
Abstract
This scoping review addresses peer-reviewed research on musical interaction with children and young people with severe/profound intellectual and multiple disabilities (S/PIMD). Twenty-five articles published between the years 2000 and 2020 met the inclusion criteria. A narrative synthesis was used to summarise and evaluate different features, including participant characteristics, study design and methods, type of musical interaction, the abilities and behaviours in focus, reported benefits, promising components of musical interaction, and quality appraisal of the studies. The results revealed a variation in participant characteristics and study designs, where small-sample descriptive case studies were most common. In terms of the type of musical interaction, active music therapy was the most commonly used approach, followed by technology-mediated and multisensory musical activities. In terms of abilities and behaviours, a large majority of the studies focused on social interaction and communication, followed by engagement, attention and affect. Six categories were identified as promising components of musical interaction: the responsivity of the interaction partner, singing songs, structure and predictability in the activities, long-term interventions, technology-mediated and multisensory musical activities, and a therapeutic alliance between interaction partners. Based on this review, we discuss future research and practical implications for musical interaction and music therapy for children and young people with S/PIMD.
Background
Almost everyone—irrespective of capabilities or disabilities—is engaged with music from birth, or even earlier (Trevarthen Citation2002). Interestingly, music therapists and researchers focusing on infants have found that communicative behaviours between infants and their caregivers have a musical structure (Bunt and Pavlicevic Citation2001). Communicative signals are unconsciously mirrored and imitated, and the melodic intonation in oral sound and speech evokes attention and affect. The synchronisation of movements and feelings between infants and caregivers forms a shared process of entrainment, which is defined as shared rhythmic timing and an affective state (Malloch and Trevarthen Citation2009, Phillips-Silver and Keller Citation2012). This kind of interaction is considered to support children’s communicative and social development (Trevarthen Citation2002).
Similarly, it has been proposed that musical-interaction activities and music therapy develop not only musical abilities, but also more general developmental abilities such as social and communicative skills in children with intellectual disabilities (Wigram et al. 2002). These kinds of music-supported interaction are often guided by findings from the general literature on infant development, including the role of responsiveness by the caregiver (Malloch and Trevarthen Citation2009). A number of narrative literature reviews focus on music and children with different kinds of disability (e.g. Meadows Citation1997, Jellison Citation2000, Stephenson Citation2006, Kantor Citation2020). However, previous research on music with children and young people with severe or profound intellectual and multiple disabilities is very scarce (Welch et al. Citation2009, McFerran and Shoemark Citation2013). In fact, to the best of our knowledge, there is no current scoping or systematic review of musical interaction involving children and young people within this group.
People with profound intellectual and multiple disabilities (PIMD) are dependent on others in all situations in life. Their communication is non-verbal, idiosyncratic and expressed by bodily movements, gestures and sounds (Griffiths and Smith Citation2016). This is a heterogeneous group when it comes to how the disability affects an individual’s abilities and functioning in everyday life (Granlund, Almqvist and Wilder Citation2013). Two characteristics form the key defining features of PIMD: (i) a profound intellectual disability and (ii) profound motor disability (Nakken and Vlaskamp Citation2007). In addition, people with PIMD almost always have a number of additional sensory disabilities and medical comorbidities (Nakken and Vlaskamp Citation2002, Axelsson et al. 2013). Since it is often very difficult to assess the exact degree of intellectual disability in children with severe (i.e. IQ 20–35) to profound ID (i.e. IQ < 20), who also have several other disabilities (Nakken and Vlaskamp Citation2007, Maes et al. Citation2021, Rensfeldt Flink et al. Citation2020), children reported to have a severe intellectual disability are also often included in studies of PIMD (Arthur-Kelly et al. Citation2018, Bindels-de Heus et al. Citation2013). By definition, adaptive difficulties are characteristic features in ID in general (ICD-11, World Health Organization, 2018). Thus, S/PIMD (severe/profound intellectual and multiple disabilities) is the term preferred by some authors (Griffiths and Smith Citation2016, Granlund, Almqvist and Wilder 2013), and this is the term which will be used in the present scoping review.
The current study focuses on musical interaction with children and young people with S/PIMD. We define musical interaction as situations in which at least one child or young person with S/PIMD is involved in making music, together with a therapist, an educator or interaction partner with primarily non-musical goals. Depending on the setting and the background of the researchers, several different terms have been used to describe this situation and activity. These include active music therapy (Wigram et al. 2002, Raglio et al. Citation2017), musical dialogues (Ockelford Citation2012) and musical interaction (Kantor Citation2020, Wimpory and Nash Citation1999). Here, the term ‘musical interaction’ is used consistently as an umbrella term, regardless of the terms used in the original studies. We acknowledge that the theoretical background and the intended outcomes for each type of intervention may vary. Also, systematic factors such as the mandatory credentials of the musical interventionist might differ across different countries and in different settings (e.g. education versus health care). Our definition excludes some aspects of music therapy activities, specifically the use of receptive music therapy methods in the form of listening to music (see Grocke and Wigram Citation2007, Grocke 2016).
People with S/PIMD are considered to benefit from musical interaction (Wigram et al. 2002, Kantor Citation2020). According to several accounts, musical interaction can be used with people with S/PIMD as a promising way of making connections, since verbal communication is often not an accessible option (e.g. Wheeler Citation2013). Wigram and Elefant (Citation2008) note that musical interaction provides a potentially important means of communication for people with S/PIMD: ‘When meeting a speechless client, the music therapist has the tools to promote communicative musicality, thus enabling a person to give their meaning a sound, and to sense that it has been received’ (p. 442). According to Wigram et al. (2002), non-musical goals are generally the focus of musical activities with this population. Examples of non-musical goals include enhanced communication and increased engagement.
We present a scoping review of research which focuses on musical interaction with children and young people with S/PIMD. A previous systematic review of research on music with children with disabilities was carried out by Brown and Jellison (Citation2012). An overwhelming majority of the studies in that review included children and adolescents with less severe disabilities than S/PIMD. In order to pinpoint the benefits of musical interaction with children and young people with S/PIMD, and to enable research about the target group to be cumulative, the aims of the current study are to identify and review research on musical interaction with children and young people with S/PIMD. Brown and Jellison (Citation2012) covered research conducted between the years 1999 and 2009 in the United States of America. The current scoping review focuses on research from 2000 to 2020 in a wider geographical context than Brown and Jellison, as it includes overall peer-reviewed research studies written in English.
Research questions
The paper sets out to examine the following research questions:
What kinds of participants have been included in research about musical interaction in children and young people with S/PIMD, specifically in terms of age, actual diagnosis, severity of the disability and additional conditions?
Which study designs and methods are used in the studies?
Which types of musical-interaction activity are carried out?
What kinds of abilities and behaviours do the studies focus on?
To what extent are musical-interaction activities reported as beneficial or effective?
Which components of the musical-interaction activities are reported as promising?
What is the scientific quality of the studies in this field?
Method
Scoping review
Scoping reviews are commonly used to identify and map available evidence in a given research area which is not sufficiently established to be suitable for a systematic review approach. It includes a variety of study designs and varies in terms of study quality (Munn et al. Citation2018, Arksey and O’Malley 2005). We argue that this is the current state of the research fields of musical interaction in children and young people with S/PIMD. Unlike the procedure for systematic reviews, it is uncommon to submit a pre-registered protocol for scoping reviews. Instead, scoping reviews are typically iterative, so that changes or critical distinctions can appear during the actual review, and these, in turn, may change the inclusion/exclusion criteria (Oudshoorn et al. Citation2021). Often, as is the case with the present study, scoping reviews can involve considerable time spent on screening articles due to broader search strings. Munn et al. (Citation2018) highlight that, unlike systematic reviews, scoping reviews are not always subject to quality appraisal and do not always involve a summary of findings. Nonetheless, we have chosen to perform a quality appraisal and include a summary of findings more in line with a systematic review approach, in an attempt to provide an overall assessment of the evidence base.
Search strategy
The review aims to identify all studies examining musical interaction in children and young people with S/PIMD in peer-reviewed journals written in English during the period 2000–2020. Potential studies were identified through computer-assisted searches in the PsychINFO, Scopus and PubMed databases. In addition, through Google Scholar, all papers were screened which cited the prior systematic review by Brown and Jellison (Citation2012). The reference lists in the identified articles, and relevant review articles, were examined with the aim of identifying additional studies of relevance. The database searches were performed using various combinations of keywords and mesh/thesaurus terms, which were developed with assistance provided by the Stockholm University Library. The search terms consisted of descriptors related to: (i) intellectual or developmental disability (ii) music and (iii) children and young people. The databases were initially searched in October 2019, and the search was updated in January 2020. presents the search terms used, and shows how they were combined in one of the databases, PubMed.
Table 1. Search strategy for PubMed database.
Inclusion criteria
Empirical research studies were included which examined children and young people with S/PIMD (age: birth-21 years old) and musical interaction, and which were published in peer-reviewed journals in English between the years 2000 and 2020. The timeline was chosen in order to focus on the most recent papers from the last two decades. Because of the heterogeneity of the specific terms/nomenclature used in both research and clinical contexts to refer to children and young people with what can be described as S/PIMD (Maes et al. Citation2021), descriptions equivalent to the term were considered for incorporation. Examples include children and adolescents with impairments, with learning disabilities, with no verbal language, in need of support in all everyday life situations, with extensive sensory-motor difficulties and with medical comorbidities. This, in turn, led to many initial hits (see ).
Exclusion criteria
Studies were excluded which did not report data from cases or groups of individuals with S/PIMD (or equivalent) or who were 21 years of age or less. A study was also excluded if the musical-interaction activities only involved listening to recorded music. Equally, the study was excluded if no empirical data were presented.
Screening process
The three databases were independently accessed and searched using the same search terms, but using different strategies and specific wording, given the unique structure of each database. shows the strategy used for searching the PubMed database. The studies retrieved were imported into the online web form ‘Rayyan’ (https://rayyan.qcri.org), where the authors coded whether the study should be included or excluded, and stated the reason.
Study selection
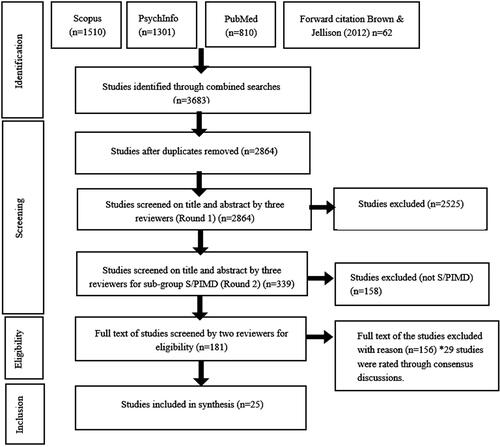
The selection process for the studies followed the four stages of the PRISMA guidelines (Liberati et al. Citation2009): (1) identification, (2) screening of title and abstracts, (3) eligibility and (4) inclusion. The first step, the identification phase, involved searches in the aforementioned databases and forward citation. This resulted in 3683 studies. The next step, the screening process, began with the removal of duplicates. Then the relevance of the studies was screened by the three authors, by reading titles and abstracts.
Given the variety of terms used in the field and in different geographic locations, we used broad search terms in order to include all relevant studies. First, we identified studies involving research participants with a developmental or intellectual disability who engaged in musical interaction. The second step was to identify studies with research participants who were non-verbal, and had severe motor or other sensory impairments, as well as an early developmental level according to IQ/DQ (developmental quotient) or adaptive functioning measures. The relevance of the studies was further examined in a third step, where two of the authors read the full text of each of the articles identified in the second step. As shown by the flow chart in , the remaining 29 studies were rated through consensus discussions. As a result, 25 studies were included.
Figure 1. Flowchart of study selection for scoping review.
Strategy for data synthesis and grading evidence
The studies that met the inclusion criteria were summarised in a standardised form to enable the findings to be compared and contrasted across studies. The aggregation of research was analysed in relation to the research questions. A summary of each study is presented in , with reference to the following aspects:
Table 2. Overview of studies on musical interaction and children with S/PIMD included in the review.
Participant characteristics. The number, age and sex of the participants were reported. The various terms and descriptions used for children and young people with S/PIMD in the original studies were maintained (e.g. profound developmental disabilities, motor-cognitive disabilities, profound and multiple learning difficulties, etc.). Eventual additional conditions were also reported (e.g. Rett syndrome, Cortical vision impairment, Autism spectrum disorder, etc.).
Study designs and data collection methods. The following study designs were found: (i) Case-study design; (ii) Single-subject experimental design; (iii) Experimental group design; (iv) Longitudinal observation study; (v) Other design. Categorising studies was challenging due to the diversity of approaches and designs. These included qualitative, quantitative and mixed-method studies, which used different kinds of epistemological premises and terminology to describe research-related concepts (e.g. outcomes/targeted abilities or behaviours, effectiveness/proposed benefits of intervention). We acknowledge the complementary benefits of qualitative and quantitative research, in that qualitative research often contributes to a deeper understanding of complex phenomena and mechanisms in music therapy, whereas quantitative research has strengths in evaluating the effectiveness of an approach (Erkkilä Citation2016). In terms of our approach to categorisation, a case-study design presents musical-interaction activities, targeted abilities or behaviours and participants in a descriptive way, and it uses predominantly qualitative data collection methods (Yin Citation2014). A single-subject experimental design, by contrast, always uses quantified variables, through which a musical-interaction activity is evaluated experimentally against a control condition. Similarly, experimental group designs evaluate the effectiveness of an intervention quantitatively, by comparing a (quasi) randomised or non-randomised musical-interaction intervention group and a comparison group. A longitudinal observation study includes a number of observations of one individual or a group of individuals participating in musical-interaction activities over a longer period of time, and is commonly evaluated quantitatively. The last category, ‘other design with musical-interaction activities’, includes studies which used a short study design format called a case report, or studies with some features and descriptions from single-subject experimental methodology, but which do not qualify as experimental due to a lack of control condition(s).
We also report data collection methods (e.g. video observations, surveys, interviews, etc.) and the types of research instrument used (e.g. author-constructed research instruments, extant/standardised research instruments, no specific research instruments, etc.).
Types of musical-interaction activity. The following categories were formed in relation to the musical-interaction activities for individuals and groups: (i) active music therapy, (ii) technology-mediated and multisensory musical activities, (iii) dual treatment, (iv) music lessons. The exact meaning of these categories is reported in the results. Additionally, we report whether there was a control/comparison condition to which the musical-interaction activities was contrasted.
Abilities and behaviours in focus. This centred on the goals of the musical-interaction activities. In quantitative studies, this was often referred to as the dependent variable. In qualitative studies, the term was not used, and we chose instead the term ‘abilities and behaviours in focus’ as an epistemologically neutral term to describe the focus and outcomes of the interventions and activities. Six categories were formed: (i) social interaction and communication; (ii) engagement, attention and affect; (iii) musical abilities; (iv) movement and motor skills; (v) cognitive abilities; (vi) other abilities and behaviours. In several studies, more than one of the abilities or behaviours in focus was highlighted in the results.
Reported benefits or effectiveness of intervention. Here we summarise the extent to which the studies report positive benefits, or the effectiveness of the musical-interaction activities. We adopted this conceptualisation because of the diversity of terms used in different studies. This section also notes whether there were any differences in relation to any eventual control conditions.
Promising components of musical interaction. We identified promising components of musical interaction, as reported in the studies. We were analytically informed by inductive content analysis used in systematic reviews (Elo and Kyngäs Citation2008, Mikkonen and Kääriäinen Citation2020): the raw data (the articles) were read through several times in order to identify and extract units of meaning involving promising components of musical interaction. The units of meaning were listed in an EXCEL sheet, and read through several times in order to identify overarching categories. The process of identifying the categories was in keeping with an inductive approach, in that it took place iteratively and exploratively, rather than basing it on an a priori checklist (Kyngäs Citation2020).
Study quality. Although quality appraisals are not always used in scoping reviews, we chose to evaluate the quality of the studies included. The quality of the evidence was assessed using the adapted Evidence-Based Librarianship Critical Appraisal Checklist (EBL-CAC) used in a recent study with the same target group (Van Keer and Maes Citation2018). The included studies were critically analysed with the EBL-CAC, to determine their validity and appropriateness from the perspective of a more quantitative research tradition. Meta-analysis was not appropriate due to the nature of the research questions, as well as the heterogeneity of the studies, methods and data types. The checklist was developed according to the conventions of the quantitative research paradigm, and was therefore not particularly suitable for assessing the qualitative aspects of the selected studies. Nonetheless, we consider that this complementary approach provides a way of evaluating the research which has been carried out, and makes it possible to identify directions for future research. In practice, the first author followed the checklist and rated each feature separately in accordance with guidelines described in Glynn (Citation2006) and Van Keer and Maes (Citation2018).
Reliability check of quality appraisal
The quality appraisal inevitably involves a subjective component. Following Tarvainen et al. (Citation2020), an interrater reliability check was conducted to examine the reliability of the quality appraisal in a randomly chosen (5/25) 20% of the studies, as performed by two of the authors. The reliability check yielded a match of 86% point-by-point agreement. A common benchmark for an acceptable percentage of agreement is >80% (Nurjannah and Siwi Citation2017).
Results
Participant characteristics
As expected, based on previous accounts (Nakken and Vlaskamp Citation2007, Maes et al. Citation2021), a heterogeneity of specific terms was used to describe participant groups, as shown in . Profound and Intellectual Developmental Disabilities, Profound and Multiple Learning Difficulties (PMLD), Severe and Multiple Disabilities, Significant Cognitive Challenges, Motor-cognitive Disabilities, Profound Developmental Delay, etc.). It is worth noting that the terms S/PIMD and PIMD were not used in any of the studies.
Figure 2. Terms used in the studies to describe the participants.
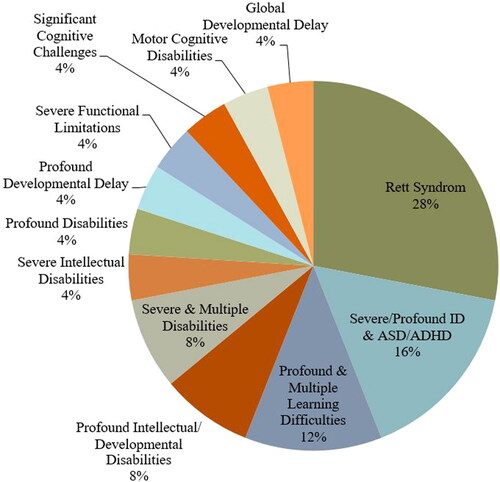
In terms of the aetiology of the ID, the largest group with a known aetiology consisted of individuals with Rett syndrome (7/25, 28% of studies). Other reported conditions consisted of a number of neurodevelopmental and medical conditions: autism spectrum disorder (ASD); attention deficit hyperactivity disorder (ADHD); epilepsy; scoliosis; hydrocephalus; premature birth complications including bronchopulmonary dysplasia; and motor and sensory difficulties. Several participants had cerebral palsy, and in terms of sensory disabilities, many were reported to have visual impairments, including cases with cortical blindness and Norrie’s disease. Nevertheless, the studies were extremely varied in terms of the level of detail they reported for the characteristics of participants. In one study involving a participant with a rare diagnosis, specific information on the condition(s) was omitted to avoid jeopardising participant confidentiality.
In terms of the number of participants in the selected studies, (12/25) 48% had 2–10 participants, followed by one single participant in (9/25) 36%, and (3/25) 12% of the studies included 11–20 participants. Only one study (4%) had more than 50 participants. The age of the participants ranged from 4 to 19 years old. In two of the studies the ages were not specified (participants were described as ‘an adolescent boy’ in one and ‘children’ in the other). In total, 187 participants with S/PIMD were included.
Study designs
A majority of the selected studies had a case-study design (15/25, 60%). Several studies were reported as single-subject experimental designs (5/25, 20%); three of these had a baseline phase (i.e. ‘single-subject experimental design’ according to the categories described previously), whereas the other two were included in the ‘other design with musical-interaction activities’ category, as there was no baseline/control phase. Another study design category consisted of longitudinal observational studies (3/25, 12%). One study (4%) had an experimental group design, and another was a case report study, allocated to the ‘other design’ category.
Data collection methods
Qualitative data were reported in (12/25) 48% of the studies. Quantitative data were reported in (9/25) 36%. In four studies (16%), a mixed-method approach to data collection and reporting had been used (a combination of qualitative and quantitative data collection methods).
A large majority of the studies used video recordings/observations as a main data collection method (20/25, 80%). In (4/25) 16% of the studies, interviews were carried out with staff or caregivers. In (2/25) eight percent of the studies, parental and staff questionnaires and rating scales were used. The categories and distribution in the studies were as follows:
Author-constructed research instruments—Newly created instruments for the study were reported in (9/25) 36% of the studies.
Systematic observation procedures—Checklists, event/duration, recordings and time sampling were reported in (6/25) 24% of the studies.
In (6/25) 24% of the studies, no specific research instrument was reported.
Extant research instruments—Standardised tests, or tests used or based on those used in other studies, were reported in (4/25) 16% of the studies.
Types of musical-interaction activity
A substantial majority (19/25, 76%) of the musical-interaction activities were carried out individually, involving one participant with S/PIMD and a musical-interaction partner (e.g. educator, therapist). In (3/25) 12% of the studies, these activities were carried out in groups of children or young people with S/PIMD. Individual as well as group activities were performed in (3/25) 12% of the studies.
In terms of the types of musical-interaction activity carried out, the following categories were formed:
Active music therapy was found in a majority of the studies (16/25, 64%). They were predominantly carried out individually, although some studies included small groups. Some studies specified the approach, such as improvisational music therapy (3/25, 12%). One study consisted of analytical music therapy and another of creative music therapy. In the other studies, music therapy activities included vocalisation and sound production, dancing and moving to the music, sensory stimulation and playing instruments.
Technology-mediated and multisensory musical activities were found in (5/25) 20% of the studies. This category included the use of digital interfaces and assisted devices in musical instruments (e.g. micro-switches or musical ‘smart-things’), with a varying level of multisensory feedback (e.g. visual, tactile) in addition to the music itself.
Dual treatment was found in (2/25) eight percent of the studies. In this type of activity, musical interaction was combined with another therapy (e.g. physiotherapy or speech and language therapy).
Music lessons were found in (2/25) eight percent of the studies. These consisted of whole-class musical activities.
Abilities and behaviours in focus
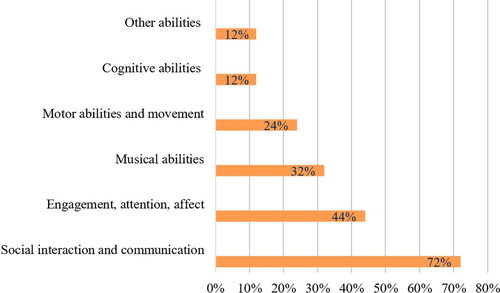
The focus of musical-interaction intervention varied in the identified studies, and several focused on two or more abilities and/or behaviours (see ). Social interaction/communication was the focus of (18/25) 72% of the studies, and engagement, attention and affect were highlighted in (11/25) 44% of the studies. Musical abilities were the focus of (8/25) 32% of the studies, and movement and motor abilities in (6/25) 24%. Cognitive abilities such as grasping object permanence, making choices and understanding causality, were highlighted in (3/25) 12% of the studies. The last category, other behaviours, (e.g. reduced parental stress, reduced frequency of epileptic seizures, participation and strategies used by music therapists) was found in (3/25) 12% of the studies.
Figure 3. Abilities and behaviours in focus in the studies.
Reported benefits and effectiveness of musical-interaction activities
A large majority (21/25, 84%) of the studies reported positive benefits or effectiveness of the musical-interaction activities (see ). Of these 21 studies, five included a control group or condition. In another (3/25) 12% of the studies, partial effectiveness was reported (e.g. in some behaviours and/or abilities, or in some participants). Finally, one study (4%) reported that musical interaction was no more effective than the control conditions. Thus, all but one study reported benefits, effectiveness or partial effectiveness of musical interaction on the abilities and behaviours of interest.
Promising components of musical interaction
Six categories were identified and developed according to the way the authors of the included studies had identified promising components of musical interaction. Several studies proposed more than one promising component. Three of the studies were not captured in any of the categories. Detailed information on the categories to which each study was allocated can be found in . The following six categories were formed:
Responsivity of the interaction partner: The most commonly noted promising component of musical interaction was the responsivity of the interaction partner (in 11/25, 44% of the studies). This involved the interaction partner listening, tuning in and following the child’s lead, as well as allowing pauses. The studies described how energy emanating from the interaction partner had the potential to motivate more responses from the child. Several studies highlighted that the level of stimulation had to be adjusted to the child’s mood and level of arousal.
Singing songs: Another commonly used and highly valued component of musical interaction involved singing songs (in 8/25, 32% of the studies). Using the names of participants and singing instructions were reported to motivate participation. Another benefit involved the naturally occurring repetition in songs, which could contribute to greater opportunities for learning skills such as greeting and making choices. The studies illustrated how pauses in songs acted as a cue for participants to become active and take the initiative.
Structure and predictability: Another component highlighted in the studies involved a set structure or framework for the musical interaction (in 8/25, 32% of the studies). This helped to identify and respond to children’s subtle communicative initiatives, and also encouraged and developed reciprocity between interaction partners. A flexible use of routines within a given structure was considered to support understanding and anticipation in the participants.
Long-term interventions: Long-term intervention periods were suggested in (6/25) 24% of the studies, due to long adaptation times, the time required to process information, small developmental steps, and the need for considerable time to establish a therapeutic alliance with the interaction partner. It was also argued that this benefited the interaction partner in terms of his/her ability to detect subtle changes or developmental steps in the child with S/PIMD, and to scaffold children’s interactions more effectively. Some of the studies also suggested more frequent musical-interaction activities (preferably several days a week), since these children take a long time to learn.
Technology-mediated and multisensory musical activities: (5/25) 20% of the studies described the potential of technology-mediated and multisensory musical activities or musical instruments to motivate children with S/PIMD to participate. These studies argued that the musical activities and instruments were motivating, providing different sensory experiences, and that they offered new opportunities for self-expression in children and young people whose physical limitations meant they had difficulties using traditional musical instruments.
Therapeutic alliance within the musical interaction: 5/25 (20%) of the studies described the essential role of the therapeutic alliance, or a well-established relationship with the interaction partner, in the success of the musical-interaction activities. A trusting relationship was considered to encourage better performance in the participants.
Quality appraisal
To address the final research question involving quality assessment of the studies, an adapted EBL-CAC was used to conduct a critical analysis of the included studies, as suggested by Van Keer and Maes (Citation2018). An overview of the results is provided in . Scores for each study can be provided by the first author on request.
Table 3. Quality appraisal, using an adapted EBL Critical Appraisal Checklist.
In a large majority (23/25, 92%) of the studies, the chosen study population was consistent with the population to which the conclusions applied. Inclusion/exclusion criteria were also clearly outlined in a large majority of the studies (21/25, 84%). The alternative ‘not applicable’ (N/A) was chosen for all the studies in items 1.3 and 1.4, as none of them claimed to be representative of the entire study population. Informed consent (from caregivers) was reported in (15/25) 60% of the studies.
The data collection methods were clearly described in a majority of the studies (18/25, 72%). The remaining studies were characterised by case descriptions where the data collection methods were not clearly described. Reliability testing was reported in (11/25) 44% of the studies, and information on the assessment instrument was included in (16/25) 64% of them. Only (2/25) eight percent of the studies used research instruments with a standardised administration format which had been subjected to psychometric evaluation, e.g. the Vineland adaptive behaviour scales (Sparrow et al. Citation2016). A majority of the studies (19/25, 76%) measured the intervention or musical-interaction activities at a time appropriate for capturing their effect according to the adapted EBL-CAC. However, it was not possible to determine this in studies characterised by short case descriptions.
In a majority of the studies (19/25, 75%) the methodology seemed appropriate according to the EBL-CAC guidelines. In the remaining studies the information was too limited. In (14/25) 56% of the studies, the level of detail was sufficient to allow the study to be replicated. Ethical approval was reported in (15/25) 60% of the studies.
In (21/25) 84% of the studies, outcomes were described and discussed in relation to the data collection and research questions. The results of 23/25 (92%) of the studies were considered to have been outlined clearly. Confounding variables were accounted for in (14/24) 56% of the studies. In (11/25) 44% of the studies, the conclusions were not fully reflected in the analyses presented. To comply with the criteria for external validity, selection of the study population, the methodology used and the results presented should be as bias-free, representative and transparent (Van Keer and Maes Citation2018) as possible. A flaw in at least one of these categories gave the study a ‘no’ score for external validity (4.6), and this was the case for all the studies.
Study origin
The studies included two based in Asia, five in the USA, four in Australia, seven in the UK and eight in Europe. A few were collaborations between researchers from different countries and continents, so that the total number was greater than 25.
Discussion
The aim of this study was to perform a scoping review of empirical research involving musical interaction with children and young people with S/PIMD, in order to provide guidance for research and practice. Peer-reviewed articles written in English were screened. A narrative synthesis was carried out to answer the research questions on participant characteristics, study designs and methods, abilities and behaviours in focus, reported benefits and promising components of musical-interaction activities. The included studies also underwent quality appraisal. Twenty-five articles were found which met the inclusion criteria between the years of 2000 and 2020. The research emanated from different countries and continents, with perhaps a small concentration to Europe and the UK.
Participant characteristics
In line with a heterogeneity of specific terms/nomenclature used in both research and clinical contexts, previously noted by Maes et al. (Citation2021), we also found a heterogeneity of specific terms used to describe the participant groups. In part, this could be because different countries use different terminologies to describe this group (Maes et al. Citation2021). For instance, in the UK, PMLD is the most commonly used term, whereas in several other parts of the world the term S/PIMD or PIMD is more commonly used (ibid). Since none of the studies in the current review used the term (S/)PIMD, it does not appear to be established among researchers in the fields of music or music therapy. Hence, it is important to use different terms to refer to the group when conducting systematic literature searches, in order to detect all available eligible studies. More generally, differences in the terminology can sometimes lead to ambiguous communication in both research and practical settings in terms of the level of functioning and (the very considerable) support needs of the individuals in question (Maes et al. Citation2021).
The largest sub-group of study participants, those with additional conditions, involved children and young people with Rett syndrome. This is a group with a known aetiology, and a relatively large body of research has been conducted with them in relation to music. The role of musical interaction for this group is also widely acknowledged in clinical contexts, as a means of developing social interaction, relatedness, communication and attention, and stimulating movement and motor abilities (Elefant Citation2001, Citation2002, Wigram and Elefant Citation2008, Bergström-Isacsson Citation2011). The second largest group involved a combination of severe or profound ID and ASD or ADHD. Similarly, the review by Brown and Jellison (Citation2012) highlights a relatively strong interest in children with ASD within the field of music therapy. They consider this interest to be due to a considerable increase in autism diagnoses in recent decades, and to reflect very considerable research interest in this group more generally, so that research on musical interaction is no exception in this regard. In a systematic Cochrane review on music therapy for people with ASD, Geretsegger et al. (Citation2014) demonstrated that music therapy was superior to standard treatment or placebo in terms of social interaction, communication, initiation and social-emotional reciprocity in people with autism (where the absolute majority did not have S/PIMD). There are no obvious indications in this review that musical interaction or music therapy is more beneficial for the subgroups of individuals with Rett syndrome or autism (combined with S/PIMD), compared with the benefits seen in the larger group with S/PIMD. However, this topic merits further examination.
Study designs
Children with S/PIMD are a heterogeneous group whose different functional limitations, comorbidities and abilities may lead to different developmental trajectories (Van Keer and Maes Citation2018). In combination with the low prevalence and great heterogeneity of subjects in the population, this may contribute to the dominance of descriptive case studies with a single or small sample size in the field. This is also reflected in this review. In fact, (15/25) 60% of the studies consisted of case-study designs, and (21/25) 84% had ten participants or fewer. Van Keer and Maes (Citation2018) noted that the data gathered from several experimental single-subject design studies can provide a knowledge base within the research field of S/PIMD, where large-scale samples are seldom feasible. In order to pool data from different studies statistically, the studies need to be sufficiently similar in terms of design, intervention and outcome measures. This was not the case in the studies we reviewed. As a consequence, we considered the studies individually and narratively presented some important themes and general conclusions. There were only three single-subject design studies (including a baseline/control condition) in the review, and only one experimental group design study. Van Keer and Maes (Citation2018) argue that more experimental single-subject experimental design studies would perhaps produce a cumulative generalisable knowledge base in terms of interventions and developmental outcomes for children and young people with S/PIMD. It is possible that this is also the case in the field of music therapy and musical interaction.
Data collection methods
Detailed video observations were the most commonly used data collection method. Since this group of participants is unable to self-report, observations are seen as a viable data collection method (Van Keer and Maes Citation2018). Nevertheless, we acknowledge that observational studies can be problematic in research with people with S/PIMD, since changes in behaviour may be very subtle, identifiable only by people who know the person well. Van keer and Maes have suggested that complementary assessment methods are preferred in terms of validating observational data, and these were applied in several studies. Examples include combining different data collection methods such as proxy-interviews, rating scales and surveys. The research instruments used had been constructed predominantly by the authors (9/25, 36%). Only (4/25) 16% of the studies used standardised tests or instruments which had been tested for their psychometric properties. It is worth noting that no specific assessment instruments were used in as many as (6/25) 24% of the studies. Waldon and Gattino (Citation2019) reported that, in general, tests and measures used in music therapy which have been tested for their psychometric properties are limited in number. In concordance with Waldon and Gattino, this review reflects a need for developing new measures and exploring psychometric properties in existing assessment instruments as they are applied in musical interaction with the S/PIMD population.
Types of musical-interaction activity
The present study used the term ‘musical interaction’ as an umbrella term to describe situations in which at least one child or young person with S/PIMD was involved in making music with a therapist, an educator or an interaction partner, with primarily non-musical goals. The majority of the musical-interaction activities used in the studies consisted of active music therapy. This was not unexpected, given that music therapy techniques used in practical settings since at least the late 1960s has had an active orientation, focusing on non-verbal communication, social relatedness and other non-musical goals (Wigram et al. 2002, Nordoff and Robbins Citation2007, Wheeler Citation2013). For example, the Nordoff Robbins Creative Music Therapy Model, one of the most established models for this population, is based on the conviction that all people, regardless of their disabilities, have an innate musical expression which can materialise as a result of supportive relations (Nordoff and Robbins Citation2007). The second largest group of musical-interaction activities involves technology-mediated and multisensory musical activities or instruments. Growing access to technology-mediated instruments within the field of music therapy and music education practices is apparent in an increasing number of studies, where the authors claim that technology-mediated musical instruments offer enriched participation (Stensaeth and Ruud Citation2014, Magee Citation2013). For participants with S/PIMD and severe motor disabilities, this will potentially provide new ways of expressing themselves musically, which are not fully accessible with traditional musical instruments. In (3/25) 12% of the studies, the multisensory elements in the musical activities were highlighted as benefiting the level of engagement and attentiveness in the participants. This is worth noting, since engagement and attentiveness are often considered important prerequisites for development and learning more generally (Carpenter et al. Citation2015, Mahoney et al. Citation2007), and are often reported to be low in people with S/PIMD (Munde et al. Citation2009). The extent to which the perceived usefulness or effectiveness of musical interaction is moderated by specific kinds of activity, the theoretical background of the approach, and the training and credentials of the interventionist were not fully addressed in this review. This would nevertheless be an interesting avenue for future studies in musical-interaction research generally, and when working with the S/PIMD group in particular.
Abilities and behaviours in focus
Not surprisingly, a majority of the studies focused on abilities and behaviours in the domain of social interaction and communication. Since this is a population with very limited means of communicating, it is of vital importance to know more about alternative avenues for communication such as musical interaction. Another large domain was ‘engagement, attention and affect’. As discussed previously, these behaviours are of major importance for development more generally (Carpenter et al. Citation2015, Mahoney et al. Citation2007), and thus very relevant in a population where low and fluctuating levels of attention and engagement are very often seen (Munde et al. Citation2009, Carpenter et al. Citation2015).
Reported benefits and promising components of musical-interaction activities
In terms of the reported benefits or effectiveness of musical interaction, all but one study considered it beneficial for the abilities and behaviours in question. However, as shown in the present study appraisal, only five of the studies which reported that the activities were effective had a control condition, so the results should be interpreted with caution. Six commonly shared categories were identified in the studies in terms of promising components of musical-interaction activities. The first category, involving responsivity of the interaction partner, was found in almost half of the studies. This is perhaps unsurprising considering that many of the musical-interaction activities were carried out by music therapists who are specifically trained to be attuned and attentive to the clients’ needs and ways of expressing themselves (Wigram et al. 2002). Furthermore, singing songs (category 2), provided a structured and predictable framework for musical interaction (category 3). Equally, long-term interventions (category 4) and establishing a therapeutic alliance between the interaction partners (category 6) were described as beneficial for both participation and development in children. In terms of singing songs, repetitive and motivational aspects were highlighted, including singing the participant’s name and using pauses to enable the participant to initiate. Furthermore, a set structure and long-term interventions were considered to enable the interaction partner to identify subtle developmental changes, and to scaffold the child more adequately. The categories are reflected in the four principles for meaningful relations through music, as suggested by McFerran and Shoemark (Citation2013): (i) the therapist listens attentively and (ii) takes responsibility for the structure, (iii) initiation is sought from the participant, and (iv) the relationship is built over time. As described earlier in this review, a considerable number of technology-mediated and multisensory musical activities and instruments (category 5) were used in musical-interaction activities. These were considered to provide the participants with enriched ways of expressing themselves musically, and to motivate and engage them in musical interaction. In sum, these are all important strategies that potentially can provide insights for future research with musical-interaction activities. Also, we believe that the findings could be of interest to practitioners working with music and children and young people with S/PIMD, e.g. therapists, teachers and direct-support staff, since the studies provide an initial summary of beneficial and evidence-based approaches and procedures which can be applied in everyday settings.
Quality appraisal
To assess the scientific quality of the studies, we used the adapted EBL-CAC (Van Keer and Maes Citation2018). The quality assessment revealed considerable heterogeneity in terms of study design, methods used, level of details reported and overall quality of the studies. The quality varied from poor validity (12%) to high validity (88%). None of the studies claimed to be representative of the entire population or free of bias in terms of participant selection/recruitment. Hence, the generalisability of the results should be interpreted with caution. There was only one between-group comparison study, in which study-group assignment was not randomised. There were a few studies with within-group (pre-post) comparisons.
In a quality appraisal, the choice of checklists clearly influences the outcome. Inevitably, certain values are assumed when it comes to scientific quality assessments, and the instrument we use tend to favour quantitative research procedures, including randomised controlled trials (RCT). In the research field of S/PIMD, large group studies or RCTs are seldom feasible (Van Keer and Maes Citation2018). In our quality appraisal, some of the studies using qualitative methods, e.g. detailed phenomenological descriptions of music therapist-client interactions, were given rather poor validity ratings. We nevertheless wish to highlight once again that the poor validity index is partially a result of the quality appraisal checklist rather than exclusively reflecting the actual quality of a study, and that many other qualities involving detailed and nuanced contextual understandings or therapeutic impressions may not be captured by the checklist ‘score’. Indeed, given the small number of studies within this research area, all studies could be seen as pioneering in a way. As noted earlier, if the data collection methods and analysis are presented transparently, the data gathered from several studies may be able to provide a cumulative knowledge base within a certain research field. For this to be possible, data collection methods and analyses need to be transparent and reported in sufficient detail to allow comparisons. Following Erkkilä (Citation2016), we suggest that qualitative, quantitative and mixed-method research are all needed to investigate different aspects of musical interaction with children and young people with S/PIMD.
Limitations, future directions and implications for practice
Many challenges are involved in research with children and young people with S/PIMD. For instance, data collection will mainly be dependent on observational studies and proxy reports, since the participants themselves are seldom able to self-report (though this can be feasible for some individuals with severe intellectual disability if alternative and augmentative communication techniques are used (e.g. Calculator Citation2009). Another identified challenge involves the lack of validated research instruments (e.g. evaluated for their psychometric properties) to assess this group of participants (Maes et al. Citation2021, Engelhardt et al. Citation2020). This is also reflected in this review. McFerran and Shanahan (Citation2011) highlighted yet another gap to address in further research, involving the need for research instruments which capture both musical and non-musical behaviours. Research instruments created within the field of musical interaction or music therapy should be used and tested by a number of researchers in order to ensure validity. Considering this situation, as well as the potential of musical-interaction activities for this vulnerable group, more creative research is called for.
This scoping review has mapped and critically reviewed the research on musical interaction and children and young people with S/PIMD. We have focused on musical-interaction activities in which two or more people are engaged in shared music-making. Pure receptive music therapy and listening to music were not targeted in this review. Since listening to (recorded) music is not an uncommon activity for people with S/PIMD, its possible benefits might be addressed in future research (Ford Citation1999). We hope that this review helps to identify promising areas of research as well as gaps in the literature. In terms of implications for practice, we specifically wish to emphasise the six categories identified for promising components of musical interaction, which could provide practical ways of engaging children and young people with S/PIMD in music education or therapy, as well as in leisure activities. Also, all but one study reported the benefits/effectiveness of musical interaction on the abilities or behaviours of interest. Thus, findings suggest that music therapy and musical-interaction sessions can improve a number of skills in children and young people with S/PIMD. Practitioners might also be inspired by certain methodological approaches in the research field. For instance, video recordings seem to be important tools in capturing subtle changes or progress in this population. While the quality of the evidence for musical interaction in not consistently strong, the findings highlight the importance of future research in this important area of knowledge.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Arksey, H. and O’Malley, L. 2005. Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8, 19–32.
- Arthur-Kelly, M., Foreman, P., Maes, B., Colyvas, K. and Lyons, G. 2018. Observational data on socio-communicative phenomena in classrooms supporting students with profound intellectual and multiple disability (PIMD): Advancing theory development on learning and engagement through data analysis. Advances in Neurodevelopmental Disorders, 2, 25–37.
- Axelsson, A. K., Granlund, M. and Wilder, J. 2013. Engagement in family activities: A quantitative, comparative study of children with profound intellectual and multiple disabilities and children with typical development. Child: Care, Health and Development, 39, 523–534.
- Azeredo, M. 2007. Real-time composition of image and sound in the (re)habilitation of children with special needs: A case study of a child with cerebral palsy. Digital Creativity, 18, 115–120.
- Bergström-Isacsson, M. 2011. Music and vibroacoustic stimulation in people with Rett syndrome: A neurophysiological study. Doctoral dissertation, Aalborg Universitet.
- Bindels-de Heus, K. G., van Staa, A., van Vliet, I., Ewals, F. V. and Hilberink, S. R. 2013. Transferring young people with profound intellectual and multiple disabilities from pediatric to adult medical care: Parents' experiences and recommendations. Intellectual and Developmental Disabilities, 51, 176–189.
- Wigram, T., Nygaard Pedersen, I. and Bonde L.O. 2002. A comprehensive guide to music therapy: Theory, clinical practice, research and training. London: Jessica Kingsley Publishers.
- Brown, L. S. and Jellison, J. A. 2012. Music research with children and youth with disabilities and typically developing peers: A systematic review. Journal of Music Therapy, 49, 335–364.
- Bunt, L. and Pavlicevic, M. 2001. Music and emotion: Perspectives from music therapy. In: P. N. Juslin and J. A. Sloboda, eds. Music and emotion. Theory and research. New York: Oxford University Press.
- Calculator, S. N. 2009. Augmentative and alternative communication (AAC) and inclusive education for students with the most severe disabilities. International Journal of Inclusive Education, 13, 93–113.
- Carpenter, B., Egerton, J., Cockbill, B., Bloom, T., Fotheringham, J., Rawson, H. and Thistlethwaite, J. 2015. Engaging learners with complex learning difficulties and disabilities: A resource book for teachers and teaching assistants. London: Routledge.
- Chou, M.-Y., Chang, N.-W., Chen, C., Lee, W.-T., Hsin, Y.-J., Siu, K.-K., Chen, C.-J., Wang, L.-J. and Hung, P.-L. 2019. The effectiveness of music therapy for individuals with Rett syndrome and their families. Journal of the Formosan Medical Association = Taiwan yi Zhi, 118, 1633–1643.
- DeBedout, J. K. and Worden, M. C. 2006. Motivators for children with severe intellectual disabilities in the self-contained classroom: A movement analysis. Journal of Music Therapy, 43, 123–135.
- Elefant, C. 2001. Speechless yet communicative: Revealing the person behind the disability of Rett syndrome through clinical research on songs in music therapy. In: D. Aldridge, G. DiFranco, E. Ruud and T. Wigram, eds. Music therapy in Europe. Rome: Ismez, pp.113–128.
- Elefant, C. 2002. Enhancing communication in girls with Rett syndrome through songs in music therapy. Doctoral dissertation, Aalborg University.
- Elefant, C. and Lotan, M. 2004. Rett syndrome: Dual intervention–music and physical therapy. Nordic Journal of Music Therapy, 13, 172–182.
- Elefant, C. and Wigram, T. 2005. Learning ability in children with Rett syndrome. Brain and Development, 27, S97–S101.
- Ellis, P. 2004. Vibroacoustic sound therapy: Case studies with children with profound and multiple learning difficulties and the elderly in long-term residential care. Studies in Health Technology and Informatics, 103, 36–42.
- Elo, S. and Kyngäs, H. 2008. The qualitative content analysis process. Journal of advanced nursing, 62, 107–115.
- Engelhardt, M., Krämer, T., Marzini, M., Sansour, T. and Zentel, P. 2020. Communication assessment in people with PIMD. Evaluating the use of the INSENSION Questionnaire–Longform (InQL). Psychoeducational Assessment, Intervention and Rehabilitation, 2, 1–14.
- Erkkilä, J. 2016. Mixed methods research in music therapy. In: J. Edwards, ed. The Oxford handbook of music therapy. New York: Oxford University Press, pp. 815–826.
- Ford, S. E. 1999. The effect of music on the self-injurious behavior of an adult female with severe developmental disabilities. Journal of Music Therapy, 36, 293–313.
- Geist, K., McCarthy, J., Rodgers-Smith, A. and Porter, J. 2008. Integrating music therapy services and speech-language therapy services for children with severe communication impairments: A co-treatment model. Journal of Instructional Psychology, 35, 311–316.
- Geretsegger, M., Elefant, C., Mössler, K. A. and Gold, C. 2014. Music therapy for people with autism spectrum disorder. Cochrane Database of Systematic Reviews, 6. Available from: https://doi.org/10.1002/14651858.CD004381.pub3 [Accessed 7 January 2021].
- Ghetti, C. M. 2002. Comparison of the effectiveness of three music therapy conditions to modulate behavior states in students with profound disabilities: A pilot study. Music Therapy Perspectives, 20, 20–30.
- Glynn, L. 2006. A critical appraisal tool for library and information research. Library Hi Tech, 24, 387–399.
- Go, T. and Mitani, A. 2009. A qualitative motion analysis study of voluntary hand movement induced by music in patients with Rett syndrome. Neuropsychiatric Disease and Treatment, 5, 499–503.
- Granlund, M., Wilder, J. and Almqvist, L. 2013. Severe multiple disabilities. In: M. Wehmeyer, ed. The Oxford handbook of positive psychology and disability. New York: Oxford University Press, pp.452–474.
- Griffiths, C. and Smith, M. 2016. Attuning: A communication process between people with severe and profound intellectual disability and their interaction partners. Journal of Applied Research in Intellectual Disabilities: JARID, 29, 124–138.
- Grocke, D. 2016. Receptive music therapy. In: J. Edwards, ed. The Oxford Handbook of Music Therapy. Oxford: Oxford University Press, pp. 684–706.
- Grocke, D. and Wigram, T. 2007. Receptive methods in music therapy: Techniques and clinical applications for music therapy clinicians, educators and students. London and Philadelphia, PA: Jessica Kingsley Publishers..
- Hackett, S., Morison, C. J. and Pullen, C. 2013. A retrospective practice based evaluation of music therapy: A single-case study of a four-year-old girl with Rett syndrome—Rebecca's story. The Arts in Psychotherapy, 40, 473–477.
- Holck, U. 2004. Interaction themes in music therapy: Definition and delimitation. Nordic Journal of Music Therapy, 13, 3–19.
- Jellison, J. A. 2000. A content analysis of music research with disabled children and youth (1975–1999): Applications in special education. In: American Music Therapy Association, ed. Effectiveness of music therapy procedures: Documentation of research and clinical practice. 3rd ed. Silver Springs, MD: The American Music Therapy Association, pp. 199–264.
- Kantor, J. 2020. “How well do i know you?”: Intersubjective perspectives in music therapy when working with persons with profound intellectual and multiple disability. In: Voices: A World Forum for Music Therapy, 20.
- Kossyvaki, L. and Curran, S. 2020. The role of technology-mediated music-making in enhancing engagement and social communication in children with autism and intellectual disabilities. Journal of Intellectual Disabilities: JOID, 24, 118–138.
- Kyngäs, H. 2020. Inductive content analysis. In: The application of content analysis in nursing science research. Cham: Springer, pp.13–21.
- Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., Clarke, M., Devereaux, P. J., Kleijnen, J. and Moher, D. 2009. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Medicine, 6, e1000100-28.
- Maes, B., Nijs, S., Vandesande, S., Van Keer, I., Arthur‐Kelly, M., Dind, J., Goldbart, J., Petitpierre, G. and Van der Putten, A. 2021. Looking back, looking forward: Methodological challenges and future directions in research on persons with profound intellectual and multiple disabilities. Journal of Applied Research in Intellectual Disabilities: JARID, 34, 250–262.
- Magee, W. L. 2013. Music technology in therapeutic and health settings. London: Jessica Kingsley Publishers.
- Magee, W. L., Bertolami, M., Kubicek, L., LaJoie, M., Martino, L., Sankowski, A., Townsend, J., Whitehead-Pleaux, A. M. and Zigo, J. B. 2011. Using music technology in music therapy with populations across the life span in medical and educational programs. Music and Medicine, 3, 146–153.
- Mahoney, G., Kim, J. M. and Lin, C. 2007. Pivotal behavior model of developmental learning. Infants & Young Children, 20, 311–325.
- Malloch, S. and Trevarthen, C. 2009. Communicative musicality. In: Exploring the basis of human companionship. New York: Oxford University Press.
- McFerran, K. and Shanahan, E. 2011. Music therapy practice in special education and children's hospice: A systematic comparison of two music therapists' strategies with three preadolescent boys. Music Therapy Perspectives, 29, 103–111.
- McFerran, K. S. and Shoemark, H. 2013. How musical engagement promotes well-being in education contexts: The case of a young man with profound and multiple disabilities. International Journal of Qualitative Studies on Health and Well-Being, 8, 20570.
- Meadows, T. 1997. Music therapy for children with severe and profound multiple disabilities: A review of literature. Australian Journal of Music Therapy, 8, 3.
- Mikkonen, K. and Kääriäinen, M. 2020. Content analysis in systematic reviews. In: The application of content analysis in nursing science research. Cham: Springer, pp.105–115.
- Munde, V. S., Vlaskamp, C., Ruijssenaars, A. J. J. M. and Nakken, H. 2009. Alertness in individuals with profound intellectual and multiple disabilities: A literature review. Research in Developmental Disabilities, 30, 462–480.
- Munn, Z., Peters, M. D., Stern, C., Tufanaru, C., McArthur, A. and Aromataris, E. 2018. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18, 1–7.
- Nakken, H. and Vlaskamp, C. 2002. Joining forces: Supporting individuals with profound multiple learning disabilities. Tizard Learning Disability Review, 7, 10–15.
- Nakken, H. and Vlaskamp, C. 2007. A need for a taxonomy for profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, 4, 83–87.
- Nielsen, J. B. and Holck, U. 2020. Synchronicity in improvisational music therapy – Developing an intersubjective field with a child with autism spectrum disorder. Nordic Journal of Music Therapy, 29, 112–131.
- Nordoff, P. and Robbins, C. 2007. Creative music therapy: A guide to fostering clinical musicianship. Gilsum: Barcelona Publishers.
- Nurjannah, I. and Siwi, S. M. 2017. Guidelines for analysis on measuring interrater reliability of nursing outcome classification. International Journal of Research in Medical Sciences, 5, 1169–1175.
- Ockelford, A. 2012. Commentary: Special abilities, special needs. In: The Oxford handbook of music education, Vol. 2. p.1.
- Ockelford, A., Welch, G., Jewell‐Gore, L., Cheng, E., Vogiatzoglou, A. and Himonides, E. 2011. Sounds of intent, phase 2: Gauging the music development of children with complex needs. European Journal of Special Needs Education, 26, 177–199.
- Oudshoorn, C. E., Frielink, N., Nijs, S. L. and Embregts, P. J. 2021. Psychological eHealth interventions for people with intellectual disabilities: A scoping review. Journal of Applied Research in Intellectual Disabilities.
- Perry, M. M. R. 2003. Relating improvisational music therapy with severely and multiply disabled children to communication development. Journal of Music Therapy, 40, 227–246.
- Phillips-Silver, J. and Keller, P. 2012. Searching for roots of entrainment and joint action in early musical interactions. Frontiers in Human Neuroscience, 6, 26.
- Raglio, A., Traficante, D. and Oasi, O. 2011. Autism and music therapy. Intersubjective approach and music therapy assessment. Nordic Journal of Music Therapy, 20, 123–141.
- Raglio, A., Zaliani, A., Baiardi, P., Bossi, D., Sguazzin, C., Capodaglio, E., Imbriani, C., Gontero, G. and Imbriani, M. 2017. Active music therapy approach for stroke patients in the post-acute rehabilitation. Neurological Sciences, 38, 893–897.
- Rensfeldt Flink, A., Åsberg Johnels, J., Broberg, M. and Thunberg, G. 2020. Examining perceptions of a communication course for parents of children with profound intellectual and multiple disabilities. International Journal of Developmental Disabilities, 1–12.
- Sparrow, S. S., Cicchetti, D. and Saulnier, C. 2016. Vineland adaptive behavior scales. 3rd ed. Circle Pines, MN: American Guidance Service.
- Stensaeth, K. 2013. "Musical co-creation"? Exploring health-promoting potentials on the use of musical and interactive tangibles for families with children with disabilities”? International Journal of Qualitative Studies on Health and Well-Being, 8, 20704.
- Stensaeth, K. and Ruud, E. 2014. An interactive technology for health: New possibilities for the field of music and health and for music therapy? A case study of two children with disabilities playing with ‘ORFI’.
- Stephenson, J. 2006. Music therapy and the education of students with severe disabilities. Education and Training in Developmental Disabilities, 41, 290–299.
- Tarvainen, S., Stolt, S. and Launonen, K. 2020. Oral language comprehension interventions in 1–8-year-old children with language disorders or difficulties: A systematic scoping review. Autism & Developmental Language Impairments, 5, 239694152094699.
- Thompson, G. A. and McFerran, K. S. 2015. Music therapy with young people who have profound intellectual and developmental disability: Four case studies exploring communication and engagement within musical interactions. Journal of Intellectual and Developmental Disability, 40, 1–11.
- Trevarthen, C. 2002. Origins of musical identity: Evidence from infancy for musical social awareness. In: R. A. R. MacDonald, D. J. Hargreaves and D. Miell, eds. Musical identities. Oxford: Oxford University Press, pp.21–38.
- Van Keer, I. and Maes, B. 2018. Contextual factors influencing the developmental characteristics of young children with severe to profound intellectual disability: A critical review. Journal of Intellectual & Developmental Disability, 43, 183–201.
- Waldon, E. G.and Gattino, G. 2019. Assessment in music therapy. Introductory Considerations. In: S. Lindahl Jacobsen, E.G. Waldon and G. Gattino, eds. Music therapy assessment: Theory, research, and application. London and Philadelphia: Jessica Kingsley Publishers, pp. 19–41.
- Welch, G., Ockelford, A., Carter, F. C., Zimmermann, S. A. and Himonides, E. 2009. Sounds of Intent: Mapping musical behaviour and development in children and young people with complex needs. Psychology of Music, 37, 348–370.
- Wheeler, B. L. 2013. Individuals with severe and multiple disabilities. In: Guidelines for music therapy practice in developmental health. Gilsum, NH: Barcelona, pp.399–440.
- Wheeler, B. L. and Stultz, S. 2008. Using typical infant development to inform music therapy with children with disabilities. Early Childhood Education Journal, 35, 585–591.
- Wigram, T. and Elefant, C. 2008. Therapeutic dialogues in music: Nurturing musicality of communication in children with autistic spectrum disorder and Rett Syndrome.
- Wigram, T. and Lawrence, M. 2005. Music therapy as a tool for assessing hand use and communicativeness in children with Rett Syndrome. Brain and Development, 27, S95–S96.
- Wimpory, D. C. and Nash, S. 1999. Musical interaction therapy-therapeutic play for children with autism. Child Language Teaching and Therapy, 15, 17–28.
- World Health Organization. 2018. International statistical classification of diseases for mortality and morbidity statistics (11th Revision). Available at: <https://icd.who.int/browse11/l-m/en> [Assessed 21 April 2021]
- Yasuhara, A. and Sugiyama, Y. 2001. Music therapy for children with Rett syndrome. Brain and Development, 23, S82–S84.
- Yin, R. K. 2014. Case study research design and methods. Thousand Oaks, CA: Sage.