
Abstract
Increased awareness, interest and use of assistive technology (AT) presents substantial opportunities for many citizens to become, or continue being, meaningful participants in society. However, there is a significant shortfall between the need for and provision of AT, and this is patterned by a range of social, demographic and structural factors. To seize the opportunity that assistive technology offers, regional, national and sub-national assistive technology policies are urgently required. This paper was developed for and through discussion at the Global Research, Innovation and Education on Assistive Technology (GREAT) Summit; organized under the auspices of the World Health Organization’s Global Collaboration on Assistive Technology (GATE) program. It outlines some of the key principles that AT polices should address and recognizes that AT policy should be tailored to the realities of the contexts and resources available. AT policy should be developed as a part of the evolution of related policy across a number of different sectors and should have clear and direct links to AT as mediators and moderators for achieving the Sustainable Development Goals. The consultation process, development and implementation of policy should be fully inclusive of AT users, and their representative organizations, be across the lifespan, and imbued with a strong systems-thinking ethos. Six barriers are identified which funnel and diminish access to AT and are addressed systematically within this paper. We illustrate an example of good practice through a case study of AT services in Norway, and we note the challenges experienced in less well-resourced settings. A number of economic factors relating to AT and economic arguments for promoting AT use are also discussed. To address policy-development the importance of active citizenship and advocacy, the need to find mechanisms to scale up good community practices to a higher level, and the importance of political engagement for the policy process, are highlighted. Policy should be evidence-informed and allowed for evidence-making; however, it is important to account for other factors within the given context in order for policy to be practical, authentic and actionable.
The development of policy in the area of asssitive technology is important to provide an overarching vision and outline resourcing priorities.
This paper identifies some of the key themes that should be addressed when developing or revising assistive technology policy.
Each country should establish a National Assistive Technology policy and develop a theory of change for its implementation.
Implications for Rehabilitation
Introduction
The aim of this position paper is to outline a broad framework for discussing the principles that should underlie assistive technology policies for application nationally or internationally. However, we will also consider aspects of strategy or action plans where such aspects are relevant to policy being realistic and achievable, across often vastly different contexts. gives our working definitions of assistive products, assistive technology systems and social exclusion; one of the major barriers that we argue can be over-come by assistive technology.
Table 1. Definitions of assistive products, assistive technology systems and social exclusion.
The difference between policy, strategy and action plans is often not clear, and these terms are used in different and often over-lapping ways in the literature. summarizes how we use these terms. Based on our engaging with the literature and our experience of working with a range of stakeholders on these issues, we suggest these are the most parsimonious and useful ways of distinguishing between these terms.
Table 2. Defining and differentiating policies, strategies and action plans.
It is also important to understand the role of legislation in relation to these processes. Legislation refers to statutory law; meaning laws that have been approved and enacted by the governing body of a country – the government. This may also require establishing State institutions to ensure that the law is practised in the way intended and that it has the anticipated results. If it does not, then it may require legislative revision. Sometimes advocacy groups may undertake strategic litigation, where they take a specially selected case (which is often representative of the experience of many people) to court in order to show that the law is unfair and, therefore, attempt to change the law. Alternatively, a local authority may have established a policy concerning an assistive technology system and citizens may have come to rely on this service; but if it is not legislated for, there may be nothing stopping the local authorities withdrawing the service at some future point.
The relationship between policy, strategy and action plans should be one of "cascading": both operationally (how things are done), locally and regionally; ensuring that there are effective mechanisms for national policies to successfully work in often quite different subnational contexts. This may mean that the same things are done in somewhat different ways and perhaps by different organizations, groups or individuals, in different places. Depending on the context, the policy may need to be flexible enough to foresee diverse ways of achieving the same ends, so that citizens can achieve the rights legislated for in their country’s law.
International policies, strategies and action plans on assistive technology
Assistive technology was first introduced in international policies through the Standard Rules on the Equalization of Opportunities for Persons with Disabilities [Citation3], and was further entrenched into international policies with the advent of the Convention on the Rights of Persons with Disabilities (CRPD) [Citation4]. The Incheon Strategy “Make the right real” is an example of a strategy that includes the provision of assistive technology as an important means to achieve disability-inclusive development [Citation5]. The World Report on Disability [Citation6] has highlighted the need for action to improve the provision of assistive technology globally, and this has been reiterated in the Global Disability Action Plan 2014–2021 [Citation7]. Similarly, the Global Strategy and Action Plan on Ageing and Health 2016–2020 [Citation8], recognizes the vital role of assistive technology.
In the Standard Rules, one of the four rules on preconditions for equal participation requires States to ensure the development and supply of assistive products to assist people with disabilities to increase their level of independence and to exercise their rights. As important measures to achieve the equalization of opportunities, States should ensure the provision of assistive products according to the need. Besides supporting the development, production, distribution and servicing of assistive products, States are to support the dissemination of knowledge about them. States should also recognize that all who need these products should have access to them, which includes financial accessibility. Assistive products should be provided free of charge or at such a low price that people requiring AT or their families can afford them. Moreover, States should consider requirements of girls and boys concerning the design, durability and age-appropriateness of assistive products [Citation3].
In contrast to the general approach of the Standard Rules, the CRPD is more selective in mentioning assistive technology as a measure that States should take to promote, protect and ensure the full and equal enjoyment of all human rights and fundamental freedoms. However, assistive technology measures are not included – at least not explicitly – in all relevant CRPD articles. Despite this limitation, the principles of Article 3 on non-discrimination, equality of opportunity, and equality between men and women, as well as Article 5 on elimination of discrimination on the basis of disability, infer that States are to ensure that all people, irrespective of disability, gender and age, have access to affordable assistive products [Citation9].
It is also important to note that accessibility (of which access to assistive technology is a part) is a precondition to the enjoyment of other rights. The CRPD Committee’s second General Comment was on Article 9: Accessibility [Citation10]. It stresses the interrelation of this right with other rights and articles (e.g., Articles 9, 19, 21, 28.2a, 26.3). The Comment asserts that “Accessibility” is related to groups, whereas reasonable accommodation is related to individuals. This means that the duty to provide accessibility is an “ex-ante” duty; meaning that it must be provided before the fact of it becoming a problem – States must ensure accessibility, ‘up front’ as it were.
The recent Report of the Special Rapporteur on the rights of persons with disabilities (2017), while broader than assistive technology, also describes how to provide rights-based support and assistance to persons with disabilities, in consultation with them. The CRPD also indicates that rehabilitation services (including assistive technology) should be provided as close as possible to where people live (Articles 26.1b, 25c). This is important for smaller countries, particularly small island countries, which may not have assistive technology production capacity. In such situations, other mechanisms need to ensure adequate procurement sources. Finally, it is important to note that the responsibility of States that have ratified the CRPD to ensure affordable provision of assistive technology is not limited by country borders. Through Article 32 on international cooperation, States commit to both technical and economic cooperation on assistive technology.
Assistive technology policy and international development
It is important to position assistive technology policy within the broader context of international development generally as well as more specific policy innovations, and conventions should be directly relevant to people with a range of impairments, including the aging population, who may benefit from the use of assistive products. The Sustainable Development Goals [Citation11] is a set of 17 goals, internationally agreed-upon, that will guide international efforts across all countries to target their development efforts to ensure that “nobody is left behind”. Recently Tebbutt et al. [Citation12] have illustrated how the achievement of each of these 17 goals can be facilitated through the incorporation of assistive technology, at the population level, when planning to reach these goals. Assistive products can be conceived as both mediators of social change (i.e., as a mechanism social change works through) and as moderators of that change (as a factor that determines the extent of the change, particularly whether it reaches the more marginalized and vulnerable groups in society).
Within this context a global increase in awareness of the need for quality, affordable, and reliable assistive products is evident. The World Health Organization (WHO) has coordinated a collaborative effort through the Global Collaboration on Assistive Technology (GATE) to maintain Assistive Technology at the forefront of global and sustainable developments. The remit of GATE necessitates that it is relevant to all people who experience impairments in whatever realm and at any age: this includes, for example, people with non-communicable diseases, injury, visual or hearing loss, mental health conditions including dementia and autism, gradual functional decline, or frailty. As such, assistive technology has an important role to play in promoting access to education, employment, justice, health and wellbeing; as well as to the broader cross-cutting values of promoting social inclusion and participation, independence and autonomy (or chosen interdependence) and leading a dignified and consequential life. Assistive technology cuts across all sectors and ages, and it is paramount that policy initiatives recognize and reflect this, rather than seeking to silo it. This presents policy makers with the significant challenge of providing a fully integrated system that is capable of delivering at the population level, while at the same time providing specific assistive technology that matches to the particular needs of individual users (namely the Matching Person and Technology (MPT) Model [Citation13] or the Human Activity Assistive Technology Model [Citation14]).
We are living in a rapidly changing world due to the digital revolution that is not only changing the way people live, learn, produce and even think; but also changing decision-making processes, the way information is delivered, problems are solved and policies are developed. This also makes the distinction between high- and low-tech assistive products increasingly blurred, and has the potential to reduce price barriers to high tech solutions. From a systems perspective the digital revolution should be seen as a resource for AT user empowerment and participation in reaching the SDGs, whilst also being careful to avoid the risk of a wider digital and technological divide by not incorporating these opportunities systemically [Citation15].
Khasnabis et al. [Citation1] have outlined some of the key components that need to be addressed in the Assistive Technology system and the Commentary paper in this special issue [Citation16] describes the principal P’s that should also be considered in policy development. To avoid overlap, we therefore refer the reader to the MacLachlan and Scherer paper [Citation16] which should be read in conjunction to this policy paper, particularly for examples of a systems thinking perspective in Assistive Technology.
Policy gaps
Different types of gaps exist in a number of areas relevant to policy development in this field. This includes, the identification of short and long-term evidence that would be useful for policy making, the use of existing data and information within policy, fostering policy development in an inclusive manner, the evaluation of existing policy according to human rights and social inclusion criteria, the implementation of policy, and its monitoring and evaluation by an appropriate range of stakeholders, especially the consumers and users of such technology. Very often policymakers – including in the health and welfare sectors – are not familiar with disability, impairment or assistive technology issues, and are, therefore, not aware of some of the policy challenges in this area, including the significant challenge of cross-sectoral working [Citation17].
In many countries, the first step in creating inclusive policy for assistive technology will be to connect different communities with an interest in assistive technology; to encourage sharing experiences and best practices, and to simply become aware of stakeholders already working in this field – from various international organizations, governments, academics, data experts, standardization bodies and of course civil society organizations. There are very different ways to build this community, and the community will be strongest if a thorough mapping process to establish existing formats, technologies and stakeholders is undertaken. Stakeholders who are often overlooked in these processes may include (but are not limited to), self-advocates for the independent-living movement, Indigenous peoples in countries where their inclusion is often marginalized, rural people – especially women and girls – in poorly resourced settings; people with intellectual disabilities [Citation18] for whom assistive technology may be especially beneficial for community living [Citation19], refugees or internally displaced people.
In the APODD (African Policy on Disability and Development) project [Citation17], three types of policy gaps were identified: A Policy Awareness Gap – where policy makers knew little about disability-specific policy instruments (e.g., CRPD), and disability representatives knew little about the policy instruments used in mainstream international development. There was also a Policy Process Gap, even where there was consultation with Disabled Peoples Organisations (DPOs), the final version of documents rarely reflected their primary concerns. A third gap, a Policy Implementation-Monitoring Gap, was also noted, where there were a lack of explicit indicators for monitoring and evaluation, that were disaggregated by disability, or had disability specific concerns. We anticipate that many of these gaps will also be apparent for the users of assistive products. For instance, Gowran et al. [Citation20] give an example of the policy gap that exists in the provision of wheelchair and seating assistive technology in Ireland; highlighting the need for greater awareness of those more distant from service provision, for example, policy makers. They also indicate the process gap across a number of facets of assistive technology systems – for example, when accessing services, assessing and delivering services, tracking, tracing and taking care of assistive technology; providing education for all and advancing research.
illustrates a simplified conceptualization of the primary components involved in policy development and implementation. While some models suggest an idealized linear sequence; again this is rarely our experience, with the components often being combined in non-ideal, time-limited and resource-constrained circumstances, substantially funnelled through the needs of local contexts and settings. Each of these components should nonetheless be addressed through inclusive policy development and implementation processes [Citation21].
Figure 1. Components of the policy process (reproduced by permission [Citation21]).
![Figure 1. Components of the policy process (reproduced by permission [Citation21]).](/cms/asset/3d42fb4b-8f93-4aeb-bb19-088ac14ead9a/iidt_a_1468496_f0001_c.jpg)
Engaging in policy often requires understanding the triggers for policy change, or renewal. While the CRPD and other international policies may well set the context for a discussion on assistive technology policy; such instruments on their own are rarely sufficient to propel government towards policy work. So what sort of argument may engage the attention of government and policy makers? Evidence concerning the social, economic and wellbeing benefits, and impact, of assistive technology, may be especially persuasive. The widespread fragmented delivery of services, which are often mainly reactive, with many silos, and often with many specialists in the “supply chain”, is a very costly way to provide a service. Thus, arguments addressing the need for improved efficiency may be relevant. With the increasingly emphasis on person-centeredness, on co-design and on user-led initiatives; it may also be argued that the ethos of the assistive technology sector, is out of kilter with government policy elsewhere, and, therefore, serves to diminish its coherence and overall effectiveness.
It is also crucial not to underestimate the challenges of producing good policy in this domain. For instance, policy has to be across all sectors, in the same way that people live across all sectors. It also needs to consider the whole-life-span approach to people’s lives. These are both difficult for government, requiring cross-ministerial work and for government to commit to long term planning, which may not be expedient for shorter-term political gain. More generally, for governments to have a policy on AT, it has to be made clear that it is all AT i.e., everything from walking sticks to digital health; and this also fits in with holistic and person-centred care and support. However, policy is often most influenced by financial rewards for doing something, or financial penalties (through prosecution or reputational damage) for not doing something. The economic case for assistive technology, therefore, needs to be strengthened and is perhaps one of the most important change factors for improving assistive technology systems. The economic case will be made most emphatically when there is evidence of the effectiveness of assistive technology at the individual, community and Sate/national levels; and so research, monitoring and evaluation has to target these different levels in ways that allows for the findings to be integrated meaningfully.
Empowering people
While it is people who empower people, assistive technology can contribute to creating the conditions where this is possible. The CRPD promotes the rights and perspectives of people to be central to policy development. A critical route to empowerment is the establishment, by States, of mechanisms for DPO (Disabled People’s Organisations) engagement in policy development, monitoring and evaluation. Articles 4–3 of the CRPD obligate State to actively consult with DPOs in decision-making. DPOs can help orient priorities, provide inputs on what works and what does not, and suggest and provide strategies to reach out to persons with disabilities. This is critical to ensure the view of users is considered and that the assistive technology policy is grounded in a rights-based approach that truly empowers them.
In addition to Articles contained within the CRPD, research suggests that around a third of assistive products that are provided may go unused; providing a powerful pragmatic and economic argument for AT user involvement and training. In other contexts, this perspective, most recently referred to as PPI (“public and patient involvement”) recognizes that public participation enhances the design and delivery of better services [Citation22]. Research also indicates that the greater the extent to which such participation is formalized in established structures, the more satisfactory are the results [Citation23].
This presents policy makers with an intriguing contradiction. If policy development or reform is to effectively address the needs of those who have been marginalized by mainstream society (and previous policy), then such processes need to be explicitly disruptive – meaning they need to explicitly change the structures that oppress and marginalize. Structures in the process of policy reform need to be established to “institutionalise disruption” (see [Citation21]). This may mean, for instance, re-imagining systems for the delivery of assistive products, it may mean the development of a new cadre working across a range of assistive products; it may mean self-assessment for some assistive products. Stronger user involvement in the policy process also presents the opportunity to potentially uproot and transform prevailing power structures that may, by design or default, be perpetuating a lack of access to assistive products.
Our overarching schematic of the strategic issues for assistive technology systems depicts the interlocking areas of People, Place, Pace, Personnel, Products, Provision and Policy; it is presented in .
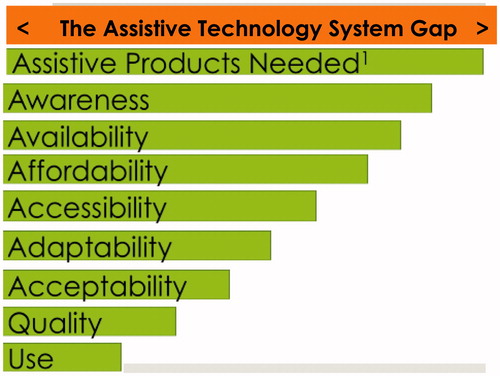
Progressive bridging of the assistive technology system gap
We base our conceptualization of access on the General Comment of the United Nations Committee on Economic, Social and Cultural Rights (2000), and we then apply this to the assistive technology systems in a country. According to the General Comment a State should have policies and programs that promote the availability (sufficient quantities), accessibility (both physically, economically and in terms of provision of information), acceptability (culturally, socially, gender and age appropriate), adaptability (appropriate to local contexts) and quality (in terms of safety, efficacy and usability and being evidence-based) of assistive products and services. These criteria – known as the “AAAAQ” – should also be adopted with regard to the rights of participation, accountability and transparency, in their performance. We also supplement this with two additional, and crucial, “A”s for assistive technology. The first additional A – Affordability – is so crucial for this sector that it needs to be unpacked from the concept of Accessibility more generally. Second, many people with functional impairments, particularly (but by no means only) in resource poor contexts, are simply not aware that many impairments that may be alleviated, or overcome, by the use of assistive technology. In fact, this applies not just to potential users but also to health and social care personnel in resource rich and poor areas. Thus, Awareness is the second addition, as a key moderator of access to assistive technology.
illustrates our understanding of how the real gap between the need for and provision and use of appropriate assistive products should be unpacked and understood in terms of access.
Figure 2. A schematic representation of Assistive Technology System gaps. 1Note this bar chart is not to scale – globally the number of assistive products needed far exceeds those available; sometimes by a ratio of 10 or more to one, and this is patterned by socioeconomic factors, marginalization and so on.
Consistent with the CRPD which promotes “progressive realization” (while all rights may not be achievable immediately, States should be able to show that they are on a path to their realistic achievement), we recognize that policy should also adopt this principle (re Pace, discussed in Scherer et al. [Citation16]; along with and recognition that “domestication” of best practice (as with the CRPD) may play out differently, in different contexts (refer to Place, as discussed in Scherer et al. [Citation16]). However, it is clear that disability and access to assistive technology is often heavily gendered; with girls and women often having less opportunity to access it; which may also reflect other inequities regarding wealth, age, ethnicity or geography (e.g., remote and rural areas). So, while progressive realization and domestication may result in variations between countries, it is very important that these do not reinforce general practices of discrimination, towards girls, and women, as a particular example.
A systems-thinking perspective (see [Citation16]) also requires taking a long-term view of the Assistive Technology system. Responding to the assistive technology needs of people is not a single step process that finishes as soon as the person has an appropriate solution. Rather, delivering on Assistive Technology involves supporting people over a longer period in their developing new or associated technology needs. The participation of empowered Assistive Technology users in sectors such as education and employment is highly desirable, as well as their political and cultural participation, but policy makers should be aware that those sectors need to be prepared to welcome the participation of all. At micro-level, this means carefully managing change. At the macro-level, Assistive Technology provision should be seen as a crucial part of wider efforts to build a more inclusive society.
Good practice in assistive technology systems: a country case study of Norway
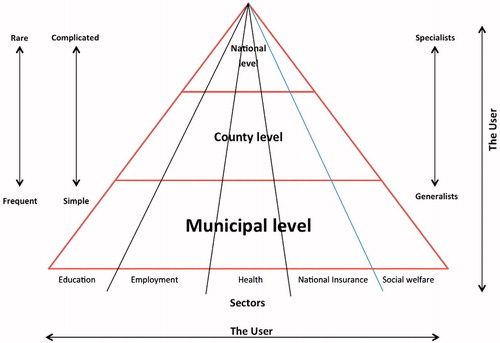
Sund [Citation24] has described the Norwegian Assistive Technology model, established in 1995. Its primary objectives included (1) establishing a unified, national system for assistive technology, (2) addressing users’ practical/functional daily problems regarding the AT they used, (3) giving the users rights in law to necessary and appropriate assistive products, free of charge, (4) providing users with the same level of services regardless of where they live, (5) establishing a common ICT system for registration of purchases, distribution, repairs, regular servicing and refurbishment of assistive product, and (6) user involvement in the system and a focus on the individual strongly emphasized. To facilitate this structurally, Norway established 18 assistive technology centres (hereafter denoted AT centres) – one in each county (administrative area) of the country. Each AT centre coordinates assistive technology activities within their county, and cooperates closely with the local health and rehabilitation services, in order to address the users` practical/functional daily problems (see also, Nordic Cooperation on Disability Issues [Citation25]).
Importantly, it is the local authorities (the municipalities) that have the fundamental responsibility for health care, and social and rehabilitation services; including the provision of assistive products. Trained personnel (usually occupational therapists or physiotherapists) are responsible for identifying and assessing the users` needs, recommending and providing assistive products, as well as following up the user`s situation in daily life.
If appropriate rehabilitation or health care services are not available in the local community, the individual will be referred to the AT centre in their county. These centres are centres of excellence serving as a referral system covering the whole county and they give services and guidance within mobility, hearing, vision, communication, cognition and the environment. The AT centres have personnel (such as occupational therapists, physiotherapists, technicians/engineers, speech therapists, opticians) with expert knowledge about the application and adaptability of assistive products. They give guidance to the local authorities and other stakeholders in the county. More local community authorities ask for assistance from the AT centre if the local network does not have sufficient expertise. In some cases, the municipalities and AT centres cooperate with retailer or suppliers of assistive products in order to solve the user`s practical/functional problems. This helps to ensure that users see professionals with the same expertise and are given the same level of service regardless of where they live.
Within the overall national AT system, there are also some national competence centres with distinct areas of expertise that also can be called upon by county AT Centres. Based on national agreements with the retailers and/suppliers, AT centres purchase assistive products and distribute them to the different municipalities. They also repair the assistive products when needed, and do regular servicing of electro-medical assistive devices at given intervals. Interestingly, in terms of sustainability, about one-third of the distributed assistive products are refurbished ones. These recycled products have had worn parts replaced and the assistive products are cleaned properly and should be “as new” before being provided to a new user. The AT centres organize and run yearly training courses on assistive technology for employees in the municipalities and hospitals. There is a considerable emphasis on the assistive products being be safe to use. highlights some relevant statistics regarding the Norwegian AT system, as of 2016.
Table 3. Some attributes of the Norwegian Assistive Technology System (see [Citation26]).
While Norway is a comparatively very rich country, its systematic-tiered approach to assistive technology is noteworthy, and its commitment to recycling a significant proportion of its assistive products – or their components – also demonstrates a strong commitment to cost-saving. These and other aspects of its geographically inclusive approach may well be relevant to many more poorly resourced policy contexts.
Areas with different resources may be able to recycle in different ways. So, in the case of wheelchairs, reusing a wheelchair means that it has been cleaned with minor repairs and issued for reuse; refurbishing means that the wheelchair has been completely revamped to “as good as new” condition, ready for reissue; while recycling a wheelchair mean taking it out of commission and recycling the materials and parts. Policy may indicate the need for, and prioritize the resources for, some or all of these; and seek to achieve them in a systemic way. Allowing them to occur in an ad hoc manner is not likely to be the most efficient use of resources at a national level.
Some dimensions of assistive technology policy: results of a stakeholder consultation
Scholl and MacLachlan [Citation27] undertook a literature review, a focus group with WHO regional representatives, Key Informant interviews and three country case studies through in-country interviews and document analysis (in South Africa, Philippines and PDR Laos). They sought to identify what people felt were important elements to include in the development of a framework to support countries in developing national assistive technology policies. Their specific aim was to explore the relevance of policy themes used in the ground-breaking and now well established WHO Essential Medicines List, which has the aim of making essential medicines more accessible, globally. This aim is, therefore, cogent to the Priority Assistive Products List (APL). The research also addressed facilitators and barriers for the AT sector across these different settings. summarizes the themes that arose from this research.
Table 4. Possible elements of, facilitators for and barriers to, the development of national assistive technology policies.
Policy in low- and middle-income countries
It is important to say that many of the critical issues for assistive technology policy are similar in high-, middle-, and low-income contexts; thus the challenges in are common. However, in poorly resourced contexts, there are often additional challenges. As assistive technology presents opportunities to address social exclusion, the allocation of resources in poorer settings is crucial. Our definition of social exclusion () stresses the “lack or denial of resources, rights, goods and services, and the inability to participate” and goes on to state that this lack or denial of resources affects “equity and cohesion of society as a whole” [Citation2]. Generally, in low- and middle-income countries (LMIC), the provision of assistive products is inadequate with poorly structured systems in place to aid service delivery [Citation28,Citation29]. We have found that policy development in such contexts – and often in higher-income contexts too – frequently excludes its intended beneficiaries, and may indeed be undertaken by consultants unfamiliar with the country in question, and with reference points related to contexts with much greater resources. Wazakili et al. [Citation30] in their study of inclusion of persons with disabilities in poverty reduction strategy processes (PRSPs) in Malawi found that they often had limited knowledge about the PRSP process, which partly accounted for their limited participation in policies that are geared towards poverty alleviation.
Figure 3. The Norwegian Assistive Technology System model: 18 Assistive Technology Centres, one in each county, cooperate closely with the health care and rehabilitation services at the municipal level.
In some countries, the situation is poor – there is a negligible assistive technology industry and/or few professionals to provide appropriate technologies. Where assistive products are available, they are often unaffordable to the majority who could benefit from them. Cheaper assistive products, when they are available, are often of poor quality, poorly adjusted and serviced, or inadequately explained, and thus difficult and off-putting to use [Citation31].
Articles 4 and 26 of the Convention make it clear that ultimately, governments are responsible to ensure that appropriate assistive technology is available and affordable and that provision is made for users to be trained to use assistive products [Citation29,Citation31].
Recently both the South African National Departments of Health and Social Development have drawn from the CRPD to develop the white paper on disability and rehabilitation framework strategy. Both documents put emphasis on the importance of available and affordable assistive technology for persons with disabilities [Citation32]. Yet other research in South Africa suggests that the failure to effectively implement the health and rehabilitation articles of the UNCRPD is largely due not only to negative attitudes in society in general [Citation32] but also from government officials and service providers towards people with disabilities [Citation33] and a rights-based approach. This certainly incorporates most people who use assistive products. Fundamentally then, it is not only improved “systems” but also changed organizational, societal, religious and cultural attitudes that are necessary to improve access at the systems and policy level. However, it may be that the actual use of assistive products can itself change attitudes in a positive way. In Bangladesh Borg et al. [Citation34] found that people using assistive products were about three times more likely to report positive attitudes from neighbours, than did people with similar impairments who did not use assistive products.
Although stigma towards disability is a worldwide problem, it is important to stress that in all cultural and economic contexts there are valuable resources that can be harnessed to promote assistive technology systems. For instance, in Africa, AfriNEAD ((the African Network for Evidence to Action on Disability) see [Citation35]) represents a ready vehicle to promote policy dialogue on assistive technology. Cultural resources such as the Ubuntu philosophy of collective support and harmony can be a facilitative context in which to develop supportive and empowering services and opportunities [Citation36]. Of course the Ubuntu ethos can be found in context elsewhere too: engaging key stakeholder to reflect and work collectively; to share understanding as a community of practice for sustainable development in AT and other support services [Citation20,Citation37].
The importance of assistive technology for the ageing population is now being recognized globally and even in resource-rich countries it is a significant challenge. For instance, a systematic review of “intelligent assistive technology” (IAT; meaning more technologically sophisticated) for dementias found that while the IAT spectrum continues to expand rapidly, in volume and variety; many structural limitations to successful adoption persist. These include insufficient clinical validation and insufficient focus on potential user’s needs; and this even in comparatively very wealthy countries. In poorer contexts, such as Puerto Rico, Hispanic older adults with functional limitations living independently, were found to have unmet assistive technology needs; particularly to compensate for physical limitations and to increase safety performance, mostly around instrumental activities of daily living [Citation38].
Access to assistive technology continues to be a problem, often especially so in rural areas. In rural China, this has also been reported along with the barrier that “vague and complex regulations” constitute their use [Citation39]. For many countries with quite rapidly aging populations, these challenges will have to be quickly and systemically addressed by resources being provided on the basis of well-articulated policy. The focus of much recent innovation and developments in assistive technology has been on high tech solutions and whilst appropriate there is probably a greater need for more low tech affordable assistive technology products for safety and instrumental activities of daily living. There are also advantages of scale in addressing the accessibility of the environment in community, workplace and public settings, through dropped curbs, ramps, lifts and handrails and communication (e.g., hearing loops).
Assistive technology across the life course
In some countries, 46% of people with disabilities are older people (aged 60 or over; https://www.un.org/development/desa/disabilities/disability-and-ageing.html). The proportion of people with disabilities who are in this older group is likely to increasing in most countries, in coming years. This being the case it will be important for assistive technology policy to adopt a life-course perspective. This should reference to global movement for older people and their work in advocating for better services, including assistive technology. Older People’s Associations (OPAs) and Disabled People’s Organisations (DPO’s) could perhaps have greater impact on assistive technology policy and provision by working more closely together; and this is something that can be promoted through the process policy development [Citation21].
From a life course perspective, we see moments along the course of our lives where we need to access assistive technology, not only for permanent use but also short term; and so policy needs to cater for these different types of scenarios and needs. The life course perspective also embraces the need for such policy to be cross-sectoral – for instance, across education, employment and health. Seeing the assistive technology implications of disability, or chronic illness, along the life course, also recognizes that assistive technology research and practise will have to develop a much stronger population science ethos; rather than being siloed in rehabilitation, with another silo in disability, another in education, and so on. This surely is the crux of the policy challenge to social inclusion at the population level.
The economic case for investing in assistive technology
Improved functioning from the use of assistive technology may have wide ranging positive economic impacts on individuals and society. As discussed below, the economic benefits stem from improved health outcomes and quality of life, better education and employment outcomes, and higher productivity. These benefits could translate into a reduction in the health and social care costs associated with impaired functioning. More broadly, the benefits of assistive technology may also extend to a stronger labour supply and industry development, which would benefit the economy as a whole.
Assistive technology has been shown to improve health outcomes and quality of life for people in need, and for care givers. This includes comparative improvements in overall health reported by users of wheelchairs [Citation40], quality of life and physical health among hearing aids users [Citation41–43]; and better quality of life and reduced symptoms of depression among nursing home residents who used spectacles [Citation44]. Evidence also shows slower functional decline and higher likelihood of maintaining independence among older people living with a disability who received assistive products and home modification [Citation45]; positive health and social effects from an accessible home environment among people with functional limitation [Citation46]; as well as positive impacts of assistive products on children with physical impairments and their caregivers [Citation47]. A systematic review by Chase and colleagues found that AT and home modifications along with other interventions prevented falls among community-dwelling older adults [Citation48] (see also Cho et al. [Citation46]).
Evidence suggests that improved health outcomes could reduce healthcare and social care costs. For example, Bensi et al. [Citation49] reported savings of €290,000 per person, over a 5-year period because of increased autonomy, reduced dependence on personal assistants and improvement in quality of life through greater control of living spaces through home adaptation, mobility and living aids, and other AT interventions. The Disability Federation of Ireland and Enable Ireland [Citation50] also found comparable annual savings of €59,000 per person, following the provision of environmental control technologies at home. Likewise, Barnard [Citation51] demonstrated that AT can result in 45% lower costs for funding authorities in a single year.
Assistive technology also has an important role to play in keeping people living in their own homes, in their own communities. In reviewing investment to allow older people to remain living within their own homes Snell, Fernandez and Forder [Citation52] found that equipment and adaptations led to reductions in the demand for other health and social care services worth on average £579 per recipient, per annum. Such services lead to improvements in quality of life of the person, which they estimated to be worth £1522 per annum in reduced service requirements. Based on an estimated average scenario and a client base of 45,000 individuals receiving interventions at a total cost of approximately £270 million, it is likely to generate reductions in the demand for health and social care services worth £156 million, over the lifetime of the equipment, and to achieve quality of life gains costed at £411 million [Citation52].
The provision of assistive technology could confer positive impacts on existing and future workforce. The impact could be as direct and immediate as returning a person to work by providing a prosthetic limb and rehabilitation; or improving the vision of workers by providing corrective lenses. For example, workers with poor vision in Rwanda, not wearing glasses, were three times more likely to be asked by supervisors to repeat their work of sorting coffee beans, than after receiving and wearing glasses [Citation53]. Importantly, assistive technology also helps with laying the foundation for a stronger future workforce through increasing levels of education and better education outcomes. Earlier fitting of hearing aids contributes to better language, academic and social outcomes in children [Citation54]. In China, the provision of free glasses to children with short-sightedness was found to improve their performance on mathematics test to a statistically significant degree [Citation55]. These are important mediators for building skills for the future workforce.
The cost of retaining an employee who acquires a disability is considerably less than the cost of hiring and training new employees. Work Without Limits [Citation56] suggest that such costs range from $3000 to $22,000 depending on the seniority of the post, considerably higher than the average $500 spent on accommodations. Parry [Citation57] notes “the average cost to accommodate an employee with a disability is $500, the benefits can be substantial: employees with disabilities are five times more likely to stay on the job than their counterparts without a disability. That translates into less money and time spent hiring employees.” Work Without Limits [Citation56] suggest that 46% of reasonable accommodations at work cost absolutely nothing; with another 45% having a one-time cost, typically around $500. They also assert that employees with disabilities often exhibit high retention rates, which can translate into financial savings for employers.
The assistive product market is set to greatly expand in the near future, fuelled by population growth and increased longevity, as well as advances in technology. For example, the global market for assistive products for the elderly and people with disability was valued at US$14.1 billion in 2015. By 2024, the market is estimated to reach US$26.0 billion, corresponding to a compound annual growth rate of 7.4% between 2016 and 2024 [Citation58].
In many countries, domestic markets for assistive products and related industries are relatively new and awaiting further development. Developing local industry could not only serve to meet the local demand at an affordable cost, but also to provide opportunities for job creation through enhancing local technical capability and innovation. Furthermore, like other industries, the benefits would have positive spillover effects to the broader economy along the value chain of the primary (raw materials), secondary (manufacturing) and tertiary (service) sectors. The potential of the sector has been noted by some governments and has been incorporated into their economic development plan. For example, the State Council of the People’s Republic of China has issued a plan to foster “innovation capability, industry upgrade, effective market supply and a favourable market environment, to enhance industry development”, with a view to generating outputs of more than ¥700 billion (US$103.3 billion) from the rehabilitation and assistive products industry [Citation59]. Other examples include the emerging hearing device manufacturing sector in a number of countries, including India, Brazil and Thailand [Citation60].
The argument for the growth of the assistive technology industry within countries may be persuasive for policy-makers, and in capturing parliamentary interest. At the First Global Assistive Technology Conference in Beijing (2014) (http://www.ispoint.org/events/global-conference-assistive-devices-technology-industry), the Heads of State from China and Germany were present to testify to their country’s support for and interest in assistive technology; this was also clearly demonstrated by the strong presence of manufactures form both countries at the accompanying EXPO trade fair. The Second Global Assistive Technology Conference, Beijing 2017, explicitly linked assistive technology to China’s ambitious “Belt and Road” initiative; for increasing its trade and cultural links with Asia, Africa and Europe. Such initiatives have highlighted the importance of policy addressing market shaping. Market shaping in the assistive technology context refers to engaging market factors with social equity; balancing these to allow genuine need due to impairment to develop into reliable demand for assistive products, and for affordable and quality supply to embrace social gain, as well as financial profitability [Citation61].
Another relevant policy issue is that many assistive technology products are viewed by States as medical devices and are subject to rigorous legislative requirements or subject to particular standards (for instance, as approved by the International Standards Organization, ISO). Whilst this may be appropriate in many circumstances, it can be restrictive for access in other contexts, where in particular some lower-tech solutions may be more realistic, more affordable and more likely to be effectively maintained. Standards may, therefore, need to be more dimensional than absolute, with of course minimum standards to ensure safety and the prevention of harm to users. Onerous legislative requirements also drive up cost, time to development and can be off putting to investment by innovators and industry; thus reducing availability and affordability.
A final and often neglected aspect of assistive technology economics is that many types of assistive products can help increase productivity for those that are not living with a disability – leading to wider application of current technologies and, therefore, increasing economic benefits. Indeed, mainstreaming accessibility and various forms of assistive technology within existing products is a key focus for many of the leading technology companies today. So for instance Apple’s development of Siri or Microsoft’s eye-gaze technology are examples of assistive technologies that have gone mainstream and can contribute to everybody’s productivity and quality of life.
The role of active citizenship
The full and active participation of civil society – in particular DPOs as organizations representing a diversity of users of assistive technology – is important in order to authenticate the policy process. We highlight three issues where civil society has an especially important role. Access to relevant information for all social actors in a timely and accurate way is crucial. In particular, with regard to persons with disabilities, it is necessary to ensure that information can be provided in accessible and alternative formats, in order to promote the full and effective participation of this group. Civil society is often the provider of accessible formats; such as through screen readers, screen magnifiers, or text to speech devices; but also formats not necessarily provided by technology, such as Easyread or Sign Language.
Capacity building programs in areas such as human rights advocacy, leadership and awareness raising, designed for and usually run by civil society organizations, are critical in enabling people with disabilities, DPOs and NGOs, to claim rights and develop focused campaigns on achieving them. Policy needs to identify channels for how this activity can contribute to policy development and implementation. Without providing such channels, and legitimizing this activity, rights claimers are placed on the ‘outside’, and can be seen as negative and critical of government, when in fact they are advocating for internationally agreed human rights principles. Creating a space for meaningful participation – including DPOs and NGOs as representative organizations – is also about ensuring the conditions for meaningful participation are created, in terms of staff sensitized, accessibility of venues and accessible information and communication. There is thus a corresponding need to heighten awareness within policy-making domains that those on the ‘outside’ share many of the same goals as policy makers. It may well be that important lessons can be learned from the experience of other marginalized groups (such as women and girls, ethnic minorities and older people) to influence mainstream policy.
Once completed, these first steps can lead to civil society representatives being empowered; this may include forming national coalitions, meeting government officials to review, monitor and oversee national policies. It may also involve people with disability securing leading roles in government, business, education, in fact, in any area of life. An important role of civil society is also to highlight the intersectionality of disability and assistive technology needs. For instance, people with impairments come from all walks of life and age; they may be men or women; members of indigenous society, who may themselves be marginalized; they may live in isolated rural areas, or urban slums. To ensure that policy becomes fully inclusive, these intersectional forms of marginalization have to be recognized and taken into account; preventing different forms of marginalization multiplying disadvantage. For instance, the use of assistive technology is associated with inclusion and wellbeing even among marginalized groups in very difficult circumstances; such as children with amputations in Gaza [Citation62]. However, we recognize that there are often greater barriers for those with a weaker voice, such as people with intellectual disability, who also have much to benefit from initiatives such as GATE [Citation18] and so greater efforts need to be made to address these barriers.
The International Disability Alliance brings together over 1100 organizations of persons with disabilities and their families; from across eight global and six regional networks, and will continue to advocate the global community to create the conditions for the effective realization of the rights enshrined in the CRPD at country level. This implies systematic and meaningful consultation with persons with disabilities (including assistive technology users) and their representative organizations to guide the definition, monitoring and evaluation of assistive technology policies (in line with CRPD Article 4.3). IDA and its members are an important conduit for mobilizing the diversity of users, including most marginalized groups such as persons with intellectual disabilities, persons with psychosocial disabilities, persons with deaf-blindness or indigenous persons with disabilities; bringing the perspective of users of assistive technology, in all service research, procurement and delivery. IDA, with its Members, is particularly concerned by the need to frame assistive technology policies that truly respond to the rights of all persons with disabilities, in particular in low and middle income countries, to access quality assistive technology, at an affordable cost, as close as possible to where people live. This includes influencing assistive technology policies, public procurement policies as well as ensuring that accessibility and reasonable accommodation, including assistive technology, is included and properly resourced in all concerned public policies [Citation63].
While civil society has a critical representational and advocating role – and, in some cases, is a major service provider – it is also important to ensure that policy cultivates the expectation of civil duty being shared among all of us. It is, therefore, crucial that such duty is not partitioned or separated; not a “them” or “us”; but rather a shared responsibility to be addressed through acknowledging ownership of the challenges of promoting equitable assistive technology systems and working through engagement with people as working as a sustainable community of practice.
Scaling good practices
National Assistive Technology policies should recognize the potential of small-scale good practices to be scaled in a variety of ways. This is particularly important in resource poor contexts, where a range of different service providers (including different civil society organizations) may have developed small-scale but innovative projects; that lack the infrastructure to be brought to the next stage. The value of adopting a systematic approach to scaling, such as Expandnet (http://www.expandnet.net/) (which chimes with a human rights perspective and with the presence of civil society actors), is a principle that should be anticipated in policy. Such scaling may require action at the structural level (scaling-up) as well as replication (scaling-out) of existing good practices. Examples of structural change that promote some aspects of the CRPD have been reported in various countries by the UNPRPD Programme (see [Citation11]); although none of these projects has as yet focused on scaling assistive technology initiatives other groups are working towards this [Citation20].
Why policy and evidence differ
Cairney [Citation64] cites four obstacles to evidence-based policymaking.
First, even where “the evidence” exists, it doesn’t actually tell you what to do: This may occur because evidence points to problems, but not solutions; it may focus more on effectiveness than appropriateness; scientists may exaggerate or disagree about findings, implications or implementation methods; evidence may be patchy because it crosses traditional disciplinary or policy boundaries; or evidence may be presented in an unsystematic, unfamiliar, or impenetrable format, perhaps coming from foreign countries and contexts.
Second, the sort of evidence that is needed, is not what is available – demand for evidence does not match the supply: Research funding may prioritize “magic bullet” interventions, that would reduce or remove the need for political choice; the scientific method may narrow focus on simplified and controllable variables, while policy makers seek solution to complex problems; “the evidence” may be interpreted selectively, or differently by policy makers; who may need to make decisions quickly amidst uncertainty; need to make decisions, the consequences of which may take years to unfold and which are influenced by other factors.
Third, in the complexity of policymaking the role of evidence may be unclear and contested: Many researchers do not understand the policy process and other stakeholders may know better how to influence it; the demand for evidence may depend on which government department is involved, which may favour some types or sources of evidence over others.
Fourth, and perhaps most surprising for researchers, evidence-based policy making and good policymaking, are not synonymous: For instance, reducing evidence-policy gaps may mean centralizing power in the hands of just a few policymakers and ignoring other sources of knowledge (such as personal experience and judgement). It may mitigate against public or user involvement, it may not value consultation with stakeholders with different perspectives, and thus it may undermine participatory approaches to policy making.
We would add a fifth element: that policies should be policy-based: By this, we mean that a National Assistive Technology Policy should articulate with other cogent polices; be they international conventions (e.g., CRPD), best practice in relevant aspects of regulation and law making [Citation65], or more context-relevant national polices (for instance, on rehabilitation or inclusive education).
In our view, Assistive Technology policy must, therefore, be evidence-informed, but its fundamental basis must be broader and more inclusive than of only evidence that accords with strictly scientific standards. A variety of stakeholder views, contextual, cultural, resources and systems perspectives must also inform policy; ideally with these perspectives being assessed and synthesized in systematic and transparent ways that also further increases their credibility. While some forms of evidence review, such as realist synthesis, give much more emphasis to contextual and process issues than do conventional systematic reviews (see for instance [Citation66,Citation67]) for participation to be genuine, there can never, in principle, exist a one-to-one transformation from scientific research to policy: this is neither realistic nor desirable.
Policy needs political engagement
Many of those who are evidence-producers (researchers, practitioners, users) are often unsure how, or simply unwilling, to undertake effective political engagement. At other times, advocates are frustrated by the difficulty of getting assistive technology on the political agenda. People may talk of political engagement wistfully; in opaque terms, as a factor outside their control; or in negative terms, as a vaguely dirty business that is a necessary evil. The reality of the demands on policy makers is that direct and persistent engagement is required to hold their attention, particularly on new ideas that may initially appear as yet another demand.
Effective political engagement is a critical success factor in a number of areas where assistive technology is salient – health, education, employment. To be realistic about developing policy on assistive technology systems, it is likely that a country will need several assistive technology leaders, or champions, who can understand the political landscape in which they work, translate technical content into compelling material to engage politicians, network and interact with key stakeholders; in short, to become policy entrepreneurs. Some elements of this work will require such advocates to be supported by, or undertake, a detailed political economy analysis of factors likely to propel change in the desired direction, and those likely to impede it.
Conclusions
This position paper demonstrates the complexity involved when generating policy towards sustainable assistive technology provision. States that have ratified the CRPD have reporting obligations to the CRPD Committee, to outline just how they are planning to do this. While the general ethos of the Convention is supportive of assistive technology, it is nonetheless rather vague (e.g., see [Citation9]). Currently, many States that have reported have not made reference to assistive technology within their reports [Citation68]. We feel the development of, and adoption of, a General Comment on Assistive Technology (i.e., a statement additional and complimentary to the CRPD) would be very helpful in both the development of National Assistive Technology Policies, and in guiding the Committee on how to most constructively respond to States reports submitted to it, especially regarding those sections pertaining to assistive technology, or indeed the absence of such reporting.
Among other things assistive technology policy should promote ageing from a life course perspective, the need for population level data, reducing rehabilitation silo-ing, promoting inter-sectoralism and intersectionality, the need for more low-tech assistive technology, universal and environmental access, the institutionalization of disruption, and the scaling of good practices. It should also value evidence-informed as opposed to evidence-based policy.
Work is currently underway on the development of a Framework to guide and evaluate assistive technology policy; and many of the ideas in this paper will inform that framework. We need to evaluate – both quantitatively and qualitatively – the extent to which policies, strategies and action plans related to AT, incorporate principles of human rights and enable equitable access in practice. This calls for analysis of policy “on the books” where it does exist, the process of policy making, it implementation, and the documentation of the lived experiences of persons using AT. Fundamentally, we need to make a leap forward to user-centred systems thinking, crossing sectors, in the same way as people’s lives cross sectors. Without this dramatic change in approach assistive technology may become increasingly siloed, divisive and inequitable; undermining basic principles of social justice, on which the CRPD, as well as other human rights Conventions and Declarations, are based.
The WHO have shown a commitment to highlighting the importance of providing appropriate assistive technology to those who need it, especially through GATE. While raising awareness about assistive technology and the broad range of people it may be crucially important for, generating an in-depth understanding of the issues and need for context specific policy remains a huge challenge. The identification of examples of good practice in terms of assistive technology systems-thinking and its applications might be useful. Borrowing from the success of Handicap International’s “Making it Work” program (referring to good practice examples of the CRPD); good practices across very different contexts could provide inspiring human stories – compelling narratives of success. A coordinated series of real life stories and case studies to aid assistive technology champions engage with policy makers might be a very useful tool for advocacy. This could feature users, carers, communities, professionals and policy makers; describing difficulties that are able to be overcome by assistive technology products and systems.
National assistive technology policy should aim to provide a national system with oversight to ensure sustainable, efficient and effective monitoring, supply and servicing of assistive technology, which appropriately meet peoples’ ever changing needs across the life course. A National institute or committee, regulatory body, or similar structure, should be representative of people with a variety of assistive technology needs. Such a body should be charged with specifying exactly how the State, as the primary duty bearer, will fulfil its obligations and embrace its responsibilities from a human rights, justice and equality of opportunity perspective.
This paper has not attempted to be either comprehensive or exhaustive, but rather to highlight some of the key policy challenges for effective national assistive technology systems. As recognized by the GATE Research Agenda [Citation69], this is a priority research area; and one that requires the involvement of all stakeholder and many different types of methodological approaches. It is therefore crucial that policies not only reflect the outcomes of research but also prioritize – and resource – the collection of data that will be used to continually inform, review and improve policy.
Acknowledgements
We very grateful to the many participants in the GREAT Summit who provided stimulating discussion points, some of which have also been included in this paper.
Disclosure statement
No potential conflict of interest was reported by the authors.
Related Research Data
References
- Khasnabis C, Mirza Z, MacLachlan M. Opening the GATE to inclusion for people with disabilities. Lancet. 2015;386:2229–2230.
- Levitas R, Pantazis C, Fahmy E, et al. The multi-dimensional analysis of social exclusion. Bristol: Bristol Institute for Public Affairs, University of Bristol; 2007.
- United Nations. Standard Rules on the Equalization of Opportunities for Persons with Disabilities. United Nations; 1994.
- United Nations. United Nations Convention on the Rights of Persons with Disabilities. United Nations; 2007.
- UNESCAP. Statistical Yearbook for Asia and the Pacific, Country Profiles. Bangkok, Thailand: UNESCAP; 2012.
- World Health Organization and World Bank. World report on disability. Geneva: World Health Organization; 2011.
- World Health Organization. WHO global disability action plan 2014–2021: better health for all people with disability. Geneva: World Health Organization; 2015.
- World Health Organization. Global strategy and action plan on ageing and health (2016–2020). Geneva: World Health Organization; 2017.
- Borg J, Larsson S, Östergren PO. The right to assistive technology: for whom, for what, and by whom? Disabil Soc. 2011;26:151–167.
- CRPD. General comment No. 2: Accessibility. Committee on the rights of persons with disabilities. Eleventh Session. New York: CRPD; 2014.
- UNDP. Sustainable Development Goals: UNDP; 2016 [cited 2016 Aug 20]. Available from: http://www.undp.org/content/dam/undp/library/corporate/brochure/SDGs_Booklet_Web_En.pdf
- Tebbutt E, Brodmann R, Borg J, et al. Assistive products and the sustainable development goals (SDGs). Global Health. 2016;12:79.
- Scherer MJ, Craddock G. Matching person & technology (MPT) assessment process. Technol Disabil. 2002;14:125–131.
- Cook AM, Polgar JM. Cook and Hussey’s assistive technologies: principles and practice. US: Elsevier Health Sciences; 2015.
- Hoogerwerf E-J. Digital inclusion. A white paper: ENTELIS consortium; 2016. Available from: http://www.entelis.net/sites/all/files/digital_inclusion-a_white_paper_final_0.pdf
- MacLachlan M, Scherer M. Systems thinking for assistive technology: a commentary on the GREAT Summit. Disability & Rehabilitation: Assistive Technology. 2018.
- MacLachlan M, Mji G, Chataika T, et al. Facilitating disability inclusion in poverty reduction processes: group consensus perspectives from disability stakeholders in Uganda, Malawi, Ethiopia, and Sierra Leone. Disabil Global South. 2014;1:20.
- Boot FH, Dinsmore J, Khasnabis C, et al. Intellectual disability and assistive technology: opening the GATE wider. Front Public Health. 2017;5:10.
- Owuor J, Larkan F, MacLachlan M. Leaving no-one behind: using assistive technology to enhance community living for people with intellectual disability. Disabil Rehabil Assist Technol. 2017;12:426–428.
- Gowran RJ, McKay EA, O'Regan B. Sustainable solutions for wheelchair and seating assistive technology provision: presenting a cosmopolitan narrative with rich pictures. Technol Disabil. 2014;26:137–152.
- Huss T, MacLachlan M. Equity and inclusion in policy processes (EquIPP): a framework to support equity & inclusion in the process of policy development, implementation and evaluation. Dublin: Global Health Press; 2016.
- Speer J. Participatory Governance Reform: a good strategy for increasing government responsiveness and improving public services? World Dev. 2012;40:2379–2398.
- Slutsky J, Tumilty E, Max C, et al. Patterns of public participation: opportunity structures and mobilization from a cross-national perspective. J Health Org and Mgt. 2016;30:751–768.
- Sund T. The Norwegian Model of Assistive Technology Provision. Presentation at the Global Research, Innovation and Education on Assistive Technology (GREAT) Summit; August; Geneva, Switzerland 2017.
- Nordic Cooperation on Disability Issues. Provision of assistive technology in the Nordic countries. Vällingby, Sweden: Nordic Cooperation on Disability Issues (NSH); 2007.
- Norwegian Labour and Welfare Service. Assistive Technology in Norway – a part of a larger system: Norwegian Labour and Welfare Service 2016. Available from: https://www.nav.no/en/Home/About+NAV/Publications/_attachment/429663?_download=true&_ts =15a5f9dfd90
- Scholl M, MacLachlan M. Towards the development of a Framework for Supporting National Assistive Technology Policies. Geneva (unpublished report): WHO GATE 2016.
- Borg J, Östergren P-O. Users’ perspectives on the provision of assistive technologies in Bangladesh: awareness, providers, costs and barriers. Disabil Rehabil Assist Technol. 2015;10:301–308.
- Visagie S, Eide AH, Mannan H, et al. A description of assistive technology sources, services and outcomes of use in a number of African settings. Disabil Rehabil Assist Technol. 2017;12:705–712.
- Wazakili M, Chataika T, Mji G, et al. Social inclusion of people with disabilities in poverty reduction policies and instruments: initial impressions from Malawi and Uganda. In: Eide AH, Ingstad B, editors. Disability & poverty: a global challenge. Bristol: The Policy Press; 2011.
- Borg J, Lindström A, Larsson S. Assistive technology in developing countries: a review from the perspective of the convention on the rights of persons with disabilities. Prosthet Orthot Int. 2011;35:20–29.
- Visagie S, Eide AH, Mannan H, et al. A description of assistive technology sources, services and outcomes of use in a number of African settings. Disabil Rehabil Assist Technol. 2016;12:705–712.
- Hussey M, MacLachlan M, Mji G. Barriers to the implementation of the health and rehabilitation articles of the United Nations Convention on the rights of persons with disabilities in South Africa. Int J Health Policy Manag. 2017;6:207–218.
- Borg J, Larsson S, Östergren P-O, et al. User involvement in service delivery predicts outcomes of assistive technology use: a cross-sectional study in Bangladesh. BMC Health Serv Res. 2012;12:330.
- Kachaje R, Dube K, MacLachlan M, et al. The African Network for evidence-to-action on disability: a role player in the realisation of the UNCRPD in Africa. Ajod. 2014;3:5.
- Mji G, Gcaza S, Swartz L, et al. An African way of networking around disability. Disabil Soc. 2011;26:365–368.
- Gowran RJ, Kennan A, Marshall S, et al. Adopting a sustainable community of practice model when developing a service to support patients with epidermolysis bullosa (EB): a stakeholder-centered approach. Patient. 2015;8:51–63.
- Orellano-Colón EM, Rivero-Méndez M, Lizama M, et al. Assistive technology unmet needs of independent living older Hispanics with functional limitations. Disabil Rehabil Assist Technol. 2018;13:194–200.
- Zhang L, Yan T, You L, et al. Functional activities and social participation after stroke in rural China: a qualitative study of barriers and facilitators. Clin Rehabil. 2017;32:10.
- Toro ML, Eke C, Pearlman J. The impact of the World Health Organization 8-steps in wheelchair service provision in wheelchair users in a less resourced setting: a cohort study in Indonesia [journal article]. BMC Health Serv Res. 2016;16:26.
- Chisolm TH, Johnson CE, Danhauer JL, et al. A systematic review of health-related quality of life and hearing aids: final report of the American Academy of Audiology Task Force on the Health-Related Quality of Life Benefits of Amplification in Adults. J Am Acad Audiol. 2007;18:151–183.
- Kochkin S, Rogin CM. Quantifying the obvious: the impact of hearing instruments on quality of life. Hear Rev. 2000;7:6–34.
- Dawes P, Cruickshanks KJ, Fischer ME, et al. Hearing-aid use and long-term health outcomes: hearing handicap, mental health, social engagement, cognitive function, physical health, and mortality. Int J Audiol. 2015;54:838–844.
- Owsley C, McGwin G, Scilley K, et al. Effect of refractive error correction on health-related quality of life and depression in older nursing home residents. Arch Ophthalmol. 2007;125:1471–1477.
- Wilson DJ, Mitchell JM, Kemp BJ, et al. Effects of assistive technology on functional decline in people aging with a disability. Assistive Technol. 2009;21:208–217.
- Cho HY, MacLachlan M, Clarke M, et al. Accessible home environments for people with functional limitations: a systematic review. Int J Environ Res Public Health. 2016;13:pii E826.
- Ferguson-Pell M, Nicholson G, Bain D, et al. The role of wheelchair seating standards in determining clinical practices and funding policy. Assist Technol. 2005;17:1–6.
- Chase CA, Mann K, Wasek S, et al. Systematic review of the effect of home modification and fall prevention programs on falls and the performance of community-dwelling older adults. Am J Occup Ther. 2012;66:284–291.
- Bensi N, Bitelli C, Hoogerwerf E-J. Assistive technologies and other solutions for independence: cost or investment? Proceedings of the 11th European Conference of the Association for the Advancement of Assistive Technology in Europe (AAATE). Maastricht, The Netherlands 2011. p. 270–277.
- Enable Ireland and the Disability Federation of Ireland. Assistive Technology for People with Disabilities and Older People: A Discussion Paper. Dublin: Enable Ireland and the Disability Federation of Ireland; 2016.
- Barnard S. Technology Care on the Cheap? 2014. Available from: http://easpd.all2all.org/en/content/building-better-services-getting-best-technology#sthash.shC487YE.dpu
- Snell T, Fernandez J-L, Forder J. Building a business case for investing in adaptive technologies in England. PSSRU Discussion Paper 2831. London: Personal Social Services Research Unit; 2012.
- World Economic Forum. Eyeglasses for Global Development: Bridging the Visual Divide 2016 [cited 2017 Aug 27]. Available from: http://www3.weforum.org/docs/WEF_2016_EYElliance.pdf
- Cupples L, Ching TY, Button L, et al. Language and speech outcomes of children with hearing loss and additional disabilities: identifying the variables that influence performance at five years of age. Int J Audiol. 2016;1–12.
- Ma X, Zhou Z, Yi H, et al. Effect of providing free glasses on children’s educational outcomes in China: cluster randomized controlled trial. BMJ. 2014;349:g5740.
- Work Without Limits. Employing people with disabilities. Massachusetts: Work Without Limits; 2014.
- Parry J. The business case for 2014; accommodating employees with disabilities [cited 2017]. Available from: https://www.bcbusiness.ca/the-business-case-for-accommodating-employees-with-disabilities
- Coherent Market Insights. Elderly and Disabled Assistive Devices Market to Surpass US$26.0 Billion by 2024 Seattle, 2017; Available from: https://www.coherentmarketinsights.com/press-release/elderly-and-disabled-assist-devices-market-to-surpass-us-260-billion-by-2024-9
- The State Council of The People’s Republic of China. China to promote industry of rehabilitation and assistive products 2016 [cited 2017 Oct 3]. Available from: http://english.gov.cn/policies/latest_releases/2016/10/27/content_281475476-503586.htm
- McPherson B. Hearing assistive technologies in developing countries: background, achievements and challenges. Disabil Rehabil Assist Technol. 2014;9:360–364.
- MacLachlan M. Access to assistive technology, systems thinking, and market shaping: a response to Durocher et al. Ethics Behav. 2018.
- Nasser K, MacLachlan M, McVeigh J. Social inclusion and mental health of children with physical disabilities in Gaza, Palestine. Dcid. 2017;27:5–36.
- Bauwens L. “Users First.” Symposium on Assistive Technologies for All; May; Cape Town, South Africa: International Society for Prosthetics and Orthotics (ISPO); 2017.
- Cairney P. Four obstacles to evidence-based policymaking. 2014 [cited 2017 Oct 2]. Available from: https://paulcairney.wordpress.com/2014/05/13/four-obstacles-to-evidence-based-policymaking-ebpm/
- Clarke D. Law, regulation and strategizing for health. In: Schmets G, Rajan D, Kadandale S, editors. Strategizing national health in the 21st century: a handbook. Geneva: World Health Organization; 2016.
- McVeigh J, MacLachlan M, Gilmore B, et al. Promoting good policy for leadership and governance of health related rehabilitation: a realist synthesis. Global Health. 2016;12. doi: 10.1186/s12992-016-0182-8
- Gilmore B, MacLachlan M, McVeigh J, et al. A study of human resource competencies required to implement community rehabilitation in less resourced settings. Hum Resour Health. 2017;15:70.
- Smith E, MacLachlan M, Mannan M. Assistive technology in State’s reports to the CRPD Committee: The need for a systematic approach to reporting, evaluation and responding. Maynooth University, Ireland: ALL (Assisting Living & Learning) Institute Working Paper; 2018.
- World Health Organization. Global priority research agenda for improving access to high-quality affordable assistive technology. Geneva: World Health Organization; 2017.