
Abstract
We introduce here a general model of Functional Neurological Disorders based on the following hypothesis: a Functional Neurological Disorder could correspond to a consciously initiated voluntary top-down process causing involuntary lasting consequences that are consciously experienced and subjectively interpreted by the patient as involuntary. We develop this central hypothesis according to Global Neuronal Workspace theory of consciousness, that is particularly suited to describe interactions between conscious and non-conscious cognitive processes. We then present a list of predictions defining a research program aimed at empirically testing their validity. Finally, this general model leads us to reinterpret the long-debated links between hypnotic suggestion and functional neurological disorders. Driven by both scientific and therapeutic goals, this theoretical paper aims at bringing closer the psychiatric and neurological worlds of functional neurological disorders with the latest developments of cognitive neuroscience of consciousness.
Introduction
While Functional Neurological Disorders (FND) rank among the most frequent category of diagnostics of both acute and chronic neurological or psychiatric conditions (up to ∼10-20% of neurology outpatients (Stone et al. Citation2009; Carson and Lehn Citation2016), and see (Garcin et al. Citation2021) for a focus on motor FND), our understanding of their mechanisms is still very limited, as well as our therapeutic efficacy for the affected patients (Espay et al. Citation2018).
In this extremely challenging context, we propose here a new general hypothesis that aims at proposing a unifying mechanistic account of various types of FND. This hypothesis and its corresponding framework originate both from our neurological experience of patients with FND, and from the Global Neuronal Workspace Theory (GNWT) of consciousness we are contributing to since its original formulation (Dehaene and Naccache Citation2001; Naccache Citation2006).
The starting point of the present hypothesis is twofold.
Residual dualism of FND conceptualisation
First, we identified an apparent form of residual dualism inherent to the conceptualisation of FND, at least since the end of nineteenth century and the iconic figure of Jean-Martin Charcot and the ‘Ecole de la Salpêtrière’ (Charcot Citation1875; Ellenberger Citation1965). This residual dualism is best captured by the weird opposition between diseases of ‘CNS structure’ on the one hand (i.e.: the concept of ‘organicity’), and diseases of ‘CNS function’ on the other hand that include FND. This original residual dualism seems to have spread until today, as evidenced by the current name of this clinical category that refers to an idea of cleavage: the adjective ‘Functional’ of ‘Functional Neurological Disorders’ clearly points to their radical distinction from organic diseases. As if function and structure of a biological system were two independent and divided attributes. At the contrary of this division, modern biology demonstrated that ultimate resolution of discrete natural objects reveal the strong entanglement of function and structure (e.g.: allosteric transitions of a protein with a tight relation between fine molecular structure and corresponding enzymatic functions (Monod et al. Citation1965). This dualistic aporia is also present in the previous names of FND, - that changed across time and space -, from ‘conversive disorders’ (i.e.: a conversion from the mind to the body) up to ‘Dissociative Neurological Symptom Disorder’ (i.e.,: a dissociation within the same mind) according to the ICD-11 (World Health Organisation International Coding manual).
From a historical point of view, it is remarkable that epilepsy, - long considered the emblematic illustration of a ‘functional neurological disorder’ -, was confused with FND under the generic name of ‘hystero-epilepsy’ (Charcot Citation1875).
One may consider this dualism being driven either by a motivation of reassuring patients about the absence of severe underlying disease (e.g.: multiple sclerosis, brain tumour, stroke, neurodegenerative disorder…), of by a kind of ‘diagnostic humility’: as if clinicians dissociated diseases with identified physical causes from those that remain out of reach. However, none of these two reasons justifies the need to translate this dichotomy into such a dualist perspective.
What type of symptoms-agentivity in FND patients?
Second, FND also raise the issue of agentivity of symptoms. Up to which point the large repertoire of FND symptoms, that can include both positive (e.g.: various types of movements and behaviours) and negative phenomena (e.g.: sensory-motor deficit, memory impairment, etc…), correspond to voluntary or to involuntary processes? It is noteworthy that this issue remains at stake even after clearly differentiating FND from pretending or malingering. Indeed, specificities of neurological examination of FND include various suggestive manoeuvres, distraction of voluntary attention to modulate positive symptoms such as the famous Hoover manoeuvre and related signs (Garcin Citation2018). What type of agentivity should we attribute to a symptom distinguished from malingering, but still sensitive to distraction of patient’s voluntary attention?
A last argument stems from the subjective experience reported by many clinicians in charge of FND patients, and that we may coin as an ‘uncanny mixed feeling of voluntary/involuntary symptoms’: this irrepressible feeling of a certain form of voluntary participation in the symptoms, in a patient who is not malingering.
Towards a voluntary then involuntary general model of FND
By combining the ‘residual dualism’ issue with the agentivity issue, we came up with the following general mechanistic hypothesis that may solve these two challenging premises (Naccache Citation2006):
Main Hypothesis: A FND could correspond to a consciously initiated voluntary top-down process causing involuntary lasting consequences (i.e.,: FND symptoms), that are consciously experienced and subjectively interpreted by the patient as involuntary.
Indeed, such a scenario may explain the uncanny mixed feeling exposed above by a diachronic phenomenon: if symptoms result from a voluntary process triggering behavioural or cognitive consequences perceived by the patient as being involuntary, they could indeed combine both voluntary and involuntary attributes separated in time. Also, the apparent ‘residual dualism’ conceptualisation of FND could be interpreted as a failed attempt to dissociate diseases that are not depending on voluntary top-down cognitive processes (i.e.: so-called ‘organic’ diseases), from those who would require a voluntary top-down triggering (i.e.: FND).
We close this introductory section by two methodological remarks and a definition clarification.
First, in this theoretical contribution, we tried to support and test our ideas and predictions in the light of the current empirical evidence. We also listed a series of explicit prediction that delineate a FND research program (see ). However, in several aspects our work remains speculative, and aims at stimulating new perspectives to address the major clinical and theoretical challenges raised by FND.
Second, our model is inspired by the GNWT of consciousness. Therefore, we will not address and discuss here alternative theories of consciousness such as Integrated Information Theory (IIT) (Tononi et al. Citation2016), Higher-Order-Thought (HOT) (Rosenthal Citation2000) or local recurrence (Lamme and Roelfsema Citation2000) models. Indeed, core ideas and predictions of the present work are specific to the functional architecture of GNW.
As for our clarification remark, we explicit here our use of the two couples of words ‘conscious/unconscious’ and ‘voluntary/involuntary’, as well as their possible combinations. We define a mental representation or a cognitive process as conscious if it is self-reported by the individual. Self-reportability criterion has the following valuable attributes: (i) it can be used for any conscious content (self-reportability of sensory, but also of motor, intentional, mnesic, emotional, … contents), (ii) it provides a solid basis to define unconscious cognition, (iii) it is not necessarily verbal and be probed with behavioural and neural measures in aphasic patients, in preverbal infants, and in other species, (iv) it does not have to be confounded with behaviours used to communicate this inner cognitive process to external observers (Dehaene and Naccache Citation2001; Naccache Citation2018). Similarly, a cognitive process is defined as being voluntary if it is associated with a conscious feeling of agentivity (e.g.: I am the agent of this act, thought or process). According to this terminology, conscious voluntary cognitive processes are both both self-reported and associated to a feeling of agentivity (e.g.: I want to forget X). Conscious but involuntary processes are self-reported but lack agentivity (e.g.: My right hand is shaking). Unconscious representations or processes are by definition involuntary. However, and as exposed below in Section “Existence of conscious influences on some unconscious processes”, some conscious processes can influence unconscious cognition unbeknownst to the individual.
Existence of conscious influences on some unconscious processes
Our hypothesis relies on the existence of conscious influences on various unconscious cognitive processes. This core and original concept has been stated and developed during the last 30 years, on the basis of both theoretical and empirical approaches. Until then, unconscious cognitive processes were mostly theorised through the theories of automaticity (Posner and Snyder Citation1975; Schneider and Shiffrin Citation1977; Eysenck Citation1984) and modularity (Fodor Citation1983). According to these dominant views, unconscious cognitive processes were not accessible to cognitive control and in particular to voluntary conscious processes mediated by top-down control (see Explanatory box #1 for a brief summary of the conceptual change). We will therefore retain the existence of conscious influences on various unconscious cognitive processes. This fundamental result strengthens the plausibility of our general hypothesis. We define here the expression ‘conscious posture’ as a GNW configuration associated with a given conscious intention (e.g.: endogenous orientation of attention to a given time-window or to a specific space location, or intentional forgetting, …).
It is noteworthy that the observation of such top-down modulation of unconscious representations or processes may serve as a diagnostic tool of residual conscious processing in clinical contexts in which this question is at stake. Indeed, if one would be able to demonstrate a modulation of behaviour or of brain activity caused by a top-down effect in a non-communicating patient, this could reveal the existence of a conscious posture responsible for it. Therefore, some univocal markers of conscious processing may concern unconscious activity rather than being direct signatures of conscious processing.
In order to better assess the applicability of this principle to FNDs, it is necessary to precise the scope of unconscious processes that may be (or not) influenced by one’s conscious posture. To do so, we will now develop it within one of the current most influential neurobiological theories of consciousness: the GNWT.
Explanatory box #1: How conscious influences on unconscious processes were discovered
A seminal and lasting tradition of cognitive psychology stated that conscious representations and processes differ from unconscious ones, not only on the sole basis of subjective self-reportable experience, but also on a list of specific and systematic attributes of information processing. The ‘automaticity’ (Posner and Snyder Citation1975; Schneider and Shiffrin Citation1977; Eysenck Citation1984) or ‘modularity’ (Fodor Citation1983) models of unconscious cognition indeed shared this view according to which unconscious mental objects are necessarily: (i) domain specific, (ii) encapsulated, (iii) fast and transient, (iv) out of executive and conscious control. Within such a perspective, while there was a considerable place for theorising unconscious influences on conscious contents and processes, the opposite class of influences was not considered as possible or relevant. Around the mid-80s several experimental findings questioned this radical view. Importantly, most of these results originated from the field of visual priming, in which participants are asked to process voluntarily a target stimulus while ignoring a prime stimulus typically flashed for a brief duration before the target. Priming effects were supposed to be ‘automatic’ and ‘modular’ and to influence conscious target processing, while being out of control. By discovering that prime processing was affected by many factors associated to task-set and to participants’ conscious posture, the alleged ‘automatic’ processing of primes was challenged (see (Stolz and Besner Citation1997) for a comprehensive survey, and (Neely and Kahan Citation2001) for a cautionary analysis of these findings). However, most of these findings were still questionable because prime stimuli were consciously perceptible, and therefore open to executive control. The first general and definitive demonstration of the existence of conscious influences on unconscious processes came from a study in which we manipulated participants’ conscious endogenous temporal attention in a visual masked priming paradigm in which prime stimuli were inaccessible to conscious access. In a set of three experiments, we discovered that unconscious priming effects vanished when temporal attention was focused away from prime onset (Naccache et al. Citation2002). Since this study, a large number of studies confirmed and extended the validity of this major theoretical revision of automaticity. Some unconscious cognitive processes can be flexible (Dehaene and Naccache Citation2006; Naccache Citation2008; Van den Bussche et al. Citation2008; Rohaut et al. Citation2016) and sensitive to various influences including endogenous spatio-temporal attention (Kentridge et al. Citation1999; Naccache et al. Citation2002; Kentridge et al. Citation2008; Rozier et al. Citation2020), conscious consideration of task instructions and stimuli sets (Greenwald et al. Citation2003; Van Opstal et al. Citation2010) and executive control (van Gaal et al. Citation2008; Citation2009; Reuss et al. Citation2014; Schouppe et al. Citation2014). In our 2002 study we proposed to refine the concept of ‘automaticity’ by separating the source of conscious strategical control from its effects: Unconscious “processing is automatic inasmuch it cannot serve as a source of information for the subsequent definition of an explicit strategy. However, this does not imply that it is impermeable to the effects of conscious top-down strategic control, originating from another source of information such as instructions and task context.”
GNWT account of conscious influences on unconscious processes
In order to explore how GNWT could theorise the notion of conscious influences on unconscious representations and processes, we will (i) first provide the reader with a synthetic primer of GNWT, then (ii) derive an updated taxonomy of all possible forms of unconscious activity, and will then propose a new form of involuntary or (inclusive or) unconscious processes coined as ‘GNW-Murmur’.
A primer of GNWT
Basically, GNWT aims at providing a biological account to one key cognitive property of conscious processing first identified by Baars: global availability property of conscious processing (Baars Citation1988). Global availability means that when we are conscious of a given mental object, this object is available to any of our conscious cognitive faculties. In other words, conscious processing which we primarily defined as a self-reported subjective experience, also includes additional specific cognitive properties among which global availability. This conscious global availability corresponds to the breaking of modularity and of automaticity described above (see Section “Existence of conscious influences on some unconscious processes”). One may question the ‘dissociability’ of conscious experience and global availability: could we consciously experience mental objects that are not globally available and self-reportable? According to such a view, reportability would not be considered here as a definition criterion of conscious experience, but only as one of the possible options offered by global availability? This discussion is out of the scope of the present article, but several solid arguments challenge this alternative view (Block Citation1995; Dehaene and Naccache Citation2001; Block Citation2007; Naccache and Dehaene Citation2007; Cohen and Dennett Citation2011; Naccache Citation2018).
GNWT follows a single axiom: the cognitive property of global availability, specific to conscious experience, should find its strict neural equivalence within brain anatomical and functional workings.
GNWT states that two types of neural spaces are present within a healthy primate brain: (i) a large set of distinct and relatively independent modular neural spaces defined as connected specialised networks distributed across a large repertoire of neural hierarchy from primary cortices to associative cortices, and (ii) a single non-modular neural space defined as a brain-scale network connecting high-level specialised processors. This non-modular space shows a rich internal (i.e.: intra-space) anatomical and functional reciprocal connectivity. This last property guarantees that at any given moment, only one representation is encoded within this GNW, in contrast with the set of largely independent modular spaces that can host a large number of simultaneous representations.
The main prediction of GNWT is that at any given moment, a subject is conscious of the current GNW representation, while many unconscious representations can be present in the modular spaces.
Note that GNWT focuses on access to representations rather than to processes, in the perspective originally proposed by Ray Jackendoff (Jackendoff Citation1987) within his ‘Intermediate-Level Representations Theory’ according to which one can only be aware of representations and not of the cognitive and computational processes that operate on them. Note however that this idea is not central to GNWT, and that it does not discard the concept of conscious agentivity: one can be only conscious of the successive states of a given representation (e.g.: X1 then X2), while experiencing his causal role as a conscious agent in the GNW-mediated transformation of X1 to X2.
The last key hypothesis of GNWT concerns the mechanism of conscious access: how do we consciously access one of the representations coded within one of the peripheral modular neural-spaces? GNWT postulates that conscious access is an all-or-none phenomenon mediated by a top-down attentional amplification (also coined ‘ignition’) connecting GNW (through its attentional processors) and the corresponding representation explicitly coded within one of the ‘modular’ neural spaces. This ignition stage requires several conditions to be fulfilled:
reciprocal anatomical connections between the considered cortical region and GNW. Representations encoded in cortical areas lacking such a bidirectional connectivity are predicted to be inaccessible to conscious content, as also predicted for instance by Crick and Koch for V1 lacking such connections with PFC (Crick and Koch Citation1995), and as we could recently illustrate by exploring a patient with cortical blindness (Hauw, Sangare et al. Citation2024)
availability of GNW that can only host one integrated mental representation at a given moment;
a minimal level of intensity and duration of the representation to be mobilised into GNW. Once the representation is mobilised and broadcasted within GNW, conscious subjective experience and global availability would occur as two facets of the same psychological phenomenon.
It is important to note that according to GNWT, while there is a stable core of cortical regions defining the GNW, the precise neuronal frontiers of a current conscious content are ‘fuzzy’ in time: a given modular neural space may well transiently lose its modularity by being mobilised within GNW content through the ignition process described above, while remaining modular at other moments.
Another important aspect of conscious access or ignition is not to confound it with a GNW epileptic seizure: during access all GNW neurons do not fire altogether, but GNW processors keep their differentiation and complexity, and they interact with this broadcasted representation according to the current GNW configuration (Dehaene and Naccache Citation2001; Arthuis et al. Citation2009; Bartolomei and Naccache Citation2011; Bartolomei et al. Citation2014; El Youssef et al. Citation2022).
Finally, according to GNWT, conscious stream would rather correspond to the chaining of discrete conscious contents associated with corresponding discrete states of GNW, each of which would last a few hundreds milliseconds. We proposed the existence of a high-level ‘filling-in’ process that would build the subjective impression of continuity across this chain of discrete conscious states (Naccache Citation2018).
In other terms, a GNW state would be defined as a meta-stable state with a minimal core neural space (core GNW) and for a minimal duration of a few hundreds milliseconds. Transient and focal activations within GNW are predicted to correspond to unconscious processes or representations (see of Dehaene and Naccache (Citation2001)), and have been confirmed by many empirical studies (Dehaene and Naccache Citation2001; Citation2006).
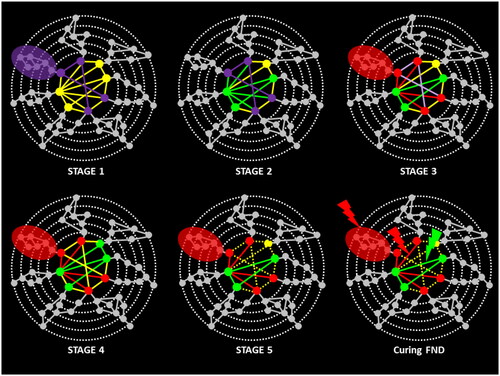
Figure 1. A 5-stages GNW-based model of FND, and of therapeutic interventions.
Legend: Hierarchy of connections between brain processors is symbolised by concentric dotted circles (after (Dehaene et al. Citation1998; Dehaene and Naccache Citation2001) and (Mesulam Citation1998)). Each cortical processor is symbolised by a full disc. Higher levels of this hierarchy (i.e.: the most inner circle) are assumed to be widely interconnected by long-distance interconnections, thus forming a global neuronal workspace. An amplified state of workspace activity, bringing together several peripheral processors in a coherent brain-scale activation pattern (coloured ellipses), can coexist with the automatic activation of multiple local chains of processors outside the workspace (gray circles).
STAGE 1: Conscious access to an emotionally traumatic conscious feeling (for all coloured texts, see corresponding coloured components in the figure)
STAGE 2: Post-experiential voluntary & conscious process: « I would like to forget this feeling »
STAGE 3: Unvoluntary efficient inhibition of specific relevant networks through conscious influences on unconscious processes & through GNW-Murmur
STAGE 4: Conscious access to unvoluntary FND symptoms: « I can’t remember this period »
STAGE 5: Persistence of FND symptoms as long as Stage-2 and Stage-3 processes are actively maintained in GNW activity.
Curing FND: Targeting current symptoms (e.g.: C.B.T.) would act on stage-3 processes, whereas interventions (represented in the figure by coloured lightning symbols) targeting introspection of subjective interpretation of FND would act on stage-2 (e.g.: self-narrative and interpretative psychoterapies).
A GNWT-derived taxonomy of unconscious processes
While all forms of conscious processing share the same GNW attributes, and therefore deserve to be regrouped under a common status (i.e.,: the generic class of conscious contents), unconscious processing can result from multiple distinct mechanisms.
We proposed the following taxonomy of unconscious information types (Dehaene et al. 2006), according to their corresponding neuronal correlates (see ). Basically, a neural information can be accessed to only if it satisfies the following criteria: i) it has to be actively encoded in neural activity and not only in neural structure such as in synaptic weights or axonal lengths; ii) it has to be encoded into an explicit neuronal code; iii) it has to be coded in a network sharing bidirectional connections with GNW neurons; iv) it has to cross a certain threshold; v) and it has to occur while GNW is not occupied by another content for a duration that would exceed the duration and intensity threshold requirement (see iv).
Table 1. Taxonomy of possible unconscious cognitive processes in a conscious individual.
A New class of involuntary and unconscious processes depending on GNW activity: ‘GNW-Murmur’
We showed above the existence of various types of conscious top-down influences on unconscious representations and processes (see Section “Existence of conscious influences on some unconscious processes”). In addition to such GNW top-down modulations exerted on the concerned ‘modular’ workspaces, some other phenomenon may correspond to involuntary processes depending on conscious processing by a within-GNW mechanism. A representation that is consciously accessed is processed by specific GNW processors that are coordinated according to the current task or more generally to the current conscious posture. As a consequence of this specific GNW configuration, some GNW processors are interacting closely together. This close interaction could induce involuntary and even unconscious effects. Crucially, these involuntary or unconscious effects would require the current GNW configuration to occur. We propose to name this possible new class of representations or processes as ‘GNW-murmur’ given the a murmur is defined as a ‘low background noise’ in the Oxford’s English Dictionary (2023). See Explanatory box #2 for a detailed illustration of GNW-Murmur phenomenon in cognitive dissonance resolution.
Explanatory box #2: Cognitive dissonance resolution as an illustration of GNW-Murmur
The ‘free choice paradigm’ constitutes one of the most explored paradigms of cognitive dissonance research (Brehm Citation1956). Typically, once asked to choose between two similarly rated items, subjects subsequently exhibit an increased preference for chosen items and a decreased preference for rejected ones. In other terms, and as initially postulated by Festinger (Festinger Citation1957), not only do we adapt our choices to our values, but it is also the case that under certain circumstances we can adapt our updated values to our previous choices. Crucially, recent and independent studies have demonstrated that such choice-induced preference change (CIPC) occur exclusively for consciously remembered choices, suggesting a mechanism that ensures subjective coherence across time (Salti et al. Citation2014; Chammat et al. Citation2017; Hagege et al. Citation2018; Voigt et al. Citation2019; Tandetnik et al. Citation2021). Interestingly, individuals never report a conscious feeling of agentivity of this CIPC who still requires them to be conscious of their previous choices. A possible explanation would be that while the subject is re-rating his preferences, task-induced GNW configuration coordinates together the value system (OFC), with the executive system (DLPFC and ACC) as well as with conceptual and perceptual networks. Then, during this GNW-coordinated process the item under consideration could sometimes trigger the recall in conscious episodic memory of a past choice concerning it (item chosen or rejected). As a consequence, once consciously accessed this new information would be broadcasted to executive networks that, in turn, would exert an updating of item preference within the value system, according to the overarching goal of ensuring a subjective coherence. In the end, the conscious posture would have enabled the coordination of these processors within GNW architecture, and would have involuntarily triggered CIPC. Interestingly, when participants are debriefed after experiments, they are usually very surprised of the very existence of this effect they were not aware of, and that they did not experience. In this context, we anticipated that this GNW-Murmur mechanism could be impaired in conscious participants with brain lesions within the prefrontal cortex affecting executive functions. More specifically we predicted that such patients should not show CIPC even for remembered items, and could confirm this prediction (Tandetnik et al. Citation2021). In another study conducted in healthy participants, we enriched the scope of GNW-Murmur in this free choice paradigm, by incidental priming of self-coherence (or self-incoherence) by exposing participants to suggestive quotes displayed as screen savers in a simulated pause within the experiment (Hagege et al. Citation2018). Not only did we replicate the main effect of memory of previous choices on CIPC, but we discovered that these suggestive quotes modulated CIPC: while CIPC was present in the condition promoting the importance of self-coherence, it vanished totally in the condition promoting self-incoherence. This suggestive effect relied on conscious recall of quotes. And again, - as for the main CIPC effect -, participants did not report any form of voluntary agentivity in this new effect.
Such a GNW-Murmur interpretation of choice-induced preference change provides a compelling physiological evidence of a FND-like phenomenon: an involuntary and unconscious cognitive process induced by a conscious posture (i.e.,: here, performing consciously the free-choice paradigm) and requiring conscious access to some information (i.e.,: here, the past ‘chosen/rejected’ fate of given items). GNW-Murmur sheds light and may solve the agentivity issue of FND mentioned in the Introduction of this article.
Of special interest for the present article, conscious influences on unconscious cognition associated to GNW-Murmur correspond to involuntary GNW influences exerted within GNW, whereas most effects reported in Section “Existence of conscious influences on some unconscious processes” (see above) correspond to unconscious GNW influences on peripheral ‘modular’ networks.
Future works could confirm the existence of our predicted GNW-Murmur phenomenon. A non-exhaustive list could include in particular the apparent lack of agentivity in GNW-mediated processes such as the trial-to-trial adaptation of the executive system to task difficulty (such as the Gratton effect, see ), and cross-modal audio-visual priming effects (see ).
Note that this new class of involuntary and unconscious processes operating from within GNW could also induce structural differences driven by mechanisms of neural plasticity related to the active maintenance of intra-GNW connectivity patterns across processors. Applied to FND in which a given conscious posture would be maintained over time for long durations, this argument introduces the hypothesis that chronic FND could lead to reinforcement and automatisation of such GNW-Murmur processes.
A 5-stages model of FND
It is now possible to re-examine our proposed main hypothesis in the light of concepts and findings developed in Sections “Existence of conscious influences on some unconscious processes” and “GNWT account of conscious influences on unconscious processes” (see ).
Main Hypothesis: A FND could correspond to a consciously initiated voluntary top-down process , causing involuntary and non-conscious lasting consequences (i.e.: FND symptoms), that are consciously experienced and subjectively interpreted by the patient as being involuntary .
Within the GNW theoretical framework, this hypothesis can be implemented in the following way. All predictions listed below are synthesised in with: i) prediction statement, ii) available evidence in favour of this prediction, iii) proposed experiments or studies to test it.
Table 2. List of 12 predictions about FND.
Stage 1: A sudden and all-or-none conscious access triggered by an emotional event
An initial and causal event would trigger a new conscious access. A rich literature suggests that this initial event would convey a strong and unusual emotional valence. In the light of the terminology proposed by Damasio between an unconscious emotion and a conscious feeling conceived as conscious access and appraisal of this emotion (Damasio Citation1999), this initial emotional event would therefore induce a conscious access to a corresponding self-referenced feeling. Note that this conscious feeling is not only determined by the initial causal event, but also by past and current states of GNW including its narrative and interpretative processes. In other terms, our framework predicts that the same initial event is not expected to trigger a FND in each and every patient, or even within the same patient on different occasions. It is noteworthy that several recent and independent studies demonstrated that unconscious emotional representations with a negative valence (e.g.: pain, fear, …) are more prone to be consciously accessed than neutral ones (Anderson and Phelps Citation2001; Gaillard et al. Citation2006).
Prediction 1: A FND would be initially caused by a sudden event (i.e.,: close to a seizure or stroke like kinetics), and not by an insidious or progressive process (i.e.,: such as a neurodegenerative process). See .
Prediction 2: A conscious feeling associated with the subjective experience of this causal event would be possible to probe. Note however in practice the risks inherent with a posteriori induction of false memories (deliberately or not), when looking actively for such a memory in a participant or in a patient (Loftus Citation1996; Loftus, Coan et al. Citation1996; Loftus Citation1997).
Stage 2: Post-perceptual processing induces a new GNW-state and its corresponding conscious content
Then this new conscious content would be followed by a transition towards a new GNW state corresponding to a new conscious posture. In this framework, this new conscious posture would be associated with a specific reportable content. In the case of FND, such new conscious postures could correspond to subjective claims close to: “I am afraid of X”, “I don’t want to recall Y”, “I don’t want to see Z”, “I can’t flee”, “I can’t move” etc.
Prediction 3: By definition, this GNW transition and next events require a working GNW. In other terms a FND could not be triggered while the individual is in a non-conscious state such as comatose, or Vegetative State (VS) that is also coined Unresponsive Wakefulness Syndrome (UWS). Later stages of the proposed FND mechanistic scenario share this requirement (see below).
Given the many studies showing how the current conscious posture can influence conscious access to an upcoming stimulus or representation, one may wonder if, prior to experiencing the causal event of Stage 1, some individuals might already be in a conscious posture facilitating Stage 2. In other terms, are there predictive factors of FND-triggering that could be identified prior to Stage 1? If such factors would exist, one may then question the generic versus specific types: would some individuals be in a generic conscious posture facilitating a large variety of symptoms, or alternatively would some individuals show risk factors for specific phenotypes of FND? In terms of GNW, this question relates to the repertoire of GNW states and of their dynamics.
Moreover, if we consider the repertoire of GNW states and of their dynamics, would FND conditions correspond to specific trajectories or manifolds of GNW dynamics (i.e.,: subspace of GNW states and trajectories), with stage-2 states corresponding to nodes of transition across a healthy state and a FND state?
Stage 3: Voluntary and conscious activity triggers involuntary cognitive processes
Stage 3 is the key prediction of our hypothesis: once being in a conscious state associated with a self-reportable feeling, will or intention (see above in Stage 2), this precise state would then cause involuntary consequences, according both to the findings reported in Section “Existence of conscious influences on some unconscious processes”, and to the GNW-Murmur mechanism developed in Section “GNWT account of conscious influences on unconscious processes”.
Prediction 4: Given the executive dimension of Stage-3 leads to the prediction that some core GNW processors implied in executive function such as ACC (see ), DLPFC or other areas of PFC should often (if not always) be implied here. Thus, our hypothesis predicts that FND should be associated with changes in executive network activity and connectivity. A close prediction was stated in another model (Ludwig Citation1972), but without linking FND to consciousness.
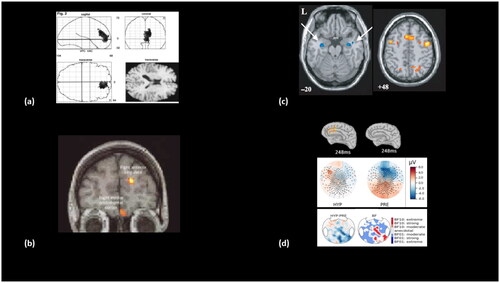
Figure 2. Role of ACC in voluntary and conscious triggering of involuntary cognitive processes in FND, in hypnotic induction and in active forgetting.
Legend: According to our 5-stage model of FND, stage-3 would consist in GNW top-down control over specific cortical networks, and it is predicted to be a stage common to other conditions such as hypnotic induction and active voluntary forgetting. Several results support this prediction such as: (a) ACC activation during FND ‘palsy’ targets motor regions (Marshall et al. Cognition 1997); (b) ACC activation during Hypnotic ‘palsy’ targets motor regions (Halligan et al. Lancet 2000); (c) ACC activation during active forgetting targets hippocampi (Anderson et al. Science 2004) as an increase of activity in GNW areas including ACC associated to an inhibition of hippocampi areas; (d) ACC activation during Hypnotic ‘deafness’ targets conscious access to auditory cortices (Munoz-Musat et al. Front. in Neurol. 2022). Source estimation of high-density EEG revealed an ACC activation around 248ms post sound onset during the induced deafness condition (top left item), that was absent in the non-hypnotic condition (PRE condition, top right item). A proposed signature of conscious access (P3b ERP component) fully disappeared during induced deafness (middle figures), and right posterior sensors showed a strong decrease of functionally connectivity with other cortical areas during hypnotic deafness (bottom items; see Prediction 10 in the main text).
Interestingly, some empirical and clinical results support this prediction by confirming correlations between FND and PFC activity. In 1995, Tiihonen et al. explored with SPECT imaging a 32 years old patient with left-sided FND paralysis and paresthaesia (Tiihonen et al. Citation1995), and discovered a simultaneous activation of frontal inhibitory areas (including ACC) and inhibition of right somatosensory cortices. Similarly, in a seminal PET study Marshall et al. (Marshall et al. Citation1997) reported the case of a patient with unilateral left FND motor loss without sensory loss. When instructed (unsuccessfully) to move her left paralysed leg, two results were observed: (i) the right motor cortex did not show the expected activation present in healthy volunteers (and in the left motor cortex of the patient when instructed to move her right leg); and (ii) right ACC and OFC showed an activation that was absent for in healthy volunteers and when the patient moved her right leg. Subsequent studies almost systematically reported the hypoactivation of contralateral sensorimotor cortices and subcortical networks (Vuilleumier et al. Citation2001) and for reviews see (Harvey et al. Citation2006; Aybek and Vuilleumier Citation2016). Importantly, in the Vuilleumier et al. study this hypoactivation pattern was present during resting state and reversed after recovery (Vuilleumier et al. Citation2001).
Concerning our predicted PFC hyperactivation, it was also reported in many of these subsequent studies, either within ACC (Mailis-Gagnon et al. Citation2003; de Lange, Roelofs et al. 2007), or within ventro-medial PFC (for a review see (Aybek and Vuilleumier Citation2016)). As noted by Aybek and Vuilleumier: ‘vmPFC operates at the interface of processes regulating emotion appraisal and memory retrieval, mediate the access to self-reflective representations, and provide important modulatory signals to both cortical and subcortical sensorimotor circuits, which could thus modulate behaviour based on personally relevant affective information’.
Crucially, reviews across FND phenotypes support our prediction of a common executive network effector pathway originating from PFC, such as ACC or vmPFC.
Prediction 5: Interfering on executive attention or executive functions should modify FND symptoms. Interestingly, and as mentioned in the Introduction section many clinical tests actually lean on this property (e.g.: Hoover test and similar tests, for a recent review see (Garcin Citation2018)).
Prediction 6: Patients with massive lesions of prefrontal cortex should be less prone to FND. Interestingly, we recently provided an empirical support to this prediction in the free choice paradigm described above to illustrate GNW-Murmur. Participants do show a CIPC for remembered items, but we speculated that some individuals should not show such a cognitive dissonance resolution effect even for remembered items: namely patients with frontal lobe lesions impairing their executive functions abilities. We confirmed this hypothesis by testing such patients and by showing that conscious episodic memory of past choices is mandatory but not sufficient for CIPC to occur (Tandetnik et al. Citation2021). Anecdotally, one of us (LN) followed a patient with fronto-temporal dementia from an early stage of disease. At diagnostic onset, while the patient showed minor cognitive deficits and behavioural disturbances he presented a uro-genital complaint the detailed exploration of which concluded to a FND symptom. A few years later, when his executive functions declined, this FND totally disappeared and never recurred (as well as any other type of FND phenotype) over the course of evolution until his death.
Note that Stage-3 could be implemented both through GNW-to-peripheral modules mechanism (see Section “Existence of conscious influences on some unconscious processes”), or through within-GNW coordination (i.e.: GNW-Murmur) that would eventually cause activity changes within specific peripheral modules. It is an open question to examine the respective contribution of these two mechanisms that are not mutually exclusive, for each FND phenotype.
Stage 4: Conscious access to involuntary symptoms
As a direct consequence of Stage-2 conscious posture and of Stage-3 processing, overt FND symptoms appear and are accessible to patient’s awareness.
Crucially, there is no identity between Stage-2 conscious content on the one hand, and Stage-4 overt cognitive or behavioural symptoms on the other hand. This mismatch or at least this absence of identity prevents the patient’s subjective agentivity of symptoms. This is distinctive from malingering or simulating.
We note that we illustrated and addressed only a limited number of FND symptoms in this article, mostly negative/positive motor or sensory signs, and functional amnesia (See Explanatory box #3 for an experimental illustration of our model during intentional forgetting). But our proposed model of FND aims at addressing all possible FND symptoms including for instance dissociative symptoms. In this view, all FND symptoms would rely on this mechanism involving top-down influences: these influences may lead to a large variety of positive or negative symptoms, and obviously the dynamics of top-down control efficacy would explain the fluctuations and variability of symptoms at various time scales (e.g.: transient disappearance of a FND symptom through distraction of endogenous attention). Future works should provide a systematic review of the validity of our hypothesis for each of all major FND signs.
We also note here that Psychogenic Non-Epileptic Seizures (PNES), - that belong to FND (Brown and Reuber Citation2016) -, are of particular importance in the light of our proposed model. First, the short time-scale dynamics of transient and acute FND episodes offer a unique perspective to test key mechanistic hypothesis of FND genesis and resolution, across the various available theoretical models (Brown and Reuber Citation2016). Second, the co-occurrence in the epileptic patients of genuine epileptic seizures and of PNES (Auxemery, Hubsch et al. Citation2011) invite to explore this clinical population to better explore the complex links between conscious/unconscious and voluntary/involuntary processes that may participate to FND (see Introduction).
Stage 5: Sustained maintenance of FND symptoms
As long as patient’s GNW configuration remains in dynamics restricted to a specific space (i.e.,: FND manifold), the conscious executive posture defined in Stage-3 remains active and entertains current FND symptoms.
Prediction 7: FND symptoms require an active GNW so to entertain Stage-3 processes. So, these symptoms should vanish when GNW is not in a conscious functional state, such for instance as during stable periods of deep sleep (N3 stage). Interestingly, some studies report such a dissociation. For instance Volhardt et al. discovered in a patient with FND ‘paraplegia’ a disappearance of motor symptoms during sleep, as revealed by sleep recordings (Vollhardt, Arnulf et al. 2022). In the same perspective frontal lobe impairment is predicted to impair or suppress FND symptomatology (see also above prediction 6).
Explanatory box #3: An experimental illustration of our model: the case of intentional forgetting
As mentioned in the Introduction, our general model of FND aims at addressing various FND phenotypes, including cognitive symptoms among which psychogenic amnesia (that affects episodic memory) is one of the most frequent (Kopelman Citation1987; Harrison et al. Citation2017). Here, a recent and very elegant experimental paradigm introduced by Anderson and his colleagues revealed some key mechanisms of conscious voluntary forgetting (Anderson and Green Citation2001). They adapted the ‘Think-No Think’ paradigm to voluntarily suppress unwanted memories in healthy volunteers. To do so, participants first learned word pairs, and then performed a ‘think/no-think’ task (i.e.,: instruction not to think to the associated word for some pairs, and instruction to think to the associated word for some other pairs). Finally, participants were tested again on all pairs with the instruction to try to find the word associated with each cue word. Active forgetting did impair memory, as cued recall for ‘No Think’ items was inferior to recall of several ingenious control conditions. A replication of this effect while scanning brain activity with fMRI during the ‘Think-No Think’ stage revealed that controlling unwanted memories was associated with increased ACC, DLPFC and VLPFC prefrontal activations, and reduced hippocampal activation. Both PFC and hippocampal activations predicted the magnitude of forgetting (Anderson et al. Citation2004). In a way, this elegant experiment recaps the 5 predicted stages of our proposed general FND mechanism, in a psychogenic amnesia version of FND. ‘No think’ instruction would combine Stage-1 and Stage-2. Of course, and close to the hypnotic suggestion condition (see below), here these two first stages are explicitly instructed and accepted voluntarily by the participant. However this difference is not major, because we postulate that in FND, stage-2 indeed also corresponds to adopting a conscious posture, but that is not instructed by the environment but triggered internally. Then, the voluntary conscious setting of forgetting would be triggered (Stage-3), with the predicted neural mechanisms: GNW activations including an increase of executive areas and notably of ACC and DLPFC that would inhibit a key hub of the episodic memory network (i.e.,: hippocampi). And crucially, the participants then realise that they cannot recall the ‘No Think’ as well as the ‘Think’, even if they voluntarily engage with a sincere motivation. This would correspond to Stage-4 and even Stage-5. Note also that contrary to the initial claim by Anderson and his colleagues who presented their results as the empirical demonstration of Freudian repression, this mechanism of voluntary conscious forgetting is not to be confounded with Freudian repression that was postulated to occur completely unconsciously (Kihlstrom 2002; Naccache 2006). Aware of this important difference, Anderson and colleagues later recognised that: ‘we use the term repression but limit our discussion to its conscious variety’ (Anderson et al. 2004). We showed that once 'Think' and 'No Thin' cues were consciously learned, and then presented subliminallt (preventing conscious access) the active forgetting/remembering effects were still observed. Applied to FND, this last result suggests that once a cognitive posture (i.e.: forgetting versus remembering or many other postures) have been consciously set in response to a given stimulus or situation, it could be reactivated unconsciously. This would enrich the scope of Stage-3 of our FND model (Salvador et al. 2018).
FND as GNW-mediated ‘laundering’ processes transforming conscious voluntary thoughts into involuntary symptoms
This proposed mechanism of FND can be metaphorically compared to ‘money laundering’ processes in which the trace of origin of money are illegally concealed. By analogy, the initial conscious and voluntary process (stage-2) would be transformed involuntarily into a FND symptom (stage-3). In the end, the patient would then consciously access the symptom, while sincerely losing its conscious and voluntary origin. Obviously, the illegality of ‘money laundering’ is the limit of this metaphor since medical symptoms are not fraudulent and FND patients are not morally responsible for their disease. This proposed mechanism solves the agentivity-issue by which we opened this article, because this diachronic process of FND symptoms genesis is both voluntary and involuntary. One of us (LN) formulated the first version of this FND framework while criticising and reinterpreting Freudian concept of unconscious repression, using the French expression ‘Blanchiment sous les topiques’ (laundering under (Freudian) topics) (Naccache Citation2006).
Two possible types of FND resolution
According to our model, resolution of FND would require two processes that may occur within a common therapeutic intervention or separately.
Indeed, therapeutic actions could target either stage-2 or stage-3 related processes.
Durable disappearance of FND symptoms would require an updating of conscious posture generated in stage-2, and induced by the conscious access to the initial triggering event (stage-1). Such a therapeutic update should suppress the initial specific contents (such as: “I am afraid of X”, “I don’t want to recall Y”, “I don’t want to see Z”, “I can’t flee”, “I can’t move” see above). As a direct consequence, stage-3 induced FND symptoms would then disappear.
However, possible intervention focusing exclusively on stage-3 related processes could also lead to the suppression of FND symptoms, while leaving stage-2 conscious posture unchanged. In a way, the transient disappearance of FND symptoms by distracting executive functions, or during sleep or other states correspond to such transient impairment of stage-3 processes. In contrast with such transient effects that only have a diagnostic value, genuine therapeutic specific behavioural interventions are characterised here by their durability and their efficacy even when the patient is not distracted. In a nutshell, the specific ‘ACC-to-module’ configuration can be targeted while GNW-stage 2 thought remains intact. Such a class of stage-3 interventions could explain the classical recurrence of FND under distinct phenotypic forms.
A more durable and deeper therapeutic effect would correspond here to interventions targeting stage-2 processes. If successful, these actions should suppress both the stemming conscious posture as well as the current FND symptoms, and should be associated with a more durable and more general cure of FND in this patient.
Prediction 8: Transient FND resolutions with a moving phenotype should be associated with a transient modification of the PFC/ACC-related process while the active conscious posture that induced it should be unaffected, as well as its GNW configuration signature.
Prediction 9: Improvements from FND symptoms should have fast dynamics related to the all-or-none dynamics of conscious access and to its discrete serial structure. However, delays between FND onset or offset and the underlying triggering factors could be variable and long, according to memory effects. In particular one may expect that inducing a change of conscious posture (stage 2) could, on average, require more conscious effort and time than curing a specific FND symptom (stage 3). Note also that according to the possibility of inducing intra-GNW structural modifications through plasticity in chronic FND, such fast dynamics might also include more linear and progressive components.
Our proposal leads to the clinical question of whether it is possible, or not, to identify a common conscious posture (stage-2) associated with successive distinct FND phenotypes (stage-3) in a given patient?
Moreover, one could classify all proposed FND therapeutic interventions according to their respective impact(s) on stage-2, stage-3 and on the prevention of possible recurrences. Would for instance CBT or suggestive TMS sessions (Garcin et al. Citation2017) show a fast efficacy on FND symptoms by ‘unlocking’ stage-3 process, while more effortful psychoanalytic inspired psychotherapies being more efficient on Stage-2?
Suggestibility as a link between hypnosis and FND: The Charcot-Bernheim debate revisited
At this stage, one may note that our 5-stages model of FND leaves one key question unaddressed: which factors may explain why some individuals will present a FND, whereas a larger proportion of individuals won’t? And why a given individual will be prone to a FND in a specific period of his/her life, whereas he/she would not enter into a FND in other periods? Since the first reports of FND as ‘conversive disorders’, this question has been related to one main factor: suggestibility. Therefore our question could be reformulated as: how would suggestibility translate in our proposed scenario across the five stages? In order to address this last question, we will explore the links between FND and hypnosis that can also be considered as a condition in which suggestibility is supposed to play a decisive role.
Actually, links between FND and hypnosis have been debated since at least the seminal works of Charcot at the end of the nineteenth century. Charcot and the Salpêtrière school considered hypnotic suggestibility and hypnotic states as pathological conditions reproducing hysterical conversive disorders and other dissociative syndromes (Charcot and Richer Citation1883; Janet Citation1907). Babinski focused even more than Charcot on the importance of suggestion and persuasion (including self-persuasion) in the genesis of hysterical symptoms through his concept of ‘pithiatism’ (i.e.: that can be cured “iatos” (curable) by “peithé” (persuasion)) (Babinski and Froment Citation1917; Haan et al. Citation2012), thus bringing hysteria and hypnosis even closer. On the contrary, Bernheim and the Nancy school considered hypnosis as a natural, physiological state of increased suggestibility unrelated to conversive disorders (Bernheim Citation1891). This debate, opposing the view of hypnotisability as an universal phenomenon, versus a specific feature of pathological conditions, is still vivid and open to multiple interpretations. In addition to this link through suggestibility, both hypnosis and FND can be described as ‘a consciously initiated voluntary top-down process causing lasting involuntary consequences’. Actually, several authors have converged to consider hypnosis as a proxy for exploring FND. Accordingly, such a proxy paves the way to an experimental investigation of FND in the laboratory through the use of hypnotic induction paradigms (Bell et al. Citation2011; Vanhaudenhuyse et al. Citation2014).
Moreover, extensive clinical evidence shows that among individuals with FND, direct verbal suggestibility and hypnotic suggestibility are increased and efficient from a therapeutic perspective. For instance, FND symptoms are usually sensitive to suggestions to induce psychogenic non-epileptic seizures (Popkirov et al. Citation2015). In addition, FND are responsive to hypnosis (Deeley Citation2016) and to other suggestion-based treatments (Garcin et al. Citation2017). This links is also supported by a recent meta-analysis (Wieder et al. Citation2021) including 316 patients with FND and 360 healthy controls. Hypnotic suggestibility was greater in FND patients than in controls on standardised behavioural scales (Cohen’s d = 0.48 [95% CI, 0.15, 0.81], p-value = 0.004). It is noteworthy that even more conclusive evidence of enhanced hypnotic suggestibility has been reported in other dissociative disorders (d = 1.25 [0.97, 1.52], Z = 8.79, p < .001)(Wieder et al. Citation2022). Note that this effect size exceeds the association found between dissociative disorders and traumatic experiences such as childhood abuse or neglect (d = 0.53) (Vonderlin et al. Citation2018). All of the above results suggest that high suggestibility, while being by itself a non-pathological neuro-cognitive profile, constitutes a risk factor for FND and other related disorders (Butler et al. Citation1996).
Hypnosis as a ‘consciously initiated voluntary top-down process causing lasting involuntary consequences’
According to the proposed general framing of FND as ‘a consciously initiated voluntary top-down process causing involuntary lasting consequences’, one could explore other mental phenomena that come close to it. Among these, hypnosis deserves special attention. From a historical perspective, the links between hypnosis and hysteria have been questioned at least since the era of Charcot, until today. Many hypnotic procedures can be described as attempts to consciously trigger a specific predetermined symptom (e.g.: induction of either negative symptoms such as deafness, blindness, palsy, amnesia, or positive symptoms such as hallucinations). From the perspective of our model, hypnotic suggestions would therefore differ subtly from FND: here, the participant would consciously and voluntarily aim at eliciting a specific stage-3 phenotype, while not being instructed about the specific subjective conscious posture (stage-2 process) required for him or her to achieve this goal. In many situations, participants seem to explore by trial-and-error a rich subjective repertoire until discovering a conscious posture inducing the desired symptom. For instance, in a previous work using a paradigm of hypnotic suggestion of deafness (Munoz-Musat et al. Citation2022) (see also below), we observed such a canonical subjective report in a participant (unpublished data): during the post-experiment debriefing, the participant told us that she tried initially to reach deafness but failed, until (>20 min of the suggestion procedure) a recent memory popped out into her conscious mind: A few months earlier she took her child to kindergarten, and discovered a group of angry parents at the school entrance. She rapidly understood the reason for their anger: a worker in blue overalls was cleaning a French glass window while turning their back to them, and he did not reply to any of their repeated ‘Hello’. She remembered that she immediately understood this worker was most probably deaf. Noteworthy and incidentally she she was actually consulting as a physician specialised in deaf patients and was therefore familiar to problems encountered by deaf individuals in everyday life. It turned out she was right, and once all parents were aware of this cause, their anger vanished. As soon as she consciously accessed this memory, she suddenly ‘jumped’ into the blue overalls of the worker, cleaning the French window, and became deaf during the whole hypnosis session. In our wording, she discovered by trial-and-error a conscious posture (stage-2 process) enabling the stage-3 consequences to cause the desired stage-3 phenotype. Interestingly, this trial-and-error suggestion stage is motivated by a conscious goal but seems to be also fed by involuntary processes such as here the episodic memory recall that she did not describe as being voluntary.
Prediction 10: The final executive stage-3 process common both to hypnotic phenomena and to FND should be similar in these two situations, and should include an executive network component (e.g.: ACC, see ), and either another GNW structure (i.e.,: in the GNW-Murmur version), or the relevant peripheral processor (i.e.,: auditory network for deafness or motor network for palsy, etc.).
Crucially, a substantial set of functional brain imaging studies of hypnotic phenomena support our prediction.
As a detailed example, and as mentioned above, we recently studied the neurophysiological correlates of complete hypnotic deafness in a highly suggestible individual (see below 6.2. Hypnotic suggestibility), using EEG during an auditory odd-ball paradigm. We could show that: (i) early evoked responses to sounds and to auditory novelty (P1 component, Mismatch Negativity (MMN)) were preserved during hypnotic deafness; (ii) late evoked responses to auditory novelty, such as the P3b component, a previously described signature of conscious access (Sergent et al. Citation2005), were absent during hypnotic deafness; (iii) a transient evoked positivity over frontal electrodes was present exclusively during the hypnotic deafness condition, in the time-window between early (P1, MMN) and late (P3b) evoked responses, with source localisation analysis in favour of a transient dACC activation; (iv) functional connectivity changed during hypnotic deafness, with an increase in the delta band over centro-anterior electrodes and a decrease in the alpha band over latero-posterior electrodes. An interpretation of these results in the light of our proposed hypothesis for FND/hypnotic phenomena would be the following:
Stages 1 and 2: Following hypnotic induction and deafness suggestion (stage 1), our participant found by trial and error an enabling conscious posture (stage 2, see above) associated with specific GNW dynamics.
Stage 3: This particular GNW configuration involved dACC activation, with inhibitory control over auditory associative areas. This inhibitory control (that could be mediated by information sharing in the delta frequency band) resulted in a functional disconnection between auditory areas and the GNW (as revealed by the decrease in functional connectivity in the alpha frequency, in the range of frequencies usually involved in conscious access (see for instance (Gaillard et al. Citation2009; El Karoui et al. Citation2015)). Global availability to auditory information was thus inhibited, resulting in the loss of the P3b component and associated late-stage fronto-parietal activation.
Stage 4: At the subjective level, all of the above described neural changes resulted in the subjective experience of deafness, without any sense of agency from the subject.
Stage 5: As long as the hypnotic suggestion is not lifted, GNW dynamics will remain in a restricted repertoire of states, sustaining the conscious experience of deafness.
Cumulative evidence from several other studies supports this proposed mechanistic account of hypnotic phenomena, with: i) a general and central implication of frontal executive processors, ii) involvement of other GNW core-hubs (such as parietal associative areas), and iii) involvement of a domain/suggestion specific role of specialised modular processors (for recent reviews see (Landry and Raz Citation2015) and (Jensen et al. Citation2017)). Hypnotic analgesia has been demonstrated to be ACC-mediated (Faymonville et al. Citation2000; Citation2003; Trujillo-Rodriguez et al. Citation2019; Del Casale et al. Citation2022), as well as involving a modulation of activity in somatosensory areas (Derbyshire et al. Citation2009). A large range of positive or negative hypnotic hallucinations are linked to domain-specific activation patterns (i.e., involvement of visual areas for visual hallucinations, of somatosensory areas for pain hallucinations/hyperalgesia, of ventromedial prefrontal cortex for valence suggestions), under the coordination of prefrontal, ACC and associative parietal areas (McGeown et al. Citation2012; Derbyshire et al. Citation2004; Ludwig et al. Citation2014). Additionally, left-arm (hypnotic) ideomotor paralysis is associated with abnormal activations of right prefrontal, right ACC and precuneus regions, with a deactivation of right motor cortex (right M1) and changes in functional connectivity between right M1 and right premotor (decrease) and precuneus (increase) (Cojan et al. Citation2009), compatible with a GNW-mediated inhibitory process over motor areas. Finally, EEG studies investigating hypnotic perceptual losses such as deafness (Franz et al. Citation2020) or blindness (Schmidt et al. Citation2017) reported a specific loss of the P3b component during the hypnotic condition, just like in our case-study. It is important to clarify that all of this evidence, while perfectly compatible with our GNW-inspired mechanistic proposition, could also accept different interpretations. Nevertheless, our proposal comes with a set of novel and specific predictions that could be tested (see below).
Hypnotic suggestibility: Definition and sources of variability
Before further exploring the links between FND and hypnosis, the notion of hypnotic suggestibility needs to be specified. Hypnotic suggestibility can be reliably measured using standardised scales (Woody and Barnier Citation2008) such as the form C of the Stanford Hypnotic Suggestibility Scale (SHSS-C) (Hilgard Citation1978). Based on these scales, hypnotic suggestibility conforms to a normal distribution (Woody and Barnier Citation2008): about 10–15% of individuals show low hypnotic suggestibility (“Lows”), often responding to few or no suggestions; 60–80% of the population exhibits moderate responsiveness to hypnotic cues (“Mediums”); while the remaining 10–15% display high hypnotic suggestibility (“Highs”), often responding to most suggestions, including challenging cognitivo-perceptual phenomena. Hypnotic suggestibility is a trait-like characteristic (stable over time, (Piccione et al. Citation1989)), and research using the twin study methodology suggests that it is heritable (Morgan et al. Citation1970; Morgan Citation1973), although only preliminary research has been conducted on its genetic basis. Hypnotic suggestibility further predicts responsiveness to non-hypnotic verbal suggestions and placebo/nocebo manipulations (Nitzan et al. Citation2015).
While cumulative evidence points towards a pivotal role of regions of the prefrontal and ACC cortices, the exact relationship between the anatomo-functional characteristics of these regions and individual differences in hypnotic responding needs to be further clarified. Structural MRI research suggests that “Highs” exhibit greater volume in the rostrum of the corpus callosum (Horton et al. Citation2004), in medial prefrontal cortex and in ACC (McGeown et al. Citation2012; Huber et al. Citation2014), as compared to “Lows”.
Beyond the large inter-individual variability exposed above, one should be aware that similar scores in standardised scales can correspond to very different qualitative patterns (Szechtman et al. Citation1998; Woody et al. Citation2005; Franz et al. Citation2020; Barnier et al. Citation2022). These multiple sources of variability suggested that hypnotic suggestibility could result from the combination of two components: first, a global non-modular (or ‘super-ordinate’ for (Woody et al. Citation2005)) factor generalising susceptibility to hypnotic suggestion to any specific condition, and second a series of modular (or ‘sub-ordinate’ for Woody et al.) suggestion-specific factors (Woody et al. Citation2005; Barnier et al. Citation2022).
Implementing suggestibility in the 5-stages model of FND and hypnosis
In the light of the precedent paragraphs it is extremely tempting to identify: (i) the modular (or subordinate) factors of hypnotic suggestibility with reciprocal connections between peripheral processors and GNW, and (ii) the non-modular (super-ordinate) factor of hypnotic suggestibility with a within-GNW component.
Concerning the modular factor, it would intervene in stage-3 of our model by facilitating top-down influences consecutive to the stage-2 conscious posture (see ). As also mentioned above (see 3.1), the influence of GNW on peripheral processors is predicted to be exerted through neuronal projections of GNW neurons onto these processors. Based on GNW neurons long-distance cortico-cortical connectivity between high-level associative cortices, we postulated that these GNW neurons should predominantly be found in cytoarchitectonic layers II-III (Dehaene et al. Citation1998; Dehaene and Naccache Citation2001). One could therefore estimate the possibility for such GNW-mediated conscious influences on a given cortical area according to the density of layers II-III. Here, GWNT converges with Reverse Hierarchy Theory (Ahissar and Hochstein Citation2004) to claim that top-down conscious influences show a gradient of performance on peripheral areas: from high-level cortical areas (i.e.,: with high density in GNW neurons) in which conscious influences are very efficient, all the way down to low-level cortical areas (i.e.,: with low density in GNW neurons) in which conscious influences are poor or even absent (see the case or primary cortices illustrated for V1 above in 3.2).
In this perspective, variability of GNW neurons density could modulate the ease of top-down conscious influences on peripheral cortical networks, or even enable such influences in cortical areas usually lacking such GNW neurons (e.g.: lack of bidirectional long-distance neurons between PFC and V1 (Felleman and Van Essen Citation1991)). Such a mechanism could result from both neuro-developmental, or acquired origins (e.g.: sustained pattern of cognitive or behavioural habits). This explanatory factor is predicted to be particularly relevant for ultra specific forms of suggestibility (both in hypnosis and in FND). Note also that in a given individual this GNW-to-peripheral processor factor could be very focal (i.e.: 1 processor) but also more diffuse and generalised, in particular when its origin is neuro-developmental.
Prediction 11: Specific efficient hypnotic suggestions and specific FND symptoms should require an increase of GNW neurons density in the corresponding peripheral processors (see ). For instance, patients with FND blindness or FND ‘hemiplegia’ are predicted to show higher GNW-neurons density in ventral visual pathway or in contralateral M1 area respectively.
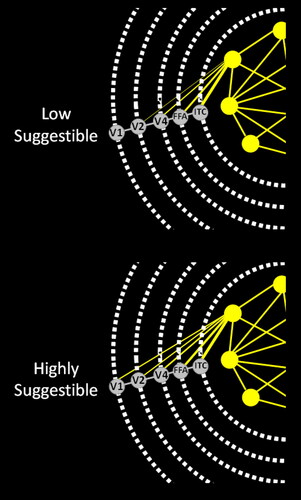
Figure 3. Hypnotic suggestibility and GNW neurons density in specific areas.
Legend: Illustration to visual perception of our prediction relating hypnotic suggestibility to an increase of GNW neurons density (in layers II-III) in corresponding cortical areas (see our Prediction #11 in the main text and in ). Such structural factor would enable increased top-down influence from GNW to targeted areas, with either excitatory (for positive symptoms such as hypnotic induction of visual hallucinations), or inhibitory (for negative symptoms such as hypnotic induction of blindness) effects. Schematic representation of the GNW bidirectional connections (yellow) with core areas of the visual ventral pathway (V1, V2, V4, Face Fusiform Area (FFA), Inferior Temporal Cortex (ITC)) are represented both for low-suggestible (top) and for highly-suggestible individuals (bottom). Bidirectional anatomical connections (GNW neurons) between key GNW areas and between GNW areas and peripheral visual areas are represented in yellow. According to our prediction number 11, responsiveness to visual suggestions (capacity for visual hallucinations) in some highly suggestible individuals should be at least partially mediated by an increased GNW neuron density in the ventral pathway, with more GNW neurons in high level visual areas (ex: FFA), and with the presence of some GNW neurons in regions normally lacking this type of neurons (ex: V1). Note that several GNW areas could be involved, including both high-level visual areas, as well as executive areas such as the dACC involved in top-down regulation. Conscious access and specific contents could be controlled through this top-down regulations. If confirmed this prediction could generalise to other conditions of GNW top-down control on specific networks such as: FND, mental imagery or synaesthesia.
Prediction 12: Conscious access threshold to the highly suggestive modality should be lower than in non-suggestible individuals.
Concerning the general non-modular factor of suggestibility, it would intervene on the transition from stage-1 (conscious access to the initial emotional event) to stage-2 (i.e.,: transition of GNW activity to a new state). This general factor would facilitate such stage-1 to stage-2 transitions, irrespective of the specific stage-3 consequences, and would therefore play a role of generic FND facilitation. One could speculate about the cognitive and affective ingredients of this facilitation: all GNW-processors related to sensitivity to external or to self-instructions, to social cognition, to emotional processing, to motivation and to decision-making could be implied.
Note that these two explanatory factors (i.e.: the general factor on the one hand, and the series of specific factors on the other hand) could be independent and provide a rich repertoire of potential cognitive and behavioural phenotypes of FND and of hypnotic effects.
FND, suggestibility and hypnosis Charcot-Bernheim debate revisited
Our proposal leads to a speculative reinterpretation of the seminal Charcot/Bernheim debate that structured theories of FND and hypnosis since the late nineteenth century. First, and in full agreement with Bernheim, - and therefore against Charcot -, hypnosis would not to be considered as a hallmark of FND and would not be specific to FND patients. However, we proposed here that FND and hypnotic suggestion do share neurophysiological similarities captured within our 5-stages mechanistic scenario.
As described above (see Prediction 10) the final executive stage-3 process is predicted to be common to hypnotic phenomena and to FND. However, at least two distinctions distinguish FND from hypnosis. First and obviously, FND differs from hypnosis according to their usual respective time-scale (i.e.: from a few minutes to tens of minutes for hypnosis typically, versus several days, weeks, months or years for FND). Second, hypnosis also differs from FND because the participant consciously and voluntarily aims at eliciting a specific stage-3 phenotype in hypnosis, - while not being instructed about the specific subjective conscious posture (stage-2 process) required to achieve this goal. In many situations, participants seem to explore by trial-and-error a rich subjective repertoire until discovering a conscious posture inducing the desired symptom.
So in the end, individual level of suggestibility (that is mobilised through hypnosis) would constitute a predisposing or a risk factor of FND, but would not per se be sufficient to elicit a FND. Other factors involved in stage-1 (i.e.: unusual emotional or affective triggering factors) and in stage-2 (i.e.: a specific conscious posture triggered by stage 1, or pre-existing in a given subject as a consequence of certain earlier life experiences such as traumatic events) may be necessary conditions to the outbreak of a FND.
Conclusion
In this article, we proposed a general theoretical framework of FND inspired by GNWT and by our neurological experience. This 5-stages model makes explicit predictions (see ) about the respective contributions of conscious (i.e.: self-reportable) and unconscious cognitive processes, - and of their interactions -, i) at FND onset, ii) during FND maintenance and evolution, and iii) at FND resolution. These predictions translate into a research program that we defined, and that could test their validity in patients and in healthy volunteers using a combination of behavioural, subjective and both structural and functional brain-imaging tools. This research program is relevant to test GNWT through the prism of FND, but also to improve the efficacy of FND care that is so challenging for patients, clinicians and all caregivers.
In addition to its theoretical interest, this work could also have several clinical applications, if validated by future empirical studies testing the listed predictions (see ). These implications concern the diagnostic and therapeutic stages. By providing a mechanistic account of FND symptoms based on the notion of top-down conscious influences on non-conscious processes, one could derive new positive signs to diagnose FND. Such new signs supporting FND diagnosis may correspond to new neuropsychological and behavioural signs implementing those ideas, but they could also correspond to structural or functional brain-imaging signs. For instance, our prediction of increased density of GNW neurons in the neural processors associated to symptoms in some FND patients could be imaged with high-field MRI (Kok et al. Citation2016; Lawrence et al. Citation2019a; Lawrence et al. Citation2019b). Similarly, the engagement of executive networks on specialised neural processors, as illustrated for instance by the inhibition effect of GNW regions on hippocampi in intentional forgetting (see Explanatory box #3) may translate in new fMRI or high-density EEG clinical tests such as used in other areas such as disorders of consciousness (Hermann et al. Citation2021).
Similarly, FND therapeutics may be improved twofold. First, our proposed taxonomy of therapeutic interventions according to their locus of action in the proposed model could help tailoring a therapeutic program for individual patients and combining different approaches within a unified framework. For instance, our distinction between therapeutic interventions targeting preferentially Stage-2 (e.g.: introspective ego-related psychotherapies or those using a psychanalytic framework) or Stage-3 (e.g.: CBT or suggestive use of TMS or hypnosis) illustrates this point. Second, our proposed model may be used to derive psycho-educative tools both for patients and for their caregivers. For patients, providing them with a non-dualistic account of their symptoms may help them at different levels: (i) providing them with a positive recognition and definition of their complaints, (ii) providing them with an explanation of the genesis of their symptoms through the interplay between initially voluntary and then unvoluntary cognitive processes. This class of explanation may be used to derive new types of CBT or psychotherapies specific to FND framework (ii) discarding feelings of culpability, (iii) helping them to engage actively and with motivation in a combined therapeutic program taking advantage of the various available tools including psychotherapies. For caregivers, our model could help them to deal with the ‘uncanny feeling’ generated by this mixture of voluntary and unvoluntary attribute of FND symptoms (see Introduction).
We recap and list herethe 5 predictions that play the most important role in our model:
(i) The sudden all-or-none dynamics of FND onset.
(ii) The requirement to be in a conscious state in order to be affected by a FND, even if several stages of the proposed pathophysiology of FND are not conscious.
(iii) The formulation of a new class of unconscious processes that originate from within GNW, and that we coined as ‘GNW-Murmur’. This new class of unconscious processes can be explored well beyond the field of FND.
(iv) The description of FND as GNW-mediated ‘laundering’ processes transforming conscious voluntary thoughts into involuntary symptoms.
(v) By describing many FND phenotypes as GNW top-down effects on various neural processors, we could state a brain-structure prediction: density of GNW neurons (that enable these top-down effects) in the neural processors associated to symptoms should be more pronounced in some FND patients than in healthy volunteers. This effect is predicted to be particularly marked in low-level cortical networks (e.g.: FND symptoms involving primary or secondary cortices that are usually not easily accessible to top-down control). Once formulated, this last prediction could have a much larger significance, like for instance by explaining some synaesthesia phenomena or mental imagery variability which also corresponds to unusual conscious contents implying GNW activity and anatomy.
Finally, several of our predictions led us to reinterpret the debated proximity and specificities of FND and hypnosis.
To conclude, if any of the proposed ideas, - that we initially developed to explore FND -, would be confirmed through empirical and experimental testing, one may even wonder if such conscious/unconscious chains of cognitive and emotional processes could not contribute to ‘healthy cognition’ in a less intense way. This last proposal would suggest a new kind of ‘psychopathology of everyday life’ could stem from this tentative model of FND (Freud Citation1901).
Acknowledgments
An initial draft of this model was presented online by Lionel Naccache at King’s College Institute of Psychiatry, Psychology & Neuroscience (IoPPN, London) on April 25th 2023 (https://www.kcl.ac.uk/events/global-neuronal-workspace-theory-of-consciousness-and-its-speculative-applications-to-hypnosis-and-functional-neurological-disorders). The authors thank Prof. Florence Thibaut for her invitation to write a Review article inspired by the theoretical model developed in this conference and by its corresponding research program.
Additional information
Funding
References
- 2023. Oxford’s English Dictionnary, Oxford, U.K.: Oxford University Press.
- Ahissar M, Hochstein S. 2004. The reverse hierarchy theory of visual perceptual learning. Trends Cogn Sci. 8(10):457–464. doi:10.1016/j.tics.2004.08.011.
- Anderson AK, Phelps EA. 2001. Lesions of the human amygdala impair enhanced perception of emotionally salient events. Nature. 411(6835):305–309. doi:10.1038/35077083.
- Anderson MC, Green C. 2001. Suppressing unwanted memories by executive control. Nature. 410(6826):366–369. doi:10.1038/35066572.
- Anderson MC, Ochsner KN, Kuhl B, Cooper J, Robertson E, Gabrieli SW, Glover GH, Gabrieli JD. 2004. Neural systems underlying the suppression of unwanted memories. Science. 303(5655):232–235. doi:10.1126/science.1089504.
- Arthuis M, Valton L, Régis J, Chauvel P, Wendling F, Naccache L, Bernard C, Bartolomei F. 2009. Impaired consciousness during temporal lobe seizures is related to increased long-distance cortical-subcortical synchronization. Brain. 132(Pt 8):2091–2101. doi:10.1093/brain/awp086.
- Auxemery Y, Hubsch C, Fidelle G. 2011. Psychogenic non epileptic seizures: a review. Encephale 37(2):153–158.
- Aybek S, Vuilleumier P. 2016. Imaging studies of functional neurologic disorders. Handb Clin Neurol. 139:73–84.
- Baars BJ. 1988. A cognitive theory of consciousness. Cambridge, MA: Cambridge University Press.
- Babinski J, Froment J. 1917. Hystérie-pithiatisme et troubles nerveux d’ordre réflexe en neurologie de guerre, Paris: Masson et Cie.
- Barnier AJ, Terhune DB, Polito V, Woody EZ. 2022. A componential approach to individual differences in hypnotizability. Psychology of Consciousness: theory, Research, and Practice. 9(2):130–140. doi:10.1037/cns0000267.
- Bartolomei F, McGonigal A, Naccache L. 2014. Alteration of consciousness in focal epilepsy: the global workspace alteration theory. Epilepsy Behav. 30:17–23. doi:10.1016/j.yebeh.2013.09.012.
- Bartolomei F, Naccache L. 2011. The global workspace (GW) theory of consciousness and epilepsy. Behav Neurol. 24(1):67–74. doi:10.1155/2011/127864.
- Bell V, Oakley DA, Halligan PW, Deeley Q. 2011. Dissociation in hysteria and hypnosis: evidence from cognitive neuroscience. J Neurol Neurosurg Psychiatry. 82(3):332–339. doi:10.1136/jnnp.2009.199158.
- Bernheim H. 1891. Hypnotisme, suggestion, psychothérapie: études nouvelles. Paris, Doin Editeur.
- Block N. 1995. On a confusion about the role of consciousness. Behav Brain Sci. 18(2):227–247. doi:10.1017/S0140525X00038188.
- Block N. 2007. Consciousness, accessibility, and the mesh between psychology and neuroscience. Behav Brain Sci. 30(5-6):481–499. doi:10.1017/S0140525X07002786.
- Brehm J. 1956. Postdecision changes in the desirability of alternatives. J Abnorm Psychol. 52(3):384–389. doi:10.1037/h0041006.
- Brown RJ, Reuber M. 2016. Psychological and psychiatric aspects of psychogenic non-epileptic seizures (PNES): a systematic review. Clin Psychol Rev. 45:157–182. doi:10.1016/j.cpr.2016.01.003.
- Brown RJ, Reuber M. 2016b. Towards an integrative theory of psychogenic non-epileptic seizures (PNES). Clin Psychol Rev. 47:55–70. doi:10.1016/j.cpr.2016.06.003.
- Butler LD, Duran RE, Jasiukaitis P, Koopman C, Spiegel D. 1996. Hypnotizability and traumatic experience: a diathesis-stress model of dissociative symptomatology. Am J Psychiatry. 153(7 Suppl):42–63.
- Carson A, Lehn A. 2016. Epidemiology. Handb Clin Neurol. 139:47–60.
- Chammat M, Karoui IE, Allali S, Hagège J, Lehongre K, Hasboun D, Baulac M, Epelbaum S, Michon A, Dubois B, et al. 2017. Cognitive dissonance resolution depends on episodic memory. Sci Rep. 7(1):41320. doi:10.1038/srep41320.
- Charcot JM. 1875. Leçons sur les maladies du système nerveux faites à la Salpêtrière. Paris: V. Adrien et Cie Editeurs.
- Charcot JM, Richer P. 1883. Note on certain facts of cerebral automatism observed in hysteria during the cataleptic period of hypnotism. Journal of Nervous and Mental Disease. 10(1):1–13. doi:10.1097/00005053-188301000-00001.
- Cock HR, Edwards MJ. 2018. Functional neurological disorders: acute presentations and management. Clin Med. 18(5): 414–417.
- Cohen MA, Dennett DC. 2011. Consciousness cannot be separated from function. Trends Cogn Sci. 15(8):358–364. doi:10.1016/j.tics.2011.06.008.
- Cojan Y, Waber L, Schwartz S, Rossier L, Forster A, Vuilleumier P. 2009. The brain under self-control: modulation of inhibitory and monitoring cortical networks during hypnotic paralysis. Neuron. 62(6):862–875. doi:10.1016/j.neuron.2009.05.021.
- Crick F, Koch C. 1995. Are we aware of neural activity in primary visual cortex? Nature. 375(6527):121–123. doi:10.1038/375121a0.
- Damasio A. 1999. The feeling of what happens. New York: Harcourt Brace & Co.
- de Lange FP, Roelofs K, Toni I. 2007. Increased self-monitoring during imagined movements in conversion paralysis. Neuropsychologia. 45(9):2051–2058. doi:10.1016/j.neuropsychologia.2007.02.002.
- Deeley Q. 2016. Hypnosis as therapy for functional neurologic disorders. Handb Clin Neurol. 139:585–595. doi:10.1016/B978-0-12-801772-2.00047-3.
- Dehaene S, Changeux JP, Naccache L, Sackur J, Sergent C. 2006. Conscious, preconscious, and subliminal processing: a testable taxonomy. Trends Cogn Sci. 10(5):204–211. doi:10.1016/j.tics.2006.03.007.
- Dehaene S, Kerszberg M, Changeux JP. 1998. A neuronal model of a global workspace in effortful cognitive tasks. Proc Natl Acad Sci U S A. 95(24):14529–14534. doi:10.1073/pnas.95.24.14529.
- Dehaene S, Naccache L. 2001. Towards a cognitive neuroscience of consciousness: basic evidence and a workspace framework. Cognition. 79(1-2):1–37. doi:10.1016/s0010-0277(00)00123-2.
- Dehaene S, Naccache L. 2006. Can one suppress subliminal words? Neuron. 52(3):397–399. doi:10.1016/j.neuron.2006.10.018.
- Del Casale A, Ferracuti S, Adriani B, Novelli F, Zoppi T, Bargagna P, Pompili M. 2022. Neural functional correlates of hypnosis and hypnoanalgesia: role of the cingulate cortex. Am J Clin Hypn. 64(1):53–61. doi:10.1080/00029157.2021.1895709.
- Derbyshire SW, Whalley MG, Oakley DA. 2009. Fibromyalgia pain and its modulation by hypnotic and non-hypnotic suggestion: an fMRI analysis. Eur J Pain. 13(5):542–550. doi:10.1016/j.ejpain.2008.06.010.
- Derbyshire SW, Whalley MG, Stenger VA, Oakley DA. 2004. Cerebral activation during hypnotically induced and imagined pain. Neuroimage. 23(1):392–401. doi:10.1016/j.neuroimage.2004.04.033.
- Driver J, Mattingley JB. 1998. Parietal neglect and visual awareness. Nat Neurosci. 1(1):17–22. doi:10.1038/217.
- Driver J, Vuilleumier P. 2001. Perceptual awareness and its loss in unilateral neglect and extinction. Cognition. 79(1-2):39–88. doi:10.1016/s0010-0277(00)00124-4.
- El Karoui I, King JR, Sitt J, Meyniel F, Van Gaal S, Hasboun D, Adam C, Navarro V, Baulac M, Dehaene S, et al. 2015. Event-related potential, time-frequency, and functional connectivity facets of local and global auditory novelty processing: an intracranial study in humans. Cereb Cortex. 25(11):4203–4212. doi:10.1093/cercor/bhu143.
- El Youssef N, Jegou A, Makhalova J, Naccache L, Bénar C, Bartolomei F. 2022. Consciousness alteration in focal epilepsy is related to loss of signal complexity and information processing. Sci Rep. 12(1):22276. doi:10.1038/s41598-022-25861-4.
- Ellenberger HF. 1965. Charcot and the Salpêtrière School. Am J Psychother. 19(2):253–267. doi:10.1176/appi.psychotherapy.1965.19.2.253.
- Espay AJ, Aybek S, Carson A, Edwards MJ, Goldstein LH, Hallett M, LaFaver K, LaFrance WC, Jr., Lang AE, Nicholson T, et al. 2018. Current concepts in diagnosis and treatment of functional neurological disorders. JAMA Neurol. 75(9):1132–1141. doi:10.1001/jamaneurol.2018.1264.
- Eysenck MW. 1984. Attention and performance limitations. A handbook of cognitive psychology. M. W. Eysenck. Hillsdale, NJ, L. Erlbaum Assoc.: p. 49–77.
- Faymonville ME, Laureys S, Degueldre C, DelFiore G, Luxen A, Franck G, Lamy M, Maquet P. 2000. Neural mechanisms of antinociceptive effects of hypnosis. Anesthesiology. 92(5):1257–1267. doi:10.1097/00000542-200005000-00013.
- Faymonville ME, Roediger L, Del Fiore G, Delgueldre C, Phillips C, Lamy M, Luxen A, Maquet P, Laureys S. 2003. Increased cerebral functional connectivity underlying the antinociceptive effects of hypnosis. Brain Res Cogn Brain Res. 17(2):255–262. doi:10.1016/s0926-6410(03)00113-7.
- Felleman DJ, Van Essen DC. 1991. Distributed hierarchical processing in the primate cerebral cortex. Cereb Cortex. 1(1):1–47. doi:10.1093/cercor/1.1.1.
- Festinger L. 1957. "A theory of cognitive dissonance."
- Fodor JA. 1983. The Modularity of Mind. Cambridge: MIT Press.
- Franz M, Schmidt B, Hecht H, Naumann E, Miltner WHR. 2020. Suggested deafness during hypnosis and simulation of hypnosis compared to a distraction and control condition: a study on subjective experience and cortical brain responses. PLoS One. 15(10):e0240832. doi:10.1371/journal.pone.0240832.
- Freud S. 1901. The Psychopathology of Everyday Life. London: Hogarth Press.
- Gaillard R, Dehaene S, Adam C, Clémenceau S, Hasboun D, Baulac M, Cohen L, Naccache L. 2009. Converging intracranial markers of conscious access. PLoS Biol. 7(3):e61. doi:10.1371/journal.pbio.1000061.
- Gaillard R, Del Cul A, Naccache L, Vinckier F, Cohen L, Dehaene S. 2006. Nonconscious semantic processing of emotional words modulates conscious access. Proc Natl Acad Sci U S A. 103(19):7524–7529. doi:10.1073/pnas.0600584103.
- Garcin B. 2018. Motor functional neurological disorders: an update. Rev Neurol (Paris)). 174(4):203–211. doi:10.1016/j.neurol.2017.11.003.
- Garcin B, Mesrati F, Hubsch C, Mauras T, Iliescu I, Naccache L, Vidailhet M, Roze E, Degos B. 2017. Impact of Transcranial Magnetic Stimulation on Functional Movement Disorders: cortical Modulation or a Behavioral Effect? Front Neurol. 8:338. doi:10.3389/fneur.2017.00338.
- Garcin B, Villain N, Mesrati F, Naccache L, Roze E, Degos B. 2021. A single-center series of 482 patients with functional motor disorders. J Psychosom Res. 148:110565. doi:10.1016/j.jpsychores.2021.110565.
- Gratton G, Coles MG, Donchin E. 1992. Optimizing the use of information: strategic control of activation of responses. J Exp Psychol Gen. 121(4):480–506. doi:10.1037/0096-3445.121.4.480.
- Greenwald AG, Abrams RL, Naccache L, Dehaene S. 2003. Long-term semantic memory versus contextual memory in unconscious number processing. J Exp Psychol Learn Mem Cogn. 29(2):235–247. doi:10.1037/0278-7393.29.2.235.
- Haan J, Koehler PJ, Bogousslavsky J. 2012. Neurology and surrealism: Andre Breton and Joseph Babinski. Brain. 135(Pt 12):3830–3838. doi:10.1093/brain/aws118.
- Hagège J, Chammat M, Tandetnik C, Naccache L. 2018. Suggestion of self-(in)coherence modulates cognitive dissonance. PLoS One. 13(8):e0202204. doi:10.1371/journal.pone.0202204.
- Harrison NA, Johnston K, Corno F, Casey SJ, Friedner K, Humphreys K, Jaldow EJ, Pitkanen M, Kopelman MD. 2017. Psychogenic amnesia: syndromes, outcome, and patterns of retrograde amnesia. Brain. 140(9):2498–2510. doi:10.1093/brain/awx186.
- Harvey SB, Stanton BR, David AS. 2006. Conversion disorder: towards a neurobiological understanding. Neuropsychiatr Dis Treat. 2(1):13–20.
- Hauw F, Sangare A, Munoz Musat E, Meyniel C, Di Donato N, Chokron S, Bozon-Auclair F, Naccache L. 2024. Are we aware of neural activity in primary visual cortex? A neuropsychological case-study response. Ann Clin Transl Neurol. 11(5):1365–1370. doi: 10.1002/acn3.52038.
- Hermann B, Sangaré A, Munoz-Musat E, Salah AB, Perez P, Valente M, Faugeras F, Axelrod V, Demeret S, Marois C, et al. 2021. Importance, limits and caveats of the use of “disorders of consciousness” to theorize consciousness. Neurosci Conscious. 2021 (2):niab048. doi:10.1093/nc/niab048.
- Hilgard ER. 1978. The Stanford Hypnotic Susceptibility Scales as related to other measures of hypnotic responsiveness. Am J Clin Hypn. 21(2-3):68–83. doi:10.1080/00029157.1978.10403965.
- Horton JE, Crawford HJ, Harrington G, Downs JH. 3rd, 2004. Increased anterior corpus callosum size associated positively with hypnotizability and the ability to control pain. Brain. 127(Pt 8):1741–1747. doi:10.1093/brain/awh196.
- Huber A, Lui F, Duzzi D, Pagnoni G, Porro CA. 2014. Structural and functional cerebral correlates of hypnotic suggestibility. PLoS One. 9(3):e93187. doi:10.1371/journal.pone.0093187.
- Jackendoff RS. 1987. "Consciousness and the computational mind."
- Janet P. 1907. The major symptoms of hysteria. London, UK: Macmillian & Co.
- Jensen MP, Jamieson GA, Lutz A, Mazzoni G, McGeown WJ, Santarcangelo EL, Demertzi A, De Pascalis V, Banyai EI, Rominger C, et al. 2017. New directions in hypnosis research: strategies for advancing the cognitive and clinical neuroscience of hypnosis. Neurosci Conscious. 3(1):nix004. doi: 10.1093/nc/nix004. Epub 2017 Apr 12.
- Kentridge RW, Heywood CA, Weiskrantz L. 1999. Attention without awareness in blindsight. Proc Biol Sci. 266(1430):1805–1811. doi:10.1098/rspb.1999.0850.
- Kentridge RW, Nijboer TC, Heywood CA. 2008. Attended but unseen: visual attention is not sufficient for visual awareness. Neuropsychologia. 46(3):864–869. doi:10.1016/j.neuropsychologia.2007.11.036.
- Kihlstrom JF. 2002. No need for repression. Trends Cogn Sci. 6(12):502. doi:10.1016/s1364-6613(02)02006-5.
- Kok P, Bains LJ, van Mourik T, Norris DG, de Lange FP. 2016. Selective activation of the deep layers of the human primary visual cortex by top-down feedback. Curr Biol. 26(3):371–376. doi:10.1016/j.cub.2015.12.038.
- Kopelman MD. 1987. Amnesia: organic and psychogenic. Br J Psychiatry. 150(4):428–442. doi:10.1192/bjp.150.4.428.
- Kouider S, Dehaene S. 2007. Levels of processing during non-conscious perception: a critical review of visual masking. Philos Trans R Soc Lond B Biol Sci. 362(1481):857–875. doi:10.1098/rstb.2007.2093.
- Lamme VA, Roelfsema PR. 2000. The distinct modes of vision offered by feedforward and recurrent processing. Trends Neurosci. 23(11):571–579. doi:10.1016/s0166-2236(00)01657-x.
- Landry M, Raz A. 2015. Hypnosis and imaging of the living human brain. Am J Clin Hypn. 57(3):285–313. doi:10.1080/00029157.2014.978496.
- Lawrence SJ, Norris DG, de Lange FP. 2019a. Dissociable laminar profiles of concurrent bottom-up and top-down modulation in the human visual cortex. Elife. 2019 May 7:8:e44422. doi: 10.7554/eLife.44422
- Lawrence SJD, Formisano E, Muckli L, de Lange FP. 2019b. Laminar fMRI: applications for cognitive neuroscience. Neuroimage. 197:785–791. doi:10.1016/j.neuroimage.2017.07.004.
- Loftus EF. 1996. Memory distortion and false memory creation. Bull Am Acad Psychiatry Law. 24(3):281–295.
- Loftus EF. 1997. Creating false memories. Sci Am. 277(3):70–75. doi:10.1038/scientificamerican0997-70.
- Loftus EF, Coan J, Pickrell JE. 1996. Manufacturing false memories using bits of reality. In: Reder LM, editor. Implicit memory and metacognition. Posner MI, Snyder CRR: Lawrence Erlbaum (Mahwah, NJ USA) 1975.
- Luck SJ, Vogel EK, Shapiro KL. 1996. Word meanings can be accessed but not reported during the attentional blink. Nature. 383(6601):616–618. doi:10.1038/383616a0.
- Ludwig AM. 1972. Hysteria. A neurobiological theory. Arch Gen Psychiatry. 27(6):771–777. doi:10.1001/archpsyc.1972.01750300043007.
- Ludwig VU, Stelzel C, Krutiak H, Magrabi A, Steimke R, Paschke LM, Kathmann N, Walter H. 2014. The suggestible brain: posthypnotic effects on value-based decision-making. Soc Cogn Affect Neurosci. 9(9):1281–1288. doi:10.1093/scan/nst110.
- Mack A, Rock I. 1998. "Inattentional blindness."
- Mailis-Gagnon A, Giannoylis I, Downar J, Kwan CL, Mikulis DJ, Crawley AP, Nicholson K, Davis KD. 2003. Altered central somatosensory processing in chronic pain patients with "hysterical" anesthesia. Neurology. 60(9):1501–1507. doi:10.1212/wnl.60.9.1501.
- Marshall JC, Halligan PW, Fink GR, Wade DT, Frackowiak RS. 1997. The functional anatomy of a hysterical paralysis. Cognition. 64(1):B1–8. doi:10.1016/s0010-0277(97)00020-6.
- Marti S, King JR, Dehaene S. 2015. Time-resolved decoding of two processing chains during dual-task interference. Neuron. 88(6):1297–1307. doi:10.1016/j.neuron.2015.10.040.
- McGeown WJ, Venneri A, Kirsch I, Nocetti L, Roberts K, Foan L, Mazzoni G. 2012. Suggested visual hallucination without hypnosis enhances activity in visual areas of the brain. Conscious Cogn. 21(1):100–116. doi:10.1016/j.concog.2011.10.015.
- Mesulam MM. 1998. From sensation to cognition. Brain. 121 (Pt 6)(6):1013–1052. : doi:10.1093/brain/121.6.1013.
- Monod J, Wyman J, Changeux JP. 1965. On the nature of allosteric transitions: a plausible model. J Mol Biol. 12(1):88–118. doi:10.1016/s0022-2836(65)80285-6.
- Morgan AH. 1973. The heritability of hypnotic susceptibility in twins. J Abnorm Psychol. 82(1):55–61. doi:10.1037/h0034854.
- Morgan AH, Hilgard ER, Davert EC. 1970. The heritability of hypnotic susceptibility of twins: a preliminary report. Behav Genet. 1(3):213–224. doi:10.1007/BF01074653.
- Mudrik L, Faivre N, Koch C. 2014. Information integration without awareness. Trends Cogn Sci. 18(9):488–496. doi:10.1016/j.tics.2014.04.009.
- Munoz-Musat E, Rohaut B, Sangare A, Benhaiem JM, Naccache L. 2022. Hypnotic Induction of Deafness to Elementary Sounds: an Electroencephalography Case-Study and a Proposed Cognitive and Neural Scenario. Front Neurosci. (16):756651. doi:10.3389/fnins.2022.756651.
- Naccache L. 2006. Le Nouvel Inconscient. Freud, Christophe Colomb des neurosciences. Paris: Odile Jacob.
- Naccache L. 2008. Conscious influences on subliminal cognition exist and are asymmetrical: validation of a double prediction. Conscious Cogn. 17(4):1359–1360; discussion 1361-1353. doi:10.1016/j.concog.2008.01.002.
- Naccache L. 2018. Why and how access consciousness can account for phenomenal consciousness. Philos Trans R Soc Lond B Biol Sci. 373(1755):20170357. doi:10.1098/rstb.2017.0357.
- Naccache L, Blandin E, Dehaene S. 2002. Unconscious masked priming depends on temporal attention. Psychol Sci. 13(5):416–424. doi:10.1111/1467-9280.00474.
- Naccache L, Dehaene S. 2007. Reportability and illusions of phenomenality in the light of the global neuronal workspace model. Behav Brain Sci. 30(5-6):518–520. doi:10.1017/S0140525X07002993.
- Naccache L, Dehaene S, Cohen L, Habert MO, Guichart-Gomez E, Galanaud D, Willer JC. 2005. Effortless control: executive attention and conscious feeling of mental effort are dissociable. Neuropsychologia. 43(9):1318–1328. doi:10.1016/j.neuropsychologia.2004.11.024.
- Neely JH, Kahan TA. 2001. Is semantic activation automatic? A critical re-evaluation. The nature of remembering. Essays in honor of Robert G. Crowder. H. L. Roediger III, J. S. Nairne, I. Neath and A. M. Surprenant. Washington, DC: APA; p. 69–93.
- Nitzan U, Chalamish Y, Krieger I, Erez HB, Braw Y, Lichtenberg P. 2015. Suggestibility as a predictor of response to antidepressants: a preliminary prospective trial. J Affect Disord. 185:8–11. doi:10.1016/j.jad.2015.06.028.
- Pashler H. 1984. Processing stages in overlapping tasks: evidence for a central bottleneck. J Exp Psychol Hum Percept Perform. 10(3):358–377. doi:10.1037/0096-1523.10.3.358.
- Piccione C, Hilgard ER, Zimbardo PG. 1989. On the degree of stability of measured hypnotizability over a 25-year period. J Pers Soc Psychol. 56(2):289–295. doi:10.1037/0022-3514.56.2.289.
- Popkirov S, Grönheit W, Wellmer J. 2015. A systematic review of suggestive seizure induction for the diagnosis of psychogenic nonepileptic seizures. Seizure. 31:124–132. doi:10.1016/j.seizure.2015.07.016.
- Posner MI, Snyder CRR. 1975. Attention and cognitive control. In: Information processing and cognition: the Loyola Symposium, 55–85. Hillsdale, NJ: Lawrence Erlbaum Associates.
- Reuss H, Desender K, Kiesel A, Kunde W. 2014. Unconscious conflicts in unconscious contexts: the role of awareness and timing in flexible conflict adaptation. J Exp Psychol Gen. 143(4):1701–1718. doi:10.1037/a0036437.
- Rohaut B, Alario F-X, Meadow J, Cohen L, Naccache L. 2016. Unconscious semantic processing of polysemous words is not automatic. Neurosci Conscious. 2016(1):niw010. doi:10.1093/nc/niw010.
- Rosenthal DM. 2000. Consciousness, content, and metacognitive judgments. Conscious Cogn. 9(2 Pt 1):203–214. doi:10.1006/ccog.2000.0437.
- Rozier C, Seidel Malkinson T, Hasboun D, Baulac M, Adam C, Lehongre K, Clémenceau S, Navarro V, Naccache L. 2020. Conscious and unconscious expectancy effects: a behavioral, scalp and intracranial electroencephalography study. Clin Neurophysiol. 131(2):385–400. doi:10.1016/j.clinph.2019.10.024.
- Salti M, El Karoui I, Maillet M, Naccache L. 2014. Cognitive dissonance resolution is related to episodic memory. PLoS One. 9(9):e108579. doi:10.1371/journal.pone.0108579.
- Salvador A, Berkovitch L, Vinckier F, Cohen L, Naccache L, Dehaene S, Gaillard R. 2018. Unconscious memory suppression. Cognition. 180:191–199. doi:10.1016/j.cognition.2018.06.023.
- Schmidt B, Hecht H, Naumann E, Miltner WHR. 2017. The power of mind: blocking visual perception by hypnosis. Sci Rep. 7(1):4889. doi:10.1038/s41598-017-05195-2.
- Schneider W, Shiffrin RM. 1977. Controlled and automatic human information processing: I. Detection, search, and attention. Psychol Rev. 84(1):1–66. doi:10.1037/0033-295X.84.1.1.
- Schouppe N, de Ferrerre E, Van Opstal F, Braem S, Notebaert W. 2014. Conscious and unconscious context-specific cognitive control. Front Psychol. 5:539. doi:10.3389/fpsyg.2014.00539.
- Sergent C, Baillet S, Dehaene S. 2005. Timing of the brain events underlying access to consciousness during the attentional blink. Nat Neurosci. 8(10):1391–1400. doi:10.1038/nn1549.
- Sigman M, Dehaene S. 2005. Parsing a cognitive task: a characterization of the mind’s bottleneck. PLoS Biol. 3(2):e37. doi:10.1371/journal.pbio.0030037.
- Smith PH, Joris PX, Yin TC. 1993. Projections of physiologically characterized spherical bushy cell axons from the cochlear nucleus of the cat: evidence for delay lines to the medial superior olive. J Comp Neurol. 331(2):245–260. doi:10.1002/cne.903310208.
- Stolz JA, Besner D. 1997. Visual word recognition effort after meaning but not (necessarily) meaning after effort. J Exp Psychol Human Perception Perform. 23(5):1314–1322. doi:10.1037/0096-1523.23.5.1314.
- Stone J, Carson A, Duncan R, Coleman R, Roberts R, Warlow C, Hibberd C, Murray G, Cull R, Pelosi A, et al. 2009. Symptoms 'unexplained by organic disease’ in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain. 132(Pt 10):2878–2888. doi:10.1093/brain/awp220.
- Szechtman H, Woody E, Bowers KS, Nahmias C. 1998. Where the imaginal appears real: a positron emission tomography study of auditory hallucinations. Proc Natl Acad Sci U S A. 95(4):1956–1960. doi:10.1073/pnas.95.4.1956.
- Tandetnik C, Sohier E, Capelle L, Du Boullay V, Obadia M, Chammat M, Pyatigorskaia N, Naccache L. 2021. Cognitive dissonance resolution depends on executive functions and frontal lobe integrity. Cortex. 139:1–11. doi:10.1016/j.cortex.2021.02.018.
- Tiihonen J, Kuikka J, Viinamäki H, Lehtonen J, Partanen J. 1995. Altered cerebral blood flow during hysterical paresthesia. Biol Psychiatry. 37(2):134–135. doi:10.1016/0006-3223(94)00230-Z.
- Tononi G, Boly M, Massimini M, Koch C. 2016. Integrated information theory: from consciousness to its physical substrate. Nat Rev Neurosci. 17(7):450–461. doi:10.1038/nrn.2016.44.
- Trujillo-Rodriguez D, Faymonville ME, Vanhaudenhuyse A, Demertzi A. 2019. Hypnosis for cingulate-mediated analgesia and disease treatment. Handb Clin Neurol. 166:327–339.
- Van den Bussche E, Segers G, Reynvoet B. 2008. Conscious and unconscious proportion effects in masked priming. Conscious Cogn. 17(4):1345–1358. doi:10.1016/j.concog.2007.08.005.
- van Gaal S, Ridderinkhof KR, Fahrenfort JJ, Scholte HS, Lamme VA. 2008. Frontal cortex mediates unconsciously triggered inhibitory control. J Neurosci. 28(32):8053–8062. doi:10.1523/JNEUROSCI.1278-08.2008.
- van Gaal S, Ridderinkhof KR, van den Wildenberg WP, Lamme VA. 2009. Dissociating consciousness from inhibitory control: evidence for unconsciously triggered response inhibition in the stop-signal task. J Exp Psychol Hum Percept Perform. 35(4):1129–1139. doi:10.1037/a0013551.
- Van Opstal F, Gevers W, Osman M, Verguts T. 2010. Unconscious task application. Conscious Cogn. 19(4):999–1006. doi:10.1016/j.concog.2010.05.002.
- Vanhaudenhuyse A, Laureys S, Faymonville ME. 2014. Neurophysiology of hypnosis. Neurophysiol Clin. 44(4):343–353. doi:10.1016/j.neucli.2013.09.006.
- Vogel EK, Luck SJ, Shapiro KL. 1998. Electrophysiological evidence for a postperceptual locus of suppression during the attentional blink. J Exp Psychol Hum Percept Perform. 24(6):1656–1674. doi:10.1037/0096-1523.24.6.1656.
- Voigt K, Murawski C, Speer S, Bode S. 2019. Hard decisions shape the neural coding of preferences. J Neurosci. 39(4):718–726. doi:10.1523/JNEUROSCI.1681-18.2018.
- Vollhardt R, Arnulf I, Garcin B. 2022. Sleep recording for the diagnosis and treatment of paraplegia. JAMA Neurol. 79(6):627. doi:10.1001/jamaneurol.2022.0619.
- Vonderlin R, Kleindienst N, Alpers GW, Bohus M, Lyssenko L, Schmahl C. 2018. Dissociation in victims of childhood abuse or neglect: a meta-analytic review. Psychol Med. 48(15):2467–2476. doi:10.1017/S0033291718000740.
- Vuilleumier P, Chicherio C, Assal F, Schwartz S, Slosman D, Landis T. 2001. Functional neuroanatomical correlates of hysterical sensorimotor loss. Brain. 124(Pt 6):1077–1090. doi:10.1093/brain/124.6.1077.
- Wieder L, Brown R, Thompson T, Terhune DB. 2021. Suggestibility in functional neurological disorder: a meta-analysis. J Neurol Neurosurg Psychiatry. 92(2):150–157. doi:10.1136/jnnp-2020-323706.
- Wieder L, Brown RJ, Thompson T, Terhune DB. 2022. Hypnotic suggestibility in dissociative and related disorders: a meta-analysis. Neurosci Biobehav Rev. 139:104751. doi:10.1016/j.neubiorev.2022.104751.
- Woody EZ, Barnier AJ. 2008. Hypnosis scales for the twenty-first century: what do we need and how should we use them? In: M. R. Nash and A. J. Barnier, editors. The Oxford handbook of hypnosis: theory, research, and practice. Oxford: Oxford University Press; p. 255–280.
- Woody EZ, Barnier AJ, McConkey KM. 2005. Multiple hypnotizabilities: differentiating the building blocks of hypnotic response. Psychol Assess. 17(2):200–211. doi:10.1037/1040-3590.17.2.200.