
Abstract
Purpose
Eye-gaze assistive technology offers children with severe motor and communication difficulties the opportunity to access and control a computer through eye movements. The aim of this study was to examine the impact of eye-gaze assistive technology intervention on participation in computer activities and technology usability among children with complex needs in Taiwan.
Materials and methods
This study involved a multiple baseline design across individuals. The participants were four children aged three to six years with severe motor and communication difficulties and low eye-control skills. The six-month intervention consisted of two collaborative team meetings and 12 individual supports to facilitate the use of eye-gaze assistive technology at home or in educational environments. Participation in computer activities (diversity, frequency, and duration) was repeatedly measured through a computer use diary. Other outcomes included assessments of goal achievements and parents/teachers’ ratings on children’s performance in computer activities.
Results
The young children increased the diversity of their computer activities and their frequency and duration of computer use from baseline to the intervention phase. The children attained six of eight predefined goals related to play, communication, and school learning. Parents and teachers perceived the children’s changes in performance as meaningful.
Conclusion
This study strengthens the evidence that eye-gaze assistive technology is useful in everyday contexts for children with complex needs in Taiwan. The findings add knowledge that children with weak eye-control skills increased participation in computer activities as a result of the eye-gaze assistive technology.
Eye-gaze assistive technology (EGAT) as an access method to control a computer can provide opportunities for children with severe motor and communication difficulties to participate in computer activities.
Children with severe motor and communication difficulties and low eye-control skills with sufficient practice can learn to use EGAT for communication and learning, with support from stakeholders and collaborative service.
EGAT could be introduced for children with complex needs at early ages as a means of using computers for play, communication, and school learning, which could be helpful for later education and learning.
Stakeholders in educational environments could include EGAT in educational computer systems so that pupils with severe motor and communication difficulties could interact with a computer, thereby enhancing their engagement and learning.
Implications for Rehabilitation
Introduction
Using a computer can facilitate a broader range of participation in educational activities, communication, and play within the classroom and the home environments for children with disabilities [Citation1]. Nevertheless, children with complex needs, (in this study, children with severe motor and communication difficulties), encountered difficulties gaining access to and interacting with a computer. Computer accessibility is declared important to enhance their communication and learning rights, which are core features of the Sustainable Development Goals and the Convention on the Rights of the Child [Citation2–4]. With the advancement of assistive technology (AT) to support social inclusion, eye-gaze assistive technology (EGAT) has become a feasible method for children with complex needs to control a computer through eye movements and perform activities [Citation5–11]. Emerging studies from Western countries have shown the feasibility of applying EGAT at home and in school [Citation5,Citation6,Citation8,Citation10,Citation11]. However, recent systematic reviews found few intervention studies in children’s everyday circumstances and have called for global, high-quality research tailored to contexts and available resources to evidence the efficacy of EGAT [Citation12,Citation13]. This study, which applied a single-case research design, adds to the evidence of EGAT applications among young children with complex needs in Taiwan.
There is sparse evidence concerning the application and impacts of EGAT in Asia, where the AT policy and service system may differ from those of Western countries. Eligibility for EGAT applications (including software) in Taiwan is granted to people who have been diagnosed with severe physical disabilities or multiple disabilities with bilateral involvement, and who are unable to use other methods besides eye-gaze to control a computer [Citation14]. The government subsidises the cost of AT, but individuals might make a co-payment depending on the device, software and mounting system, unlike in some Western countries such as Sweden, which offer full funding support. EGAT is a fairly new technology in Taiwan’s paediatric population, although a previous study on adults with amyotrophic lateral sclerosis revealed positive impacts in terms of improving their quality of life and reducing caregiver burden [Citation15]. Hence, it is urgent to research EGAT implementation and to contribute contextual implications to global EGAT research.
Children with severe motor and communication difficulties may have multiple health issues, with associated impairments in vision and cognition [Citation16,Citation17]. They face significant challenges to social interaction, engaging in play and learning, and developing independence compared to their same-age peers [Citation18–20]. They mostly use vocalisation, facial expressions, or eye-pointing to interact with others [Citation21] and are highly dependent on their parents’ and teachers’ assistance in everyday life [Citation7,Citation22]. Communication and motor difficulties affect their ability to respond on traditional assessments; as a consequence, their cognition and learning potential may be underestimated [Citation23,Citation24].
Eye-tracking systems can be applied to study passive gaze behaviours during cognitive and attention processing for diagnostic purposes or can be used in interactive gaze application as assistive technology (the focus of the present study) [Citation25,Citation26]. For children with complex needs who have limited use of other interfaces such as a switch, touchpad, or voice to access a computer, EGAT might be their last option. EGAT harnesses an infra-red camera to detect the direction of the gaze by calculating the relationship between the child’s moving eyes and corneal reflection from infra-red light [Citation26]; it enables direct pointing with the eyes to control a cursor and to execute a mouse click by gazing at an object for a certain amount of time (i.e., “dwelling”). Thus, this computer technology helps those children to emulate the ordinary use of a mouse and keyboard to access a number of computer activities, including playing games, aided communication as a means of augmentative and alternative communication (AAC), or performing learning tasks [Citation5,Citation6,Citation8,Citation10]. Using EGAT requires eye-control abilities, such as gaze exploration on the screen and visual fixation on a screen target to activate it [Citation26,Citation27]. Children with visual problems, such as strabismus, may require extended time to practice eye-control skills in navigating a screen and dwelling on a target for selection [Citation27,Citation28].
To date, there has been little research on the usability and efficacy of EGAT for children with complex needs under everyday circumstances [Citation13]. Usability suggests how well an AT device and service enable a user to achieve goals effectively and to become satisfied with the use [Citation29]. A recent systematic review reported fewer than five multiple case studies conducted in real-life settings [Citation13]. The researchers primarily targeted children with severe cerebral palsy (CP) or Rett syndrome. The intervention phase varied, from trialling EGAT for approximately six weeks to up to one year. Two studies have addressed the process of participation in computer activities, showing that children with complex needs increased the frequency of computer use after they were exposed to EGAT [Citation5,Citation6]. They also showed increased duration of computer use and were engaged in using EGAT for communication and playing/games at home or in school, in an average of four different activities. In addition, empirical studies indicate that children with complex needs increase their expressive communication skills [Citation6,Citation11]. The use of EGAT increases children’s initiations of communicative interactions and their intelligibility and facilitates the sharing of information [Citation30]. Nevertheless, it could take several months or more than a year to develop eye-control skills [Citation28]. Children with limited experience with communication aids need time to build not only eye-gaze skills but also their skills in using EGAT for communication and operating a computer. Eye-pointing experiences in the context of low-tech AAC methods (e.g., looking at graphic symbols on a communication board to communicate a message) [Citation31] may be helpful for transferring skills for EGAT use. Notably, specialised services provided to parents/teachers are crucial Citation5,Citation32,Citation33 to support children’s use in carrying out meaningful activities at home or in school and to help children cultivate EGAT and reap the associated long-term benefits.
As indicated above, there are only a few longitudinal studies on EGAT application in children, and most research employs a case study methodology [Citation13]. Although randomised control trials are used to examine efficacy, a single case design can also demonstrate causal relationships between an intervention and participant outcomes [Citation34]. Through serial observation of targeted behaviours of each participant at baseline and in the intervention phase, with replication across participants, this design can provide causal inferences of the effects on the manipulated independent variable, the EGAT intervention [Citation35]. This study used a single-case research design [Citation36] to investigate the impact of an EGAT intervention on participation in computer activities, and to examine technology usability for children with complex needs in Taiwan.
The researchers sought to answer three research questions:
Do children with complex needs increase their computer activity participation (diversity of computer activities, frequency, duration) after receiving an EGAT intervention?
Do children with complex needs attain predetermined goals for computer participation after a six-month intervention?
Do parents/teachers perceive positive changes in children’s performance in computer activities, and are they satisfied with their children’s performance?
Methods
Design
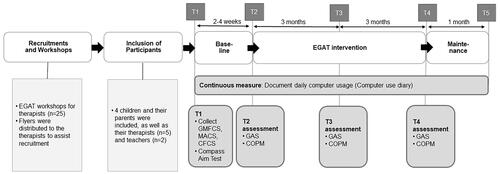
A single-case research design was applied with a multiple baseline design across individuals [Citation36]. The inclusion of participants was non-concurrent [Citation37], with the study beginning with different students (i.e., the initial baselines) starting zero to three months apart due to recruitment difficulties. This study involved a baseline period (T1–T2), followed by a six-month EGAT intervention (T2–T4) and a one-month maintenance phase (T4–T5) (see ).
Figure 1. The study procedure and measurements at each time point. Note. T1= the beginning of the baseline phase. T2= before the intervention started. T3= at the three-month intervention, T4= at the six-month intervention, T5= one-month after the intervention ended. GMFCS = Gross Motor Function Classification System; MACS = Manual Ability Classification System; CFCS = Communication Function Classification System; GAS = Goal Attainment Scaling; COPM = Canadian Occupational Performance Measure. The study began with a workshop for therapists and participant recruitment. Then, the included participants were involved in a procedure, with a two to four-week baseline, followed by a six-month intervention and a one-month maintenance phase. The figure also presents the measurements conducted from T1 to T5.
Intersubject replication and systematic manipulation of the EGAT intervention [Citation35,Citation38] was conducted for four participants. The onset of the intervention was randomised for each participant to control for potential confounders [Citation35,Citation38], with baseline periods of 14, 17, 20, and 23 days before the intervention onset. Neither participants nor assessors were blinded due to the nature of the intervention. Also, the study protocol was registered at Clinicaltrials.gov (NCT04377893). The report conformed to the Single-Case Reporting Guideline in Behavioural Interventions (SCRIBE) [Citation39].
Recruitment and participants
Since EGAT for the paediatric population is somewhat new in Taiwan, a two-day workshop was organised for therapists (physiotherapists [PTs], occupational therapists [OTs], and speech-language pathologists [SLPs]) (n = 25) and they were invited to recruit potential participants in northern Taiwan. Flyers containing research information and recruitment criteria were distributed to the therapists. The therapists first screened potential participants to become candidates for the EGAT. Next, the first author contacted interested families to inform them about the study’s aims and procedures, and obtained informed consent. Furthermore, the children’s teachers at school/or child development centres were invited to participate.
The inclusion criteria applied to children/youths who (1) were one to 25 years old; (2) had severe physical disabilities and communication difficulties according to a medical diagnosis and the disability evaluation system; (3) had no or limited possibilities of interacting with computers using an input method other than EGAT (e.g., switches or touchpads); (4) were new to EGAT or had tried out EGAT, but had not used it in their daily routines; and (5) students’ parents and/or teacher agreed to support the use of EGAT at home or school. They knew that the eye-gaze device had been borrowed from the local distributor of Tobii (company name) and would be returned after the intervention ended. The exclusion criteria were (1) having progressive diseases that cause functional declines or serious illness (e.g., progressive childhood encephalopathy, adrenoleukodystrophy); and (2) being placed in an adult daycare centre.
Four young children and their parents, along with their therapists (n = 5) and teachers (n = 2), participated in the study. Participant characteristics were gathered from parents and medical reports. The severity of gross motor, fine motor, and communication performance was evaluated based on the Gross Motor Function Classification System (GMFCS) [Citation40], the Manual Ability Classification System (MACS) [Citation41], and the Communication Function Classification System (CFCS) [Citation42] with levels I (a less affected function) through V (a severely restricted function). In addition, their eye-control skills were assessed using the Compass Aim test [Citation43] following the assessment procedure described in Borgestig et al. [Citation28]. It included accuracy to determine whether a child gazed at the target for selection within the time threshold (30 s), and time on task to establish the time required to successfully select a target. Each test trial, lasting approximately six minutes, contained 12 targets randomly presented on the screen at three distances from the mouse cursor. High percentage scores for accuracy (maximum 100%) and short duration in time on tasks (maximum 30 s) indicate good eye-control skills. This measure has high test-retest reliability, high construct validity, and good internal consistency [Citation43].
presents detailed information about each participant (LiHao, ChiaYu, ShuWen and YiFen [pseudonyms]). The four participants (female to male = 3:1) were aged between three and six years (mean = 5.1 years, SD = 1.1) and had a diagnosis of dyskinetic CP (LiHao, ShuWen and YiFen) or neurometabolic disorder (ChiaYu). All had profound impairments in gross and fine motor function (GMFCS, MACS level IV-V), as well as cognitive impairments based on their medical charts. LiHao and YiFen had visual impairments, namely refractive errors, astigmatism, and/or strabismus. The participants had low eye-control skills in accuracy (5.55–27.78%) and speed of target selection (13.01–22.90 s) according to the Compass Aim test. They used non-verbal communication through vocalisation, facial expressions, or looking to refuse, obtain attention, express their needs, or interact with familiar people, but their communication might not be intelligible enough for their communication partners to understand them (CFCS level IV-V). They had few experiences using eye-pointing or low-tech communication devices.
Table 1. Participant characteristics, baseline and intervention context.
Ethical approval
Written informed consent was received from parents on behalf of their children. Parents, therapists, and teachers knew the research group would assist with the EGAT application if, after the study, the participants and their parents decided to continue to use it. They were notified that they could withdraw from the study at any time without explanation, and this would not affect the services given to the children. The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the ethical review boards in Taiwan (201812EM004) for study implementation and in Sweden (Dnr 2019-04902) for data transfer and data analysis. None of the families withdrew their children from the study and there were no overt indicators of discomfort for the participants. At no point were there any reports of harm from the intervention.
Baseline (T1 to T2)
The baseline data was observed when the participants took part in computer activities as usual. All participants had a computer/tablet available at home or in school. As shown in , LiHao and ChiaYu occasionally used their personal eye-gaze device (i.e., Eye-tracker 4 C). ShuWen and YiFen used EGAT sporadically at a hospital in therapist-led treatment sessions. None of them received services to support their computer use at home or in educational environments.
The EGAT intervention (T2 to T4)
summarises the intervention content following the Template for Intervention Description and Replication (TIDieR) guide [Citation44]. The EGAT intervention, which included eye-gaze devices and collaborative service delivery, focussed on facilitating the use of EGAT to participate in computer activities such as playing, communication, and school tasks in daily contexts. Seven key elements were encompassed: (1) getting access to an eye-gaze device with adapted and personalised software; (2) participating in computer activities via EGAT at least three days per week; (3) fitting the activity content to a child’s interests, and (4) adjusting the difficulty level to keep a child motivated; (5) implementing computer activities based on the predefined goals; (6) parents/teachers providing support and interacting with the child during his/her use; and (7) collaboration among parents, teachers and therapists to monitor the child’s progress and modify strategies.
Table 2. The EGAT intervention content.
Device and personalised content
The participants used the Tobii PCEye Mini (Tobii Dynavox Ltd.) during the intervention phase. It is an add-on eye-gaze device system for a laptop computer with 12 or 14 screen dimensions and a Windows environment. The PCEye Mini has higher accuracy and primary use for computer access and communication, compared to Eye-tracker 4 C, which is mainly for gaming and basic Windows interaction. The laptop with the device was mounted on the desk with an adjustable table mount. EGAT software, HelpKidzLearn (Inclusive Technology Ltd.), or Look to Learn (Tobii Dynavox Ltd.) included play/leisure programs to target different eye-control activities. Each participant received an individualised program (i.e., Communicator 5 [Tobii Dynavox Ltd.]) tailored to their individual needs and preferences, including adapted communication pages (e.g., choices, feelings), leisure activities (e.g., music, photos), and learning tasks (e.g., naming, reading).
Service delivery
The collaborative team included (1) parents/teachers to implement the intervention in everyday contexts; (2) the participants’ therapists to support implementation and problem-solving; and (3) the researcher to support parents, teachers and therapists in the use of EGAT and to facilitate information exchange.
Service delivery involved a collaborative approach to problem identification, joint goal-setting and intervention planning, and joint review progress. Before the intervention, participants’ information related to the EGAT service was gathered, including their functions, preferences, routine activities, positioning needs, and environmental settings. Following this, the researcher interviewed parents/teachers using the Canadian Occupational Performance Measure (COPM, see outcome measures) to identify two to three prioritised activities that their children/students could perform using the EGAT based on each child’s motivation and interests. The six-month intervention started with a planning meeting to set up goals using Goal Attainment Scaling (GAS, see outcome measures) and to formulate an individualised plan. The predetermined goals were connected to an individualised education programme in educational settings. Next, parents/teachers received individualised support on the use of EGAT every two weeks. One follow-up meeting was held after a three-month intervention to evaluate goal progress and adjust strategies.
Parents/teachers were trained in how to operate the EGAT system, as well as positioning for the participant and the computer’s ergonomic setting. They were given an EGAT manual to enhance use of the device and software. In addition, they were taught strategies to offer the children communication opportunities and models and to respond to attempts to support user communication/interactions via the EGAT. Due to the impact of the COVID-19 pandemic from January to April 2020, individual support was modified such that it involved a hybrid method combining physical visits and teleconsultation with the same frequency.
Context
LiHao and ShuWen used EGAT at home. ChiaYu used the EGAT at school predominantly except for one-and-a-half months at home on winter holidays and the school closure period due to the COVID-19 pandemic. YiFen used the EGAT at home and once a week at the child development centre where it provides pre-school special education and early intervention programmes for children with disabilities.
The therapists (two PTs, one OT, and two SLPs) had 2.5–25 years of experience working with children with complex needs and were trained on AT assessments and applications. They had 0–1.5 years of experience with EGAT services. The teachers had three to 15 years of experience working with students with complex needs and zero to two months of experience with eye-gaze devices.
Maintenance phase (T4 to T5)
A one-month maintenance phase was implemented after the EGAT intervention to assess whether participation in computer activities in daily contexts had been maintained. The condition of eye-gaze devices was the same as the baseline phase.
Treatment integrity
The fidelity checklist included items covering seven key elements described in the EGAT intervention to evaluate the extent to which they implemented the intervention with fidelity. The assessment used a three-point scale (2 = always, 1 = sometimes, 0 = none). The first author examined the treatment integrity once a month primarily by interviewing the therapists, supplemented by field observations on some items during home/school visits. The parents/teachers were interviewed when the therapists reduced direct observation of the participants’ use due to the pandemic. The percentage was computed by summing each item's score and dividing this by the maximum total scores. The overall integrity throughout the intervention revealed high integrity, with 93–96% in four participants. The integrity of implementing each intervention element was 83–100% for all items, except for Item 2 (participating in computer activities via the EGAT at least three times per week), with lower integrity of 50–83%. For this item aspect, parents and teachers were reinstructed to provide regular opportunities for computer use with support from therapists on possible adjustments in execution.
Summative outcome measures
The continuous dependent variable was participation in computer activities, assessed through a computer use diary. Social validity measures to determine the social importance of the intervention’s effects [Citation36] included (a) achievements of predefined goals by GAS and (b) parents/teachers’ ratings on the children’s performance and their satisfaction with the children’s performance via the COPM.
Participation in computer activities
Participation in computer activities was defined as the children actively performing and interacting with computers via an access method, such as eye-gaze technology. A computer use diary, developed and examined in previous EGAT studies [Citation5], was used. This diary encompassed (1) diversity of computer activities, to document the types of predefined activities engaged in each day (e.g., playing games, talking to someone), with possibilities to add additional activities (e.g., naming objects); (2) the number of uses per day; and (3) the duration of participation in computer activities (minutes/day) for each activity and the total duration in a day. Parents/teachers were instructed to document computer activity participation each day, from baseline continuously to the intervention and maintenance phases.
Inter-assessor reliability
Diary data was validated with log data from the FocusMe program (FocusMe Inc., London, UK), which is software that displays the amount of time spent and the types of apps/software used on the computer each day. The agreement was defined as minutes per user day documented in the diary equal to or less than the minutes recorded by the FocusMe program since the program noted every user’s data including the time when the stakeholder adjusted the content. A difference within ten minutes per user day was defined as acceptable given the human estimation. When the participants used the EGAT at the clinic, the diary data were compared with the log data from the therapists. The percent agreement showed acceptable inter-assessor reliability [Citation45], with 100% in duration of computer use and diversity of activities, based on 50–100% user days at baseline, and 77.8–89.3% in duration of computer use and 89.3–100% in the diversity of activities, grounded in 23–100% user days at the intervention phase.
Goal attainment scaling (GAS)
The collaboration team used GAS to set individualised, measurable goals [Citation46]. The instrument was based on a five-point response scale as follows: −2 = baseline or a child’s present level of performance; −1 = progress but less than the expected outcome; 0 = expected level of the outcome; +1 = somewhat more than expected, +2 = much more than the expected outcome [Citation47]. A score of zero represented improvement consistent with the predetermined level of performance [Citation46]. The GAS has good responsiveness [Citation48] and content validity [Citation49]. At T2, T3, and T4 (), a trained independent tester evaluated GAS based on field observations and information from parents/teachers and therapists.
Canadian occupational performance measure (COPM)
The COPM [Citation50] was used as a proxy report to identify and prioritise important daily activities. The parents and teachers rated each activity according to their perception of the child’s performance and their satisfaction with the child’s performance, using the performance and satisfaction scales [Citation51]. The rating score ranged from 1 (poor performance, low satisfaction) to 10 (good performance, high satisfaction). The measure has acceptable to good internal consistency in parent proxies (Cronbach’s alpha = 0.73, 0.82) and good construct validity and responsiveness [Citation50,Citation51].
At T2, T3, and T4 (), the independent tester held interviews with parents/teachers to evaluate their ratings for the identified activities. They were blinded to the previous scoring [Citation52], and a narrative description of their observation of each child’s changes was documented.
Analysis
Participation in computer activities was analysed and presented to show (1) the diversity of activities; (2) the frequency of use (days with use in percent); and (3) duration (total minutes per user day). Days excluded for analysis were when the participant or his/her parent was sick, the device was broken, the family was on holiday, or on weekend days when the participant only used the EGAT in school during the intervention phase (i.e., ChiaYu). Descriptive statistics (mean, SD, range) were computed for each variable at each phase.
Daily usage and the duration of participation in computer activities were graphed per day for each participant for visual inspection. On the graph, the data presentation changed from individual data to data for a week after 50 days for ease of presentation due to the long intervention and space constraints. Criteria for visual inspection contained level (i.e., mean) changes across phases, variability differences across phases, the immediacy of the effect, and consistency in the overall pattern [Citation38,Citation53]. The mean of the data points within a phase was calculated and then compared across phases. The range (high minus low data points) in each phase indicated the extent of variability. The immediacy of the effect [Citation36] was examined by projecting a split middle trend line at baseline into the first three data points of the intervention phase and comparing the predicted data to the actual data points for the first three days. Consistency in the overall pattern entailed determining the extent to which the data patterns across phases remained similar.
Supplementary to visual analysis, restricted maximum likelihood estimation (REML) was used to obtain design-comparable effect sizes for group effects [Citation54] via a web calculator (https://jepusto.shinyapps.io/scdhlm/) [Citation55]. REML has the advantages of using hierarchical linear models, less restricted assumptions for between-case variations, and unbiased effects with at least three participants [Citation56]. Concerning no obvious trends and the parsimonious assumption in the small sample, a model was selected with varying intercepts, varying intervention effects, and no trends [Citation54], allowing for the assumption that the intervention effect varied across participants. Interpretation of the effect size involved the benchmark of Cohen’s d at 0.2 (small), 0.5 (medium), and 0.8 (large) [Citation54].
Descriptive analysis reported the number of achieved goals (GAS≧0) and presented the changes in the average score (range: 1–10) on the two scales of COPM at T3 and T4 from T2. A score change of two points or more on the COPM indicates clinically important differences [Citation50].
Results
The results were structured to first present the outcomes of participation in computer activities for each participant, with demonstrating computer usage at each phase and demonstrating visual inspection of the duration of computer use (Daily data graphs for each participant are presented in supplement 1 to show variability). Furthermore, the goal achievements by GAS assessment and the changes in COPM ratings are presented in .
Figure 2. Duration of participation in computer activities for each participant. Note. Data were aggregated from daily to weekly average after 50 days because of space constraints. Zero performance days of data mean that the computer was available, but the participants did not use it. A hatch mark (//) indicates interruption (that is days when the intervention was usually followed but there was no opportunity because the computer was not available to the children). Horizontal solid line (blue) = level (mean) at each phase. Horizontal dash line (red) = split middle trend line at baseline. This graph displayed that ChiaYu, ShuWen, and YiFen showed a clear level (mean) change from baseline to the intervention phase, and the immediacy of effects was evident. LiHao only showed a small level change across phases, and there was no immediacy of response to the intervention.
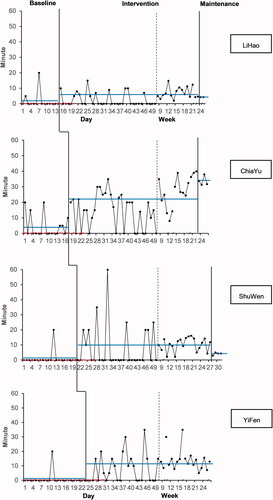
Table 3. Computer usage at baseline and the intervention phases.
Table 4. GAS scores and the score changes of the performance and satisfaction scales of COPM at T3 and T4.
Participants performed computer activities with varied numbers of pictures/symbols on computer pages of the play, communication or learning activities, as shown in the Appendix. In general, there were 2–12 pictures per activity page and 2–6 symbols per communication page. There was an increase in the total number of symbols/pictures from the beginning (46–111 pictures/symbols) to the end of the intervention (69–204 pictures/symbols).
Participation in computer activities
Participant 1: LiHao
LiHao used the computer to play games during baseline (diversity of activities = 1) and increased the diversity of activities during the intervention phase: playing games, playing music/videos, watching photos, making choices/communicating, performing learning tasks, and using an activity calendar (n = 6). As shown in , LiHao increased the frequency of use from baseline to the intervention phase (14–37%, 1–2.5 days). He mostly used the EGAT once per user day.
During the baseline, LiHao performed computer activities twice, with durations of 5 and 20 min. Throughout the intervention phase, LiHao slightly increased the duration of computer use, with a mean duration of 16.2 min per user day (SD = 11.59). LiHao exhibited a longer duration of computer use from T3 to T4 (mean = 21.3 min, SD = 11.57) than T2 to T3 (mean = 12.4 min, SD = 10.13). A small level change across phases (mean difference = 4.14) is displayed in . There was greater variability during the intervention phase than during the baseline phase (range = 56 min vs. 15 min). There was no immediacy of response to the intervention.
During the maintenance phase, LiHao performed play activities and listened to/watched music/videos using his eye-gaze device. He decreased the frequency of computer use (1.3 days/week on average), with a mean duration per user day of 12 min (SD = 4.47, range = 10–20 min).
Participant 2: ChiaYu
During the baseline phase, ChiaYu interacted with a computer to play games or name objects in a language lesson (n = 2). During the intervention phase, she increased her diversity of activities, encompassing choice-making/communication, responding to learning tasks in the language class, counting in a maths lesson, and occasionally playing videos, games, and looking at photos (n = 6).
ChiaYu increased the frequency of use from baseline to the intervention phase (35–71%, 2–3.1 days/week) (). She used the EGAT more frequently during the intervention (mean = 2.2 times [SD = 0.71] per user day) than during the baseline phase (once per user day).
During the baseline, ChiaYu performed computer activities with a mean duration of 14.7 min per user day (SD = 7.26). Throughout the intervention phase, ChiaYu increased the duration of computer use by a mean of 30.8 min per user day (SD = 11.71). ChiaYu had a longer duration of use from T3 to T4 (mean = 36.6 min, SD = 9.78) than T2 to T3 (mean = 24.5 min, SD = 10.37). As shown in , she demonstrated a clear change in levels across phases in the duration of computer use (mean difference = 17.12), although there was a large variability during the intervention phase compared to the baseline phase (range = 55 min vs. 15 min). The immediacy of effects was evident once the EGAT was implemented.
During the maintenance phase, ChiaYu used her eye-gaze device for choice-making/communication, and language and maths lessons. She increased participation in computer activities to four days per week on average and increased the duration of computer use per user day (mean = 34.1 min, SD = 5.54, range = 25–45 min).
Participant 3: ShuWen
During baseline, ShuWen used a computer with the EGAT to play games and look at photos (n = 2), and increased her diversity of activities during the intervention phase, including playing games, choice-making/communication, looking at photos, and playing music/watching videos (n = 4).
ShuWen increased the frequency of use from baseline to the intervention phase (5–34%, 0.3–2.2 days/week). She mainly used the EGAT once per user day (mean = 1.1, SD = 0.31). During baseline, ShuWen performed computer activities once for a duration of 20 min. Throughout the intervention phase, she increased the duration of computer use, with a mean of 29.4 min per user day (SD = 11.03). She also demonstrated a more extended duration of use from T3 to T4 (mean = 35 min, SD = 9.81) than T2 to T3 (mean = 24.6 min, SD = 9.80). As shown in , ShuWen exhibited a clear level change across phases in the duration of use (mean difference = 8.91), but the variability was large during the intervention phase (range = 50 min). Immediate effects of the intervention were observed.
During the maintenance phase, she used computers for the same activities as in the intervention phase. She did not have a personal device and thus used the EGAT once a week in a hospital setting. She slightly decreased the duration of computer use (mean = 28.8 min per user day, SD = 6.29, range = 25–35 min). ShuWen’s parents met the teacher at the child centre to discuss a further arrangement to use the EGAT in the classroom.
Participant 4: YiFen
YiFen used a computer to play games only (n = 1) during the baseline phase and increased her diversity of activities during the intervention phase, encompassing playing games, listening to music/watching videos, and choice-making/communication (n = 3).
YiFen increased the frequency of use from baseline to the intervention phase (4–50%, 0.3–3.2 days/week on average). She mostly used the EGAT once per user day (mean = 1.01, SD = 0.12). During baseline, YiFen performed computer activities once for a duration of 20 min. Throughout the intervention phase, she increased the duration of computer use by a mean of 22.8 min per user day (SD = 8.92). She showed slightly prolonged use from T3 to T4 (mean = 25 min, SD = 8.31) than T2 to T3 (mean = 20.9 min, SD = 9.09). In , YiFen displayed a level change across phases in the duration of use (mean difference = 10.5), although there was large variability during the intervention phase (range = 40 min). There was an immediacy of response to the intervention. During the maintenance phase, YiFen did not have access to the EGAT and hence did not perform computer activities. Her parents decided to apply for a personal device and received assistance from the SLP.
Group results
All participants demonstrated an increase in the diversity of activities from baseline to the intervention phase (between one to two and three to six activities). The most common computer activities the children performed were playing games and communication. The participants exhibited an increased frequency of use, from baseline to the intervention phase (0.3–2 days/week and 2.2–3.2 days/week). All participants displayed a longer duration of computer use in the second half of the intervention than in the first half of the intervention. In , three participants (except for LiHao) showed positive changes in the duration of computer use and consistent patterns across phases when the EGAT was implemented, despite considerable variability during the intervention phase. ChiaYu also demonstrated an increase in computer use duration during the maintenance phase.
REML model estimates indicated moderate group effects, with a between-case standardised mean difference equal to 0.76 (standard error = 0.23, 95% confidence interval = 0.31–1.21, degrees of freedom = 327.8, autocorrelation = 0.05). The positive effects on the duration of computer use, from visual inspection and statistical analysis, coincided with manipulation of the independent variable, demonstrating a functional relationship [Citation35,Citation36] between the EGAT and participation in computer activities.
Social validity: goal achievements and parents’ and teachers’ ratings
As presented in , six of eight predetermined goals were achieved, including goals related to play (n = 3/3), choice-making/communication (n = 2/4), or school learning tasks (n = 1/1) with adults’ verbal prompts. Examples of the predefined goals are as follows: (a) Play: During playtime/leisure, LiHao can engage in computer play activities for at least 10 min each time; (b) Choice-making/communication: ShuWen can purposefully choose activities/objects she wants from the communication pages in four situations daily; (c) School learning tasks: ChiaYu can use the EGAT to respond to learning tasks in the language lesson, pointing out 10 pictures correctly.
LiHao attained the first goal of engagement in computer play activities but did not reach the expected level for the second goal (GAS= −1, purposefully choosing objects/activities three to four times daily). ChiaYu achieved both goals at the end of the EGAT intervention, choosing activities during school lessons and recess time, and responding to learning tasks for a language lesson. ShuWen attained both goals at the end of the EGAT intervention in terms of engagement in computer play activities and choice-making for activities/objects in daily contexts. The second goal was achieved beyond expectations (GAS= +1, choosing a daily activity in at least five situations). YiFen attained the first play goal but did not reach the second goal (GAS= −1, purposefully choosing activities/snacks in one situation daily).
Parents’ and teachers’ ratings on the child’s performance revealed clinical significance for all participants at T4 (a score change of performance scale on the COPM for LiHao, ChiaYu, ShuWen and YiFen at 7, 3.3, 2, and 4.5, respectively) (). Their satisfaction ratings with the children’s performance reached clinical significance for LiHao, ChiaYu and YiFen (a score change on the satisfaction scale of the COPM at T4 at 8.5, 2.5, and 5, respectively), except for ShuWen (score change = 1.5).
Discussion
To the best of our knowledge, this study is one of the few studies using a single-case research design to demonstrate the effects of applying EGAT in everyday contexts. Four young children with complex needs and low eye-control skills demonstrated increased participation in computer activities when the EGAT was implemented. Three participants exhibited a substantial change and an immediate effect in the duration of computer use. The results met the criteria for causal inference in single-case designs with at least three demonstrations (i.e., participants) at three points in time [Citation38], indicating that the changes in computer participation can be attributable to the EGAT intervention. Moreover, the evaluation for social validity supplemented the experimental findings in which participants achieved (fully or partially) predefined goals that were socially important, and the teachers and parents perceived the children’s improvement to be meaningful.
Increase in computer activity participation
The findings supported two earlier intervention studies [Citation5,Citation6], regarding improved diversity of computer activities, and the frequency and duration of computer use after introducing EGAT, although the young participants in the present study had lower eye-control skills initially and all had cognitive impairments. These findings are encouraging since the young children had previously encountered many challenges in participation in activities. The results demonstrated similar findings of increased diversity of computer activities (n = 3–6 vs. mean =3.8 [7] and mean = 4.1 [8]) with playing games and communication/making choices as the most common activities, demonstrating that these activities were appropriate and doable for young novice users.
The increased duration of computer use entailed that the children showed an extended time to actively perform and get involved in activities for play, communication, or learning via EGAT. This finding could indicate that the children demonstrated a willingness to use this new technology within everyday contexts and increased engagement in computer activities over time. Nevertheless, compared with previous studies [Citation5,Citation6], the participants showed lower frequencies (2.2–3.2 days/week vs. weekly to daily use) and shorter durations per user day (mean = 25 min vs. 40 or 70 min per user day). It was noted that low frequencies of use (i.e., low exposure) might make it difficult for these children to use EGAT spontaneously for communication or other activities and in many situations. The children usually used EGAT on one or two occasions per day, and still, the activity diversity increased. Different findings could be explained by the participants’ characteristics, the technology system, and opportunities of use.
As regards the participants’ characteristics, the children had younger ages on average and demonstrated weaker eye-control skills and fewer eye-pointing experiences than those in an earlier Swedish study [Citation28], which may impact their attention span and endurance when starting computer use. This study indicates that 20–30 min each time might be optimal for these young beginners to maintain attention and engage in computer activities without fatiguing and negatively impacting their motivation and performance. The findings revealed that eye-pointing for communication could be critical for learning to use EGAT. Practicing gaze fixations and gaze shifts to direct a communication partner’s attention to an object [Citation31], can be generalised to EGAT operation; for example, purposefully pointing at graphic symbols/pictures on a screen to communicate with teachers. Therefore, service delivery could incorporate this skill training (gaze fixation and gaze shifts) to enhance future EGAT use.
For the technology system, added-on EGAT with a laptop might require more time to set up and calibrate compared to all built-in devices, in which all components are integrated within a single system [Citation11]. Due to the high cost and extensive self-funding of all-in-one devices in Taiwan, their use was not investigated. Moreover, a device with a table stand might limit portability within and across environments. These factors may be attributes regarding the frequency of use based on stakeholders’ feedback, indicating that the convenience of an eye-gaze system is crucial for teachers and parents.
Moreover, children with complex needs depend on the adults setting up opportunities for EGAT use and positioning them in front of computers [Citation6,Citation57]. ChiaYu’s teacher integrated eye-control activities into different school activities, and YiFen used the EGAT both at home and in the centre; thus, their frequency of use increased. The findings suggest that it is imperative to support parents/teachers in embedding EGAT use into daily routines to provide regular (but short) sessions to increase exposure, thus enhancing opportunities for use and skill acquisition. A forthcoming study will further investigate what impacts the provision of frequent opportunities for computer use based on stakeholders’ perceptions and experiences when supporting the child in everyday contexts.
Positive impacts on technology usability
The participants achieved all goals related to play, indicating that the children could use the EGAT to participate in play/leisure, gradually increasing independence. Engagement in play activities and having fun are critical for early learners to comprehend gaze-computer interaction, learn eye-control skills, and gain motivation to explore other computer activities. The positive outcome might be related to the increasing duration of computer use during T3–T4 for all participants. From a transactional perspective [Citation58], children’s engagement in play might also influence the engagement of parents/teachers when supporting their use, towards a positive interaction. From field notes, parents/teachers recognised these meaningful changes, reporting that the participants exhibited increased active responses during the interactions as well as independence when performing these activities rather than relying completely on adults’ assistance.
ChiaYu and ShuWen achieved their communication goals. LiHao and YiFen showed progress but did not attain the expected outcomes. The results indicate that the EGAT enabled children with communication difficulties to make choices to communicate their wants and to demonstrate self-determination in daily activities. This echoes a recent finding, reporting that children could benefit from using EGAT to enhance communication skills and to communicate information intelligibly [Citation6,Citation11,Citation30], which could have a long-term impact on their learning and development. Nevertheless, children with visual impairments and weak eye-control skills, such as LiHao and YiFen, might require an extended time to build gaze control skills and learn to operate an alternative communication system. Recent studies suggest that AAC exposure to augmented communication learning and adult modelling affect a child’s augmented expressive communication [Citation33,Citation59]; this highlights the importance of providing daily communication opportunities and scaffolding EGAT use as a means of communication. Further training on communication strategies for parents/teachers, along with team support [Citation9,Citation33,Citation60], would be critical to enhance communication outcomes. Although it would only be a small step, children expressing their wants or needs intelligibly could be meaningful for parents/teachers to discover the child/student’s abilities and interests for future learning.
For clinical implications, in line with recent guidelines for EGAT [Citation32], it is necessary to evaluate individual functioning and needs and the child’s environment to develop individualised goals for EGAT use. For children with dyskinetic CP, appropriate positioning to reduce the interference of involuntary movements and fatigue would be critical since their comfort impacts their performance and eye stamina. It is recommended to gradually increase the duration of use (e.g., 20–30 min) but use EGAT every day. As children with dyskinetic CP commonly have unstable gaze fixations, particularly when visual impairments coexist [Citation27], starting an activity where children are motivated and could actively participate (e.g., playing games) is paramount for building familiarity with gaze computer interaction and reducing frustration. With increasing gaze control skills, they can exercise a broader range of activities to maximise the benefits of using EGAT for play, communication, and learning. Additionally, follow-up services are essential to support parents/teachers on EGAT implementation and to facilitate technology uptake.
Limitations
This study used a non-concurrent multiple baseline design, which might not be as robust as the concurrent version of this design [Citation36]. To improve the internal validity, a previously identified baseline and randomisation of the onset of the intervention phase were employed for each participant [Citation37,Citation61]. However, the short interval for the staggered onset of intervention might be a constraint, given the lack of opportunity to observe the effects before proceeding to the next participant’s intervention. The reason for choosing a three-day interval was practical since it reduced the waiting time and possible attrition. However, a longer delay in the onset of the intervention between participants would provide a more robust basis from which to draw inferences.
Wide variability in the duration of computer use was noted. The considerable variability might be related to the performance characteristics in this unique group since their health conditions and multiple disabilities might result in fluctuating performance on a daily basis [Citation16,Citation17]. The variability was also associated with the opportunities parents and teachers provided each day. Concerning the variability, this study included an extended intervention phase to observe the pattern of responses.
An additional limitation was that the presence of eye-gaze devices during the baseline differed among participants. However, according to the visual graphs, the device alone did not make apparent differences, nor did it indicate effectiveness for LiHao and ChiaYu, and these facts represent a rationale for implementing an EGAT intervention. The finding indicates that the EGAT service, and not just providing the technology, is critical to support the use of EGAT.
This study assessed treatment integrity using interviews with partial items validated by field observations. The intervention conducted in everyday settings made it challenging to observe the implementation of all items, and video recording was judged as disruptive for parents/teachers. However, it should be noted that the interview approach might be more susceptible to bias than observation data, even though it has advantages of clarifying implementation issues and offering immediate feedback on intervention adjustments [Citation62].
Lastly, the results could only be generalised to similar participant characteristics and with a specific collaborative team service. Further research is needed, for example, at least five single-case research design studies by independent research groups with at least 20 cases and meta-analysis studies to enhance external validity and inform evidence-based practice [Citation34,Citation36]. The small population presented a challenge in establishing evidence with statistical power [Citation6]. With knowledge progress and an increasing number of children with access to EGAT, future large-scale intervention studies could be made possible to strengthen the effectiveness of EGAT and improve generalisation.
Conclusion
This study adds knowledge that, with sufficient practice, children with complex needs and low eye-control skills benefit from using EGAT to increase the diversity of computer use by involving three to six different activities. They showed an increased frequency (although not daily) and duration of computer use, with about half an hour per user day after applying EGAT for three months (research question 1). This study, using a single-case research design, strengthens the evidence for the effects of EGAT application in everyday contexts in an Asian context. The findings support the usability of EGAT at home and in educational environments for children with complex needs to attain play, communication or learning goals (question 2), with support from stakeholders and collaborative service. The parents and teachers expressed satisfaction with the children’s change in performance (question 3). Overall, the findings suggest that EGAT is a useful method to enhance children’s participation and learning potential and can be introduced at early ages to facilitate their computer use.
Given that the availability and funding for EGAT may differ among cultural contexts, future studies are critical to investigate facilitators and barriers for the effective use of EGAT to support the recommendations for EGAT provision. Long-term follow-up studies are needed to provide insights into sustained effects.
Supplementary_material_revised.docx
Download MS Word (72.9 KB)Acknowledgement
The authors would like to thank all participants, parents, teachers and therapists for participating in this study, and the chiefs in schools, child developmental centres, and rehabilitation hospitals to support this study. We are grateful to Tobii and Boyang Medical Technology for supporting the eye-gaze device and software, assisting the workshop practicum for service providers, and providing technical assistance during the study period.
Disclosure statement
The authors report no conflict of interest. The research team borrowed an eye-gaze device and software from Tobii and Boyang Medical Technology companies during the intervention phase. The companies had no role in the study protocol and study execution.
Additional information
Funding
References
- Hasselbring TS, Glaser CH. Use of computer technology to help students with special needs. Future Child. 2000;10(2):102–122.
- MacLachlan M, Banes D, Bell D, et al. Assistive technology policy: a position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil Rehabil Assist Technol. 2018;13(5):454–466.
- Tebbutt E, Brodmann R, Borg J, et al. Assistive products and the sustainable development goals (SDGs). Global Health. 2016;12(1):79.
- World Health Organization. International classification of functioning. In: Disability and health: children & youth version (ICF-CY). Geneva: WHO; 2007.
- Borgestig M, Sandqvist J, Ahlsten G, et al. Gaze-based assistive technology in daily activities in children with severe physical impairments- an intervention study. Dev Neurorehabil. 2017;20(3):129–141.
- Borgestig M, Al Khatib I, Masayko S, et al. The impact of eye-gaze controlled computer on communication and functional independence in children. Dev Neurorehabil. 2021;24(8):511–524.
- Hemmingsson H, Borgestig M. Usability of eye-gaze controlled computers in Sweden: a total population survey. IJERPH. 2020;17(5):1639.
- Karlsson P, Bech A, Stone H, et al. Eyes on communication: trialling eye-gaze control technology in young children with dyskinetic cerebral palsy. Dev Neurorehabil. 2019;22(2):134–140.
- van Niekerk K, Tönsing K. Eye gaze technology: a South African perspective. Disabil Rehabil Assist Technol. 2015;10(4):340–346.
- Vessoyan K, Steckle G, Easton B, et al. Using eye-tracking technology for communication in Rett syndrome: perceptions of impact. Augment Altern Commun. 2018;34(3):230–241.
- Lui M, Maharaj A, Shimaly R, et al. User experiences of eye gaze classroom technology for children with complex communication needs. J Spec Educ Technol. 2021. doi:10.1177/01626434211019399.
- Karlsson P, Allsop A, Dee-Price BJ, et al. Eye-gaze control technology for children, adolescents and adults with cerebral palsy with significant physical disability: findings from a systematic review. Dev Neurorehabil. 2018;21(8):497–505.
- Perfect E, Hoskin E, Noyek S, et al. A systematic review investigating outcome measures and uptake barriers when children and youth with complex disabilities use eye gaze assistive technology. Dev Neurorehabil. 2020;23(3):145–159.
- Ministry of Health and Welfare. Taipei: Laws & Regulations Database of The Republic of China; 2021. Regulations on Subsidization for Medical Treatment and Auxiliary Appliances for the Disabled. [updated 2012 Jul 9; cited 2021 Aug 30]. Available from: https://law.moj.gov.tw/LawClass/LawAll.aspx?pcode=D0050060.
- Hwang CS, Weng HH, Wang LF, et al. An eye-tracking assistive device improves the quality of life for ALS patients and reduces the caregivers burden. J Mot Behav. 2014;46(4):233–238.
- Patel DR, Neelakantan M, Pandher K, et al. Cerebral palsy in children: a clinical overview. Transl Pediatr. 2020;9(Suppl 1):S125–S135.
- Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007;109:8–14.
- Raghavendra P, Virgo R, Olsson C, et al. Activity participation of children with complex communication needs, physical disabilities and typically-developing peers. Dev Neurorehabil. 2011;14(3):145–155.
- Kang LJ, Hsieh MC, Liao HF, et al. Environmental barriers to participation of preschool children with and without physical disabilities. IJERPH. 2017;14(5):518.
- Mei C, Reilly S, Reddihough D, et al. Activities and participation of children with cerebral palsy: parent perspectives. Disabil Rehabil. 2015;37(23):2164–2173.
- Dhondt A, Van Keer I, van der Putten A, et al. Communicative abilities in young children with a significant cognitive and motor developmental delay. J Appl Res Intellect Disabil. 2020;33(3):529–541.
- Horn EM, Kang J. Supporting young children with multiple disabilities: what do we know and what do we still need to learn? Topics Early Child Spec Educ. 2012;31(4):241–248.
- Noyek S, Vowles C, Batorowicz B, et al. Direct assessment of emotional well-being from children with severe motor and communication impairment: a systematic review. Disabil Rehabil Assist Technol. 2022;17:501–514.
- Stadskleiv K. Cognitive functioning in children with cerebral palsy. Dev Med Child Neurol. 2020;62(3):283–289.
- Wadhera T, Kakkar D. Eye tracker: an assistive tool in diagnosis of autism spectrum disorder. In: Gupta SK, Venkatesan S, Goswami SP, et al. editors. Emerging trends in the diagnosis and intervention of neurodevelopmental disorders. Hershey (PA): IGI Global; 2019. p. 125–152.
- Majaranta P, Donegan M. Introduction to gaze interaction. In: Majaranta P, Aoki H, Donegan M editors. Gaze interaction and applications of eye tracking: advances in assistive technologies. Hershey (PA): IGI Global; 2012. p. 1–9.
- Bekteshi S, Konings M, Vanmechelen I, et al. Eye gaze gaming intervention in children with dyskinetic cerebral palsy: a pilot study of task performance and its relation with dystonia and choreoathetosis. Dev Neurorehabil. 2020;23(8):548–556.
- Borgestig M, Sandqvist J, Parsons R, et al. Eye gaze performance for children with severe physical impairments using gaze-based assistive technology—a longitudinal study. Assist Technol. 2016;28(2):93–102.
- International Organization for Standardization. ISO 9241-11: ergonomics of human-system interaction—part 11: usability: definitions and concepts. Geneva: ISO; 2018.
- Hsieh YH, Borgestig M, Gopalarao D, et al. Communicative interaction with and without eye-gaze technology between children and youths with complex needs and their communication partners. IJERPH. 2021;18(10):5134.
- Clarke MT, Sargent J, Cooper R, et al. Development and testing of the eye-pointing classification scale for children with cerebral palsy. Disabil Rehabil. 2020;12:1–6.
- Karlsson P, Griffiths T, Clarke MT, et al. Stakeholder consensus for decision making in eye-gaze control technology for children, adolescents and adults with cerebral palsy service provision: findings from a Delphi study. BMC Neurol. 2021;21(1):63.
- Wandin H, Lindberg P, Sonnander K. Aided language modelling, responsive communication and eye-gaze technology as communication intervention for adults with Rett syndrome: three experimental single case studies. Disabil Rehabil Assist Technol. 2021:1–15. doi:10.1080/17483107.2021.1967469.
- Odom SL. Education of students with disabilities, science, and randomized controlled trials. Res Pract Persons Severe Disabl. 2021;46(3):132–145.
- Horner RH, Odom SL. Constructing single-case research designs: logic and options. In: Kratochwill TR, Levin JR, editors. Single-case intervention research: methodological and statistical advances. Washington (DC): American Psychological Association; 2014. p. 27–51.
- Kazdin AE. Single-case research designs: methods for clinical and applied settings. New York (NY): Oxford University Press; 2021.
- Watson PJ, Workman EA. The non-concurrent multiple baseline across-individuals design: an extension of the traditional multiple baseline design. J Behav Ther Exp Psychiatry. 1981;12(3):257–259.
- Kratochwill TR, Hitchcock JH, Horner RH, et al. Single-case intervention research design standards. Remedial Spec Educ. 2013;34(1):26–38.
- Tate RL, Perdices M, Rosenkoetter U, et al. The single-case reporting guideline in behavioural interventions (SCRIBE) 2016 statement. J Sch Psychol. 2016;56:133–142.
- Palisano RJ, Copeland WP, Galuppi BE. Performance of physical activities by adolescents with cerebral palsy. Phys Ther. 2007;87(1):77–87.
- Eliasson AC, Krumlinde-Sundholm L, Rösblad B, et al. The manual ability classification system (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol. 2006;48(7):549–554.
- Hidecker MJ, Paneth N, Rosenbaum PL, et al. Developing and validating the communication function classification system for individuals with cerebral palsy. Dev Med Child Neurol. 2011;53(8):704–710.
- Koester HH, Simpson RC, Spaeth D, et al. Reliability and validity of compass software for access assessment. In: Proceedings of RESNA 2007 annual conference. Phoenix, AZ. Washington (DC): RESNA Press; 2007. p. 16–19.
- Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687.
- Hartmann DP, Barrios BA, Wood DD. Principles of behavioural observation. In: Haynes SN, Heiby EM, editors. Comprehensive handbook of psychological assessment, vol. 3. Behavioural assessment. Hoboken (NJ): Wiley; 2004. p. 108–127.
- Kiresuk T, Smith A, Cardillo J. Goal attainment scaling: applications, theory, and measurement. Hillsdale (NJ): Lawrence Erlbaum Associates; 1994.
- Schlosser RW. Goal attainment scaling as a clinical measurement technique in communication disorders: a critical review. J Commun Disord. 2004;37(3):217–239.
- Steenbeek D, Gorter JW, Ketelaar M, et al. Responsiveness of goal attainment scaling in comparison to two standardized measures in outcome evaluation of children with cerebral palsy. Clin Rehabil. 2011;25(12):1128–1139.
- Palisano RJ. Validity of goal attainment scaling in infants with motor delays. Phys Ther. 1993;73(10):651–658. 1993
- Law M, Baptiste S, Carswell A, et al. Canadian occupational performance measure. 4th ed. Ottowa, ON: CAOT Publications ACE; 2005.
- Cusick A, Lannin NA, Lowe K. Adapting the Canadian occupational performance measure for use in a paediatric clinical trial. Disabil Rehabil. 2007;29(10):761–766.
- Wallen MA, Ziviani JM. Canadian occupational performance measure: impact of blinded parent-proxy ratings on outcome. Can J Occup Ther. 2012;79(1):7–14.
- Vannest KJ, Ninci J. Evaluating intervention effects in single-case research designs. J Couns Dev. 2015;93(4):403–411.
- Pustejovsky JE, Hedges LV, Shadish WR. Design-comparable effect sizes in multiple baseline designs: a general modelling framework. J Educ Behav Stat. 2014;39(5):368–393.
- Pustejovsky JE, Chen M, Hamilton B. scdhlm: A web-based calculator for between-case standardized mean differences (Version 0.5.2); 2021. [cited 2021 Aug 10]. Available from: https://jepusto.shinyapps.io/scdhlm.
- Manolov R, Moeyaert M, Fingerhut JE. A priori justification for effect measures in single-case experimental designs. Perspect Behav Sci. 2022;45:153–186.
- Rytterström P, Borgestig M, Hemmingsson H. Teachers’ experiences of using eye gaze-controlled computers for pupils with severe motor impairments and without speech. Eur J Spec Needs Educ. 2016;31(4):506–519.
- King G, Granlund M, Imms C. Measuring participation as a means: participation as a transactional system and a process. In: Imms C, Green D, editors. Participation optimizing outcomes in childhood-onset neurodisability. London: Mac Keith Press; 2020. p. 143–160.
- Barker RM, Romski M, Sevcik RA, et al. Intervention focus moderates the association between initial receptive language and language outcomes for toddlers with developmental delay. Augment Altern Commun. 2019;35(4):263–273.
- Granlund M, Björck-Akesson E, Wilder J, et al. AAC interventions for children in a family environment: implementing evidence in practice. Augment Altern Commun. 2008;24(3):207–219.
- Christ TJ. Experimental control and threats to internal validity of concurrent and nonconcurrent multiple baseline designs. Psychol Schs. 2007;44(5):451–459.
- Perepletchikova F, Kazdin AE. Treatment integrity and therapeutic change: issues and research recommendations. Clin Psychol Sci Pract. 2005;12(4):365–383.
Appendix Individualised content of EGAT use at the beginning and the end of the intervention phase