
ABSTRACT
The present study examined the effect of Acetaminophen on the painful experience of social rejection by examining brain, cardiac and behavioral measures reflecting different aspects of social feedback processing. Healthy students (N = 72), after ingesting either Acetaminophen or a placebo, performed a social judgment paradigm (SJP), in which they could be expectedly or unexpectedly rejected or accepted. During the task, cardiac and brain responses to different types of feedback were measured, as well as expectancies relating to the given feedback. Enhanced cardiac deceleration was found after unexpected social rejection as compared to all other conditions. Larger mean P3 amplitude was found after expected positive and negative feedback stimuli as compared to unexpected stimuli. While cardiac deceleration and P3 were not affected by Acetaminophen, behavioral responses were. While in the control group the percentage of acceptance predictions decreased over the experiment (learning from negative feedback), the Acetaminophen group did not adjust their positive prediction bias over time. The unexpected effect of Acetaminophen on prediction behavior suggests that Acetaminophen might indeed play a role in social pain perception. The normally observed social pain-based learning effect seems to disappear when participants ingest Acetaminophen, which can be interpreted as a reduced pain perception after Acetaminophen.
Introduction
“I don’t like you” is a prototypical example of social rejection that most of us have experienced in our lives. Since friendship, intimacy and a sense of connection are fundamental human needs (Maslow, Citation1981), a refusal of this need, e.g., social rejection, can therefore be a painful experience. Indeed, there is neuronal evidence to suggest that social rejection is a painful experience, comparable to the experience of physical pain. Namely, the dorsal anterior cingulate cortex (dACC), which has consistently been related to the affective response to physical pain (Price, Citation2000; Rainville et al., Citation1997), seems more active during social exclusion than during social inclusion (Eisenberger et al., Citation2003). During social exclusion, dACC activity seems positively correlated with self-reported distress, further indicating the involvement of the dACC in the affective response to social rejection (Eisenberger et al., Citation2003). This overlap between the neural substrates of social and physical pain (Eisenberger & Lieberman, Citation2004) makes evolutionary sense too. Namely, the social attachment system may have latched on to the opioid substrates of physical pain to maintain closeness with others, causing distress upon separation and comfort upon reunion (Eisenberger, Citation2012). Arguably, social connectedness in the presence of noxious stimuli (e.g., tigers, quicksand) increases survival likelihood. Critically, however, it is still highly debatable whether “painful” is a truly scientifically or merely metaphorically appropriate reference to experiences of social rejection (Iannetti et al., Citation2013). Although various research groups have confirmed the strong overlap between the brain networks involved in social and physical pain (e.g., Kross et al., Citation2011), it should be noted that this overlap might be due to similar higher order properties of all painful stimuli, but also other important stimuli, such as salience (Iannetti et al., Citation2013; Wager et al., Citation2016).
Rather than social pain, however, cognitive conflict might explain dACC activity during social exclusion experiments as well (Somerville et al., Citation2006). Namely, a bifunctionality of the ACC has been proposed. While the ventral ACC (vACC) is often related to social and emotional processes (Bush et al., Citation2000; Whalen et al., Citation1998), the dACC is typically associated with the occurrence of cognitive conflicts (Botvinick et al., Citation2004; Carter et al., Citation1998). Perhaps, during experimentally manipulated social exclusion, the expectation to participate is violated, resulting in cognitive conflict and thereby, independently of the effects of social rejection, in dACC activity (Somerville et al., Citation2006). Fortunately, the neural substrates of social rejection and expectancy violation can be independently examined using the Social Judgment Paradigm (SJP; Somerville et al., Citation2006). In the SJP, participants believe a panel of individuals judged a photo of them. During the experiment, pictures of these panel members are subsequently presented, where the participant is asked to predict whether they liked them or not. Then, the judgments (which are, unbeknownst to the participant, computer-generated) are presented. Four stimulus conditions arise; the participant is expectedly or unexpectedly accepted or rejected. SJP results suggest that the dACC and the vACC are functionally dissociated (Somerville et al., Citation2006). The dACC seems sensitive to expectancy violation (expected versus unexpected) and the vACC seems sensitive to feedback type (acceptance versus rejection). Thus, to the extent that people expect consistency in social exchange, dACC activity may reflect violations of the expectation of social inclusion or acceptance (Somerville et al., Citation2006).
Although these findings suggest that the dACC is rather involved in cognitive aspects of the SJP (expectancy violation), it should be noted that those cognitive aspects could still be associated with social pain (Eisenberger, Citation2015). Namely, autonomic nervous system function has also been linked to social pain perception in the SJP (Gunther Moor et al., Citation2010). Specifically, relative to the other stimulus conditions, unexpected social rejection seems to lengthen the interval between consecutive heartbeats (the interbeat interval; IBI). Considering the previously discussed role of the dACC, unexpected social rejection possibly triggers an alarm system by noticing a discrepancy between the expected state of social belonging (i.e., acceptance) and the actual state of belonging (i.e., rejection). Cardiac deceleration might reflect this process (Gunther Moor et al., Citation2010). This effect, referred to as the “heartbrake of social rejection”, has been replicated in several studies (e.g., Dekkers et al., Citation2015; Van Der Veen et al., Citation2014, Citation2016).
On the neural level, P3 amplitudes in response to social feedback in the SJP have also been investigated using Electroencephalography (EEG; Van Der Molen et al., Citation2014). The P3 is a positive going event-related brain potential component, maximal around 300 ms after stimulus onset. In the SJP, expected acceptance seems to evoke a stronger P3 than the other stimulus conditions, maximal at fronto-central positions. This effect is thought to be related to vACC activity and motivational properties of positive social evaluations. Arguably, it might be important and therefore particularly rewarding, for individuals to both be liked and confirmed in their expectations, because it shows that the individual’s social theory (i.e., who likes him/her and who does not) is correct (Van Der Veen et al., Citation2014). This effect, sometimes referred to as the “brain wave of social acceptance”, has been replicated in several studies (e.g., Gu et al., Citation2020; Sun & Yu, Citation2014; Van Der Molen et al., Citation2018; Van Der Veen et al., Citation2016). Lastly, in the SJP, healthy controls seem positively biased regarding their predictions; they expect acceptance about sixty percent of the time (e.g., Gu et al., Citation2020; Van Der Veen et al., Citation2016).
Arguably, the neural overlap between physical and social pain implies that factors that influence one type of pain, influence the other as well (Eisenberger & Lieberman, Citation2004). For example, seeing pictures of a romantic partner, a social influence, reduces experimentally induced physical pain as measured by fMRI (Younger et al., Citation2010). Hypothetically, the other way around, painkillers like Acetaminophen (Paracetamol), an analgesic widely used for reducing physical pain, could relieve social pain. The underlying mechanisms for Acetaminophen’s effects are poorly understood. However, cyclooxygenase enzyme inhibition and serotonergic, cannabinoid, and opioidergic neural pathways have been suggested (Smith, Citation2009; Toussaint et al., Citation2010). Considering the richness of μ-opioid receptors in the ACC (Firestone et al., Citation1996; Schlaepfer et al., Citation1998), an area implicated in affective and social pain perception (Eisenberger et al., Citation2003; Somerville et al., Citation2006), Acetaminophen could affect social pain.
Fortunately, the effects of Acetaminophen on social pain have been investigated (DeWall et al., Citation2010; Mischkowski et al., Citation2016). In one study, three weeks of Acetaminophen intake gradually decreased subjectively measured hurt feelings and social pain resulting from experimentally induced social exclusion. Moreover, Acetaminophen attenuated dACC and anterior insula (AI) activity (DeWall et al., Citation2010). In another study, Acetaminophen reduced empathy to (social) pain (Mischkowski et al., Citation2016). In a more recent study, interactive effects of forgiveness and Acetaminophen on social pain were found. Acetaminophen, as compared with placebo or no pill, reduced 18.5% of participants’ social pain levels over twenty days, but only for those exhibiting high levels of forgiveness (Slavich et al., Citation2019). More generally, multiple studies suggest that the effects of Acetaminophen extend beyond the relief of physical pain (e.g., inhibited evaluative analysis of errors; Randles et al., Citation2016). Together, these findings suggest that Acetaminophen is effective in reducing social pain, but the literature is limited to subjectively experienced rejection and experimentally manipulated social exclusion. Moreover, the effects of Acetaminophen in the SJP have not been evaluated.
The present study primarily investigated whether cardiac deceleration resulting from unexpected rejection in the SJP, which is thought to reflect social pain (e.g., Gunther Moor et al., Citation2010), is decreased by Acetaminophen. For our primary hypothesis, we specifically focused on the third IBI following the onset of unexpected rejection, which is the IBI showing the largest effect of social rejection (e.g., Gunther Moor et al., Citation2010; Van Der Veen et al., Citation2014, Citation2016). In addition, the effects of Acetaminophen on P3 amplitudes in response to social feedback were also investigated. While, considering the literature, a stronger P3 amplitude following expected acceptance is hypothesized, a clear hypothesis regarding the effect of Acetaminophen on these P3 amplitudes cannot be stated. Finally, behavioral outcomes and the effects of Acetaminophen on these outcomes were exploratively analyzed. Again, while, considering the literature, a positive prediction bias is expected in the control group, a clear hypothesis regarding the effect of Acetaminophen on cannot be stated.
Method
Participants
Participants were Dutch speaking, were below thirty years of age, had previous successful experience with Acetaminophen as a painkiller and were willing to send in a picture of themselves. Exclusion criteria were the presence of neurological or psychiatric illness and the use of medication. Furthermore, participants were prohibited to consume drugs or alcohol 24 hours in advance of the experiment. In order to determine the number of participants we performed a power analysis using an online tool (http://powerandsamplesize.com/Calculators/Compare-2-Means/2-Sample-Equality). Power was calculated based on our primary outcome measure, cardiac deceleration following unexpected social rejection. In previous studies it was found that in the unexpected rejection condition heart rate slowed in comparison to other conditions and we expected that this slowing would be reduced by acetaminophen. Based on previous studies we predicted a slowing of 10 ms in the third interval following rejection in the Placebo condition and no slowing in the Acetaminophen condition (comparable to other conditions in previous studies). With power set to 0.8, a two-sided alpha of 0.05 and a standard deviation of 15 (based on previous studies), we had to include two groups of 36 participants each. In total, 76 participants were tested, of which 72 participants’ data were eligible for analysis (mean age, M = 21.78, SD = 3.57; 48 females, 24 males). The data of four participants was removed because of technical errors. Sample characteristics and subjective measures outcomes are, per group, presented in . Independent samples t-tests did not reveal significant differences between the groups on any of the presented variables (all p’s> .086). All participants signed a written informed consent and were paid €25. This study was approved by the local Medical Ethical Review Committee.
Table 1. Sample characteristics and subjective measures outcomes. Independent samples t-tests did not reveal significant differences between the groups on any of the presented variables (all p’s> .086)
Stimuli and procedure
After having signed up online for the study, participants were contacted via e-mail and instructed by using a cover story. At least one week before the actual experiment, they were asked to send in a picture of themselves to the experimenter. They were told that this picture was to be judged (i.e., “liked” or “not liked”) by a panel of students of multiple universities and that these evaluations were to be send back to our research team alongside the pictures of the panel members. In the actual experiment, participants also watched and assessed emotional movie clips after performing the Social Judgment Paradigm (SJP). These assessments, however, are not described in this paper. After having signed informed consent, participants were asked to take two Acetaminophen or placebo pills. Acetaminophen and placebo pills were prepared by Tiopharma (Kerkrade, the Netherlands). The two experimental pills consisted of 500 mg acetaminophen each and the placebo pills of microcrystalline cellulose. Both types of pills were physically indistinguishable, and both the experimenter and participant were unable to determine whether placebo or acetaminophen was given. Participants had been randomly assigned through a double-blind procedure. Participants consecutively completed several questionnaires (see: Questionnaires) using Qualtrics (Qualtrics, Provo, UT). Afterward, the participants were attached to the EEG equipment and the SJP commenced. The SJP started 1 hour after ingestion of the pills, which is known to guarantee maximal and comparable plasma levels during the whole experiment (e.g., Rawlins et al., Citation1977). In the SJP, participants were asked to look at the pictures of the panel members, which were presented for a total fixed period of six seconds in the screen in front of them. The faces were presented in black and white against a black background. Participants were instructed to predict whether the person in the picture had (dis)liked them (“z” for “like” and “m” for “not like”). After the onset of the face, the participants had a three seconds response window. Then, their prediction (“Yes” for “like” or “No” for “not like”) was shown on the screen to the left of the picture of the panel member. After another second, the judgment (“yes” or “no”) was presented to the right of the picture. Participants’ predictions were still visible. Actually, there were no panel members, nor judgments. Instead, 120 faces with a neutral face expression were derived from the Chicago Face Database (Ma et al., Citation2015). The selection of pictures consisted of fifty percent male and fifty percent female faces. The judgments were based on a computer-generated pseudo-random sequence consisting of fifty percent “Yes” and fifty percent “No” judgments. The same sequence of faces and judgments were presented for each participant. An example trial is shown in . After the task, participants were detached from the EEG equipment and a second task regarding crying behavior was performed. This task, however, is part of another study and will not be discussed here. It lasted about fifteen minutes. After the second task, participants were asked to complete a questionnaire. Finally, after a short debriefing in which it was explained that there were no real social evaluations, the participants could leave the laboratory.
Figure 1. Example of a trial sequence (YY (= expected acceptance) condition) for the social judgment task. Example picture was derived from the Chicago face database (Ma et al., Citation2015)
Questionnaires
The Beck Depression Inventory (BDI-II; Beck et al., Citation1961), the shortened and revised Eysenck Personality Questionnaire (EPQ-rss; Eysenck et al., Citation1985), and the Liebowitz Social Anxiety Scale (LSAS; Liebowitz, Citation1987) were used as self-report questionnaires.
Data acquisition
EEG was recorded with BioSemi Active-Two using 32 channels (10–20 System) with Ag/AgCl active electrodes mounted in an elastic cap. An electrocardiogram (ECG) was recorded from a single lead placed below the left ribcage. Signals were recorded with a low-pass filter of 134 Hz and were digitized with a sample rate of 512 Hz and 24-bit analog/digital conversion. The signals were referenced offline to mathematically linked mastoids. A vertical electrooculogram (EOG) was derived from electrodes placed above and below the left eye. A horizontal EOG was derived from electrodes next to each eye. BioSemi uses the common mode sense (CMS) and driven right-leg electrodes to create a feedback loop that replaces the conventional ground electrode. The CMS was used as an online reference. The EEG and ECG data were analyzed offline using Vision Analyzer (Brain Products GmbH, Munich, Germany). The EEG signals were filtered using a band-pass filter between 0.1 and 30 Hz (phaseshift-free Butterworth filters, 24 dB/octave slope). For the ERP analysis, a 200-ms pre-feedback period was used for baseline correction. Visual inspection of the grand average ERPs showed that the P3 amplitude was maximal between 325 and 425 ms after stimulus onset, and therefore we decided to quantify the P3 amplitude as the average voltage in the area between 325 and 425 ms after the stimulus onset. On average 32 trials were included for the expected acceptance feedback (YY), 33 for unexpected rejection (YN), 26 for unexpected acceptance (NY) and 23 for expected rejection (NN).
For the interbeat intervals (IBIs), R peaks were detected in the ECG signal using the peak detection algorithm implemented in BrainVision Analyzer, and interbeat intervals (IBIs) were computed between consecutive r peaks. Missing values and artifacts were detected by visual inspection and corrected manually. We selected six IBIs surrounding the judgment stimulus for further analysis, that is, two preceding IBIs (−2 and −1), the current IBI (i.e., IBI 0), and the three subsequent IBIs (i.e., IBIs 1, 2, and 3). IBIs 0 to 3 were referenced to the second IBI preceding stimulus onset (IBI −2).
Statistical analysis
Data was analyzed using SPSS 23 (SPSS Inc., Chicago, IL). Primarily, an independent samples t-test was done to assess whether the placebo and Acetaminophen groups differed in cardiac deceleration on IBI 3 after unexpected rejection. To further explore the cardiac data, a repeated measures ANOVA was performed with “expectation” (two levels: like vs. do not like), “judgement” (two levels: like vs. do not like) and “IBI” (four levels: IBI’s 0–3) as within-subjects factors and “group” (placebo vs. Acetaminophen) as between-subjects factor. P3 amplitudes were statistically evaluated in a repeated measures ANOVA design with “electrode position” (three levels: Pz, Fz and Cz), “expectation” and “judgement” as within-subjects factors and “group” as between-subjects factors. Performance was quantified as the percentage of “like”-judgments in either the first or last twenty (out of 120) trials of the experiment. Outcomes were compared using a repeated measures ANOVA design with “trials” (two levels: trials 0–20 vs. trials 100–120) as within-subjects factor and “group” as between-subjects factor. Huynh-Feldt corrections were applied where needed, but uncorrected degrees of freedom are reported. Bonferroni-corrected follow-up analyses were performed where significant effects were found. Significance levels were set at 5% (α = .05).
Interbeat intervals
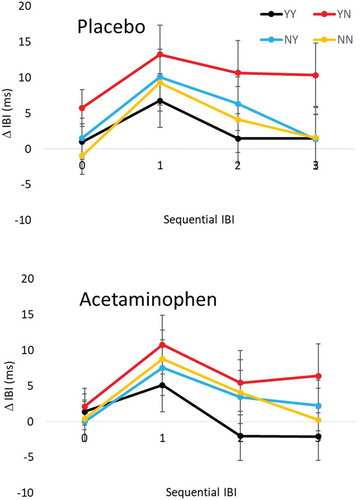
Cardiac responses are shown in . An independent samples t-test did not reveal any differences between placebo and Acetaminophen in cardiac deceleration on IBI 3 succeeding unexpected rejection, t(70) = .62, p = .538. A repeated measures ANOVA of the cardiac response revealed a main effect of sequential IBI, F(3,210) = 7.19, p = .001, ηp2 = .093, and a two-way interaction between expectation and judgment, F(1,70) = 6.53, p = .013, ηp2 = .085. For group, main and interactive effects remained insignificant (all F’s< .63, all p’s≥ .431). Follow-up analyses showed significant differences between IBI 0 and 1 (p < .001), IBI 1 and 2 (p = .026) and IBI 1 and 3 (p = .016). Further follow-up analyses revealed that cardiac deceleration resulting from unexpected rejection was larger overall than cardiac deceleration resulting from expected acceptance (p = .003) and from expected rejection (p = .013).
Figure 2. Cardiac responses (±SEM) to expected or unexpected acceptance or rejection for the placebo group and the Acetaminophen group. Cardiac responses are shown for IBI’s 0, 1, 2 and 3 and are referenced to IBI −2. Y = Yes, N = No, so that YY = expected acceptance, YN = unexpected rejection, NY = unexpected acceptance, NN = expected rejection, IBI = Interbeat interval, ms = milliseconds
P3 amplitude
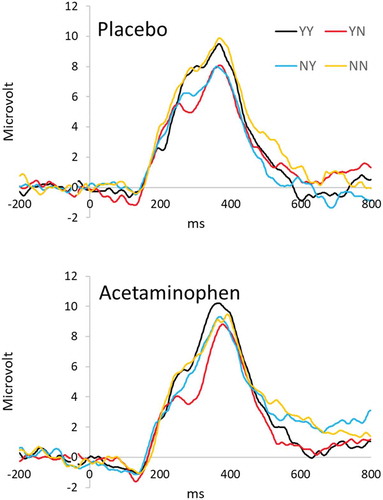
Averaged waveforms for the Fz electrode are presented in and P3 amplitudes are shown in . A repeated measures ANOVA revealed a main effect for electrode location, F(2,140) = 83.28, p < .001, ηp2 = .543, two-way interactions between electrode location and prediction, F(2,140) = 4.54, p = .015, ηp2 = .061, and between expectation and judgment, F(1,70) = 6.64, p = .012, ηp2 = .087, and a three-way interaction between electrode location, expectation and judgment, F(2,140) = 3.72, p = .043, ηp2 = .05. For group, main and interactive effects remained not significant (all F’s< 2.19, all p’s≥ .134). Follow-up analyses showed overall P3 amplitude to be equal at Pz and Cz and statistically lower at Fz (p < .001, for both Pz and Cz). Further follow-up analyses revealed that acceptance resulted in a larger P3 amplitude when it was expected as opposed to unexpected (p = .013). In addition, this effect interacted with electrode location; it was significant at Fz (p = .005) and Cz (p = .013), but not at Pz.
Figure 3. ERP waveforms on the frontal position (Fz), separate for placebo and acetaminophen groups and the four stimulus conditions. Y = Yes, N = No, so that YY = expected acceptance, YN = unexpected rejection, NY = unexpected acceptance, NN = expected rejection, ms = milliseconds
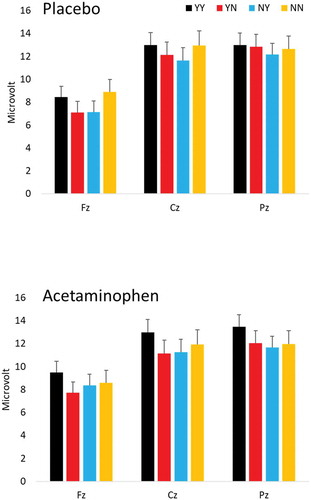
Figure 4. P3 amplitudes (+SEM) as measured at the frontal position (Fz) for the placebo group and the Acetaminophen group. The P3 amplitude is quantified as the average amplitude in an area between 325 milliseconds (ms) and 425 ms poststimulus. Y = Yes, N = No, so that YY = expected acceptance, YN = unexpected rejection, NY = unexpected acceptance, NN = expected rejection, Cz = central position, Pz = parietal position
Expectation bias
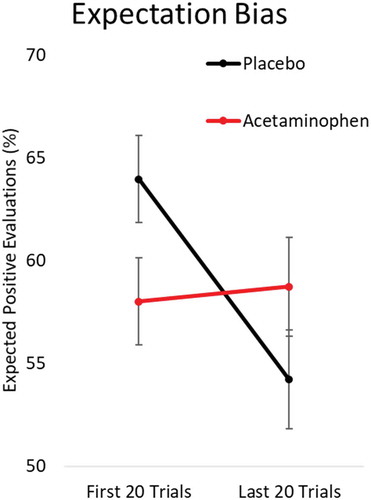
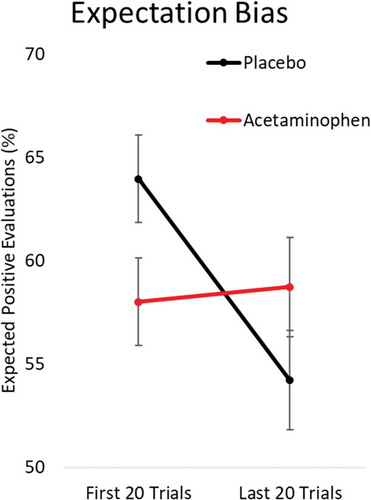
A repeated measures ANOVA was performed to analyze the behavioral outcomes (i.e., predictions) over the experiment. A main effect was found for trials (i.e., trials 1 to 20 versus 100 to 120), F(1,70) = 7.73, p = .007, ηp2 = .099, and a two-way interaction between trials and group, F(1,70) = 10.44, p = .002, ηp2 = .13.Footnote1 On average, participants expected to be accepted more often in trials 1 to 20 than in trials 100 to 120. This effect interacted with group; the effect was significant in the placebo group (p < .001), but not in the Acetaminophen group (p = .750). These effects are presented in . This figure seems to show that the interaction is at least partly driven by the placebo group being more positive in the beginning of the task, but a direct comparison of bias in the first 20 trials between both groups did not show a significant difference (t(70) = 1.98, p> .05).Footnote2
Figure 5. Expectation bias (±SEM) per group quantified as the percentage of acceptance expectations in the first or last part of the experiment
Discussion
This study examined the effect of Acetaminophen on the painful experience of social rejection. The primary finding of the present study was that the cardiac deceleration associated with unexpected rejection in a social evaluation task, which is thought to reflect social pain, was not affected by Acetaminophen. Secondarily, P3 amplitudes, which supposedly reflect the rewarding value of the feedback stimulus, were also not affected by Acetaminophen. Finally, the percentage expected positive feedback decreased during the task in the placebo condition but was constant during the Acetaminophen condition.
To our knowledge, the present study was the first to study the effects of Acetaminophen on cardiac responses to unexpected social rejection in the Social Judgment Paradigm (SJP). In line with previous studies, findings indicated that unexpected rejection resulted in enhanced cardiac deceleration, compared to the unexpected acceptance or expected rejection and acceptance (e.g., Gunther Moor et al., Citation2010; Van Der Veen et al., Citation2014, Citation2016). Contrary to hypothesis however, Acetaminophen did not reduce this enhanced cardiac deceleration, suggesting that Acetaminophen is ineffective in reducing experienced social pain resulting from social rejection, at least as operationalized as enhanced cardiac deceleration. The hypothesis was mainly based on the findings of DeWall et al. (Citation2010), who found that three weeks of daily Acetaminophen intake reduced subjectively experienced social pain (experiment 1) and neural pain responses in the Cyberball-paradigm (experiment 2). It should be noted, however, that in DeWall et al. (Citation2010), participants were given Acetaminophen over the course of three weeks (and in their second experiment even twice the dose), while in the current study, participants received a single dose. Over three weeks, DeWall et al. (Citation2010) found subjectively measured hurt feelings to gradually decrease with the intake of Acetaminophen. With the current findings in mind, this could indicate that long-term intake is required for Acetaminophen to affect the (subjectively experienced) pain of social rejection. Furthermore, the current study did not directly investigate subjectively experienced social pain, as in DeWall et al.’s (Citation2010) first experiment, but attempted to objectively quantify social pain as enhanced cardiac response in response to social feedback. Considering the current findings and the suggested effect of Acetaminophen on evaluative processes (Randles et al., Citation2016), it could be argued that the physiological reflection of social pain perception, as quantified by cardiac deceleration, is unaltered by Acetaminophen, whereas through an effect on evaluative processes, its subjective experience could be still altered. Finally, it should be mentioned that DeWall et al.’s (Citation2010) second experiment studied a related but clearly different construct, namely social exclusion, which might implicate that Acetaminophen specifically influences the pain of social exclusion and not the pain caused by social rejection.
The current study is also unique in investigating whether Acetaminophen could alter neural responses (i.e., P3 amplitudes) to the SJP. In line with the literature, mean P3 amplitude was larger after expected acceptance than after both unexpected stimuli. However, Acetaminophen did not affect P3 amplitudes. As mentioned, a hypothesis could not be stated. Van Der Molen et al. (Citation2014), (Citation2016)) argued that P3 amplitudes possibly reflect reward processing and there is no indication, in the literature and in the current findings, of an effect of Acetaminophen on reward processing. One study did report a blunting effect on arousal ratings of both positive and negative emotional stimuli (Durso et al., Citation2015) which might lead to the prediction that lower P3 amplitudes could be expected for all stimulus categories. The findings of Durso et al. were, however, not specific to feedback stimuli and the relation between subjective arousal ratings and P3 amplitude is complex. It has been proposed that P3 might reflect phasic noradrenergic arousal responses as mediated by the Locus Coeruleus (Nieuwenhuis et al., Citation2005), but it is unclear how this precisely affects subjective arousal ratings.
In contrast to our cardiac and brain measures, Acetaminophen affected behavior, namely the decrease in acceptance expectations over time. At the start of the experiment, participants in the placebo condition expected to be accepted more often than to be rejected. At the end of the experiment, however, participants’ acceptance expectations had lowered to around 54%. The positive bias with which the placebo group started, had been reduced to almost match the actual acceptance/rejection proportion in the SJP, namely fifty percent. Interestingly, Acetaminophen altered the reduction in positive predictions, that is, participants’ positive predictions remained unchanged over the experiment.Footnote3 This adaptation to the task could be interpreted as a learning effect, that is, participants adapt their predictions to the actual rate of positive evaluations. One could argue that this adaptation is caused by the experience of social pain of unexpected rejection, which can be reduced by expecting more negative evaluations. In this way the adaptive response can be a reflection of learning from painful experiences and the disappearance of the effect with Acetaminophen could in this way be attributed to experiencing less pain from rejection. Effects of Acetaminophen on learning have also been shown in a recent study by Pearson et al. (Citation2018). The authors linked the effect of Acetaminophen to its effect on the serotonin system, which might be interesting to explore in future studies. It should be mentioned that the effect on the expectancy bias was unpredicted, and the analyses were explorative, so there is a clear need of direct replication in an independent sample. On the other hand, the effect is also present when Bayesian analysis techniques were applied and when males and females were tested separately. Moreover, the experimental and the placebo group did not differ with respect to gender, psychopathology and personality characteristics. Importantly, although seems to suggest an initial difference in bias between the placebo and Acetaminophen group, this difference was not significant. Therefore, we would like to argue that the finding should be taken seriously, but more research is clearly needed to further explore the found association.
Previous studies have shown that depression and anxiety may influence neural, cardiac and behavioral responses to social evaluative feedback (Harrewijn et al., Citation2018; Van Der Molen et al., Citation2018; Van Der Veen et al., Citation2016) and the prediction of social feedback (Quarmley et al., Citation2019; Van Der Molen et al., Citation2014). Furthermore, Fung and Alden (Citation2017) found that Acetaminophen can reduce social anxiety, although half of the reported effect was mediated by a reduction in social pain. In the current study, however, individual differences in self-reported anxiety and depression cannot explain the group differences and did not influence the effect of Acetaminophen on expectancy bias. Groups did not differ with respect to their depression and anxiety scores and adding these score as a covariate did not influence statistical significance of the reported effects of Acetaminophen.
Some limitations must be noted. The sample size was based on the primary outcome measure (i.e., unexpected rejection on IBI 3: placebo versus Acetaminophen), increasing the risk of false-positive results in the behavioral outcome measure. Together, the current findings must be directly replicated in order for firm conclusions to be made. A second limitation pertains the design of the study. Acetaminophen was compared with placebo and if significant differences appeared, they were interpreted as effects of Acetaminophen. However, because this study was the first of its kind, it did not assess placebo effects. On the one hand, the observed effects of Acetaminophen should therefore be interpreted as relative to placebo effects. On the other hand, the results found in the placebo group are in line with previously found results. In these previous studies there could not be placebo effects, because there were no experimental conditions. Therefore, at least with some certainty, effects can be attributed to Acetaminophen. Still, investigating placebo effects in the SJP, for example, by comparing with a no-pill or some physical pain condition, could be helpful for future studies surrounding the SJP and interesting for practical purposes, namely those of reducing social pain. A third limitation is that the analysis strategy for physiological and behavioral measures differed, and therefore it is hard to directly compare effects. For the bias measure we had the possibility to look in a more detailed way at how behavior changed over time within the task. Unfortunately, this was not possible for the physiological measures, as we did not have enough trials available to compute a reliable ERP or cardiac response for different parts of the task. Lastly, as with most studies, the ecological validity (i.e., the degree to which it corresponds with reality) of the SJP is questionable. Participants are rejected or accepted by unknown faces on a screen. It could be questioned whether these experiences of rejection and acceptance, are comparable to actual experiences of rejection and acceptance. For real-life acceptance or rejection, it is necessary that a more thorough impression is formed. Whether findings within the SJP can be generalized to everyday life is doubtful.
In conclusion, while the current study did not find any effects of Acetaminophen on social pain as quantified by enhanced cardiac deceleration and social acceptance as quantified as larger P3 amplitudes, it did demonstrate an effect of Acetaminophen on behavioral responses to a social evaluation task. The pattern of behavioral findings might reflect a social pain-based learning effect, involved in the avoidance of social pain. This effect, however, disappears with the ingestion of Acetaminophen, suggesting that Acetaminophen might reduce the experience of social pain. Although this conclusion is based on an explorative analysis, it is interesting and inviting to further exploration. This study, in its entirety, contributes to the literature and understanding of Acetaminophen, as well as social feedback processing. It preliminarily demonstrates that Acetaminophen might influence social feedback processing, specifically the processing of social rejection.
Data availability statement
None of the data or materials for the experiments reported here is available, and none of the experiments was preregistered.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Notes
1 An alternative statistical approach using Bayesian statistics seems to point in the same direction (Bayes Factor in favor of a difference between groups was 1.287).
2 An anonymous reviewer suggested that including either depression or neuroticism as covariates might change the results. To test this hypothesis we added both separately as covariates to the GLM analysis. Neither depression nor neuroticism affected the reported interaction (p’s>.5) between trials and group, which remained significant. Furthermore, an anonymous reviewer suggested that degree of deceleration to the rejection might predict the changes in positive expectation bias. To test this hypothesis, we computed the correlation between the change in expectation bias and cardiac deceleration at our IBI of prime interest and did not find a significant correlation (p > .4). We also added the IBI of interest as a covariate to our primary analysis of expectation bias and did not find a significant interaction between trials (first 20 compared to last 20 trials) and cardiac deceleration at IBI 3 (p > .6).
3 Although not reported in previous papers with the SJP, the adaptive response in the placebo condition is consistently found in studies using the SJP. In an unpublished bachelor thesis based on the combination of 8 studies in our lab (N = 399) we found that the adaptation in expectations from the beginning (57%) to the end of the task (51%) is strong and consistent (T = 9.4, p < .001). Moreover, the effect of Acetaminophen on this adaptation effect (interaction between trials and group) is significant for both males (p = .041) and females (p = .024) when tested separately. Finally, an alternative statistical approach using Bayesian statistics seems to point in the same direction (Bayes Factor in favor of an effect of Acetaminophen was 18.4).
References
- Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An Inventory for Measuring Depression. Archives of General Psychiatry, 4(6), 561–571.
- Botvinick, M. M., Cohen, J. D., & Carter, C. S. (2004). Conflict monitoring and anterior cingulate cortex: An update. Trends in Cognitive Sciences, 8(12), 539–546. https://doi.org/10.1016/j.tics.2004.10.003
- Bush, G., Luu, P., & Posner, M. I. (2000). Cognitive and emotional influences in anterior cingulate cortex. Trends in Cognitive Sciences, 4(6), 215–222. https://doi.org/10.1016/S1364-6613(00)01483-2
- Carter, C. S., Braver, T. S., Barch, D. M., Botvinick, M. M., Noll, D., & Cohen, J. D. (1998). Anterior cingulate cortex, error detection, and the online monitoring of performance. Science, 280(5364), 747–749. https://doi.org/10.1126/science.280.5364.747
- Dekkers, L. M., Van Der Molen, M. J., Gunther Moor, B., Van Der Veen, F. M., & Van Der Molen, M. W. (2015). Cardiac and electro-cortical concomitants of social feedback processing in women. Social Cognitive and Affective Neuroscience, 10(11), 1506–1514. https://doi.org/10.1093/scan/nsv039
- DeWall, C. N., MacDonald, G., Webster, G. D., Masten, C. L., Baumeister, R. F., Powell, C., … Eisenberger, N. I. (2010). Acetaminophen reduces social pain: Behavioral and neural evidence. Psychological Science, 21(7), 931–937. https://doi.org/10.1177/0956797610374741
- Durso, G. R., Luttrell, A., & Way, B. M. (2015). Over-the-counter relief from pains and pleasures alike: Acetaminophen blunts evaluation sensitivity to both negative and positive stimuli. Psychological Science, 26(6), 750–758. https://doi.org/10.1177/0956797615570366
- Eisenberger, N. I. (2012). The pain of social disconnection: Examining the shared neural underpinnings of physical and social pain. Nature Reviews Neuroscience, 13(6), 421–434. https://doi.org/10.1038/nrn3231
- Eisenberger, N. I. (2015). Social pain and the brain: Controversies, questions, and where to go from here. Annual Review of Psychology, 66(1), 601–629. https://doi.org/10.1146/annurev-psych-010213-115146
- Eisenberger, N. I., & Lieberman, M. D. (2004). Why rejection hurts: A common neural alarm system for physical and social pain. Trends in Cognitive Sciences, 8(7), 294–300. https://doi.org/10.1016/j.tics.2004.05.010
- Eisenberger, N. I., Lieberman, M. D., & Williams, K. D. (2003). Does rejection hurt? An fMRI study of social exclusion. Science, 302(5643), 290–292. https://doi.org/10.1126/science.1089134
- Eysenck, S. B., Eysenck, H. J., & Barrett, P. (1985). A revised version of the psychoticism scale. Personality and Individual Differences, 6(1), 21–29. https://doi.org/10.1016/0191-8869(85)90026-1
- Firestone, L. L., Gyulai, F., Mintun, M., Adler, L. J., Urso, K., & Winter, P. M. (1996). Human brain activity response to fentanyl imaged by positron emission tomography. Anesthesia & Analgesia,82(6), 1247–1251.
- Fung, K., & Alden, L. E. (2017). Once hurt, twice shy: Social pain contributes to social anxiety. Emotion, 17(2), 231. https://doi.org/10.1037/emo0000223
- Gu, R., Ao, X., Mo, L., & Zhang, D. (2020). Neural correlates of negative expectancy and impaired social feedback processing in social anxiety. Social Cognitive and Affective Neuroscience, 15(3), 285–291. https://doi.org/10.1093/scan/nsaa038
- Gunther Moor, B., Crone, E. A., & Van Der Molen, M. W. (2010). The heartbrake of social rejection: Heart rate deceleration in response to unexpected peer rejection. Psychological Science, 21(9), 1326–1333. https://doi.org/10.1177/0956797610379236
- Harrewijn, A., Van Der Molen, M. J., Van Vliet, I. M., Tissier, R. L., & Westenberg, P. M. (2018). Behavioral and EEG responses to social evaluation: A two-generation family study on social anxiety. NeuroImage: Clinical, 17, 549–562. https://doi.org/10.1016/j.nicl.2017.11.010
- Iannetti, G. D., Salomons, T. V., Moayedi, M., Mouraux, A., & Davis, K. D. (2013). Beyond metaphor: Contrasting mechanisms of social and physical pain. Trends in Cognitive Sciences, 17(8), 371–378. https://doi.org/10.1016/j.tics.2013.06.002
- Kross, E., Berman, M. G., Mischel, W., Smith, E. E., & Wager, T. D. (2011). Social rejection shares somatosensory representations with physical pain. Proceedings of the National Academy of Sciences, 108(15), 6270–6275. https://doi.org/10.1073/pnas.1102693108
- Liebowitz, M. R. (1987). Social phobia. Modern Problems in Pharmacopsychiatry, 22, 141–173.
- Ma, D. S., Correll, J., & Wittenbrink, B. (2015). The Chicago face database: A free stimulus set of faces and norming data. Behavior Research Methods, 47(4), 1122–1135. https://doi.org/10.3758/s13428-014-0532-5
- Maslow, A. H. (1981). Motivation and personality. Prabhat Prakashan.
- Mischkowski, D., Crocker, J., & Way, B. M. (2016). From painkiller to empathy killer: Acetaminophen (paracetamol) reduces empathy for pain. Social Cognitive and Affective Neuroscience, 11(9), 1345–1353. https://doi.org/10.1093/scan/nsw057
- Nieuwenhuis, S., Aston-Jones, G., & Cohen, J. D. (2005). Decision making, the P3, and the locus coeruleus--norepinephrine system. Psychological bulletin,131(4), 510.
- Pearson, R., Koslov, S., Hamilton, B., Shumake, J., Carver, C. S., & Beevers, C. G. (2018). Acetaminophen enhances the reflective learning process. Social Cognitive and Affective Neuroscience, 13(10), 1029–1035. https://doi.org/10.1093/scan/nsy074
- Price, D. D. (2000). Psychological and neural mechanisms of the affective dimension of pain. Science, 288(5472), 1769–1772. https://doi.org/10.1126/science.288.5472.1769
- Quarmley, M. E., Nelson, B. D., Clarkson, T., White, L. K., & Jarcho, J. M. (2019). I knew you weren’t going to like me! neural response to accurately predicting rejection is associated with anxiety and depression. Frontiers in Behavioral Neuroscience, 13, 219. https://doi.org/10.3389/fnbeh.2019.00219
- Rainville, P., Duncan, G. H., Price, D. D., Carrier, B., & Bushnell, M. C. (1997). Pain affect encoded in human anterior cingulate but not somatosensory cortex. Science, 277(5328), 968–971. https://doi.org/10.1126/science.277.5328.968
- Randles, D., Kam, J. W., Heine, S. J., Inzlicht, M., & Handy, T. C. (2016). Acetaminophen attenuates error evaluation in cortex. Social Cognitive and Affective Neuroscience, 11(6), 899–906. https://doi.org/10.1093/scan/nsw023
- Rawlins, M. D., Henderson, D. B., & Hijab, A. R. (1977). Pharmacokinetics of paracetamol (acetaminophen) after intravenous and oral administration. European Journal of Clinical Pharmacology, 11(4), 283–286. https://doi.org/10.1007/BF00607678
- Schlaepfer, T. E., Strain, E. C., Greenberg, B. D., Preston, K. L., Lancaster, E., Bigelow, G. E., & Pearlson, G. D. (1998). Site of opioid action in the human brain: mu and kappa agonists' subjective and cerebral blood flow effects. American Journal of Psychiatry,155(4), 470–473.
- Slavich, G. M., Shields, G. S., Deal, B. D., Gregory, A., & Toussaint, L. L. (2019). Alleviating social pain: A double-blind, randomized, placebo-controlled trial of forgiveness and acetaminophen. Annals of Behavioral Medicine, 53(12), 1045–1054. https://doi.org/10.1093/abm/kaz015
- Smith, H. S. (2009). Potential analgesic mechanisms of acetaminophen. Pain Physician, 12(1), 269–280. https://doi.org/10.36076/ppj.2009/12/269
- Somerville, L. H., Heatherton, T. F., & Kelley, W. M. (2006). Anterior cingulate cortex responds differentially to expectancy violation and social rejection. Nature Neuroscience, 9(8), 1007–1008. https://doi.org/10.1038/nn1728
- Sun, S., & Yu, R. (2014). The feedback related negativity encodes both social rejection and explicit social expectancy violation. Frontiers in Human Neuroscience, 8, 556. https://doi.org/10.3389/fnhum.2014.00556
- Toussaint, K., Yang, X. C., Zielinski, M. A., Reigle, K. L., Sacavage, S. D., Nagar, S., & Raffa, R. B. (2010). What do we (not) know about how paracetamol (acetaminophen) works? Journal of Clinical Pharmacy and Therapeutics, 35(6), 617–638. https://doi.org/10.1111/j.1365-2710.2009.01143.x
- Van Der Molen, M. J., Harrewijn, A., & Westenberg, P. M. (2018). Will they like me? Neural and behavioral responses to social-evaluative peer feedback in socially and non-socially anxious females. Biological Psychology, 135, 18–28. https://doi.org/10.1016/j.biopsycho.2018.02.016
- Van Der Molen, M. J., Poppelaars, E. S., Van Hartingsveldt, C. T., Harrewijn, A., Gunther Moor, B., & Westenberg, P. M. (2014). Fear of negative evaluation modulates electrocortical and behavioral responses when anticipating social evaluative feedback. Frontiers in Human Neuroscience, 7, 936. https://doi.org/10.3389/fnhum.2013.00936
- Van Der Veen, F. M., Van Der Molen, M. J., Van Der Molen, M. W., & Franken, I. H. A. (2016). Thumbs up or thumbs down? Effects of neuroticism and depressive symptoms on psychophysiological responses to social evaluation in healthy students. Cognitive, Affective & Behavioral Neuroscience, 16(5), 836–847. https://doi.org/10.3758/s13415-016-0435-2
- Van Der Veen, F. M., Van Der Molen, M. W., Sahibdin, P. P., & Franken, I. H. (2014). The heart-break of social rejection versus the brain wave of social acceptance. Social Cognitive and Affective Neuroscience, 9(9), 1346–1351. https://doi.org/10.1093/scan/nst120
- Wager, T. D., Atlas, L. Y., Botvinick, M. M., Chang, L. J., Coghill, R. C., Davis, K. D., Yarkoni, T. (2016). Pain in the ACC? Proceedings of the National Academy of Sciences, 113(18), E2474–E2475. https://doi.org/10.1073/pnas.1600282113
- Whalen, P. J., Bush, G., McNally, R. J., Wilhelm, S., McInerney, S. C., Jenike, M. A., & Rauch, S. L. (1998). The emotional counting Stroop paradigm: A functional magnetic resonance imaging probe of the anterior cingulate affective division. Biological Psychiatry, 113(18), 1219–1228. https://doi.org/10.1016/S0006-3223(98)00251-0
- Younger, J., Aron, A., Parke, S., Chatterjee, N., & Mackey, S. (2010). Viewing pictures of a romantic partner reduces experimental pain: Involvement of neural reward systems. PloS One, 5(10), 10. https://doi.org/10.1371/journal.pone.0013309