

ABSTRACT
Background
The oral cavity is the most important link between the human body and the external environment and is well-equipped to protect the body against invading pathogens. Emerging data on the bidirectional relationship between oral health and the severity of COVID-19 symptoms has prompted us to reexamine our role as the guardians of the oral cavity - the true gateway to the body. Recent studies have shown that the oral microbiome is a complex ecological system and the interactions between its residents and the host cells influence human health and disease. This narrative review elaborates on the oral-systemic connection from an oral microbiome standpoint and discusses the future role of oral health professionals.
Methods
A PubMed literature search using the keywords “Oral Microbiome and Diseases” and “Oral microbiome and Health” for a range of ten years between 2012-2022 was completed. Meta-Analyses, Reviews, Randomized Control Trials, Clinical Trials, and books were included in the search.
Results
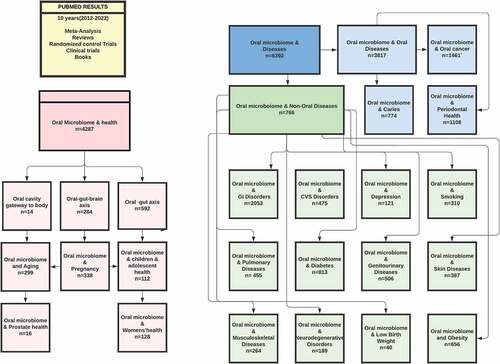
“Oral microbiome and Diseases” yielded 6392 results and “Oral microbiome and Health” yielded 4287 results.
Conclusion
Oral health professionals need to be trained on the oral-systemic connection periodically to appreciate the recent advances in this field.
Practical Implications
A deeper understanding of the impact of existing treatment modalities on the oral microbiome could expand the role of oral health professionals in preventing and maintaining patients' overall health. Implementing point-of-care salivary diagnostics to detect salivary biomarkers for oral and non-oral diseases and conditions may be a significant leap toward this goal.
Introduction
The oral microbiota has 700 species of different taxa of microorganisms in various sites of the oral cavity including bacteria, fungi and viruses, whereas the oral microbiome is the collective entity that includes the microorganisms, the extracellular matrix, protein signals, molecular communications, enzymatic byproducts and other interactions with the host cell.Citation1 With the recent advances in culture independent, next-generation sequencing (NGS) techniques, polymerase chain reaction (PCR), gel-based techniques and DNA microarrays, it is possible to analyze the genomes and their activity in the oral microbiome.Citation2 The healthy oral microbiome provides colonization resistance to pathogenic invaders of the mucosal barrier in the mouth. The commensal bacterium of the oral microbiome is predominantly comprised of the phyla Actinobacteria, Proteobacteria, Firmicutes, Bacteroidetes and Fusobacter with a smaller number of Spirochetes. The fungal members of the oral microbiome include Candida, Cladosporium, Aureobasidium, Saccharomyces, Aspergillus, Fusarium and Cryptococcus. The saprophytic protozoa include Entamoeba gingivalis and Trichomonas tenax.Citation3 The salivary microbiome has 17.5% of Streptococcus, 15.5% Prevotella, 15.3% Veillonella, 12.7% Neisseria and 10% Haemophilus.Citation4 The viruses found in the oral microbiome are bacteriophages and are very different from the viruses inhabiting other parts of the body.Citation5 These bacteriophages function by releasing lytic enzymes that can wipe out bacterial communities and change the composition of the oral microbiome.Citation6 Other viruses include 66% herpesviruses, 24% retroviruses and 1.2% papilloma viruses. The oral virome and its function are poorly understood, and researchers believe that they may act as hubs for gene function resulting in infections.Citation7 Now, with the COVID-19 pandemic, the salivary glands may serve as a reservoir of SARS-CoV-2 viruses, even in asymptomatic carriers.Citation8
Several mechanisms in the oral cavity protect the symbiotic relationship between the microbiome and the host cells to maintain homeostasis. The microbial interactions could be between different species such as bacteria interacting with fungi and protozoa in the microbiome. The results of these interactions could be positive, negative or neutral. Secondary metabolites are important for such communications. An example of such a system is quorum sensing activated by small molecules, such as the peptides, to help bacteria adapt to the host environment and adhere to a biofilm.Citation9 Direct interspecies electron transfer is another communication channel in anaerobic systems.Citation10 Saliva has antimicrobial components, secretory immunoglobulin A and the buffering capacity to alkalinize the pH of the oral cavity. The glycoproteins in the saliva influence the attachment apparatus of microbes entering the mouth and contribute to the immune response.Citation11 Salivary glands produce copious amounts of nitrite into the saliva that converts it into nitric oxide, adding to the antimicrobial properties.
When there is a disruption to the composition, activity and function of the oral microbiome, it causes dysbiosis. The major categories influencing the microbiome are age, host, environment, habitat and biofilm maturation. The subcategories include age-related physiological changes, habits, transfer of microbes from the external environment, genetics, lifestyle, immune responses, medications, hormonal changes, living environment, nutrition, oral hygiene, pH and salivary rate and volume, molecular biochemistry in the oral biofilm, probiotic, the extracellular matrix, etc.Citation12 Dysbiosis of the oral microbiome in turn causes pro-inflammatory reactions orally and elsewhere in the body, causing oral and non-oral diseases. The main pathways are through the bloodstream via a bacteremia, endotoxins from oral pathogens circulating and causing damage and immune responses to oral pathogens and endotoxins initiating a cascade of reactions, causing further damage.Citation13
A literature review of the past 10 years (2012–2022) was performed in PubMed using the keywords “oral microbiome and diseases” and yielded 6,392 results ().
Figure 1. PubMed Results.
Non-Oral Diseases
is a concise summary of articles and results with clinical relevance.
Table 1. Oral microbiome and its influence on non-oral diseases.
Interesting mechanisms of oral microbiome and its interactions with the host in causing systemic diseases are described below.
Gastrointestinal Disease Citation14–18
The pathophysiology of oral microbiota invading the gut is investigated in a study by Kitamoto et al. who proposed that gut dysbiosis could be a requirement for colonization by oral microbiota. Though the gastric acid may be a successful barrier for most pathogens, oral microbiota-like P. gingivalis is acid resistant and crosses the stomach barrier. The researchers examined the role of oral microbes such as Fusobacterium nucleatum, Fusobacterium varium and P. gingivalis in the gut and their mechanisms of damage in the gut. It is highly possible that an overgrowth of oral microbes leads to migration to the gut to colonize it and cause diseases. Fusobacterium nucleatum utilizes matrix metalloproteinases (MMPs) and lipopolysaccharides to invade the gut and promote tumor cell proliferation, chemotherapy resistance and immune evasion. Fusobacterium varium potentiated adhesion and invasion of gut cells. P. gingivalis acted as an antiapoptotic and promoted cell proliferation. The fact that MMPs play an important role in the progression of gut tumors, and oral microbiota residing in tumors of the colon could be responsible for metastasis. The oral bacteria Klebsiella may be the connection between oral and gut microbiome in colonizing and inducing certain types of irritable bowel syndrome.
Liver Disease Citation19–23
Primary biliary cholangitis (PBC) and autoimmune hepatitis (AIH) are both autoimmune conditions affecting the liver. Studies have shown the connection between dysbiosis in the oral-gut axis causing inflammation in the liver. Veillonella dispar is a lipopolysaccharide-producing bacterium found in abundance in the saliva of patients with AIH, and it is unclear if the liver disease caused this change in the oral microbiome or vice versa. Both Veillonella and Eubacterium are increased in patients with PBC, with a decrease in the frequency of Fusobacterium, compared to healthy subjects. P. gingivalis, a periopathogen, has an adverse effect on nonalcoholic fatty liver disease and may even hasten the progression to carcinoma of the liver. This highlights the need for further research on the oral-liver axis of the microbiome.
Diabetes
Oral microbiome dysbiosis has been found to be responsible for the initiation and progression of diabetes mellitus. Patients with diabetes mellitus had an abundance of Fusobacteria and Actinobacteria and a decrease in Proteobacteria compared to healthy patients.Citation24–27
Obesity
Coker et al.Citation28 examined the variation in oral microbiome in 3- and 4-year-old preschool children and gathered data on the diversity of the oral microbiome, body mass index and overweight status. They identified that phylum Firmicutes, Actinobacteria and Bacteroidetes were associated with weight gain in the first 2 years of life. The diversity of the oral microbiome was found to be decreased as the BMI increased. The conclusion was that the changes in body composition impacted the diversity of the oral microbiome, leading to increased risk factors for developing diseases in adult life. This process has immune modulating effects because of gut and oral microbiome dysbiosis. This is an important interaction in the oral-gut axis.Citation29–31
Cardiovascular Disease
Giordano-Kelhoffer et al.Citation32 did a systematic review on articles published between January 2003 and April 2022 on the oral microbiome and its impact on systemic diseases. Evidence showed that individuals with periodontal disease had a 25% to 50% higher chance of developing an adverse cardiovascular event than individuals without periodontal disease.Citation33 The bacterial products released into the blood activate pro-inflammatory processes and facilitate the progression of cardiovascular disease. Additionally, the immune system is also triggered to react to this resulting in further damage to the circulatory system. Blekkenhorst et al.Citation34 examined the role of oral microbiome in nitrate metabolism that directly affects cardiovascular health. Koch et al.Citation35 studied the connection between nitrate metabolism and cardiac and pulmonary health. According to this study, the pathophysiology of pulmonary hypertension, obesity, hypertension and cardiovascular disease are all the result of poor nitrate metabolism by oral microbiome. Hezel et al.Citation36 traced the uptake of nitrate into the parotid salivary glands (25%) from food such as leafy green vegetables, recirculation into saliva and conversion to nitric oxide after commensal bacteria act on it. Rothia mucilaginosa and Neisseria flavescens in the oral microbiome were responsible for the nitrate-to-nitrite metabolism.Citation37 Chronic endotoxemia due to lipopolysaccharide producing gram-negative bacteria from periodontitis, may be responsible for local and systemic inflammation that is responsible for many of the cardiometabolic conditions.Citation38
Increased numbers of P. gingivalis, increased Firmicutes/Bacteroidetes ratio in the oral microbiome may be an indication for an upregulation in the inflammatory response, mediated by cytokines. Metabolites such as lipopolysaccharides from bacterial infections of P. gingivalis, Helicobacter pylori, Chlamydia pneumoniae, Prevotella intermedia and A. actinomycetemcomitans may be responsible for the development of atherosclerosis.Citation39
Respiratory Diseases
Smokers have a diverse, unstable, early colonizations of oral biofilms with periodontal pathogens such as Fusobacterium, Cardiobacterium, Synergistes and Selenomonas genera and respiratory pathogens belonging to the genera Haemophilus and Pseudomonas compared to nonsmokers.Citation40
The oral cavity is anatomically positioned to translocate microorganisms to the lungs either by aspiration or through the bloodstream. Studies on the composition of the lung microbiome have a great overlap between oral microbiomes.Citation41,Citation42 One very old theory posits that dysbiosis from the oral cavity results in migration of pathogens and their metabolites to other parts of the body causing diseases.Citation43 Many studies have shown that there is a continuity of the microbiome from the nasal passages and oral cavity to the upper respiratory tract and lungs as well as the gut.Citation44 Overall, the oral-lung axis may exchange components of their microbiome in health and disease, as confirmed by a study that found respiratory pathogens in the teeth of patients in intensive care units.Citation45 In chronic obstructive pulmonary disease (COPD), researchers have found that the “vicious circle hypothesis” results in smoke-related injury to the lungs and dysbiosis of the lung microbiome causing poor immune responses, which leads to complications.Citation46 In cystic fibrosis, studies found less diversity in the oral and lung microbiome, with an abundance of candida in the mouth and lungs, along with an increased number of oral and respiratory pathogens.Citation47
Neurodegenerative Diseases
Alzheimer’s disease is a chronic inflammatory disease of the brain resulting in tissue destruction. The presence of proinflammatory cytokines and lipopolysaccharides from T. denticola, T. forsythia and P. gingivalis suggests that oral microbiota plays an important role in disease progression of Alzheimer’s disease. Inversely, disease processes in the brain have affected the oral microbiota as well. Because gram-negative bacteria are implicated in oral dysbiosis and amyloid production in the brain, interventions aimed at this process could be a focus in the future research.Citation48–50
Psychiatric Disorders
Many studies examined the diversity of the oral microbiome and dysbiosis and found correlations between increased levels of Neisseria spp. and Prevotella nigrescens and depression in young adults.Citation51–53 Ahrens et al.Citation54 performed an interesting study to show the correlation between salivary microbiome and suicidal tendencies in college students. Along with the salivary microbiome, major histocompatibility complexes (MHC) were also compared between 47 students with a history of suicidal thoughts and 325 control subjects. The absence of four specific types of MHC in the students with suicidal tendencies was a stark contrast to others. They were also missing Alloprevotella rava, which produces an organic acid for brain homeostasis. The study concluded that depression was in fact an inflammatory disease and warranted further research on human leukocyte antigen (HLA) complexes and their role in depression.
Genitourinary Diseases
P. gingivalis and F. nucleatum may potentiate chronic inflammation of the prostate. Periodontal therapy reduced the levels of prostate-specific antigen in older patients. Levels of Pseudomonas could be measured as a biomarker for patients at risk for chronic kidney diseases.Citation55–58
Cancer
Several studies in the last two decades have provided an association between colonization of specific bacteria in the oral microbiome and types of cancer.Citation59–64 The mechanism of involvement of the oral microbiome could be manifold. Chronic inflammatory mediators from periopathogens help with unregulated cell growth, mutagenesis and oncogene activation. P. gingivalis is suggested to be antiapoptotic due to the metabolism of nucleoside-diphosphate-kinase homolog, which is an enzyme in bacteria. S. gordonii, S. mitis, S. oralis, S. salivarius, S. sanguinis and Candida produce carcinogenic substances such as acetaldehyde from ethanol and other sulfuric compounds that promote gene mutations resulting in oral cancer. Cytomegalovirus has been associated with oral cancer due to its immunosuppressive and antiapoptotic properties. Esophageal cancer is associated with increased numbers of T. forsythia and P. gingivalis. P. gingivalis and A. actinomycetemcomitans have been implicated in pancreatic cancer. Fusobacterium nucleatum, a commensal in the oral cavity, has been identified in 30% of patients, with colorectal cancer revealing the role in progression to cancer.
Adverse Pregnancy Outcomes
Recent studies on periodontal therapy interventions during the second trimester did not see strong evidence on reduction of adverse pregnancy outcomes. This may be due to migration of oral pathogens before conception. Pregnancy gingivitis is associated with an increase in P. intermedia in the oral biofilm. Chronic periodontal infections cause pro-inflammatory cytokines to be released into the body, causing a systemic response. Though not abundant, the pathogens involved in periodontitis, Prevotella intermedia and P. gingivalis, are involved in adverse outcomes in pregnancy such as preterm delivery and low birth weight.Citation65–68
Autoimmune Diseases
Research shows that autoimmune diseases like rheumatoid arthritis could have keystone pathogens as triggers. The autoimmune response initiation for Sjogren’s syndrome is in the salivary gland tissues.Citation69–72
Age-Related Changes
The oral microbiome is affected by age-related changes. In a study comparing the oral and gut microbiomes of healthy aging individuals versus nonhealthy aging individuals (those with one or more chronic diseases) aged 70 t0 82, the salivary microbiome had more alpha diversity in the healthy aging individuals. Akkermansia muciniphilia and Erysipelotrichaceae UCG-003 were abundant in healthy aging, while Streptococcus was decreased in number. It is believed that these microbes are abundant because they function as probiotics.Citation73
Effect of Medications on Oral Microbiome
Amoxicillin is the most prescribed antibiotic for oral infections. One study investigated the effect of this antibiotic on the oral microbiome and found imbalances in 35 taxa of microorganisms that reduced the richness and the diversity of the oral microbiome considerably, and the recovery was incomplete even after 3 weeks.Citation74
Oral Diseases
An in-depth study by Socransky and Haffajee in 1998 published certain criteria to be classified as key perio pathogens. Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis fulfill these criteria. They classified all the bacteria involved in periodontitis into six colored complexes that were indicated in health and diseaseCitation75 ().
Table 2. Bacterial Complexes in Six Colored Groups.
A meta-analysis reviewed the studies that utilized saliva samples and subgingival plaque samples to detect red complex bacteria in more than 60% of the patients with periodontitis. Recent research has highlighted the importance of the interaction between the oral microbiome with the host cell under specific circumstances resulting in a “personalized pathology” of periodontitis.Citation76–78
Peri-implant microbiota has been shown to be less diverse and less variable with a healthy peri-implant environment with mostly Streptococcus (45% to 86%) in the supragingival and subgingival sites. In peri-implantitis, 12 species were enriched, with the red complex bacteria colonizing the most followed by P. endodontalis, F. fastidiosum, Prevotella intermedia and F. nucleatum. Of these, F. nucleatum was closely associated with peri-implant mucositis.Citation79
Caries is a multifactorial oral disease and has been researched extensively.Citation80 It is manifested as a cavitation due to the presence of three factors: aciduric bacteria, carbohydrates from diet and host factors. The process starts with the biofilm in the oral cavity and factors resulting in dysbiosis. Once dysbiosis occurs, certain cariogenic bacteria like Bifidobacterium dentium, Bifidobacterium longum and S. mutans, S. salivarius and A. viscosus and Firmicutes strains are increased in numbers compared to Bacteroidetes.Citation81 Cariogenic microorganisms produce acid that reduces the pH of the oral environment, causing demineralization of the enamel and further loss of tooth structure. Streptococcus mutans, non-mutans Streptococci, Lactobacillus and Actinomyces are involved in this process. Another study reported the beneficial role of the oral biofilm in replenishing nutrients to increase the protective factors of saliva.Citation82 New techniques in genomic analysis have revealed the presence of extracellular polymeric substances (EPS) in the biofilm that is related to virulence factors of pathogenic bacteria like mutans streptococci in early childhood caries.Citation83
Role of Salivaomics in Early Detection of Oral and Systemic Diseases
Salivaomics is the study of the various components of saliva and the genomics, proteomics, transcriptomics, metabolomics and microbiomics.Citation84 Emerging technology that detects specific biomarkers in saliva could be revolutionary in terms of personalized and precision medicine.Citation85 This biomarker technology can be used in all branches of health care to facilitate prevention, diagnosis, prognosis and management of diseases and conditions. Saliva could be easily utilized in point-of-care applications at medical and dental offices because of convenient collecting and testing. The FDA-NIH defines biomarkers as “defined characteristics that (are) measured as indicator(s) of normal biological processes, pathogenic processes or response to an exposure or intervention, including therapeutic interventions.”Citation86 Biomarkers in the biofluids could be classified into susceptibility biomarkers; screening and diagnostic biomarkers; prognostic biomarkers; predictive biomarkers; response or safety biomarkers; and monitoring biomarkers.
The identification of biomarkers in biofluids especially saliva is an inexpensive, noninvasive method for prevention, early diagnosis and therapeutic interventions for many oral and systemic diseases. Human whole mouth saliva (WMS) contains DNA, RNA, microRNA, messenger RNA, proteins, peptides, cytokines, profilin, transferrin and many more biomarkers that indicate premalignant lesions and cancer in the oral cavity.Citation87 MicroRNA as a biomarker could be significant for certain types of cancer and inflammatory and autoimmune conditions.Citation88 Salivary cortisol levels have been used as a biomarker for oral lichen planus.Citation89 Measuring levels of uric acid could be a diagnostic for metabolic syndromes, cancer, neurological conditions, HIV, psychiatric conditions and gout.Citation90 Patients with Crohn’s disease had decreased activity of antioxidants and increased lipid peroxidation. Salivary diagnostics show that malondialdehyde is a good biomarker for Crohn’s disease along with overexpression of certain types of microRNA.Citation91 Salivary diagnostics in a patient with Sjogren’s syndrome has detected twice the amount of lipids and elevated level of IgA, IgG, IL-6, prostaglandins and antibodies compared to healthy individuals. Some salivary biomarkers for Sjogren’s syndrome are profilin, anhydrase-I, IL-4 and IL-5. C-reactive proteins, cardiac troponin and creatinine phosphokinase are whole-mouth salivary biomarkers for cardiovascular diseases.Citation92 A recent study found differences in salivary versus serum in levels of glucose, amylase, calcium and phosphorus in diabetic versus nondiabetic patients.Citation93
One study utilized nuclear magnetic resonance (NMR) metabolomicsCitation94 to understand the biomarkers responsible for the diagnosis and prognosis and monitoring of several types of oral and systemic cancers.Citation95 The data collected from this study may be used to design targeted therapy and interventions for patients.
The biggest limitation has been difficulty in finding specific biomarkers for oral and systemic diseases. Most of the biomarkers already discovered from various research are generic biomarkers of inflammation or infection. Moreover, the presence of biomarkers in the saliva is influenced by many factors such as the circadian cycle, diet and so on. The challenges of implementing point-of-care salivary diagnostics are understanding the collection guidelines, storage and processing protocols and the need for improvement in the standardization. Further studies on the specificity and the sensitivity of these salivary diagnostics are required for accuracy. In summary, point-of-care salivary diagnostics could be the answer to understanding the oral systemic connection and dysbiosis in the oral-gut-brain-liver-lung axes and addressing the needs of our patients with complex medical needs.Citation96
If implemented into clinical practice, salivary diagnostics could lead to a paradigm shift in treatment of oral and systemic diseases with a focus on the reversal of dysbiosisCitation97 and targeted interventions aimed at the microbial interactions in the microbiome including phage therapy, probiotics and prebiotic supplements,Citation98 photodynamic therapy, quorum-quenching therapy, antibiotics bound to nanoparticles (NP) or oral microbiome transplants.
Conclusion
Although there have been multiple studies on the oral dysbiosis and its effects on systemic diseases; this is just the tip of the iceberg with regard to understanding the complexity of the relationship between the host cells and the oral microbiome. Further research on the unculturable oral microbiota may be essential to map out the key players that initiate, facilitate and advance oral and non-oral diseases. The first step is to periodically educate and train oral health-care professionals on this crucial topic. The next step is to implement salivary diagnostics as part of screening at routine dental visits to assess risk factors. Educating other health-care providers and forming alliances with them to coordinate care would elevate the quality of care and improve outcomes. Longitudinal studies on dysbiosis and treatment outcomes aided by salivary diagnostics may be the future. Translational research on designing precision medicine that is directed toward prevention is the goal.
Additional information
Notes on contributors
Parvati Iyer
Parvati Iyer is a tenure-track Assistant Professor in the Department of Diagnostic Sciences at the University of the Pacific, School of Dentistry. After graduating from the University of Michigan, School of Dentistry, and completing a residency in Hospital Dentistry at the University of California San Francisco, she practiced cosmetic dentistry in Scottsdale, AZ. She has been an academic since 2011 and has developed an identity as an educational researcher. Parvati is the recipient of the Omicron Kappa Upsilon Charles Craig Award for Teaching Innovation in 2020 and is passionate about promoting critical thinking, utilizing technology to teach, and increasing student engagement in an integrated curriculum. She is a Fellow of Pierre Fauchard Academy, ADA, CDA, and the San Francisco Dental Society.
References
- Peng X, Cheng L, You Y, et al. Oral microbiota in human systematic diseases. Int J Oral Sci. 2022;14(1):14. doi:10.1038/s41368-022-00163-7.
- Deo PN, Deshmukh R. Oral microbiome: unveiling the fundamentals. J Oral Maxillofac Pathol. 2019;23(1):122–11. doi:10.4103/jomfp.JOMFP_304_18.
- Kilian M, Chapple IL, Hannig M, et al. The oral microbiome - an update for oral healthcare professionals. Br Dent J. 2016;221(10):657–666. doi:10.1038/sj.bdj.2016.865.
- Lee YH, Chung SW, Auh QS, et al. Progress in oral microbiome related to oral and systemic diseases: an update. Diagn (Basel). 2021;11(7):1283. doi:10.3390/diagnostics11071283.
- Edlund A, Santiago-Rodriguez TM, Boehm TK, Pride DT. Bacteriophage and their potential roles in the human oral cavity. J Oral Microbiol. 2015;7(1):27423. doi:10.3402/jom.v7.27423.
- Pride DT, Salzman J, Haynes M, et al. Evidence of a robust resident bacteriophage population revealed through analysis of the human salivary virome. ISME J. 2012;6(5):915–926. doi:10.1038/ismej.2011.169.
- Parras-Moltó M, López-Bueno A. Methods for enrichment and sequencing of oral viral assemblages: saliva, oral mucosa, and dental plaque viromes. Methods Mol Biol. 2018;1838:143–161. doi:10.1007/978-1-4939-8682-8_11.
- Berg G, Rybakova D, Fischer D, et al. Microbiome definition re-visited: old concepts and new challenges. Microbiome. 2020;8(1):103. doi:10.1186/s40168-020-00875-0.
- Tutuncu EE, Ozgur D, Karamese M. Saliva samples for detection of SARS-CoV-2 in mildly symptomatic and asymptomatic patients. J Med Virol. 2021;93(5):2932–2937. doi:10.1002/jmv.26821.
- Dubé CD, Guiot SR. Direct interspecies electron transfer in anaerobic digestion: a review. Adv Biochem Eng Biotechnol. 2015;151:101–115. doi:10.1007/978-3-319-21993-6_4.
- Amerongen AV, Veerman EC. Saliva–the defender of the oral cavity. Oral Dis. 2002;8(1):12–22. doi:10.1034/j.1601-0825.2002.1o816.x.
- Fábián TK, Hermann P, Beck A, Fejérdy P, Fábián G. Salivary defense proteins: their network and role in innate and acquired oral immunity. Int J Mol Sci. 2012;13(4):4295–4320. doi:10.3390/ijms13044295.
- Li X, Kolltveit KM, Tronstad L, Olsen I. Systemic diseases caused by oral infection. Clin Microbiol Rev. 2000;13(4):547–558. doi:10.1128/CMR.13.4.547.
- Abdelbary MMH, Hatting M, Bott A, et al. The oral-gut axis: salivary and fecal microbiome dysbiosis in patients with inflammatory bowel disease. Front Cell Infect Microbiol. 2022;12:1010853. doi:10.3389/fcimb.2022.1010853.
- Kitamoto S, Nagao-Kitamoto H, Hein R, Schmidt TM, Kamada N. The bacterial connection between the oral cavity and the gut diseases. J Dent Res. 2020;99(9):1021–1029. doi:10.1177/0022034520924633.
- Atarashi K, Suda W, Luo C, et al. Ectopic colonization of oral bacteria in the intestine drives TH cell induction and inflammation. Science. 2017;358(6361):359–365. doi:10.1126/science.aan4526.
- Qi Y, Wu HM, Yang Z, et al. New insights into the role of oral microbiota dysbiosis in the pathogenesis of inflammatory bowel disease. Dig Dis Sci. 2022;67(1):42–55. doi:10.1007/s10620-021-06837-2.
- Zhao H, Zhang W, Cheng D, You L, Huang Y, Lu Y. Investigating dysbiosis and microbial treatment strategies in inflammatory bowel disease based on two modified Koch’s postulates. Front Med (Lausanne). 2022;9:1023896. doi:10.3389/fmed.2022.1023896.
- Kuraji R, Sekino S, Kapila Y, Numabe Y. Periodontal disease-related nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: an emerging concept of oral-liver axis. Periodontol 2000. 2021;87(1):204–240. doi:10.1111/prd.12387.
- Yoneda M, Naka S, Nakano K, et al. Involvement of a periodontal pathogen, porphyromonas gingivalis on the pathogenesis of non-alcoholic fatty liver disease. BMC Gastroenterol. 2012;12(1):16. doi:10.1186/1471-230X-12-16.
- Abe K, Fujita M, Hayashi M, Okai K, Takahashi A, Ohira H. Gut and oral microbiota in autoimmune liver disease. Fukushima J Med Sci. 2020;65(3):71–75. doi:10.5387/fms.2019-21.
- Rao B, Lou J, Lu H, et al. Oral microbiome characteristics in patients with autoimmune hepatitis. Front Cell Infect Microbiol. 2021;11:656674. doi:10.3389/fcimb.2021.656674.
- Bajaj JS, Matin P, White MB, et al. Periodontal therapy favorably modulates the oral-gut-hepatic axis in cirrhosis. Am J Physiol Gastrointestinal Liver Physiol. 2018;315(5):G824–837. doi:10.1152/ajpgi.00230.2018.
- Xiao E, Mattos M, Vieira GHA, et al. Diabetes enhances IL-17 expression and alters the oral microbiome to increase its pathogenicity. Cell Host & Microbe. 2017;22(1):120–128.e4. doi:10.1016/j.chom.2017.06.014.
- Matsha TE, Prince Y, Davids S, et al. Oral microbiome signatures in diabetes mellitus and periodontal disease. J Dent Res. 2020;99(6):658–665. doi:10.1177/0022034520913818.
- Negrini TC, Carlos IZ, Duque C, Caiaffa KS, Arthur RA. Interplay among the oral microbiome, oral cavity conditions, the host immune response, diabetes mellitus, and its associated-risk factors-an overview. Frontiers in Oral Health. 2021;2:697428. doi:10.3389/froh.2021.697428.
- Isola G, Polizzi A, Santonocito S, Alibrandi A, Williams RC. Periodontitis activates the NLRP3 inflammasome in serum and saliva. J Periodontol. 2022;93(1):135–145. doi:10.1002/JPER.21-0049.
- Coker MO, Lebeaux RM, Hoen AG, et al. Metagenomic analysis reveals associations between salivary microbiota and body composition in early childhood. Sci Rep. 2022;12(1):13075. doi:10.1038/s41598-022-14668-y.
- Keller A, Rohde JF, Raymond K, Heitmann BL. Association between periodontal disease and overweight and obesity: a systematic review. J Periodontol. 2015;86(6):766–776. doi:10.1902/jop.2015.140589.
- Li N, Li Y, Qian C, et al. Dysbiosis of the saliva microbiome in patients with polycystic ovary syndrome. Front Cell Infect Microbiol. 2021;10:624504. doi:10.3389/fcimb.2020.624504.
- Yang Y, Cai Q, Zheng W, et al. Oral microbiome and obesity in a large study of low-income and African-American populations. J Oral Microbiol. 2019;11(1):1650597. doi:10.1080/20002297.2019.1650597.
- Giordano-Kelhoffer B, Lorca C, March Llanes J, et al. Oral microbiota, its equilibrium, and implications in the pathophysiology of human diseases: a systematic review. Biomedicines. 2022;10(8):1803. doi:10.3390/biomedicines10081803.
- Bartova J, Sommerova P, Lyuya-Mi Y, et al. Periodontitis as a risk factor of atherosclerosis. J Immunol Res. 2014;2014:636893. doi:10.1155/2014/636893.
- Zhang J, Xie M, Huang X, et al. The effects of porphyromonas gingivalis on atherosclerosis-related cells. Front Immunol. 2021;12:766560. doi:10.3389/fimmu.2021.766560.
- Blekkenhorst LC, Bondonno NP, Liu AH, et al. Nitrate, the oral microbiome, and cardiovascular health: a systematic literature review of human and animal studies. Am J Clin Nutr. 2018;107(4):504–522. doi:10.1093/ajcn/nqx046.
- Koch CD, Gladwin MT, Freeman BA, Lundberg JO, Weitzberg E, Morris A. Enterosalivary nitrate metabolism and the microbiome: intersection of microbial metabolism, nitric oxide, and diet in cardiac and pulmonary vascular health. Free Radical Biology & Medicine. 2017;105:48–67. doi:10.1016/j.freeradbiomed.2016.12.015.
- Hezel MP, Weitzberg E. The oral microbiome and nitric oxide homoeostasis. Oral Dis. 2015;21(1):7–16. doi:10.1111/odi.12157.
- Kapil V, Haydar SM, Pearl V, Lundberg JO, Weitzberg E, Ahluwalia A. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radical Biology & Medicine. 2013;55:93–100. doi:10.1016/j.freeradbiomed.2012.11.013.
- Pussinen PJ, Kopra E, Pietiäinen M, et al. Periodontitis and cardiometabolic disorders: the role of lipopolysaccharide and endotoxemia. Periodontol 2000. 2022;89(1):19–40. doi:10.1111/prd.12433.
- Kleinstein SE, Nelson KE, Freire M. Inflammatory networks linking oral microbiome with systemic health and disease. J Dent Res. 2020;99(10):1131–1139. doi:10.1177/0022034520926126.
- Kumar PS, Matthews CR, Joshi V, de Jager M, Aspiras M. Tobacco smoking affects bacterial acquisition and colonization in oral biofilms. Infect Immun. 2011;79(11):4730–4738. doi:10.1128/IAI.05371-11.
- Mammen MJ, Scannapieco FA, Sethi S. Oral‐lung microbiome interactions in lung diseases. Periodontol 2000. 2020;83(1):234–241. doi:10.1111/prd.12301.
- Pathak JL, Yan Y, Zhang Q, Wang L, Ge L. The role of oral microbiome in respiratory health and diseases. Respir Med. 2021;185:106475. doi:10.1016/j.rmed.2021.106475.
- Bassis CM, Erb-Downward JR, Dickson RP, et al. Analysis of the upper respiratory tract microbiotas as the source of the lung and gastric microbiotas in healthy individuals. MBio. 2015;6(2):e00037. doi:10.1128/mBio.00037-15.
- Didilescu AC, Skaug N, Marica C, Didilescu C. Respiratory pathogens in dental plaque of hospitalized patients with chronic lung diseases. Clin Oral Investig. 2005;9(3):141–147. doi:10.1007/s00784-005-0315-6.
- Mammen MJ, Sethi S. COPD and the microbiome. Respirology. 2016;21(4):590–599. doi:10.1111/resp.12732.
- Willis JR, Saus E, Iraola-Guzmán S, et al. Citizen-science based study of the oral microbiome in cystic fibrosis and matched controls reveals major differences in diversity and abundance of bacterial and fungal species. J Oral Microbiol. 2021;13(1):1897328. doi:10.1080/20002297.2021.1897328.
- Fleury V, Zekeridou A, Lazarevic V, et al. Oral dysbiosis and inflammation in parkinson’s disease. J Parkinson’s Dis. 2021;11(2):619–631. doi:10.3233/JPD-202459.
- Fan Z, Li Z, Zhao S, et al. Salivary Aβ1–42 may be a quick-tested biomarker for clinical use in Alzheimer’s disease: a meta-analysis. J Neurol. 2022. doi:10.1007/s00415-022-11509-w.
- Liu S, Dashper SG, Zhao R. Association between oral bacteria and alzheimer’s disease: a systematic review and meta-analysis. J Alzheimer Dis. 2022; Advance online publication. doi:10.3233/JAD-220627.
- Li C, Chen Y, Wen Y, et al. A genetic association study reveals the relationship between the oral microbiome and anxiety and depression symptoms. Front Psychiatry. 2022;13:960756. doi:10.3389/fpsyt.2022.960756.
- Simpson CA, Adler C, du Plessis MR, et al. Oral microbiome composition, but not diversity, is associated with adolescent anxiety and depression symptoms. Physiol Behav. 2020;226:113126. doi:10.1016/j.physbeh.2020.113126.
- Wingfield B, Lapsley C, McDowell A, et al. Variations in the oral microbiome are associated with depression in young adults. Sci Rep. 2021;11(1):15009. doi:10.1038/s41598-021-94498-6.
- Ahrens AP, Sanchez-Padilla DE, Drew JC, Oli MW, Roesch L, Triplett EW. Saliva microbiome, dietary, and genetic markers are associated with suicidal ideation in university students. Sci Rep. 2022;12(1):14306. doi:10.1038/s41598-022-18020-2.
- Yuan S, Fang C, Leng WD, et al. Oral microbiota in the oral-genitourinary axis: identifying periodontitis as a potential risk of genitourinary cancers. Mil Med Res. 2021;8(1):54. doi:10.1186/s40779-021-00344-1.
- Fang C, Wu L, Zhu C, Xie WZ, Hu H, Zeng XT. A potential therapeutic strategy for prostatic disease by targeting the oral microbiome. Med Res Rev. 2021;41(3):1812–1834. doi:10.1002/med.21778.
- Alwithanani N, Bissada NF, Joshi N, et al. Periodontal treatment improves prostate symptoms and lowers serum PSA in men with high PSA and chronic periodontitis. Dentistry. 2015;5(3):1. doi:10.4172/2161-1122.1000284.
- Lee J, Roberts JS, Atanasova KR, Chowdhury N, Yilmaz Ö. A novel kinase function of a nucleoside‐diphosphate‐kinase homologue in porphyromonas gingivalis is critical in subversion of host cell apoptosis by targeting heat‐shock protein 27. Cell Microbiol. 2018;20(5):e12825. doi:10.1111/cmi.12825.
- Meurman JH, Uittamo J. Oral micro-organisms in the etiology of cancer. Acta Odontol Scand. 2008;66(6):321–326. doi:10.1080/00016350802446527.
- Nauclér CS, Geisler J, Vetvik K. The emerging role of human cytomegalovirus infection in human carcinogenesis: a review of current evidence and potential therapeutic implications. Oncotarget. 2019;10(42):4333–4347. doi:10.18632/oncotarget.27016.
- Peters BA, Wu J, Pei Z, et al. Oral microbiome composition reflects prospective risk for esophageal cancers. Cancer Res. 2017;77(23):6777–6787. doi:10.1158/0008-5472.CAN-17-1296.
- Castellarin M, Warren RL, Freeman JD, et al. Fusobacterium nucleatum infection is prevalent in human colorectal carcinoma. Genome Res. 2012;22(2):299–306. doi:10.1101/gr.126516.111.
- Gaba FI, González RC, Martïnez RG. The role of oral Fusobacterium nucleatum in female breast cancer: a systematic review and meta-analysis. Int J Dent. 2022;2022:1876275. doi:10.1155/2022/1876275.
- Cobb CM, Kelly PJ, Williams KB, Babbar S, Angolkar M, Derman RJ. The oral microbiome and adverse pregnancy outcomes. Int J Women Health. 2017;9:551–559. doi:10.2147/IJWH.S142730.
- Balan P, Chong YS, Umashankar S, et al. Keystone species in pregnancy gingivitis: a snapshot of oral microbiome during pregnancy and postpartum period. Front Microbiol. 2018;9:2360. doi:10.3389/fmicb.2018.02360.
- Ye C, You M, Huang P, et al. Clinical study showing a lower abundance of Neisseria in the oral microbiome aligns with low birth weight pregnancy outcomes. Clin Oral Investig. 2022;26(3):2465–2478. doi:10.1007/s00784-021-04214-x.
- Wang X, Buhimschi CS, Temoin S, Bhandari V, Han YW, Buhimschi IA. Comparative microbial analysis of paired amniotic fluid and cord blood from pregnancies complicated by preterm birth and early-onset neonatal sepsis. PLoS One. 2013;8(2):e56131. doi:10.1371/journal.pone.0056131.
- Cheng Z, Do T, Mankia K, et al. Dysbiosis in the oral microbiomes of anti-CCP positive individuals at risk of developing rheumatoid arthritis. Ann Rheum Dis. 2021;80(2):162–168. doi:10.1136/annrheumdis-2020-216972.
- Corrêa JD, Calderaro DC, Ferreira GA, et al. Subgingival microbiota dysbiosis in systemic lupus erythematosus: association with periodontal status. Microbiome. 2017;5(1):34. doi:10.1186/s40168-017-0252-z.
- Hajishengallis G, Chavakis T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat Rev Immunol. 2021;21(7):426–440. doi:10.1038/s41577-020-00488-6.
- Tseng YC, Yang HY, Lin WT, et al. Salivary dysbiosis in Sjögren’s syndrome and a commensal-mediated immunomodulatory effect of salivary gland epithelial cells. NPJ Biofilms Microbiomes. 2021;7(1):21. doi:10.1038/s41522-021-00192-w.
- Singh H, Torralba MG, Moncera KJ, et al. Gastro-intestinal and oral microbiome signatures associated with healthy aging. Geroscience. 2019;41(6):907–921. doi:10.1007/s11357-019-00098-8.
- Lazarevic V, Manzano S, Gaïa N, et al. Effects of amoxicillin treatment on the salivary microbiota in children with acute otitis media. Clin Microbiol Infect. 2013;19(8):E335–342. doi:10.1111/1469-0691.12213.
- Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr. Microbial complexes in subgingival plaque. J Clin Periodontol. 1998;25(2):134–144. doi:10.1111/j.1600-051x.1998.tb02419.x.
- Christina P, Velitchka DP, Vladimir P. Microbiology of periodontal diseases. A Rev, Biotechnol Biotechnol Equip. 2013;27(3):3754–3759. doi:10.5504/BBEQ.2013.0027.
- Scannapieco FA, Dongari-Bagtzoglou A. Dysbiosis revisited: understanding the role of the oral microbiome in the pathogenesis of gingivitis and periodontitis: a critical assessment. J Periodontol. 2021;92(8):1071–1078. doi:10.1002/JPER.21-0120.
- Zhu J, Chu W, Luo J, Yang J, He L, Li J. Dental materials for oral microbiota dysbiosis: an update. Front Cell Infect Microbiol. 2022;12:900918. doi:10.3389/fcimb.2022.900918.
- Struzycka I. The oral microbiome in dental caries. Pol J Microbiol. 2014;63(2):127–135. doi:10.33073/pjm-2014-018.
- Inchingolo AD, Malcangi G, Semjonova A, et al. Oralbiotica/Oralbiotics: the impact of oral microbiota on dental health and demineralization: a systematic review of the literature. Children (Basel). 2022;9(7):1014. doi:10.3390/children9071014.
- Kaidonis J, Townsend G. The ‘sialo-microbial-dental complex’ in oral health and disease. Ann Anat. 2016;203:85–89. doi:10.1016/j.aanat.2015.02.002.
- Bowen WH, Burne RA, Wu H, Koo H. Oral biofilms: pathogens, matrix, and polymicrobial interactions in microenvironments. Trends Microbiol. 2018;26(3):229–242. doi:10.1016/j.tim.2017.09.008.
- Kaczor-Urbanowicz KE, Martin Carreras-Presas C, Aro K, Tu M, Garcia-Godoy F, Wong DT. Saliva diagnostics - current views and directions. Exp Biol Med (Maywood). 2017;242(5):459–472. doi:10.1177/1535370216681550.
- Dawes C, Wong D. Role of saliva and salivary diagnostics in the advancement of oral health. J Dent Res. 2019;98(2):133–141. doi:10.1177/0022034518816961.
- Landry V, Coburn P, Kost K, Liu X, Li-Jessen N. Diagnostic accuracy of liquid biomarkers in airway diseases: toward point-of-care applications. Front Med (Lausanne). 2022;9:855250. doi:10.3389/fmed.2022.855250.
- Khurshid Z, Zafar MS, Khan RS, Najeeb S, Slowey PD, Rehman IU. Role of salivary biomarkers in oral cancer detection. Adv Clin Chem. 2018;86:23–70. doi:10.1016/bs.acc.2018.05.002.
- Setti G, Pezzi ME, Viani MV, et al. Salivary MicroRNA for diagnosis of cancer and systemic diseases: a systematic review. Int J Mol Sci. 2020;21(3):907. doi:10.3390/ijms21030907.
- Martina E, Campanati A, Diotallevi F, Offidani A. Saliva and oral diseases. J Clin Med. 2020;9(2):466. doi:10.3390/jcm9020466.
- Jaiswal A, Madaan S, Acharya N, Kumar S, Talwar D, Dewani D. Salivary uric acid: a noninvasive wonder for clinicians? Cureus. 2021;13(11):e19649. doi:10.7759/cureus.19649.
- Nijakowski K, Surdacka A. Salivary biomarkers for diagnosis of inflammatory bowel diseases: a systematic review. Int J Mol Sci. 2020;21(20):7477. doi:10.3390/ijms21207477.
- Khan RS, Khurshid Z, Yahya Ibrahim Asiri F. Advancing point-of-care (PoC) testing using human saliva as liquid biopsy. Diagn (Basel). 2017;7(3):39. doi:10.3390/diagnostics7030039.
- Ladgotra A, Verma P, Raj SS. Estimation of salivary and serum biomarkers in diabetic and non-diabetic patients - a comparative study. J Clin Diagn Res. 2016;10(6):ZC56–61. doi:10.7860/JCDR/2016/19135.7995.
- Grootveld M, Percival BC, Page G, et al. Updates and original case studies focused on the nmr-linked metabolomics analysis of human oral fluids part II: applications to the diagnosis and prognostic monitoring of oral and systemic cancers. Metabolites. 2022;12(9):778. doi:10.3390/metabo12090778.
- Assad DX, Mascarenhas ECP, de Lima CL, et al. Salivary metabolites to detect patients with cancer: a systematic review. Int J Clin Oncol. 2020;25(6):1016–1036. doi:10.1007/s10147-020-01660-7.
- Kapila YL. Oral health’s inextricable connection to systemic health: special populations bring to bear multimodal relationships and factors connecting periodontal disease to systemic diseases and conditions. Periodontol 2000. 2021;87(1):11–16. doi:10.1111/prd.12398.
- Radaic A, Kapila YL. The oralome and its dysbiosis: new insights into oral microbiome-host interactions. Comput Struct Biotechnol J. 2021;19:1335–1360. doi:10.1016/j.csbj.2021.02.010.
- Tanner A, Kressirer CA, Rothmiller S, Johansson I, Chalmers NI. The caries microbiome: implications for reversing dysbiosis. Adv Dent Res. 2018;29(1):78–85. doi:10.1177/0022034517736496.
- Gheisary Z, Mahmood R, Harri Shivanantham A, et al. The clinical, microbiological, and immunological effects of probiotic supplementation on prevention and treatment of periodontal diseases: a systematic review and meta-analysis. Nutrients. 2022;14(5):1036. doi:10.3390/nu14051036.
- Nath S, Zilm P, Jamieson L, et al. Development and characterization of an oral microbiome transplant among Australians for the treatment of dental caries and periodontal disease: a study protocol. PLoS One. 2021;16(11):e0260433. doi:10.1371/journal.pone.0260433.