
ABSTRACT
Delivering specialised care for major burns requires a multidisciplinary health workforce. While health systems ‘hardware’ issues, such as shortages of the healthcare workforce and training gaps in burn care are widely acknowledged, there is limited evidence around the systems ‘software’ aspects, such as interest, power dynamics, and relationships that impact the healthcare workforce performance. This study explored challenges faced by the health workforce in burn care to identify issues affecting their performance. Qualitative in-depth interviews were conducted with a purposively selected sample (n = 31, 18 women and 13 men) of various cadres of the burn care health workforce in Uttar Pradesh, India. Inductive coding and thematic analysis identified three major themes. First, the dynamics within the multidisciplinary team where complex relations, power and normative hierarchy hampered performance. Second, the dynamics between health workers and patients due to the clinical and emotional challenges of dealing with burn injuries and multitasking. Third, dynamics between specialised burn units and broader health systems are narrated in challenges due to inadequate first response and delayed referral from primary care facilities. These findings indicate that burn care health workers in India face multiple challenges that need systemic intervention with a multipronged human resource for health framework.
Introduction
Burn injury is a major public health problem with high mortality, morbidity and significant socio-economic implications for survivors (Jeschke et al., Citation2020). In India, burns is a major challenge with a high burden of incidence, mortality, and disability. Minor burn injuries can be treated across primary, secondary, and tertiary care health facilities, depending on severity and complications. However, major burn injuries require treatment in a specialised burn care unit for better recovery outcomes. A team of multidisciplinary health workers is needed for comprehensive services in any specialised burn unit (Kruk et al., Citation2010). Health facilities at secondary and primary care levels should be equipped with level-appropriate infrastructure and a trained health workforce for proper response (Atiyeh et al., Citation2009; Calland et al., Citation2014; Grimes et al., Citation2011). Globally, the availability of a skilled multidisciplinary health workforce in the burn unit is recognised as a critical bottleneck for the delivery of comprehensive burn care (Botman et al., Citation2021; Cochran & Greenhalgh, Citation2018); similar challenges have been recognised in India (Chamania, Citation2018; Singh, Citation2018).
In India, the National Programme for Prevention and Management of Burn Injury (NPPPMBI) is one of the important policy responses to address the burden of burns on mortality, morbidity, and disability (Gupta et al., Citation2010). The programme was started as a pilot project in 2010 which was later scaled up across India in 2014. The NPPMBI aimed to strengthen burn care centres, improve burn care training and capacity building, promote burn prevention, and implement a burn registry system in India (Gupta et al., Citation2010; NPPMTBI, Citation2020). However, despite the implementation of the NPPMBI, the network of specialised burn units is limited in both the public and private sectors (Ranganathan et al., Citation2020). The health workforce shortage and capacity in burn care in India remain a concern (Singh, Citation2018; Jagnoor, Bekker et al., Citation2018). Similarly, there is recognition of a training gap in burns care at the primary care level and among front-line health workers (FLW) working in the community, such as Auxiliary Nurse Midwives (ANM) and Accredited Social Health Activists (ASHA) (Chamania, Citation2010). More importantly, the health worker’s capacity, interest, and team dynamic in the multidisciplinary team are not well understood (Jagnoor, Bekker et al., Citation2018; Singh, Citation2018).
Health systems are composed of both; ‘hardware’, such as infrastructure, human resources, service delivery, financing, governance, medical products, information systems, and ‘software’, such as ideas and interests, values and norms, power, and relationships in health systems are equally important (Sheikh et al., Citation2011; WHO, Citation2007). Though the role of ‘hardware’ in health systems is extensively studied, the exploration of ‘software’ issues has been limited. Addressing these ‘software’ issues is essential to holistically strengthen health systems (Ramani et al., Citation2022) and develop robust health policies (Karim et al., Citation2022; Witter et al., Citation2022) across diverse settings and contexts. In the burns care system, multiple hardware issues such as inadequate infrastructure, shortage of health workforces and training gaps have been documented across different contexts (Chamania, Citation2010; Citation2018; Jagnoor, Lukaszyk et al., Citation2018). There is limited evidence on software issues, such as the emotional challenges of working in the burn unit, the need for collaboration and teamwork, and the lack of interest of surgical resident doctors in burns, mostly coming from studies conducted in high-income countries (HICs) context (Boeira Fuculo Junior et al., Citation2021; Kornhaber & Wilson, Citation2011; Win et al., Citation2018). However, elaborative evidence on systems software issues affecting health workers in burn care in low and middle-income countries (LMICs) remains limited.
In this study, we aim to explore the health workforce challenges for burn care in Uttar Pradesh, India, and identify systems software and hardware issues affecting health workers’ performance.
Materials and methods
We carried out an exploratory qualitative study using a thematic analysis approach based on in-depth interviews (IDI) with the health workforce engaged in burn care in Uttar Pradesh, India.
Settings
The health system in India is complex and there is lack of clarity on the structure of burn care delivery system. However, in the NPPMBI, burn care systems were categorised into a three-tier structure (DteGHS, Citation2010; Gupta et al., Citation2010). At the tertiary level, a burn unit in a tertiary care hospital with specialised burn beds, an intensive care unit, and a multidisciplinary team. At the secondary level, dedicated burn beds at public district hospitals. At the primary care level, minor burn treatment, triage, and referral for major burns (DteGHS, Citation2010).
Uttar Pradesh is the most populous state in India, with constrained health systems, and a limited network of burn units (NITI Aayog, Citation2021; Ranganathan et al., Citation2020). This study was conducted in two of the largest burn units embedded within the plastic surgery departments of tertiary care teaching institutes and an affiliated primary health centre (PHC). Both burn units provide comprehensive burn care and have a multidisciplinary health workforce team. These centres are also residency training centres for plastic surgery.
Sampling frame
We enlisted all health workers in burn units, such as plastic surgeons, anaesthetists, surgical resident trainees, junior resident doctors, physiotherapists, psychiatrists, nurses, dressersFootnote1, and intensive care unit (ICU) technicians.Footnote2 This formed our sampling universe, the respondents were then purposively selected from this list to ensure a diverse representation of health workers, gender, and experience level. At the PHC, we included health personnel with direct contact with patients including medical officers and FLWs, such as ANMs and their supervisors, ASHAs and their supervisors. ANMs provide services at one of the sub-centres within the PHC. ASHAs serve a village of 1000 population and function as a link between health facilities and the community. The sample size was guided by thematic saturation, we noted thematic saturation after 18–19 interviews at the burn unit. However, we interviewed a few more respondents to ascertain the pattern. At the PHC, thematic saturation was observed after 4–5 interviews, but we interviewed more health workers to ensure reliability. We did not use any specific inclusion or exclusion criteria for the selection of respondents.
Data collection and ethics
We used an interview guide to conduct IDIs. The guide included questions on basic demographic details, experience in burn care, patient care, and potential solutions to identified challenges (Supplementary File 1). The IDI guide was pilot tested with team members and burn care providers, following which a few questions were modified and added as relevant to respondents. Two interviewers (the first and second author) interviewed the respondents. The first interviewer is a male medical doctor with a specialisation in public health and currently researching health systems response to burns in India. The second interviewer is a female public health specialist. Both interviewers are trained in qualitative research and have performed IDIs in similar settings.
Interviews were conducted between November 2021 and February 2022, either in-person (face to face) or by telephone depending on the restrictions imposed by COVID-19. For in-person interviews, interviewers independently approached respondents to set a mutually agreed time for the interview. Respondents were then requested to read the Participant Information Sheet (PIS) and provide written consent. A surge in COVID-19 cases in India in January 2022 restricted in-person interviews. For telephone interviews, respondents were approached via email/messages to seek a suitable time for an interview call, after which the PIS and consent sheet were shared with a request to return the signed consent form before starting the interview. Interviews were done in the respondents’ preferred language; however, the most commonly preferred language was English or Hindi. Some respondents used both English and Hindi. The sample size was guided by thematic saturation collecting data until we no longer obtained new themes in response (Guest et al., Citation2020). We noted thematic saturation after 17–18 interviews at the burns units but conducted a few more to validate the pattern. In total, 22 health workers were interviewed at the burn units, and an additional nine participants were interviewed at the PHC. 25 interviews were conducted in person, while 6 were conducted telephonically. The average duration of interviews was 34 minutes, with a range of 22–59 minutes. After obtaining consent, in-person interviews were recorded using a recorder, while telephonic interviews were recorded by recording the telephonic call. Interviews were recorded to capture the full verbatim response. One participant did not consent to recording, so extensive field notes were taken. Interviewers held regular post-interview discussions to reflect on the process and responses.
Analysis
The interviewers listened to the recordings and read field notes to familiarise themselves with the data. The interviewers then discussed the interview process and data with the senior author. After that, certified professionals simultaneously transcribed and translated interview recordings in Hindi and mixed languages into English. A research assistant did a verbatim transcription of interviews in English. Transcripts and translations were later checked for accuracy by the interviewers. Once transcripts were checked, the interview recording was scrapped.
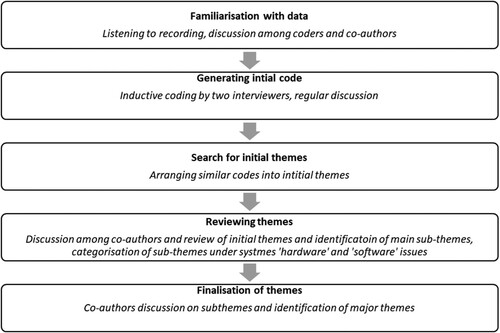
We used an inductive approach for initial coding in NVivo ver.12 software (NVivo, Citation2020). The two interviewers did the initial coding. Regular discussions were held to ensure uniformity in the process. The codebook is given as supplementary file 2. A thematic analysis approach was used for identifying themes. We grouped similar codes to generate broad themes. The identified systems issues within each theme were then categorised into ‘hardware’ and ‘software’ issues. We noted a gender differential in the response and explored the same in our analysis. The schematic flow of the process of thematic analysis is depicted in .
Figure 1. Schematic representation of the process of developing subthemes and major themes.
Rigour and trustworthiness
We used multiple strategies to ensure the rigour and trustworthiness of the analysis. Firstly, we used purposive sampling to include all cadres of health workers to gather the perspective of the multidisciplinary team. Secondly, the sample size was guided by thematic saturation. Thirdly, two co-authors separately coded the data and held regular discussions to ensure homogeneity and consistency. Other co-authors, including those actively working in burn care reviewed the codes, sub-theme, and analysis. Fourthly, we used verbatim quotes from the interview transcript to support our observations. The study complies with COREQ guidelines for reporting qualitative research (Supplementary file 3).
Results
A total of 31 IDIs were done with health workers (18 women and 13 men). Among the female health workers, were two medical faculty members, four resident doctors, four nurses and eight FLWs, including ANMs and ASHAs, and their supervisors. Male health workers included two medical faculty members, two resident doctors, one medical officer, two nurses, two physiotherapists, one ICU technician, two dressers, and one multi-purpose worker. Participants were between 23 to 54 years of age. Participants working in burn units had a mean work experience of 8.3 years, ranging from one to 29 years. Their mean experience in burn care was 5.9 years, with a range of one to 20 years. Participants from primary care settings had an average work experience ranging from 3 to 16 years, with a mean of 10.4 years ().
Table 1. Study participants: healthcare workers in burn units and primary health centre.
We identified three major themes representing complex health workforce issues in burn care: dynamics within the multidisciplinary burn teams, dynamics between health workers and patients, and dynamics between health facilities (burn units and health systems). In addition, systems ‘hardware’ or ‘software’ issues were identified within each theme. Themes and related issues are presented in .
Table 2. Themes and sub-themes.
Dynamics within multidisciplinary burn teams
Participants highlighted the importance of the multidisciplinary team and teamwork for optimal functioning of the burn unit and recovery outcomes. However, multiple software issues, such as complex relationships, power, and hierarchy within teams were also highlighted. Across cadres, participants saw the doctor-in-charge as the apparent leader on the day and senior doctors as overall leaders of the burn team. However, doctors had divergent views about their ownership and agency of burn care. Senior plastic surgeons considered burn care as their responsibility, while resident trainees viewed it as an added responsibility. Nurses were recognised as key team members, but they lacked clarity about their roles. Senior nurses were generally clear and content with their roles, while those new to systems struggled to clearly understand their roles and responsibilities. Other cadres of health workers also had a dilemma regarding their role in burn care. The absence of a written job description contributed to confusion among different categories of health workers. The lack of role clarity also promoted normative hierarchy and centralisation of power to doctors, given their advanced clinical training. Participants narrated the importance of teamwork, mutual respect, appreciation, and team cohesion for effective patient care and as one of the critical determinants of team performance. There was, however, little involvement of the non-doctor health workers in the clinical and systems improvement process.
If the government or the hospital administration provides some set of protocols or guidelines …… hellip; then I would have clarity about my scope of practicing (R4 – Nurse)
I feel so hectic (exerted) in this (burn) ward for the last six months, so I asked my ward in-charge to switch me to another ward, (R-4, Nurse).
Here, burn care has a major component. I am from different part of the country; we don't see these many burn patients in those parts of the country (R 19 – plastic surgery resident).
Dynamics between health workers and patients
Participants highlighted how existing system hardware issues constrained patient care in the burn unit, thus affecting care provider’s work satisfaction. Shortage of staff across cadres often requires them to multi-task and do task shifting. Health workers in burn units engage in counselling and often guide the rehabilitation process. Managing emotions and communicating with patients and caregivers require soft skills training. Other challenges identified by participants were communicating with anxious family members and relatives, ensuring wound hygiene, and managing patients with severely debilitated major burns in the burn unit. The diversity of patients who sustained different types of burns and complications makes the burn unit a difficult place to work. For health workers posted in the burn unit for the first time, the early days of burn posting are trying, as they struggle to cope with the psychological and emotional challenges of managing complicated burn patients. Noting existing gaps in pre-service training for burn care, respondents across health worker categories expressed the need for specialised burn training before posting in the burn unit and continuous ‘on-the-job’ training.
Like a kind of continuous review going on, new people learning things by observation, and the experienced ones are getting a refresher or recapitulation (R 14, Multi-purpose worker).
Table 3. Themes and supporting quotes.
Some patients really bring tears to my eyes when they narrate their ordeals (R 17).
Dynamics between health facilities (burn units and health systems)
Health workers at burn units frequently highlighted the hardware problems of incoordination between health facilities at different levels of care and challenges due to inadequate first response and delayed referral. They also spoke about patient complications due to improper initial care and delayed referral which often prove detrimental to recovery. There was a call for training of health workers at primary and secondary level health facilities covering triage, initial care, and timely referral.
Here, we don’t have so much facility, we try to see the patient in the ambulance itself and refer. (C9, PHC medical officer).
Till now I have not come across any people with burns. If I get such a report, immediately we will call 102 ambulances (C 1, ASHA facilitators).
Gendered pattern in healthcare workers’ responses
Our primary objective did not include gender perspectives, and we did not include any specific prompts for gender-based responses in the interview guide. However, during the interviews and analysis, we noted many distinct responses based on the respondent’s gender. Hence, we have described them in Box 1.
Box 1. Gendered pattern in healthcare workers’ responses
Interviewers noted a pattern in interviewees’ responses based on gender. The two interviewers discussed and reflected on this during post-interview discussions. A detailed discussion with the senior investigator provided neutral affirmation of the interviewers’ reflections. All three investigators agreed there was a distinct gendered pattern in responses. This pattern was also noted during coding and analysis. We found that male respondents were more forthcoming in sharing the challenges in burns care and their rights, roles, and responsibilities. They were more forthcoming in explaining the challenges and more expressive in suggesting solutions and reforms for the existing issues. Female respondents, on the other hand, expressed more satisfaction with their jobs than men. The selected quotes from two nurses, almost similar in age and experience but different genders, illustrate the gender patterns in response.
All our madams and sirs, our respected consultants, and all our JRs (Junior Resident Doctors), and SRs (Senior Resident Doctors) who are with us, we have first-hand communication with them. Like, the interaction that we have with them is first-hand/first level interaction. They say everything to us directly regarding patients, and we follow that.
R8, Female Nurse
Hierarchy is there; we have to go through that. There are problems because of that. I think that these things must change. Maybe the head or whoever is there, can get to know about the things directly from us. I am not saying that they have to work on our orders; they can look at things in their aspects and work accordingly.
R9, Male Nurse
Discussion
Our research attempted to decipher the conundrum of health workforce issues in burn care in India. The importance of a multidisciplinary team and training challenges for burns care in India have been documented (Chamania, Citation2010; Jagnoor, Bekker et al., Citation2018). However, to our knowledge, this is the first attempt at a deeper understanding of the health workforce concerns and health system software issues for burn care in India. We also identified a few health systems ‘hardware’ issues, such as shortage, training concerns, lack of clarity of job responsibilities and several software issues, such as power dynamics, hierarchical relationships, unclear roles and responsibilities, poor job satisfaction, and lack of motivation. Plastic surgery trainees face a dilemma in burn care due to the training-career aspiration gap. Clinical complexity and emotional challenges of dealing with burns require soft skills training, which include critical thinking, social aptitudes, communication capability, and teamwork abilities. An affirmative policy is also needed for the psychological safety of health workers in burn units. The PHC workers and FLWs lack orientation and training on burns but see their role in minor burns, triage, referral, and community-based rehabilitation. Hardware issues such as training gaps and sub-optimally aligned burn training packages are also critical.
The absence of written human resource policies, job descriptions and standard operating procedures caused confusion, supported power asymmetry towards medical doctors and ensured normative hierarchy among health workforces. These factors also prevent team approaches and collective decision-making, thus, influencing satisfaction and motivation. Existing evidence highlights the importance of team coherence and an integrated approach for effective burns response (Boeira Fuculo Junior et al., Citation2021; Jagnoor, Bekker et al., Citation2018; Kornhaber et al., Citation2019; Win et al., Citation2018). There was a clear recognition of the training gaps and the need for rigorous capacity building. The current pre-service training needs revision to impart essential skills required for burns care. There is also a recognised need for structured induction training and on-the-job capacity building. The need for an appropriate training package for burns, especially in LMIC settings, has been previously documented (Chamania, Citation2010; Jagnoor, Lukaszyk et al., Citation2018; Potokar et al., Citation2010). Our findings suggest revisiting the burn care training design for burns in India.
Plastic surgeons have pioneered burn care and are recognised leaders. However, burn care is not ‘mandatory’ in plastic surgery residency training. The trainee residents see burn care as an added responsibility and interference with career aspirations. These findings necessitate deeper deliberation on curriculum, training, and ownership of burn care. Burnout among plastic surgery residents in India is previously documented (Panse et al., Citation2020); however, there is no evidence of trainees’ concerns and interest in burns. Findings from the HIC context indicate diverging interest in burns among plastic surgery residents (Brown & Mills, Citation2004; Sreedharan et al., Citation2021; Vrouwe et al., Citation2020). Limited exposure to burns during residency, the nature of burns surgery, inadequate opportunities, and more lucrative alternative career opportunities influenced their interest in burns in HICs (Brown & Mills, Citation2004; Sreedharan et al., Citation2021; Vrouwe et al., Citation2020). Our findings specify the need to re-examine the intensity of burns training for plastic surgery. Policy action must be taken to expand burn care practice opportunities in the public and private sectors.
Clinical and patient care in burns requires dedication, perseverance, and emotional resilience. Healthcare workers in burn care often require communicating sympathetically and effectively with patients and caregivers. Thus, soft skills training for better communication, improving patient compliance and motivation are needed. continuous psychological support. Findings from the HIC context also highlight the need to manage emotional challenges and build resilience among burn unit health workers (Kornhaber & Wilson, Citation2011). Existing evidence also suggests the importance of soft skills training in nursing and medical education (Ng, Citation2020; Steinmair et al., Citation2022). Considering the high patient load, and limited human resources in burn units in India, strategies for emotional resilience and psychological support must get policy priority.
Currently, the health workers at the primary care level have limited involvement in burn care. However, they see a role in minor burn management, facilitating referral, burn prevention, and community-based rehabilitation if they receive training and additional financial incentives. Health workers in burn units also emphasised training peripheral health workers for improved initial response and continuum of post-discharge care. Empirical evidence shows significant improvement in burns care after level-appropriate facility preparedness (Potokar et al., Citation2020). Existing guidelines in India also mandate a comprehensive primary care approach for burn care (NHSRC, Citation2020). Our findings indicate an implementation gap that should be appropriately addressed.
Globally, women are the majority (67%) of the health workforce (Mathieu Boniol et al., Citation2019). However, inequality persists in the form of occupational segregation, pay parity, nature of employment and working conditions (Morgan et al., Citation2018). Gender inequality and norms in health systems also reflect the power and hierarchy of the overall social system (Hay et al., Citation2019). Existing evidence also suggests that women health workers have lower career-growth opportunities than their male counterparts (Kinshella et al., Citation2022; Morgan et al., Citation2018). We identified similar gender patterns in the perceived role, satisfaction, and motivation, even within the health workforce in the same cadres. However, this was not the primary objective, so we suggest more research on health workers’ gender issues.
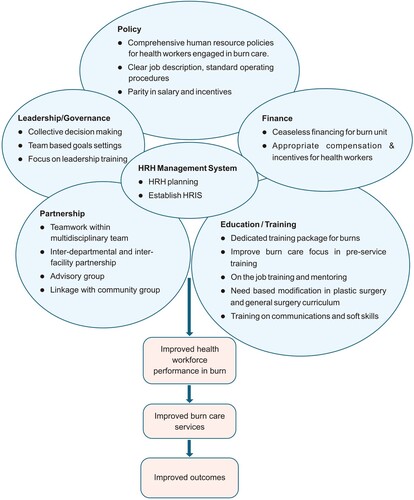
Health workers also shared insightful solutions to some of the identified challenges. We used the Human Resources for Health (HRH) action framework to organise and propose solutions. The HRH action framework was developed by the United States Agency for International Development and endorsed by the World Health Organization for sustainable HRH planning and implementation (Human Resource for Health framework, Citation2005). We used this framework to propose solutions for health workforce challenges in burns care (). In summary, these cover six domains:
Policy: There should be a comprehensive human resource policy, including clear roles and responsibilities, salaries and incentives, approaches for motivation, and proposed career progression for all cadres of health workers in the burn unit. Accreditation of burn units by an accrediting agency can support uniformity in the quality of care across burn units.
Leadership and Governance: Multidisciplinary burn care teams require collective decision-making and effective leadership. Leadership and management training for burn unit leaders should be considered. Burn unit leaders should focus on team-based goals to encourage teamwork and improve team performance.
Partnerships: Partnerships and collaboration are essential for health workers in burns. Such partnerships are required at multiple levels: between individuals within the unit, between departments within a hospital and between various health facilities. An efficient way to institute partnerships can involve forming an advisory group of all cadres of health workers, multiple departments, and burn survivors. Inter-facility partnerships can boost referral linkages, and a partnership with community health workers and leaders can improve follow-up care.
Education and training: Training for burn care needs urgent attention and must be strengthened at multiple points. Increased focus on burns care in pre-service training, provision of comprehensive induction training before posting in the burn unit, and continuous on-the-job mentoring should be prioritized. There is a need to develop a holistic burn care syllabus for plastic surgery residency. Primary health care workers and FLWs must be trained in burn first aid, triage, and referral. In addition, training in communications and soft skills should be imparted.
Financing: The policy should prioritise supplies and adequate financial risk protection for patients for the health workers to function optimally. In addition, efforts should be aimed at bringing parity in incentive structures among the same cadre of health workers. Performance-based financial incentives for burn care should be introduced to motivate health workers.
Human resource management systems: Human resource management systems should be harnessed for rationale use of limited health workers.
Figure 2. Human Resource for Health (HRH) action framework for health workforce in burns.
There are a few limitations of the study. First, the study was only conducted in two tertiary care burn units in Uttar Pradesh state of India and catchment PHC. So, the findings may vary in different health systems contexts. However, our objectives were more exploratory than representative, and we included multiple cadres of health workers to get a holistic viewpoint. Second, we interviewed health workers in burn units embedded within plastic surgery departments, not in smaller burn units located in general surgery departments, where other hardware issues such as limited infrastructure and shortage of health workers may exist. However, we prioritised bigger burn units to cover multiple cadres of health workers. Third, we noted a diverse nature of issues for various cadres of health workers, such as medical residents, nursing, and rehabilitation practitioners, which require separate further exploration.
Final considerations
We identified multiple challenges for health workers involved in burns care in India. These challenges are not restricted to frequently identified ‘hardware’ issues, such as workforce shortages, training gaps and clinical complications. Rather, multiple ‘software’ issues such as team dynamics, power, hierarchy, emotional challenges, and training – career aspiration gaps exist, which influence performance and satisfaction. The PHC workers and FLWs are not well aligned with the overall burn care. Our findings indicate that urgent policy action is needed to address health workforce issues for burns. There is a need for comprehensive HR policies with clearly articulated position descriptions and a well-designed incentive structure. Burn care training for all cadres should be redesigned with induction training and on-the-job mentoring for continuous capacity building. Plastic surgery training should be balanced with burns components to ensure interest, training, and career aspirations. PHC workers and FLWs should be trained, and incentives for optimising their services in burns care provided. Future research on burns must endeavour to explore these issues elsewhere in India, in other low-resource settings and globally.
Authors’ contributions
VRK conceptualised the study with inputs from JJ and SA. VRK and SP collected data and conducted coding. VRK did the analysis; JJ and SA provided critical input to the analysis. BM and MFK supported data collection and provided input in the analysis and interpretation of data. VRK drafted the manuscript. JJ, SA, MP, and RN provided critical inputs to the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent
The study protocol was approved by the George Institute Ethics Committee, The George Institute for Global Health, New Delhi, India (Ref. no. 13/2019) and ratified by the Human Research Ethics Committee of the University of New South Wales, Sydney, Australia. Written informed consent was obtained from all study participants. The study complies with the ‘National Ethical Guidelines for Biomedical and Health Research Involving Human Participants’ by the Indian Council of Medical Research, India.
Consent for publication
Written informed consent was obtained from all participants included in the study.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Supplemental Material
Download Zip (112.3 KB)Acknowledgements
We thank Dr. Shamim and Dr. Jamal Masood for facilitating the interviews with health workers at the burn unit and primary health centre. We also thank Ms. Pratishtha Singh and the TRID India team for their transcription support.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 A Dresser’s (Medical) main job is to perform dressing of patients and its related activities as instructed by healthcare professional. The person also maintains the set-up under supervision. (National Qualification Register, India).
2 Intensive care unit technicians are health care workers who ensure the safe and effective use of technological systems used in the care of critically ill patients.
References
- Atiyeh, B., Masellis, A., & Conte, C. (2009). Optimizing burn treatment in developing Low-and middle-income countries with limited health care resources (part 2). Annals of Burns and Fire Disasters, 22(4), 189–195. https://pubmed.ncbi.nlm.nih.gov/21991180
- Boeira Fuculo Junior, P. R., Rutz Porto, A., Echevarría-Guanilo, M. E., Mayer, B. L., Sartini Coimbra, R., & Martins, T. (2021). Difficulties experienced by multiprofessional health teams in providing primary care for burn victims. Revista Enfermagem UERJ, 29, 1–7. https://search.ebscohost.com/login.aspx?direct=true&db=cin20&AN=155169646&site=ehost-live
- Botman, M., Hendriks, T. C. C., de Haas, L., Mtui, G., Binnerts, J., Nuwass, E., Niemeijer, A. S., Jaspers, M. E. H., Winters, H. A. H., Nieuwenhuis, M. K., & van Zuijlen, P. P. M. (2021). Access to burn care in low- and middle-income countries: An assessment of timeliness, surgical capacity, and affordability in a regional referral hospital in Tanzania. Journal of Burn Care & Research, 43(3), 657–664. https://doi.org/10.1093/jbcr/irab191
- Brown, T. L. H., & Mills, S. (2004). Where are all the burn surgeons?: A survey of plastic surgical trainees in Australasia. Burns, 30(6), 577–580. https://doi.org/10.1016/j.burns.2004.04.003
- Calland, J. F., Holland, M. C., Mwizerwa, O., Petroze, R. T., Ntakiyiruta, G., Patel, K., Gampper, T. J., Byiringiro, J. C., Campbell, C. A., & Calland, J. F. (2014). Burn management in sub-Saharan Africa: Opportunities for implementation of dedicated training and development of specialty centers. Burns, 40(1), 157–163. https://doi.org/10.1016/j.burns.2013.05.015
- Chamania, S. (2010). Training and burn care in rural India. Indian Journal of Plastic Surgery, 43(Suppl), 126–130. https://doi.org/10.4103/0970-0358.70735
- Chamania, S. (2018, August/September). Burns care in India: Unique and continuing challenges [Interview]. THE PMFA JOURNAL.
- Cochran, A., & Greenhalgh, D. G. (2018). Building the burn physician workforce for the 21st century: Report from February 2014 burns workforce conference. Journal of Burn Care & Research, 39(6), 853–857. https://doi.org/10.1093/jbcr/iry020
- Directorate General of Health Services (DteGHS). (2010). Ministry of Health and Family Welfare, Government of India. Operational guideline for establishment of burn units at medical colleges under national programme for prevention and management burn injury. https://dghs.gov.in/WriteReadData/userfiles/file/Operational_Guidlines_Medical_College.pdf
- Grimes, C. E., Bowman, K. G., Dodgion, C. M., & Lavy, C. B. D. (2011). Systematic review of barriers to surgical care in Low-income and middle-income countries. World Journal of Surgery, 35(5), 941–950. https://doi.org/10.1007/s00268-011-1010-1
- Guest, G., Namey, E., & Chen, M. (2020). A simple method to assess and report thematic saturation in qualitative research. PLoS One, 15(5), e0232076. https://doi.org/10.1371/journal.pone.0232076
- Gupta, J. L., Makhija, L. K., & Bajaj, S. P. (2010). National programme for prevention of burn injuries. Indian Journal of Plastic Surgery, 43(S 01), S6–S10. https://doi.org/10.1055/s-0039-1699455
- Hay, K., McDougal, L., Percival, V., Henry, S., Klugman, J., Wurie, H., Raven, J., Shabalala, F., Fielding-Miller, R., Dey, A., Dehingia, N., Morgan, R., Atmavilas, Y., Saggurti, N., Yore, J., Blokhina, E., Huque, R., Barasa, E., Bhan, N., … Rao Gupta, G. (2019). Disrupting gender norms in health systems: Making the case for change. The Lancet, 393(10190), 2535–2549. https://doi.org/10.1016/S0140-6736(19)30648-8
- Human Resource for Health framework. (2005). https://www.capacityproject.org/framework
- Jagnoor, J., Bekker, S., Chamania, S., Potokar, T., & Ivers, R. (2018). Identifying priority policy issues and health system research questions associated with recovery outcomes for burns survivors in India: A qualitative inquiry. BMJ Open, 8(3), e020045. https://doi.org/10.1136/bmjopen-2017-020045
- Jagnoor, J., Lukaszyk, C., Christou, A., Potokar, T., Chamania, S., & Ivers, R. (2018). Where to from here? A quality improvement project investigating burns treatment and rehabilitation practices in India. BMC Research Notes, 11(1), 224. https://doi.org/10.1186/s13104-018-3314-9
- Jeschke, M. G., van Baar, M. E., Choudhry, M. A., Chung, K. K., Gibran, N. S., & Logsetty, S. (2020). Burn injury. Nature Reviews Disease Primers, 6(1), 11. https://doi.org/10.1038/s41572-020-0145-5
- Karim, A., de Savigny, D., Awor, P., Cobos Muñoz, D., Mäusezahl, D., Kitoto Tshefu, A., Ngaima, J. S., Enebeli, U., Isiguzo, C., Nsona, H., Ogbonnaya, I., Ngoy, P., & Alegbeleye, A. (2022). The building blocks of community health systems: A systems framework for the design, implementation and evaluation of iCCM programs and community-based interventions. BMJ Global Health, 7(6), e008493. https://doi.org/10.1136/bmjgh-2022-008493
- Kinshella, M. W., Boene, H., Sevene, E., Valá, A., Sharma, S., Vidler, M., Magee, L. A., von Dadelszen, P., Munguambe, K., & Payne, B. A. (2022). How gender influenced the experience of using a mHealth intervention in rural Mozambique: Secondary qualitative analysis of community health worker survey data. Frontiers in Global Women's Health, 3, 661000. https://doi.org/10.3389/fgwh.2022.661000
- Kornhaber, R., Rickard, G., McLean, L., Wiechula, R., Lopez, V., & Cleary, M. (2019). Burn care and rehabilitation in Australia: Health professionals’ perspectives. Disability and Rehabilitation, 41(6), 714–719. https://search.ebscohost.com/login.aspx?direct=true&db=cin20&AN=135461705&site=ehost-live.
- Kornhaber, R. A., & Wilson, A. (2011). Building resilience in burns nurses: A descriptive phenomenological inquiry. Journal of Burn Care & Research, 32(4), 481–488. https://doi.org/10.1097/BCR.0b013e3182223c89
- Kruk, M. E., Wladis, A., Mbembati, N., Ndao-Brumblay, S. K., Hsia, R. Y., Galukande, M., Luboga, S., Matovu, A., de Miranda, H., Ozgediz, D., Quiñones, A. R., Rockers, P. C., von Schreeb, J., Vaz, F., Debas, H. T., & Macfarlane, S. B. (2010). Human resource and funding constraints for essential surgery in district hospitals in Africa: A retrospective cross-sectional survey. PLoS Medicine, 7(3), e1000242. https://doi.org/10.1371/journal.pmed.1000242
- Mathieu Boniol, M. M., Xu, L., Wuliji, T., Diallo, K., & Campbell, J. (2019). Gender equity in the health workforce: Analysis of 104 countries (Health Workforce Working paper 1, Issue. https://apps.who.int/iris/bitstream/handle/10665/311314/WHO-HIS-HWF-Gender-WP1-2019.1-eng.pdf
- Morgan, R., Ayiasi, R. M., Barman, D., Buzuzi, S., Ssemugabo, C., Ezumah, N., George, A. S., Hawkins, K., Hao, X., King, R., Liu, T., Molyneux, S., Muraya, K. W., Musoke, D., Nyamhanga, T., Ros, B., Tani, K., Theobald, S., Vong, S., & Waldman, L. (2018). Gendered health systems: Evidence from low- and middle-income countries. Health Research Policy and Systems, 16(1), 58. https://doi.org/10.1186/s12961-018-0338-5
- National Health Systems Resource Centre (NHSRC), Government of India. (2020). Management of Common Emergencies, Burns and Trauma at Primary Care Level. https://nhsrcindia.org/sites/default/files/2021-07/Emergency%20OGs%20at%20HWC.pdf
- National Programme for Prevention & Management of Trauma & Burn Injuries (NPPMTBI). Ministry of Health and Family Welfare, Government of India. Programme brief on burn injury programme. https://main.mohfw.gov.in/sites/default/files/Prog%20brief%20Burn%20component.pdf
- Ng, L. K. (2020). The perceived importance of soft (service) skills in nursing care: A research study. Nurse Education Today, 85, 104302. https://doi.org/10.1016/j.nedt.2019.104302
- NITI Aayog. (2021). Government of India. Healthy States Progressive India: Report on the Ranks of States and Union Territories http://social.niti.gov.in/uploads/sample/SHI_Round_fourth_Report.pdf
- NVivo. (2020). QSR International Pty Ltd. NVivo (released in March 2020). In.
- Panse, N., Panse, S., Ravi, S., Mankar, H., Karanjkar, A., & Sahasrabudhe, P. (2020). Burnout among plastic surgery residents in India: An observational study. Indian Journal of Plastic Surgery, 53(3), 387–393. https://doi.org/10.1055/s-0040-1719238
- Potokar, T., Ali, S., Bouali, R., Walusimbi, M., & Chamania, S. (2010). Training of medical and paramedical personnel in burn care and prevention. Indian Journal of Plastic Surgery, 43(S01), S121–S125. https://doi.org/10.4103/0970-0358.70734
- Potokar, T., Bendell, R., Chamania, S., Falder, S., Nnabuko, R., & Price, P. E. (2020). A comprehensive, integrated approach to quality improvement and capacity building in burn care and prevention in low and middle-income countries: An overview. Burns, 46(8), 1756–1767. https://doi.org/10.1016/j.burns.2020.05.029
- Ramani, S., Parashar, R., Roy, N., Kullu, A., Gaitonde, R., Ananthakrishnan, R., Arora, S., Mishra, S., Pitre, A., Saluja, D., Srinivasan, A., Uppal, A., Bose, P., Yellappa, V., & Kumar, S. (2022). How to work with intangible software in public health systems: Some experiences from India. Health Research Policy and Systems, 20(1), 52. https://doi.org/10.1186/s12961-022-00848-9
- Ranganathan, K., Mouch, C. A., Chung, M., Mathews, I. B., Cederna, P. S., Raja Sabapathy, S., Raghavendran, K., & Singhal, M. (2020). Geospatial mapping as a guide for resource allocation Among burn centers in India. Journal of Burn Care & Research, 41(4), 853–858. https://doi.org/10.1093/jbcr/irz210
- Sheikh, K., Gilson, L., Agyepong, I. A., Hanson, K., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: Framing the questions. PLoS Medicine, 8(8), e1001073. https://doi.org/10.1371/journal.pmed.1001073
- Singh, A. (2018). Burns management in India- The way ahead. Indian Journal of Burns, 26(1), 3–5.
- Sreedharan, S., Cleland, H., & Lo, C. H. (2021). Plastic surgical trainees’ perspectives toward burn surgery in Australia and New Zealand: Changes in the last 17 years? Burns, 47(8), 1766–1772. https://doi.org/10.1016/j.burns.2021.09.013
- Steinmair, D., Zervos, K., Wong, G., & Löffler-Stastka, H. (2022). Importance of communication in medical practice and medical education: An emphasis on empathy and attitudes and their possible influences. World Journal of Psychiatry, 12(2), 323–337. https://doi.org/10.5498/wjp.v12.i2.323
- Vrouwe, S. Q., Pham, C. H., Minasian, R. A., Yenikomshian, H. A., Garner, W. L., & Gillenwater, T. J. (2020). The state of burn care training during plastic surgery residency. Annals of Plastic Surgery, 85(2), 122–126. https://doi.org/10.1097/SAP.0000000000002267
- Win, T. S., Nizamoglu, M., Maharaj, R., Smailes, S., El-Muttardi, N., & Dziewulski, P. (2018). Relationship between multidisciplinary critical care and burn patients survival: A propensity-matched national cohort analysis. Burns, 44(1), 57–64. https://doi.org/10.1016/j.burns.2017.11.003
- Witter, S., Sheikh, K., & Schleiff, M. (2022). Learning health systems in low-income and middle-income countries: Exploring evidence and expert insights. BMJ Global Health, 7(Suppl 7), e008115. https://doi.org/10.1136/bmjgh-2021-008115
- World Health Organization. (2007). Everybody business: strengthening health systems to improve health outcomes: WHO’s framework for action. https://www.who.int/healthsystems/strategy/everybodys_business.pdf
