
Abstract
Purpose
This review aimed to collate and summarize available research literature about wheelchair service provision education available to healthcare professional students, healthcare personnel and educators across low- to high-resourced settings.
Methods
The Joanna Briggs Institute methodological steps for scoping reviews were followed. Included studies were mainly sourced from Medline, Embase, CINAHL, Scopus, Academic Search Complete and ProQuest. Independent title, abstract and full-text screening with defined inclusion and exclusion criteria was performed. All screening and extraction were performed independently by two authors. A thematic approach was used to synthesize results. Data extracted from included studies were charted according to a template that we created. The study quality was also appraised.
Results
A total of 25 articles were included (11, 36% from high-income settings) with 12 (48%) observational studies and 13 (52%) experimental studies. The literature addressed three main topics: (1) assessing wheelchair service provision knowledge, (2) implementing training interventions using in-person, online and/or hybrid learning approaches and (3) describing current wheelchair service provision education globally. The most frequently reported training programs used were the Wheelchair Skills Program and the World Health Organization Wheelchair Service Training Package – Basic Level.
Conclusion
Limited information has been published about the integration of wheelchair content into the curricula of professional rehabilitation programs. Efforts to build international partnerships, improve the quality and currency of training programs and build resources that can assist educators in the integration of wheelchair-related content into professional rehabilitation programs should be prioritized.
This is the first review that examined and synthesized the current state of wheelchair service provision education for rehabilitation students and personnel across low- to high-income countries.
Findings from this review indicate that there is limited information about the integration of wheelchair-related content into professional rehabilitation programs.
Efforts to build international partnerships, standardize wheelchair service provision content and evaluation and integrate training into professional rehabilitation programs worldwide should be prioritized.
Implications for Rehabilitation
Introduction
Access to assistive products, such as wheelchairs, can reduce inequalities experienced by people with disabilities by enabling them to participate in society and enjoy fundamental freedoms [Citation1]. A wheelchair has been defined as an extrinsic and intrinsic enabler that allows people with posture and mobility impairments to actively participate in their daily living across their life spans [Citation2]. An appropriate wheelchair, defined by the World Health Organization (WHO) as “a wheelchair that meets the user’s needs and environmental conditions; provides proper fit and postural support; is safe and durable; is available in the country; and can be obtained and maintained and services sustained in the country at the most economical and affordable price” [Citation3] can promote well-being, function and independence to people with disabilities [Citation4,Citation5]. Conversely, an inappropriate wheelchair can result in poorer health outcomes [Citation6]; decreased functional abilities and quality of life [Citation7,Citation8]; social isolation and even death [Citation9]. The WHO has published global guidelines that highlight eight sequential steps involved in wheelchair service provision (i.e., referral and appointment, assessment, prescription, funding and ordering, product preparation, fitting, user training, and follow-up, maintenance and repairs) [Citation3] and a series of open-source Wheelchair Service Training Packages in multiple languages to support appropriate wheelchair service delivery worldwide [Citation10–14]. Yet, providing an appropriate wheelchair and its associated services remains a challenge worldwide. There is an increasing volume of evidence revealing the need to build a competent workforce of rehabilitation professionals and strengthen the wheelchair service provision curricula in professional rehabilitation programs [Citation15–19].
Evidence has emerged demonstrating limited competency in wheelchair service provision among entry-to-practice students [Citation15,Citation16,Citation19,Citation20] and clinicians [Citation21–23] who are primarily responsible for wheelchair service delivery (i.e., those in physical therapy [PT], occupational therapy [OT], and prosthetics and orthotics [P&O] programs). A survey completed by 72 representatives from PT, OT and P&O university programs from low- to high-income countries reported that ∼21% of programs do not include wheelchair-related education in their curricula [Citation18]. Among those institutions that do, on an average, wheelchair-related content was taught for 20 h or less instead of the 35 to 40 h recommended by the WHO [Citation24]. In addition, these institutions varied in their curriculum, teaching methods, and evaluation approaches to teach and assess wheelchair service provision competency. [Citation18]. Recently, Kirby et al. surveyed 110 OTs in Nova Scotia, Canada on their wheelchair-skills-training practices and views. Few professionals reported providing wheelchair-skills training to their clients and only about one-third considered themselves adequately prepared for the trainer role [Citation25]. A similar survey was completed by 309 wheelchair service providers from 35 countries [Citation26]. Although a higher proportion of respondents provided training, the amount of training was minimal with a median total of training time for clients and caregivers of 45 and 30 min [Citation26]. Moreover, in their scoping review of wheelchair service provision education and training in low and lower middle income countries (LLMIC), McSweeney and Gowran found that wheelchair-related education and training is particularly limited in less-resourced settings and not integrated into university programs; instead, education is mainly provided by non-governmental organizations [Citation19]. The review recommended the integration of wheelchair-related content into existing curricula in universities to guarantee a sustainable and competent workforce to undertake wheelchair service provision globally [Citation19]. Although the situation may be more problematic in LLMICs, the lack of wheelchair service delivery competency among rehabilitation professionals and the limited integration of wheelchair content into professional rehabilitation programs is a global concern, not just limited to less-resourced settings [Citation20].
Despite the availability of open-source, evidence-based wheelchair service provision training materials [Citation10,Citation11,Citation27,Citation28] and the development of effective novel training methods to teach wheelchair content [Citation22,Citation23,Citation29–31], there is a lack of integration of such content into professional rehabilitation programs resulting in limited competencies among rehabilitation professionals that limits the pace of workforce training and therefore appropriate wheelchair service provision. Fung et al. uncovered barriers to the integration of wheelchair service provision content into rehabilitation programs curricula related to difficulties in the integration process, limited human and physical resources, limited funding and time constraints [Citation17]. Other studies have reported lack of awareness among educators in rehabilitation programs of existing open-source resources for wheelchair service provision education as additional barriers [Citation18,Citation19].
The need to build a competent workforce has been prioritized in the 2018 Wheelchair Stakeholders’ Meeting as an action item to meet the sector goal: “By 2030, 10 countries have new or strengthened evidence-based, adequately resourced, integrated wheelchair services supported by policies, competent personnel, and a range of appropriate wheelchairs” [Citation32]. More recently, a group of stakeholders published a position paper that identified several global challenges to accessing appropriate wheelchairs, including the need for a competent workforce of wheelchair service providers. These authors posit that “building capacity and delivering adequate education and training for all” is a key component to the development of sustainable wheelchair provision systems [Citation4].
The shortage of competent wheelchair service providers and the lack or limited integration of wheelchair-related content into professional rehabilitation programs have been recognized; however, it is unclear what information is available about wheelchair service provision education for healthcare students and personnel and who is offering that education. A review is needed to systematically synthesize the evidence, map the key concepts and provide suggestions for future research priorities. We selected a scoping review method because (1) wheelchair service education is an emerging topic in rehabilitation and we were interested in synthesizing evidence from a variety of sources [Citation33–35]; (2) we were seeking to identify and describe the key characteristics and factors in wheelchair service provision education that can assist in bridging the research gaps [Citation33,Citation35]; (3) we formulated exploratory questions and were not interested solely in comparing the effectiveness of educational interventions as a systematic review might do [Citation33]; and (4) we recognized that much of the current evidence is low-level with a variety of study designs [Citation34,Citation35]. The results from such a review will inform the development of the International Society of Wheelchair Professionals (ISWP) Wheelchair Educators’ Package (WEP), an online toolkit that will assist educators of rehabilitation professionals globally to overcome barriers in the integration of wheelchair content into their curricula.
Materials and methods
Our review follows the methodological steps outlined by the Joanna Briggs Institute [Citation36] and the reporting guidelines for the conduct of scoping reviews, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [Citation37]. A brief overview of our process is outlined below including deviations from the initial protocol; the details of the methods are published in a previous protocol paper [Citation38]. The protocol was registered at Open Science Framework (Registration doi: 10.17605/OSF.IO/C5P3T).
Stage 1: Identifying research questions
The overarching research question for the scoping review was: “What is known about wheelchair service provision education for healthcare professional students, healthcare personnel and educators as offered by universities, organizations, and industries?”. To delineate exploration of the overarching question, three sub-questions were identified: (1) “How are wheelchair service provision education curricula developed, integrated and delivered"; (2) “What are the expected skills and competencies after wheelchair service provision education and how are these evaluated?”; and (3) "What is the evidence for educational effectiveness and clinical impact, and how are these measured?”
Stage 2: Identifying relevant articles
A comprehensive search strategy was developed with specific concepts and key terms. The primary search strategy was then implemented using the following electronic databases: Medline, Embase, EBM Reviews, CINAHL, SCOPUS and Academic Search Complete. Additionally, a grey literature search was conducted using ProQuest (ERIC, PAIS Index, Dissertations & Theses Global, Canadian Research Index and Dissertations & Theses @ Université de Montréal). The search strategy, adapted for each indexed database, is presented in Supplementary File 1.
Following full-text screening of indexed articles, the grey literature was subsequently searched using OpenGrey, Campbell Collaboration, Health Systems Evidence, WHO Library and key websites involved in or related to wheelchair service provision. The reference lists of the included studies were searched to identify additional articles. In addition, a selection of four journals pertinent to the field (i.e., Disability and Rehabilitation: Assistive Technology; Archives of Physical Medicine and Rehabilitation; PLOS ONE; and Advances in Health Sciences Education) were hand searched to ensure that no relevant and recently non-indexed articles, published between January to August 2020, were missed.
The literature search was designed to retrieve both peer-reviewed and non peer-reviewed publications pertaining to wheelchair service provision education offered to healthcare profession personnel, students and educators (including rehabilitation engineers and technicians as well as community-based rehabilitation workers) and by universities, organizations and industries from low-to-high income countries. The inclusion period was from January 1993 onwards in accordance with the publication of the Standard Rules on the Equalization of Opportunities for Persons with Disabilities. Languages considered for inclusion were English and French, as translation support was available. The exclusion criteria are detailed in the protocol paper [Citation38].
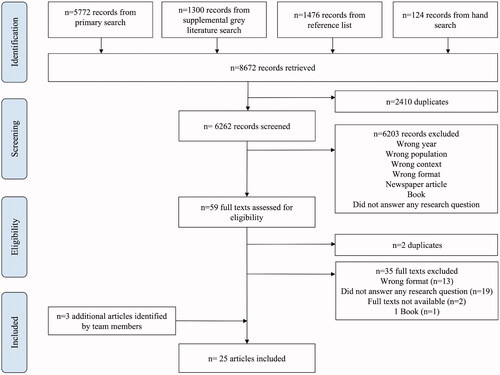
Additional articles were identified by the research team and accepted as eligible studies after Stage 2 was completed (). These articles underwent the same process for the remaining Stages as the initially screened articles.
Figure 1. PRISMA-ScR flowchart.
Stage 3: Article selection
Two reviewers (S. A. B. and M. N. – acknowledgement section) independently screened the titles and abstracts of identified studies and the full-text records were obtained for articles deemed eligible. The results of the independent screening were compared and there was 98.9% agreement during title and abstract screening and 91.8% agreement during full-text screening. Discrepancies between reviewers were resolved by discussion.
Covidence® software was used for screening titles and abstracts. The software was also used to manage citations throughout the selection process.
Stage 4: Charting the data
Data were extracted using a piloted and refined data template which was developed for the purpose of this review (Supplementary File 2). The following information was extracted: author(s), year of publication, location or country of origin, aims, study population and sample size (if applicable) as well as content related to the review questions (wheelchair service provision education and training development, integration and delivery; skills and competencies for safe and effective wheelchair service provision; skills and competencies evaluation; effectiveness and clinical impact of wheelchair service provision education and training). This process involved independent data extraction by two reviewers (Y. B. M. and S. K.), a minor deviation from the four reviewers originally proposed in the protocol. Each reviewer independently reviewed half of the included articles and subsequently engaged in a meeting to review and discuss the data extraction with a third team member (P. W. R.) to ensure consistency and accuracy of data extraction. One of the independent reviewers (Y. B. M.) was lead author for three included studies [Citation22,Citation23,Citation29] and thus was not involved in the data extraction for these studies.
Two independent reviewers (S. A. B. and Y. B. M.) appraised the quality of the included articles using the Mixed Methods Appraisal Tool (MMAT) version 2018, an established and validated assessment tool for quantitative, qualitative and mixed-methods studies [Citation39,Citation40]. The reviewers held discussions until consensus was reached. As the MMAT is not appropriate for review papers and reports, three included articles [Citation19,Citation41,Citation42] were not assessed.
Stage 5: Collating, summarizing and reporting the results
The data were narratively synthesized using a thematic-analysis approach. Direct text quotations from the included articles were extracted and used for the narrative synthesis. As a first step, the direct text quotations were populated in the data-extraction form and then condensed into content-related categories. Second, the three sub-questions of the review were considered as the primary themes and, for each primary theme, sub-themes were identified and extracted data were collated and summarized into a table (content-related categories). This table was formatted to report the synthesized results with specific details relating directly to the three key sub-questions of the scoping review. Descriptive statistics (e.g., frequency, percentages) were used to summarize the amount and range of the related literature, including publication type, year and country.
Results
Eligible studies
provides the PRISMA-ScR flowchart of this review. Of 6262 records initially screened, 59 underwent a full-text review and 22 were selected to be included in the study. Three additional studies [Citation43–45] were identified and selected post-study-selection stage, resulting in the inclusion of a total of 25 articles. presents the analyzed articles in reverse chronological order by type of study, study design, study purpose, location and setting, and target population. Among the 25 articles, 12 (48%) were observational studies and 13 (52%) were experimental studies. Twenty-two articles (88%) represented studies conducted across 30 countries; some articles included more than one setting: three (10%) low income; eight (26.7%) lower-middle income; eight (26.7%) upper-middle income; and 11 (36.7%) high-income. The remaining three articles [Citation19,Citation41,Citation42] did not represent studies in a specific country but met the inclusion criteria and provided information from >70 countries across low to high-income. The majority of articles, n = 19 (76%), were published within the last five years (2017–2021) and were focussed on (1) assessing wheelchair service provision knowledge in specific settings [Citation15,Citation16], (2) implementing training interventions to teach wheelchair service provision knowledge and/or skills [Citation22,Citation23,Citation29,Citation31,Citation42–50] and (3) enhancing understanding on current wheelchair service provision education globally [Citation17–19,Citation41]. The most frequent target population were students, clinicians or professors from OT, followed by PT and P&O. After identifying the main topics, the articles were organized in tables to provide structure to answer this study’s research questions and present the data in an efficient way. Sub-question #1, “How are wheelchair service provision education curricula developed, integrated and delivered", is addressed in . Sub-question #2, “What are the expected skills and competencies after wheelchair service provision education and how are these evaluated?”, and sub-question #3, "What is the evidence for educational effectiveness and clinical impact, and how are these measured?” are addressed in . Three articles [Citation18,Citation19,Citation41] that were not included in and are described in the section “Current state of integration of wheelchair-content into curricula globally” below.
Table 1. Purpose, design, location, and target population of included studies.
Table 2. Development, integration and delivery of wheelchair service provision education.
Table 3. Wheelchair service provision education: course effectiveness and competencies.
Wheelchair service provision education curricula
Course development
A total of four studies [Citation44,Citation47,Citation50,Citation51] reported information about course development of wheelchair-related content (: A. Development, integration and delivery of a novel course). Only two articles [Citation47,Citation50] indicated the resource used (i.e., the WHO training materials [Citation10], the Rehabilitation Engineering and Assistive Technology (RESNA) [Citation52] and Australian guidelines [Citation53]) to develop their courses. The learning activities implemented included lectures, videos and hands-on practice. Three articles reported the integration of the course in the curricula in university programs but did not include details about the integration process [Citation44,Citation50,Citation51]. In these programs, one course was mandatory for fourth year medical students [Citation44] and the other two were optional courses for OT students [Citation50] and PT, OT, and Biomedical Engineering students or clinicians [Citation51]. The course that was not integrated into a university program curricula was developed to train clinicians and wheelchair users on basic wheelchair maintenance activities [Citation47]. In the four articles, the duration of the courses varied from 2 to 20 h. Overall, the articles contained limited information about course topics, distribution of the time allocated for teaching wheelchair content, and process implemented to develop the course.
Course adaptation and delivery
About half of the articles, n = 13 (52%), described the adaptation of existing wheelchair-related training materials using different learning environments (: B. Adaptation and integration of existing training courses). Authors of eight articles (62%) reported using the Wheelchair Skills Program (WSP) [Citation54] as the training resource adapted and/or tested in a different learning environment. The WHO WSTP-Basic level [Citation10] was the second most used training package, n = 4 (31%). The learning environments used were in-person, n = 5 (39%), a hybrid combination of online and in-person, n = 4 (31%) and exclusively online training, n = 3 (23%).
The articles that employed an in-person learning approach adapted the WSP using a condensed-practice training format (e.g., boot camp, workshop) [Citation30,Citation49,Citation55,Citation56] and a distributed-practice university course approach [Citation31] to teach wheelchair skills at Canadian universities. The course duration varied from 1 day of 2 to 8 h [Citation30,Citation31,Citation55,Citation56] to 2 days of 6.5 h each [Citation49] and 5 days of three hours each [Citation31]. These courses, or components of courses, were exclusively focussed on wheelchair skills, relating to step 7: User training of the WHO 8-steps for wheelchair service provision [Citation57].
The articles that followed a hybrid learning approach (n = 4) [Citation22,Citation23,Citation29,Citation43] used a combination of online and in-person environments as the teaching strategy. Most studies, n = 3 (75%) [Citation22,Citation23,Citation29] adapted the WHO WSTP-Basic level 40-h in-person course into a hybrid approach in English and Spanish, detailing the content, teaching and learning strategies, evaluation processes, material and procedures implemented in the online and in-person sections. The course adaptation strategies for the online portion included creating videos, discussion forums, interactive online modules, short quizzes and interactive activities that were completed asynchronously. The in-person sessions followed the strategies recommended by WHO WSTP-Basic level [Citation24]. The duration of the online portion ranged from 14 to 16 h (35–40% of the course) and was followed by 3 to 3.5 days of 8 to 9 h per day in-person training [Citation22,Citation23,Citation29] for international rehabilitation professionals and/or students (i.e., OT, PT, P&O and Biomedical Engineers). The other article that implemented a hybrid learning approach [Citation43] adapted the WSP into a 4-h boot camp with one online module to teach wheelchair skills to OT students at a Canadian university. No details were included about the adaptation strategies and duration of the online component of the course.
The articles that reported using an online learning approach (n = 3) [Citation42,Citation45,Citation48], provided limited information about the procedures used to adapt the course online. Two studies adapted the WSP to teach manual wheelchair skills to clinicians (i.e., PT, OT, physician and therapy assistant) located in the USA [Citation45,Citation48]. These studies reported use of instructional video recordings, handouts, case studies, guided skills practice sessions, asynchronous feedback, discussion forums and quizzes as teaching and learning resources. One article reported a wheelchair skills practicing time among participants that ranged from 40 to 330 min [Citation48]. The other study adapted the WHO WSTP-Basic level into a Massive Open Online Course (MOOC) in English and French with a course duration of 16 to 24 h over 4 weeks [Citation42]. This study reported a registration of 5559 participants from 148 countries in a course running from September to October of 2018 [Citation42]. The report does not include information about dropouts and course completion rates.
Only three studies (23.1%) [Citation31,Citation43,Citation56] reported integration of courses into university program curricula; all of them were Canadian OT programs and related to wheelchair skills. All courses (or course components) were optional: one used exclusively a boot camp approach (4 h) [Citation43], another used a wheelchair skills workshop (2 to 3 h) [Citation56] and the third compared a boot camp approach (5 h) with a distributed-practice (14 h) university course [Citation31]. This last study provided the content of the university course reflecting the integration of the WHO 8-steps [Citation31].
Course competencies and effectiveness
No articles explicitly stated the expected skills and competencies after wheelchair service provision education. However, targeted competencies among the studies that tested the effectiveness of a specific course or a specific competency among rehabilitation professionals (n = 17, ) included knowledge (n = 11) [Citation15,Citation16,Citation22,Citation23,Citation29,Citation44,Citation47,Citation50,Citation51,Citation55,Citation56] and the combination of wheelchair skills and self-efficacy (n = 6) [Citation30,Citation31,Citation43,Citation45,Citation49,Citation55].
The most frequent evaluation of knowledge was on basic manual wheelchair service provision knowledge, defined as the knowledge and skills to provide wheelchair service to people with mobility impairment who can sit upright without additional postural support [Citation24]. These articles (n = 5) [Citation15,Citation16,Citation22,Citation23,Citation29] used the ISWP Basic Test [Citation58] as the outcome measure. Other studies tested wheelchair skills knowledge [Citation55,Citation56], basic maintenance skills [Citation47] and general wheelchair service provision knowledge (unspecified content) [Citation44,Citation50,Citation51]. Regardless of the selected outcome to measure knowledge, most studies used a quasi-experimental pre-post design to evaluate knowledge change after educational interventions [Citation22,Citation23,Citation29,Citation44,Citation47,Citation50,Citation51].
A total of six articles [Citation30,Citation31,Citation43,Citation45,Citation49,Citation55] evaluated WSP [Citation27] impact on wheelchair skills and self-efficacy in wheelchair use or provision of wheelchair skills training. The outcome measures most frequently used, in their different versions, were the Wheelchair Skills Test – Questionnaire (WST-Q) [Citation30,Citation31,Citation43,Citation45,Citation49] to measure self-report wheelchair skills capacity, confidence and/or performance; the Self Efficacy for Assessment, Treatment and Spotting (SEATS) [Citation31,Citation43,Citation45,Citation49] to measure self-efficacy in clinical application of wheelchair skills training and documentation; and the Wheelchair Use Confidence scale (WheelCon) [Citation30,Citation31,Citation43] to measure self-efficacy for wheelchair mobility and self-management. Similar to the studies that tested knowledge, the most frequent study design to evaluate wheelchair skills and self-efficacy was the quasi-experimental pre-post design.
Current state of integration of wheelchair-content into curricula globally
Three articles described practices in the integration of wheelchair-related content into professional rehabilitation programs (: Wheelchair service provision education: State of integration) [Citation17,Citation59,Citation60]. One study reported wheelchair-related content integration practices in 11 low- to high-income countries with a course duration that ranged from 2 to 45 h of teaching in mandatory or optional courses in academic rehabilitation programs [Citation17]. This study described barriers that educators experience integrating content into curricula (e.g., time constraints, limited human resources) and proposed strategies to overcome those difficulties (e.g., use of open-source online modules, guest lectures) [Citation17]. The two other studies described practices in high-income countries. In one Canadian survey [Citation59], OT and PT programs integrated wheelchair skills content in the format of a mandatory course or course component at the undergraduate level, with a course duration that ranged from <1 to >6 h. Almost a quarter, n = 5 (24%), of the surveyed institutions offered no training. In a UK survey, OT and PT programs at the undergraduate level reported a mean of 17.73 h of teaching wheelchair-related content with no details of the courses’ format [Citation60].
The three articles reported exclusively in provide an overview of wheelchair service provision education globally and current capacity of personnel in enabling access to assistive technology [Citation18,Citation19,Citation41]. McSweeney and Gowran reported limited competency among wheelchair service providers and a lack of integration of wheelchair service provision education in university programs in low and low- to middle-income countries (LMICs). They emphasized the need to integrate wheelchair content into university programs, endorse accreditation, and promote standardization of minimum competencies in wheelchair service provision to guarantee the development of a sustainable training strategy [Citation19]. Fung et al. investigated the global situation of wheelchair service provision education which evidenced a lack of standardization in wheelchair content among professional rehabilitation programs and variability in course duration, with most courses allocating less time than recommended by the WHO. The authors encouraged the development of tools for educators that assist them in the integration of wheelchair content [Citation18].
Methodological quality assessment
Overall, the articles had high methodological quality. The MMAT reported a total of 88% of questions fulfilling the methodological criteria. In the majority articles grouped as “quantitative non-randomized,” the question “Are the confounders accounted for in the design and analysis?” could not be addressed by the information reported in the paper. Similarly, all articles that used a mixed methods design did not report information that may help reviewers to assess the question “Are divergences and inconsistencies between quantitative and qualitative results adequately addressed?.”
Discussion
Summary of eligible studies
Up to August 2021, a total of 25 publications were identified with the majority being published in the last 5 years reflecting an emergent interest in the field and the necessity to better understand the current state of wheelchair service education globally. This growth in research aligns with the agenda of the 2018 Wheelchair Stakeholders Meeting [Citation32], the 2017 Global Priority Research Agenda and ultimately [Citation61], the Members States commitment to fulfilling the promise of the United Nations (UN) Convention of the Rights of People with Disabilities [Citation62] and the UN Sustainable Development Goals [Citation63].
As expected, we found low-level evidence with a similar representation of descriptive (48%) and experimental studies (52%) using a variety of study designs. Among experimental studies, the quasi-experimental design using pre–post measures was the most common with sample sizes that range from 6 to 123 participants and only one article reporting a sample size bigger than 100 participants [Citation44]. Quasi-experimental designs have become widely used in education research since 2009 as some topics in education are not amenable for randomized controlled trials (RCTs) as they present ethical challenges and/or may be too expensive [Citation64]. Our scoping review yielded only two RCTs, one published in 2004 [Citation56] and the second one in 2011 [Citation55] and 10 quasi-experimental designs published between 2015 and 2021. In terms of study location, the results provided information from more than 30 countries; however, only three articles (10%) were conducted in low-income countries while most of the evidence came from high-income countries, n = 11 (36%).
Despite the broad population of this scoping review inclusion criteria, the majority of studies focussed on target populations for a limited number of professional groups (i.e., student and clinicians; overwhelmingly OT and PT) and has the potential to be biased from this professional/educational perspective. Additional assistive technology profession educators are encouraged to be more active in the development of the evidence base in this area so that educational, and ultimately, patient outcomes can benefit from multiple, collaborative professional perspectives.
Wheelchair service provision education globally: programs used and delivery methods
The WSP was the most frequently reported training package used to teach wheelchair-related content in high-income settings. The WSP is a set of assessments, tools and training protocols related to wheelchair skills exclusively [Citation27]. This program was used in eight (62%) of the experimental studies that adapted and delivered training materials using different learning environments such as condensed-practice training formats (i.e., workshops and boot camps) delivered in-person to OT students and clinicians and self-paced training formats delivered online to clinicians. Both learning environments and training formats have been effective in increasing wheelchair skills. Although the frequency in use of the WSP may indicate that the WSP has been widely distributed and incorporated in wheelchair-related education, it is important to note that all the studies were implemented in English-speaking, high-income countries (i.e., Canada and USA) using mostly in-person and online learning approaches (only one study used a hybrid approach). No evidence has been published about the adaptation and use of the WSP in less-resourced environments except for one article that explored the potential applicability of the WSP to the Indian context [Citation65]. Many factors can limit the use of the WSP in LMICs; for instance, the WSP is available exclusively in English and French-Canadian, this is a fundamental barrier for researchers and educators whose mother tongue is not English or French [Citation66]. Some groups have translated parts of the materials, but official translations are limited to the aforementioned languages. Even for those educators who may be proficient in the language, translating and adapting the content into their curricula will represent a burden on their already busy schedules. Another potential barrier to the use of the WSP is limited physical resources (e.g., limited wheelchairs and equipment) and human resources (e.g., trained instructors) [Citation17] encountered in many LMICs. Moreover, the WSP’s Manual of over 300 pages, may represent an obstacle for health care providers with limited literacy. In many LMICs, community health workers also known as village health workers, lay health workers, or promotores, play a critical role in healthcare delivery [Citation67], including rehabilitation services [Citation68,Citation69]. These workers, who may not have received professional rehabilitation education might find the format and length of the WSP manual challenging.
It is important to note that the WSP’s scope is focussed on wheelchair skills and it does not cover all the WH0-8 steps in comprehensive wheelchair service delivery. Therefore, resolving the challenges listed here for the WSP do not address the training gap.
The WHO WSTP-Basic level was the second most frequently reported training package used to adapt and deliver training. The package was used in four (31%) of the experimental studies that adapted and delivered training materials to teach wheelchair-related content. One article adapted the WHO WSTP-Basic level into a continuing education course using a hybrid format [Citation29]; subsequently, two studies implemented the course among rehabilitation professionals from LMICs (i.e., Colombia, India and Mexico) [Citation22,Citation23]. The hybrid methodology combines online and in-person learning environments and has been widely used in health education among LMICs to overcome barriers to knowledge dissemination [Citation70,Citation71]. In order to be considered a hybrid course, 30 to 80% of the content needs to be delivered online [Citation72]. None of the articles provided the percentage of content delivered online; however, we could infer from the articles’ tables that describe the courses’ content, that this criterion was fulfilled [Citation22,Citation23,Citation29]. One article used an online self-paced tutorial prior to a 4-h boot camp on wheelchair skills to train OT students at a Canadian university [Citation43]. It is unknown if the extent of the online module ranged between 30% and 80% of the total content course to be considered as a hybrid.
As opposed to high-income countries, training programs that targeted LMICs exclusively used the WHO WSTP-Basic level, a 40-h comprehensive course that covers the WHO-8 steps of wheelchair service provision. The availability of the WHO WSTP-Basic level in multiple languages, access to training materials for trainees (e.g., working book, reference manual) and trainers (e.g., PowerPoint presentations, trainer’s manual, videos, posters) and the fact the content covers all steps of wheelchair service provision, may increase its dissemination and usage. Nevertheless, some research teams have identified limited content and training time for various wheelchair service provision steps. For instance, the WSP includes 32 mobility skills for manual wheelchair users as opposed to the seven skills encompassed in the WHO WSTP-Basic level [Citation10,Citation27]. Another training package, the Wheelchair Maintenance Training Program (WMTP) considered a more extensive list of maintenance activities to be taught to wheelchair users and caregivers than the ones included in the WHO WSTP-Basic level [Citation28,Citation47]. The WHO WSTP-Basic level is a high-profile and globally impactful training that was developed through a consensus rather than evidence-based process and is not frequently updated like typical curriculum is. The WSP and the WMTP are examples of evidence-based packages that serve to both highlight the gaps in the WHO-WSTP and provide examples of how they can be supplemented and expanded.
Integration of wheelchair-related content into curricula: the need for further support
Limited information is known about the integration of wheelchair content into the curricula of professional rehabilitation programs. Three articles reported on the development and integration of wheelchair related courses; one for medical students in the USA (high-income country) [Citation44], another for OT students in Jordan (upper-middle-income country) [Citation50], and a third for PT, OT and Rehabilitation Engineers in the UK (high-income country) [Citation51]. These articles provided minimal to no information about the process involved in the course development and the methods used to integrate the content. From the articles that adapted a pre-existing training course (i.e., WSP) using an alternative learning methodology, three articles [Citation31,Citation43,Citation56] integrated the courses (or components of the courses) into the curricula in OT programs in Canada (high-income country), the majority of them as optional. Among these articles, only one [Citation31] provided details about the distribution of content, practical activities, and evaluation resources that may benefit other programs in a similar context to integrate wheelchair-related content into their curriculum. In addition, it was the only article that has reported the WHO 8-steps content integrated into the curriculum [Citation31].
The integration of wheelchair-related content into professional rehabilitation programs is limited but emerging primarily in high-income countries. This review yielded no articles reporting the integration of wheelchair content into rehabilitation programs at academic institutions in low-income countries. The educational initiatives to build a competent workforce in wheelchair service provision in LMICs are still offered as continuing education programs by non-governmental organizations [Citation22,Citation23]. This finding aligns with the results from the scoping review of wheelchair service provision education and training in LLMIC [Citation19] and reinforces the need to standardize and integrate training into university programs.
Recently, Fung et al. reported that time constraints and difficulties in the integration process (e.g., lack of teaching materials) have been identified by a sample of educators from low-to high-income settings as principal barriers to the integration of wheelchair content [Citation17]. These barriers are not exclusive to the rehabilitation field. Heavy workloads and time constraints to manage academic activities (e.g., teaching, conducting research) are inherent problems of the academic system. Ziker et al. reported faculty members at a University in the USA worked ∼61 h per week [Citation73]. Similarly, a survey conducted in Spain reported that, on an average, faculty work 49 h per week (11.5 h more than stipulated by law) with 20% of faculty members reporting they worked more than 60 h/week [Citation74]. The coronavirus pandemic extenuated an already unbalanced workload by increasing stress, burnout, poor mental health and career uncertainty among academics [Citation75]. Conducting teaching online can triplicate the preparation time [Citation75] leaving educators less time to update their courses and conduct other activities. Educators worldwide need support and resources to facilitate the integration of content into their courses and curricula.
Since July of 2020, ISWP and an international group of 32 wheelchair educator experts from 21 low- to high-income countries have been working on the development of the Wheelchair Educators’ Package, an online toolkit that attempts to address barriers in the integration of wheelchair content into curricula. This toolkit is to be launched in 2022 and will be a resource that may assist educators in improving wheelchair-related content in professional rehabilitation programs worldwide.
Limitations
A limitation of this study is its potential language bias; only English and French publications were included, which may not reflect a global view on wheelchair service provision education. Also, the time frame considered may have excluded some relevant evidence which has prevented us from drawing further conclusions; nevertheless, this is unlikely considering that most evidence has been published in the last 5 years.
Call-to-action
Build international partnerships for wheelchair sector professional education and research: “leave no one behind”
The underrepresentation of wheelchair service provision education in LMICs limits the scope of analysis and threatens that the recommendations that arise from this review could be biased towards what is known in middle- and high-income settings. Many of the papers included in this study refer to health professionals, including OT and PT, who have received more comprehensive training. It is less likely that wheelchair service delivery is provided by these professionals in LMICs [Citation19]. Researchers in LMICs struggle with multiple barriers to conducting research and this may be attenuated by establishing collaborative partnerships with research teams at academic institutions in high-income countries. Such partnerships would reduce disparities in education and research [Citation76,Citation77] and contribute to more accessible education for all wheelchair service provision personnel. Sponsoring micro-credentials towards professional qualifications and post-graduate are specific examples worth pursuing. This type of collaboration could lessen the gap across income level countries and enhance understanding of wheelchair service education globally to better identify the key characteristics and factors that may assist in “building capacity and delivering adequate education and training for all,” a crucial component to address the global challenge of developing sustainable wheelchair provision systems [Citation4].
Integrate wheelchair content into university programs worldwide
This scoping review found limited reporting of wheelchair-related content integration or evidence of guidelines to support educators in the integration process. Moreover, there is little detail pertaining to the specific learning outcomes used to measure knowledge, skills and attitudes nor how to best assess the transfer of acquired competencies into clinical practice. We call for a wheelchair sector education task force that includes professional societies, academic institutions, practitioners, providers and industry representatives to take action with the mission to establish guidelines for developing, integrating and updating content. If we are to achieve the promising goals to support competency development and stimulate collaboration by 2023 [Citation32] good health and well-being, promote quality education and reduce inequalities among countries, leaving no one behind [Citation63] these actions are paramount.
Conclusions
An appropriate wheelchair is essential for many people with a physical disability to meet personal posture and mobility needs, supporting health, well-being and inclusion. Wheelchair sector education and training are critical to promoting best practice. This is the first scoping review to provide a comprehensive synthesis of the current state of wheelchair service provision education for rehabilitation students and personnel across low- to high-income countries. The results from this synthesis indicate that there is limited information about the integration of wheelchair-related content into professional rehabilitation programs. Efforts to build international partnerships, standardize wheelchair service provision content and evaluation forms and integrate training into professional rehabilitation programs worldwide should be prioritized.
Supplementary_File_2_Data_Extraction_Table.docx
Download MS Word (18.7 KB)Supplementary_File_1_Search_Strategies.docx
Download MS Word (20.1 KB)Acknowledgements
The authors thank Myrian Grondin, an Academic Librarian at Université de Montréal for her help in conducting the literature search in the above-mentioned databases, Melodie Nadeau for her contribution to the protocol paper and her assistance in the first two stages of the methods, and Jenn McKee research assistant at the University of Limerick for her contribution to the protocol paper.
Disclosure statement
The authors report no conflict of interest.
Additional information
Funding
Related Research Data
References
- Tebbutt E, Brodmann R, Borg J, et al. Assistive products and the sustainable development goals (SDGs). Global Health. 2016;12(1):1–6.
- Gowran RJ. Guest editorial, special edition wheelchair and seating provision. Irish J Occup Ther. 2012;39(2):2.
- World Health Organization. Guidelines on the provision of manual wheelchairs in less resourced settings. Geneva: WHO; 2008.
- Gowran RJ, Bray N, Goldberg M, et al. Understanding the global challenges to accessing appropriate wheelchairs: position paper. IJERPH. 2021;18(7):3338.
- World Health Organization. Assistive technology. 2018. [cited 2021 August 16]. Available from: https://www.who.int/news-room/fact-sheets/detail/assistive-technology
- Thyberg M, Gerdle B, Samuelsson K, et al. Wheelchair seating intervention. Results from a client-centred approach. Disabil Rehabil. 2001;23(15):677–682.
- Kittel A, Marco AD, Stewart H. Factors influencing the decision to abandon manual wheelchairs for three individuals with a spinal cord injury. Disabil Rehabil. 2002;24(1–3):106–114.
- Chaves ES, Boninger ML, Cooper R, et al. Assessing the influence of wheelchair technology on perception of participation in spinal cord injury. Arch Phys Med Rehabil. 2004;85(11):1854–1858.
- World Health Organization. Policy brief: access to assistive technology. Geneva: World Health Organization; 2020.
- World Health Organization. Wheelchair service training package: basic level. Geneva: WHO; 2012.
- World Health Organization. Wheelchair service training package: intermediate level. Geneva: WHO; 2013.
- World Health Organization. Wheelchair service training package: managers. Geneva: WHO; 2015.
- World Health Organization. Wheelchair service training package: stakeholders. Geneva: WHO; 2015.
- World Health Organization. Wheelchair service training of trainers package. Geneva: WHO; 2018.
- Toro-Hernández ML, Alvarez L, Vargas-Chaparro MC, et al. Final year students’ knowledge on basic manual wheelchair provision: the state of occupational therapy programs in Colombia. Occup Ther Int. 2020;2020:3025456.
- Toro-Hernández ML, Mondragón-Barrera MA, Torres-Narváez MR, et al. Undergraduate physiotherapy students’ basic wheelchair provision knowledge: a pilot study in two universities in Colombia. Disabil Rehabil Assist Technol. 2020;15(3):336–336.
- Fung K, Miller T, Rushton PW, The International Society of Wheelchair Professionals, et al. Integration of wheelchair service provision education: current situation, facilitators and barriers for academic rehabilitation programs worldwide. Disabil Rehabil Assist Technol. 2020;15(5):553–510.
- Fung KH, Rushton PW, Gartz R, et al. Wheelchair service provision education in academia. Afr J Disabil. 2017;6(340):340.
- McSweeney E, Gowran RJ. Wheelchair service provision education and training in low and lower middle income countries: a scoping review. Disabil Rehabil Assist Technol. 2017;14:1–13.
- Giesbrecht E, Rushton PW, Dubé E. Wheelchair service provision education in Canadian occupational therapy programs. PLoS ONE. 2022;17(2):e0262165. DOI:10.1371/journal.pone.0262165
- Best KL, Routhier F, Miller WC. A description of manual wheelchair skills training: current practices in Canadian rehabilitation centers. Disabil Rehabil Assist Technol. 2015;10(5):393–400.
- Burrola-Mendez Y, Bonilla-Escobar FJ, Goldberg M, et al. Comparing the effectiveness of a hybrid and in-person courses of wheelchair service provision knowledge: a controlled quasi-experimental study in India and Mexico. PLoS One. 2019;14(5):e0217872.
- Burrola-Mendez Y, Toro-Hernandez ML, Goldberg M, et al. Implementation of the hybrid course on basic wheelchair service provision for Colombian wheelchair service providers. PLoS One. 2018;13(10):e0204769.
- World Health Organization. Wheelchair service training package. Trainer’s manual basic level. Geneva: WHO; 2012.
- Kirby RL, Smith C, Parker K, et al. Practices and views of occupational therapists in Nova Scotia regarding wheelchair-skills training for clients and their caregivers: an online survey. Disabil Rehabil Assist Technol. 2020;15(7):773–780.
- Kirby RL, Smith C, Parker K, et al. Practices and views of wheelchair service providers regarding wheelchair-skills training for clients and their caregivers: a global online survey. Disabil Rehabil: Assist Technol. 2021;1–8. DOI:10.1080/17483107.2021.1989505
- Kirby RR, Smith C, Routhier F, et al. Wheelchair skills program manual version 5.1. Halifax, Nova Scotia, Canada: Published Electronically at Dalhousie University; 2020. Available from: www.wheelchairskillsprogram.ca/eng/manual.php
- University of Pittsburgh Model Center on Spinal Cord Injury. Wheelchair Maintenance Training Program; 2017. [April 10 2019]. Available from: http://www.upmc-sci.pitt.edu/node/927
- Burrola-Mendez Y, Goldberg M, Gartz R, et al. Development of a hybrid course on wheelchair service provision for clinicians in international contexts. PLoS One. 2018;13(6):e0199251.
- Giesbrecht EM, Wilson N, Schneider A, et al. Preliminary evidence to support a "boot camp" approach to wheelchair skills training for clinicians. Arch Phys Med Rehabil. 2015;96(6):1158–1161.
- Rushton PW, Daoust G. Wheelchair skills training for occupational therapy students: comparison of university-course versus “boot-camp” approaches. Disabil Rehabil: Assist Technol. 2019;14(6):595–601.
- World Learning. Wheelchair Stakeholders' Meeting: Executive Summary. 2018. Available from: https://wheelchairnetwork.org/wp-content/uploads/2019/08/01a-WL-Wheelchair-Two-Pager-FINAL.pdf
- Munn Z, Peters MD, Stern C, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):1–7.
- Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):1–9.
- Peters MD, Godfrey CM, Khalil H, et al. Guidance for conducting systematic scoping reviews. JBI Evid Implement. 2015;13(3):141–146.
- Peters MD, Godfrey CM, McInerney P, et al. Methodology for JBI Scoping Reviews South Australia The Joanna Briggs Institute Reviewers’ Manual 2015; 2015.
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473.
- Kamalakannan S, Rushton PW, Giesbrecht E, et al. Wheelchair service provision education for healthcare professional students, healthcare personnel and educators across low-to high-resourced settings: a scoping review protocol. Disabil Rehabil: Assist Technol. 2020:1–7. DOI:10.1080/17483107.2020.1852325
- Hong QN, Fàbregues S, Bartlett G, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. EFI. 2018;34(4):285–291.
- Pace R, Pluye P, Bartlett G, et al. Testing the reliability and efficiency of the pilot mixed methods appraisal tool (MMAT) for systematic mixed studies review. Int J Nurs Stud. 2012;49(1):47–53.
- Smith EM, Gowran RJ, Mannan H, et al. Enabling appropriate personnel skill-mix for progressive realization of equitable access to assistive technology. Disabil Rehabil Assist Technol. 2018;13(5):445–453.
- Physiopedia. Wheelchair Service Provision Course – Evaluation Report [cited 2021. July 13]. Available from: https://www.physio-pedia.com/Wheelchair_Service_Provision_Course_-_Evaluation_Report
- Giesbrecht E, Carreiro N, Mack C. Improvement and retention of wheelchair skills training for students in entry-level occupational therapy education. Am J Occup Ther. 2021;75(1):7501205160p1–7501205160p9.
- Gilbert C, Hsieh S, Donovan J, et al. Effect of an interventional educational wheelchair program on medical students' understanding of manual wheelchair use. PM&R. 2021;13(12):1350–1356.
- Worobey LA, Kirby RL, Cowan RE, et al. Efficacy of a remote train-the-trainer model for wheelchair skills training administered by clinicians: a cohort study with pre-vs. post-training comparisons. Arch Phys Med Rehabil. 2021. DOI:10.1016/j.apmr.2021.03.042
- Munera S, Goldberg M, Kandavel K, et al. Development and evaluation of a wheelchair service provision training of trainers programme. Afr J Disabil. 2017;6:360.
- Toro ML, Bird E, Oyster M, et al. Development of a wheelchair maintenance training programme and questionnaire for clinicians and wheelchair users. Disabil Rehabil Assist Technol. 2017; 12(8):843–851.
- Worobey LA, Kirby RL, Cowan RE, et al. Using remote learning to teach clinicians manual wheelchair skills: a cohort study with pre-vs post-training comparisons. Disabil Rehabil: Assist Technol. 2020:1–8. DOI:10.1080/17483107.2020.1804633
- Smith EM, Best KL, Miller WC. A condensed wheelchair skills training ‘bootcamp’ improves students’ self-efficacy for assessing, training, spotting, and documenting manual and power wheelchair skills. Disabil Rehabil Assist Technol. 2020;15(4):418–420.
- Sarsak H. Developing wheelchair training program for rehabilitation and occupational therapy students. MOJ Yoga Phys Ther. 2018;3(4):79–83.
- White E. Impact of training for wheelchair service specialists. Br J Ther Rehabil. 2003;10(2):60–63.
- Arledge S, Armstrong W, Babinec M, et al. RESNA wheelchair service provision guide. RESNA (NJ1). Geneva: WHO; 2011.
- Lukersmith S, Radbron L, Hopman K. Development of clinical guidelines for the prescription of a seated wheelchair or mobility scooter for people with traumatic brain injury or spinal cord injury. Aust Occup Ther J. 2013;60(6):378–386.
- Wheelcahir Skills Program Dalhousie University[cited 2019. April 10]. Available from: https://wheelchairskillsprogram.ca/en/
- Kirby RL, Crawford KA, Smith C, et al. A wheelchair workshop for medical students improves knowledge and skills: a randomized controlled trial. Am J Phys Med Rehabil. 2011;90(3):197–206.
- Coolen A, Kirby R, Landry J, et al. Wheelchair skills training program for clinicians: a randomized controlled trial with occupational therapy students. Arch Phys Med Rehabil. 2004;85(7):1160–1167.
- World Health Organization. Guidelines on the provision of manual wheelchairs in less-resourced settings 2018. [Mar 01 2018]. Available from: http://www.who.int/disabilities/publications/technology/wheelchairguidelines/en/
- Gartz R, Goldberg M, Miles A, et al. Development of a contextually appropriate, reliable and valid basic wheelchair service provision test. Disabil Rehabil Assist Technol. 2016;12(4):333–340.
- Best KL, Miller WC, Routhier F. A description of manual wheelchair skills training curriculum in entry-to-practice occupational and physical therapy programs in Canada. Disabil Rehabil Assist Technol. 2015;10(5):401–406.
- Silcox L. Assessment for the prescription of wheelchairs: what training is available to therapists? Br J Occup Ther. 1995;58(3):115–118.
- World Health Organization. Global priority research agenda for improving access to high-quality affordable assistive technology. Geneva: WHO; 2017.
- United Nations Treaty Collection. Convention on the Rights of Persons with Disabilities (CRPD): United Nations; 2018 [updated April 17, 2018; cited 2018 April 17]. Available from: https://treaties.un.org/Pages/ViewDetails.aspx?src=TREATY&mtdsg_no=IV-15&chapter=4&clang=_en
- United Nations. Sustainable Development Goals. 2018. [cited 2019 October 14]. Available from: https://sustainabledevelopment.un.org/?menu=1300
- Gopalan M, Rosinger K, Ahn JB. Use of quasi-experimental research designs in education research: growth, promise, and challenges. Rev Res Educ. 2020;44(1):218–243.
- Kirby RL, Cooper RA. Applicability of the wheelchair skills program to the Indian context. Disabil Rehabil. 2007;29(11–12):969–972.
- Langer A, Díaz-Olavarrieta C, Berdichevsky K, et al. Why is research from developing countries underrepresented in international health literature, and what can be done about it? Bull World Health Organ. 2004;82(10):802–803.
- Pallas SW, Minhas D, Pérez-Escamilla R, et al. Community health workers in low- and middle-income countries: what do we know about scaling up and sustainability? Am J Public Health. 2013;103(7):e74–e82.
- Rowe M, Gamiet S. The role of rehabilitation care workers in South African healthcare: a Q-methodological study. Afr J Disabil. 2019;8(1):1–7.
- Organization WH. Access to rehabilitation in primary health care: an ongoing challenge. Geneva: World Health Organization; 2018.
- Liyanagunawardena TR, Aboshady OA. Massive open online courses: a resource for health education in developing countries. Glob Health Promot. 2018;25(3):74–76.
- Frehywot S, Vovides Y, Talib Z, et al. E-learning in medical education in resource constrained low- and Middle-income countries. Hum Resour Health. 2013;11:4.
- Smith B, Brame C. Blended and Online Learning. Vanderbilt University Center for Teaching 2014. [cited 2021 August 30]. Available from: https://cft.vanderbilt.edu/guides-sub-pages/blended-and-online-learning/
- Ziker J, Demps K, Nolin D, et al. Time Allocation Workload Knowledge Study, Phase 1 Report; 2013.
- Cabero I, Epifanio I. A data science analysis of academic staff workload profiles in Spanish universities: gender gap laid bare. Educ Sci. 2021;11(7):317.
- Gewin V. Pandemic burnout is rampant in academia. Berlin: Nature Publishing Group; 2021.
- Chetwood JD, Ladep NG, Taylor-Robinson SD. Research partnerships between high and low-income countries: are international partnerships always a good thing? BMC Med Ethics. 2015;16(1):36.
- Plancikova D, Duric P, O’May F. High-income countries remain overrepresented in highly ranked public health journals: a descriptive analysis of research settings and authorship affiliations. Crit Public Health. 2021;31(4):487–493.