
ABSTRACT
Healthcare systems are under pressure to control costs and improve performance. Efforts to apply improvement trends such as “Lean” and other industrial engineering approaches have led to degradation of the working environment for healthcare professionals. Research is increasingly demonstrating how poor working environments contribute to declines in care quality and has led to calls for a “quadruple aim” with a focus on the working environment alongside quality, cost, and patient experience factors. This paper contributes to the debate by using a “systems” perspective to propose seven strategies by which healthcare systems might be improved without compromising the working environment. This article presents a rationale for these strategies based on current organisational psychology and human factors research and how these strategies might be deployed in practice. The authors argue that better working conditions leads to better care for patients and presents a viable approach for both practitioners and researchers to pursue the “Better Work, Better Care” agenda.
1. Introduction
Healthcare systems (HCS) are under pressure to reduce costs and improve care quality while facing increased demands for service. In this context, HCS managers have begun drawing on industrial engineering techniques, such as “Lean” and “6-Sigma”, originally developed for manufacturing environments (Chassin, Citation2008; Costa & Godinho Filho, Citation2016; Trusko et al., Citation2003). Efforts to improve cost-efficiency in healthcare facilities have contributed to cutbacks resulting in increased mental and physical workloads for healthcare professionals (HCP) (Berry & St. Pierre, Citation2012; Westgaard & Winkel, Citation2011). In this article, HCP can include any paid health care provider, although we will frequently refer to nurses who pose the largest single category of HCPs in most healthcare systems (Nursing Task Force, Citation1999). Reviews have demonstrated that implementing “Lean” methodologies can result in poorer work environments and increased occupational health problems to realise short-term cost savings, thereby undermining the process improvement initiatives (Koukoulaki, Citation2014; Landsbergis et al., Citation1999; Holden, Citation2011; Westgaard & Winkel, Citation2011). Meanwhile, there is considerable evidence indicating that the quality of the work environment (WE; here defined broadly including here all physical and psychosocial aspects experienced by healthcare providers at work, per Neumann et al. (Citation2014)) affects the quality of patient care, patient safety, and patient satisfaction (Aiken et al., Citation2008; Carayon & Gürses, Citation2005; J. Needleman et al., Citation2006; Purdy et al., Citation2010). The World Health Organisation has highlighted the importance of healthcare worker wellbeing as a prerequisite to the delivery of high-quality care in their patient safety charter (WHO, Citation2020).
The issues of HCP wellbeing, HCS efficiency, and quality of care delivery are intertwined. Burnout in healthcare is widely reported, with over 50% of nurses reporting emotional exhaustion and burnout (Melnyk et al., Citation2020; Schuckhart, Citation2010). After working in pandemic conditions, burnout rates have exceeded 60% among nurses, physicians, and other HCPs in Canada (Maunder et al., Citation2021). Fatigue in employees has been found to have performance effects similar to alcohol intoxication (Dawson & Reid, Citation1997). Nurses working longer hours are much more likely to make errors (Australian Nursing Federation, Citation2009; Griffiths et al., Citation2014; Rogers et al., Citation2004; Stimpfel & Aiken, Citation2013). Eighty percent of nurses in the UK report working extra hours (Nurses, I.C.o, Citation2015). In Canada in 2017, nurses worked over 20 million hours of overtime – equivalent to 11,100 full-time HCPs (Canadian Federation of Nurses, Citation2017). The trend of increasing patient acuity also increases nurse workload (Daly & Brennan, Citation2009; MacPhee et al., Citation2017). Combined with inadequate staffing, this can increase injury rates and decrease care efficiency (Kalisch & Williams, Citation2009; Silas, Citation2015), also compromising the quality of care (Brennan et al., Citation2013; McGillis Hall & Visekruna, Citation2020; McGillis Hall et al., Citation2005; Rogers et al., Citation2004). Healthcare has one of the highest injury rates of all sectors (Bureau of Labor, Citation2011) and nurses absenteeism rates are almost double those of other HCS employees (Gormanns et al., Citation2011). Musculoskeletal disorders are a leading cause of nurses changing jobs (Trinkoff et al., Citation2003) and international surveys have shown that between 17% and 39% of nurses intend to leave their jobs within the next year due to physical and psychological demands. Critical nursing shortages are being experienced globally with a predicted shortage of 10.4 to 13 million nurses worldwide by 2030 (International Council of Nurses, Citation2020). While most of the literature here focuses on nurses, other HCPs are similarly affected by work overload and must be considered in improvement processes, including doctors (Wallace Citation2009; Chênevert et al., Citation2021; Elliott et al., Citation2014; Linzer et al., Citation2009), personal support workers (Braedley et al., Citation2018; Sayin et al., Citation2021), and other healthcare professionals (Rosted et al., Citation2021). This sample of the existing research demonstrates how the interactions between efficiency, HCPs’ work environments, and care quality are interlinked in complex ways. It sets the stage for the application of systems theory to help understand the problem and identify a viable approach to addressing the issue of improving HCSs in a more sustainable way. This article pursues sustainable work systems (Docherty et al., Citation2002) using a systems thinking approach to identify practical strategies for improvement.
Attempts have been made to integrate WE considerations into the quality improvement process by extending the triple aim (enhancing the care experience, improving health and reducing the costs of care) to a quadruple aim approach (improving the worker experience in providing care) (Bodenheimer & Sinsky, Citation2014; Committee, Citation2017). Several authors agree that enhancing the provider experience is the means by which other aims can be achieved (Bodenheimer & Sinsky, Citation2014; Privitera, Citation2018; Sikka et al., Citation2015). While there are legitimate concerns of overloading improvement teams with goals, we see that a failure to attend to WE in a deliberate way risks a further drift to unsafe states (c.f. Rasmussen, Citation1997) as teams fail to consider the negative impacts their changes on the HCP with secondary negative effects on patients and costs. The authors’ stance is that a high-quality work environment is the means to achieving quality care and can be advanced through other approaches, such as applying concepts of systems theory, rather than separating it out as an additional aim. This extends previous arguments that ergonomics and resulting employee well-being can be seen as a strategic means, or method for improvement, rather than as an immediate goal of the organisation (Dul & Neumann, Citation2009). Regardless of the label “goal” vs “means”, the practical advice is that all improvement or design efforts must account for WE aspects or risk compromising all goals for the HCS.
For supporters of a “quadruple” aim, the way in which the fourth aim is defined in the literature is inconsistent varying from finding joy in work, meaningful work, freeing up time to enable time for patient care, capacity building, and employee satisfaction (Association, Citation2017; Perlo et al., Citation2017; Research, Citation2021; Valaitis et al., Citation2020). Each of these definitions fails to acknowledge a comprehensive view of the work environment that considers all of the factors of a work system shown to impact work processes and work outcomes (Carayon et al., Citation2020; R. J. Holden et al., Citation2013). Using a systems approach to improving the work environment for healthcare professions, with an organisational approach to employee wellbeing and performance (Hendrick & Kleiner, Citation2001; Kleiner, Citation2006), can provide direction for organisations who seek to operationalise the aim of enhancing the provider experience in the delivery of care.
The aim of this paper is to present a set of seven interrelated strategies that can support managers and change agents in achieving sustainable improvements in healthcare delivery that result in improved working environments for the healthcare professionals affected, improved care quality and patient experience, while also attending to fiscal responsibilities. The article is organised as follows:
Section 2 presents a brief conceptual and theoretical framework that helps the reader understand the underlying systems theoretical rationale for the approach and how the strategies might operate in practice.
Section 3 describes the seven strategies for sustainable healthcare system improvement
Section 4, set in Text Box 1, provides an example of how the strategies might be deployed in a context sensitive way.
Section 5 Discusses the proposed strategies and addresses issues for future research in this arena.
We begin by examining the healthcare delivery system from a systems perspective.
2. Healthcare innovation needs a systems based approach
In 2014, the United States President’s Council of Advisors on Science and Technology called for a “systems engineering” approach to health care systems improvement efforts (PCAST, Citation2014). Despite this call, improvement efforts in HCS, we argue, are largely divided by goals: efforts to improve efficiency (Nicosia et al., Citation2018), efforts to improve quality (Goodman et al., Citation2018) and efforts to improve HCPs’ working environments (Paguio & Yu, Citation2020). The problem with this approach is that any change to the system has the potential to affect performance in all three (or four) domains of the system’s performance. A more integrated approach is therefore called for if a “systems” solution is to be achieved.
illustrates a critical feedback loop in HC systems that is central to the systems framework proposed here that illustrates how the design of the system (Left side - with key HCS design elements identified) will determine HCP workload in the system. This workload will have effects on the HCP as well as on the patient receiving the care. As workload begins to affect care quality and HCP wellbeing (for better or for worse), this will influence costs to the system (right side ). This view is consistent with the systems engineering model for patient safety (SEIPS) model of Carayon et al. (Citation2006) and its more recent updates (Holden & Carayon, Citation2021; Holden et al., Citation2013), that is one of the most comprehensive systems model for understanding healthcare systems performance and Human Factors. The current framework also draws on more design-oriented models that aim to illuminate the chain of cause and effect from design and management decisions, effects on those working in the system, and the effect their performance has on patient quality of care (Neumann & Village, Citation2012; Rose et al., Citation2013). This places the specific HCS design elements in focus as the leverage points for change in the system, while further emphasising the extended effects that design impacts on HCP will have on patient outcomes and system costs. Recognising the design of HCS explicitly in this model (left side ) also emphasises the presence of stakeholders who carry responsibility for, and influence over, these aspects in the creation and management of the healthcare delivery system that, when combined, result in a given workload and WE for HCP in operations ().
Figure 1. Systems model illustrating mechanisms of feedback by which HCP outcomes re-enter and affect care delivery operations and hence patient outcomes (adapted from Neumann & Dul, Citation2010; R. J. Holden et al., Citation2013). Arrows indicate lines of impact within the system, and illustrate the feedback loops that HCP and patient outcomes can have, positively or negatively, on the daily operations.
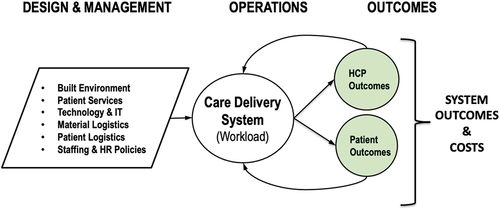
We note here (, left side) that the care delivery operations for example, a care unit in an acute hospital, are the product of many design and management decisions about the physical, technological, and organisational aspects of the care delivery system. Thus, the “patient services” (left side ) that define the nature of the care to be delivered according to patient needs and current medical practice, define the core tasks to be performed. Other design decisions, such as the architecture of the built environment, technologies in use, and operational considerations such as bed assignments and material supply strategies (intralogistics) will influence staff workloads required to deliver patient care. These decisions define the operational conditions of the given system (i.e., care unit) and also the working environment for HCPs. The WE will, in turn, affects HCPs in positive and negative ways. These effects on HCPs will then begin to affect the quality and quantity of care delivery, creating feedback in the system – a hallmark of systems thinking (Sterman, Citation2000). If, for example, HCP competency increases with work, then both quality and quantity of care will improve – a virtuous cycle. If excess workload causes HCP fatigue at work to increase, then the probability of error increases and the quality of care decreases (Cho & Steege, Citation2021; Cho et al., Citation2022). Errors in care delivery can have negative consequences for patients and require extra care tasks to ameliorate, which may further increase HCP fatigue levels – a vicious cycle with cost implications for the system (, right side). These feedback cycles are illustrated in the backwards linkages from HCP and patient outcomes into the care delivery system’s operations in . When pushed far enough, as we have seen from the inappropriate workloads on HCP caused by the COVID Pandemic (RNAO, Citation2022; Tomblin Murphy et al., Citation2022), staff begin to leave the profession leading to further staff shortages and loss of competencies, which will deepen the challenge of delivering high-quality care. Critical nursing staff shortages are now being experienced globally (McCarthy et al., Citation2020). , therefore, helps explain how changes in the design or circumstances of the care unit, left side , will affect HCPs and, ultimately, the quality and quantity of care provided in either positive or negative ways. This then, in turn, will affect system level financial outcomes (Right side of ).
One implication of is that efforts to improve quality or efficiency of care that inadvertently worsen the WE for HCPs will ultimately compromise their own goals as negative effects of work overload, in terms of fatigue, stress, or pain, begin to affect the system. This effect – in which anticipated performance improvements from an innovation are compromised by lack of attention to their human impacts – has been called the “innovation pitfall” (Neumann et al., Citation2021; Neumann, et al., Citation2018). and the innovation pitfall helps explain how a wide variety of process improvement efforts have been associated with declines in HCP health (Westgaard & Winkel, Citation2011). It also explains why efforts to improve the WE for HCPs lead to improved care quality and better patient outcomes (Nurses, Citation2007). , therefore, helps explain why WE needs to be considered in improvement work. Regardless of whether it is labelled a “goal” or a “means” - poor WE will compromise care quality and increase system costs.
Extending the call for “systems thinking” in HCS innovation, we draw on Sociotechnical Systems Theory (Skyttner, Citation2001) that recognises the criticality of interactions between the HC system and the people within it (Carayon, Citation2006; Cherns, Citation1976; Clegg, Citation2000). As the sociotechnical movement has shown, joint optimisation of system elements, particularly the human interaction aspects, is required for sustainable long-term improvement (Carayon et al., Citation2015; Eijnatten et al., Citation1993). In particular, we use Actor Network Theory (Kaghan & Bowker, Citation2001), an outgrowth of sociotechnical systems, that recognises the complex web of inter-relationships between different stakeholders (patients, nurses, doctors, cleaners, management, etc.) and technologies (e.g., IT systems and medical devices) within the system. The “actor network” helps describe the web of interactions between actors and technologies during regular operations. This is important in understanding the impacts that changes in one part of the system can have on others in the system – for better or for worse. For those engaged in process improvement in their organisations, there is only one operations system design (at the target unit or hospital level) - with one actor network implicated – to act on. There is not, for example, a separate care unit design for quality aspects and another design for cost aspects - the design of the unit affects all outcomes. All design changes can impact all outcomes. Any change in the system will also imply changes to the actor network within the system as each stakeholder is affected – therefore change efforts need to be sensitive to the actor network for successful, sustainable change (Broberg & Hermund, Citation2004; Kaghan & Bowker, Citation2001). Changes made to one part of the system may provide short-term benefits for one actor in the network, such as the patient, while also posing unexpected consequences to other actors, in this example increased nurse fatigue levels that may start to compromise the aims of the original innovation. Studies of safety-critical systems have shown that complex systems are prone to “drifting” into unsafe states as the various actors in the system try to make their own sub-system more efficient over time – with eventually catastrophic results for the system as a whole (Rasmussen, Citation1997, Citation2000). Participatory approaches can be one strategy for engaging the actor network in more robust improvement efforts (Abdullah et al., Citation2016) in order to avoid these innovation pitfalls. New computer modelling approaches are also helping clarify the interacting effects of specific design choices on HCP workload and care quality (Farid et al., Citation2020; Ibrahim Shire et al., Citation2018; Qureshi et al., Citation2019, Citation2020). These tools can integrate the available technical, patient, and policy information about the HCS design (left side ) and provide potential decision support tools helping designers and managers understand the effect of these features on the WE and on care quality over longer periods.
We now turn our attention to what a “systems” approach to HCS improvement might look like. When shifting to application, we note the importance of local context and the need to be sensitive to the current state of the system before proposing changes – a system theoretical insight. We do not therefore propose a specific “universal”, generalised recipe or method for change. Instead, we propose strategies for a context sensitive approach that can, and should, be adapted to the local and current situation for any given HCS or sub-system. There are a wide range of process improvement approaches that can be deployed within this strategic position (Karwowski, Citation2001; Salvendy, Citation2001). The approach recommended here is complementary to summaries for managing macro-ergonomic change in organisations (e.g., Holden et al., Citation2008). Here we emphasise first a set of seven core process improvement strategies for managers. We then provide a brief example (text Box 1) of a possible procedural approach by which the continuous improvement approach can be launched and managed as part of the ”better work, better care” framework.
3. Seven strategies for sustainable innovation in healthcare systems
The approach being proposed here is to draw on the industrial engineering toolkit and systems approaches while addressing a common “blind spot” in engineering approaches – a lack of attention to the human in the system (Broberg, Citation1997; Grosse et al., Citation2017; Neumann et al., Citation2021). The aim is to create a more human-centred HC innovation system that is sensitive to the local context. This addresses the “how” question emerging from calls for “systems engineering” approaches to HC with more holistic views of the process (e.g., Carayon, Citation2006; PCAST, Citation2014).
Seven interrelated strategic elements are suggested to help change managers choose and implement improvement approaches that yield innovation processes that result in sustainable health care system improvements that are not compromised by degraded work environments for staff:
Strategy #1: Set Integrated Goals combining objectives of care quality, cost-efficiency, the patient experience, and a healthy WE into a single innovation process. This is more efficient and yields more sustainable improvement than parallel mono-goal processes. Why, for example, deal with patient falls and HCP back injury (from trying to catch patients) separately, when these problems are linked? Similarly, changes to improve efficiency, by deploying “Lean” for example, may be counterproductive if they increase injury and absence rates in staff as found in systematic review (Westgaard & Winkel, Citation2011). Since any changes made in the healthcare process may potentially affect all three (or four) goals, proposed improvement efforts should address all system goals. Procedurally, integrated goals can also help build buy-in from a broader range of interests in the organisation through the mechanism of “Goal Hooking” (Poggi, Citation2005) which has shown in case research to help engage a broader range of actors than single-objective organisational change efforts (Village et al., Citation2015). Understanding the inter-relatedness of the “four aims” put forward under the “quadruple aim” banner (Bodenheimer & Sinsky, Citation2014), opens the door to simpler, more powerful improvement efforts. If the WE is understood as a precursor of, or even a necessary condition for (c.f. Dul, Citation2015), high-quality care then it becomes much easier to build supportive coalitions and coordinated improvement projects with integrated goals. In this view, the pursuit of HCP wellbeing may well be positioned as a means to achieving the triple aim, as much as a fourth (quadruple) aim in itself. Regardless of the theoretical or rhetorical positioning of WE as an end goal or as an intermediary constraint, we argue that every design and improvement project should include attention to all goals or risk compromised long-term results.
Separate projects for specific goals, such as cost-efficiency, will ultimately compromise performance as teams’ changes negatively impact other goals and will lead to system drifting to unsafe states (Rasmussen, Citation1997). In particular, efficiency-oriented change efforts that fail to attend to WE can lead to “brittle” systems that lack resilience (Woods, Citation2019), contribute to work-related ill health in HCP (Westgaard & Winkel, Citation2011) and can lead to dysfunctional side-effects referred to as the “innovation pitfall” in which expected performance gains are compromised by the effects of degraded working conditions (Neumann et al., Citation2021; Neumann, Citation2017, Citation2018). Managing this approach requires the use of indicators that allow verification of the full set of goals needed to achieve system-level improvements – our second core change strategy.
Strategy #2: Use Key Performance Indicators for all improvement domains. As the management adage goes: “You can’t manage what you don’t measure”. Here, in particular, we note a weakness in healthcare organisations to quantitatively manage staff workload levels when compared to the extensive measures of care quality and cost aspects (Neumann et al., Citation2018, Arsenault Knudsen et al., Citation2018; OECD, Citation2017). While cost aspects should be minimised, and quality aspects maximised, WE must instead find an optimal balance point of demands (Carayon, Citation2009) so as to avoid overloading or underloading healthcare staff (Jang et al., Citation2007). Quantitative indicators can help in this effort and should be meaningful, associated with clear, attainable, and realistic targets to provide a framework in which teams can design, evaluate, and verify proposed improvements (Ogbeiwi, Citation2017). Key performance indicators can include leading and lagging indicators across the model (; Greig et al., Citation2023) according to the needs and data available for a given project context should be chosen and regularly revisited and updated, so that the indicators are not being “gamed” within the process (Prather, 2005). For WE, in particular, there are many different dimensions of demand that may be of relevance. Possible indicators could include time demands to complete a task, biomechanical loads in task performance, or perceived mental workload and psychosocial conditions -, all of which can cause problems for both staff well-being and thus for the quality of care delivered (Carayon, Citation2011; Karwowski, Citation2001, Qureshi et al., Citation2021, Citation2020). In the absence of quantitative indicators of the WE, these aspects may be downplayed or ignored by system designers in the face of other quantitative performance specifications like cost (Greig et al., Citation2023; Wulff et al., Citation1999, Citation2000). Work in other sectors has shown that creating appropriate indicators for use in an organisational design process, can be difficult and may benefit from the support of specialists who can create measurement and indicator approaches that are appropriate for the particular process in focus (Village, Greig, Salustri, et al., Citation2014; Village, Greig, Zolfaghari, et al., Citation2014).
Strategy #3: Active Stakeholder Engagement including managers, inter-professional healthcare personnel and patient perspectives are critical. This strategy of organisational change (Holden et al., Citation2008; Oxtoby et al., Citation2002; Holden et al., Citation2013) is central to the concept of “Participatory Ergonomics” (Hignett et al., Citation2005) and “High Performance Work Systems” from the Human Resources discipline (Den Hartog et al., Citation2004; Harmon et al., Citation2003). Active engagement is seen as a critical element for organisational improvement (Hasle & Jensen, Citation2006; Zink et al., Citation2008) and a central tenet of participatory ergonomics (Noro and Imada, Citation1991). Any efforts at HCS change will need to address the needs of all stakeholders – including patients and HCP – but should also consider middle managers who are essential to the sustainability of change efforts (Abdullah et al., Citation2016). Similarly, other stakeholders like cleaners may be implicated in a given project (Xie et al., Citation2018), so change managers need to consider who to engage and when in their improvement programs. Including stakeholders broadly in the change process is an important mechanism for achieving successful and sustained process improvement as it draws on their knowledge while also building acceptance and understanding of the eventual design change. There are a range of tools available to support participation in the improvement process (e.g., Balbale et al., Citation2016; Hignett et al., Citation2005; Kuorinka, Citation1997). Regardless of the participatory methods chosen, systematically engaging users of a system design, in this case front-line staff and patients, should be an essential strategy of each improvement effort to ensure that the innovation does not compromise the experience of these key stakeholders. Those engaged in the process must have sufficient initiative to adapt the approach to the current situation to ensure the process is resilient enough to be adapted to the current needs (Woods, Citation2019). Engaging those who do the work also helps distinguish where the “work as done” may differ from the “work as imagined” by designers and managers (Braithwaite et al., Citation2016; Hollnagel & Clay-Williams, Citation2022) - a noted gap that participatory approaches can help close by drawing on local knowledge and communities of practice.
Strategy #4: Use A Human-Centred Design Thinking Approach drawing on the human factors discipline’s participatory impulses and deep understanding of human capability (Carayon, Citation2011; Haimes & Carayon, Citation1998). Human-centred design aims to make designs more usable by focusing on the needs of the people interacting with the design (Giacomin, Citation2014). This involves thinking closely about the needs and goals of stakeholders, the variety of conditions or scenarios under which those needs must be met and then considering how the possible combinations of design elements (i.e., see left side of ) interact to affect the experience of those in the system (Razzouk & Shute, Citation2012; Roberts et al., Citation2016). This applies to HCPs, patients, and families who, per the previous strategy, should be engaged in the design process. The Human Factors discipline provides tools to assess mental and physical workloads, error probabilities, and fatigue among other critical design aspects – which also support Strategy #2 (Carayon, Citation2011; Charlton & O’brien, Citation2002; Karwowski, Citation2001; Holden & Carayon, Citation2021; Stanton et al., Citation2004). These tools can help ensure that new processes do not overload the perceptual, cognitive, or physical capabilities of those in the system delivering care. Evaluation of possible system solutions can be conducted with a variety of simulation testing approaches including, for example, using simulation techniques that actively engage users (Strategy #3), such as “table-top” simulations (Abdullah et al., Citation2016; Andersen & Broberg, Citation2015) and mock-up simulation evaluations (Health Quality Council of Alberta, Citation2016; Shultz et al., Citation2019). New approaches to computer-based process simulation are also creating opportunities to test the effects of system changes on HCP workload and care quality in quantitative ways (per Strategy #2 - Qureshi et al., Citation2019, Citation2020, Citation2021). These approaches can provide useful information to support the design of improvements that meet the needs of both staff and patients. If the HCS innovation is not human-centred, it is unlikely to be safe and effective in the long term, compromising system sustainability.
Strategy #5: Foster “Organizational Learning”. Organizational learning refers to an organisation’s ability to take up and deploy new knowledge in order to improve their systems (Hasle & Jensen, Citation2006; Cummings, Citation2008; Ratnapalan & Uleryk, Citation2014; Senge, Citation1990; Tucker et al., Citation2007). HC organisations need to establish a culture of continuous learning – not just trying to do things faster, but also examining and refining the health care delivery process itself to find better ways to meet patient and family needs. Organizational learning perspectives that emphasise the ability to identify and improve work processes as a team (per Strategy #3) can help here (Easterby-Smith & Lyles, Citation2011; Mishra, Citation2018). Managers fostering organisational learning will need to consider a competency lens and develop a sense of “ambidextrousness” in the healthcare systems in which staff develop competencies to perform routine operational duties efficiently, on the one hand, and, on the other hand, to learn to engage effectively in the participatory development process in order to improve those care routines and processes (Helbin & Van Looy, Citation2021; Tushman & O’reilly, Citation1996). This implies a new set of change-process related skills and capabilities for those engaged in improvement work (Mishra, Citation2018; Purdy et al., Citation2017). Open access training resources have begun to emerge that can support the need to develop staff change competencies (Purdy et al., Citation2017). Organisational learning can be supported by drawing in the change competencies that may exist inside the organisation (internal expertise) and also by adapting (not just adopting) best practices for business process improvement approaches and system evaluation tools from outside the organisation (Brocke et al., Citation2014; Karwowski, Citation2001; Neumann & Village, Citation2012; Salvendy, Citation2001). Organisational learning can be achieved by helping hospitals to routinely apply key measures, proven methods, and scientific knowledge from Industrial Engineering and Human Factors toolkits combined with proven organisational development approaches (Neumann & Village, Citation2012; Neumann et al., Citation2012). Here too, stakeholders need to have the authority and initiative to adjust improvement procedures to their actual situation so as to ensure resiliency of the change approach (Woods, Citation2019) - a point we illustrate in the example process below (Text box 1).
Strategy #6: A Developmental Stance aiming to supplement (not supplant) current approaches in each hospital can help reduce the “adoption costs” of the innovation process and foster uptake by organisations as discussed in the “technology acceptance model” (Venkatesh & Davis, Citation2000). By evaluating and building on current routines – rather than trying to toss them out and install an unfamiliar and non-adapted change recipe – it becomes possible to build on current knowledge and efforts in a way that is meaningful to those engaged in the process. This also relates to the use of organisational learning perspectives (Strategy #4). An emphasis on building healthcare organisational capacity, rather than executing a researcher’s preconceived plan, can reduce resistance, leverage current knowledge, and also avoid the pitfalls associated with “n-step” programs that pre-specify methods and techniques (Collins, Citation1998). This lowers the cost of adoption of the approach – a barrier to adoption of innovation as noted in the Technology Acceptance Model (Holden & Karsh, Citation2010). The result is a more sustainable process at lower uptake cost than a forced external methodology.
This is a pragmatic approach that avoids trying to adopt a “perfect” (or popular) improvement method without accounting for the current knowledge and change competency level of the organisational unit in question. Change managers should be aware of the absorptive capacity limits of the organisation that may limit the rates of change (Neumann et al., Citation2009), and work within these boundaries to foster long-term change that is understood and supported by affected HCP. While new change methodologies and frameworks continue to emerge, managers are encouraged not to “let the perfect be the enemy of the good” (Buckle, Citation2010).
Strategy #7: Respect Local Priorities. This strategy is closely related to the developmental stance and is directed in particular to researchers and other external agents who may not be fully familiar with the local development needs. By letting the management steering group work on priorities of importance to them rather than, from an outsiders position, insisting that a specific problem or area of care be prioritised for improvement. This is another strategy, particularly important for external change agents like researchers who might not be aware of ongoing long-term planning in the organisation, to reduce start-up resistance and build manager support. Focusing on local priorities forms another “goal-hooking” strategy (Poggi, Citation2005) to align with the interests of other players in the organisational development arena, it has proven an important feature in our successful recruitment discussions with potential sites and industrial field research (Village, Greig, Salustri, et al., Citation2014; Village et al., Citation2014b). In this strategy ideas such as “best practices” should not be considered as absolutes but instead judged for suitability to the local context (Nat Natarajan, Citation2006). This has been articulated metaphorically by the adage “Horses for Courses” – based on the understanding that different change tactics, like different horses, succeed better depending on the context and situation at hand (Ghoshal & Nohria, Citation1993; Thomas & Fitter, Citation1997).
The Seven Strategy Set: The seven strategies presented here are neither exhaustive nor mutually exclusive. Instead, they are overlapping and mutually supportive approaches that the organisational change literature (Argyris, Citation1993; Badham, Citation2006; Collins, Citation1998; Holden et al., Citation2008; Oxtoby et al., Citation2002; Pettigrew et al., Citation2001) and our field experience suggests are helpful in initiating and sustaining organisational development processes. Managers and change agents in healthcare can deploy these strategies in a flexible way in order to be sensitive to their current context and avoid the “innovation pitfalls” that emerge with more single-goal programmatic approaches, such as has been observed with implementations of new technologies (Neumann et al., Citation2021; Neumann, Steege, et al., Citation2018) and “Lean” approaches (Westgaard & Winkel, Citation2011). Thus, the strategies noted here form a kind of strategic set that can be deployed in combination to achieve sustainable improvements while avoiding the “innovation pitfall” of presumed improvements that are compromised by degraded working environments or other unanticipated side-effects – which lies at the heart of the”Better Work better Care” framework.
4. Example of how strategies can be deployed
The strategies proposed here can be deployed in different ways according to the needs and context of the organisation. We encourage change agents to be creative and responsive in their situations to develop an approach that suits their needs. As an example, we place, in Text Box 1, a sketch of how an organisation might organise their improvement efforts in ways that capitalise on the proposed strategic elements for sustainable process improvement. There are other ways this “better work, better care” strategic framework might be successfully deployed, with the current illustration being but one example.
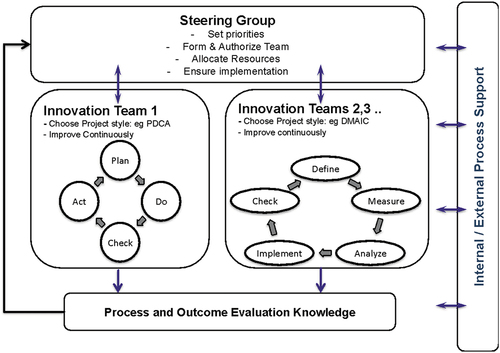
Text Box 1 - Example of a “Context Sensitive” approach for healthcare innovation using the proposed innovation strategies.
Figure 2. Illustrates the “double-loop” of learning in which Innovation teams are formed and engage in improvement cycles, while the leadership team monitors each cycle to examine outcomes and process effectiveness, to learn to better manage the improvement program.
5. Discussion
The proposed strategies for healthcare system design and improvement in the “Better Work, Better Care” framework, summarised in text box 2, explicitly try to overcome the problems associated with uncritical adoptions of engineering improvement methods that can have negative effects on HCP’s WE (Westgaard & Winkel, Citation2011) that can compromise care quality and cost-efficiency objectives. This approach to using better working conditions to achieve better care in HCS now requires implementation testing in real organisations. The set of strategies proposed here is consistent with the SEIPS model – the most widely promulgated human centred model in HCS research (Carayon et al., Citation2020). It is also consistent with the latest advice on organisational implementations from the organisational psychology field (von Thiele Schwarz et al., Citation2020). It is also aligned with current research in the area of Industry 4.0 and 5.0 trends where there is growing understanding that WE in operations will define performance – and that a failure to include WE considerations will lead to “phantom profits” in which expected gains are eroded by ill health and errors induced by poor WE (Neumann et al., 2022; Sgarbossa et al., Citation2020). We draw on these disciplines to propose both an action path forward and a research agenda by which HCs improvement efforts can achieve improvements in healthcare delivery processes that are sustainable from staff and financial perspectives, while providing the highest possible care quality for patients. While there is considerable writing on “change methods” and “tools” in the literature, the “Better Work Better Care” framework aims to expose the higher level – strategic - considerations that can help healthcare organisations improve their processes in ways that are not compromised by degraded WE for healthcare staff.
Text Box 2: Summary of strategies for the Better Work Better Care framework.
5.1. Research challenges
The strategic framework proposed here implies a range of research issues. Framed broadly one might ask: How can healthcare system designers and managers establish robust, systems level approaches to achieving high performing and cost-effective care systems that provide excellent care for patients and superior working environments for HCP? The deployment of the strategies and the specific approaches developed under these also warrant examination. This might usefully be pursued using, for example, realist evaluation stances (Pawson & Tilley, Citation1997; Salter & Kothari, Citation2014) that aim to understand what approaches work best under which specific contexts. Case studies using action research modes have been suggested as particularly helpful in studying organisational learning and approaches (Neumann & Village, Citation2012; Coghlan & Brydon-Miller, Citation2014) - although barriers to their use are noted below. These studies can examine the factors influencing the use of such system-based improvement approaches, advance theoretical understandings of how change processes can be fostered and managed in healthcare settings and can contribute to the development of context-specific methods and tools aimed at supporting the current and future case sites in deploying the integrated strategies proposed here. The adaptation of methods to the healthcare system, and particularly the challenges of quantifying workload aspects (Arsenault Knudsen et al., Citation2018; Neumann, Steege, et al., Citation2018), provide opportunities for useful research and development work. With a sufficient number of cases, cross-case comparisons and meta-analyses become possible – although the manager seeking to act on such knowledge should always consider the unique contexts of the people and systems in their particular actor network as the strategies presented here recommend.
The initial research question here is “How” can such a context sensitive improvement process best be initiated and supported? While “action research” type methodologies are a suitable way to study this problem from a close, embedded, position (Gustavsen, Citation2008; Reason & Bradbury, Citation2001; Sneyd & Rowley, Citation2004), these approaches require a shift from the paradigm of hypothesis testing, to one of learning from the experience of the process (Gustavsen, Citation2003a; Neumann et al., Citation2012). This approach to research can be resisted by researchers and reviewers trained in more traditional experimental evaluation methodologies (Greenwood, Citation2002; Neumann et al., Citation2012). While stronger, researcher-led evaluation techniques might be applied here, there is a risk that these methods leave the organisation in a dependency relationship and compromise the goal of having an independently functioning innovation process per the organisational learning strategy #5 (Toulmin & Gustavsen, Citation1996). Action Research represents a shift in research focus away from the summative “Does intervention X work?” to the formative question of how to drive improvement processes that integrate goals of quality, efficiency, the patient experience, and HCP wellbeing (Neumann et al., Citation2012).
Researchers working in this area, particularly those engaged in action research will face barriers that inhibit progress in this healthcare systems improvement agenda. These are discussed briefly next.
“That’s not science” – A barrier to developing the proposed approach lies with the research and health-science community who are well versed in experimental research approaches rooted in pharmacological studies like randomised controlled study designs. This community can be resistant to organisational science and macroergonomics approaches that are rooted in observational and developmental methods (Kleiner, Citation2006; Holden et al., Citation2015). This argument parallels the long-running and fruitless debate between the relative merits of quantitative vs. qualitative empirical evidence (C. Needleman & Needleman, Citation1996). While “evidence based” practice is useful for some patient care decisions, it can become a barrier to organisational innovation where highly adaptive and context-sensitive approaches are needed: what does “evidence” look like when every situation is unique? We argue that the evaluation of what works in their workplaces needs to be owned by the stakeholders themselves. Since the rate of organisational change such as the one described can be expected to take three or more years (Neumann et al., Citation2009; Village, Greig, Salustri, et al., Citation2014), studies of this approach must be sensitive to such long timelines. Under these circumstances, with complex and variable change approaches over a long period of time, longitudinal observational approaches such as action research methodologies become increasingly important. Such methods are better suited to answering the complex “How” questions of formative evaluation in complex systems compared to purely experimental study designs (Patton, Citation2011). Action research approaches can also usefully be used in theory generating to support future research and knowledge mobilisation efforts (e.g., Village et al., Citation2015). This is not to say that, inside the development process, specific experiments cannot be useful ways to answer very specific questions such as to determine the modes and probability of error when using a particular piece of equipment (Neumann et al., Citation2012). These questions that emerge “inside” the development process can, and indeed often should, be examined with quantitative experimental trials. The process of conducting such studies in the organisation could, itself, then be studied within the action research project.
Gaining buy-in for the development stance: It is ironic that the strength of this approach; the adaptive and context-sensitive nature of the improvement strategy creates a weakness in terms of the ability to pursue this agenda since the program can only be described in general terms. This leaves managers and funding proposal reviewers wondering “just what is going to be done?”. In contrast, it seems easier to sell very specific mono-goal improvement programs with explicit procedural elements, such as “Lean Production”, which are less likely to succeed in the long run since they do not respect local needs (Gustavsen et al., Citation1996, Citation2007) and they are prone to degrading HCP’s WE (Westgaard & Winkel, Citation2011). It is hoped that this articulation of the proposed framework will help build credibility for the context sensitive, systems-based approach we argue is needed for multidimensional and sustainable healthcare system improvement.
5.2. Implementation challenges for managers
“Boundary” problems are not just a challenge in research as conflicts arise between disciplinary views (as noted above), they are also an issue that must be managed with the organisation seeking improvements. The structural divisions within an organisation, such as the traditional separation into functional roles of human resources, care quality, and finance can be a problem as each function has separate aims. This can result in organisational “fiefdoms” that lead to mono-goal improvement activities (violating strategy #1) even though these domains interact and are driven by a singular design of operations in the healthcare organisation (Holden et al., Citation2011). This has resulted in situations where hospitals have multiple initiatives targeting the same issue. In one case, a hospital had simultaneous teams looking at patient falls from both a care quality perspective and, due to nurse injuries from trying to catch patients, from an occupational health and safety perspective. This exemplifies the lack of the kind of systems thinking that is currently being called for in the healthcare system (Carayon, Citation2011; PCAST, Citation2014; Holden et al., Citation2013) and can contribute to organisation fiefdoms where efforts to improve within each area interact to slowly drive the entire system towards unsafe states (Rasmussen, Citation1997, Citation2000). In our experience, creating cooperation across fiefdoms can be difficult in practice as actors attempt to preserve their own personal power and value their disciplinary frameworks above those of other stakeholders. This problem is not unique to healthcare organisations where organisational boundaries form barriers to cooperation that hinder organisational learning (Senge, Citation1990). Human factors have been suggested as a possible bridge to span this gap by contributing to multiple goals (Neumann & Dul, Citation2010) and case study research has shown this to be feasible in manufacturing settings (Village et al., Citation2015; Village, Greig, Salustri, et al., Citation2014). If an integrated improvement approach is to be established, then change agents will need to engage in organisational work (Theberge & Neumann, Citation2010), using the strategies outlined here, to gain buy and support from the individuals currently responsible for their individual goals of cost-control, care quality, the patient experience and employee’s working environments. Here again, organisational learning stances (Strategy #5) and change competency training (e.g., Purdy et al., Citation2017) can help develop common frames of reference needed for meaningful development. The use of key indicators that span WE, quality and cost dimensions inside every project, can help teams find appropriate balances when these aspects come into conflict within a project (per Strategy #2). This avoids the time and cost of having to correct problems that emerge from single goal initiatives that have negative secondary effects on other organisational goals.
5.3. Framework limitations
The strategic framework described here is, by necessity, limited. In the presentation of the current systems-based framework, a number of issues have not been discussed in detail. There is, for example, no discussion of how the knowledge gained in the change efforts in individual healthcare organisations should be gathered and applied within the design of new HC facilities. Although work is being done on helping ensure human factors knowledge and methods enter the design process (Broberg, Citation1997, Citation2010; Hall-Andersen & Broberg, Citation2014; Shultz et al., Citation2019), this work has not addressed the flow of knowledge from process improvement work into “greenfield” design processes in healthcare contexts. Similarly, there is good potential for the knowledge from change processes to be usefully shared across sites to create “innovation clusters” (Davis & Schaefer, Citation2003; Meng, Citation2005) in which different organisations learn from each other to leverage insights gained in each project. The current articulation has focused primarily on strategies at the organisational level with less attention paid to system dynamics beyond these institutional boundaries in order to establish an innovation system within a regional or international healthcare system. Such larger frames and perspectives would ultimately be helpful in supporting the application of human factors to reach a “critical mass” towards routine application in healthcare system design and improvement processes in which better working conditions for HCP allow for better care quality for patients.
6. Conclusions
Attention to the needs of HCP is an under-recognised element in the effort to improve cost-efficiency, care quality, and the patient experience – even though these elements are intertwined in healthcare systems. This paper provides a framework and macroergonomic approach for organising process improvement that addresses calls for a “systems” based approach to healthcare systems improvement. The core of this model is a realisation that the goals of cost control, high care quality, the patient experience, and good working environments are intertwined in the complex healthcare system. The underlying rationale of the “Better Work, Better Care” framework is that good working environments for HCPs are essential to control costs and ensure high quality of care for patients. Seven strategies are identified that can provide principled guidance in a systems-based approach to developing process improvement capacity: 1) integration of goals to include work environment aspects, 2) use of quantitative key performance indicators across goals, 3) active engagement of stakeholders in improvement processes, 4) using human centred design thinking approaches that are sensitive to stakeholder needs, 5) taking an organisational learning stance, 6) using a developmental approach sensitive to initial conditions, and 7) respecting local priorities within the system. This set of strategies work in concert to support the creation of sustainable healthcare system improvement approaches. An example of a context sensitive, adaptable approach to developing improvement capacity in healthcare systems is then presented. This strategic approach has the potential to overcome the risks of the “innovation pitfall” observed when goals are pursued separately or when systems orientations are ignored in healthcare system intervention efforts.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Abdullah, A., Deborah, M. R., Barbara, M. S., & Jana, R. (2016). The impact of middle management commitment on improvement initiatives in public organisations. Business Process Management Journal, 22(5), 924–938. https://doi.org/10.1108/BPMJ-01-2016-0018
- Aiken, L. H., Clarke, S. P., Sloane, D. M., Lake, E. T., & Cheney, T. (2008). Effects of hospital care environment on patient mortality and nurse outcomes. The Journal of Nursing Administration, 38(5), 223. https://doi.org/10.1097/01.NNA.0000312773.42352.d7
- Andersen, S. N., & Broberg, O. (2015). Participatory ergonomics simulation of hospital work systems: The influence of simulation media on simulation outcome. Applied Ergonomics, 51, 331–342. https://doi.org/10.1016/j.apergo.2015.06.003
- Anderson, S. N., & Broberg, O. (2016). A framework of knowledge creation processes in participatory simulation of hospital work systems. Ergonomics, 51, 1–17.
- Argyris, C. (1993). Knowledge for action. A guide to overcoming barriers to organisational change. Jossey-Bass.
- Arsenault Knudsen, É. N., Brzozowski, S. L., & Steege, L. M. (2018). Measuring work demands in hospital nursing: A feasibility study. IISE Transactions on Occupational Ergonomics and Human Factors, 6, 143–156. https://doi.org/10.1080/24725838.2018.1509910
- Autralian Nursing Federation. (2009). Ensuring quality, safety and positive patient outcomes. Autralian Nursing Federation. ISBN: 978-0-909599-56-0. https://anmf.org.au/documents/reports/Issues_Ensuring_quality.pdf
- Badham, R. J. (2006). Mudanças not removalists: rethinking the management of organizational change. Human Factors and Ergonomics in Manufacturing & Service Industries, 16, 229–245. https://doi.org/10.1002/hfm.20050
- Balbale, S. N., Locatelli, S. M., & LaVela, S. L. (2016). Through their eyes: Lessons learned using participatory methods in health care quality improvement projects. Qualitative Health Research, 26(10), 1382–1392. https://doi.org/10.1177/1049732315618386
- Berry, L., & St. Pierre, I. (2012). Nursing workload and patient care: Understanding the value of nurses, the effects of excessive workload, and how nurse-patient ratios and dynamic staffing models can help. The Canadian Federation of Nurses.
- Bodenheimer, T., & Sinsky, C. (2014). From triple to quadruple aim: Care of the patient requires care of the provider. Annals of Family Medicine, 12, 573–576. https://doi.org/10.1370/afm.1713
- Braedley, S., Owusu, P., Przednowek, A., & Armstrong, P. (2018). We’re told, ‘Suck it up’: Long-term care workers’ psychological health and safety. Psychological Health and Safety: Ageing International, 43(1), 91–109. https://doi.org/10.1007/s12126-017-9288-4
- Braithwaite, J., Wears, R., & Hollnagel, E. (2016). Resilient health care, volume 3: Reconciling work-as-imagined and work-as-done. CRC Press.
- Brennan, C. W., Daly, B. J., & Jones, K. R. (2013). State of the science: The relationship between nurse staffing and patient outcomes. Western Journal of Nursing Research, 35, 760–794. https://doi.org/10.1177/0193945913476577
- Broberg, O. (1997). Integrating ergonomics into the product development process. International Journal of Industrial Ergonomics, 19, 317–327. https://doi.org/10.1016/S0169-8141(96)00041-8
- Broberg, O. (2010). Workspace design: A case study applying participatory design principles of healthy workplaces in an industrial setting. International Journal of Technology Management, 51, 39–56. https://doi.org/10.1504/IJTM.2010.033127
- Broberg, O., & Hermund, I. (2004). The OHS consultant as a ‘political reflective navigator’ in technological change processes. International Journal of Industrial Ergonomics, 33, 315–326. https://doi.org/10.1016/j.ergon.2003.10.005
- Brocke, J. V., Schmiedel, T., Recker, J., Trkman, P., Mertens, W., & Viaene, S. (2014). Ten Principles of good business process management. Business Process Management Journal, 20(4), 530–548. https://doi.org/10.1108/BPMJ-06-2013-0074
- Buckle, P. (2010). ‘The perfect is the enemy of the good’ – Ergonomics research and practice. Institute of ergonomics and human factors annual lecture 2010. Ergonomics, 54(1), 1–11. https://doi.org/10.1080/00140139.2010.542251
- Bureau of Labor, S. (2011). U.S. department of labor, occupational outlook handbook: A review of 50 years of change. Monthly Labor Review.
- Canadian Federation of Nurses, U., (2017). Quick facts 2017. 1–6.
- Carayon, P. (2006). Human factors of complex sociotechnical systems. Applied Ergonomics, 37, 525–535. https://doi.org/10.1016/j.apergo.2006.04.011
- Carayon, P. (2009). The balance theory and the work system model … Twenty years later. International Journal of Human-Computer Interaction, 25(5), 313–327. https://doi.org/10.1080/10447310902864928
- Carayon, P. (2011). Handbook of human factors and ergonomics in health care and patient safety. CRC Press.
- Carayon, P., & Gürses, A. P. (2005). A human factors engineering conceptual framework of nursing workload and patient safety in intensive care units. Intensive & Critical Care Nursing: The Official Journal of the British Association of Critical Care Nurses, 21, 284–301. https://doi.org/10.1016/j.iccn.2004.12.003
- Carayon, P., Hancock, P., Leveson, N., Noy, I., Sznelwar, L., & van Hootegem, G. (2015). Advancing a sociotechnical systems approach to workplace safety – developing the conceptual framework. Ergonomics, 58, 548–564. https://doi.org/10.1080/00140139.2015.1015623
- Carayon, P., Hundt, A. S., Karsh, B., Gurses, A., Alvarado, C., Smith, M., & Brennan, P. F. (2006). Work system design for patient safety: the seips model. Quality & Safety in Health Care, 15(suppl 1), i50–58. https://doi.org/10.1136/qshc.2005.015842
- Carayon, P., Wooldridge, A., Hoonakker, P., Hundt, A. S., & Kelly, M. M. (2020). Seips 3.0: human-centered design of the patient journey for patient safety. Applied Ergonomics, 84, 103033. https://doi.org/10.1016/j.apergo.2019.103033
- Charlton, S. G., & O’brien, T. G. (2002). Handbook of human factors testing and evaluation. Lawrence Erlbaum Assoc.
- Chassin, R. (2008). The six sigma initiative at mount sinai medical center. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 75, 45–52. https://doi.org/10.1002/msj.20011
- Chênevert, D., Kilroy, S., Johnson, K., & Fournier, P. -L. (2021). The determinants of burnout and professional turnover intentions among Canadian physicians: application of the job demands-resources model. BMC Health Services Research, 21, 993. https://doi.org/10.1186/s12913-021-06981-5
- Cherns, A. (1976). The principles of sociotechnical design. Human Relations, 29, 783–792. https://doi.org/10.1177/001872677602900806
- Cho, H., Sagherian, K., Scott, L. D., & Steege, L. M. (2022). Occupational fatigue, individualized nursing care, and quality of nursing care among hospital nurses. Journal of Nursing Scholarship, 54(5), 648–657. https://doi.org/10.1111/jnu.12768
- Cho, H., & Steege, L. M. (2021). Nurse fatigue and nurse, patient safety, and organizational outcomes: A systematic review. Western Journal of Nursing Research, 43, 1157–1168. https://doi.org/10.1177/0193945921990892
- CIHR. 2021. Strategic plan 2021–2026 accelerate health system transformation through research to achieve the quadruple aim and health equity for all. In Research, I. O. H. S. A. P. Ed. Canadian institutes of health research. www.cihr-irsc.gc.ca
- Clegg, C. W. (2000). Sociotechnical principles for system design. Applied Ergonomics, 31, 463–477. https://doi.org/10.1016/S0003-6870(00)00009-0
- Coghlan, D., & Brydon-Miller, M. (2014). The SAGE encyclopedia of action research. SAGE Publications Ltd.
- Collins, D. (1998). Organizational change: Sociological perspectives. Routledge.
- Costa, L. B. M., & Godinho Filho, M. (2016). Lean healthcare: Review, classification and analysis of literature. Production Planning & Control, 27, 823–836. https://doi.org/10.1080/09537287.2016.1143131
- Cummings, T. (2008). Organization Development and Change Dynamics of Organizational Change and Learning. United Kingdom: John Wiley & Sons Ltd. 25–42. https://doi.org/10.1002/9780470753408.ch2
- Daly, B. J., & Brennan, C. W. (2009). Patient acuity: A concept analysis. Journal of Advanced Nursing, 65(5), 1114–1126. https://doi.org/10.1111/j.1365-2648.2008.04920.x
- Davis, C. H., & Schaefer, N. V. (2003). Development dynamics of a startup innovation cluster: The ICT sector in new brunswick. Clusters Old and New: The Transition to a Knowledge Economy in Canada’s Regions, 3(3) , 121–160.
- Dawson, D., & Reid, K. (1997). Fatigue, alcohol and performance impairment. Nature, 388, 235. https://doi.org/10.1038/40775
- Deming, W. E. (2000). Out of the Crisis. MIT Press.
- Den Hartog, D. N., & Verburg, R. M. (2004). High performance work systems, organisational culture and firm effectiveness. Human Resource Management Journal, 14, 55–79. https://doi.org/10.1111/j.1748-8583.2004.tb00112.x
- Docherty, P., Forslin, J., & (Rami) Shani, A. B. (2002). Creating Sustainable Work Systems. Routledge.
- Dul, J. (2015). Necessary condition analysis (NCA): Logic and methodology of “necessary but not sufficient” causality. Organizational Research Methods, 19(1), 10–52. https://doi.org/10.1177/1094428115584005
- Dul, J., & Neumann, W. P. (2009). Ergonomics contributions to company strategies. Applied Ergonomics, 40, 745–752. https://doi.org/10.1016/j.apergo.2008.07.001
- Easterby-Smith, M., & Lyles, M. A. (2011). Handbook of organizational learning and knowledge management. Wiley.
- Eijnatten, F. M. V., Sitter, U. D., Gustavsen, B., Emery, F., & Beinum, H. V. (1993). The paradigm that changed the work place. Van Gorcum; Arbetslivscentrum.
- Elliott, D. J., Young, R. S., Brice, J., Aguiar, R., & Kolm, P. (2014). Effect of hospitalist workload on the quality and efficiency of care. JAMA Internal Medicine, 174(5), 786–793. https://doi.org/10.1001/jamainternmed.2014.300
- Farid, M., Purdy, N., & Neumann, W. P. (2020). Using system dynamics modelling to show the effect of nurse workload on nurses’ health and quality of care. Health and Quality of Care: Ergonomics, 63(8), 952–964. https://doi.org/10.1080/00140139.2019.1690674
- Ghoshal, S., & Nohria, N. (1993). Horses for courses: Organizational forms for multinational corporations. Sloan Management Review, 34(2), 23.
- Giacomin, J. (2014). What is human centred design? Design Journal, 17, 606–623. https://doi.org/10.2752/175630614X14056185480186
- Goodman, L., Khemani, E., Cacao, F., Yoon, J., Burkoski, V., Jarrett, S., Collins, B., & Hall, T. N. T. (2018). A comparison of hospital-acquired pressure injuries in intensive care and non-intensive care units: A multifaceted quality improvement initiative. BMJ Open Quality, 7, e000425. https://doi.org/10.1136/bmjoq-2018-000425
- Gormanns, N., Lasota, M., McCracken, M., & Zitikyte, D., (2011). Quick facts: Absenteeism and Overtime. adapted from: trends in own illness or disability-related absenteeism and overtime among publicly-employed registered nurses — summary of key findings. Report Prepared by Informetrica Limited for Canadian Federation.
- Greenwood, D. (2002). Action research: Unfulfilled promises and unmet challenges. Concepts and Transformation, 7, 117–139. https://doi.org/10.1075/cat.7.2.02gre
- Greig, M. A., Village, J., Salustri, F. A., & Neumann, W. P. (2023). Examining human factors and ergonomics aspects in a manufacturing organisation’s metrics system: Measuring up to stakeholder needs. Ergonomics, 1–22. https://doi.org/10.1080/00140139.2023.2168065
- Griffiths, P., Dall’ora, C., Simon, M., Ball, J., Lindqvist, R., Rafferty, A. -M., Schoonhoven, L., Tishelman, C., Aiken, L. H., & Consortium, R. C. (2014). Nurses’ shift length and overtime working in 12 European countries: the association with perceived quality of care and patient safety. Medical Care, 52(11), 975–981. https://doi.org/10.1097/MLR.0000000000000233
- Grosse, E. H., Glock, C. H., & Neumann, W. P. (2017). Human factors in order picking: a content analysis of the literature. International Journal of Production Research, 55, 1260–1276. https://doi.org/10.1080/00207543.2016.1186296
- Gustavsen, B. (2003a). Action research and the problem of the single case. Concepts & Transformation, 8, 93. https://doi.org/10.1075/cat.8.1.07gus
- Gustavsen, B. (2008). Action Research, Practical Challenges and the Formation of Theory. Action Research, 6, 421–437. https://doi.org/10.1177/1476750308094130
- Gustavsen, B., Ekman Philips, M., Wikman, A., & Hofmaier, B. (1996). Concept-driven development and the organization of the process of change : An evaluation of the Swedish working life fund. John Benjamins Publishing Company.
- Gustavsen, B., Nyhan, B., & Ennals, R. (2007). Learning together for local innovation: promoting learning regions. In B. Nyhan (Ed.), Cedefop reference series (p. 68). Office for Official Publications of the European Communities.
- Haimes, M. C., & Carayon, P. (1998). Theory and practice for the implementation of ‘in-house’, continuous improvement participatory ergonomic programs. Applied Ergonomics, 29(6), 461–472. https://doi.org/10.1016/S0003-6870(98)00012-X
- Hall-Andersen, L. B., & Broberg, O. (2014). Integrating ergonomics into engineering design: The role of objects. Applied Ergonomics, 45, 647–654. https://doi.org/10.1016/j.apergo.2013.09.002
- Harmon, J., Scotti, D. J., Behson, S., Farias, G., Petzel, R., Neuman, J. H., & Keashly, L. (2003). Effects of high-involvement work systems on employee satisfaction and service costs in veterans healthcare. Journal of Healthcare Management, 48(6), 393–405. https://doi.org/10.1097/00115514-200311000-00009
- Harry, M. J., & Schroeder, R. (2005). Six sigma: The breakthrough management strategy revolutionizing the world’s top corporations. Currency/Random House.
- Hasle, P., & Jensen, P. L. (2006). Changing the internal health and safety organization through organizational learning and change management. Human Factors and Ergonomics in Manufacturing, 16, 269–284. https://doi.org/10.1002/hfm.20053
- Health Quality Council of Alberta. (2016). Simulation-based mock-up evaluation framework, calgary. https://hqca.ca/resources-for-improvement/human-factors/healthcare-facility-mock-up-evaluation-framework-guidelines/
- Health_Quality_Ontario. 2017. Quality Matters: Realizing excellent care for all. Committee, H. Q. O. S. S. Q. A. . Ed. Queen’s Printer for Ontario, Toronto.https://www.hqontario.ca/Portals/0/documents/health-quality/realizing-excellent-care-for-all-1704-en.pdf
- Helbin, T., & Van Looy, A. (2021). Is business process management (Bpm) ready for ambidexterity? Conceptualization, implementation guidelines and research agenda. Sustainability, 13(4), 1906. https://doi.org/10.3390/su13041906
- Hendrick, H. W., & Kleiner, B. M. (2001). Macroergonomics - an introduction to work system design. Human Factors and Ergonomics Society.
- Hignett, S., Wilson, J. R., & Morris, W. (2005). Finding ergonomic solutions—participatory approaches. Occupational Medicine-Oxford, 55(3), 200–207. https://doi.org/10.1093/occmed/kqi084
- Holden, R. J. (2011). Lean thinking in emergency departments: a critical review. Annals of Emergency Medicine, 57, 265–278. https://doi.org/10.1016/j.annemergmed.2010.08.001
- Holden, R. J., & Carayon, P. (2021). Seips 101 and seven simple seips tools. BMJ Quality & Safety, 30, 901. https://doi.org/10.1136/bmjqs-2020-012538
- Holden, R. J., Carayon, P., Gurses, A. P., Hoonakker, P., Hundt, A. S., Ozok, A. A., & Rivera-Rodriguez, A. J. (2013). Seips 2.0: A human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics, 56, 1669–1686. https://doi.org/10.1080/00140139.2013.838643
- Holden, R. J., & Karsh, B. -T. (2010). The technology acceptance model: Its past and its future in health care. Journal of Biomedical Informatics, 43, 159–172. https://doi.org/10.1016/j.jbi.2009.07.002
- Holden, J. H., Or, C. K. L., Alper, S. J., Rivera, S. J., & Karsh, B. T. (2008). a change management framework for macroergonomics field research. Applied Ergonomics, 39(4), 459–474. https://doi.org/10.1016/j.apergo.2008.02.016
- Holden, R. J., Rivera, A. J., & Carayon, P. (2015). Occupational macroergonomics: Principles, scope, value, and methods. IIE Transactions on Occupational Ergonomics and Human Factors, 3, 1–8. https://doi.org/10.1080/21577323.2015.1027638
- Holden, R. J., Scanlon, M. C., Patel, N. R., Kaushal, R., Escoto, K. H., Brown, R. L., Alper, S. J., Arnold, J. M., Shalaby, T. M., & Murkowski, K. (2011). A human factors framework and study of the effect of nursing workload on patient safety and employee quality of working life. BMJ Quality & Safety, 20(1), 15–24. https://doi.org/10.1136/bmjqs.2008.028381
- Hollnagel, E., & Clay-Williams, R. (2022). Work-as-imagined and work-as-done, implementation science. Routledge.
- Ibrahim Shire, M., Jun, G. T., Moon, S., & Robinson, S. (2018). A system dynamics approach to workload management of hospital pharmacy staff: Modeling the tradeoff between dispensing backlog and dispensing errors. IISE Transactions on Occupational Ergonomics and Human Factors, 6, 209–224. https://doi.org/10.1080/24725838.2018.1555563
- International_Council_of_Nurses, (2007). Fact Sheet: Positive practice environments. International Centre for Human Resources in Nursing, https://neltoolkit.rnao.ca/sites/default/files/International%20Centre%20for%20Human%20Resources%20in%20Nursing_Positive%20Practice%20Environments.pdf
- International_Council_of_Nurses. (2020). The global nursing shortage and nurse retention, international council of nurses policy breif. https://www.icn.ch/system/files/2021-07/ICN%20Policy%20Brief_Nurse%20Shortage%20and%20Retention.pdf
- Jang, R., Karwowski, W., Quesada, P. M., Rodrick, D., Sherehiy, B., Cronin, S. N., & Layer, J. K. (2007). Biomechanical evaluation of nursing tasks in a hospital setting. Ergonomics, 50(11), 1835–1855. https://doi.org/10.1080/00140130701674661
- Kaghan, W. N., & Bowker, G. C. (2001). Out of machine age? Complexity, sociotechnical systems, and actor network theory. Journal of Engineering and Technology Management, 18(3–4), 253–269. https://doi.org/10.1016/S0923-4748(01)00037-6
- Kalisch, B. J., & Williams, R. A. (2009). Development and psychometric testing of a tool to measure missed nursing care. The Journal of Nursing Administration, 39(5), 211–219. https://doi.org/10.1097/NNA.0b013e3181a23cf5
- Karwowski, W. (2001). International encyclopedia of ergonomics and human factors. Taylor & Francis US.
- Kleiner, B. M. (2006). Macroergonomics: Analysis and design of work systems. Applied Ergonomics, 37, 81–89. https://doi.org/10.1016/j.apergo.2005.07.006
- Koukoulaki, T. (2014). The impact of lean production on musculoskeletal and psychosocial risks: An examination of sociotechnical trends over 20 years. Applied Ergonomics, 45, 198–212. https://doi.org/10.1016/j.apergo.2013.07.018
- Kuorinka, I. (1997). Tools and means of implementing participatory ergonomics. International Journal of Industrial Ergonomics, 19, 267–270. https://doi.org/10.1016/S0169-8141(96)00035-2
- Landsbergis, A. P., Cahill, J., & Schnall, P. (1999). The impact of lean production and related new systems of work organization on worker health. Journal of Occupational Health Psychology, 4(2), 108. https://doi.org/10.1037/1076-8998.4.2.108
- Linzer, M., Manwell, L. B., Williams, E. S., Bobula, J. A., Brown, R. L., Varkey, A. B., Man, B., McMurray, J. E., Maguire, A., Horner-Ibler, B., & Schwartz, M. D., (2009). Working conditions in primary care: physician reactions and care quality. Ann Intern Med 151: 28–36, w26-29.
- MacPhee, M., Dahinten, V. S., & Havaei, F. (2017). The impact of heavy perceived nurse workloads on patient and nurse outcomes. Administrative Sciences, 7(1), 7. https://doi.org/10.3390/admsci7010007
- Maunder, R. G., Heeney, N. D., Strudwick, G., Shin, H. D., O’neill, B., Young, N., Jeffs, L. P., Barrett, K., Bodmer, N. S., Born, K. B., Hopkins, J., Jüni, P., Perkhun, A., Price, D. J., Razak, F., Christopher, J., Mushquash, C. J., & Linda Mah, L. (2021). on behalf of the Ontario COVID-19 science advisory table and mental health working group, (2021), burnout in hospital-based healthcare workers during COVID-19. Science Briefs of the Ontario COVID-19 Science Advisory Table, 2(46). https://doi.org/10.47326/ocsat.2021.02.46.1.0
- McCarthy, C., Boniol, M., Daniels, K., Cometto, G., Diallo, K., Lawani, A., & Campbell, J. (2020). State of the world’s nursing 2020: Investing in education, jobs and leadership. World Health Organization.
- McGillis Hall, L., Doran, D., Tregunno, D., McCutcheon, A., O’brien-Pallas, L., Tranmer, J., Rukholm, E., Patrick, A., White, P., & Thomson, D. (2005). Quality work environments for nurse and patient safety. Jones and Barlett Publishers, Inc.
- McGillis Hall, L., & Visekruna, S. (2020). The outlook on nursing: A snapshot from Canadian nurses on work environments pre-Covid-19. Canadian Federation of Nurses Unions.
- Melnyk, B. M., Kelly, S. A., Stephens, J., Dhakal, K., McGovern, C., Tucker, S., Hoying, J., McRae, K., Ault, S., Spurlock, E., & Bird, S. B. (2020). Interventions to improve mental health, well-being, physical health, and lifestyle behaviors in physicians and nurses: A systematic review. American Journal of Health Promotion, 34, 929–941. https://doi.org/10.1177/0890117120920451
- Meng, H. -C. (2005). Innovation cluster as the national competitiveness tool in the innovation driven economy. International Journal of Foresight and Innovation Policy, 2(1), 104–116. https://doi.org/10.1504/IJFIP.2005.007598
- Michalsksi, W. J., & King, D. G. (2003). Six sigma tool navigator: The master guide for teams. Productivity Press.
- Mishra, B. (2018). The organizational learning inventory: An assessment guide for understanding your institution’s learning capabilities. The Learning Organization, 25, 455–456. https://doi.org/10.1108/TLO-09-2018-128
- Nat Natarajan, R. (2006). Transferring best practices to healthcare: Opportunities and challenges. The TQM Magazine, 18(6), 572–582. https://doi.org/10.1108/09544780610707084
- Needleman, J., Buerhaus, P. I., Stewart, M., Zelevinsky, K., & Mattke, S. (2006). Nurse staffing in hospitals: Is there a business case for quality? Health Affairs, 25, 204–211. https://doi.org/10.1377/hlthaff.25.1.204
- Needleman, C., & Needleman, M. L. (1996). Qualitative methods for intervention research. American Journal of Industrial Medicine, 29(4), 329–337. https://doi.org/10.1002/(SICI)1097-0274(199604)29:4<329:AID-AJIM10>3.0.CO;2-3
- Neumann, W. P., (2007). Inventory of human factors tools and methods – a work-system design perspective, in: W. P. Neumann (Ed.), Human Factors Engineering Lab – Technical Report. Ryerson University, www.ryerson.ca/hfe
- Neumann, W. P. (2017). The obliquity strategy as a means of overcoming the “Drift to Unsafe States” effect. Joint Proceedings of the 48th Annual Conference of the Association of Canadian Ergonomists & 12th International Symposium on Human Factors in Organizational Design and Management, Banff: Canada. ( July 31 – August 3, 2017)
- Neumann, W. P., Dixon, S. M., & Ekman, M. (2012). Ergonomics action research I: Shifting from hypothesis testing to experiential learning. Ergonomics, 55, 1127–1139. https://doi.org/10.1080/00140139.2012.700327
- Neumann, W. P., Dixon, S. M., & Nordvall, A. -C. (2014). Consumer demand as a driver of improved working conditions: The ‘Ergo-Brand’ proposition. Ergonomics, 57, 1113–1126. https://doi.org/10.1080/00140139.2014.917203
- Neumann, W. P., & Dul, J. (2010). Human factors: Spanning the Gap between OM & HRM. International Journal of Operations & Production Management, 30, 923–950. https://doi.org/10.1108/01443571011075056
- Neumann, W. P., Ekman, M., & Winkel, J. (2009). Integrating ergonomics into production system development – the Volvo Powertrain case. Applied Ergonomics, 40(3), 527–537. https://doi.org/10.1016/j.apergo.2008.09.010
- Neumann, W. P., & Purdy, N. 2019. Designing smarter healthcare: Turning nurses’ ideas into process improvements. E. Ontario. Ed., https://www.ecampusontario.ca/designing-smarter-healthcare-turning-nurses-ideas-into-process-improvements/
- Neumann, W. P., Steege, L. M., Jun, G. T., & Wiklund, M. (2018). Ergonomics and human factors in healthcare system design – an introduction to this special issue. IISE Transactions on Occupational Ergonomics and Human Factors, 6, 109–115. https://doi.org/10.1080/24725838.2018.1560927
- Neumann, W. P., & Village, J. (2012). Ergonomics action research Ii: A framework for integrating hf into work system design. Ergonomics, 55, 1140–1156. https://doi.org/10.1080/00140139.2012.706714
- Neumann, W. P., Winkelhaus, S., Grosse, E. H., & Glock, C. H. (2021). Industry 4.0 and the human factor – a systems framework and analysis methodology for successful development. International Journal of Production Economics, 233, 107992. https://doi.org/10.1016/j.ijpe.2020.107992
- Neumann, W. P., Winkel, J., Palmerud, G., & Forsman, M. (2018). Innovation and employee injury risk in automotive disassembly operations. International Journal of Production Research, 56, 3188–3203. https://doi.org/10.1080/00207543.2018.1432910
- Nicosia, F. M., Park, L. G., Gray, C. P., Yakir, M. J., & Hung, D. Y. (2018). Nurses’ perspectives on lean redesigns to patient flow and inpatient discharge process efficiency. Global Qualitative Nursing Research, 5, 2333393618810658. https://doi.org/10.1177/2333393618810658
- Noro, K., & Imada, A. S. (1991). Participatory Ergonomics. Taylor & Francis.
- Nurses, I.C.o. (2015). International classification for nursing practice (Icnp®).
- Nursing Task Force. (1999). Good nursing, good health: An investment for the 21st century – Report of the nursing task force. Ontario Ministry of Health.
- OECD. (2017). OECD guidelines on measuring the quality of the working environment. OECD Publishing. https://doi.org/10.1787/9789264278240-en.
- Ogbeiwi, O. (2017). Why written objectives need to be really smart. British Journal of Healthcare Management, 23, 324–336. https://doi.org/10.12968/bjhc.2017.23.7.324
- Ontario_Medical_Association, (2017). A healthy Ontario: building a sustainable health care system. 2nd report from the premier’s council on improving healthcare and ending hallway medicine. https://content.oma.org//wp-content/uploads/private/Devlin_Summary.pdf
- Oxtoby, B., McGuiness, T., & Morgan, R. (2002). Developing organisational change capability. European Management Journal, 20, 310–320. https://doi.org/10.1016/S0263-2373(02)00047-6
- Paguio, J. T., & Yu, D. S. F. (2020). A mixed methods study to evaluate the effects of a teamwork enhancement and quality improvement initiative on nurses’ work environment. Journal of Advanced Nursing, 76, 664–675. https://doi.org/10.1111/jan.14270
- Patton, M. Q. (2011). Developmental evaluation - applying complexity concepts to enhance innovation and use. The Guilford Press.
- Pawson, R., & Tilley, N. (1997). Realistic Evaluation. Sage.
- PCAST, (2014). Report to the president better health care and lower costs: Accelerating improvement through systems engineering executive office of the president, President’s Council of Advisors on Science and Technology p. 66. www.whitehouse.gov/ostp/pcast
- Perlo, J., Balik, B., Swensen, S., Kabcenell, A., Landsman, J., & Feeley, D., (2017). Framework for improving joy in work. Ihi white paper. http://www.ihi.org/resources/Pages/IHIWhitePapers/Framework-Improving-Joy-in-Work.aspx
- Pettigrew, A. M., Woodman, R. W., & Cameron, K. S. (2001). Studying organizational change and development: Challenges for future research. Academy of Management Journal, 44(4), 697–713. https://doi.org/10.2307/3069411
- Poggi, I. (2005). The goals of persuasion. Pragmatics & Cognition, 13, 297–335. https://doi.org/10.1075/pc.13.2.04pog
- Privitera, M. R. (2018). Addressing human factors in burnout and the delivery of healthcare: quality & safety imperative of the quadruple aim. Health, 10(05), 629–644. https://doi.org/10.4236/health.2018.105049
- Purdy, N., Neumann, W. P., Searcy, C., Sears, K., English, K., Davies, M. -A., Nkain, B., Innis, J., Mastrilli, P., & Hanna, D. (2017). QI methods and tools for nurses. https://de.ryerson.ca/games/patient-safety/index.html.
- Purdy, N., Spence Laschinger, H. K., Finegan, J., Kerr, M., & Olivera, F. (2010). Effects of Work Environments on Nurse and Patient Outcomes. Journal of nursing management, 18, 901–913. https://doi.org/10.1111/j.1365-2834.2010.01172.x
- Qureshi, S. M., Purdy, N., Mohani, A., & Neumann, W. P. (2019). Predicting the Effect of Nurse–Patient Ratio on Nurse Workload and Care Quality Using Discrete Event Simulation. Journal of nursing management, 27, 971–980. https://doi.org/10.1111/jonm.12757
- Qureshi, S. M., Purdy, N., & Neumann, W. P. (2020). Development of a Methodology for Healthcare System Simulations to Quantify Nurse Workload and Quality of Care. IISE Transactions on Occupational Ergonomics and Human Factors, 8, 27–41. https://doi.org/10.1080/24725838.2020.1736692
- Qureshi, S. M., Purdy, N., & Neumann, W. P. (2021). A Computerized Model Quantifying the Impact of Geographical Patient- Bed Assignment on Nurse Workload and Quality Care. Nursing Economics, 39(1), 23–34.
- Rasmussen, J. (1997). Risk Management in a Dynamic Society: A Modelling Problem. Safety science, 27, 183–213. https://doi.org/10.1016/S0925-7535(97)00052-0
- Rasmussen, J. (2000). Human Factors in a Dynamic Information Society: Where Are We Heading?. Ergonomics, 43, 869–879. https://doi.org/10.1080/001401300409071
- Ratnapalan, S., & Uleryk, E. (2014). Organizational Learning in Health Care Organizations. Systems, 2(1), 24–33. https://doi.org/10.3390/systems2010024
- Razzouk, R., & Shute, V. (2012). What Is Design Thinking and Why Is It Important?. Review of educational research, 82, 330–348. https://doi.org/10.3102/0034654312457429
- Reason, P., & Bradbury, H. (2001). Handbook of Action Research. Sage.
- RNAO. (2022). Nursing through Crisis - a Comparative Perspective. Registered Nurses’ Association of Ontario, 140. https://rnao.ca/sites/default/files/202205/NursingThroughCrisis-AComparativeAnalysis2022.pdf
- Roberts, J. P., Fisher, T. R., Trowbridge, M. J., & Bent, C. (2016). A Design Thinking Framework for Healthcare Management and Innovation. Healthcare, 4, 11–14. https://doi.org/10.1016/j.hjdsi.2015.12.002
- Rogers, A. E., Hwang, W. T., Scott, L. D., Aiken, L. H., & Dinges, D. F. (2004). The Working Hours of Hospital Staff Nurses and Patient Safety. Health affairs, 23(4), 202–212. https://doi.org/10.1377/hlthaff.23.4.202
- Rose, L. M., Orrenius, U. E., & Neumann, W. P. (2013). Work Environment and the Bottom Line: Survey of Tools Relating Work Environment to Business Results. Human Factors and Ergonomics in Manufacturing & Service Industries, 23, 368–381. https://doi.org/10.1002/hfm.20324
- Rosted, E., Thomsen, T. G., Krogsgaard, M., Busk, H., Geisler, A., Thestrup Hansen, S., Kjerholt, M., Mortensen, C. B., Thomsen, T. H., Beck, M., & Petersen, M. (2021). On the Frontline Treating Covid-19: A Pendulum Experience—from Meaningful to Overwhelming—for Danish Healthcare Professionals. Journal of clinical nursing, 30, 3448–3455. https://doi.org/10.1111/jocn.15821
- Salter, K., & Kothari, A. (2014). Using Realist Evaluation to Open the Black Box of Knowledge Translation: A State-of-the-Art Review. Implementation Science, 9, 115. https://doi.org/10.1186/s13012-014-0115-y
- Salvendy, G. (2001). Handbook of Industrial Engineering: Technology and Operations Management. Wiley-Interscience.
- Sayin, F., Denton, M., Brookman, C., Davies, S., & Zeytinoglu, I. (2021). Workload, Workplace Violence and Harassment, and Well-Being of Personal Support Workers in Home and Community Care. Relations Industrielles/Industrial Relations, 76(2), 312–335. https://doi.org/10.7202/1078509ar
- Schuckhart, M. C., (2010). The Misscare Nursing Survey: A Secondary Data Analysis.
- Senge, P. M. (1990). The Fifth Discipline - the Art & Practice of the Learning Organisation. Century Business.
- Sgarbossa, F., Grosse, E. H., Neumann, W. P., Battini, D., & Glock, C. H. (2020). Human Factors in Production and Logistics Systems of the Future. Annual reviews in control, 49, 295–305. https://doi.org/10.1016/j.arcontrol.2020.04.007
- Shultz, J., Borkenhagen, D., Rose, E., Gribbons, B., Rusak-Gillrie, H., Fleck, S., Muniak, A., & Filer, J. (2019). Simulation-Based Mock-up Evaluation of a Universal Operating Room. HERD: Health Environments Research & Design Journal, 13(1), 68–80. https://doi.org/10.1177/1937586719855777
- Sikka, R., Morath, J. M., & Leape, L. (2015). The Quadruple Aim: Care, Health, Cost and Meaning in Work. BMJ Quality & Safety, 24, 608. https://doi.org/10.1136/bmjqs-2015-004160
- Silas, L. (2015). Creating Safe Cultures and Work Environments for Nurses Occupational Health & Safety: How to Make Our Workplace Safe Lessons Learned from Sars Commission Inquiry.
- Skyttner, L. (2001). General Systems Theory - Ideas and Applications. World Scientific.
- Sneyd, K. P., & Rowley, J. (2004). Linking Strategic Objectives and Operational Performance: An Action Research-Based Exploration. Measuring business excellence, 8, 42–51. https://doi.org/10.1108/13683040410555609
- Stanton, N. A., Hedge, A., Brookhuis, K., Salas, E., & Hendrick, H. (2004). Handbook of Human Factors and Ergonomics Methods. CRC Press.
- Sterman, J. D. (2000). Business Dynamics: Systems Thinking and Modeling for a Complex World. McGraw-Hill.
- Stimpfel, A. W., & Aiken, L. H. (2013). Hospital Staff Nurses’ Shift Length Associated with Safety and Quality of Care. Journal of nursing care quality, 28(2), 122–129. https://doi.org/10.1097/NCQ.0b013e3182725f09
- Theberge, N., & Neumann, W. P. (2010). Doing ‘Organizational Work’: Expanding the Conception of Professional Practice in Ergonomics. Applied ergonomics, 42, 76–84. https://doi.org/10.1016/j.apergo.2010.05.002
- Thomas, K. J., & Fitter, M. J. (1997). Evaluating Complementary Therapies for Use in the National Health Service: ‘Horses for Courses’. Part 2: Alternative Research Strategies. Complementary therapies in medicine, 5, 94–98. https://doi.org/10.1016/S0965-2299(97)80006-4
- Tomblin Murphy, G., Sampalli, T., Bourque Bearskin, L., Cashen, N., Cummings, G., Elliott Rose, A., Etowa, J., Grinspun, D., Jones, E. W., Lavoie-Tremblay, M., MacMillan, K., MacQuarrie, C., Martin-Misener, R., Oulton, J., Ricciardelli, R., Silas, L., Thorne, S., & Villeneuve, M. (2022). Investing in Canada’s Nursing Workforce Post-Pandemic: A Call to Action. FACETS, 7, 1051–1120. https://doi.org/10.1139/facets-2022-0002
- Toulmin, S. E., & Gustavsen, B. (1996). Beyond Theory : Changing Organizations through Participation. John Benjamins Publ.
- Trinkoff, A. M., Lipscomb, J. A., Geiger-Brown, J., Storr, C. L., & Brady, B. A. (2003). Perceived Physical Demands and Reported Musculoskeletal Problems in Registered Nurses. American journal of preventive medicine, 24, 270–275. https://doi.org/10.1016/S0749-3797(02)00639-6
- Trusko, B. E., Pexton, C., Gupta, P. K., & Harrington, J. (2003). Improving Healthcare Quality and Cost with Six Sigma. FT Press.
- Tucker, A. L., Nembhard, I. M., & Edmondson, A. C. (2007). Implementing New Practices: An Empirical Study of Organizational Learning in Hospital Intensive Care Units. Management science, 53, 894–907. https://doi.org/10.1287/mnsc.1060.0692
- Tushman, M. L., & O’reilly, C. A. (1996). Ambidextrous Organizations: Managing Evolutionary and Revolutionary Change. California management review, 38, 8–29. https://doi.org/10.2307/41165852
- Valaitis, R. K., Wong, S. T., MacDonald, M., Martin-Misener, R., O’mara, L., Meagher-Stewart, D., Isaacs, S., Murray, N., Baumann, A., Burge, F., Green, M., Kaczorowski, J., & Savage, R. (2020). Addressing Quadruple Aims through Primary Care and Public Health Collaboration: Ten Canadian Case Studies. BMC Public Health, 20(1), 1–16. https://doi.org/10.1186/s12889-020-08610-y
- Venkatesh, V., & Davis, F. D. (2000). A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Management science, 46, 186–204. https://doi.org/10.1287/mnsc.46.2.186.11926
- Village, J., Greig, M., Salustri, F., Zolfaghari, S., & Neumann, W. P. (2014a). An Ergonomics Action Research Demonstration: Integrating Human Factors into Assembly Design Processes. Ergonomics, 57, 1574–1589. https://doi.org/10.1080/00140139.2014.938128
- Village, J., Greig, M., Zolfaghari, S., Salustri, F., & Neumann, W. P. (2014b). Adapting Engineering Design Tools to Include Human Factors. IIE Transactions on Occupational Ergonomics and Human Factors, 2, 1–14. https://doi.org/10.1080/21577323.2014.905884
- Village, J., Searcy, C., Salustri, F., & Neumann, W. P. (2015). Design for Human Factors (Dfhf): A Grounded Theory for Integrating Human Factors into Production Design Processes. Ergonomics, 58, 1529–1546. https://doi.org/10.1080/00140139.2015.1022232
- von Thiele Schwarz, U., Nielsen, K., Edwards, K., Hasson, H., Ipsen, C., Savage, C., Simonsen Abildgaard, J., Richter, A., Lornudd, C., Mazzocato, P., & Reed, J. E. (2020). How to Design, Implement and Evaluate Organizational Interventions for Maximum Impact: The Sigtuna Principles. European Journal of Work and Organizational Psychology, 30(3), 1–13. https://doi.org/10.1080/1359432X.2020.1803960
- Wallace J E, Lemaire J B and Ghali W A. (2009). Physician wellness: a missing quality indicator. The Lancet, 374(9702), 1714–1721. https://doi.org/10.1016/S0140-6736(09)61424-0
- Westgaard, R., & Winkel, J. (2011). Occupational Musculoskeletal and Mental Health: Significance of Rationalization and Opportunities to Create Sustainable Production Systems–a Systematic Review. Applied ergonomics, 42, 261–296. https://doi.org/10.1016/j.apergo.2010.07.002
- WHO. (2020). In Organization, W. H. (Ed.), Charter - Health Worker Safety: A Priority for Patient Safety. https://www.who.int/docs/default-source/world-patient-safety-day/health-worker-safety-charter-wpsd-17-september-2020-3-1.pdf?sfvrsn=2cb6752d_2
- Woods, D. (2019). Essentials of resilience, revisited. In M. Ruth & S. Goessling-Reisemann (Eds.), Handbook on Resilience of Socio-Technical Systems (pp. 52–65). Edward Elgar Publishing.
- Wulff, I. A., Rasmussen, B., & Westgaard, R. H. (2000). Documentation in Large-Scale Engineering Design: Information Processing and Defensive Mechanisms to Generate Information Overload. International journal of industrial ergonomics, 25, 295–310. https://doi.org/10.1016/S0169-8141(99)00020-7
- Wulff, I. A., Westgaard, R. H., & Rasmussen, B. (1999). Ergonomic criteria in large-scale engineering design—II Evaluating and applying requirements in the real world of design. Applied ergonomics, 30(3), 207–221. https://doi.org/10.1016/S0003-6870(98)00030-1
- Xie, A., Rock, C., Hsu, Y. -J., Osei, P., Andonian, J., Scheeler, V., Keller, S. C., Cosgrove, S. E., & Gurses, A. P. (2018). Improving Daily Patient Room Cleaning: An Observational Study Using a Human Factors and Systems Engineering Approach. IISE Transactions on Occupational Ergonomics and Human Factors, 6, 178–191. https://doi.org/10.1080/24725838.2018.1487348
- Zink, K. J., Steimle, U., & Schröder, D. (2008). Comprehensive Change Management Concepts: Development of a Participatory Approach. Applied ergonomics, 39, 527–538. https://doi.org/10.1016/j.apergo.2008.02.015
