
ABSTRACT
Background: Gay, bisexual and other men who have sex with men (GBMSM) are at far greater risk of experiencing poor mental health (MH) than wider society. This disparity was exacerbated by additional ‘unique to sexual minority status’ COVID-19 stressors.
Objective: This sequential, mixed-methods study examined remote MH help-seeking among GBMSM in the U.K. and Ireland during the first COVID-19 lockdown.
Methods and Results: Quantitative survey data (n = 1368), analysed with logistic regression, suggested GBMSM experiencing moderate-to-severe anxiety and those with a past MH diagnosis were most likely to seek MH support. Thematic analysis of qualitative interview (n = 18) data identified multiple barriers and enablers to GBMSM seeking remote MH help, with the help primarily sought from GBMSM-facing organisations and generic online resources. Finally, the behaviour change wheel was used to generate theoretically informed recommendations to promote MH help-seeking among GBMSM in Scotland.
Implications: We discuss how applying these recommendations in the short, medium and long term will begin to address GBMSM’s MH needs, post COVID-19.
Introduction
Our attempts to understand and mitigate the harms caused by COVID-19 are only just beginning. Herein, we consider how COVID-19 impacted one, often marginalised, group and appears to have exacerbated previously established health inequalities. We explore how mental health (MH) help-seeking amongst gay, bisexual, and other men who have sex with men (GBMSM) was shaped by the impact of COVID-19 during the U.K.’s first lockdown. To take forward recovery and build resilience within these communities, we begin the process of learning from COVID-19-related experiences both to conceptualise and plan services differently and address the long-standing inequalities affecting GBMSM. Then we use our findings to develop preliminary theory-based recommendations to reduce long-standing inequalities in GBMSM’s health.
GBMSM, MH, and COVID-19
Before COVID-19, GBMSM were disproportionately affected by multiple health inequalities compared to the wider population, including poorer MH (McDaid et al., Citation2020; McGarty et al., Citation2021). For instance, according to an Australian study, before COVID-19, 18% of all GBMSM were suffering from moderate-severe anxiety, 28% from moderate-severe depression, and half reported use of illicit drugs in the previous six months (Prestage et al., Citation2018). During COVID-19, further impacts upon GBMSM’s health have been documented, including a rise in levels of anxiety, depression, and loneliness (Frankis, Strongylou, & Kincaid, Citation2020; Holloway et al., Citation2021). In an Australian online cohort study of gay and bisexual men, the proportion of participants with moderate-severe depression increased from 19% to 26%, while the proportion of participants with moderate-severe anxiety increased from 13% to 17% (Bavinton et al., Citation2022). Indeed, sexual minorities reported greater psychological stress, depression, and anxiety associated with the pandemic than sexual majorities (Moore, Wierenga, Prince, Gillani, & Mintz, Citation2021; Peterson, Vaughan, & Carver, Citation2020). This is because additional, sexual minority-specific stressors (e.g. reduced connection to the LGBT community, sexual orientation-related family conflict etc.) further impacted LGBT people's MH, in addition to those generic COVID-19 stressors (Suen, Chan, & Wong, Citation2020) experienced by all. Thus, while studies have focused upon GBMSM’s MH during the COVID-19 pandemic, less is known about their MH help-seeking behaviours.
MH help-seeking behaviour in GBMSM
The high prevalence of mental health problems among GBMSM is mismatched with their efforts to seek mental health support. Despite the growing research in the area, there is lack of consensus on the definition of MH help seeking, given the complexity of the construct. Rickwood et al. (Citation2012) explain that ‘[mental health] help-seeking is an adaptive coping process that is the attempt to obtain external assistance to deal with a mental health concern’. MH support can be sought from several sources, specifically, informal (e.g. friends, family), formal (e.g. MH professionals), semi-formal (e.g. other health professionals such as GPs, nurses, support workers), and self-help (e.g. MH apps, books, CDs) sources (Kauer, Mangan, & Sanci, Citation2014; Xu et al., Citation2018). Rickwood et al.’s (Citation2005) model proposes that MH help-seeking behaviour requires: (1) an initial self-awareness of a MH problem, (2) a recognition of both symptoms and the need for support, (3) the identification of accessible sources of support, and, finally, (4) a willingness to seek support and disclose relevant information where necessary.
Before COVID-19, MH help-seeking behaviour was widely examined in a number of groups, including young people (Divin et al., Citation2018; Kauer et al., Citation2014; Pretorius, Chambers, & Coyle, Citation2019), African American youth (Planey, Smith, Moore, & Walker, Citation2019), men (Galdas, Cheater, & Marshall, Citation2005), rural residents (Cheesmond, Davies, & Inder, Citation2019), and the armed forces (Coleman, Stevelink, Hatch, Denny, & Greenberg, Citation2017). Systematic review evidence suggests that MH help-seeking rates are relatively low among people with diagnosed mental health issues, with around one-third seeking help in the last year (Gulliver, Griffiths, & Christensen, Citation2010). However, there is a scarcity of research examining MH help-seeking behaviour among GBMSM and none during COVID-19. Generally, GBMSM-related MH help-seeking research has predominantly focused upon identity-specific barriers that exist among GBMSM when seeking help for their MH (McDermott, Citation2015; Wu & Lee, Citation2021; Zay et al., Citation2021) such as LGBTQ stigma and a dual LGBTQ MH stigma (McDermott, Citation2015; Zay et al., Citation2021). However, since the social distancing requirements of COVID-19 shifted most health services to online (websites) or telehealth delivery (Murphy, Citation2020), we now need to understand this remote MH help-seeking, which has increased 12-fold during the pandemic (Pierce, Perrin, Tyler, McKee, & Watson, Citation2021).
Remote MH help-seeking
While websites have offered therapeutic MH resources since the late 1990s, the quality of information provided is unregulated and so may be lacking (Reavley & Jorm, Citation2011) or biased (Read & Cain, Citation2013). Despite this, several websites, mostly drawing on cognitive behavioural therapy (CBT) and mindfulness, have been evaluated as being effective (Rogers, Lemmen, Kramer, Mann, & Chopra, Citation2017). More recently, meta-analyses and systematic review evidence suggest that specific smartphone apps (again primarily drawing on CBT-derived therapy (e.g. Woebot) or mindfulness-based meditation (e.g. InsightTimer, Headspace)) can reduce stress, depression, anxiety and improve psychological well-being (Firth et al., Citation2017a, Citation2017b; Gál, Ștefan, & Cristea, Citation2021; Rathbone, Clarry, & Prescott, Citation2017). In an Australian study, it was found that among young men with MH issues, talking online helped (81%), and these men were also satisfied or very satisfied with the online help they received (83%) (Collin et al., Citation2011). Similarly, crisis phone-lines have been assessed as cost-effective and easy to access compared to face-to-face services (Bradford & Rickwood, Citation2014) and are effective in relation to several MH-related outcomes including enhanced mood and prevention of self-directed violence (Hoffberg, Stearns-Yoder, & Brenner, Citation2020).
However, the user’s ability to identify scientifically robust websites, apps and phone lines is unknown (Rogers et al., Citation2017). This has led health psychologists to examine how individuals seek support from services available to them.
MH services in the U.K. and Republic of Ireland
Within the U.K., health is a devolved matter, meaning each constituent country sets its own agenda to approach MH. Mental health policy of the four U.K. countries and The Republic of Ireland is largely similar; each country’s MH strategy focusses on prevention and early intervention, explicitly recognising inequalities relating to sexuality, alongside other characteristics (Dean, Citation2017). This is underpinned by MH services delivered by nationwide governmental health services and various non-governmental organisations. For example, in Scotland the NHS and several Scotland- (e.g. SAMH, Breathing Space) and U.K.-wide (e.g. Mental Health Foundation, MIND) charities deliver MH services on a population-wide basis, the charity LGBT Health and Wellbeing provide LGBTQI+ people with specialised MH support, whilst GBMSM-facingFootnote1 sexual health services and additional sexual health / blood-borne viruses charities (i.e. Waverley Care/S-X, Terrence Higgins Trust and HIV Scotland) offer holistic services engaging with GBMSM about their wider mental and physical health, albeit within a sexual health and HIV prevention context. Services include online information and self-help guides, telephone, online-chat and group-based support, GP pharmacological, brief-intervention, and individual counselling/ psychological support, provided through a combination of remote and in-person delivery. MH service provision adopts a largely similar model in the remaining U.K. countries and The Republic of Ireland, although availability, service waiting times and level of LGBTQI+ tailored support varies both within and across different countries.
Research questions
As well as shifting most semi-formal and formal sources of support remotely, COVID-19 lockdown removed many informal sources of support for GBMSM (e.g. commercial gay scene, sexual contacts, face-to-face meeting with friends). This study aims to address the sources of Rickwood et al.’s MH help-seeking model (Citation2005); formal and self-help sources; in the present study formal sources primarily relate to gay facing organisations facing organisations whilst self-help sources concern the remote help-seeking described above. Accordingly, we examine GBMSM’s MH help-seeking behaviours during the first COVID-19 lockdown (Mid-March to End June, 2020), to develop evidence and theory-based recommendations for service providers by addressing the following research questions (RQ).
RQ1: What are the key sociodemographic and psychological factors predicting remote MH help-seeking among GBMSM during the first COVID-19 lockdown in the UK and Republic of Ireland?
RQ2: What are the barriers and facilitators to remote MH help-seeking among GBMSM in Scotland?
RQ3: What are the preliminary recommendations to enable services to enhance MH help-seeking among GBMSM?
Methods
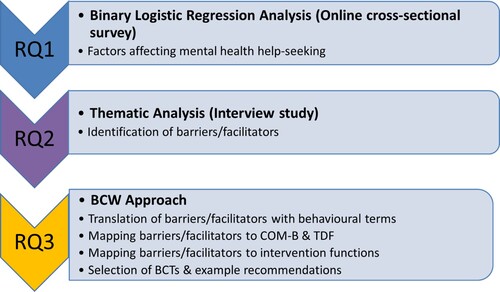
A sequential mixed-methods design was employed (see ), where online quantitative data analysis informed qualitative data theoretical sampling. Subsequently, findings were categorised and subjected to further behavioural analysis to provide holistic recommendations to improve MH help-seeking among GBMSM ( summarises the analytical steps taken to address our three research questions).
Figure 1. The sequential mixed-methods design employed in the current study.

Figure 2. Analytical steps taken to address RQ1, RQ2 & RQ3.
Quantitative study
The Social Media, Men who have sex with men, Sexual and Holistic Health – Pandemic study (SMMASH-Pan) collected anonymous, self-completed questionnaires from GBMSM in the U.K. and the Republic of Ireland. Ethical approval was granted by Glasgow Caledonian University (ref no: HLS/NCH/19/050). The survey was administered online via REDCap between June and July 2020 during the first COVID-19 lockdown. Adult GBMSM using gay-specific social media websites and/or apps (Grindr, Gaydar, Recon, Squirt, and Scruff) and/or mainstream social media (Facebook, Twitter, and Instagram) were invited to participate in their profile location, IP address or smartphone GPS co-ordinates were located in one of the five target countries (Scotland, Wales, Northern Ireland, England or the Republic of Ireland). Participants were also asked to circulate survey invites to relevant friends and family via email and text. In addition, our study collaborators sent invitations to their service users (HIV Scotland, Waverley Care SX, THT Scotland) to boost the Scottish sample since this country was the focus of our wider study. Similar to previous SMMASH surveys (e.g. McGarty et al., Citation2021), SMMASH-Pan examined mental, sexual, and physical health among GBMSM in the U.K. and Republic of Ireland, but also included questions on COVID-19 lockdown, social distancing and health service use. A copy of the questionnaire can be found on the SMMASH website https://www.smmash2020.org/surveys. The specific SMMASH-Pan measures examined herein are as follows;
Demographics: Age, sexual orientation (gay/bisexual or straight/other), education status (none/secondary or post-secondary), living situation (alone or with company) and ethnicity (white or person of colour).
Mental and Physical Health: Self-perceived health and mental health were assessed by asking participants ‘Currently, how is your (mental) health?’, with responses on a 5-point Likert-scale from ‘very good’ to ‘very poor’ and were also asked whether they had ever received a MH diagnosis by a doctor. Recent depression and anxiety were measured with the Patient Health Questionnaire-9 (PHQ-9 Kroenke, Spitzer, & Williams, Citation2001) and Generalized Anxiety Disorder-7 (GAD-7; Spitzer, Kroenke, Williams, & Löwe, Citation2006) questionnaires, respectively. PHQ-9 measures the frequency of various depression-related problems experienced in the last two weeks and has been validated for use in high income countries (Levis, Benedetti, Thombs, & DEPRESsion Screening Data (DEPRESSD) Collaboration, Citation2019). Responses are combined so participants could score between 0 (not affected by any of the issues at all) and 27 (affected by every issue nearly every day). Depression severity was then categorised as none/mild (score 0-9) or moderate/severe (score 10-27) depression. GAD-7 measures the frequency of various anxiety-related problems experienced in the last two weeks, with scores ranging from 0 (not affected by any issue at all) to 21 (affected by every issue nearly every day), validated for use in high income countries (Manea, Gilbody, & McMillan, Citation2015). Anxiety severity was then categorised as either none/mild anxiety (score 0-9) or moderate/severe (score 10-21) anxiety. Although these questionnaires are not necessarily diagnostic tools, people rated as experiencing moderate-/severe anxiety and/or depression would normally be considered by a clinician for pharmacological or counselling intervention (Manea et al., Citation2015).
Remote MH help-seeking behaviour during the first COVID-19 lockdown: Men were asked about their use of remote resources to seek MH support during lockdown as follows; ‘Have you accessed any of the following resources to help with your mental health since lockdown?’. Participants could select from ‘Websites’, ‘Apps’, ‘Phone Lines’, ‘None of the above’.
Statistical analysis
An a priori power analysis was not conducted for the SMMASH-Pan survey in anticipation of achieving a large sample size and the exploratory nature of the project. Participants were asked not to complete this iteration of the survey if they had already done so, but duplicates were not screened for. Fraudulent and partial entries were screened and deleted. Given the large sample size of the study (n = 1801), outliers were included in the analysis. Data were analysed using SPSS version 24. Given the lack of existing evidence on factors predicting help seeking among GBMSM an exploratory statistical approach (backward binary logistic regression) was chosen over a theory-based (hierarchical binary logistic regression) statistical analysis to address RQ1. The backward binary logistic regression analysis calculated estimated odds ratios (ORs) and 95% confidence intervals (CIs) to explore factors associated with MH help-seeking behaviour during the first COVID-19 lockdown in GBMSM in the U.K. and Republic of Ireland. The final model contained all variables significant at the bivariate level (P < 0.05) to assess which remained statistically significant.
Qualitative study
One-to-one phone and online interviews were conducted with 18 GBMSM living in Scotland between July and September 2020 (funding constraints meant interviews were only conducted with participants in Scotland). Ethical approval was obtained from Glasgow Caledonian University: ref no: HLS/NCH/19/054. Survey participants were asked to check a box if they would potentially take part in an interview to examine their experiences of lockdown and social distancing. To address self-selected bias of participants with MH issues being more likely to participate in those interviews, purposive sampling was used to identify interviewees from all potential participants, in three MH experience groups;
men who reported poor MH and had used MH online resources during lockdown,
men who reported poor MH and had not used MH online resources during lockdown,
men who reported good MH but nevertheless had used MH online resources during lockdown.
Maximum variation sampling (see Palinkas et al., Citation2015) was then used to obtain a diverse range of individuals by stratifying and recruiting potential participants across different gender, sexual identity, ethnicity, employment and living situation changes (experienced during the first COVID-19 lockdown), attempting to recruit equal numbers across the three MH experience groups.
An interview topic guide was used to facilitate discussion regarding men’s experiences of MH and MH help seeking during the first COVID-19 lockdown. Interviews were independently conducted by four authors of the paper (JF, PF, RM, DS). Interviewers were all white, cis-gendered and included both gay/straight and female/male researchers. DS led the analysis with support from PF.
Qualitative data analysis
The 18 interviews were transcribed verbatim, anonymised and imported into NVIVO 12 for analysis. Deductive thematic analysis (Braun & Clarke, Citation2013) was employed to address RQ2, to identify the self-perceived barriers and facilitators to GBMSM’s MH help-seeking behaviour during the first COVID-19 lockdown in Scotland.
Behaviour change wheel approach
To address RQ3, the barriers and facilitators to MH help-seeking were further analysed using the Behaviour Change Wheel (BCW) approach (Michie, Atkins, & West, Citation2014) by DS and verified by PF. The BCW was developed to provide a comprehensive, evidence-based, and theoretically informed guide to behaviour change. The BCW brings together 19 frameworks of behaviour change, each of which places greater emphasis on different drivers of behaviour. For example, some of these frameworks assume that behaviour is driven by beliefs and perceptions, while others highlight the role of the social environment in behaviour. By synthesising the core drivers of behaviour, the BCW adopts a holistic perspective, providing a model broad enough to be applied to any behaviour and setting (Michie et al., Citation2014).
Barriers and facilitators were conceptualised in behavioural terms, checking they relate to the prevention or facilitation of MH help-seeking by GBMSM. Then each of the identified barriers and facilitators were mapped to the Capability, Opportunity, Motivation - Behaviour (COM-B) model components (West & Michie, Citation2020) and corresponding Theoretical Domains Framework (TDF) domains (Atkins et al., Citation2017; Cane, O’Connor, & Michie, Citation2012). Next, the corresponding intervention functions were systematically selected to align with the selected TDF domains. Finally, we considered which Behaviour Change Techniques (BCTs) (Michie et al., Citation2013) could best operationalise the intervention functions, then generated draft recommendations which sought to systematically reduce the barriers we had identified and build on any facilitatory factors to enable GBMSM-facing organisations, services and online resources to meet unmet needs and enhance GBMSM’s MH help-seeking behaviours.
Synthesis of findings to generate service provider and research recommendations
Following independent quantitative and qualitative data analysis, the key findings of each study were combined in a single matrix, to generate recommendations for clinical practice, community-based organisations, and future research. These initial recommendations were further synthesised by DS, PF, JF, and RMc (see Online Appendix, Table A3). Discussion enabled these authors to reach consensus and the final recommendations were further categorised as short, medium, or long-term (Table A3). For ease of reading, the final recommendations are presented within the discussion section of this paper.
Findings
Quantitative findings
RQ1: What are the key sociodemographic and psychological factors predicting MH help-seeking among GBMSM during the first COVID-19 lockdown in UK and Republic of Ireland?
Demographic characteristics
1368 of 1801 the SMMASH-Pan survey participants completed the MH resources questions and are included in the analysis. Demographic characteristics are shown in . The average age of participants was M = 41.5 years (SD = 13.5) with the largest sub-group aged 46+ (40.1%, n = 549). Almost all men identified themselves as gay or bisexual (98.5%, n = 1348). Most participants were living in Scotland (47.5%, n = 650) followed by England (21.0%, n = 287) and the Republic of Ireland (19.2%, n = 262), with fewer from Wales (7.5%, n = 103) and Northern Ireland (4.6%, n = 63). The vast majority self-identified as white (97%, n = 1327), most (88.1%, n = 1205) reported post-secondary school education and over one-third (37.7%, n = 516) were living alone at the time of participation. Overall, 38.3% (n = 520) reported ever receiving a MH diagnosis from a doctor, 35.9% (n = 470) were assessed as experiencing moderate to severe depression and 23.9% (n = 309) moderate to severe anxiety in the past 2 weeks. Although relatively few (8%, n = 109) men said that their physical health was poor/very poor, over one quarter (26.5%, n = 353) reported poor or very poor MH at the time of participating in the survey. Correspondingly, 21.7% (n = 297) of men reported using remote MH resources during lockdown.
Table 1. Demographic characteristics for all SMMASH-Pan Participants.
Cumulatively 44.9% (n = 583) of participants reported either recent moderate/severe anxiety or depression or self-reported poor MH during the first COVID-19 lockdown. Amongst these men, just under one-third (31.4%, n = 183) had used remote MH resources since the start of the COVID-19 pandemic.
Predictors of remote MH help-seeking during the first COVID-19 lockdown
presents the results of the backwards binary logistic regression analysis to predict remote MH help-seeking behaviour among GBMSM during lockdown. Variables entered into the constant model were age, education, self-perceived MH, ethnicity, self-perceived health, PHQ-9 depression, GAD-7 anxiety, lifetime MH diagnosis, living situation and sexual orientation. As shows, the predictive independent variables included in the final model, that was set in 9 steps, were MH diagnosis and anxiety. This means that men suffering from moderate/severe anxiety and those having received a MH diagnosis in the past were more likely to report seeking help for MH issues since the start of the COVID-19 lockdown. None of the remaining variables were significant predictors of MH help-seeking in the final model. The internal validity of the model was good (Hosmer–Lemeshow = 0.26, p > 0.05, confirming goodness of fit).
Table 2. Constant only & final logistic regression model – coefficients of the model predicting MH help-seeking behaviour among GBMSM in the SMMASH-PAN study.
Qualitative findings
RQ2: What are the barriers and facilitators to MH help-seeking among GBMSM in Scotland?
When discussing barriers and facilitators to MH help-seeking, qualitative interview participants distinguished between accessing online resources (specifically, websites and apps) and ‘GBMSM-facing’ organisations. Therefore, we use this distinction to structure our analysis as shown below.
Barriers and facilitators of MH help-seeking from GBMSM-facing organisations during the first COVID-19 lockdown
Multiple barriers and facilitators to men’s MH help-seeking from GBMSM-facing organisations were identified (see ). Participants’ lack of knowledge about GBMSM-facing organisations and their lack of confidence to seek help from such organisations were described as major barriers impacting their help-seeking behaviour across our data. For example, men’s lack of knowledge around GBMSM-facing organisations is summarised below:
In terms of mental health and gay men, I had no idea that there were specific charities for that. I always thought, well, I’m gay, I have sex with men, if I did have a mental health issue and I wanted to speak to somebody about it I would just phone like a Samaritans or whatever, you know. It didn’t occur to me that there are specific charities that deal with gay men with those issues. I didn’t even know they existed, if I’m honest.
Table 3. Key barriers & facilitators to GBMSM’s MH help-seeking from GBMSM-facing Organisations & Online Resources.
As a gay man, I don’t really feel all the sexual health obsession helps me as a gay man. It would help a lot more to be given more mental health support that goes beyond just handing out free condoms (at a gay) festival. I don’t want that. I want to be able to feel that I can actually have that conversation with somebody and express myself in a way that makes sense.
So, I think there probably are barriers to accessing (counselling) but I think some of those barriers are like internal in terms of not recognising the benefit that therapy might have.
I know there would be nothing bad about asking for help, it’s just one of those things like I don’t want to do it.
So, you put all this effort into (a counsellor) who you know who is heterosexual, has different values than you do, and a different reasoning. You tend to hold back, you know, whereas (with) a gay man, or a … probably a gay man, I would be much more relaxed and able to talk to him in a way that it is easier for me to talk to him without having these other thoughts of … well, ‘I said that’ and then, if they are, you know, straight, then they would think that’s awful. They may not necessarily think that, but this is what I think they think.
I go along to those (GBMSM-facing organisations) and feel like I’m understood quite well there because it’s a space where I can be (accepted) as a disabled person and as a queer person and that really feels nice to have that.
Barriers and facilitators to MH help-seeking using online resources during the first COVID-19 lockdown
Our analysis identified three key barriers hindering men’s MH help-seeking using online resources; men distinguished between apps and websites, so we use this definition herein (see ). GBMSM described (1) the lack of a tailored and person-centered approach employed by MH apps, (2) their perceptions of the likely low efficacy of online resources and (3) their belief that they are resourceful in themselves, as described below.
I wasn’t feeling the benefits (of a mental health app), enough, quick enough, so I don't know, I probably just gave up with that. So yeah, I wouldn’t really say that helped, but I did try it to begin with.
I have an app that I sometimes use on, I forget what it’s called, it’s like a mindfulness app. But I get sort of frustrated with these things when it tells you how to think and breathe. I think, ‘Oh I’d much rather go for a walk actually’ and think myself. So I guess I am sort of resourceful myself in some ways’.
Maybe if, you know, at (Hospital) or (MH organisation) someone I was seeing, some therapist, introduced me to an app and told me about it, I might have more interest.
I was really distressed and I was looking for places, if … you went onto their site and there was bullet-point, bullet-point, bullet-point, that could then maybe help … does that make sense? ‘That’s the course of action I want to go down’ … If there was something there to go, ‘bang, bang, bang, (That’s) what to do’. And then also you’ve got to be discreet, … , they don’t want it in their face, they just need somewhere to look (for) help.
I think sometimes particularly going to sleep, like I listen to the sleep cast function (of the app) on that just … to distract my conscious mind as I'm going to sleep. And I find that can be quite helpful to listen to something soothing as I drift off.
Behaviour Change Wheel analysis
RQ3: What are the preliminary recommendations to enable services to enhance MH help-seeking among GBMSM?
Our analysis of the key barriers and facilitators to GBMSM’s MH help-seeking separately addresses (1) online resources and (2) GBMSM-facing organisations during the first COVID-19 lockdown. Tables A1 & A2 (in the online appendix) show our BCW analysis in detail.
Behavioural Domain: ‘GBMSM seek help for MH issues using online resources during the first COVID-19 lockdown
Key barriers and facilitators to MH help-seeking using online resources were linked to either reflective motivation (n = 3 barriers/facilitators) or physical opportunity (n = 3) within the COM-B model (see Table A1, in online appendix), meaning they were related to GBMSM’s motivation to perform the behaviour or the physical environment where the behaviour occurred, respectively. Next, the TDF was used to expand the COM-B components, acknowledging the explicit links between COM-B and the TDF; five of the 14 TDF domains were identified as being particularly important in relation to the barriers and facilitators to online help-seeking for MH. The majority of barriers and facilitators were theorised as relating to ‘Environmental context and resources’ (n = 3) and the ‘Beliefs about consequences’ (n = 2) domains. Corresponding ‘functions’ were then selected based on their resonance with the relevant TDF domains. In particular, four different intervention functions (Environmental restructuring (n = 3), Enablement (n = 3), Education (n = 3), Persuasion (n = 3)) were identified as likely to be useful in enhancing GBMSM’s MH help-seeking behaviour using online resources.
The penultimate step was to select BCTs that operationalised these intervention functions. BCTs selected to address the barriers and facilitators to MH help-seeking behaviour included ‘restructuring the physical environment’, ‘information about social and environmental consequences’, ‘information about emotional consequences’, ‘credible source’, ‘social support (unspecified)’, ‘framing/reframing’, ‘identity associated with changed behaviour’, and ‘incompatible beliefs’. Overall, these BCTs related to the broader BCT grouping ‘antecedents’ (n = 3), ‘natural consequences’ (n = 3), ‘associations’ (n = 3), ‘social support’ (n = 1), and ‘identity’ (n = 1).
Finally, by bringing together these BCTs, theoretically driven and systematic recommendations were generated that are expected to increase GBMSM’s help-seeking behaviour with the use of online resources (see final column, Table A1, in online appendix).
Behavioural Domain: ‘GBMSM seek help for MH issues from GBMSM-facing organisations during the first COVID-19 lockdown’
This same process was used to generate theoretically driven and evidence-based recommendations likely to enhance GBMSM’s MH help-seeking from GBMSM-facing organisations. Barriers and facilitators were mapped to the COM-B model as follows: reflective motivation (n = 7), followed by physical opportunity (n = 3), social opportunity (n = 2), and psychological capability (n = 2) (see Table A2, in online appendix). Using the TDF, these barriers and facilitators were theorised as relating to environmental context and resources (n = 7); professional/social role and identity (n = 4); cognitive and interpersonal skills (n = 1); social influences (n = 2); knowledge (n = 1); beliefs about capabilities (n = 1); intentions (n = 1); and beliefs about consequences (n = 1). Drawing on this analysis, the intervention functions seen as more likely to be effective in bringing about enhanced help-seeking behaviour with GBMSM-facing organisations were persuasion (n = 6), education (n = 5), environmental restructuring (n = 5), enablement (n = 2), modelling (n = 2), and training (n = 1).
Several BCTs were then identified based upon the selected intervention functions; ‘information about other’s approval’, ‘identification of self as role mode’, ‘restructuring the social environment’, ‘information about social and environmental consequences’, ‘demonstration of a behaviour’, ‘instruction on how to perform a behaviour’, ‘feedback on the behaviour’, ‘framing/reframing’, ‘information about emotional consequences’, ‘prompts/cues’, ‘focus on past success’, ‘imaginary reward’, ‘identity associated with changed behaviour’, and ‘incompatible beliefs’. These recommended BCTs related to the broader BCT groupings of ‘comparison of behaviour’ (n = 8), ‘natural consequences’ (n = 7), ‘identity’ (n = 5), ‘antecedents’ (n = 5), ‘shaping knowledge’ (n = 1), ‘feedback and monitoring’ (n = 1), ‘associations’ (n = 1), ‘self-belief’ (n = 1), ‘covert learning’ (n = 1).
Finally, the last column of Table A2 (see online appendix) illustrates the end product of our analyses and details the way behaviour change techniques could be operationalised to boost GBMSM’s MH help-seeking behaviour and enable GBMSM-facing organisations to address unmet needs both during the COVID-19 pandemic and, crucially, afterwards.
Discussion
This is the first sequential mixed-methods study worldwide to examine MH help-seeking among GBMSM during the COVID-19 pandemic. For the first time, we have explored factors affecting GBMSM’s MH help-seeking behaviours during the pandemic in the U.K. and Republic of Ireland and identified barriers and facilitators to MH help-seeking among GBMSM in Scotland. By applying the BCW approach (Michie et al., Citation2014) we also performed a comprehensive analysis of the factors affecting MH help-seeking behaviours and systematically identified evidence and theory-based preliminary recommendations aimed at enhancing GBMSM’s MH help-seeking behaviours. The aim of this discussion is to examine and synthesise the key findings to generate short, medium, and long-term recommendations for clinical practice, NHS, GBMSM-facing and MH services, online resources, and future research (see ).
Table 4. Short, medium & long-term recommendations to improve MH help-seeking among GBMSM in the U.K..
Short, medium & long-term recommendations
Our short-term recommendations mainly focus upon raising GBMSM’s awareness around existing evidence-based resources that can improve their MH, increasing the visibility of MH services appropriate to GBMSM, such that diverse GBMSM and those with new MH problems are reached. To these ends, we recommend services’ branding is inclusive and visibly welcoming to all GBMSM by celebrating diversity of services users and, where possible, staff (see ).
In the medium term (see ) we recommend a holistic and collaborative approach between researchers, communities, GBMSM-facing organisations, and MH services is adopted to develop MH resources for GBMSM. This includes identifying and promoting existing high quality MH resources, especially materials and apps appropriate to GBMSM’s needs. GBMSM and MH ambassadors could fruitfully cooperate at different levels to promote and support (i) MH help-seeking, (ii) MH resources and organisations and (iii) high-quality evidence-based MH apps, using personal testimonials from community members. Significant others, such as peers and partners, could also play a role in enhancing GBMSM’s confidence and self-efficacy in MH help-seeking. Moreover, it is suggested that GBMSM-facing organisations endorse a more holistic rather than a sexual health focus by (i) rebranding their services to explicitly promote MH issues, (ii) developing and delivering a GBMSM staff training package for generic MH and wider services, (iii) promoting high-quality MH apps suitable to GBMSM, and (iv) adapting outreach activities to promote MH. GBMSM-facing organisations should also ensure their MH services are promoted as widely as possible and include digitally excluded GBMSM when services are delivered remotely. Future research should explore those factors affecting the MH of GBMSM and, critically, their interaction with other health inequalities which produce syndemic ill-health among GBMSM (McDaid et al., Citation2020). Social and discrete spaces should be developed for physical and digital services, whilst communicating MH issues via webinars and short briefings will ensure consistency across the sectors. It is proposed that future mass and social media campaigns advertise personal testimonials of MH service use that explain how to successfully access services, and GBMSM-tailored resources need to be developed that support GBMSM with poor MH. Finally, and perhaps most importantly, MH help-seeking among GBMSM should be framed as normative, while MH maintenance should be re-framed as a long-term commitment rather than a ‘quick fix’.
Our long-term recommendations advocate an inclusive MH approach be promoted across different organisational levels that emphasises the importance of MH awareness and maintenance for all. Raising awareness about GBMSM’s MH should also be prioritised across different services, given the unique multiple vulnerabilities (i.e. syndemics) of the GBMSM population. Based on our recommendations, researchers should collaborate with GBMSM communities, GBMSM-facing and MH organisations alongside app designers to both endorse an asset-based approach towards GBMSM’s MH and co-produce MH apps tailored to GBMSM’s needs. The effectiveness and efficacy of these newly designed MH apps should be further examined within RCT interventions. Boldly, we propose that GBMSM could be guided to re-frame their identity as ‘MH maintainers’, that is someone who actively engages in activities to maintain their MH. Finally, further work is needed to ensure that generic U.K.-based MH organisations are GBMSM friendly whilst, where possible, national-level services should celebrate of diversity of their staff to promote diversity and inclusivity (see ).
Importance and implications of the results
The results of the quantitative analysis suggest that men experiencing recent anxiety and those with a previous MH diagnosis were most likely to access MH resources during the COVID-19 lockdown, regardless of any socio-demographic variables. Thus, it is important to enhance access to resources for those men with recent depression and those experiencing new, undiagnosed mental health problems. The latter are particularly challenging to identify, but prioritising GBMSM as a vulnerable population alongside promoting the importance of mental health awareness and maintenance for all GBMSM would begin to address this issue. Our qualitative analysis identified a series of issues, across individual and contextual factors, that GBMSM said influenced their help-seeking behaviour from online MH resources and GBMSM-facing organisations. These factors must be acknowledged by the relevant organisations, in order to develop more tailored and inclusive approaches that reach a larger, more diverse group of GBMSM.
Limitations and future research recommendations
The key strength of this study is its originality; this is the first study to examine barriers and facilitators to MH help-seeking among GBMSM globally during the COVID-19 pandemic. The mixed-methods design strengthens research rigour, compensating the shortcomings of each individual methodology. In addition, employing the BCW approach enabled us to draw upon a wealth of prior theoretical work to assist with the systematic development of recommendations to enhance GBMSM’s engagement with MH services (Michie et al., Citation2014). However, the inherent limitations of cross-sectional research, our hybrid online/offline sampling frame, as well as the sample demographic characteristics, limited generalisability of these data; most participants were highly educated, self-identified as gay and our 5 countries were unequally represented. Moreover, another limitation concerns the skewed age of our sample and the subsequent utilisation of remote, especially online, resources that may differ by age. Similarly, recruiting interview participants only in Scotland, albeit a diverse, theory-driven sample, potentially limited the transferability of these qualitative findings. Although the use of social media resources to recruit participants yielded rapid results and provided anonymity in questionnaire and interview responding, it could also have biased the sample towards individuals utilising technology for support already. Due to funding limitations, this study did not include follow-up data collection during subsequent U.K. lockdowns. However, it is likely that MH and gay facing organisations implemented a number of these recommendations over the course of the pandemic. Similarly, as the pandemic continued, GBMSM may have shifted their help-seeking behaviours to utilise more online resources, and this is not reflected in the findings of this study. In addition, selection of intervention functions and BCTs is inevitably subject to some interpretation by the authors. This could be addressed if, for example, follow-up interviews with GBMSM were conducted, where men were asked to gauge which BCTs were most likely to be successful in improving their MH help-seeking behaviour. Finally, although remote help-seeking examined herein included the use of MH apps and websites, online support groups and telehealth, that are potentially other important ways to meet GBMSM's mental health needs, were not examined.
Finally, we have presented a range of systematic and theoretically informed recommendations to increase GBMSM’s engagement with MH resources, including GBMSM-facing organisations and online resources, developed herein with the use of the BCW approach. As such, they are ready to be implemented into practice. Our next step is to use these recommendations to develop a focused intervention that will aim to improve the MH of GBMSM in Scotland during and beyond COVID-19. We will review the feasibility and appropriateness of these recommendations against the APEASE criteria (Affordability, Practicability, Effectiveness/Cost-Effectiveness, Acceptability, Safety and Equity) with the help of expert key stakeholders and GBMSM (Michie et al., Citation2014), then employ follow-up qualitative interviews with GBMSM, GBMSM-facing, and MH service providers to gauge BCT feasibility and potential efficacy, in order to further enhance the rigour of these recommendations.
Ethical approval
Nursing Department Research Ethics Committee, Glasgow Caledonian University (HLS/NCH/19/050; HLS/NCH/19/054).
Supplemental Material
Download MS Word (50.3 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 Services for whom a key remit is to work with GBMSM or who identify GBMSM as one of their key client groups.
References
- Atkins, L., Francis, J., Islam, R., O’Connor, D., Patey, A., Ivers, N., … Grimshaw, J. M. (2017). A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implementation Science, 12(1), 77.
- Bavinton, B. R., Chan, C., Hammoud, M. A., Maher, L., Haire, B., Degenhardt, L., … Prestage, G. P. (2022). Increase in depression and anxiety among Australian Gay and bisexual men during COVID-19 restrictions: Findings from a prospective online cohort study. Archives of Sexual Behavior, 51, 355–364. doi:10.1007/s10508-021-02276-2
- Bradford, S., & Rickwood, D. (2014). Adolescent's preferred modes of delivery for mental health services. Child and Adolescent Mental Health, 19(1), 39–45.
- Braun, V., & Clarke, V. (2013). Successful qualitative research: A practical guide for beginners sage. London: Sage Publications Ltd.
- Cane, J., O’Connor, D., & Michie, S. (2012). Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science, 7(1), 37. doi:10.1186/1748-5908-7-37
- Cheesmond, N. E., Davies, K., & Inder, K. J. (2019). Exploring the role of rurality and rural identity in mental health help-seeking behavior: A systematic qualitative review. Journal of Rural Mental Health, 43(1), 45–59. doi:10.1037/rmh0000109
- Coleman, S. J., Stevelink, S. A. M., Hatch, S. L., Denny, J. A., & Greenberg, N. (2017). Stigma-related barriers and facilitators to help seeking for mental health issues in the armed forces: A systematic review and thematic synthesis of qualitative literature. Psychological Medicine, 47(11), 1880–1892.
- Collin, P. J., Metcalf, A. T., Stephens-Reicher, J. C., Blanchard, M. E., Herrman, H. E., Rahilly, K., & Burns, J. M. (2011). Reachout. Com: The role of an online service for promoting help-seeking in young people. Advances in Mental Health, 10(1), 39–51.
- Dean, E. (2017). Scotland's new mental health strategy. Mental Health Practice (2014), 20(9), 10.
- Divin, N., Harper, P., Curran, E., et al. (2018). Help-seeking measures and their use in adolescents: A systematic review. Adolescent Resarch Review, 3, 113–122. doi:10.1007/s40894-017-0078-8
- Firth, J., Torous, J., Nicholas, J., Carney, R., Pratap, A., Rosenbaum, S., & Sarris, J. (2017b). The efficacy of smartphone-based mental health interventions for depressive symptoms: A meta-analysis of randomized controlled trials. World Psychiatry, 16, 287–298. doi:10.1002/wps.20472
- Firth, J., Torous, J., Nicholas, J., Carney, R., Rosenbaum, S., & Sarris, J. (2017a). Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. Journal of Affective Disorders, 218, 15–22. doi:10.1016/j.jad.2017.04.046
- Frankis, J., Strongylou, D., & Kincaid, R. (2020). How has Covid-19 social distancing amplified the mental health vulnerabilities of gay, bisexual and other men who have sex with men (GBM)? COV/GCU/20/10, Rapid Research in Covid-19 programme (RARC-19). https://www.cso.scot.nhs.uk/wp-content/uploads/COVGCU2010-1.pdf
- Gál, É, Ștefan, S., & Cristea, I. A. (2021). The efficacy of mindfulness meditation apps in enhancing users’ well-being and mental health related outcomes: A meta-analysis of randomized controlled trials. Journal of Affective Disorders, 279, 131–142.
- Galdas, P. M., Cheater, F., & Marshall, P. (2005). Men and health help-seeking behaviour: Literature review. Journal of Advanced Nursing, 49(6), 616–623.
- Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry, 10(1), 1–9.
- Hoffberg, A. S., Stearns-Yoder, K. A., & Brenner, L. A. (2020). The effectiveness of crisis line services: A systematic review. Frontiers in Public Health, 7, 399.
- Holloway, I. W., Garner, A., Tan, D., Ochoa, A. M., Santos, G. M., & Howell, S. (2021). Associations between physical distancing and mental health, sexual health and technology use among gay, bisexual and other men who have sex with men during the COVID-19 pandemic. Journal of Homosexuality, 68(4), 692–708.
- Kauer, S. D., Mangan, C., & Sanci, L. (2014). Do online mental health services improve help-seeking for young people? A systematic review. Journal of Medical Internet Research, 16(3), e66.
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613.
- Levis, B., Benedetti, A., Thombs, B. D., & DEPRESsion Screening Data (DEPRESSD) Collaboration. (2019). Accuracy of patient health questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ (Clinical research ed.), 365, l1476. doi:10.1136/bmj.l1476
- Manea, L., Gilbody, S., & McMillan, D. (2015). A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. General Hospital Psychiatry, 37(1), 67–75.
- McDaid, L., Flowers, P., Ferlatte, O., McAloney, K., Gilbert, M., & Frankis J. (2020) Informing theoretical development of salutogenic, asset-based health improvement to reduce syndemics among gay, bisexual and other men who have sex with men: Empirical evidence from secondary analysis of multi-national, online cross-sectional surveys. Social Science and Medicine: Population Health, 10(4). doi:10.1016/j.ssmph.2019.100519
- McDermott, E. (2015). Asking for help online: Lesbian, gay, bisexual and trans youth, self-harm and articulating the ‘failed’self. Health, 19(6), 561–577.
- McGarty, A., McDaid, L., Flowers, P., Riddell, J., Pachankis, J., & Frankis, J. (2021). Mental health, potential minority stressors and resilience: Evidence from a cross-sectional survey of gay, bisexual and other men who have sex with men within the Celtic nations. BMC Public Health, 21(1), 1–15.
- Michie, S., Atkins, L., & West, R. (2014). The behaviour change wheel. A guide to designing interventions (1st ed.). Great Britain: Silverback Publishing. p. 1003–1010
- Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., … Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95.
- Moore, S. E., Wierenga, K. L., Prince, D. M., Gillani, B., & Mintz, L. J. (2021). Disproportionate impact of the COVID-19 pandemic on perceived social support, mental health and somatic symptoms in sexual and gender minority populations. Journal of Homosexuality, 68(4), 577–591.
- Murphy, M. P. (2020). COVID-19 and emergency eLearning: Consequences of the securitization of higher education for post-pandemic pedagogy. Contemporary Security Policy, 41(3), 492–505.
- Palinkas, L. A., Horwitz, S. M., Green, C. A., Wisdom, J. P., Duan, N., & Hoagwood, K. (2015). Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Administration and Policy in Mental Health and Mental Health Services Research, 42(5), 533–544.
- Peterson, Z. D., Vaughan, E. L., & Carver, D. N. (2020, October 5). Sexual identity and psychological reactions to COVID-19. Traumatology. Advance Online Publication, doi:10.1037/trm0000283
- Pierce, B. S., Perrin, P. B., Tyler, C. M., McKee, G. B., & Watson, J. D. (2021). The COVID-19 telepsychology revolution: A national study of pandemic-based changes in U.S. Mental health care delivery. American Psychologist, 76(1), 14–25. doi:10.1037/amp0000722
- Planey, A. M., Smith, S. M., Moore, S., & Walker, T. D. (2019). Barriers and facilitators to mental health help-seeking among African American youth and their families: A systematic review study. Children and Youth Services Review, 101, 190–200.
- Prestage, G., Hammoud, M., Jin, F., Degenhardt, L., Bourne, A., & Maher, L. (2018). Mental health, drug use and sexual risk behavior among gay and bisexual men. International Journal of Drug Policy, 55, 169–179.
- Pretorius, C., Chambers, D., & Coyle, D. (2019). Young people’s online help-seeking and mental health difficulties: Systematic narrative review. Journal of Medical Internet Research, 21(11), e13873.
- Rathbone, A. L., Clarry, L., & Prescott, J. (2017). Assessing the efficacy of mobile health apps using the basic principles of cognitive behavioral therapy: Systematic review. Journal of Medical Internet Research, 19(11), e399.
- Read, J., & Cain, A. (2013). A literature review and meta-analysis of drug company–funded mental health websites. Acta Psychiatrica Scandinavica, 128(6), 422–433.
- Reavley, N. J., & Jorm, A. F. (2011). The quality of mental disorder information websites: A review. Patient Education and Counseling, 85(2), e16–e25.
- Rickwood, D., Deane, F., Wilson, C., & Ciarrochi, J. (2005). Young people’s help-seeking for mental health problems. Australian e-Journal for the Advancement of Mental Health, 4(3), 3–34.
- Rickwood, D., Thomas, K., Bradford, S., & The Sax Institute. (2012). Help-seeking measures in mental health: A rapid review. https://www.saxinstitute.org.au/wp-content/uploads/02_Help-seeking-measures-in-mental-health.pdf
- Rogers, M. A., Lemmen, K., Kramer, R., Mann, J., & Chopra, V. (2017). Internet-delivered health interventions that work: Systematic review of meta-analyses and evaluation of website availability. Journal of Medical Internet Research, 19(3), e7111.
- Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097.
- Suen, Y. T., Chan, R. C., & Wong, E. M. Y. (2020). Effects of general and sexual minority-specific COVID-19-related stressors on the mental health of lesbian, gay, and bisexual people in Hong Kong. Psychiatry Research, 292, 113365.
- West, R., & Michie, S. (2020). A brief introduction to the COM-B Model of behaviour and the PRIME theory of motivation [v1]. Qeios.
- Wu, C. Y., & Lee, M. B. (2021). Suicidality, self-efficacy and mental health help-seeking in lesbian, gay, bisexual and transgender adults in Taiwan: A cross-sectional study. Journal of Clinical Nursing, 30(15-16), 2270–2278.
- Xu, Z., Huang, F., Kösters, M., Staiger, T., Becker, T., Thornicroft, G., & Rüsch, N. (2018). Effectiveness of interventions to promote help-seeking for mental health problems: Systematic review and metaanalysis. Psychological Medicine, 48, 2658–2667. doi:10.1017/S0033291718001265
- Zay, H., Tam, M. K., Au, C. L., Yeoh, S. Y., Tan, G., Lee, M. M., … V, V. (2021). Barriers and facilitators to professional mental health help-seeking behavior: Perspective of Malaysian LGBT individuals. Journal of LGBTQ Issues in Counseling, 15(1), 38–58.