection programme. The programme we examined is the Government of Kenya's CT-OVC, the country's largest social protection programme. The basic design features of this programme are similar to most of those found in ESA – targeting includes an important community element, cash is provided to families and not specific individuals, and payments are unconditional – thus greatly enhancing the external validity of these results to other countries in the region.
Background and conceptual model
Sexual debut has important implications for HIV risk, educational attainment, and subsequently, future productivity. In this article we explore three pathways through which a cash transfer could affect sexual debut based on our own conceptual model (). We provide an explanation for each of these pathways, including schooling, economic well-being, and mental health and well-being ().
Figure 1. Conceptual model.
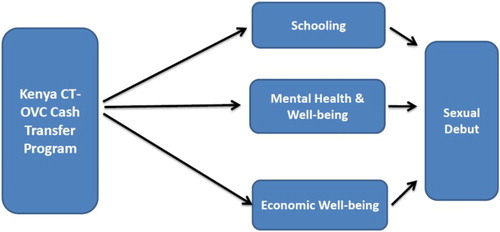
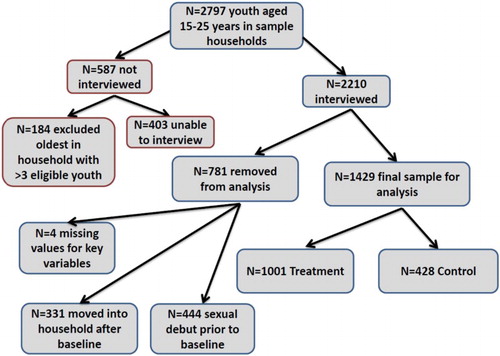
Figure 2. Overview of youth sample, Kenya OVC-CT, 2011.
Schooling
Schooling may be protective against early sexual debut for different reasons. First, school provides an environment where sex is less likely to occur (Jukes, Simmons, & Bundy, Citation2008; Rosenberg, Pettifor, Thirumurthy, Halpern, & Handa, Citation2014). Education may also provide hope for the future, increasing the opportunity cost of sex and childbearing, causing young people to defer risk in order to invest in their own potential (Birdthistle et al., Citation2009). Alternatively, young people who remain in school or complete more education may be systematically different from those who drop-out in other ways such as in socio-economic status or resiliency; thus school attendance may be a proxy for those factors.
The existing evidence on the relationship between educational attainment and sexual debut generally supports a protective effect of education on timing of sexual debut, particularly among females. A recent review of Demographic and Health Surveys (DHS) from 24 countries in Africa between 2000 and 2010 found that individuals with more education were less likely to report early sexual debut. However, associations with partner number were in the opposite direction; women with more education reported more partners (Doyle, Mavedzenge, Plummer, & Ross, Citation2012). This unexpected association is likely explained by the fact that individuals with more education often marry later, accounting for increased partner numbers. Those with more education were also more likely to report using condoms (Doyle et al., Citation2012). Another recent review of sexual behaviour and educational attainment in SSA found protective effects of education on sexual debut in 14 out of 22 studies among girls and mixed evidence among males (Zuilkowski & Jukes, Citation2012). Specifically, current attendance was protective among females in five out of seven studies (and three out of seven studies among males). Together, this body of evidence supports the hypothesis that education is protective against early sexual debut but also underscores the importance of examining this relationship separately by gender. A limitation of existing studies reviewed above is that they are largely cross-sectional and cannot always infer causality. Evidence from two randomised studies (which can better infer causality) in Kenya, where the interventions provided a combination of school fees and/or school uniforms, found that interventions led to decreased probabilities of sexual debut. In one study, where students in upper primary school were provided an education subsidy in the form of free uniforms, a two-year evaluation found a 2.3 percentage point reduction in sexual debut among females as a result of the intervention but no impact among males (Duflo, Dupas, Kremer, & Sinei, Citation2006). Furthermore, after two years, girls receiving free uniforms in this study were 1.5 percentage points less likely to have started childbearing and 1.4 percentage points less likely to be married. A longer term evaluation (after approximately seven years) of the same intervention found no statistically significant programme impacts on sexual debut or age at first sex (Duflo, Dupas, & Kremer, Citation2014). However, the long-term study did find a lasting reduction in childbearing rates (46% of treatment girls and 49% of control girls) as a result of the programme. A second intervention among 105 orphaned children in a rural location near Kisumu, Kenya, randomised treatment (n = 53), which comprised school fees and uniforms, and found that the intervention led to a decrease in sexual debut (19.2% among treatment versus 33.3% among control at follow-up); however the study's authors did not provide gender-disaggregated results (Cho et al., Citation2011), likely because of the small sample size.
Overall, cash transfer programmes, both unconditional and conditional, have a strong track record of keeping young people in school (Paul Schultz, Citation2004; The Kenya CT-OVC Evaluation Team, Citation2012a). We hypothesise that increased attendance leads to reduced probability of sexual debut and subsequent HIV risk.
Mental health
A second potential pathway through which cash transfers may affect sexual risk involves improvements in mental health. Neuropsychiatric disorders are one of the six main contributors to disability-adjusted life years, defined as the equivalent of loss of one year of healthy life, lost among youth aged 10–25 years (Gore et al., Citation2011). While often undiagnosed and untreated, approximately half of mental health disorders manifest by age 14 (World Health Organization, Citation2014). The social causation hypothesis posits that stress, social exclusion, decreased social capital, malnutrition, and other factors associated with poverty increase the risk of mental illness. Further, poverty and poor mental health are mutually reinforcing and increase vulnerability to each condition (Lund et al., Citation2011). Patel and colleagues propose a conceptual model illustrating these reinforcing links between poverty and poor mental health, whereby economic deprivation, low education, unemployment, and lack of basic amenities lead to social exclusion, stressors, and malnutrition, which ultimately lead to higher prevalence, lack of care for, and more severe courses of mental health. The latter then lead to loss of employment, increased health expenditures, reduced productivity, and social drift (Flisher et al., Citation2007; Lund et al., Citation2011; Patel & Kleinman, Citation2003).
The provision of cash transfers may improve mental health and well-being of adolescents in recipient households via their positive impacts on food security, future expectations, and physical health. These improvements may, in turn, result in reductions in risky sexual behaviour. Indeed, previous research has shown that adolescents with mental disorders face a higher risk of acquiring HIV/AIDS. This association may be due to limited sexual communication skills, susceptibility to negative peer influence, apathy, as well as limited perceptions of self-efficacy, and poor assertiveness and negotiation skills (Brown, Danovsky, Lourie, DiClemente, & Ponton, Citation1997; Donenberg, Citation2005; Donenberg, Emerson, Bryant, Wilson, & Weber-Shifrin, Citation2001).
The impact of cash transfer programmes on the mental health of youth is an understudied topic. In the past, evaluations of social cash transfers have been more generally focused on outcomes related to consumption, food security, schooling, and physical health. Mental health has only more recently been incorporated in instruments used in evaluations of social cash transfers (Baird, De Hoop, & Özler, Citation2013; Paxson & Schady, Citation2007; The Transfer Project, Citation2015). A recent review of evaluations of cash transfer programmes concluded that evidence on the ability of poverty alleviation programmes to improve mental health is inconclusive to date (Lund et al., Citation2011). One study of a localised experiment involving a combination of conditional and unconditional cash transfers in Malawi did show positive impacts, but these dissipated once the experiment ended (Baird et al., Citation2013), while another study from Ecuador measured maternal mental health using the Center for epidemiologic studies depression scale (CES-D) scale and found a positive but insignificant link between receipt of cash transfers and mental health among women in the lowest income quartile (Paxson & Schady, Citation2007).
Guided by the social causation hypothesis, we hypothesise that social cash transfers can positively impact mental health through reductions in food insecurity and social exclusion. This in turn may lead to a reduction in risky sexual behaviours and subsequent HIV risk based on the aforementioned literature linking mental health and adolescent sexual risk-taking.
Economic well-being
A third pathway through which cash transfer programmes may delay sexual debut is through increased economic well-being. Cash transfer programmes were developed as social safety nets targeting poor and vulnerable households so that families could afford to improve their well-being through better food, education, and health care. Existing evidence supports the fact that cash transfer programmes have been successful at improving overall consumption and diet diversity (Hoddinott & Skoufias, Citation2004; The Kenya CT-OVC Evaluation Team, Citation2012b).
Economic insecurity may encourage earlier sexual debut through incentivising engagement in transactional sex (for goods such as food, housing, social status, or money) or by lowering future expectations. Young women are at particularly heightened risk for transactional sex relationships compared to young men, due to their relative economic vulnerability and disenfranchisement (Luke, Citation2003; Robinson & Yeh, Citation2011). Existing empirical studies using population-based data from Africa show that poverty is a risk factor for early sexual debut. A study from four African countries showed that poorer girls (but not boys) had sex earlier than their wealthier counterparts in three of the four countries studied (Madise, Zulu, & Ciera, Citation2007). Further, among urban residents, individuals residing in slums report earlier sexual debut and riskier sexual behaviours compared to those not residing in slums (Greif, Dodoo, & Jayaraman, Citation2011).
If cash transfer programmes successfully improve economic well-being, then this improved economic well-being may, in turn, improve sexual risk outcomes, including age at sexual debut, among programme recipients. However, in cash transfer programmes where cash is going directly to the household head and not to the young women or adolescents, changes in economic welfare at the household-level may not have as strong a relationship with the risk of transactional sex or other risk behaviours.
Study design
Intervention: The Kenya CT-OVC programme
The Kenya CT-OVC operated in approximately 100 districts, reaching over 200,000 households and 300,000 OVC across the country as of 2015. The programme began as a pilot in Garissa, Kwale, and Nairobi in 2004, with technical assistance from United Nations Children’s Fund (UNICEF), and was subsequently integrated into the national budget and began phased expansion in 2007. The objective of the programme is to provide regular cash transfers to families living with orphans and vulnerable children (OVC) to encourage fostering and retention of children and to promote their human capital development. Eligible households, those who are ultra-poor (falling in the lowest expenditure quintile based on proxy means testing) and contain an OVC, receive a flat monthly transfer of 25 USD 2000 Kenyan Shilling (Ksh), which was equivalent to approximately 20% of baseline monthly household expenditures among the evaluation sample. An OVC is defined as a household resident between 0 and 17 years old with at least one deceased parent, or who is chronically ill, or whose main caregiver is chronically ill. Payments are made through post offices and benefits are paid every two months. Beneficiary households are informed that, in exchange for the cash payment, the care and protection of the resident OVC is their responsibility though there are currently no punitive sanctions for noncompliance with this responsibility. Support lasts until all children age out (i.e. turn 19).
Targeting of households for the programme is conducted in three stages. In stage one, each location (a location is the fourth administrative level below province, district, and division) forms an OVC Committee that prepares a list of all potentially eligible households in the location that meet the demographic and poverty criteria. In stage two, the list of eligible households is sent to the programme's central office (located within the Ministry of Gender, Children and Social Development), which then administers a detailed socio-economic questionnaire to assess poverty and confirm eligibility in order to rank households. The final number of households that enters the programme in each district depends on funding to that district, but approximately 20% of the poorest households in each location are enrolled in the programme. In cases where more households meet the eligibility criteria than funds are available, households are prioritised with child-headed households receiving the first priority (of which there are very few), followed by elderly headed households. An evaluation of the targeting performance of the programme reports very favourable targeting relative to other cash transfer programmes across the developing world (Handa et al., Citation2012).
The impact evaluation design
Prior to programme expansion of the CT-OVC in 2007, UNICEF designed a social experiment to track the impact of the programme on a range of household welfare indicators including food security, child health, and schooling. The evaluation entailed a cluster randomised longitudinal design, with a baseline household survey conducted in 2007 and a 24-month follow-up in 2009. The ethical rationale for the design was that the programme could not expand to all eligible locations at the same time, so locations whose entry would occur later in the expansion cycle could be used as control sites to measure impact. Thus within each of seven districts across the country (Kisumu, Homa Bay, Migori, Suba, Nairobi, Garissa, and Kwale), four locations were identified as eligible, and two were randomised for immediate implementation and two were randomised for deferred expansion, serving as control locations. More information on the evaluation study design and results from the impact evaluation can be found elsewhere (Handa, Halpern, et al., Citation2014; The Kenya CT-OVC Evaluation Team, Citation2012a, Citation2012b).
In 2011, we returned to the households in the original evaluation sample that had been re-interviewed in 2009 and administered the same household survey plus an additional module for up to three young people aged 15–25 in the household. The additional module covered sexual activity, mental health, and knowledge about HIV. This module was administered face-to-face in a private area by an enumerator of the same sex, and research protocols followed those used in the Kenya DHS. Informed consent was obtained from youth aged 18 or above, and assent plus parental informed consent was obtained for youth aged 15–17 years. If privacy could not be assured, then enumerators were instructed to not conduct the interview. In households where there were more than three youth in the age range, enumerators were instructed to interview the youngest three in order to prioritise respondents who were less likely to have had their sexual debut. Since this module was only administered in 2011, we reconstructed baseline sexual debut status by recording the age at which the respondent first had sex and calculating whether it occurred before or after baseline. It is important to note that HIV prevention is not the main objective of the CT-OVC and so the sample size for the original evaluation was not based on this sexual risk indicator. The 2011 study was approved by the University of North Carolina at Chapel Hill Institutional Review Board and the Kenya Medical Research Institute Ethics Review Committee.
Attrition and balance between intervention and control arms
The initial study period coincided with a time of political turmoil in Kenya resulting from the disputed national elections in December 2007. Over 1000 people died and approximately 400,000 people were internally displaced at this time. Consequently, household-level attrition between baseline and the first follow-up in 2009 was 17% and concentrated in Kisumu and Nairobi, the two locations in the study that experienced the most election-related unrest. Attrition between the 2009 and 2011 rounds was only 5%. Supplementary table (Table 1, see supplementary material) shows means of selected demographic and poverty measures for households in each arm across the three waves for all households in the evaluation sample (panel A includes all households in the evaluation sample, while panel B includes only those households that contained a youth interviewed in the youth module). Means for these indicators were stable across the three waves despite the relatively high attrition rate between 2007 and 2009, indicating that the representativeness of the sample remained intact.
To further explore the potential for selective attrition we estimated the probability of households attriting between 2007 and 2009 using baseline values for the variables reported in supplementary table (Table 1, see supplementary material) plus district dummy variables, the number of residents in each of five age categories and the log of household size. The only statistically significant variables out of the 26 total variables in this regression were the indicators for Kisumu and Nairobi, the number of residents aged 12–17, log of household size, and unprotected water source. The probability of attriting was 19 and 9 percentage points higher for households in Nairobi and Kisumu, respectively (relative to the reference), while households in the intervention group were 8 points less likely to be lost at follow-up relative to the control group. To assess whether there was any differential determinant of attrition between the two groups we re-estimated this model interacting each regressor with the indicator for intervention status. In only two cases (out of a possible 26) was there a statistically significant interaction effect (the indicator for residence in Kwale, and the number of residents aged 6–11). Based on the stability of characteristics in each arm across the waves, the fact that the two most important determinants of attrition stem from residence in Kisumu and Nairobi, which were disproportionately affected by the election violence relative to other study sites, and the minimal differences in the determinants of attrition across arms (results available from authors upon request), we believe that selective attrition is not a concern in the subsequent analysis.
Supplementary table (Table 1, see supplementary material) shows differences between intervention and control arms of the study at the household-level in each wave. The poverty-related variables are balanced – that is, there are no statistically significant differences – across arms in each wave, but there are statistically significant differences in the age, sex, and schooling levels of household heads across arms. This is due to the prioritisation process that occurred at the central Ministry because the number of households on the list exceeded the budget. Due to the small number of child-headed households, the prioritisation process effectively gave the most weight to elderly headed households. Since the final prioritisation process was not conducted in control locations as they were not scheduled to immediately enter the programme, households in the control arm of the study were drawn from a slightly larger eligibility list than those from the intervention arm resulting in the differences in heads’ characteristics observed in supplementary table (Table 1, see supplementary material). Furthermore, panel B indicates that among this sub-sample of households (i.e. those that had a youth interviewed in the youth module), there were differences in some household-level poverty indicators (material of walls, floors and source of water), and we control for these characteristics as detailed below. It is important to note however that there is no element of self-selection into the programme; household eligibility was completely supply driven and take-up was universal.
Response rate in adolescent survey
We administered the special module on sexual activity to up to three household residents aged 15–25 in the household. A total of 2210 out of a possible 2797 individuals aged 15–25 were interviewed. Of the 588 individuals not interviewed, 184 were purposefully excluded because they were the oldest in a household with more than three members in the target group, leaving an actual response rate of 85%. The most common reason for non-response was that respondents were in boarding school or away from home during the study period due to work or other reasons. The response rate is higher in the control arm (87% versus 83%), which is consistent with the fact that the CT-OVC has had a positive impact on secondary school attendance and individuals in treatment households were thus more likely to be away in boarding school.
We performed several checks to understand the potential implications of the non-response rate for our results. We posited that age, sex, schooling of the household head, and per capita household expenditure would be the most important determinants of non-response. We tested to see whether variables that predict non-response might also predict sexual debut, as this would then be a cause for concern because it would change the underlying distribution of determinants in our main regression on sexual debut. First we compared the age and sex of respondents versus those that should have been interviewed but were not, and found no statistical differences between the two groups. However non-respondents were 4 percentage points more likely to be attending school relative to respondents (66% versus 62%). When comparing the age, sex, schooling of the head of household, and per capita household expenditure between respondents and non-respondents, we did not find any statistically significant differences.
For our sample for analysis, we removed youth who joined the household after the programme began, and therefore had less exposure to the programme than youth living in the household the entire period; inclusion of these ‘movers-in’ may have attenuated estimation of programme impacts. Finally, we restricted our analysis to those who had not had sex prior to baseline interviews (since those debuting before baseline could not be impacted by the programme with respect to this outcome). We examined the full age range available in this resulting sample in order to examine a key facet in the transition to adulthood among the group of individuals with the highest incidence of HIV infection – those aged 15–24 accounted for 42% of new HIV infections among all individuals aged 15 and older (UNAIDS, Citation2012).
We checked for differences between households in treatment and control arms among the following characteristics: (1) those households with three or fewer youth versus those with more than three youth and (2) those with ‘movers-in’ versus those with none, and found no statistically significant differences (i.e. the sample was balanced on these characteristics). The percentage of households with more than three youth in the target age range for this analysis was 10.6% and 12.7% of control and treatment households, respectively (p = .29). Furthermore, 24.9% and 24% of control and treatment households, respectively, had any ‘movers-in’ (p = .35). Finally, there was balance between individuals in treatment and control arms with respect to sexual debut at baseline (25% of control and 23% of treatment had already sexually debuted at baseline; p = .35).
Methods and measures
Measures
Our outcome of interest was sexual debut (reported in 2011), defined as first vaginal sex having occurred since the intervention began (i.e. after 2007).
We measured schooling (as reported in 2009) as a dichotomous variable that equals one if the respondent was either in school at the time of the survey or, if not in school, had completed at least grade 12 (secondary education) and zero otherwise. We used this definition rather than a simple measure of current enrollment or attendance because our sample includes respondents up to age 25 who may have completed their secondary schooling without early drop-out. Most drop-outs in Kenya occur either during the transition between primary and secondary school (age 13–14) or after completion of secondary school (age 18) (The Kenya CT-OVC Evaluation Team, Citation2012a); therefore, a significant portion of our sample had aged out of schooling by the time of the follow-up survey. Earlier work has shown that the CT-OVC had a strong positive impact on school attendance among the 12–17 age group (The Kenya CT-OVC Evaluation Team, Citation2012a), which would presumably be reflected in higher levels of grade attainment and ultimately more young people completing secondary school. Note that grade attainment itself would not account for those who are still currently in school; our constructed measure reflects both current attendance and the attainment of an important schooling milestone in rural Kenya. We use youth's current attendance (in 2009) as reported by the household and do not check against school attendance rosters because the latter is not available in our data but may also be unreliable due to incomplete recording.
We measured mental health and well-being in our survey (reported in 2011) using two indicators: depression and hope. For depression, we used a 10-item short-form of the CES-D scale (Radloff, Citation1977). The 10-item scale is based on a longer 20-item scale and has been validated internationally (Boey, Citation1999; Bojorquez Chapela & de Snyder, Citation2009; Cheung, Liu, & Yip, Citation2007) and implemented in Africa (Onuoha, Munakata, Serumaga-Zake, Nyonyintono, & Bogere, Citation2009). It has high internal consistency and reliability in household surveys across a variety of demographic characteristics (Andresen, Malmgren, Carter, & Patrick, Citation1994); in our sample Cronbach's α was 0.75. The short-form is interpreted as a measure of the current level of depressive symptoms, focusing on the affective component of the depressed mood. Questions were asked on a Likert scale that elicits self-reported answers about whether certain feelings or behaviours occurred ‘rarely or none of the time', ‘some or a little of the time', ‘occasionally or a moderate amount of the time', or ‘all the time’ in the past seven days. To calculate the scale, scores are summed for all 10 questions and can range from 0 to 30, with higher scores reflecting more depressive symptoms. We constructed a binary outcome variable indicating whether the respondent scored 10 or lower on the scale as this is considered to be a threshold for depression (Ardington & Case, Citation2009; Radloff, Citation1977).
For our second psycho-social indicator, we utilised a six-item Hope Scale (Snyder et al., Citation1997). This measure is intended to capture hope and optimism by assessing respondents’ perception of their ability to achieve a desired goal. This measure takes into account awareness, self-agency, and available pathways (Snyder et al., Citation1997), and has been used elsewhere in SSA (Barnett, Seeley, Levin, & Katongole, Citation2015; Senefeld, Strasser, Campbell, & Perrin, Citation2011). Items for this scale were assessed using a one to five Likert scale (total range of 6–30), with higher scores signifying greater optimism. For purposes of analysis, we converted the Hope Scale into a binary variable to indicate hopefulness (=1 if score ≥ median of 22). Cronbach's α was 0.68 for these items in our sample.
Economic welfare was measured using total household per capita consumption expenditures on food and non-food items (reported in 2009), which is considered the gold standard in the measurement of poverty and monetary well-being (Deaton, Citation1997; Ravallion, Citation1998). We collected expenditure information on 70 separate items of consumption, including the value of own production, which we aggregate and divide by household size to obtain a monthly total per capita consumption measure.
Additional controls used in our analysis included youth's age in years, binary indicators for whether the youth is the child or grandchild of the household head (reference = other relationship), gender of household head (=1 if female), household head's highest educational attainment (in years), household head's age (in years), walls made of mud/dung/grass/sticks, floors made of mud/dung, and unprotected water source. These controls were all measured at baseline (2007), with the exception of youth's age in years (measured at 2011).
Statistical analysis
To explore the potential mediating effects of schooling, mental health, and consumption expenditures we followed the conceptual framework and approach originally published by Baron and Kenny (Citation1986). We first estimated the main effect of the intervention (residence in a household receiving the CT-OVC) and the dependent variable (sexual debut). We then included each of the potential mediators (separately) along with CT-OVC status in the main model predicting sexual debut to see if they attenuate the treatment effect. Finally we ran a model with treatment and all mediators included together.Footnote1 Impacts of the programme on mediators (a pre-condition for each of them to act as a potential mediator) are presented in Appendix A (full sample) and Appendix B (by gender) (see supplementary material for appendices). All of the mediators were taken from interviews in 2009, with the exception of mental health indicators (depression and hopefulness), which were available only in the 2011 wave (contemporaneous with the sexual debut measure). We did this to reflect the temporal ordering of the programme, mediators, and, finally, sexual debut.
We estimated multivariate probit regression models and report marginal effects for binary outcomes (sexual debut, not depressed, hopefulness, educational status) and ran linear regressions for expenditures. In all regressions, we included a binary treatment indicator, comparing differences in 2011 between treatment and control groups and controlled for the household characteristics that are statistically different between intervention and control arms in supplementary table (Table 1, see supplementary material). We also included the age and sex of the respondent, indicators for whether the respondent is the child or grandchild of the household head, and six district dummy variables. We corrected the standard errors for clustering at the household-level to account for multiple respondents in the same home.
Finally, we ran all analyses stratified by gender given existing evidence that cash transfers and at least one of our mediators (education) may influence sexual debut among males and females differently, and also because these mediation pathways may be different if there are different gender norms or expectations, or if there is preferential family spending for one sex over the other.
Identification
In the comparison of intervention and control arms four years after programme initiation, our key identification assumption in order to attribute differences in observed outcomes to the programme was that the outcomes were balanced at baseline and both groups experienced ‘parallel trends’. By removing all respondents who had their sexual debut prior to baseline, we ensure balance at baseline. Schooling and household expenditures are balanced at baseline as reported previously (The Kenya CT-OVC Evaluation Team, Citation2012a, Citation2012b). The only outcomes for which we could not confirm baseline balance was the CES-D and Hope Scale, which were not collected at baseline. Parallel trends were addressed in the original study design by drawing control households from the same district as the intervention.
Results
Sample
Starting from N = 2210 youth for our sample for analysis, we removed 333 youth who joined the household after the programme began, 444 who had had sex prior to baseline interviews, and an additional 4 observations missing information on variables used in our analysis. Our final sample for analysis was N = 1429 youth aged 15–25.
Descriptive statistics
Supplementary table (Table 2, see supplementary material) presents the distribution of the main outcome variable, potential mediating variables, and controls by intervention and control arms of the analytic sample. We see differences in our outcome of interest (35.7% of treatment youth and 44.4% of control youth have sexually debuted; p < .01) and two of the mediators (depression, p < .10 and expenditures p < .01), suggesting programme impacts on these variables, which we further tested below in multivariate models. In general, examining control variables, the two arms were well-balanced in terms of characteristics of the adolescents themselves (gender, age). However, the distribution of the relation between the adolescent and household head was different by study arm: participants in intervention households were more likely to be grandchildren of the household head and less likely to be children or siblings of the household head, compared to control participants; we included these variables as controls in all models. The differences in characteristics of the household head (age and education) reflect those shown in supplementary table (Table 1, see supplementary material) (at the household-level) and so we included these as controls as well. The proportion of females is only 39% in the analytic sample, which is the same as at baseline for children in this age group. Among the target population for the programme (ultra-poor and containing OVC), there appear to be significantly more males than females resident in these households.
Programme impacts on mediators
Programme impacts on hypothesised mediators are shown in Appendix A (full sample) and Appendix B (by gender). In the combined sample on the Hope Scale (Appendix A, column 3; p < .10) and household expenditures (Appendix A, column 4; p < .05). More in-depth analysis of programme impacts on mental health is available elsewhere (Kilburn, Thirumurthy, Halpern, Pettifor, & Handa, Citation2014). When examining impacts by gender, we see heterogeneous effects, with the cash transfer programme being strongly associated with schooling and hope among males but not among females (Appendix B). Indeed, findings from the first two waves of the evaluation showed a large and statistically significant impact of the programme on secondary school attendance among both males and females (The Kenya CT-OVC Evaluation Team, Citation2012a); the lack of significance among females and in our combined sample is likely due to the smaller size of our analytic sample which is derived from the sample of individuals interviewed in the young person's module as well as the different age range examined. Among females, household expenditure was the only hypothesised mediator for which we found programme impacts (Appendix B, column 4), whereas, among males, there were significant impacts on education, hope, and expenditures (Appendix B, columns 9, 11, 12; p < .05).
Main effects and mediation
Next we examined mediation by those variables for which we found significant treatment impacts (). Column 1 shows the impact of the CT-OVC on sexual debut. Individuals between the ages of 15 and 25 who were residing in treatment households were 9.4 percentage points less likely to have had sex. The remaining columns (columns 2–3) show this relationship after controlling for potential mediators. In the overall sample, we found no evidence of mediation.
Table 1. Impacts of Kenya CT-OVC and mediators on sexual debut, probit regression models, Kenyan adolescents, aged 15–25 years, 2011 (N = 1429).
When examining impacts and mediation separately by gender (see Table 3 in supplementary material), we found larger programme impacts among females (14 percentage points; p < .01; columns 1–2) than among males (ranging from 7 to 8 percentage points; p < .10; columns 3–6). However, we only find evidence of mediation among males, and this mediation is limited to schooling. When controlling for education, programme impacts attenuated slightly (from 7.8 percentage points to 7.0 percentage points).
In Appendix C (see supplementary material) we provide additional models which control for schooling and mental health, and fully adjusted models which were not included in supplementary table (Table 3, see supplementary material). Since there were no programme impacts on schooling and mental health, these indicators cannot work as mediators; however, we wanted to demonstrate the protective effects of schooling and mental health among females. Schooling elicited a strong protective effect on sexual debut, particularly among women, where the probability of sexual debut is reduced by 31 percentage points if a female was either still in school or completed grade 12 (Appendix C, column 1) compared to a 12.5 percentage point reduction among males (Supplementary Table 3, column 4).Footnote2 This pattern of results may help explain why we do not observe a larger mediating effect of the grant through schooling on sexual debut. Though we did not find programme impacts on mental health among females, we did find large protective associations between mental health and sexual debut among females. Females not experiencing depressive symptoms were 10 percentage points less likely to have had sex (p < .10, Appendix C, column 2), and females with scores above the median on the Hope Scale, which measures agency, were 8.6 percentage points less likely to have had sex (p < .05, Appendix C, column 3). Neither of the mental health indicators were associated with sexual debut among males (Table 3, see supplementary material).
Extensions
We conducted three extensions to the main analyses described above. Since the Kenya CT-OVC explicitly targets families with at least one orphan or vulnerable child, we investigated whether our results differed for orphans. Previous literature has suggested that orphans in particular may be more at risk of HIV because of worse mental health (Cluver & Gardner, Citation2007) or because they may be more likely to engage in transactional sex (Beegle & Krutikova, Citation2007; Palermo & Peterman, Citation2009). In our analytic sample 81% are orphans, of which 64% are single orphans and the remaining are double orphans. We found no differential treatment effect of the CT-OVC on sexual debut for orphans, single orphans or double orphans. We also did not find any differential treatment effects on the potential mediators by OVC status, with the exception of the Hope Scale (OVC status is negatively associated with hope, and the programme mitigates some of this impact among orphans).
The second extension we conducted was to restrict our analysis to a younger age range (15–21 years), since these are the children on which programme eligibility would have been based in 2007 (at which point they were aged 17 or under). Results mirrored those in the main analyses presented above (namely, no evidence of mediation), but overall treatment impacts were slightly lower (7.4 percentage point reduction in sexual debut versus 9.4 percentage points in sample will full age range). Among females, impacts ranged from 8.3 to 9.2 percentage points, and among males, they ranged from 6.9 to 8.3 percentage points in this younger sample.
The third extension we conducted was to expand our analytic sample to include ‘movers-in', or youth who were not present in the household at baseline, but rather had entered at some point between 2007 and 2011 and were thus exposed to the treatment for less time. The results when we used this expanded sample were similar to those reported here, though with a slightly lower main treatment effect (8.9 percentage point impact among the expanded sample compared to 9.4 in the full sample and 10.7 percentage points among females in the expanded sample compared to 14.2 percentage points among females in the full sample; in both samples impacts among males more closely mirrored impacts in the pooled gender analyses). The pattern of results, however, remained the same (results not shown).
Discussion
This paper is the first to investigate the pathways through which a national poverty targeted cash transfer programme, the Kenya CT-OVC, affects the sexual behaviour of young people, and was possible thanks to an innovative feature of the evaluation, namely direct interviews with youth. To date, few evaluations of cash transfers not specifically targeted to adolescents have included youth modules, which can help elucidate programme impacts on the transition to adulthood. Adolescence is a critical juncture in life, and timing and context of these transitions have implications for future outcomes, including educational attainment, productivity, and health. Social cash transfers have been highlighted as promising interventions to prevent HIV and adolescent childbearing in low- and middle-income countries (McQueston, Silverman, & Glassman, Citation2013; Pettifor et al., Citation2012). We posited and tested three potential pathways that cash transfers may delay sexual debut among youth: schooling, mental health, and economic well-being. The programme had an effect on postponing sexual debut among young people aged 15–25. The programme also improved household economic well-being and the mental health of young people in our analytic sample. However, we do not find convincing evidence that these are mediating the effect of the CT-OVC on sexual debut.
There is an important gender difference in the pattern of effects that is worth highlighting. Specifically, schooling is much more strongly protective for sexual debut among young women yet the impact of the CT-OVC on schooling is stronger for men. This pattern of relationships may well explain why we do not observe a mediating effect of the cash transfer through schooling on sexual debut. These differential impacts are consistent with existing evidence on gender and the protective effects of schooling on sexual debut (Zuilkowski & Jukes, Citation2012), as well as barriers to school attendance (Duflo et al., Citation2006).
Similarly, while the programme had stronger positive impacts for mental health among males than among females (Kilburn et al., Citation2014), we found mental health to be protective in preventing sexual debut among females but not males. These differential impacts could again explain the lack of mediation by mental health found here, and impacts of cash transfers on sexual behaviours could still be mediated by mental health status, particularly among females, in other settings where cash transfers are found to have strong direct impacts on mental health. Indeed, the impact of cash transfers on youth mental health is an understudied area that warrants further investigation. Our findings of no treatment impacts on mental health among females are at odds with initial findings from a small, non-government-run programme in Malawi (Baird et al., Citation2013); however, even impacts from the latter study dissipated after the programme ended.
The characteristics of the target population are such that the majority of young people are male (two-thirds), which likely explains why we tend to see stronger impacts on males. From a statistical perspective, there is also more power to detect differences between treatment and control among males. The policy implication is that the programme may need to provide additional support (e.g. information, case management) for beneficiary households with females in this age range. Additionally, these relationships should be further examined in other African contexts.
Poverty alleviation and reducing the need for young people to engage in transactional sex is an important goal in reducing HIV risk. While previous studies have demonstrated large impacts of the Kenya OVC-CT programme on household expenditures, we found no evidence that this improved economic well-being mediated the programme impact for this particular HIV risk-related indicator. However, the programme may still reduce HIV risk; it has previously been demonstrated that the programme reduced engagement in transactional sex (p < .10) among young women currently in school, but not among males or the larger sample of youth (Rosenberg et al., Citation2014).
An alternative pathway not fully explored here may include expectations for the future. For example, it is possible that cash transfer programmes may simultaneously affect current school attendance and expectations about schooling and future opportunities. Those expectations, and not the act of being in school currently, may be what drive lower rates of sexual debut, as increased expectations increase the opportunity cost of sex and childbearing. In fact, quasi-experimental studies from Kenya have found that increased schooling leads to delayed childbearing (Ferré, Citation2009; Ozier, Citation2011). Indeed, our Hope Scale measure, which we included as a mental health mediator, is more directly measuring agency than hope for the future. Further research should examine future expectations as a pathway for cash transfers impacting sexual behaviours.
One limitation of our analysis is that sexual behaviours are self-reported and may suffer from social desirability bias. However, we have no reason to believe reporting on this topic differed systematically between the treatment and control groups and thus was not likely to have impacted our findings. Relatedly, our interviews were face-to-face, which may inhibit accurate responses on sensitive topics such as sexual behaviour, but face-to-face interviews on sexual behaviour have been shown to be valid in an African setting (Kelly, Soler-Hampejsek, Mensch, & Hewett, Citation2013; Mensch, Hewett, Gregory, & Helleringer, Citation2008). Further, gender norms may create bias in different directions between males and females (Kelly et al., Citation2013), and in fact, studies among adolescents have shown that bias in sexual behaviour reporting is higher among males than females (Beguy, Kabiru, Nderu, & Ngware, Citation2009; Eggleston, Leitch, & Jackson, Citation2000; Kelly et al., Citation2013; Palen et al., Citation2008). To address these limitations to the best of our ability, as mentioned above, interviews were conducted in a private setting by enumerators of the same sex. A second limitation is the temporal ordering of the mental health mediator, which was measured during the same survey round as the outcome. It is therefore possible that mental health is a mediator but that our study design is not precise enough to identify this effect. On the other hand, if the CES-D captures longer term mental health, then our design would still pick up some potential mediation if it existed.
We have provided evidence that large-scale government run, unconditional cash transfers can positively impact sexual behaviours of young people in Africa, but the pathways remain unclear. Taken together with previously published findings, the evidence shows that the programme delays sexual debut and may reduce engagement in transactional sex among certain groups, but largely does not impact sex partner characteristics among Kenyan youth. More studies are needed from national programmes of this nature that operate at scale, and which build in research questions on HIV risk behaviours from the beginning to ensure that sample sizes are adequate and other potential mediation pathways are captured (such as expectations or aspirations).
Supplemental file
Download MS Word (35.4 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Tia Palermo http://orcid.org/0000-0003-0419-2049
Additional information
Funding
Notes
1. Including mediator variables which are themselves outcomes as right-hand-side variables may lead to endogeneity bias if there are other factors aside from the treatment which affect both the outcome variable and the mediator (Angrist & Pischke, Citation2009). However, methods to account for endogeneity such as instrumental variables would not allow us to test for mediation (i.e. whether controlling for the mediator attenuates the programme impact).
2. We formally tested for a gender difference in the schooling effect on sexual debut by pooling the samples and adding an interaction between the female dummy and the schooling indicator. This interaction is highly statistically significant with an estimated coefficient of −0.185.
References
- Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D. American Journal of Preventive Medicine, 10(2), 77–84.
- Angrist, J. D., & Pischke, J.-S. (2009). Mostly harmless econometrics: An empiricist's companion. Princeton: Princeton University Press.
- Ardington, C., & Case, A. (2009). Health: Analysis of the NIDS wave 1 dataset [Discussion Paper No. 2]. Cape Town: NIDS, University of Cape Town.
- Baird, S., Chirwa, E., McIntosh, C., & Ozler, B. (2010). The short-term impacts of a schooling conditional cash transfer program on the sexual behavior of young women. Health Economics, 19(Suppl), 55–68. doi: 10.1002/hec.1569
- Baird, S., De Hoop, J., & Özler, B. (2013). Income shocks and adolescent mental health. Journal of Human Resources, 48(2), 370–403. doi: 10.1353/jhr.2013.0014
- Baird, S. J., Garfein, R. S., McIntosh, C. T., & Ozler, B. (2012). Effect of a cash transfer programme for schooling on prevalence of HIV and herpes simplex type 2 in Malawi: A cluster randomised trial. The Lancet, 379(9823), 1320–1329. doi: 10.1016/S0140-6736(11)61709-1
- Barnett, T., Seeley, J., Levin, J., & Katongole, J. (2015). Hope: A new approach to understanding structural factors in HIV acquisition. Global Public Health, 10(4), 417–437. doi: 10.1080/17441692.2015.1007154
- Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. doi: 10.1037/0022-3514.51.6.1173
- Beegle, K., & Krutikova, S. (2007). Adult mortality and children's transition into marriage. World Bank Policy Research Working Paper (4139).
- Beguy, D., Kabiru, C. W., Nderu, E. N., & Ngware, M. W. (2009). Inconsistencies in self-reporting of sexual activity among young people in Nairobi, Kenya. Journal of Adolescent Health, 45(6), 595–601. doi: 10.1016/j.jadohealth.2009.03.014
- Behrman, J. R., & Hoddinott, J. (2005). Programme evaluation with unobserved heterogeneity and selective implementation: The Mexican progresa impact on child nutrition. Oxford Bulletin of Economics and Statistics, 67(4), 547–569. doi: 10.1111/j.1468-0084.2005.00131.x
- Birdthistle, I., Floyd, S., Nyagadza, A., Mudziwapasi, N., Gregson, S., & Glynn, J. R. (2009). Is education the link between orphanhood and HIV/HSV-2 risk among female adolescents in urban Zimbabwe? Social Science & Medicine, 68(10), 1810–1818. doi: 10.1016/j.socscimed.2009.02.035
- Bjorkman Nyqvist, M., Corno, L., De Walque, D., & Jakob, S. (2015). Using lotteries to incentivize safer sexual behavior: Evidence from a randomized controlled trial on HIV prevention. World Bank Policy Research Working Paper (7215).
- Boey, K. W. (1999). Cross-validation of a short form of the CES-D in Chinese elderly. International Journal of Geriatric Psychiatry, 14(8), 608–617. doi: 10.1002/(SICI)1099-1166(199908)14:8<608::AID-GPS991>3.0.CO;2-Z
- Bojorquez Chapela, I., & de Snyder, N. S. (2009). Psychometric characteristics of the center for epidemiological studies-depression scale (CES-D), 20- and 10-item versions, in women from a Mexican rural area. Salud Mental, 32(4), 299–307.
- Brown, L. K., Danovsky, M. B., Lourie, K. J., DiClemente, R. J., & Ponton, L. E. (1997). Adolescents with psychiatric disorders and the risk of HIV. Journal of the American Academy of Child & Adolescent Psychiatry, 36(11), 1609–1617.
- Cheung, Y. B., Liu, K. Y., & Yip, P. S. F. (2007). Performance of the CES-D and its short forms in screening suicidality and hopelessness in the community. Suicide and Life-Threatening Behavior, 37(1), 79–88. doi: 10.1521/suli.2007.37.1.79
- Cho, H., Hallfors, D. D., Mbai, I. I., Itindi, J., Milimo, B. W., Halpern, C. T., & Iritani, B. J. (2011). Keeping adolescent orphans in school to prevent human immunodeficiency virus infection: Evidence from a randomized controlled trial in Kenya. Journal of Adolescent Health, 48(5), 523–526. doi: 10.1016/j.jadohealth.2010.08.007
- Cluver, L., Boyes, M., Orkin, M., Pantelic, M., Molwena, T., & Sherr, L. (2013). Child-focused state cash transfers and adolescent risk of HIV infection in South Africa: A propensity-score-matched case–control study. The Lancet Global Health, 1(6), e362–e370. doi: 10.1016/S2214-109X(13)70115-3
- Cluver, L., & Gardner, F. (2007). Risk and protective factors for psychological well-being of children orphaned by AIDS in cape town: A qualitative study of children and caregivers’ perspectives. AIDS Care, 19(3), 318–325. doi: 10.1080/09540120600986578
- Covarrubias, K., Davis, B., & Winters, P. (2012). From protection to production: Productive impacts of the Malawi social cash transfer scheme. Journal of Development Effectiveness, 4(1), 50–77. doi: 10.1080/19439342.2011.641995
- Davis, B., Gaarder, M., Handa, S., & Yablonski, J. (2012). Evaluating the impact of cash transfer programmes in sub-Saharan Africa: An introduction to the special issue. Journal of Development Effectiveness, 4(1), 1–8. doi: 10.1080/19439342.2012.659024
- Deaton, A. (1997). The analysis of household surveys: A microeconometric approach to development policy. Washington, DC: World Bank Publications
- De Walque, D., Dow, W. H., Nathan, R., Abdul, R., Abilahi, F., Gong, E., … Krishnan, S. (2012). Incentivising safe sex: A randomised trial of conditional cash transfers for HIV and sexually transmitted infection prevention in rural Tanzania. BMJ Open, 2(1), 1–10. doi:10.1136/bmjopen-2011-000747
- Donenberg, G. R. (2005). Youths and HIV/AIDS: Psychiatry's role in a changing epidemic. Journal of the American Academy of Child & Adolescent Psychiatry, 44(8), 728–747. doi: 10.1097/01.chi.0000166381.68392.02
- Donenberg, G. R., Emerson, E., Bryant, F. B., Wilson, H., & Weber-Shifrin, E. (2001). Understanding AIDS-risk behavior among adolescents in psychiatric care: Links to psychopathology and peer relationships. Journal of the American Academy of Child & Adolescent Psychiatry, 40(6), 642–653. doi: 10.1097/00004583-200106000-00008
- Doyle, A. M., Mavedzenge, S. N., Plummer, M. L., & Ross, D. A. (2012). The sexual behaviour of adolescents in sub-Saharan Africa: Patterns and trends from national surveys. Tropical Medicine & International Health, 17(7), 796–807. doi: 10.1111/j.1365-3156.2012.03005.x
- Duflo, E., Dupas, P., & Kremer, M. (2014). Education, HIV, and early fertility: Experimental evidence from Kenya ( Working Paper No. w20784). National Bureau of Economic Research. Retrieved from http://www.nber.org/papers/w20784
- Duflo, E., Dupas, P., Kremer, M., & Sinei, S. (2006). Education and HIV/AIDS prevention: Evidence from a randomized evaluation in Western Kenya ( Working Paper No. 4024). World Bank. Retrieved from http:10.1596/1813-9450-4024.
- Eggleston, E., Leitch, J., & Jackson, J. (2000). Consistency of self-reports of sexual activity among young adolescents in Jamaica. International Family Planning Perspectives, 26(2), 79–83. doi: 10.2307/2648271
- Fernald, L. C. H., Gertler, P. J., & Neufeld, L. M. (2008). Role of cash in conditional cash transfer programmes for child health, growth, and development: An analysis of Mexico's Oportunidades. The Lancet, 371(9615), 828–837. doi: 10.1016/S0140-6736(08)60382-7
- Ferré, C. (2009). Age at first child does education delay fertility timing? The Case of Kenya, World Bank Policy Research (Working Paper No. 4833). Retrieved from http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1344718
- Flisher, A. J., Lund, C., Funk, M., Banda, M., Bhana, A., Doku, V., … Omar, M. (2007). Mental health policy development and implementation in four African countries. Journal of Health Psychology, 12(3), 505–516. doi: 10.1177/1359105307076237
- Gore, F. M., Bloem, P. J. N., Patton, G. C., Ferguson, J., Joseph, V., Coffey, C., … Mathers, C. D. (2011). Global burden of disease in young people aged 10–24 years: A systematic analysis. The Lancet, 377(9783), 2093–2102. doi: 10.1016/S0140-6736(11)60512-6
- Greif, M. J., Dodoo, F. N.-A., & Jayaraman, A. (2011). Urbanisation, poverty and sexual behaviour: The tale of five African cities. Urban Studies, 48(5), 947–957. doi: 10.1177/0042098010368575
- Hallfors, D., Cho, H., Rusakaniko, S., Iritani, B., Mapfumo, J., & Halpern, C. (2011). Supporting adolescent orphan girls to stay in school as HIV risk prevention: Evidence from a randomized controlled trial in Zimbabwe. American Journal of Public Health, 101(6), 1082–1088. doi: 10.2105/AJPH.2010.300042
- Handa, S., Halpern, C. T., Pettifor, A., & Thirumurthy, H. (2014). The government of Kenya's cash transfer program reduces the risk of sexual debut among young people age 15–25. PLoS One, 9(1), e85473. doi:10.1371/journal.pone.0085473
- Handa, S., Huang, C., Hypher, N., Teixeira, C., Soares, F. V., & Davis, B. (2012). Targeting effectiveness of social cash transfer programmes in three African countries. Journal of Development Effectiveness, 4(1), 78–108. doi: 10.1080/19439342.2011.641994
- Handa, S., Peterman, A., Huang, C., Halpern, C., Pettifor, A., & Thirumurthy, H. (2015). Impact of the Kenya cash transfer for orphans and vulnerable children on girls’ early pregnancy and marriage. Social Science and Medicine, 141, 36–45.
- Heinrich, C., Hoddinott, J., Samson, M., MacQuene, K., van Nikerk, I., & Renaud, B. (2012). The South African child support grant impact assessment. Pretoria: Department of Social Development, South African Social Security Agency, UNICEF.
- Heise, L., Lutz, B., Ranganathan, M., & Watts, C. (2013). Cash transfers for HIV prevention: Considering their potential. Journal of the International AIDS Society, 16(18615). Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752431/pdf/JIAS-16-18615.pdf
- Hoddinott, J., & Skoufias, E. (2004). The impact of Progresa on food consumption. Economic Development and Cultural Change, 53(1), 37–61. doi: 10.1086/423252
- Jukes, M., Simmons, S., & Bundy, D. (2008). Education and vulnerability: The role of schools in protecting young women and girls from HIV in southern Africa. AIDS, 22, S41–S56. doi: 10.1097/01.aids.0000341776.71253.04
- Kelly, C. A., Soler-Hampejsek, E., Mensch, B. S., & Hewett, P. C. (2013). Social desirability bias in sexual behavior reporting: Evidence from an interview mode experiment in rural Malawi. International Perspectives on Sexual and Reproductive Health, 39(1), 14–21. doi: 10.1363/3901413
- The Kenya CT-OVC Evaluation Team. (2012a). The impact of Kenya's cash transfer for orphans and vulnerable children on human capital. Journal of Development Effectiveness, 4(1), 38–49. doi: 10.1080/19439342.2011.653578
- The Kenya CT-OVC Evaluation Team. (2012b). The impact of the Kenya cash transfer program for orphans and vulnerable children on household spending. Journal of Development Effectiveness, 4(1), 9–37. doi: 10.1080/19439342.2011.653980
- Kilburn, K., Thirumurthy, H., Halpern, C. T., Pettifor, A., & Handa, S. (2014). Effects of a large-scale unconditional cash transfer program on mental health outcomes of young people in Kenya: A cluster randomized trial. Chapel Hill: University of North Carolina.
- Kohler, H.-P., & Thornton, R. L. (2012). Conditional cash transfers and HIV/AIDS prevention: Unconditionally promising? The World Bank Economic Review, 26(2), 165–190 doi: 10.1093/wber/lhr041
- Luke, N. (2003). Age and economic asymmetries in the sexual relationships of adolescent girls in sub-Saharan Africa. Studies in Family Planning, 34(2), 67–86. doi: 10.1111/j.1728-4465.2003.00067.x
- Lund, C., De Silva, M., Plagerson, S., Cooper, S., Chisholm, D., Das, J., … Patel, V. (2011). Poverty and mental disorders: Breaking the cycle in low-income and middle-income countries. The Lancet, 378(9801), 1502–1514. doi: 10.1016/S0140-6736(11)60754-X
- Madise, N., Zulu, E., & Ciera, J. (2007). Is poverty a driver for risky sexual behaviour? Evidence from national surveys of adolescents in four African countries: Original research article. African Journal of Reproductive Health, 11(3), 83–98. doi: 10.2307/25549733
- McQueston, K., Silverman, R., & Glassman, A. (2013). The efficacy of interventions to reduce adolescent childbearing in low- and middle-income countries: A systematic review. Studies in Family Planning, 44(4), 369–388. doi: 10.1111/j.1728-4465.2013.00365.x
- Medlin, C., & De Walque, D. (2008). Potential applications of conditional cash transfers for prevention of sexually transmitted infections and HIV in sub-Saharan Africa. World Bank Policy Research Working Paper Series.
- Mensch, B. S., Hewett, P. C., Gregory, R., & Helleringer, S. (2008). Sexual behavior and STI/HIV status among adolescents in rural Malawi: An evaluation of the effect of interview mode on reporting. Studies in Family Planning, 39(4), 321–334. doi: 10.1111/j.1728-4465.2008.00178.x
- Niño-Zarazúa, M., Barrientos, A., Hickey, S., & Hulme, D. (2012). Social protection in sub-Saharan Africa: Getting the politics right. World Development, 40(1), 163–176. doi: 10.1016/j.worlddev.2011.04.004
- Onuoha, F. N., Munakata, T., Serumaga-Zake, P. A. E., Nyonyintono, R. M., & Bogere, S. M. (2009). Negative mental health factors in children orphaned by AIDS: Natural mentoring as a palliative care. AIDS and Behavior, 13(5), 980–988. doi: 10.1007/s10461-008-9459-0
- Ozier, O. (2011). The impact of secondary schooling in Kenya: A regression discontinuity analysis. Berkeley. Retrieved from http://economics.ozier.com/owen/papers/ozier_JMP_20110117.pdf
- Palen, L.-A., Smith, E. A., Caldwell, L. L., Flisher, A. J., Wegner, L., & Vergnani, T. (2008). Inconsistent reports of sexual intercourse among South African high school students. Journal of Adolescent Health, 42(3), 221–227. doi: 10.1016/j.jadohealth.2007.08.024
- Palermo, T., & Peterman, A. (2009). Are female orphans at risk for early marriage, early sexual debut, and teen pregnancy? Evidence from sub-Saharan Africa. Studies in Family Planning, 40(2), 101–112. doi: 10.1111/j.1728-4465.2009.00193.x
- Patel, V., & Kleinman, A. (2003). Poverty and common mental disorders in developing countries. Bulletin of the World Health Organization, 81(8), 609–615.
- Paul Schultz, T. (2004). School subsidies for the poor: Evaluating the Mexican Progresa poverty program. Journal of Development Economics, 74(1), 199–250. doi: 10.1016/j.jdeveco.2003.12.009
- Paxson, C., & Schady, N. (2007). Cognitive development among young children in Ecuador the roles of wealth, health, and parenting. Journal of Human Resources, 42(1), 49–84. doi: 10.3368/jhr.XLII.1.49
- Pettifor, A., MacPhail, C., Nguyen, N., & Rosenberg, M. (2012). Can money prevent the spread of HIV? A review of cash payments for HIV prevention. AIDS and Behavior, 16(7), 1729–1738. doi: 10.1007/s10461-012-0240-z
- Radloff, L. S. (1977). The CES-D scale a self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. doi: 10.1177/014662167700100306
- Ravallion, M. (1998). Poverty lines in theory and practice. Washington, DC: World Bank Publications.
- Robinson, J., & Yeh, E. (2011). Transactional sex as a response to risk in Western Kenya. American Economic Journal: Applied Economics, 3(1), 35–64.
- Rosenberg, M., Pettifor, A., Thirumurthy, H., Halpern, C. T., & Handa, S. (2014). The impact of a national poverty reduction program on the characteristics of sex partners among Kenyan adolescents. AIDS and Behavior, 18(2), 311–316. doi: 10.1007/s10461-013-0487-z
- Senefeld, S., Strasser, S., Campbell, J., & Perrin, J. (2011). Measuring adolescent well-being: The development of a standardized measure for adolescents participating in orphans and vulnerable children programming. Vulnerable Children and Youth Studies, 6(4), 346–359. doi: 10.1080/17450128.2011.635722
- Snyder, C., Richard, B. H., Pelham, W. E., Rapoff, M., Ware, L., Danovsky, M., … Stahl, K. J. (1997). The development and validation of the children's hope scale. Journal of Pediatric Psychology, 22(3), 399–421. doi: 10.1093/jpepsy/22.3.399
- The Transfer Project. (2015). Measuring health and well-being of young people in the transfer project (research brief). Chapel Hill, NC: Carolina Population Center.
- UNAIDS. (2012). Fact sheet: Adolescents, young people and HIV. Author.
- Wamoyi, J., Mshana, G., Mongi, A., Neke, N., Kapiga, S., & Changalucha, J. (2014). A review of interventions addressing structural drivers of adolescents’ sexual and reproductive health vulnerability in sub-Saharan Africa: Implications for sexual health programming. Reproductive Health, 11(1), Article no. 88. doi: 10.1186/1742-4755-11-88
- World Bank. (2009). Conditional cash transfers: Reducing present and future poverty. Washington, DC: Author.
- World Health Organization. (2014). Health for the world's adolescents: A second chance in the second decade. Geneva: WHO.
- Zuilkowski, S. S., & Jukes, M. C. H. (2012). The impact of education on sexual behavior in sub-Saharan Africa: A review of the evidence. AIDS Care, 24(5), 562–576. doi: 10.1080/09540121.2011.630351