
Abstract
Background and purpose — Knowledge regarding patient-reported outcomes (PROs) after dislocation and closed reduction is lacking. We report health- and hip-related quality of life (QoL) after dislocation, following primary total hip arthroplasty (THA).
Patients and methods — We conducted a cross-sectional study with patients registered in the Danish Hip Arthroplasty Register from 2010 to 2014. Dislocations were captured based on diagnosis/procedure codes and patient file reviews. Patients with dislocation were matched 1:2, according to age, sex, date, and hospital of primary surgery, to patients without dislocation. 2 PRO questionnaires were applied (EQ-5D, HOOS).
Results — We identified 1,010 living patients with dislocation. Mean follow-up was 7.2 years from index surgery and 4.9 years (range 0.6–9.7) from the latest dislocation. Patients without dislocation reported a higher EQ VAS score of 76 (95% CI 75–77) compared with 68 (CI 66–70) for the dislocation group. The EQ-5D-5L mean index score was 0.89 (CI 0.88–0.90) for the control group, compared with 0.78 (CI 0.76–0.80) for the cases with dislocation without revision. Patients with dislocation reported a lower HOOS-QoL domain score of 63 (CI 60–65), compared with 83 (CI 82–84) for the control group. Even 5 years after the latest dislocation, the HOOS-QoL score remained low, at 66 (CI 62–69). The other HOOS domains were consistently 8–10 points worse after dislocation.
Interpretation — Both health- and hip-related QoL were markedly and persistently reduced among dislocation patients compared with those in controls, for several years. Therefore, the avoidance of the initial dislocation episode is important because the THA does not appear to achieve the full relieving potential.
Hip dislocation is observed in 0.2–10% of patients after total hip arthroplasty (THA) and represents one of the most common early complications (Kwon et al. Citation2006, Brooks Citation2013, Berstock et al. Citation2015, Hermansen et al. Citation2021a). Dislocation leads to immediate pain and requires hospital admission, for the reduction of the dislocated hip, often under general anesthesia. After the first dislocation, recurrent dislocations are reported in roughly 50% of patients (Brennan et al. Citation2012, Hermansen et al. Citation2021a), which may eventually necessitate reoperation. Therefore, hip dislocations result in major immediate impacts and may potentially plague the patient for years.
Although being a quite prevalent complication, there is no understanding of the patient-reported outcomes (PROs) associated with both general health-related quality of life (QoL) and subjective hip function, as demonstrated in a recent systematic review (Hermansen et al. Citation2018). This information is required when discussing indications for surgery, when advising patients after hip dislocation, and to better understand the impacts of this complication. Most likely, QoL may be affected and continuously decrease with recurrent events. Likewise, confidence and trust in hip function and stability become impaired. However, these statements require scientific support.
We report health- and hip-related QoL and patient satisfaction among patients with single or recurrent dislocation episodes, compared with patients without complications, following primary THA due to osteoarthritis (OA), in a large-scale, cross-sectional study.
Patients and methods
Design
We designed a cross-sectional study, involving patients registered in the Danish Hip Arthroplasty Register (DHR) and conducted in accordance with the STROBE guidelines.
Study population
The study was based on a population identified in a recently published paper that reported the “true” 2-year incidence of dislocation after primary THA (Hermansen et al. Citation2021a). We included all patients older than 40 years, who received a THA because of primary OA between January 1, 2010, and December 31, 2014, at both public and private hospitals in Denmark. We excluded patients with acute femoral neck fractures, patients with previous hip surgeries (secondary OA), and patients younger than 40 years, as primary OA rarely occurs in younger individuals. We also excluded any secondary, contralateral THA that was inserted during the inclusion period, to avoid dependency among observations (Ranstam and Robertsson Citation2010).
We defined dislocation cases as patients with 1 or more THA dislocations, either with or without subsequent revision surgery. We excluded cases with revisions that were indicated by any other cause than dislocation.
Dislocations that occurred within the initial 2-year postoperative period were captured in the Danish National Patient Register (DNPR) and verified during a comprehensive review of patient files (Hermansen et al. Citation2021a). Based on these results, we created an algorithm that was designed to identify dislocations with high sensitivity (91%), specificity (> 99%), and positive predictive value (93%) (Hermansen et al. Citation2021b). This algorithm was used to identify dislocations that occurred after the end of the original 2-year follow-up period, until August 1, 2019.
All patients from the original cohort (Hermansen et al. Citation2021a) with no history of dislocation or revision surgery were eligible for the control group. We matched 2 controls without dislocation with each patient with dislocation, based on 4 parameters: age (± 5 years), sex, date of primary THA surgery (± 3 months), and the hospital that performed the THA.
Data sources
Primary THAs are registered in the DHR, with a completeness of 98%, whereas the completeness of reporting revisions is 93% (Pedersen et al. Citation2004, DHR Citation2019). The DHR provided data regarding age, sex, and the surgical specifications of the primary THA and any following revisions.
Dislocations treated with closed reductions were extracted from the DNPR, as these are not reported to the DHR. The DNPR is an administrative database, in which all contacts with the Danish healthcare system are registered with diagnosis and procedure codes, including laterality. The DNPR completeness is 99.7% (Schmidt et al. 2015). We extracted all diagnosis codes in the DNPR up to 10 years prior the date for questionnaire return to calculate a Charlson Comorbidity Index (CCI) (Quan et al. Citation2011). The unique Danish social security number of each Danish citizen enabled the unambiguous cross-linking of registers.
Outcome
By September 2019, our study participants received 2 questionnaires: a generic questionnaire that measures health-related QoL (the EuroQuality of life-5 Dimensions [EQ-5D-5L]) (EuroQol Citation1990), and a hip-specific questionnaire (the Hip disability and Osteoarthritis Outcome Score [HOOS]) (Nilsdotter et al. Citation2003).
The EQ-5D-5L questionnaire covers 5 dimensions of current health status for the specific date of questionnaire completeness. An index value of 1 represents the best possible health; 0 represents a health state comparable with death. A visual analog scale (VAS), ranging from 0 to 100, is also included to record an individual’s rating of their current health-related QoL state (EuroQol Citation1990). A Danish version was available, and approval from the EUROQOL group was obtained before use.
The HOOS questionnaire is hip-specific and consists of 5 domain scores (Nilsdotter et al. Citation2003). The last week is considered when answering the questions. A normalized score was calculated, where 100 indicated no problems, and 0 indicated extreme problems. A subscale was excluded for a given patient if fewer than 50% of the items in a subscale were unanswered. The HOOS has been validated for THA patients, and a validated Danish version exists that can be used free of charge.
We also asked 3 additional questions, regarding patient satisfaction with the original operation, which have previously been described by the Royal College of Surgeons of England (Unit Citation2009).
Q1: “Overall, how are the problems now in the hip on which you had surgery, compared with before your operation?” (much better/a little better/no difference/a little worse/much worse)
Q2: “How would you describe the results of your original hip operation?” (excellent/very good/good/fair/poor)”
Q3: “With the knowledge and experience you have gained after the hip operation, would you then undergo the surgery again?” (yes/no)
The questionnaires were sent using the mandatory Danish electronic mailing system (e-boks), which is coupled to the patient’s social security number. The questionnaires were electronic and were automatically returned and captured in a Research Electronic Data Capture (REDCap) database that was designed for this study. A reminder was emailed after 3 weeks. If the system registered an unsuccessful attempt to answer online, we mailed the questionnaires using regular mail to those patients. In Denmark, exemption from the electronic mailing system can be obtained for individuals who are either mentally or physically impaired or who have no computer access. We were automatically notified regarding any study participants with exemptions, and we distributed the questionnaires by regular mail to these patients, including a pre-paid return envelope. They received a reminder after 2 months, also by regular mail. The answers from the paper questionnaires were manually entered into the REDCap database (single-entry). Cases were able to indicate if they had never experienced a dislocation, despite our information, and controls could indicate if they had experienced a dislocation that required hospitalization and reduction.
Statistics
The EQ VAS scores are presented as means with 95% confidence intervals (CI). The EQ-5D-5L health states are summarized as the index value means with CIs, relative to the norms established for the United Kingdom, as Danish data norms are not currently available (Devlin et al. Citation2018). Multiple linear regression was used to compare the scores, adjusting for age, sex, number of dislocations, and CCI. We used a 2-way quadratic prediction plot to illustrate the change in HOOS QOL domain score as a function of time elapsed since the latest dislocation. Statistical analysis was performed with STATA version 16.0 (StataCorp, College Station, TX, USA).
Ethics, registration, funding, and potential conflicts of interest
The Danish Patient Safety Authority (3-3013-2128) and the Danish Data Protection Agency (2008-58-0035) approved this study. The study was registered in Clinical Trials (NCT03860025). Clara Hansens Memorial Fund; Appropriation Merchant Sven Hansen & Wife Ina Hansens Foundation; the Danish Rheumatism Association; the A.P. Møller Foundation for the Advancement of Medical Science; and Karola Joergensens Fund provided funding for the study. The authors have no conflicts of interest to declare.
Results
Participants
According to the DHR, 36,693 primary THA operations had been performed during our inclusion period, and 31,762 THA operations met our inclusion criteria (). We identified dislocations in 1,344 THA patients, yielding an incidence of dislocation at 4.2% (CI 3.9–4.4) after a mean follow-up of 7.2 years. Among these cases, 282 were deceased and 52 underwent revision for causes other than dislocation, resulting in 1,010 patients eligible for participation. This cohort included 770 patients with 1 or more dislocations and no revision, and 240 patients with dislocation and 1 or more subsequent revisions due to dislocation. We were able to match 2 controls for each of 1,001 cases, 1 control for an additional 6 cases, and no controls for the remaining 3 cases. The questionnaire response rate was 66% among the case group and 72% among the control group. After excluding those cases who denied experiencing dislocation and controls with a self-reported dislocation, 640 cases and 1,422 controls were included in further analyses (). In the case group, the mean (range) follow-up from the latest dislocation was 4.9 years (0.6–9.7).
Figure 1. Flowchart of the inclusion/exclusion process: selection process from DHR data retrieval to the return of questionnaires.
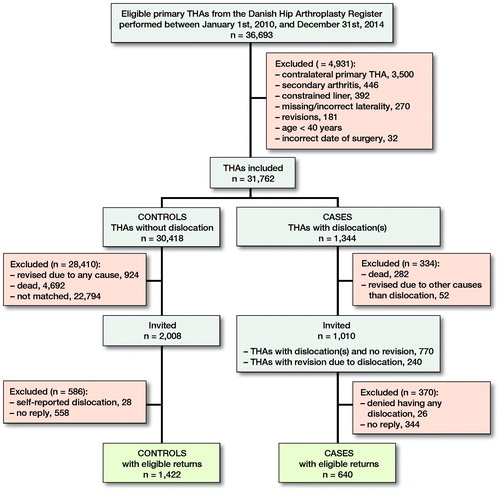
Table 1. Patient demographics. Values are percentage unless otherwise specified
EQ-5D
Patients without dislocation reported a higher mean EQ VAS score of 76 (CI 75–77) compared with 68 (CI 66–70) in the dislocation group (p < 0.001), which further declined to 61 (CI 57–65) in cases with revision(s). The EQ-5D-5L index mean score was 0.89 (CI 0.88–0.90) for the control group, 0.78 (CI 0.76–0.80) for the cases with dislocation without revision (p < 0.001), and the index declined further to 0.72 (CI 0.68–0.77) for the cases with revision(s). The EQ-5D-5L results, presented as health profiles with column charts, can be found in the supplementary data (Figure 2, see Supplementary data).
HOOS
Overall, a decrease of approximately 10 points was observed for 4 out of 5 domains (Pain, Symptoms, ADL, and Sport/Rec) in patients with dislocation(s) compared with scores for controls, and an additional decrease was observed in cases with dislocation and revision(s) compared with cases without revision (). Regarding hip-related QoL, patients with dislocations reported a lower mean HOOS-QoL domain score of 63 (CI 60–65), compared with 83 (CI 82–84) for the control group (). When the case group was divided based on the number of dislocations, we found that an increasing number of dislocations was associated with lower QoL scores (, see Supplementary data). In the case group, females reported lower QoL than males, whereas we saw no difference among age or CCI groups (, see Supplementary data). We also divided the cases based on the length of follow-up from the latest dislocation. The HOOS-QoL score was 54 (CI 48–59) if fewer than 2 years had passed, whereas scores of 64 (CI 59–69) and 66 (CI 62–69) were reported for 2–5 years’ and more than 5 years’ follow-up since the last dislocation, respectively. illustrates the predicted non-linear HOOS QOL domain score as a function of time elapsed since the latest dislocation.
Figure 3. HOOS domain scores presented as means with 95% CIs for all cases with dislocation, cases with dislocation and revision(s), and the control group. A score of 100 indicates no problems and 0 indicates extreme problems. We compared the control group with cases with dislocation (no revision) by multiple linear regression analysis adjusting for CCI and stated statistical significance for all 5 domains (p-value < 0.001).
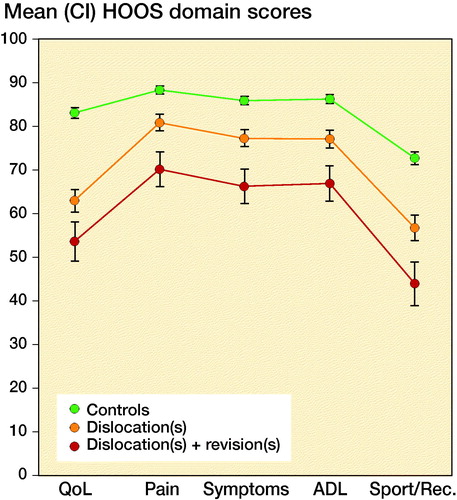
Figure 4. Predicted HOOS QoL score after hip dislocation: graph illustrating the predicted HOOS QoL domain score as a function of time elapsed since the latest dislocation, irrespective of the number of dislocations per patient.
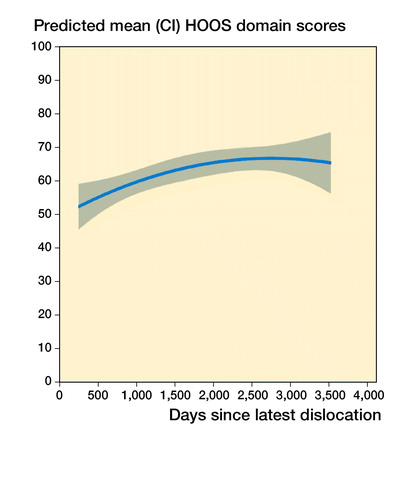
Table 2. HOOS results based on number of dislocations
Table 3. Differences in HOOS QoL score for patients with dislocation(s) depending on age, sex, and CCI, analyzed by multiple linear regression adjusted for number of dislocations, age, sex, and CCI
The third item incorporated in the HOOS-QoL domain is particularly relevant for our study cohort and is related to the lack of hip confidence. Nearly 30% of patients with dislocation reported being either severely or extremely troubled by a lack of confidence, whereas this only applied for 5% of the controls.
Patient satisfaction
Nearly 90% of patients without dislocation reported that the hip is “much better” than before the primary surgery, whereas only 70% of cases with dislocation reported the same (, see Supplementary data). Similarly, only 59% of the dislocation group reported either an “excellent” or a “very good” overall result, whereas the figure was 85% for the control group. This is also reflected in the fact that only 80% of patients with dislocation would undergo the primary surgery again, compared with 93% of controls. The results after revision were worse than the results without revision, as 44% of patients who experienced revisions reported a poor result, compared with 9% of patients who experienced dislocation without revision.
Table 4. Patient satisfaction. Values are % unless otherwise specified
Discussion
To our knowledge, this study represents the largest of its kind reporting PROs in OA patients who experienced hip dislocation after primary THA. We showed that even a single dislocation after THA markedly affected the reported hip-related QoL and patient satisfaction, and that the impact persisted for up to 5 years. The other domains surveyed, including health-related QoL, pain, hip-specific symptoms, ADL, activity levels, and patient satisfaction, were all consistently lower among patients with dislocation and worsened among patients who underwent revision surgery. For those who subsequently undergo revision surgery due to dislocation, the overall result was disappointing, and 44% reported a poor result.
This study has some limitations. We could not obtain preoperative or immediate postoperative PRO measures, as these are not yet routinely registered in Denmark (DHR Citation2019). Therefore, this study was performed as a cross-sectional study, and we do not know whether any patient selection is overrepresented in either the case or control groups. We believe this is unlikely because the cases and controls were matched according to 4 parameters, and because we conducted this study based on a nationwide, high-quality register. We chose not to exclude patients with a non-responding match because this would considerably reduce the number of eligible participants, due to our 70% response rate. As expected, the responders were slightly younger and healthier than the non-responders, which was evident in both the case and control groups. With 30% non-responders, it is also a legitimate question whether the condition of these patients would change the post-dislocation scores significantly. We believe it is reasonable to assume that the non-responders are more likely to suffer from conditions like cognitive impairments, which is not captured in the CCI, or reduced function, and increased dependence on others. This patient group is likely to report lower post-dislocation scores, however, and is not likely to change our overall result (Hutchings et al. Citation2013).
A gap in knowledge exists regarding the patient experience of dislocation impacts. A recently published systematic review identified only 2 studies that compared cases with dislocation with controls without complications after THA due to primary OA (Hermansen et al. Citation2018). The included studies were either very small or used partly patient-reported outcomes (Forsythe et al. Citation2007, Edmunds and Boscainos Citation2011). In our study, the large case group examined enabled us to identify both the consequences of recurrent events and the time factor. We found only a slight improvement in the HOOS-QoL score over time among patients with dislocation, and the score remained persistently 20 points lower than that for controls, even after two years. We focused solely on the patient’s perspective in our study. The EQ-5D was chosen as a generic questionnaire, based on its widespread use, which provides excellent opportunities for comparisons. Compared with the Oxford Hip Score and the HHS, we found the HOOS questionnaire to be more relevant after dislocation, due especially to the hip-related QoL subscale. A number of papers have combined patients with different diagnoses, including patients with revision, without reporting the PRO scores for OA patients separately (Enocson et al. Citation2009, Kotwal et al. Citation2009, Stroh et al. Citation2013, Abdel et al. Citation2015), which is why caution is required when comparing these results for any particular patient group. We defined our cohort of interest as patients with a primary diagnosis of OA and chose to exclude patients receiving THA for other causes, as we believe they are not comparable.
Our study revealed a clear association between dislocation and inferior PRO scores and patient satisfaction. Due to the large number of cases included over a 5-year period, there is good reason to assume that the dislocation is responsible for the inferior results. Earlier studies have reported a difference of approximately 9–17 points on the HOOS to represent the minimal clinically important difference (MICD), depending on the domain examined and the statistical method (Paulsen et al. Citation2014, Lyman et al. Citation2018). Originally, the MICD value is strictly meant for comparing 2 longitudinal measurements for a single individual and not for comparing 2 groups (Beaton et al. Citation2002). However, in our study, we believe it serves as an indicator for a clinically relevant difference between the cases and controls because the threshold has been exceeded, particularly for the HOOS-QoL domain. The reported HOOS and EQ VAS scores for the control group in our study were comparable to those reported in other studies after THA (Paulsen et al. Citation2012, Greene et al. Citation2015). Dislocation is one of the few complications after THA for which non-surgical treatment is an option. Other complications, such as prosthetic joint infection, peri-prosthetic fracture, or aseptic loosening after longer follow-up, are more often deemed to require revision surgery and are, therefore, not comparable to our non-revised cases.
Conclusively, this study has provided new and solid information regarding patients’ experience after a hip dislocation. Even 1 dislocation after a THA was associated with poorer long-term self-reported outcome scores. Health- and hip-related QoL were markedly and persistently reduced, confidence regarding hip stability was lacking, and patients were less satisfied, with more than 20% indicating that they would not choose to have a THA again if armed with their present knowledge. Therefore, the most important aspect must be to avoid the first episode of dislocation, since the full relieving potential for this THA never seems to be achieved, even after many years of follow-up. However, we focused on a single complication and the complete complication profile for every treatment strategy should always be kept in mind. In perspective, this information should be incorporated with other objective aspects when discussing indications for primary THA and when advising patients after a hip dislocation.
Supplemental Material
Download PDF (69.7 KB)LLH, BV, and SO were responsible for the conception of the study; LLH was responsible for the handling of questionnaires and data analysis; LLH drafted the manuscript; BV and SO revised the manuscript critically for important intellectual content, and all authors approved the final version to be published.
Acta thanks Max Gordon and Ola Rolfson for help with peer review of this study.
Supplementary data
Figure 2 and are available as supplementary data in the online version of this article, http://dx.doi.org/10.1080/17453674.2021.1983973
- Abdel M P, Cross M B, Yasen A T, Haddad F S. The functional and financial impact of isolated and recurrent dislocation after total hip arthroplasty. Bone Joint J 2015; 97-b(8): 1046–9.
- Beaton D E, Boers M, Wells G A. Many faces of the minimal clinically important difference (MCID): a literature review and directions for future research. Curr Opin Rheumatol 2002; 14(2): 109–14.
- Berstock J R, Blom A W, Beswick A D. A systematic review and meta-analysis of complications following the posterior and lateral surgical approaches to total hip arthroplasty. Ann R Coll Surg Engl [Meta-Analysis Research Support, Non-U.S. Government Review] 2015; 97(1): 11–16.
- Brennan S A, Khan F, Kiernan C, Queally J M, McQuillan J, Gormley I C, O’Byrne J M. Dislocation of primary total hip arthroplasty and the risk of redislocation. Hip Int 2012; 22(5): 500–4.
- Brooks P J. Dislocation following total hip replacement: causes and cures. Bone Joint J 2013; 95-b(11 Suppl. A): 67–9.
- Devlin N J, Shah K K, Feng Y, Mulhern B, van Hout B. Valuing health-related quality of life: an EQ-5D-5L value set for England. Health Econ 2018; 27(1): 7–22.
- DHR. Danish Hip Arthroplasty Register—Annual Report. Available from: “http://danskhoftealloplastikregisterdk/wp-content/uploads/2019/09/DHR-årsrapport-2019_til-offentliggørelsepdf 2019.
- Edmunds C T, Boscainos P J. Effect of surgical approach for total hip replacement on hip function using Harris Hip scores and Trendelenburg’s test: a retrospective analysis. Surgeon 2011; 9(3): 124–9.
- Enocson A, Pettersson H, Ponzer S, Tornkvist H, Dalen N, Tidermark J. Quality of life after dislocation of hip arthroplasty: a prospective cohort study on 319 patients with femoral neck fractures with a one-year follow-up. Qual Life Res 2009; 18(9): 1177–84.
- EuroQol G. EuroQol—a new facility for the measurement of health-related quality of life. Health Policy 1990; 16(3): 199–208.
- Forsythe M E, Whitehouse S L, Dick J, Crawford R W. Functional outcomes after nonrecurrent dislocation of primary total hip arthroplasty. J Arthroplasty 2007; 22(2): 227–30.
- Greene M E, Rolfson O, Gordon M, Garellick G, Nemes S. Standard comorbidity measures do not predict patient-reported outcomes 1 year after total hip arthroplasty. Clin Orthop Relat Res 2015; 473(11): 3370–9.
- Hermansen L L, Haubro M H, Viberg B L, Overgaard S. Patient-reported outcome after hip dislocation in primary total hip arthroplasty is virtually unknown: a systematic literature review. Acta Orthop 2018: 89(6): 595–6.
- Hermansen L L, Viberg B, Hansen L, Overgaard S. “True” cumulative incidence of and risk factors for hip dislocation within 2 years after primary total hip arthroplasty due to osteoarthritis: a nationwide population-based study from the Danish Hip Arthroplasty Register. J Bone Joint Surg Am 2021a; 103(4): 295–302
- Hermansen L L, Viberg B, Overgaard S. Development of a diagnostic algorithm identifying cases of dislocation after primary total hip arthroplasty-based on 31,762 patients from the Danish Hip Arthroplasty Register. Acta Orthop 2021b: 92(2): 137–42.
- Hutchings A, Grosse Frie K, Neuburger J, van der Meulen J, Black N. Late response to patient-reported outcome questionnaires after surgery was associated with worse outcome. J Clin Epidemiol 2013; 66(2): 218–25.
- Kotwal R S, Ganapathi M, John A, Maheson M, Jones S A. Outcome of treatment for dislocation after primary total hip replacement. J Bone Joint Surg Br 2009; 91(3): 321–6.
- Kwon M S, Kuskowski M, Mulhall K J, Macaulay W, Brown T E, Saleh K J. Does surgical approach affect total hip arthroplasty dislocation rates? Clin Orthop Relat Res 2006; 447: 34–8.
- Lyman S, Lee Y Y, McLawhorn A S, Islam W, MacLean C H. What Are the minimal and substantial improvements in the HOOS and KOOS and JR versions after total joint replacement? Clin Orthop Relat Res 2018; 476(12): 2432–41.
- Nilsdotter A K, Lohmander L S, Klassbo M, Roos E M. Hip disability and osteoarthritis outcome score (HOOS): validity and responsiveness in total hip replacement. BMC 2003; 4:10.
- Paulsen A, Pedersen A B, Overgaard S, Roos E M. Feasibility of 4 patient-reported outcome measures in a registry setting. Acta Orthop 2012; 83(4): 321–7.
- Paulsen A, Roos E M, Pedersen A B, Overgaard S. Minimal clinically important improvement (MCII) and patient-acceptable symptom state (PASS) in total hip arthroplasty (THA) patients 1 year postoperatively. Acta Orthop 2014; 85(1): 39–48.
- Pedersen A, Johnsen S, Overgaard S, Soballe K, Sorensen H T, Lucht U. Registration in the Danish Hip Arthroplasty Registry: completeness of total hip arthroplasties and positive predictive value of registered diagnosis and postoperative complications. Acta Orthop Scand 2004; 75(4): 434–41.
- Quan H, Li B, Couris C M, Fushimi K, Graham P, Hider P, Januel J M, Sundararajan V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol 2011; 173(6): 676–82.
- Ranstam J, Robertsson O. Statistical analysis of arthroplasty register data. Acta Orthop 2010; 81(1): 10–14.
- Schmidt M, Schmidt S A, Sandegaard J L, Ehrenstein V, Pedersen L, Sorensen H T. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol 2015; 7: 449–90.CLEP.S91125.
- Stroh D A, Issa K, Johnson A J, Delanois R E, Mont M A. Reduced dislocation rates and excellent functional outcomes with large-diameter femoral heads. J Arthroplasty 2013; 28(8): 1415–20.
- Unit CE. Clinical Effectiveness Unit. Questionnaire for patients who have had hip surgery. Ann R Coll Surg Engl; 2009.