
Abstract
Background: People with intellectual and multiple disabilities often fail to achieve constructive occupation independent of external supervision. Technology-aided intervention systems might be used as a way to help them achieve such a goal. Method: A new technology-aided system was assessed with four participants with moderate to severe intellectual disability and blindness or blindness and motor impairment. The system (a) allowed the participants to access music events and telephone calls through simple responses, and (b) provided the participants with timely activity step instructions (i.e. instructions tied to their response performance). The system was based on the use of a smartphone linked to a proximity sensor and was introduced according to a non-concurrent multiple baseline across participants design. Results: During baseline, the participants were not able to independently access music and telephone calls or perform activities. During the intervention sessions, they managed all three forms of occupation independently (i.e. with the technology system), remaining constructively active throughout the sessions. Their mean occupation time per session was 18-28 min and their percentage of correct activity steps was higher than 95. Conclusions: The new technology-aided system might be useful for helping people with intellectual and other disabilities manage basic forms of constructive occupation.
Introduction
People with moderate to severe intellectual disability often fail to manage constructive occupation independent of external supervision (Ashley et al. Citation2019, Channon Citation2014, King et al. Citation2022, Mahoney et al. Citation2016). Indeed, they may require external support to engage in functional occupational or vocational activities, to access leisure events, and to establish basic forms of social contact (communication) with distant partners (Desideri et al. Citation2021, Lancioni et al. Citation2019, Savage and Taber-Doughty Citation2017, Shepley et al. Citation2018a, Citation2018b). The situation may become even more problematic when intellectual disability is combined with visual or visual and motor impairments (Dijkhuizen et al. Citation2016, Jarjoura Citation2019, Lancioni et al. Citation2020a, Nair et al. Citation2022, Wachaja et al. Citation2017). Given the negative implications of this situation for the people involved and their context, there is consensus on the need to find strategies that could bring some benefits (Ayres et al. Citation2013, Desideri et al. Citation2021, Heider et al. Citation2019, Lancioni et al. Citation2017). It is clear that staff supervision may not be a viable long-term strategy due to its heavy cost on staff time and the fact that it might not necessarily build self-determination and independence (Desideri et al. Citation2021, Lancioni et al. Citation2018, Citation2020b, Moreno et al. Citation2021, OʼNeill et al. Citation2018).
In light of the above, technology-aided programs have been developed with the aim of providing people with a level of support sufficient to enable them to manage various forms of constructive occupation independent of staff (Cuturi et al. Citation2016, Golisz et al. Citation2018, Goo et al. Citation2019, Moreno et al. Citation2021, Randall et al. Citation2020). Most programs have focused on enabling people to carry out multistep activities through the use of instructions for the single activity steps (Desideri et al. Citation2021, Lin et al. Citation2018, Randall et al. Citation2020). Within those programs, participants (a) could be required to seek the instructions for each activity step through a response such a touching an iPad screen (Cannella-Malone et al. Citation2017, Savage and Taber-Doughty Citation2017, Shepley et al. Citation2018b), (b) could be automatically provided with instructions at preset time intervals (Desideri et al. Citation2021, Lancioni et al. Citation2020a, Citation2020b), and (c) could also receive instructions tied to their responding (Lancioni et al. Citation2021, Lin et al. Citation2018, Mihailidis et al. Citation2016). For example, Lin et al. (Citation2018) adopted the last type of instruction approach by using two dance pads in front of two desks each containing a computer. When a participant stood on the first dance pad, the computer on the table in front of it presented a video clip illustrating the response of taking an object as well as the verbal instruction matching the video. When the participant moved to the second dance pad, the computer on the table in front of it presented a video of what to do with the object as well as the matching verbal instruction.
Other programs have attempted to simultaneously focus on different forms of constructive occupation such as leisure and functional activities (Lancioni et al. Citation2020a, Citation2020b) or leisure, communication with distant partners and functional activities (Lancioni et al. Citation2022a, Citation2022b). For example, Lancioni et al. (Citation2022a) developed a program relying on a smartphone with SIM card, Internet connection, Google account, and MacroDroid application, and mini voice recording devices. These devices contained specific verbal requests capable of activating the smartphone’s Google assistant and the participants were to use them to request leisure events and activate telephone calls. The program was set up to alternate periods in which the participants could access leisure and carry out telephone calls with periods in which the smartphone presented instructions for the performance of daily activities at preset time intervals.
The two groups of programs mentioned above were reported to be successful in helping participants to independently carry out multistep activities (Desideri et al. Citation2021, Lin et al. Citation2018) or to access leisure and communication, or to combine these options with multistep activities (Lancioni et al. Citation2020a, Citation2022a, Citation2022b). In spite of the encouraging results, those programs might not always be (easily) applicable. For example, programs such as that reported by Lin et al. (Citation2018) may not be suitable for participants who have blindness and/or motor impairment (Lancioni et al. Citation2020b, Nair et al. Citation2022, Wachaja et al. Citation2017). Programs such as that reported by Lancioni et al. (Citation2022a) might not be suitable for participants who present with moderate to severe intellectual disability and combinations of visual and motor impairments. These participants, for example, might have difficulties managing the responses required to select preferred leisure stimuli or preferred communication partners and might also have difficulties following activity step instructions delivered at preset time intervals. The latter difficulties might stem from the fact that the time the participants need for performing the step responses can vary within and across days making the preset intervals too short or too long (Lancioni et al. Citation2021).
The objective of this study was to set up an intervention program that would suit participants with moderate to severe intellectual disability and blindness or blindness and motor impairment (i.e. participants who could have difficulties using programs such as those described above). The new program was to (a) allow the participants to access leisure events and telephone calls through simple responses, and (b) provide the participants with activity step instructions tied to their response performance rather than at prefixed time intervals (Lancioni et al. Citation2021, Schlosser et al. Citation2016, Citation2017). In essence, the new program was a form of prosthetic tool serving to foster a level of independent performance that the participants’ condition could not ensure and to sustain such performance in a friendly manner (i.e. minimizing failure and frustration). An increased level of independent (program-mediated) performance free from frustration/failure was considered critically relevant for improving the participants’ personal and social outlook (Chang et al. Citation2022, Gentry et al. Citation2015, Lancioni et al. Citation2022a, Citation2022b). The program was based on the use of a smartphone linked to a proximity sensor via a Bluetooth interface. Four participants were involved in the study.
Method
Participants
The participants were four adults who are here identified with the pseudonyms of Willy, Adelyn, Frances, and Oliver (see ). They presented with intellectual disability and blindness. Three of them (Adelyn, Frances, and Oliver) also had severe motor impairment and used a wheelchair. Their chronological ages ranged from 43 to 51 years. Their age equivalents assessed via the second edition of the Vineland Adaptive Behavior Scales (Balboni et al. Citation2016, Sparrow et al. Citation2005) varied from 2 years and 8 months to 3 years and 1 month on daily living skills (personal subdomain), from 3 years and 8 months to 4 years and 3 months on receptive communication, and from 2 years and 1 month to 4 years and 1 months on expressive communication (see ). Communication occurred verbally. While no formal intelligence tests could be carried out with them (given their conditions), estimates of their intellectual functioning made by the psychological services of the centers they attended placed them in the moderate to severe intellectual disability range.
Table 1. Participants listed with their pseudonyms, chronological age, and Vineland age equivalents for daily living skills (personal Sub-domain) (DLSP), receptive communication (RC), and expressive communication (EC).
The participants were selected for the study based on a number of conditions. First, they enjoyed access to leisure events, such as music and songs, and were known to have clear preferences within this area. Second, they had positive social ties with some family and staff members who were not regularly available in their context and enjoyed contacting these members via telephone. Third, they could carry out basic activities such as placing series of objects into specific containers with the support of simple verbal instructions (i.e. they had the prerequisites for the activities to be carried out in this study). Fourth, they expressed willingness to use the support technology developed for this study that would help them access music and telephone calls and carry out simple activities. Fifth, staff (a) viewed the use of an intervention program aimed at helping the participants increase their independent engagement favorably and (b) considered the technology system (which was shown to them in advance) suitable for the participants and their context.
Ethical approval and informed consent
Prior to the study, all participants (a) had been introduced to the program’s content areas, that is, preferred music, telephone calls, and instructions for simple activity steps, and (b) had verbally signaled their interest in accessing those areas and thus being involved in the study. In spite of this apparent interest, the participants’ level of intellectual disability and inability to read and sign a consent form made it necessary for their legal representatives to be directly involved in the consent process. That is, the legal representatives were requested to read and sign the consent form on the participants’ behalf. The study complied with the 1964 Helsinki declaration and its later amendments and was approved by an institutional Ethics Committee.
Setting, sessions, activities, music stimuli, and research assistants
The participants’ regular context (i.e. quiet areas of the rehabilitation and care centers they attended) constituted the setting for the study. Baseline and intervention sessions were carried out for each participant individually. The participants received one or two sessions per day, 3 to 6 days a week. Each session contained three music stimulation sequences plus two combinations of music stimulation and a telephone call and four occupational activities considered functional for the participants within their rehabilitation context. Each activity consisted of distributing 10 objects into two kits of five (i.e. placing the objects into two bags and then placing the bags into a carton). The only exception was Willy who typically completed a kit of five objects and a kit of four objects. The types of objects to arrange into specific kits varied for different activities and across participants. For example, one activity could involve morning hygiene objects (e.g. toothpastes and toothbrushes) and cooking/kitchen items (e.g. salt and ketchup) or basic kitchen utensils (e.g. wooden spoon and fork).
The music stimuli consisted of instrumental pieces or songs, which were age-appropriate and familiar to the participants. They were selected following staff recommendation and a brief stimulus preference screening process. This process involved (a) the presentation of three 10-s segments of each song or instrumental piece for about 10 non-consecutive times and (b) the observation of the participants’ reactions to those presentations. A stimulus was considered preferred when the people carrying out the screening process (e.g. a research assistant and a staff member) agreed that the participants had a positive reaction (e.g. smiled or vocalized) on more than 50% of the segments’ presentations. Only stimuli considered preferred were used during the study. The research assistants were three psychology graduates who were familiar with people with disabilities, technology-aided programs, and data recording procedures.
Technology system
The technology system used during the intervention sessions involved a Samsung Galaxy smartphone with Android operating system, which was (a) linked via a Bluetooth Encore Plus interface (leonardoausili.com) to a proximity sensor (i.e. a Big Candy Corn, a triangle with a 9-cm side; leonardoausili.com), and (b) fitted with the MacroDroid application. This application served to program the smartphone’ functioning according to the intervention conditions and to assist in data recording as described below. (A copy of the program format used in this study is available from the authors.) The smartphone also contained (a) numerous pieces of preferred music (instrumental pieces or songs), which had been selected through stimulus preference screening, (b) a SIM card that allowed the participants to make telephone calls, (c) the telephone numbers of preferred communication partners (see Participants), and (d) recorded messages from those partners (that the smartphone could play whenever those partners did not answer a call).
At the start of an intervention session, the system verbally invited the participant to touch the smartphone. This was fixed at their chest and the participant was to touch a spongy circle that was pasted around the smartphone’s proximity sensor. This response led the system to deliver 30-40 s of preferred music (i.e. instrumental pieces or songs). At the end of this music period, the system invited the participant to touch the smartphone again for a new music period. This process was then repeated for a third time to complete the music sequence. Next, the system provided instructions for the performance of the first activity. The objects for the activity were in the first of the four boxes arranged on a sliding plane, at the right or left side of the desk at which the participant sat (see ).
Figure 1. The diagram shows the desk at which the participants sat during the sessions with (a) four boxes containing the objects for the activities, which were arranged on a sliding plane at the right side of the desk, (b) a bag in which the participants were to place the objects of a kit, (c) the carton in which the participants were to deposit each completed kit as well as each box once the objects available in it had been used, and (d) a Big Candy Corn sensor for detecting the participants’ responses.
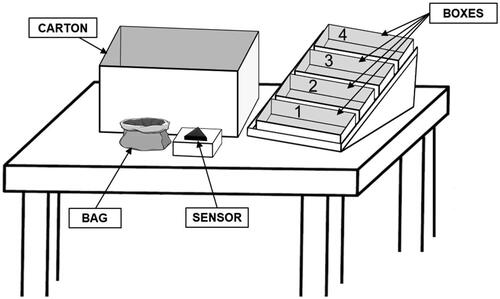
The right or left location of the boxes depended on whether the participant typically used the right or left arm/hand for responding. The system provided instructions for each activity step separately. The first instruction was to take a bag (i.e. a bag that was to be used for making the first kit). This was followed by the instructions of taking the objects to be placed in the bag/kit (one instruction at a time) and eventually by the instruction of putting the completed kit inside a carton just in front of the participant (see ). The sequence was repeated to complete and put away the second kit and the box from which the objects had been taken (i.e. the first of the four boxes). This last response made the second box with the objects for the second activity move downward in the sliding plane so as to get near the participant, ready for the participant to use. The interval between instructions was determined by the participant’s response performance. This was possible through the use of the Big Candy Corn sensor. In fact, the sensor was placed in a position that it would detect each participant response (i.e. each arm movement required for bringing an object to the bag; see ) as well as the arm lowering movement that followed the response of putting a kit or putting a box in the carton. Only after detecting the performance of a response, the system provided the instruction for the next response (instruction which could also be repeated at programmable intervals).
Once the first activity was completed, the system instructed the participant to touch the smartphone. This would lead to a 30-40 s music period. Following this period, the participant was to touch the smartphone again (independently or following the instruction). This time the system announced the start of a telephone call with one of the participant’s preferred partners. In case the partner being called did not answer, the system presented an audio recording of that partner containing greetings and encouragements. After the end of the call, the system instructed the participant to start the second activity (using the objects of the second box, which was now close to the participant). Following the end of the second activity, the participant had access to a new music sequence (i.e. three music periods) as at the beginning of the session. Subsequently, the system provided instructions for the third activity. This was followed by a new music period and a new telephone call (i.e. as after the first activity). Finally, the system presented instructions for the fourth activity and then the participant had access to a final music sequence.
Experimental conditions and data analysis
The technology system was introduced following a non-concurrent multiple baseline design across participants (Barlow et al. Citation2009). Initially, there was a baseline phase whose length changed across participants. During this phase, the technology system was not available. Thereafter, the intervention phase was implemented with the use of the system. Two precautions were taken to ensure high levels of procedural fidelity (Sanetti and Collier-Meek Citation2014). The first precaution consisted of having the research assistants practice their role (i.e. the implementation of the procedural conditions) prior to the start of the study, that is, during two simulated baseline and intervention sessions. The second precaution consisted of supervising the research assistants during the study. This was carried out via a study coordinator, who had access to video-recordings of the sessions and provided feedback and guidance to the research assistants to ensure their performance accuracy. The Kolmogorov-Smirnov test (Siegel and Castellan Citation1988) was scheduled for comparing the participants’ baseline and intervention performance regarding their session occupation time and correct activity steps (see the Measures and Data Recording section). In practice, however, the test was omitted given the large differences between the data of the two phases (Parker et al. Citation2011).
Baseline
During the 5 to 10 baseline sessions, the participants had a standard smartphone fixed at the chest and sat at a desk containing boxes with objects (see ). At the start of a session, the research assistant provided verbal or verbal and physical guidance to help the participants touch the smartphone screen in connection with a small sponge (which indicated the position of a music file). Touching (stroking) the screen near the sponge led to the start of music. After a few seconds, the music was interrupted and the research assistant (a) provided guidance to help the participants reach the objects in the first (closest) box, (b) told the participants that those objects were to be arranged into two bags, and (c) then, invited the participants to proceed with the music or the activity. If the participants failed to access music or perform correct activity steps for over 1 min, the research assistant provided guidance to start a 30- to 40-s music period. Thereafter, the research assistant repeated the invitation to proceed with music or activity. Failure to access music or perform correct activity steps for over 1 min led the research assistant to remove any objects on the desk, put away the first box, and guide the participant to touch the objects of the second box/activity. This was followed by an invitation to proceed with this new activity or music. Three additional guidance instances were available in the session. They were aimed at helping the participants access music, touch the objects of the next activity, and access music, respectively (i.e. according to the criteria described above).
Intervention
During the 70 to 101 intervention sessions, the participants sat at the same desk and with the same boxes with objects as during the baseline sessions. The difference was that the participants were now provided with the technology system. At the start of the sessions, the participants received via the system the instruction to touch the smartphone (i.e. the spongy ring around the smartphone’s proximity sensor). By doing so, the participants received 30 to 40 s of preferred music. The response was to be repeated, as three music periods were scheduled (see the Technology System section). Then, the system provided instructions for the first activity and monitored the participants’ responses (performance of the activity steps) through the Big Candy Corn sensor (see the Technology System section and ). After the participants had performed the responses related to the first set of objects to be arranged in the first kit, the smartphone provided the instruction of putting that kit in the carton in front. Then, it provided the instructions for completing the second kit, for putting the kit in the carton, and for putting the box in the carton. Following the completion of the activity, the participants were instructed to touch the smartphone. This led to 30-40 s of preferred music the first time and to the start of a telephone call with a preferred partner the second time. The end of the telephone call led to (a) the second activity followed by access to three music periods, (b) the third activity followed by access to a music period and a telephone call, and (c) the fourth activity followed by access to three music periods.
The intervention phase was preceded by 6 or 7 introductory sessions, in which the participants were to practice the use of the technology system and the activity responses. Initially, research assistants’ guidance was available to help the participants practice successfully. Then, it was gradually faded out. The fading process was to ensure that the participants managed to be independent of any guidance by the end of the introductory sessions. Following these introductory sessions, guidance was no longer available. An exception would occur only if the participants failed to remove a box correctly at the end of an activity and this prevented the sliding down of the next box with the objects needed for the next activity (see the Technology System section).
Measures and data recording
Two measures were recorded. The first measure was the session occupation time. This involved the sum of the session time spent performing the steps of the scheduled activities (regardless of whether those steps were correct or incorrect) plus the session time spent with independently accessed music and telephone calls. The second measure was the percentage of activity steps carried out correctly over the four activities. Those steps included all the objects placed in the kits where they belonged, the kits put in the carton after being completed, and the boxes put in the carton after the objects had been taken from them. The research assistants recorded both measures during the baseline and the second measure during the intervention. The recording of the first measure during the intervention was carried out via the MacroDroid application, which provided session logs with duration times for activities, stimulation periods, and telephone calls.
Interrater agreement on the data recorded by the research assistants was checked through the presence of a reliability observer during all baseline sessions and about 25% of the intervention sessions of each participant. The level of agreement on the first measure (computed for the baseline by dividing the number of sessions in which research assistant and reliability observer reported occupation times differing less than 1.5 min by the total number of baseline sessions, and multiplying by 100%) was 100%. The level of agreement on the second measure (computed through the study by dividing the sessions in which research assistant and reliability observer reported identical numbers of correct activity steps by the total number of sessions checked, and multiplying by 100%) was above 90% for all participants.
Results
summarizes the participants’ baseline and intervention data regarding the two measures. The black squares and empty triangles represent the mean occupation time (in minutes) and the mean percentage of correct activity steps per session over blocks of sessions, respectively. The blocks, which are used to simplify the graphic display of the results, contain two sessions during the baseline and four sessions during the intervention. Blocks with different numbers of sessions (i.e. at the end of the phases) are marked with a numeral. This indicates how many sessions the blocks include. The figure does not report the introductory sessions carried out at the start of the intervention phase.
Figure 2. The black squares and empty triangles represent the mean occupation time (in minutes) and the mean percentage of correct activity steps per session over blocks of sessions, respectively. The blocks include two sessions during the baseline and four sessions during the intervention. Blocks with different numbers of sessions (i.e. at the end of the phases) are marked with a numeral indicating the sessions included. The numbers in the boxes indicate how many sessions the participants received during baseline and intervention.
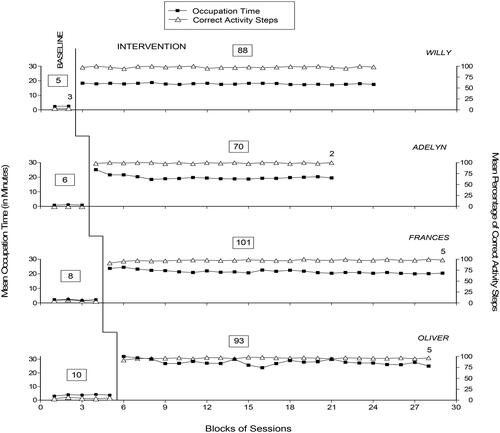
During the baseline, the participants’ mean session occupation time was below 5 min, as they did not manage to independently access music and only performed a few activity steps. Their mean percentage of correct activity steps was below 6. In light of this performance (i.e. dependence on research assistants’ guidance for music and minimal management of activity steps), the sessions were regularly interrupted (see the Baseline section).
During the intervention sessions (which followed the introductory sessions), the participants’ performance showed a clear change. In fact, they were able to use the technology system profitably and thus managed to access the music and telephone calls and perform the activity steps with the system’s support and independent of research assistants’ guidance. The occupation time averaged between 18 min (Willy) and 28 min (Oliver) per session. The mean percentage of correct activity steps was above 95 for all participants. Incorrect activity steps seemed to be mainly connected with difficulties in recognizing the objects or a tendency to respond rapidly, sometimes ignoring or misinterpreting the instructions.
Discussion
The results suggest that the technology system was adequate to support participants with moderate to severe intellectual disability, blindness and motor impairments enabling them to access preferred music and telephone calls and to perform simple occupational/vocational activities independent of staff support. In light of these results and of the outcome of previous studies focused on the development and use of technology-aided programs for people with intellectual and multiple disabilities, a few considerations may be put forward.
First, the technology system used in this study might be viewed as a practical and functional tool for a group of people who are not able to use or can only marginally benefit from previous programs available in the area (Lancioni et al. Citation2022a, Citation2022b, Lin et al. Citation2018, Nair et al. Citation2022). These people, for example, may not be able to consistently and independently seek instructions for the single steps of complex tasks (as required by some of those programs; e.g. Cannella-Malone et al. Citation2017, Savage and Taber-Doughty Citation2017, Shepley et al. Citation2018b) given their limited initiative and attention (Desideri et al. Citation2021). Similarly, they might have some difficulties using instructions provided at fixed intervals (as envisaged by some other programs; Lancioni et al. Citation2020a, Citation2020b) because of the time variations in their response performance. They may also be unable to manage complex response sequences to access preferred music or call preferred communication partners as required by existing programs (Lancioni et al. Citation2022a, Citation2022b).
Second, managing independent access to leisure events, basic forms of communication, and functional occupational activity may be considered a meaningful achievement for people with intellectual disability, blindness and motor impairment (Chokron et al. Citation2020, Evenhuis et al. Citation2009, Lancioni et al. Citation2022a). Typically, the aforementioned combination of disabilities prevents people from mastering such an achievement and drastically reduces their personal perspectives and outlook in life. The possibility of subverting their outlook through the use of a simple technology system might be viewed as a new opportunity also for care and rehabilitation contexts. The use of the system, in fact, may not be too demanding in terms of staff time and thus could prove viable and realistic for those contexts (Chang and Huang Citation2022, Gentry et al. Citation2015, Lancioni et al. Citation2017, Citation2020a, Citation2020b).
Third, the system reported might be viewed as friendly to the participants given the presence of timely instructions to support their performance of the activity steps and the availability of music and telephone calls. Instructions tied to the participants’ responses may be important to facilitate responding and limit uncertainty and frustration (Desideri et al. Citation2021, Lancioni et al. Citation2021). Music was judged to be a pleasant event that could foster enjoyment and motivation to remain engaged throughout the sessions (Kazdin Citation2012, Pierce and Cheney Citation2017). Telephone calls offered the participants an occasion of positive social-emotional interaction with their preferred communication partners and thus were thought to increase the participants’ session enjoyment (Lancioni et al. Citation2023).
Fourth, the fact that the system’s components are easily accessible and largely affordable might increase its suitability for daily contexts (Boot et al. Citation2018, Borg Citation2019, Desmond et al. Citation2018, De Witte et al. Citation2018, Federici and Scherer Citation2017). Indeed, the smartphone, the proximity sensor (i.e. Big Candy Corn), the Bluetooth Encore Plus interface, and the MacroDroid application are all commercially available and have a total cost ranging around US$500. Setting up the system for use within a daily context, albeit not particularly complex, will require staff familiarity with the MacroDroid application and its working rules. The availability of the program format used in this study (see the Technology System section) might be helpful for staff with more limited experience in the area.
Limitations and future research
The two most obvious limitations of the study concern the involvement of a small number of participants and the lack of a social validation of the system. The first limitation prevents one from making general statements about the overall effectiveness of the intervention system and possible implications of the results. To counter this limitation, new research will need to extend the number of participants involved in direct and systematic replication studies, which may also entail an assessment of the system’s maintenance and generalization effects (Kazdin Citation2011, Citation2012, Locey Citation2020, Travers et al. Citation2016). The outcome of those studies would provide the necessary evidence to determine the potential role of the system in future work with people with intellectual, visual and motor disabilities. The second limitation prevents one from making statements as to the perception that staff and other stakeholders may have about the system suitability for use in daily contexts. The assessment of this perception, which is important to understand the acceptability and applicability of the system, might be carried out through interviews of staff and other rehabilitation personnel and service providers (Plackett et al. Citation2017, Worthen and Luiselli Citation2019). The interviews could consist of (a) showing all these persons videos of intervention sessions involving the use of the system and (b) asking the same persons to rate the system in terms of effectiveness and overall applicability.
In conclusion, the results suggest that the system used in the present study might be helpful to support people with intellectual, visual and motor disabilities in accessing music and telephone calls and carrying out functional occupational activities. Although promising, the results are to be taken with caution given the aforementioned limitations of the study and the need for new research and more extensive and solid evidence about the impact and suitability of the system.
Compliance with ethical standards
Author contributions
GL was responsible for setting up the study, acquiring and analyzing the data, and writing the manuscript. NS, MO, and JS collaborated in setting up the study, analyzing the data, and writing/editing the manuscript. GA and MS contributed in evaluating and arranging the technological aspects of the study, acquiring and analyzing the data, and editing the manuscript.
Ethical approval
The study was approved by an institutional Ethics Committee. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
The participants’ legal representatives provided written informed consent for the participants’ involvement in the study.
Disclosure statement
The authors declare that they have no conflicts of interest.
Data availability
Data not available publicly.
References
- Ashley, D., Fossey, E. and Bigby, C. 2019. The home environments and occupational engagement of people with intellectual disabilities in supported living. British Journal of Occupational Therapy, 82, 698–709.
- Ayres, K. M., Mechling, L. and Sansosti, F. J. 2013. The use of mobile technologies to assist with life skills/independence of students with moderate/severe intellectual disability and/or autism spectrum disorders: Considerations for the future of school psychology. Psychology in the Schools, 50, 259–271.
- Balboni, G., Belacchi, C., Bonichini, S. and Coscarelli, A. 2016. Vineland II. Vineland adaptive behavior scales. 2nd ed. Firenze: Standardizzazione Italiana, OS.
- Barlow, D. H., Nock, M. and Hersen, M. 2009. Single-case experimental designs. 3rd ed. New York: Allyn & Bacon.
- Boot, F. H., Owuor, J., Dinsmore, J. and MacLachlan, M. 2018. Access to assistive technology for people with intellectual disabilities: A systematic review to identify barriers and facilitators. Journal of Intellectual Disability Research : Jidr, 62, 900–921.
- Borg, J. 2019. Commentary on selection of assistive technology in a context with limited resources. Disability and Rehabilitation. Assistive Technology, 14, 753–754.
- Cannella-Malone, H. I., Chan, J. M. and Jimenez, E. D. 2017. Comparing self-directed video prompting to least-to-most prompting in post-secondary students with moderate intellectual disabilities. International Journal of Developmental Disabilities, 63, 211–220.
- Chang, T. Y. and Huang, S. W. 2022. Factors influencing the reputation of assistive technology resources center: An example from Yunlin County, Taiwan. Healthcare (Basel, Switzerland), 10, 243.
- Channon, A. 2014. Intellectual disability and activity engagement: Exploring the literature from an occupational perspective. Journal of Occupational Science, 21, 443–458.
- Chokron, S., Kovarski, K., Zalla, T. and Dutton, G. N. 2020. The inter-relationships between cerebral visual impairment, autism and intellectual disability. Neuroscience and Biobehavioral Reviews, 114, 201–210.
- Cuturi, L. F., Aggius-Vella, E., Campus, C., Parmiggiani, A. and Gori, M. 2016. From science to technology: Orientation and mobility in blind children and adults. Neuroscience and Biobehavioral Reviews, 71, 240–251.
- De Witte, L., Steel, E., Gupta, S., Delgado Ramos, V. and Roentgen, U. 2018. Assistive technology provision: Towards an international framework for assuring availability and accessibility of affordable high-quality assistive technology. Disability and Rehabilitation. Assistive Technology, 13, 467–472.
- Desideri, L., Lancioni, G., Malavasi, M., Gherardini, A. and Cesario, L. 2021. Step instruction technology to help people with intellectual and other disabilities perform multistep tasks: A literature review. Journal of Developmental and Physical Disabilities, 33, 857–886.
- Desmond, D., Layton, N., Bentley, J., Boot, F. H., Borg, J., Dhungana, B. M., Gallagher, P., Gitlow, L., Gowran, R. J., Groce, N., Mavrou, K., Mackeogh, T., McDonald, R., Pettersson, C. and Scherer, M. J. 2018. Assistive technology and people: A position paper from the first global research, innovation and education on assistive technology (GREAT) summit. Disability and Rehabilitation. Assistive Technology, 13, 437–444.
- Dijkhuizen, A., Hilgenkamp, T. I., Krijnen, W. P., van der Schans, C. P. and Waninge, A. 2016. The impact of visual impairment on the ability to perform activities of daily living for persons with severe/profound intellectual disability. Research in Developmental Disabilities, 48, 35–42.
- Evenhuis, H. M., Sjoukes, L., Koot, H. M. and Kooijman, A. C. 2009. Does visual impairment lead to additional disability in adults with intellectual disabilities? Journal of Intellectual Disability Research : Jidr, 53, 19–28.
- Federici, S. and Scherer, M. J. (Eds). 2017. Assistive technology assessment handbook. 2nd ed. London, UK: CRC Press.
- Gentry, T., Kriner, R., Sima, A., McDonough, J. and Wehman, P. 2015. Reducing the need for personal supports among workers with autism using an iPod Touch as an assistive technology: Delayed randomized control trial. Journal of Autism and Developmental Disorders, 45, 669–684.
- Golisz, K., Waldman-Levi, A., Swierat, R. P. and Toglia, J. 2018. Adults with intellectual disabilities: Case studies using everyday technology to support daily living skills. British Journal of Occupational Therapy, 81, 514–524.
- Goo, M., Maurer, A. L. and Wehmeyer, M. L. 2019. Systematic review of using portable smart devices to teach functional skills to students with intellectual disability. Education and Training in Autism and Developmental Disabilities, 54, 57–68.
- Heider, A. E., Cannella-Malone, H. I. and Andzik, N. R. 2019. Effects of self-directed video prompting on vocational task acquisition. Career Development and Transition for Exceptional Individuals, 42, 87–98.
- Jarjoura, W. 2019. Disorientation and loss of wayfinding in individuals with congenital blindness and other affecting comorbidities. British Journal of Visual Impairment, 37, 240–247.
- Kazdin, A. E. 2011. Single-case research designs: Methods for clinical and applied settings. 2nd ed. New York: Oxford University Press.
- Kazdin, A. E. 2012. Behavior modification in applied settings. 7th ed. New York: Waveland Press.
- King, E., Brangan, J., McCarron, M., McCallion, P., Bavussantakath, F. R. and O'Donovan, M.-A. 2022. Predictors of productivity and leisure for people aging with intellectual disability. Canadian Journal of Occupational Therapy. Revue Canadienne D'ergotherapie, 89, 135–146.
- Lancioni, G. E., O’Reilly, M. F., Sigafoos, J., Alberti, G., Tenerelli, G., Ricci, C., Marschik, P. B. and Desideri, L. 2021. Tying the delivery of activity step instructions to step performance: Evaluating a basic technology system with people with special needs. Advances in Neurodevelopmental Disorders, 5, 488–497.
- Lancioni, G. E., Olivetti Belardinelli, M., Singh, N. N., O'Reilly, M. F., Sigafoos, J. and Alberti, G. 2019. Recent technology-aided programs to support adaptive responses, functional activities, and leisure and communication in people with significant disabilities. Frontiers in Neurology, 10, 643.
- Lancioni, G. E., Singh, N. N., O’Reilly, M. F., Sigafoos, J., Alberti, G., Campodonico, F. and Desideri, L. 2022a. A smartphone-based program enabling people with intellectual and other disabilities to access leisure, communication, and functional activities. Universal Access in the Information Society, 22, 581–590.
- Lancioni, G. E., Singh, N. N., O’Reilly, M. F., Sigafoos, J., Alberti, G., Perilli, V., Zimbaro, C., Chiariello, V. and Campodonico, F. 2018. Supporting leisure and functional activity engagement in people with multiple disabilities via a technology-aided program. Technology and Disability, 29, 173–181.
- Lancioni, G. E., Singh, N. N., O’Reilly, M. F., Sigafoos, J., Boccasini, A., Perilli, V. and Spagnuolo, C. 2017. Persons with multiple disabilities manage positive leisure and communication engagement through a technology-aided program. International Journal of Developmental Disabilities, 63, 148–157.
- Lancioni, G. E., Singh, N. N., O’Reilly, M. F., Sigafoos, J., Grillo, G., Desideri, L., Alberti, G. and Campodonico, F. 2020b. A new tablet-based program to support leisure and video calls in people with intellectual and motor disabilities. Technology and Disability, 32, 111–121.
- Lancioni, G. E., Singh, N. N., O'Reilly, M. F., Sigafoos, J., Alberti, G., Chiariello, V. and Carrella, L. 2020a. Everyday technology to support leisure and daily activities in people with intellectual and other disabilities. Developmental Neurorehabilitation, 23, 431–438.
- Lancioni, G. E., Singh, N. N., O'Reilly, M. F., Sigafoos, J., Alberti, G., Chiariello, V., Desideri, L. and Buono, S. 2023. Low-cost technology-aided programs for supporting people with motor, visual, and intellectual disabilities in functional forms of occupation and communication: Proof-of-concept study. JMIR Rehabilitation and Assistive Technologies, 10, e44239.
- Lancioni, G. E., Singh, N. N., O'Reilly, M. F., Sigafoos, J., Alberti, G. and Fiore, A. 2022b. People with intellectual and multiple disabilities access leisure, communication, and daily activities via a new technology-aided program. Frontiers in Psychology, 13, 994416.
- Lin, M. L., Chiang, M. S., Shih, C. H. and Li, M. F. 2018. Improving the occupational skills of students with intellectual disability by applying video prompting combined with dance pads. Journal of Applied Research in Intellectual Disabilities : Jarid, 31, 114–119.
- Locey, M. L. 2020. The evolution of behavior analysis: Toward a replication crisis? Perspectives on Behavior Science, 43, 655–675.
- Mahoney, W. J., Roberts, E., Bryze, K. and Parker Kent, J. A. 2016. Occupational engagement and adults with intellectual disabilities. The American Journal of Occupational Therapy, 70, 7001350030p1–7001350030p6. doi:10.5014/ajot.2016.016576
- Mihailidis, A., Melonis, M., Keyfitz, R., Lanning, M., Van Vuuren, S. and Bodine, C. 2016. A nonlinear contextually aware prompting system (N-CAPS) to assist workers with intellectual and developmental disabilities to perform factory assembly tasks: System overview and pilot testing. Disability and Rehabilitation. Assistive Technology, 11, 604–612.
- Moreno, M. T., Sans, J. C. and Colomina Fosch, M. T. 2021. Behavioral and cognitive interventions with digital devices in subjects with intellectual disability: A systematic review. Frontiers in Psychiatry, 12, 647399. doi:10.3389/fpsyt.2021.647399
- Nair, V., Olmschenk, G., Seiple, W. H. and Zhu, Z. 2022. ASSIST: Evaluating the usability and performance of an indoor navigation assistant for blind and visually impaired people. Assistive Technology, 34, 289–299.
- OʼNeill, B., Best, C., Oʼneill, L., Ramos, S. D. S. and Gillespie, A. 2018. Efficacy of a micro-prompting technology in reducing support needed by people with severe acquired brain injury in activities of daily living: A randomized control trial. The Journal of Head Trauma Rehabilitation, 33, E33–E41.
- Parker, R. I., Vannest, K. J. and Davis, J. L. 2011. Effect size in single-case research: A review of nine nonoverlap techniques. Behavior Modification, 35, 303–322.
- Pierce, W. D. and Cheney, C. D. 2017. Behavior analysis and learning. 6th ed. New York: Routledge.
- Plackett, R., Thomas, S. and Thomas, S. 2017. Professionals’ views on the use of smartphone technology to support children and adolescents with memory impairment due to acquired brain injury. Disability and Rehabilitation. Assistive Technology, 12, 236–243.
- Randall, K. N., Johnson, F., Adams, S. E., Kiss, C. W. and Ryan, J. B. 2020. Use of a iPhone task analysis application to increase employment-related chores for individuals with intellectual disabilities. Journal of Special Education Technology, 35, 26–36.
- Sanetti, L. M. H. and Collier-Meek, M. A. 2014. Increasing the rigor of procedural fidelity assessment: An empirical comparison of direct observation and permanent product review methods. Journal of Behavioral Education, 23, 60–88.
- Savage, M. N. and Taber-Doughty, T. 2017. Self-operated auditory prompting systems for individuals with intellectual disability: A meta-analysis of single-subject research. Journal of Intellectual & Developmental Disability, 42, 249–258.
- Schlosser, R. W., O’Brien, A., Yu, C., Abramson, J., Allen, A. A., Flynn, S. and Shane, H. C. 2017. Repurposing everyday technologies to provide just-in-time visual supports to children with intellectual disability and autism: A pilot feasibility study with Apple Watch. International Journal of Developmental Disabilities, 63, 221–227.
- Schlosser, R. W., Shane, H. C., Allen, A. A., Abramson, J., Laubscher, E. and Dimery, K. 2016. Just-in-Time supports in augmentative and alternative communication. Journal of Developmental and Physical Disabilities, 28, 177–193.
- Shepley, S. B., Ayres, K. M., Cagliani, R. and Whiteside, E. 2018b. Effects of self-mediated video modeling compared to video selfprompting for adolescents with intellectual disability. Education and Training in Autism and Developmental Disabilities, 53, 264–275.
- Shepley, S. B., Spriggs, A. D., Samudre, M. and Elliot, M. 2018a. Increasing daily living independence using video activity schedules in middle school students with intellectual disability. Journal of Special Education Technology, 33, 71–82.
- Siegel, S. and Castellan, N. J. 1988. Nonparametric statistics for the behavioral sciences. 2nd ed. New York: Macgraw-Hill.
- Sparrow, S. S., Cicchetti, D. V. and Balla, D. A. 2005. Vineland Adaptive Behavior Scales. 2nd ed. Vineland II, Minneapolis: Pearson.
- Travers, J. C., Cook, B. G., Therrien, W. J. and Coyne, M. D. 2016. Replication research and special education. Remedial and Special Education, 37, 195–204.
- Wachaja, A., Agarwal, P., Zink, M., Adame, M. R., Möller, K. and Burgard, W. 2017. Navigating blind people with walking impairments using a smart walker. Autonomous Robots, 41, 555–573.
- Worthen, D. and Luiselli, J. K. 2019. Comparative effects and social validation of support strategies to promote mindfulness practices among high school students. Child & Family Behavior Therapy, 41, 221–236.