
ABSTRACT
Herpes zoster (HZ) is caused by reactivation of the varicella-zoster virus. The life-time risk of developing HZ is ~ 30%. Management of HZ can be challenging due to limited efficacy of oral antivirals on pain control, and neuropathic pain that may require aggressive management. Post-herpetic neuralgia (PHN) can cause substantial pain and occurs in up to one-quarter of patients with HZ. Up to 48,000 HZ cases are estimated to occur annually in Belgium, estimated to cost almost 7 million euros in treatment. The recombinant zoster vaccine (RZV, Shingrix, GSK) was approved in Europe in 2017. In 2022, the Belgian Superior Health Council recommended vaccination with RZV for immunocompetent adults aged ≥ 60 years, and immunocompromised patients aged ≥ 16 years, including those receiving immunosuppressive therapy, in particular Janus kinase inhibitors. RZV showed high age-independent efficacy in preventing HZ infection and in clinical trials that has since been confirmed in real-world effectiveness studies. In clinical trials, protection was sustained for at least 10 years after vaccination. As of 1 November 2023, RZV is reimbursed for three immunocompromised patient groups aged ≥ 18 years: malignancy treated in the past 5 years, HIV infection, and organ or haematological stem cell transplantation or are a transplant candidate. HZ is vaccine-preventable and RZV provides a highly effective tool for HZ prevention. While reimbursement for some at-risk groups is welcomed, reimbursement currently falls well short of Superior Health Council recommendations. Adult immunisation strategies should be promoted to achieve high vaccination coverage against HZ, contributing to healthy aging in Belgium.
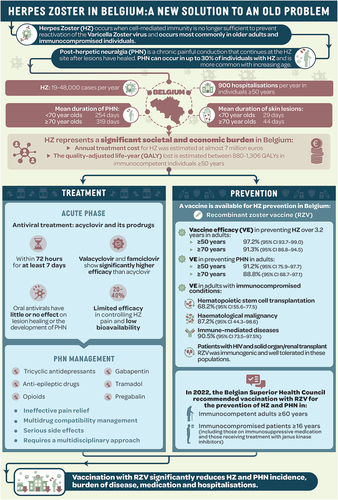
GRAPHICAL ABSTRACT
Plain Language Summary
What is the context?
Shingles (herpes zoster) is a common disease in adults that occurs more frequently as people age. The shingles’ rash is frequently intensely painful. Antiviral treatments and pain killers can help, but they are usually not fully effective in reducing pain or shortening the disease.
Shingles can be prevented in more than 90% of adults by vaccination.
What is new?
In 2022, the Belgian Superior Health Council recommended vaccination with recombinant zoster vaccine for immunocompetent adults aged ≥60 years, immunocompromised patients, including those receiving immunosuppressive therapy aged ≥16 years.
What is the impact?
Implementation of the new recommendations can be expected to lead to fewer cases of shingles and its most common complication – post-herpetic neuralgia. In turn, fewer patients will need prescriptions for antivirals, sedatives, and strong pain killers or other drugs with significant side effects.
Introduction
Herpes zoster (HZ) is a dermatomal rash caused by the reactivation of latent varicella zoster virus (VZV) residing within sensory ganglia. The rash is typically vesicular and painful, may be preceded by some days to weeks by a prodrome of flu-like symptoms or itching or pain within the affected dermatome. Pustules form over 48–72 hours, ulcerate and scab [Citation1]. Skin lesions persist for a mean of 29 days in <70 year-olds and 44 days in ≥70 year-olds [Citation2]. Around 50% of patients will experience a rash at the thoracic level, one third at the lumbar or cervical level, and around 13% will have a trigeminal presentation at high risk of ophthalmic complications [Citation3]. Approximately 90% of patients with HZ experience pain, which may be severe and unresponsive to simple analgesics [Citation4]. The cutaneous lesions resolve spontaneously, but long-term neuropathic pain (post-herpetic neuralgia [PHN]), resulting from inflammatory-mediated damage to peripheral and central neurons, can occur in up to 30% of individuals [Citation5,Citation6]. The life-time risk of developing HZ is 30% [Citation7].
HZ occurs when cell-mediated immunity is no longer sufficient to prevent VZV reactivation [Citation8]. The most important risk factor for declining cell-mediated immunity is progressive ageing of the immune system, a phenomenon called immunosenescence (BOX 1) [Citation9–11]. Besides advanced age, other risk factors for HZ include a family history of HZ, female sex, physical trauma including fracture or recent surgery, psychological stressors like stress or depression, some co-morbidities (diabetes or poor nutrition), and all forms of immunosuppression, particularly individuals infected with human immunodeficiency virus (HIV) with low CD4+ counts or uncontrolled viral load, and with drug-induced immunosuppression, specifically JAK inhibitors [Citation12–14].
Box 1. Immunosenescence is the major risk factor for developing shingles.
Immunosenescence refers to multi-faceted age-associated effects on innate and adaptive immunity that render older persons more susceptible to infectious diseases and their complications [9]. Key features of immunosenescence are age-related thymus atrophy with alterations at all levels of T cell functioning and reduced ability to respond to infections, lower phagocytic and macrophagic capacity, a reduction of naïve B and T lymphocytes and an increase of memory lymphocytes [10].
A reduction in plasma cells reduces the ability to produce antigen-specific antibodies, and a state of low-grade chronic inflammation (‘inflammaging’) results in high levels of pro-inflammatory cytokines and CD8+ T cells that predispose older persons to chronic disease, cancer, and infection [11].
Cell-mediated immune responses are necessary to prevent reactivation of varicella zoster virus over a lifetime. The gradual loss of T cell functioning as individuals age puts them at increasing risk of viral escape and herpes zoster disease.
PHN is prolonged neuropathic pain usually defined as present for 90 days or more after onset of the HZ rash. Older age, severe pain during the acute stage, severe prodromal symptoms, an extensive rash, and severe immunodeficiency, are risk factors for developing PHN [Citation15,Citation16].
Other complications of HZ can include secondary bacterial infection, pneumonia, neurological complications including sensory or hearing loss, encephalitis, vasculopathy leading to stroke, as well as disseminated disease, particularly in the immunocompromised individual [Citation17]. HZ ophthalmicus affects the first division of the trigeminal nerve and may be complicated by acute or chronic keratitis and iritis, neurotrophic keratopathy, PHN, or stroke. Chronic eye disease develops in approximately 25% of cases of HZ ophthalmicus [Citation18].
Epidemiology of HZ
Available data suggest that the epidemiology of HZ is similar all over the world [Citation7]. The annual incidence rate of HZ ranges between 40–50 per 10,000 person-years, but increases from < 30 per 10,000 person-years in those aged <60 years to > 100 per 10,000 person-years after the age of 80 years, with women more affected than men [Citation17,Citation19–21]. Immunocompromised persons are at increased risk of developing HZ; nevertheless, more than 90% of HZ cases occur in immunocompetent persons, and two-thirds of cases occur in individuals ≥50 years [Citation17,Citation19,Citation22]. HZ may recur in approximately 5% of individuals and is more common in patients with risk factors such as concurrent haematological malignancies and autoimmune disease [Citation23].
The epidemiology of HZ in Belgium mirrors that of other countries [Citation2,Citation7,Citation24]. Between 19,000–48,000 HZ cases are estimated to occur annually in Belgium, of which two-thirds are in individuals aged 50 years or older [Citation2,Citation22]. Around 900 individuals aged ≥50 years are hospitalised for HZ annually, and 63.2% of hospitalised patients were aged ≥70 years [Citation22]. The median length of stay was 9 days but ranged from 1–229 days. PHN occurred in up to 53% of hospitalised patients aged ≥80 years [Citation24]. Deaths due to HZ are infrequent (<1 per 100,000 person-years) but more common in older persons and immunocompromised patients [Citation6,Citation22]. The total annual treatment cost for HZ in Belgium was estimated at almost 7 million euros [Citation2]. Data from general practice (GP) sentinel surveillance in Belgium 2006 to 2012 reported a GP consultation rate for HZ of 335–432 cases per 100,000 person-years, with 58% of cases occurring in women. Consultation rates increased markedly with age, reaching 1738 per 100,000 person-years in individuals aged ≥90 years () [Citation25]. Surveillance re-started in 2021 and 2021–2022 data showed an incidence of HZ in Belgium of 168.5 per 100,000 person-years in the overall population. The reduced rate can be attributed to disrupted reporting during the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-COV-2) pandemic. The incidence of PHN was 61.1/100,000 person-years with a 58.9% of cases in patients aged 75 years and over [Citation26]. In a cohort of patients aged ≥50 years with HZ, 20.6% reported pain after 3 months, and 9.2% continued to have pain after 6 months [Citation27]. The mean duration of PHN in < 70-year-olds is 254 days, vs 319 days in ≥ 70-year-olds [Citation2].
Figure 1. Incidence (per 10,000 person-years) of consultations for herpes zoster by age group, 2006–2012, Belgian sentinel network of general practitioners (reproduced from Sabbe et al., with authorisation [Citation25]).
![Figure 1. Incidence (per 10,000 person-years) of consultations for herpes zoster by age group, 2006–2012, Belgian sentinel network of general practitioners (reproduced from Sabbe et al., with authorisation [Citation25]).](/cms/asset/ece1b51b-2d6e-4b76-ae11-9c5460bb42fb/yacb_a_2350258_f0001_oc.jpg)
Disease burden of HZ
HZ and PHN can have significant effects on quality of life, with a major impact on the performance of usual activities of daily living, such as self-care. Patients have increased rates of anxiety and depression and problems in social functioning. Furthermore, one-quarter of HZ patients experience a complication [Citation22,Citation28].
Acute HZ-related pain is variously described as burning, stinging, aching, throbbing, stabbing, itching, tingling, or shooting and may be intermittent or unrelenting [Citation4]. Patients can also experience allodynia (pain to stimuli that are not normally painful). The level of pain during the acute phase of HZ has been shown to directly affect patient wellbeing, including their general activity, ability to work, sleep and overall enjoyment of life [Citation4].
The individual, economic, and societal burden of HZ in Europe was captured in a systematic literature review [Citation29]. Adults aged ≥50 years with HZ had approximately 1.9 visits to their GP, while patients with PHN had 12 visits and 74% were referred to specialists. Work absenteeism due to HZ or PHN was common (up to 65% of employed persons) and was the major driver of indirect costs associated with HZ. In Belgium, the quality adjusted life years (QALYs) lost due to HZ is estimated to range between 880 and 1,306 in immunocompetent ≥ 50-year-olds [Citation22].
Pain severity was a significant predictor of the impact of HZ on individuals, healthcare systems and society [Citation29]. Compared to age-matched populations, patients with HZ and PHN demonstrated clinically relevant deficits across all health-related quality of life domains, with the largest impacts on bodily pain, vitality, social functioning, and mental health [Citation29]. Moderate anxiety or depression were reported by up to 29% of patients with HZ and 43% with PHN, and 50% of patients reported negative consequences for their family and social contacts [Citation29]. Aside from the impact of pain, the effects on quality of life of other symptoms of HZ, including fatigue, allodynia and numbness have not been explored. Furthermore, the impact of the illness on caregivers and partners, and the long term social and economic impacts of reduced physical functioning and loss of independence that may follow an episode of HZ, particularly in older persons [Citation4], have not been quantified.
The availability of data on the risk of recurrence of HZ after a first episode is still limited. The risk is 2–3% in the first 2 years but studies with longer follow-up periods report a risk of recurrence of 4–6% after 15 to 20 years [Citation6].
Treatment options for HZ and PHN
Antivirals
Management of HZ aims to relieve pain during the acute phase, to limit the duration and extent of the rash and to prevent complications. In Belgium, available antiviral treatments include acyclovir and its prodrug valacyclovir, brivudine, and penciclovir. Acyclovir resistance is exceptionally encountered in immunocompromised patients, requiring non-TK (thymidine kinase) dependent antiviral drugs such as foscarnet [Citation30]. TK-dependent drugs are nucleoside analogues that specifically block viral DNA replication in infected cells [Citation31]. Currently available oral antiviral drugs show limited efficacy (20–40%) in controlling HZ pain and are limited by their low oral bioavailability [Citation31]. Antivirals are most effective if started within 72 hours of the onset of the rash and need to be continued for at least 7 days. However, in 2021–2022, antivirals were prescribed to Belgian patients on average 11 days after symptom onset, highlighting the difficulty in starting treatment early [Citation26]. Antivirals reduce pain and shorten the duration of active viral replication, but have little or no effect on lesion healing or the development of PHN [Citation32].
Antiviral treatments are recommended in all immunocompromised patients with HZ, and in cases involving the trigeminal nerve [Citation33]. In these severe cases, patients are frequently referred to hospital for intravenous administration. Oral antiviral treatment may also be indicated for patients ≥60 years, in cases with clinically significant rash, and if pain precedes rash onset. Valacyclovir has better bioavailability and significantly higher efficacy than acyclovir in reducing pain associated with HZ, with a similar adverse event profile, but is more expensive than acyclovir [Citation34].
Management of HZ and PHN-associated pain
Pain management in HZ should be aggressive and guided by validated tools for the evaluation of pain severity. Treatment of pain should not be stepwise but appropriate medications should be started according to the severity of pain [Citation35]. Rates of opioid use are high (25%) during the acute disease phase [Citation36].
PHN is difficult to treat and in more difficult cases may require a multidisciplinary approach that includes pain specialists, dermatologists or ophthalmologists as well as psychological support [Citation17]. In frail older patients, a comprehensive geriatric assessment can be leveraged to prevent associated functional decline. Treatments found to be effective in pain management include tricyclic antidepressants, some opioids, tramadol, gabapentin, and pregabalin, and sometimes intrathecal lidocaine and steroids. Topical treatments include lidocaine 5% patch and capsaicin [Citation37]. Codeine, non-steroidal anti-inflammatory drugs, lorazepam, acyclovir, and some 5HT1 receptor agonists provide little or no pain relief in HZ [Citation37]. Overall, oral systemic treatments have only moderate impacts on PHN and their adverse effects can be significant, in particular amongst older persons, leading to non-compliance. Rates of treatment satisfaction are low in PHN [Citation4]. There is little information about PHN pain management in Belgium. In a cohort of 10 patients with PHN, seven received antiepileptic drugs (gabapentin or pregabalin), two received lidocaine or capsaicin dressing, and 1 received a tricyclic antidepressant [Citation26].
Options for prevention: HZ vaccines
Two vaccines have been approved for prevention of HZ. Both aim to boost VZV-specific cell-mediated immunity to prevent viral reactivation.
Live-attenuated HZ vaccine (ZVL or zoster-vaccine live: ZostavaxFootnote1, Merck & Co. Inc)
ZVL is a live attenuated viral vaccine composed of >19,400 plaque-forming units of the VZV Oka strain, which is the same viral strain included in Merck’s paediatric varicella vaccine, but at a higher dose (>1,350 plaque-forming units in the paediatric formulation) [Citation38,Citation39]. The vaccine is administered as a single intramuscular (IM) or subcutaneous dose.
ZVL was first approved by the European Medicines Agency and the US Food and Drug Administration in 2006 and is indicated for the prevention of HZ and PHN in adults aged ≥50 years. It is contraindicated in persons with primary and acquired immunodeficiency, those receiving immunosuppressive therapy, persons with active untreated tuberculosis and during pregnancy [Citation39]. The production and marketing of ZVL has halted in many parts of the world.
In randomised controlled trials, ZVL demonstrated significant vaccine efficacy (VE) (69.8%, 95% confidence interval [CI] 54.1–80.6) in preventing HZ in patients aged 50–59 years, and 63.9% (95% CI 56–71) in 60–69-year-olds [Citation40,Citation41,]. VE waned from year 2 onward and was non-significant approximately 8 years after vaccination [Citation42]. VE decreased with age and was not significant over the age of 80 years (18%, 95% CI −29–48) [Citation41,Citation43]. VE against PHN was approximately 66% in patients aged 60–69 years and ≥70 years [Citation41,Citation42].
The introduction of ZVL into national immunisation programmes for older adults has been linked to reductions in HZ-related GP consultations and hospitalisations in the United Kingdom and Canada, and reduced prescriptions of antivirals in Australia [Citation44–46]. A meta-analysis reported that the effectiveness of ZVL in adults aged ≥50 years was 45.9% (95% CI 42.2–49.4) in preventing HZ and 59.7% (95% CI 58.4–89.7) in preventing PHN [Citation47].
Recombinant zoster vaccine (RZV, ShingrixFootnote2, GSK)
RZV is composed of the VZV glycoprotein E (gE) viral surface antigen and AS01B,Footnote3 a liposome-based adjuvant that contains 3-O-desacyl-4’-monophosphoryl lipid A (MPL) and Quillaja saponaria Molina, fraction 21 (QS-21Footnote4) that specifically boosts cellular and humoral immune responses. Two intramuscular doses are administered 2–6 months apart, or 1–2 months apart in immunocompromised persons who might benefit from a shorter schedule [Citation48]. Two doses are required for full protection [Citation49].
RZV was first approved in Europe by the European Medicines Agency in 2018, and is indicated for the prevention of HZ and PHN in adults aged ≥50 years and in adults aged ≥18 years who are at increased risk of HZ [[Citation39]]. In randomised controlled trials, RZV demonstrated very high efficacy in preventing HZ over 3.2 years in adults aged ≥50 years (VE 97.2%, 95% CI 93.7–99.0) that was largely unchanged across age groups; VE in adults aged ≥70 years was 91.3% (95% CI 86.8–94.5) [Citation50,Citation51]. VE in preventing PHN was 91.2% (95% CI 75.9–97.7) in adults aged ≥50 years, and 88.8% (95% CI 68.7–97.1) in those aged ≥70 years [Citation50]. In an ongoing long-term historically-controlled efficacy study, follow-up of clinical trial participants for up to 10 years showed VE of 81.6% over the entire follow-up period, and VE of 73.2% (95% CI 46.9–87.6) in the 10th year post vaccination in those aged ≥50 years [Citation52] (). Information of long-term efficacy in immunocompromised patients is currently lacking.
Figure 2. Long term vaccine efficacy of RZV against herpes zoster in adults ≥50 years of age [Citation52]. RZV, recombinant zoster vaccine.
![Figure 2. Long term vaccine efficacy of RZV against herpes zoster in adults ≥50 years of age [Citation52]. RZV, recombinant zoster vaccine.](/cms/asset/2b407c8a-0453-45e7-87f7-3f33848734c2/yacb_a_2350258_f0002_oc.jpg)
Adverse reactions after vaccination were usually transient and of mild-to-moderate intensity. Injection site pain was the most frequently reported local adverse reaction. Myalgia, fatigue, and headache were the most frequently reported systemic reactions [Citation53].
In studies in immunocompromised patients aged ≥18 years, VE of RZV against HZ was 68.2% (95% CI 55.6–77.5) in patients after a hematopoietic stem cell transplantation, and 87.2% (95% CI 44.3–98.6) in patients with a haematological malignancy (post hoc analysis) [Citation54]. RZV had an acceptable safety profile in immunocompromised individuals [Citation55,Citation56]. A post hoc analysis of randomised controlled trials found that VE was 90.5% (95% CI 73.5–97.5%) in study participants with underlying potential immune-mediated diseases [Citation57]. RZV was immunogenic and well tolerated in patients with a range of other underlying conditions, including solid tumours, HIV, and solid organ, and renal transplant recipients. No differences were observed by age group [Citation54].
Clinical trial results have been confirmed by real-world effectiveness studies (). In the largest of these, vaccine effectiveness in ≥ 65-year-olds was 70.1% (95% CI 68.6–71.5), and was similar in subcohorts of patients who were immunocompromised (64.1%, 95% CI 57.2–69.8) or had underlying autoimmune diseases (68.0%, 95% CI 62.3–72.8) [Citation60]. In studies using different healthcare claims databases, estimates of vaccine effectiveness in non-immunocompromised ≥50-year-olds ranged from 83.5% to 85.5% against HZ, and 89.1% to 93.3% against HZ ophthalmicus [Citation58,Citation59,Citation61]. Vaccine effectiveness was not compromised by same day concomitant vaccination [Citation64] and RZV vaccination significantly reduced the risk of post-HZ stroke [Citation62]. A cohort study reported VE of 64% (95% CI 44–77) in patients aged ≥50 years with inflammatory bowel disease [Citation63].
Table 1. RZV real-world evidence of vaccine effectiveness in studies conducted in the United States.
There is early evidence that RZV may also confer non-specific immune benefits as has been observed for some other vaccines such as Bacille Calmette-Guérin and rotavirus vaccines [Citation65]. One study showed that RZV vaccination was associated with a 16% lower risk of a coronavirus disease 2019 (COVID-19) diagnosis and a 32% lower risk of hospitalisation due to COVID-19 [Citation66], possibly through epigenetic reprogramming [Citation65].
Recommendations and reimbursement for HZ prevention in Belgium
The Belgian Superior Health Council published their first recommendation for the prevention of HZ through vaccination in 2017 using ZVL. Following the availability of the RZV on the Belgian market, the Superior Health Council updated their recommendation in 2022, preferentially recommending vaccination with RZV for immunocompetent adults aged ≥60 years, immunocompromised patients, including those receiving immunosuppressive therapy- aged ≥16 years and patients receiving treatment with anti-Janus kinase therapy [Citation67]. Of note, RZV is indicated for the prevention of HZ and PHN in adults at increased risk of HZ from 18 years of age. Clinical efficacy and safety data in children and adolescents <18 years of age are lacking [Citation39].
As of 1 November 2023, RZV is reimbursed in Belgium for individuals aged 18 years or older if they have a haematological malignancy or a malignant tumour and have been actively treated within the past 5 years, have HIV infection, or have received organ or haematological stem cell transplantation or are a candidate for transplantation [Citation68]. Notable exclusions are patients on JAK inhibitors who show a dose-related increase in the risk of HZ of up to 5.9-fold [Citation13], and patients with chronic haematological malignancies who have not commenced active treatment. Since December 2022, ZVL is no longer commercialised in Belgium following the preferential recommendation from the Superior Health Council for the use of RZV [Citation67].
There are no data available that describe attitudes of GPs and physicians to HZ vaccination in Belgium, nor how the availability of a significantly more effective vaccine [Citation69] and preferential recommendation from the Superior Health Council might influence their intention to vaccinate. Rates of vaccine hesitancy in the French-speaking part of Belgium are as high as 50%, linked to concerns about vaccine safety and demographic characteristics such as younger age, no children, and no exposure to vaccine-preventable diseases [Citation70]. A recent study highlighted that vaccine confidence in the Dutch-speaking part of Belgium in 2023 is comparable to the average percentages observed for Belgium in a 2022 study that ranked European countries according to vaccine confidence [Citation71]. The reported vaccination confidence scores for the Dutch-speaking part of Belgium in 2023 and Belgium in 2022 place them in the mid-ranking among the European countries [Citation71]. Globally, only around 50% of older adults were willing to receive HZ vaccination, due to low trust in vaccine effectiveness and safety, and financial concerns [Citation72]. Frequently asked questions about the use of RZV are answered in Box 2 [Citation53,Citation54,Citation73].
Box 2. Common questions (Q) and answers (A) about the recombinant zoster vaccine (RZV).
Q: What if the second dose was missed?
A The second dose can be given up to 6 months after the first dose [73]. The benefits and risks of HZ vaccination later than 6 months after the second dose need to be weighed up on an individual basis.
Q: Is a booster dose needed?
A: The need for booster doses following the primary vaccination schedule has not been established.
Q: Can you be vaccinated with RZV if you have already received zoster-vaccine live (ZVL)?
A: Yes. RZV can be given with the same schedule in individuals previously vaccinated with ZVL. Two US studies showed vaccine effectiveness of 63.0–84.8% in individuals who had received ZVL within the past 5 years [53,54]. Several countries including Italy, Germany, Luxembourg, United States (US), Austria, Australia, Canada, Spain, and New Zealand, recommend RZV doses at intervals after ZVL ranging from 2 months to 5 years.
Q: Can you be vaccinated with RZV if you have already had shingles?
A: Eight countries (Germany, Luxembourg, US, Austria, Australia, Canada, Ireland, and New Zealand) recommend that RZV be administered to persons who have already had shingles due to the risk of recurrence. However, there are limited data to support the use of RZV in individuals with a history of HZ. The benefits and risks of HZ vaccination need to be weighted up on an individual basis.
Q: Can RZV be co-administered with other vaccines?
A: Yes. RZV can be given concomitantly with unadjuvanted inactivated seasonal influenza vaccine, 13-valent pneumococcal conjugate vaccine, 23-valent pneumococcal polysaccharide vaccine, or reduced antigen diphtheria-tetanus acellular pertussis vaccine. The vaccines should be administered at different injection sites.
Q: Can RZV be administered to pregnant women?
A: There are no data about the use of RZV in pregnant women. Animal studies do not indicate direct or indirect harmful effects. However, as a precautionary measure, it is preferable to avoid RZV during pregnancy.
Q: What are the most common expected adverse reactions?
A: RZV is generally well tolerated. In adults aged ≥50 years, the most frequently reported adverse reactions were pain at the injection site, myalgia, fatigue and headache. Most were not long-lasting (median duration of 2–3 days). Reactions reported as severe lasted 1–2 days.
Q: Can RZV be given to individuals with diabetes or other chronic diseases?
A: Yes. RZV is a non-live subunit vaccine that can be administered to individuals with chronic diseases including diabetes.
Q: Can RZV be given to individuals who are immunocompromised?
A: Yes. RZV is a non-live subunit vaccine so there is no risk that vaccination could cause disseminated herpes infection in immunocompromised individuals. Note that the vaccine is licenced for immunocompromised persons at risk 18 years of age and older.
Studies assessing the intention of healthcare providers to vaccinate against HZ were mostly conducted prior to availability of RZV. Studies in the Netherlands and the US found that physicians were more positive about recommending HZ vaccination if they perceived the illness as severe and causing a significant burden, and if they perceived that the vaccine was effective [Citation74,Citation75]. Another US study noted that physicians were less likely to recommend HZ vaccination (with ZVL) to patients over 85 years of age. It is uncertain whether this reluctance to vaccinated older people stemmed from awareness of the low efficacy of ZVL in this age group, or other concerns [Citation76].
Existing barriers to implementation are the lack of any recommendation for patients who have been previously vaccinated with ZVL, and for persons who have experienced a HZ episode. Nine countries provide information on prior HZ vaccination and/or previous HZ infection [Citation77]. Also lacking is clarity on which groups of immunocompromised patients should be vaccinated. There is a need to update the 2019 specific vaccine recommendations for these patients that currently state that inactivated zoster vaccine is not available and that vaccination is not applicable [Citation78]. Guidance is also needed on the optimal time to vaccinate, for example, before or after transplantation or immunosuppressive treatment, and whether antiviral prophylaxis should be continued. National authorities and specialists’ associations in other countries including Spain and Italy have issued detailed guidance in this respect [Citation79,Citation80].
The number-needed-to-vaccinate with RZV to prevent one case of HZ varies as a function of factors such as the vaccine efficacy, the duration of vaccine protection, population characteristics, and the incidence of the disease. In literature, the number-needed-to-vaccinate to avoid 1 case of HZ in persons aged 60 years ranges between 6 and 12. For PHN, the number-needed-to-vaccinate ranges between 33 and 39 in 60-year-olds [Citation2,Citation73,Citation81–88]. In immunocompromised patients, the number-needed-to-vaccinate with RZV to prevent one case of HZ/PHN was 9/47 in recipients of hematopoietic stem cell transplant, 8/88 in women with breast cancer and 10/91 in people with Hodgkin’s lymphoma [Citation88,Citation89]. Healthcare professionals who immunise according to RZV vaccine recommendations in Belgium can expect to see fewer cases of HZ or PHN in the future. This will be accompanied by fewer prescriptions for antivirals, benzodiazepines, and systemic pain killers including opioids, as well as lower costs associated with hospitalisation, physician visits and work absenteeism [Citation36].
The 2022 recommendation by the Belgian Superior Health Council provides an independent advisory guidance for HZ prevention in Belgium. However, the current narrow reimbursement structure is not aligned with these recommendations. Data from ongoing studies, such as in patients using JAK inhibitors, may go some way to support a broader reimbursement approach. The high cost of RZV remains a significant barrier and providing affordable access to effective vaccines and medicines is an ongoing challenge for Belgium [Citation90,Citation91].
RZV shows that the adverse impact of immunosenescence can be overcome by appropriate immune stimulants, bringing in a new era for adult vaccination strategies [Citation48]. RZV is also effective in preventing HZ and PHN in immunocompromised patients [Citation92]. HZ is a vaccine-preventable disease and the availability of a vaccine with high efficacy and an acceptable safety profile provides GPs and specialists with an effective tool for prevention. RZV can positively contribute to healthy aging by preventing HZ and its potential long-term sequelae [Citation93].
Ageing populations are anticipated to have significant impacts on the healthcare finances in coming years. If current vaccination rates are maintained, healthcare utilisation and costs associated with vaccine-preventable diseases, including HZ, are anticipated to increase disproportionately relative to the increase in the population aged ≥50 years [Citation94]. Indeed, Belgium is currently experiencing fiscal challenges that may worsen due to expenditure associated with ageing based on current policies [Citation91]. These data starkly highlight the need to successfully implement and fund adult immunisation strategies to achieve high vaccine uptake of RZV in older adults to mitigate the medical and societal burden associated with ageing populations. In the first instance, adult vaccination platforms rolled out to great effect during the SARS-CoV-2 pandemic can be leveraged [Citation95]. Vaccination policies will need to be adapted and updated as new evidence becomes available, and cost-effectiveness analyses using direct as well as indirect costs are needed to provide an overall economic picture of the potential impact of RZV.
Acknowledgments
The authors thank Business & Decision Life Sciences Medical Communication Service Center for editorial assistance and manuscript coordination, on behalf of GSK. Dr Joanne Wolter (independent, on behalf of GSK) provided writing support.
Disclosure statement
FS and FK are employees of GSK and hold shares in GSK. DS declares being the president (unpaid) of the Belgian working group on herpes zoster vaccination, part of the Belgian Superior Health Council. All authors declare no other financial and non-financial relationships and activities.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Additional information
Funding
Notes
1. Zostavax is a trademark of Merck & Co. Inc.
2. Shingrix is a trademark owned by or licensed to GSK.
3. AS01 is a trademark owned by or licensed to GSK.
4. QS-21 (Quillaja saponaria Molina, fraction 21) is licensed by GSK from Antigenics LLC, a wholly owned subsidiary of Agenus Inc., a Delaware, USA corporation.
References
- Patil A, Goldust M, Wollina U. Herpes zoster: a review of clinical manifestations and management. Viruses. 2022;14(2):192. doi: 10.3390/v14020192
- Pieters Z, Ogunjimi B, Beutels P, et al. Cost-effectiveness analysis of herpes zoster vaccination in 50- to 85-year-old immunocompetent Belgian cohorts: a comparison between no vaccination, the adjuvanted subunit vaccine, and live-attenuated vaccine. Pharmacoeconomics. 2022;40(4):461–476. doi: 10.1007/s40273-021-01099-2
- Abbasi R, Abdou Y, Ackermann M, et al. Limits on a muon flux from neutralino annihilations in the sun with the IceCube 22-string detector. Phys Rev Lett. 2009;102(20):201302. doi: 10.1103/PhysRevLett.102.201302
- Johnson RW, Bouhassira D, Kassianos G, et al. The impact of herpes zoster and post-herpetic neuralgia on quality-of-life. BMC Med. 2010;8(1):37. doi: 10.1186/1741-7015-8-37
- Mallick-Searle T, Snodgrass B, Brant JM. Postherpetic Neuralgia: Epidemiology, Pathophysiology, and Pain Management Pharmacology. J Multidiscip Healthc. 2016;9:447–454. doi: 10.2147/JMDH.S106340
- Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6):e004833. doi: 10.1136/bmjopen-2014-004833
- Yawn BP, Gilden D. The global epidemiology of herpes zoster. Neurology. 2013;81(10):928–930. doi: 10.1212/WNL.0b013e3182a3516e
- Arvin AM. Humoral and cellular immunity to varicella-zoster virus: an overview. J Infect Dis. 2008;197(Suppl 2):S58–60. doi: 10.1086/522123
- Gruver AL, Hudson LL, Sempowski GD. Immunosenescence of ageing. J Pathol. 2007;211(2):144–156. doi: 10.1002/path.2104
- Tu W, Rao S. Mechanisms underlying T cell immunosenescence: aging and cytomegalovirus infection. Front Microbiol. 2016;7:2111. doi: 10.3389/fmicb.2016.02111
- Fulop T, Larbi A, Dupuis G, et al. Immunosenescence and inflamm-aging as two sides of the same coin: friends or foes? Front Immunol. 2017;8:1960. doi: 10.3389/fimmu.2017.01960
- Marra F, Parhar K, Huang B, et al. Risk factors for herpes zoster infection: a meta-analysis. Open Forum Infect Dis. 2020;7(1):ofaa005. doi: 10.1093/ofid/ofaa005
- Din S, Selinger CP, Black CJ, et al. Systematic review with network meta-analysis: risk of herpes zoster with biological therapies and small molecules in inflammatory bowel disease. Aliment Pharmacol Ther. 2023;57(6):666–675. doi: 10.1111/apt.17379
- Dauby N, Motet C, Libois A, et al. The value of herpes zoster prevention in people aging with HIV: a narrative review. HIV Med. 2023;24(12):1190–1197. doi: 10.1111/hiv.13548
- Zhou H, Wang Z, Jin H, et al. A systematic review and meta-analysis of independent risk factors for postherpetic neuralgia. Ann Palliat Med. 2021;10(12):12181–12189. doi: 10.21037/apm-21-3028
- Forbes HJ, Thomas SL, Smeeth L, et al. A systematic review and meta-analysis of risk factors for postherpetic neuralgia. Pain. 2016;157(1):30–54. doi: 10.1097/j.pain.0000000000000307
- Johnson RW, Alvarez-Pasquin M-J, Bijl M, et al. Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Ther Adv Vaccines. 2015;3(4):109–120. doi: 10.1177/2051013615599151
- Cohen EJ, Jeng BH. Herpes zoster: a brief definitive review. Cornea. 2021;40(8):943–949. doi: 10.1097/ICO.0000000000002754
- Johnson BH, Palmer L, Gatwood J, et al. Annual incidence rates of herpes zoster among an immunocompetent population in the United States. BMC Infect Dis. 2015;15(1):502. doi: 10.1186/s12879-015-1262-8
- Pierik JG, Gumbs PD, Fortanier SA, et al. Epidemiological characteristics and societal burden of varicella zoster virus in the Netherlands. BMC Infect Dis. 2012;12(1):110. doi: 10.1186/1471-2334-12-110
- Bardach AE, Palermo C, Alconada T, et al. Herpes zoster epidemiology in Latin America: a systematic review and meta-analysis. PLOS ONE. 2021;16(8):e0255877. doi: 10.1371/journal.pone.0255877
- Roberfroid D, Zeevaert R, Maertens de Noordhout C, et al. Evaluation of shingrix vaccine against herpes zoster. Health Tech Ass (HTA) Brussels: Belgian Health Care Knowe Cen (KCE). 2022. KCE Reports 360. D/2022/. https://kce.fgov.be/sites/default/files/2022-10/KCE_360_Evaluation_Of_Vaccine_Against_Herpes_Report.pdf
- Kim YJ, Lee CN, Lee MS, et al. Recurrence rate of herpes zoster and its risk factors: a population-based cohort study. J Korean Med Sci. 2019;34(2):e1. doi: 10.3346/jkms.2019.34.e1
- Bilcke J, Ogunjimi B, Marais C, et al. The health and economic burden of chickenpox and herpes zoster in Belgium. Epidemiol Infect. 2012;140(11):2096–2109. doi: 10.1017/S0950268811002640
- Sabbe M, Grammens T, Braeye T, et al. Maladies infectieuses pédiatriques à prévention vaccinale. 2014. [cited 2023 Nov8]. Available from: https://www.sciensano.be/en/biblio/maladies-infectieuses-pediatriques-a-prevention-vaccinale-synthese-annuelle-2014
- Jacquinet S, Bensemmane S, Smeesters P, et al. Surveillance épidémiologique de la Varicelle et du Zona – varicella-zoster virus (VZV) – aperçu 2010-2022 et résultats détaillés 2019–2022. Sciensano. 2023:1–17.
- Bricout H, Perinetti E, Marchettini P, et al. Burden of herpes zoster-associated chronic pain in Italian patients aged 50 years and over (2009–2010): a GP-based prospective cohort study. BMC Infect Dis. 2014;14(1):637. doi: 10.1186/s12879-014-0637-6
- Yawn BP, Saddier P, Wollan PC, et al. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc. 2007;82(11):1341–1349. doi: 10.4065/82.11.1341
- Gater A, Uhart M, McCool R, et al. The humanistic, economic and societal burden of herpes zoster in Europe: a critical review. BMC Public Health 2015;15(1):193. doi: 10.1186/s12889-015-1514-y
- Wauters O, Lebas E, Nikkels AF. Chronic mucocutaneous herpes simplex virus and varicella zoster virus infections. J Am Acad Dermatol. 2012;66(6):e217–27. doi: 10.1016/j.jaad.2010.07.011
- Andrei G, Snoeck R. Advances and perspectives in the management of varicella-zoster virus infections. Molecules 2021;26(4):1132. doi: 10.3390/molecules26041132
- Chen N, Li Q, Yang J, et al. Antiviral treatment for preventing postherpetic neuralgia. Cochrane Database Syst Rev. 2014;2014(2): CD006866. 10.1002/14651858.CD006866.pub3
- Belgian Antibiotic Policy Coordination Commission. Guide belge de traitement anti-infectieux en pratique ambulatoire 2022. [cited 2023 Nov 8]. https://organesdeconcertation.sante.belgique.be/sites/default/files/content/bapcoc_guide_traitement_antiinfectieux_2022.pdf
- McDonald EM, de Kock J, Ram FS. Antivirals for management of herpes zoster including ophthalmicus: a systematic review of high-quality randomized controlled trials. Antivir Ther. 2012;17(2):255–264. doi: 10.3851/IMP2011
- Gross GE, Eisert L, Doerr HW, et al. S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. J Dtsch Dermatol Ges. 2020;18(1):55–78. doi: 10.1111/ddg.14013
- Poirrier JE, DeMartino JK, Nagar S, et al. Burden of opioid use for pain management among adult herpes zoster patients in the US and the potential impact of vaccination. Hum Vaccin Immunother. 2022;18(5):2040328. doi: 10.1080/21645515.2022.2040328
- Hempenstall K, Nurmikko TJ, Johnson RW, et al. Analgesic therapy in postherpetic neuralgia: a quantitative systematic review. PLOS Med. 2005;2(7):e164. doi: 10.1371/journal.pmed.0020164
- Summary of Product Characteristics. Varivax®. Varicella Virus Vaccine Live. 2022. [cited 2023 Sept 23]. Available from: https://www.medicines.org.uk/emc/product/5582/smpc
- European Medicines Agency. Zostavax: Summary of product characterstics. 2009. [cited 2023 Sept 23]. Available from. https://www.ema.europa.eu/en/documents/product-information/zostavax-epar-product-information_en.pdf
- Schmader KE, Levin MJ, Gnann JW Jr, et al. Efficacy, safety, and tolerability of herpes zoster vaccine in persons aged 50-59 years. Clin Infect Dis. 2012;54(7):922–928. doi: 10.1093/cid/cir970
- Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271–2284. doi: 10.1056/NEJMoa051016
- Morrison VA, Johnson GR, Schmader KE, et al. Long-term persistence of zoster vaccine efficacy. Clin Infect Dis. 2015;60(6):900–909. doi: 10.1093/cid/ciu918
- ZOSTAVAX® (Zoster Vaccine Live). Product information. 2006. [cited 2024 Feb 21]. Available from: https://www.fda.gov/media/119879/download
- Litt J, Booy R, Bourke D, et al. Early impact of the Australian national shingles vaccination program with the herpes zoster live attenuated vaccine. Hum Vaccin Immunother. 2020;16(12):3081–3089. doi: 10.1080/21645515.2020.1754702
- Andrews N, Stowe J, Kuyumdzhieva G, et al. Impact of the herpes zoster vaccination programme on hospitalised and general practice consulted herpes zoster in the 5 years after its introduction in England: a population-based study. BMJ Open. 2020;10(7):e037458. doi: 10.1136/bmjopen-2020-037458
- Martins D, McCormack D, Tadrous M, et al. Impact of a publicly funded herpes zoster immunization program on the burden of disease in Ontario, Canada: a population-based study. Clin Infect Dis. [2021 Jan 27];72(2):279–284. doi: 10.1093/cid/ciaa014
- Mbinta JF, Nguyen BP, Awuni PMA, et al. Post-licensure zoster vaccine effectiveness against herpes zoster and postherpetic neuralgia in older adults: a systematic review and meta-analysis. Lancet Healthy Longev. 2022;3(4):e263–e275. doi: 10.1016/S2666-7568(22)00039-3
- Lecrenier N, Beukelaers P, Colindres R, et al. Development of a recombinant adjuvanted herpes zoster subunit vaccine and its implications for shingles prevention. Expert Rev Vaccines. 2018;17(7):619–634. doi: 10.1080/14760584.2018.1495565
- Orru S, Bierbaum S, Enk A, et al. Skin manifestations after immunisation with an adjuvanted recombinant zoster vaccine, Germany, 2020. Euro Surveill. 2023;28(50). doi: 10.2807/1560-7917.ES.2023.28.50.2300261
- Cunningham AL, Lal H, Kovac M, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019–1032. doi: 10.1056/NEJMoa1603800
- Lal H, Cunningham AL, Godeaux O, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Eng J Med. 2015;372(22):2087–2096. doi: 10.1056/NEJMoa1501184
- Strezova A, Diez-Domingo J, Al Shawafi K, et al. Long-term protection against herpes zoster by the adjuvanted recombinant zoster vaccine: interim efficacy, immunogenicity, and safety results up to 10 years after initial vaccination. Open Forum Infect Dis. 2022;9(10):ofac485. doi: 10.1093/ofid/ofac485
- Fiore J, Co-van der Mee MM, Maldonado A, et al. Safety and reactogenicity of the adjuvanted recombinant zoster vaccine: experience from clinical trials and post-marketing surveillance. Ther Adv Vaccines Immunother. 2021;9:25151355211057479. doi: 10.1177/25151355211057479
- Racine E, Gilca V, Amini R, et al. A systematic literature review of the recombinant subunit herpes zoster vaccine use in immunocompromised 18-49 year old patients. Vaccine. 2020;38(40):6205–6214. doi: 10.1016/j.vaccine.2020.07.049
- Lopez-Fauqued M, Co-van der Mee M, Bastidas A, et al. Safety profile of the adjuvanted recombinant zoster vaccine in immunocompromised populations: an overview of six trials. Drug Saf. 2021;44(7):811–823. doi: 10.1007/s40264-021-01076-w
- Mullane KM, Morrison VA, Camacho LH, et al. Safety and efficacy of inactivated varicella zoster virus vaccine in immunocompromised patients with malignancies: a two-arm, randomised, double-blind, phase 3 trial. Lancet Infect Dis. 2019;19(9):1001–1012. doi: 10.1016/S1473-3099(19)30310-X
- Dagnew AF, Rausch D, Herve C, et al. Efficacy and serious adverse events profile of the adjuvanted recombinant zoster vaccine in adults with pre-existing potential immune-mediated diseases: a pooled post hoc analysis on two parallel randomized trials. Rheumatology (Oxford). 2021;60(3):1226–1233. doi: 10.1093/rheumatology/keaa424
- Sun Y, Kim E, Kong CL, et al. Effectiveness of the recombinant zoster vaccine in adults aged 50 and older in the United States: a claims-based cohort study. Clin Infect Dis. 2021;73(6):949–956. doi: 10.1093/cid/ciab121
- Sun Y, Jackson K, Dalmon CA, et al. Effectiveness of the recombinant zoster vaccine among Kaiser Permanente Hawaii enrollees aged 50 and older: a retrospective cohort study. Vaccine. 2021;39(29):3974–3982. doi: 10.1016/j.vaccine.2021.05.056
- Izurieta HS, Wu X, Forshee R, et al. Recombinant zoster vaccine (shingrix): real-world effectiveness in the first 2 years post-licensure. Clin Infect Dis. 2021;73(6):941–948. doi: 10.1093/cid/ciab125
- Lu A, Sun Y, Porco TC, et al. Effectiveness of the recombinant zoster vaccine for herpes zoster ophthalmicus in the United States. Ophthalmol. 2021;128(12):1699–1707. doi: 10.1016/j.ophtha.2021.04.017
- Parameswaran GI, Wattengel BA, Chua HC, et al. Increased stroke risk following herpes zoster infection and protection with zoster vaccine. Clin Infect Dis. 2022;76(3):e1335–e1340. doi: 10.1093/cid/ciac549
- Kochhar GS, Desai A, Caldera DF, et al. Effectiveness of recombinant zoster vaccine (RZV) in patients with inflammatory bowel disease. Vaccine. 2021;39(30):4199–4202. doi: 10.1016/j.vaccine.2021.05.043
- Bruxvoort KJ, Qian L, Wu J, et al. Herpes zoster following recombinant zoster vaccine with or without concomitant vaccination. Open Forum Infect Dis. 2022;9(3):ofac011. doi: 10.1093/ofid/ofac011
- Laupeze B, Del Giudice G, Doherty MT, et al. Vaccination as a preventative measure contributing to immune fitness. NPJ Vaccin. 2021;6(1):93. doi: 10.1038/s41541-021-00354-z
- Bruxvoort KJ, Ackerson B, Sy LS, et al. Recombinant adjuvanted zoster vaccine and reduced risk of COVID-19 diagnosis and hospitalization in older adults. J Infect Dis. 2022;225(11): 1915–1922. doi:10.1093/infdis/jiab633
- Belgian Superior Health Council. Vaccination against herpes zoster. Report 9684. (Brussels: SCH). 2022. [cited 2023 Sept 23]. Available from: https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/20220906_shc-9684_herpes_zoster_vweb.pdf
- Centre Belge d’Information Pharmacothérapeutique (CBIP). Folia Pharmacotherapeutica novembre 2023. 2023;50(11): 1–9. [cited 2023 Nov 24]. Available from: https://www.bcfi.be/nl/articles/query?number=F50N11I#zon
- Tricco AC, Zarin W, Cardoso R, et al. Efficacy, effectiveness, and safety of herpes zoster vaccines in adults aged 50 and older: systematic review and network meta-analysis. BMJ. 2018;363:k4029. doi: 10.1136/bmj.k4029
- Gobert C, Semaille P, Van der Schueren T, et al. Prevalence and determinants of vaccine hesitancy and vaccines recommendation discrepancies among general practitioners in French-speaking parts of Belgium. Vaccines (Basel). 2021;9(7):771. doi: 10.3390/vaccines9070771
- Pattyn J, Hendrickx G, Valckx S, et al. Studie over vaccinatie vertrouwen voor het vaccinatiebeleid in Vlaanderen - Een observationele, crosssectionele online vragenlijst om vaccinatie vertrouwen in Vlaanderen te meten OVERHEIDSOPDRACHT: BESTEK NR AP/IZ-VAC/2023/62023. [cited 2024 Apr 11]. https://laatjevaccineren.paddlecms.net/sites/default/files/2024-02/Rapport%20VCF%20overheidsopdracht%20NR%20APIZ-VAC20236.pdf
- Wang Q, Yang L, Li L, et al. Willingness to vaccinate against herpes zoster and its associated factors across who regions: global systematic review and meta-analysis. JMIR Public Health Surveill. 2023;9:e43893. doi: 10.2196/43893
- Drolet M, Zhou Z, Sauvageau C, et al. Effectiveness and cost-effectiveness of vaccination against herpes zoster in Canada: a modelling study. CMAJ. 2019;191(34):E932–E939. doi: 10.1503/cmaj.190274
- Lehmann BA, Eilers R, Mollema L, et al. The intention of Dutch general practitioners to offer vaccination against pneumococcal disease, herpes zoster and pertussis to people aged 60 years and older. BMC Geriatr. 2017;17(1):122. doi: 10.1186/s12877-017-0511-7
- Hurley LP, Harpaz R, Daley MF, et al. National survey of primary care physicians regarding herpes zoster and the herpes zoster vaccine. J Infect Dis. 2008;197(Suppl 2):S216–23. doi: 10.1086/522153
- Hurley LP, Allison MA, Dooling KL, et al. Primary care physicians’ experience with zoster vaccine live (ZVL) and awareness and attitudes regarding the new recombinant zoster vaccine (RZV). Vaccine. 2018;36(48):7408–7414. doi: 10.1016/j.vaccine.2018.09.018
- Parikh R, Widenmaier R, Weller R, et al. An update on national recommendations for the use of the adjuvanted recombinant zoster vaccine. Abstract. 15th European Public Health Conference 2022; Berlin, Germany; 2022.
- Belgian Superior Health Council. Publication of the Superior Health Council. Report 9158. Brussels: SHC. 2019. [cited 2023 Sept 23]. Available from: https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/20200212_shc_9158_ic_and_vaccination_vweb.pdf
- Andreoni M, Sticchi L, Nozza S, et al. Recommendations of the Italian society for infectious and tropical diseases (SIMIT) for adult vaccinations. Hum Vaccin Immunother. 2021;17(11):4265–4282. doi: 10.1080/21645515.2021.1971473
- Ministerio de Sanidad. Recomendaciones de vacunacio n frente a herpes zoster, 25 marzo 2021. [cited 2023 Aug 1]. Available from: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/programasDeVacunacion/docs/HerpesZoster_RecomendacionesVacunacion.pdf
- Curran D, Patterson B, Varghese L, et al. Cost-effectiveness of an adjuvanted recombinant zoster vaccine in older adults in the United States. Vaccine. 2018;36(33):5037–5045. doi: 10.1016/j.vaccine.2018.07.005
- de Boer PT, van Lier A, de Melker H, et al. Cost-effectiveness of vaccination of immunocompetent older adults against herpes zoster in the Netherlands: a comparison between the adjuvanted subunit and live-attenuated vaccines. BMC Med. 2018;16(1):228. doi: 10.1186/s12916-018-1213-5
- Van Oorschot D, Anastassopoulou A, Poulsen Nautrup B, et al. Cost-effectiveness of the recombinant zoster vaccine in the German population aged ≥60 years old. Hum Vaccin Immunother. 2019;15(1):34–44. doi: 10.1080/21645515.2018.1509645
- You JHS, Ming WK, Tsang OT, et al. Optimal gender-specific age for cost-effective vaccination with adjuvanted herpes zoster subunit vaccine in Chinese adults. PLOS ONE. 2019;14(1):e0210005. doi: 10.1371/journal.pone.0210005
- McGirr A, Van Oorschot D, Widenmaier R, et al. Public health impact and cost-effectiveness of non-live adjuvanted recombinant zoster vaccine in Canadian adults. Appl Health Econ Health Policy. 2019 ;17(5):723–732. doi: 10.1007/s40258-019-00491-6
- Curran D, Van Oorschot D, Matthews S, et al. Long-term efficacy data for the recombinant zoster vaccine: impact on public health and cost effectiveness in Germany. Hum Vaccin Immunother. 2021;17(12):5296–5303. doi: 10.1080/21645515.2021.2002085
- Ultsch B, Weidemann F, Koch J, et al. Modellierung von epidemiologischen und gesundheitsökonomischen: Effekten von impfungen zur prävention von herpes zoster. 2017 [cited 2023 Sept 21]. Available from: https://www.rki.de/DE/Content/Infekt/Impfen/ImpfungenAZ/Zoster/Modellierung_Zoster_Impfung.pdf?__blob=publicationFile
- Ortega-Sanchez I. Economics of vaccinating immunocompromised 19–49-years-old adults against herpes zoster in the US.September 29, 2021; ACIP zoster vaccines session. [cited 2023 Aug 21]. Available from: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-09-29/02-ZosterVaccines-OrtegaSanchez-508.pdf
- Curran D, Patterson BJ, Carrico J, et al. Public health impact of recombinant zoster vaccine for prevention of herpes zoster in US adults immunocompromised due to cancer. Hum Vaccin Immunother. 2023;19(1):2167907. doi: 10.1080/21645515.2023.2167907
- Simoens S, Abdallah K, Barbier L, et al. How to balance valuable innovation with affordable access to medicines in Belgium? Front Pharmacol. 2022;13:960701. doi: 10.3389/fphar.2022.960701
- Recommendation for a council recommendation on the 2023 national reform programme of Belgium and delivering a council opinion on the 2023 stability programme of Belgium. Brussels, 24 5.2023 COM(2023) 601 final. [cited 2023 Aug 21]. Available from: https://commission.europa.eu/system/files/2023-05/COM_2023_601_1_EN.pdf
- Bastidas A, de la Serna J, El Idrissi M, et al. Effect of recombinant zoster vaccine on incidence of herpes zoster after autologous stem cell transplantation: a randomized clinical trial. JAMA. 2019;322(2):123–133. doi: 10.1001/jama.2019.9053
- Doherty TM, Del Giudice G, Maggi S. Adult vaccination as part of a healthy lifestyle: moving from medical intervention to health promotion. Ann Med. 2019;51(2):128–140. doi: 10.1080/07853890.2019.1588470
- Talbird SE, La EM, Carrico J, et al. Impact of population aging on the burden of vaccine-preventable diseases among older adults in the United States. Hum Vaccin Immunother. 2021;17(2):332–343. doi: 10.1080/21645515.2020.1780847
- Doherty TM, Pasquale AD, Finnegan G, et al. Sustaining the momentum for adult vaccination post-COVID-19 to leverage the global uptake of life-course immunisation: a scoping review and call to action. Int J Infect Dis. 2024;142:106963. doi: 10.1016/j.ijid.2024.02.006