
ABSTRACT
Aim: Colorectal cancer (CRC) is one of the leading cancers in the world. Even though its mortality and pathophysiology are well documented in the US and the European countries, it is seldom studied in North African population. Recent studies have shown link of HER2 overexpression in oesophageal and gastric cancers. The aim of this study is to assess the HER2 protein and mRNA expression and its correlation with tumor pathogenesis in Libyan CRC patients.
Methodology: A total of 17 FFPE tissue blocks were collected from patients with primary CRC. The HER2 protein expression was assessed by immunohistochemistry and the mRNA expression was assessed using qRT-PCR. Survival analysis of the role of HER2 overexpression on rectal adenocarcinoma was carried out on additional 165 patients.
Results: From the CRC cohort, adenocarcinoma was found to be more frequent accounting for 88.2%, and 11.8% for mucinous adenocarcinomas. Almost 47% of the cases were positive for HER2 (score ≥ 2+) and about 50% adenocarcinoma cases with tumor grade II were positive for HER2. Moreover, 57.4% adenocarcinoma patients with grade-II tumor had undergone right hemicolectomy. Furthermore, significant correlation (p = 0.03) between the HER2 mRNA expression with the tumor grade was observed. In addition, poor overall all survival was observed with high HER2 expression in rectum adenocarcinoma.
Conclusion: To our knowledge, this is the first study that HER2 overexpression correlates with more aggressive colorectal cancer in North African population. Our study shows that HER2 overexpression associates with right colon surgeries. Also, the correlation of mRNA and protein expression could warrant the implementation of a nationwide screening program for HER2 positivity in CRC patients. Taken together, stratifying patients according to HER2 expression can help in the diagnosis and prognosis of CRC patients from North African origin.
1. Introduction
Colorectal cancer (CRC) is a major health problem, ranking second in the United States, for men and women combined [Citation1]. Worldwide, the incidence of CRC is 6.1% and the mortality 9.2%. Among females, it is the second cause of death, after breast cancer and along with lung cancer [Citation2]. In Africa, CRC is still the fifth most common malignancy with a higher incidence in male than female, and the highest risk is found in North, Southern, and East Africa [Citation3]. Libya reports the highest age-standardized rates and age-specific incidence (ASRs) for CRC among the North African countries and it amounts to the first malignancy in Libyan men [Citation4,Citation5]. Since the prevalence of CRC in the Libyan population has been increasing over the last decade, a more targeted approach to the surveillance and screening programs is needed to mitigate CRC-related morbidity and mortality. Despite the ever-growing health burden of CRC, very few breakthroughs have been recorded in its treatment, especially in the area of targeted treatment.
One of the most prominent oncogenic targets is the receptor tyrosine-protein kinase erbB-2, also known as human epidermal growth factor receptor 2 protein (HER2), a member of the EGFR family of receptor tyrosine kinases, that are involved transmembrane signal transduction pathways. It has been reported to have an altered expression in multiple cancers, either because of multiple copies or because of mutations of the respective gene ERBB2 [Citation6]. Amplification of wild‐type ERBB2 is observed in 15%–20% of breast carcinomas and 20% of the gastric and gastroesophageal adenocarcinomas. Moreover, CRC cells also show expression of HER2 oncoprotein and the frequency of HER2 has been found to vary in colorectal tumors [Citation7]. There is also obscurity regarding the relationship between HER2 and the aggressiveness of colorectal tumors [Citation8]. Hence, better understanding of the role of HER2 in CRC cells is required for diagnostic and therapeutic purposes.
Moreover, alterations in the HER2 dimerization partner HER3, encoded by the ERBB3 gene, also affects HER2 signaling and the sensitivity to targeted therapies. Namely, the first anti‐HER2 targeting antibody, trastuzumab, used since 1998, binds the extracellular domain of HER2 transmembrane receptor, crucial for its dimerization, in selected patients based on their immunohistochemical and PCR profile [Citation9]. Another drug targeting the dimerization domain, at a different binding site than trastuzumab, is pertuzumab, which is still a recombinant humanized anti-HER2 IgG1 monoclonal antibody. Its effectiveness is rather low when used alone, but the combination of both trastuzumab and pertuzumab has been shown to act synergistically both in vitro and in vivo in inhibiting tumor growth, at least for breast cancer. Phase II clinical trials, such as CLEOPATRA and APHINITY study have shown prolonged overall survival and disease free survival Similar studies are now under way for colorectal cancer. Another line of treatment involves the Lapatinib, an intracellular blocker approved for both HER2 and EGFR receptors simultaneously, which shows much greater overall inhibitory effects [Citation6].
Nowadays, ERBB2 genomic alterations are emerging as an important target also for CRC. However, the impact of ERBB2 overexpression and gene amplification in CRC is limited and sometimes contradictory [Citation10,Citation11]. It has been reported that 2%–3% of all CRCs show HER2 amplification [Citation12], while the intracellular localization of HER2 has also been postulated to also have clinical significance [Citation13,Citation14], although not conclusive [Citation15]. Therefore, the knowledge of HER2 status in CRC cancers is of paramount importance, not only because HER2 might interfere with EGFR treatment options, as vastly reported [Citation11,Citation13], but also because it might aggravate a burdened genetic background. The present study assesses the expression of ERBB2 both at the protein level using immunohistochemistry and the mRNA level using qRT-PCR, in samples of Libyan CRC patients. The aim of this study is to evaluate the HER2 status in a well characterized North African population as a prerequisite to possibly implementing patient screening for CRC in North African region.
2. Materials and methods
Patients and tissue specimen
This is a clinical retrospective study of 17 Libyan patients with primary CRC. Patients with secondary cancers were excluded, whilst all primary CRC patients were included, regardless of age, gender, or tumor stage. Initial diagnosis was performed prior and independently to our testing to determine the TNM score. Tissue was sectioned from formalin-fixed, paraffin-embedded (FFPE) biopsies for molecular and immunohistochemical analysis. The patients’ characteristics are listed in .
Table 1. Clinico-pathological characteristics of the participants
Ethical approval was obtained from the Ministry of Health’s National Cancer Institute Research Ethics Committee in Libya (Reference No: NCI_MOH_23_11_2020). All methods were performed in accordance with the relevant guidelines based on the Declaration of Helsinki and the Belmont Report. We obtained a written informed consent from all study participants.
In addition to the 17 cases, 165 patients with rectum adenocarcinoma were obtained from publicly available database (www.kmplot.com) and Kaplan-Meier curve for Overall Survival (OS) analysis of 48 months in rectum adenocarcinoma were carried out.
Immunohistochemistry
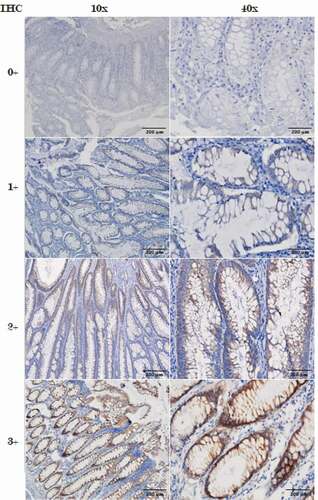
About 3 μm sections from 17 FFPE CRC patients’ biopsies were immunohistochemically stained using the rabbit monoclonal antibody for HER2 (ab214275-abcam) with 1:4000 dilutions according to the manufacturer’s instructions. Two experienced pathologists (N.M and R.H) scored independently, following the consensus recommendations for HER2 scoring for CRC [Citation15,Citation16], on a 4-point scale (0, 1+, 2+, 3+). As far as HER2 localisation is concerned, 2+ and 3+ showed predominantly membrane localisation, while 1+ and 0+ showed more staining in the cytoplasm of the tumour cells. Our study focused on assessment of the membranous HER2 expression.
RNA Extraction
RNA extraction was carried out from three sequential (3 µm) sections from the same FFPE block. Needle microdissection was carried out to enrich for the tumor content. This was carried out by marking the tumor areas on the slides and carefully removing the unmarked nontumor areas using sterile needle and collect each marked area for molecular analysis.
RNA was extracted using the RNA RecoverAll kit (Thermofisher Scientific) according to the manufacturer’s instructions. DNA removal was ensured by treating the extract with Turbo DNase. RNA content was measured at 260–280 nm using the Nanodrop and stored at −20°C until used.
Quantitative reverse transcriptase-PCR (qRT-PCR)
qRT-PCR was performed using the Superscript First-strand Synthesis system (Invitrogen). Real-time qPCR was performed in triplicates, using SYBR green (Solis BioDyne), on Quant Studio 3 (Applied Biosystem). HER2 and reference gene were preamplified using the following primer sets HER2_sense: ACATGCTCCGCCACCTCTACCA; HER_Antisense: GGATCTGCCTCACTTGGTTGTG; 18srRNA_sense: TGACTCAACACGGGAAACC; 18srRNA_antisense: TCGCTCCACCAACTAAGAAC. A total 40 PCR cycles were performed consisting of 15 secs denaturation at 95°C and a combined annealing/extension cycle of 10 min at 60°C. The threshold cycle value (Ct) was normalized against the Ct value of internal control 18s RNA. The primer sequence has been previously published [Citation16].
Statistical Analysis
All statistical analysis was carried out using SPSS (version 24) and Graph Pad Prism (version 8.1.2). Comparisons with p < 0.05 were considered to be statistically significant. One-way Annova was used to calculate the difference in the mRNA expression between the study groups. Correlation between IHC and the mRNA expression was assessed and Pearson’s r > 0.9 was indicative of minimal assay variability. Survival curves were constructed with the use of the Kaplan-Meier method, and survival differences were analyzed by the log rank test.
3. Results
Clinicopathological characteristics of CRC patients
Our study group comprised of eight males and eight females (in one case, gender was not recorded). The patients’ age ranged from 33 to 86 years (mean: 61 years). All clinico-pathological data are shown in . Histopathological examination identified most cases as adenocarcinomas (15/17, 88.2%) and 2 mucinous adenocarcinomas (11.8%). According to the TNM classification, the patient biopsies were classified as stage I (2/17, 11.8%), stage II (12/17, 70.6%), and stage III (3/17, 23.5%). No difference in classification and staging were observed with respect to gender or age.
Table 2. Table of the HER2 IHC and qRT-PCR
HER2 protein expression using IHC analysis
Following the HER2 diagnostic criteria, 2+ staining in ≥10% but less than 50% of tumor cells were considered negative while the others were retested as they were still equivocal [Citation17]. A representative image of the HER2 staining is shown in . Among the CRC cases tested, 47% (8/17) of the cases were positive for HER2 (Score ≥ 2+) whereas, 52.94% (9/17) were negative for HER2 (≤ 1+). Amongst the HER2 positive cases, 23.52% (4/17) were identified to be equivocal with a score of 2+ and 23.52% (4/17) were identified to be strongly positive with a score of 3+ .
Figure 1. IHC staining images with (0, 1+, 2+, 3+) different scoring, were the 0, 1+ considered to be negative and 3+ considered to be positive
HER2 mRNA expression by qRT-PCR
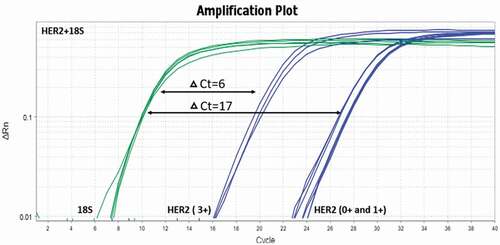
Regardless of their HER2 IHC profile, all samples were evaluated using qPCR for the quantification of HER2 mRNA. A representative image of the qPCR amplification plot with HER2 positive and negative samples is seen in . Ct for the 18S rRNA varied from 11.7 to 25.7 while the Ct for HER2 ranged from 27.1 to 35.9. The results of PCR are summarized in .
Figure 2. ERBB2 mRNA expression. Examples of real time PCR with SYBER Green. This was carried out in triplicate using RNA samples extracted from tumour cells microdissection from paraffin-embedded tissue sections
Correlation between HER2 mRNA and protein expression in CRC patients
Similar to the HER2 protein expression and varying levels of mRNA expression was observed in all the study samples. Strong correlation with the r2 value of 0.77 was observed with the HER2 protein and mRNA expression (). Significant difference in the mRNA expression was observed between HER2 negative and HER2 positive groups (p = 0.03) however, no significant difference in the expression was observed with HER2 negative and equivocal groups ().
Figure 3. (a) Correlation of IHC group to HER2 protein expression and (b) correlation of HER2 mRNA expression between CRC study groups delta Ct mean to HER2 mRNA expression. * p < 0.05
Correlation of HER2 and CRC clinical pathological data
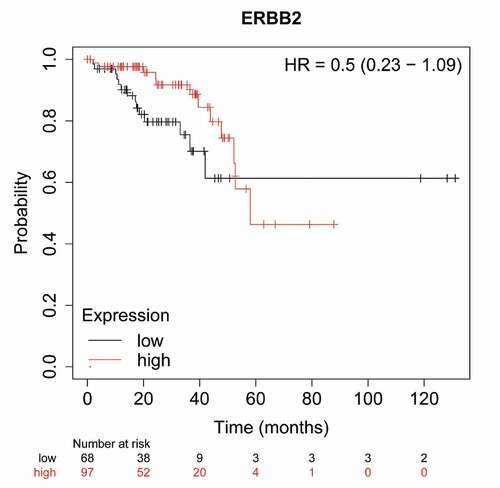
From the cohort of adenocarcinoma (88.23%), 50% adenocarcinoma cases with tumor grade II was observed to be positive for HER2 (score ≥ 2). Also, the female CRC cases found to be highly positive for HER expression (62.5%) whereas, only 50% of HER2 positivity was observed in male CRC specimens. HER2 mRNA expression and the tumor grade was found to be significantly correlated with the (r2 = 0.33, p = 0.03). However, survival analysis on 165 patients with rectum adenocarcinoma revealed poor overall survival with high HER2 expression showing steep drop between after 40 and 60 months (). This further strengthens our understanding of the association between HER2 expression and CRC severity.
Figure 4. In large cohort of 165 patients, high HER2 expression show a trend, after 40 months, towards poor overall survival in rectum adenocarcinoma
4. Discussion
This is the first study linking HER2 expression to colorectal cancer in Libya, which has the highest CRC incident in North Africa. The study show that HER2 overexpression seems to correlate with more aggressive colorectal cancer so stratification of patients according to HER2 status can be beneficial in the therapeutic management of patients and early detection of aggressive CRC, which can better inform the type of treatment needed for the patient thereby improving their survival and quality of life. In addition, the findings show that HER2 overexpression associates with right colon surgeries, which may help surgeons to plan resections in a more efficient manner resulting in less adverse effects thereby improving the patients’ quality of life postsurgery. In addition, the study shows that HER2 mRNA expression correlates with protein expression levels, and this finding could warrant the implementation of a nationwide screening program for HER2 positivity in CRC patients.
Moreover, current clinical trials, such the HER2 Amplification for Colorectal Cancer Enhanced Stratification (HERACLES) cohort A and the My Pathway have already provided evidence of the usefulness anti-HER2 therapies in the abovementioned cohort of patients [Citation17]. The combination of trastuzumab, the anti-HER2 monoclonal antibody, and lapatinib, the dual EGFR/HER2 small-molecule inhibitor, is more effective in reducing tumor size in ERBB2-amplified metastatic CRCs, than each one alone [Citation18].
Our results suggest that HER2 positive samples are the 47% of the tested samples which is highly larger than the generally reported percentage. In a Chinese population, the reported positivity with the same scoring criteria is 2.6% which is more aligned to the generally reported [Citation19]. Membranous expression of HER2 was observed in samples with score of 2+ and above. Although some samples showed cytoplasmic staining, based on the intensity and distribution, the cytoplasmic staining was not more than +1 score and are grouped as HER2 negative. In addition, ΔCt is an indication of the normalized quantitative HER2 expression within tumor cells. We have found that ΔCt correlated significantly to the IHC groups. This further confirms HER2 positivity in colorectal cancer in Libyan samples. The lack of established scoring system of HER2 in CRC is responsible for the variability of the reported percentages, ranging from 1.3 to 82%. The United Kingdom has undertaken an initiative to unify HER2 scoring nationwide, through its UK-NEQAS scheme, mostly for breast cancer [Citation20].
The findings from this study are especially important to using HER2 screening for a wide nationwide search, in the future. In Libya, the field of disease mapping has not been developed enough, although cancer is the third leading cause of death in the country, after car accident and cardiovascular disease [Citation20].
It has been clearly demonstrated that HER2 gene amplification differs significantly between right/left-sided and rectal carcinomas. In our study, most of the cases that scored 2+ and 3+ CRC ended up having right hemicolectomy. A right hemicolectomy is usually performed for cancer of the cecum and ascending colon, and for some hepatic flexure. A left hemicolectomy is appropriate for tumors in the distal transverse or descending colon and for selected patients with proximal sigmoid colon cancer. While mortality and major complications are comparable to both sides, in right-sided colectomies, patients were less likely to have a superficial infection due to the surgery. Regarding the malignancy status, patients with right-sided colon cancers are different than those with left-sided cancers. They are older, present at a more advanced stage, and have a higher unadjusted mortality rate postoperatively [Citation21]. In our study, the patients are rather older in age and with more advanced cancer, matching the previous reports. Moreover, previous studies in Libya have revealed that women are more likely to be affected by a right colon tumour [Citation3]. Furthermore, another study found that distal CRC was more prevalent in Libya [Citation4].
The issue of regionality of CRC cancer is very important because of the genetic component and the regional diet and traditions that may enhance or decrease the CRC risk. The shift from traditional food to more universal processed food has been seen across the globe. In Tunisia, within 15 years (1994–2009), the incidence of CRC has markedly increase and it is postulated that if no interventions are implemented it is going to double by 2024. This increase is mostly due to the change of living of Tunisians, which leads to obesity, sedentary living, and junk food eating [Citation22].
Due to the lack of infrastructure and the awareness in HER2 colorectal cancer testing, almost 80% of the colorectal tumors were identified in the late stages of tumorgenesis and only 20% of the patients are identified with early stages of CRC [Citation23]. In addition, as the secondary tumors and tumors with no proper clinical records were excluded from the study, the number of samples would be reduced. In addition, there is a single specialist oncology center, whilst peripheral clinics accept and treat cancer patients, however without consistent patients’ record keeping. Therefore, longitudinal studies cannot be performed, since patients are lost after initial recover and no follow up is set up. These limitations, however, just further highlights the value of this research, as the first that records and assesses CRC patients in this North Africa, in terms of HER2 link to cancer severity. Having said that, this study employed multiple molecular methods to identify the HER2 expression in the patients’ cohort. Taken together, the prevalence from this study provides an accurate representation of the HER2 expression in the larger cohort of Libyan colorectal cancer patients. In addition, considering the limited sample size included herein, the available TCGA database with 165 samples was used to further illustrate the effect of HER2 expression on the overall survival of colorectal cancer patients.
5. Conclusions
Based on the above findings, we conclude that HER2 amplification at the transcript and protein level correlates to aggressive CRC disease in Libyan population and can be used as a reliable screening tool for aggressive CRC in Libya and other North African countries. Once extensive database of CRC patients is established, molecular screening of HER2 (such as those from blood) in the population may be used to determine the risks associated with the constantly increasing CRC risk in North Africa.
Disclosure statement
The authors declare no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Funding
References
- Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145–7. Epub 2020/03/07.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. Epub 2018/09/13.
- El Mistiri M, Salati M, Marcheselli L, et al. Cancer incidence, mortality, and survival in eastern libya updated report from the benghazi cancer registry. Ann Epidemiol. 2015;25(8):564–568. Epub 2015/04/29.
- Bodalal Z, Bendardaf R. Colorectal carcinoma in a southern mediterranean country: The libyan scenario. World J Gastrointest Oncol. 2014;6(4):98–103. Epub 2014/04/16.
- Bodalal Z, Azzuz R, Bendardaf R. Cancers in eastern libya: first results from benghazi medical center. World J Gastroenterol. 2014;20(20):6293–6301. Epub 2014/05/31.
- Oh DY, Bang YJ. HER2-targeted therapies - a role beyond breast cancer. Nat Rev Clin Oncol. 2020;17(1):33–48. Epub 2019/09/25.
- Koeppen HK, Wright BD, Burt AD, et al. Overexpression of HER2/neu in solid tumours: an immunohistochemical survey. Histopathology. 2001;38(2):96–104. Epub 2001/02/24.
- Kruszewski WJ, Rzepko R, Ciesielski M, et al. Expression of HER2 in colorectal cancer does not correlate with prognosis. Dis Markers. 2010;29(5):207–212. Epub 2011/01/06.
- Ross JS, Fakih M, Ali SM, et al. Targeting HER2 in colorectal cancer: The landscape of amplification and short variant mutations in ERBB2 and ERBB3. Cancer. 2018;124(7):1358–1373. Epub 2018/01/18.
- Wang XY, Zheng ZX, Sun Y, et al. Significance of HER2 protein expression and HER2 gene amplification in colorectal adenocarcinomas. World J Gastrointest Oncol. 2019;11(4):335–347. Epub 2019/05/02.
- Li G, Zheng J, Xu B, et al. Simvastatin inhibits tumor angiogenesis in HER2-overexpressing human colorectal cancer. Biomed Pharmacother. 2017;85:418–424. [ Epub 2016/11/27].
- Sartore-Bianchi A, Amatu A, Porcu L, et al. HER2 positivity predicts unresponsiveness to EGFR-targeted treatment in metastatic colorectal cancer. Oncologist. 2019;24(10):1395–1402. Epub 2019/04/07.
- Buhmeida A, Assidi M, Al-Maghrabi J, et al. Membranous or cytoplasmic HER2 expression in colorectal carcinoma: evaluation of prognostic value using both IHC & BDISH. Cancer Invest. 2018;36(2):129–140. Epub 2018/03/06.
- Pyo JS, Kang G, Park K. Clinicopathological significance and diagnostic accuracy of HER2 immunohistochemistry in colorectal cancer: a meta-analysis. Int J Biol Markers. 2016;31(4):e389–e94. Epub 2016/10/30.
- Owen DR, Wong HL, Bonakdar M, et al. Molecular characterization of ERBB2 amplified colorectal cancer identifies potential mechanisms of resistance to targeted therapies: a report of two instructive cases. Cold Spring Harb Mol Case Stud. 2018;4(2):2. Epub 2018/02/14.
- Pye H, Butt MA, Funnell L, et al. Using antibody directed phototherapy to target oesophageal adenocarcinoma with heterogeneous HER2 expression. Oncotarget. 2018;9(33):22945–22959. Epub 2018/05/26.
- Tadmouri GO, Sastry KS, Chouchane L. Arab gene geography: from population diversities to personalized medical genomics. Glob Cardiol Sci Pract. 2014;2014(4): 394–408. Epub 2014/01/01
- Dowsett M, Hanby AM, Laing R, et al. HER2 testing in the UK: consensus from a national consultation. J Clin Pathol. 2007;60(6):685–689. Epub 2007/02/27.
- Valtorta E, Martino C, Sartore-Bianchi A, et al. Assessment of a HER2 scoring system for colorectal cancer: results from a validation study. Mod Pathol. 2015;28(11):1481–1491. Epub 2015/10/10.
- Liu F, Ren C, Jin Y, et al. Assessment of two different HER2 scoring systems and clinical relevance for colorectal cancer. Virchows Arch. 2020;476(3):391–398. Epub 2019/11/14.
- Khiari H, Ben Ayoub HW, Ben Khadhra H, et al. Colorectal cancer incidence trend and projections in tunisia (1994–2024). Asian Pac J Cancer Prev. 2017;18(10): 2733–2739. Epub 2017/10/27.
- Lo AC, Soliman AS, Khaled HM, et al. Lifestyle, occupational, and reproductive factors and risk of colorectal cancer. Dis Colon Rectum. 2010;53(5):830–837. Epub 2010/04/15.
- Wang XY, Zheng ZX, Sun Y, et al. Significance of HER2 protein expression and HER2 gene amplification in colorectal adenocarcinomas. World J Gastrointest Oncol. 2019;11(4):335–347.