
Abstract
Grandparents may often be involved in childcare and in some settings, may be a primary caregiver. It may be assumed that as grandparents have raised their own children, their capabilities in terms of child care have been achieved through such experience. However, experience does not necessarily equate to expertise. Parenting interventions have beneficial effects for both parent and child outcomes. If such skills can be taught to parents, they may also be of benefit to grandparents. This systematic review explores the evidence base on parenting interventions for grandparents. The aim is to examine the implications of parenting interventions on outcomes for the grandparents, the parents and the child. A keyword data base search generated 191 manuscripts and eight studies met the criteria for inclusion. Overall, this review identifies relatively weak literature on interventions for grandparenting skills. Studies identified predominantly originated from the USA, and focused on the outcomes for the grandparents with sparse information on implications for the child or parent. However, despite such limitations, the studies all seem to report benefits of parenting interventions for grandparents. The interventions identified are varied and range from short to longer courses as well as support groups and home visits. As such, conclusions are limited. However, an enticing range of interventions with a growing evidence base of efficacy is seemingly emerging, laying the foundations for future studies honing the parenting provision for grandparents.
Public Interest Statement
Child care is an important factor in healthy child development with benefits to the child, the caregivers and society at large. Although grandparents play an increasing role in providing child care, there are very few attempts to include them in parenting training. Despite the fact that there is good evidence that parenting skills can be learned and are of benefit. This systematic review set out to examine grandparenting interventions in the global literature and to summarise the state of understanding. The findings show poor roll out of parenting training to grandparents, despite their role. This could easily be remedied with benefits to the child as well as the grandparents themselves.
1. Background
Children rely on a quality caretaking environment. They thrive best under optimum parenting conditions. Early studies have shown the long-term benefits of good parenting, and the effectiveness of interventions have been well explored (Barlow, Bergman, Kornør, Wei, & Bennett, Citation2016; Barlow, Smailagic, Huband, Roloff, & Bennett, Citation2014; Walker, Chang, Vera-Hernández, & Grantham-McGregor, Citation2011). Parents are usually the key providers of child care and their strategies, relationships and interactions are assumed to impact multiple aspects of child development (Carlo, Mestre, Samper, Tur, & Armenta, Citation2011; Coore Desai, Reece, & Shakespeare-Pellington, Citation2017; Gardner et al., Citation2017; Landry, Smith, & Swank, Citation2003). A longitudinal study in Jamaica provided clear evidence that good early child interventions had short- and long-term benefits on a number of key life outcome measures including development, education and career attainments in early adulthood (Samms-Vaughan, Citation2008; Walker et al., Citation2011). Given the importance of parenting, (Black et al., Citation2017) a number of initiatives have explored the question on whether parenting skills could be taught or improved. Interventions to improve parenting have evolved and a series of systematic reviews, both in resource rich (Barlow et al., Citation2014), and resource poor settings, (Knerr, Gardner, & Cluver, Citation2013; Sandler, Schoenfelder, Wolchik, & MacKinnon, Citation2011) have provided solid evidence on the efficacy of such interventions. Such parenting interventions have been targeted at population levels or targeted at subgroups of parents—such as those in poverty, or those with mental health difficulties (Hutchings et al., Citation2007; McDonald, FitzRoy, Fuchs, Fooken, & Klasen, Citation2012). For some the focus has been sub-groups of children (Furlong et al., Citation2010) such as those with conduct problems, antisocial behaviour (Piquero, Farrington, Welsh, Tremblay, & Jennings, Citation2009), disruptive behaviour (Burke et al., Citation2018) or attention deficit disorder (Zwi, Jones, Thorgaard, York, & Dennis, Citation2011) (Ogden & Hagen, Citation2008)
Child care is not confined to biological parents. Grandparents play a key role in child care. In some cultural settings, they are involved as primary caregivers (Clottey, Scott, & Alfonso, Citation2015; Yancura, Citation2013). In many other settings, a variety of factors have contributed to the growing role of grandparents in child care. As women enter the workforce, child care arrangements have very often involved grandparents (Di Gessa, Glaser, Price, Ribe, & Tinker, Citation2016). The growing costs of child care is also a factor in grandparent provision (Anderson, Liu, & Liao, Citation2013). Parental illness and death, such as in the HIV and Ebola epidemics has increased the role of grandparents in primary child care (Heymann, Earle, Rajaraman, Miller, & Bogen, Citation2007; Mhaka-Mutepfa, Cumming, & Mpofu, Citation2014). Legal proceedings and care orders may often involve grandparents as appointed caregivers. In some cultural settings, the extended family and especially the grandparents, create a social institution in which children are reared. In many low-income settings, the absence of sophisticated social welfare systems often results in the reliance on the family, notably grandparents, to care for children. The extended life expectancy and good health enjoyed by many older people may also contribute to caregiving availability. Close family ties and bonds with their grandchildren and the rewards of caregiving also play a role. Indeed active engagement and care responsibilities may potentially provide an upward intergenerational influence on cognitive ageing. In some cultural contexts, grandparents play a key role within the extended family and have specific child care responsibilities.
There may be assumptions that as grandparents have raised their own children, their capabilities in terms of child care have been achieved through such experience. However, if parenting skills can be taught to parents, it is important to explore whether such skills are also of benefit to grandparents. Research has explored the extent to which grandparenting can improve or impact upon the elderly in terms of psychological and physical health (Di Gessa, Glaser, & Tinker, Citation2016). Yet, there are fewer studies exploring the effects of grandparent care on a range of child outcomes. In the USA, some studies have provided a particular focus on nutrition outcomes for children and have concluded that grandparents play a role in poor dietary consumption patterns of some children (Pulgaron, Marchante, Agosto, Lebron, & Delamater, Citation2016). However, this is a narrow sphere of influence, and there may be a need for a wider understanding of grandparenting effects. There may well be positive gains for both the grandparents and the child from grandparenting care.
If grandparents are undertaking a major role in childcare, they too may benefit from parenting interventions. This systematic review was set up to explore the evidence base on parenting interventions for grandparents. The aim was to examine the impacts of such interventions examining outcomes for the grandparents, the parents and the child. The research question specifically aims to explore the extent of such provision globally, and the evidence of efficacy on multiple recipients.
2. Methods
2.1. Search strategy
A systematic literature review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher, Liberati, Tetzlaff, Altman, & Group, Citation2009) to identify studies reporting on parenting interventions for grandparents. Parenting interventions include all kinds of specific programmes to enhance parenting type skills. Data were obtained from a systematic databases conducted in March 2017 using keyword searches (see appendix 1.) Databases included within the study are PsycINFO (1872–2017), Medlline (1950–2017) and EMBASE (1947–2017). Keyword search terms used topics including; parenting, parenting intervention, grandparent and grandchild. References of relevant papers were also interrogated regarding inclusion and hand searching was undertaken. An additional 10 manuscripts were identified from these processes and screened for inclusion.
2.2. Criteria for inclusion and exclusion
All studies were sorted for inclusion. The criteria for inclusion for studies included in this review were original research manuscripts reporting on quantitative data and a parenting intervention for grandparents, which was assessed against a comparison or control group or via pre-post methods. Grandparents was interpreted widely and all studies mentioning a grandparent—whatever the relationship—were eligible. Studies were included if they provided information on a programme, had pre- and post-outcome measures for either the grandparent, the parent or the child. Inclusion was considered for randomized controlled trials, pre-post designs, repeated measures and before and after studies. Non-English language manuscripts, books, unpublished theses and case reports were excluded. An initial screen was conducted based on abstracts, and a subsequent full screen on full text articles was carried out. Although grandparents were mentioned in the key words, on examination many papers were not relevant to the core research question of grandparenting interventions. Screening was coordinated by a team of four psychologists and all possible manuscripts to be included were discussed. Four researchers were involved in screening abstracts and at least two authors looked independently at each one A final decision regarding all manuscripts was made by the first author after consulting with the full research team. There were no disagreements in the final inclusion group. See Figure for the process of inclusion within the review.
Figure 1. Flow chart: Parenting interventions for grandparents systematic review—paper inclusion
2.3. Data extraction
Data extraction was carried out according to a standardised data extraction sheet for all articles. Data extraction was carried out by two researchers with double checking to agree content. Information extracted from all relevant studies included, publication details, study method, place, sample, intervention detail, details of measures and relevant findings. This information was then compiled into a single combined table. Eight manuscripts were identified in total for inclusion within the systematic review.
2.4. Quality assessment
The quality of the included studies was assessed using the Standard Quality Assessment Criteria for evaluating primary research papers (Kmet, Lee, & Cook, Citation2004). This assessment provided an overall view of the quality of the evidence and methods used to collect the data in the included studies. Two independent researchers reviewed the papers with any discrepancies discussed, increasing inter-rater reliability.
A summary score was totalled for each included paper, ranging from 0 to 1 with a minimum summary score of 0.75 to be attained for inclusion of the paper into a review (Kmet et al., Citation2004). Based on the boundaries outlined by Lee et al (Lee, Packer, Tang, & Girdler, Citation2008), 5 studies were given a strong status as summary scores were above 0.80 (Kirby & Sanders, Citation2014; Littlewood, Strozier, & Whittington, Citation2014; McCallion, Janicki, & Kolomer, Citation2004; N’zi, Stevens, & Eyberg, Citation2016; Zauszniewski, Musil, Burant, & Au, Citation2014) and three were deemed good as a summary score between 0.71 and 0.79 was totalled (Boon et al., Citation2009; Kelley, Whitley, & Sipe, Citation2007; Kelley, Yorker, Whitley, & Sipe, Citation2001). See Figure for the score set of each study.
Figure 2. Quality of data summary
2.5. Risk of bias
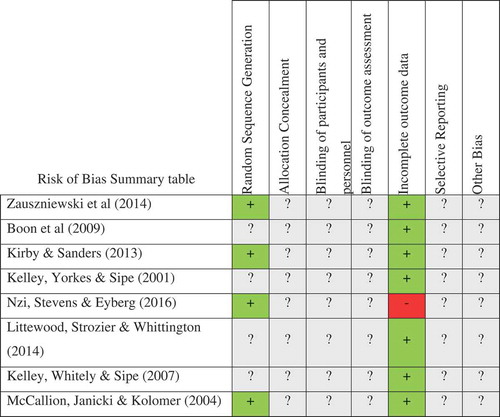
All studies included with the review were each independently examined for risk of bias, using the Cochrane assessment tool (Higgins et al., Citation2011). An informed analysis was made on random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other sources of bias. The studies were categorised into high, low or unclear risk of bias by two independent researchers with differences in judgement discussed between the authors.
2.5.1. Allocation
Many of the studies included did not need to use the random generation technique as they included a pre-post study design which led to half of the studies being classified as unclear (Boon et al., Citation2009; Kelley et al., Citation2007, Citation2001; Littlewood et al., Citation2014). The studies which overtly stated a randomised control trial procedure were deemed a low risk, however they did not detail the process used (Kirby & Sanders, Citation2014; McCallion et al., Citation2004; N’zi et al., Citation2016; Zauszniewski et al., Citation2014). All studies included were judged to be unclear due to the lack of detail provided. As mentioned, half of the studies included a pre-post test design, this meant allocation concealment was not applicable (Boon et al., Citation2009; Kelley et al., Citation2007, Citation2001; Littlewood et al., Citation2014).
2.5.2. Blinding
All eight studies, including four with a RCT design failed to comment on blinding within their methodology so all eight were categorised as unclear (Boon et al., Citation2009; Kelley et al., Citation2007, Citation2001; Kirby & Sanders, Citation2014; Littlewood et al., Citation2014; McCallion et al., Citation2004; N’zi et al., Citation2016; Zauszniewski et al., Citation2014). Following on from the previous statement made, all of the eight studies were judged unclear as they failed to comment on their blinding procedure (Boon et al., Citation2009; Kelley et al., Citation2007, Citation2001; Kirby & Sanders, Citation2014; Littlewood et al., Citation2014; McCallion et al., Citation2004; N’zi et al., Citation2016; Zauszniewski et al., Citation2014).
2.5.3. Incomplete outcome data
The majority of the included studies scored a low risk of bias as a detailed account was provided on attrition (Boon et al., Citation2009; Kelley et al., Citation2001; Kirby & Sanders, Citation2014; McCallion et al., Citation2004; Zauszniewski et al., Citation2014). Two studies, although of low risk, were ambiguous as they failed to provide any data on attrition so no missing outcome data was assumed (Kelley et al., Citation2007; Littlewood et al., Citation2014). (N’zi et al., Citation2016) findings were judged to be at a high risk as three participants in one condition failed to fully complete the assessment, which may have caused a bias in the results in an already participant deficient study.
2.5.4. Selective reporting
All eight studies were expectedly judged as unclear as no previous protocol information could be obtained (Boon et al., Citation2009; Kelley et al., Citation2007, Citation2001; Kirby & Sanders, Citation2014; Littlewood et al., Citation2014; McCallion et al., Citation2004; N’zi et al., Citation2016; Zauszniewski et al., Citation2014).
2.5.5. Other potential sources of bias
Each study was given an unclear status as potential sources of bias included differences in age and health ratings, previous access to support and the omission of data from grandfathers (Boon et al., Citation2009; Kelley et al., Citation2007, Citation2001; Kirby & Sanders, Citation2014; Littlewood et al., Citation2014; McCallion et al., Citation2004; N’zi et al., Citation2016; Zauszniewski et al., Citation2014).
The risk of bias assessments have been summarised in Figure .
Figure 3. Risk of bias summary table of studies included within the review
3. Results
From database searches, 191 hits were made, 39 duplicates were deleted and 152 manuscripts were screened in full, resulting in eight studies which met the criteria for inclusion, see Figure . Due to the heterogeneity of the data regarding populations, geographical settings, measures taken, outcomes, analyses and study reporting, meta-analysis was not possible. Therefore, characteristics of included studies and emerging findings are discussed narratively.
The studies were predominantly from the United States of America (n = 6) with one from South Africa and one from Australia. The data were based on 696 grandparents in total. All eight studies included grandmothers exclusively, while four studies included grandfathers as well—often in small numbers and rarely powered to disaggregate findings by gender. Six studies provided grandparent outcomes, four studies provided parent outcomes and four studies provided child outcomes, See Table for details. Only two studies provided outcomes for all three generations.
Table 1. Summary of inclusiveness of generational outcomes within the studies included within this review
Grandparenting interventions were varied in length and content. Table below sets out details of the intervention, methodology of the evaluation, and outcomes.
Table 2. Summary of 8 Grandparenting intervention studies, evaluation and outcomes
The interventions all differed in length—ranging from 4 sessions (Boon et al., Citation2009), 9 weeks (Kirby & Sanders, Citation2014), 6 months (Kelley et al., Citation2001), 7 sessions (N’zi et al., Citation2016), 1 year (Kelley et al., Citation2007), 2 years (Littlewood et al., Citation2014) and a 2 part case management and summer camp intervention (McCallion et al., Citation2004). The mode of delivery ranged from individual case work (Kelley et al., Citation2001; McCallion et al., Citation2004), home visits (Kelley et al., Citation2001; group work (Zauszniewski et al., Citation2014; Boon et al., Citation2009; Kirby & Saunders Citation2014)), coaching (N’zi et al., Citation2016) and summer camps (McCallion et al., Citation2004), provided by a range of providers including kin, social workers, nurses, trained workers, legal providers and supervised workers. The content and theoretical underpinnings were rarely in harmony with no underlying construct on the general needs of grandparents. Much of the focus was related to the impact of grandparenting on the mental health and wellbeing of the grandparent with not a single study interviewing the grandchildren. Indeed, only some of the studies included child outcome measures in their outcome variables, and these were confined to grandparent report rather than direct measurement.
The outcomes of interest across the studies covered 11 core concepts, measured in various ways. These included forms of support (measured in two studies), parenting inventories, measured in four studies, grandparent stress measured in four studies, relationship factors measured in two studies, grandparent depression measured in six studies, grandparent anxiety measured in two studies, quality of life measured in one study, communication measured in one study, child behaviour measured in three studies, coping measured in one study and satisfaction with the intervention measured in one study. The various validated scales used are set out in Table . Of note was the fact that there were very few overlap measurements other than the two different studies carried out by the same research group (Kelley et al., Citation2007, Citation2001). The Eyberg Child Behaviour Inventory (Eyberg & Pincus, Citation1999) was used in two studies. The most common measure across studies was that of depression, which was scored using various depression scales such as the CES-D; (Radloff, Citation1977), Depression Anxiety Stress Scale-21 (DASS; (Lovibond & Lovibond, Citation1995), Brief Symptom Inventory (Derogatis & Spencer, Citation1993); 2 studies); Beck Depression Inventory II (BDI-II; (Beck, Steer, & Brown, Citation1996).
A summary of the studies provides insight into the different contents, aims, structure, evaluation methodology and outcomes. (Boon et al., Citation2009) conducted their study in South Africa in the wake of the HIV and AIDS epidemic. They provided grandparenting training for 202 grandparents over 60 years of age, using a four-module intervention. These contained practical as well as parenting skills covering the grandparenting role as well as nursing needs. There were no control groups for this study and the analysis compared those who completed all four modules (n = 141) with those who did not. They combined non-attenders (n = 22) and partial attenders (n = 13) and follow up was available for 177 participants (88%) immediately post, and 182 (90%) at 3 months. The workshop attenders showed increases in positive attitudes and expressed an ability to deliver nursing care with greater endorsement. Of the 19 outcome measures, five were significantly improved at immediate follow up and three remained significantly improved three months later. The outcomes relating to communication, care and control had no effects.
Zauszniewski et al. (Citation2014 carried out a pilot study on 102 grandmothers in the USA, 40 of whom received resourcefulness training reinforced by expressive writing and verbal disclosure compared to those given expressive writing and verbal disclosure only, and an attention control group. They studied the effects on stress, depression and quality of life in a repeated measures design, with follow up from baseline at weeks 6, 12 and 18. The resourcefulness training was seen as being more effective in reducing depression and stress scores and increasing quality of life scores. No measures of the grandchildren they cared for were taken.
A programme specifically designed for grandparents was examined (Kirby & Sanders, Citation2014). This Australian study examined 54 grandparents with 12–20 h per week of childcare responsibilities. This study measured effects on the grandparents, the parents and the children. The sample was small but at short and longer term follow up the intervention group showed improvements in grandparent reported behaviour ratings of the child, their confidence in parenting, reduced levels of depression, anxiety and stress with the added benefit of improved relationship with the parents. The child behaviour reductions were also noted by the parents who had not been the direct recipients of the grandparenting intervention. The benefits largely sustained at longer term follow up.
Two studies by Kelley et al(Kelley et al., Citation2007, Citation2001) report on an exploratory study followed by a comprehensive intervention for grandmothers in the USA. The exploratory study on 24 grandparents showed some benefits from this varied intervention including social work home visits as well as legal resources. The report of a more fully developed home-based programme for 120 grandmothers and great grandmothers and a pre-post test design was used, which showed significant reductions in psychological distress, and increases in ratings of resources, social support, physical health and coping. No measures on the children were taken.
Another USA study (N’zi et al., Citation2016) piloted a twice weekly 8 session intervention using a randomized controlled trial design with a waitlisted control for a small sample of 14 grandmothers and great grandmothers. When compared to the waitlisted controls, there were noted effects, but not all completed the assessment in full and by 3 months the waiting list control had received the intervention and there was only follow up from 4 in the intervention group.
Outcomes related to mental health as well as child behaviour assessed by the grandparent. (Littlewood et al., Citation2014) explored the efficacy of an intervention using kin as teachers for a group of 83 grandparents in the USA. The pre- post-intervention comparisons showed a number of improvements over time but the follow up rate is not reported and the analysis appears to be confined to a sample of 30 grandparents.
In a USA study, McCallion et al. (Citation2004) studied 97 grandparents in New York specifically those caring for children with developmental disabilities. The group were divided into an intervention arm receiving case management and support group compared to a waiting list control. They reported significant reductions in depression scores and increases in empowerment and caregiving mastery assessments.
4. Discussion
Despite the acknowledged importance of grandparents in providing child care, there is a relatively weak literature on interventions for grandparenting skills. The studies identified in this review are very USA biased, concentrate on the outcomes for the grandparents with sparse information on the impact on the child or the parent. Notwithstanding, the studies all seem to report benefits, even in the presence of very small sample sizes and reduced follow up for some. The interventions are varied and range from short to longer courses as well as support groups and home visits. Thus, the conclusions from the literature in this review cannot provide any insight into ideal length, components, mode of delivery or intervention content.
There were a wide range of outcomes of interest—mostly measuring the grandparent and only a few monitoring the child outcomes. The most common measurement was grandparent depression, but studies also looked at other mental health issues such as stress, anxiety and quality of life; interaction and relationship issues such as support, parenting, communication and coping. Child behaviour was invariably measured by the grandparent report rather than objective or third-party appraisal. The exception to this was one study where the parent who had not been the target of the intervention also completed an appraisal of child behaviour. For all the studies, the samples were generally convenience samples with no insight into refusal rates or the population at large. Some concentrated on specific groups of grandparents such as those caring for a grandchild with disability, while others confined their recruitment according to time spent caring for the grandchild. Although no sub analysis was available, two studies included great grandparents and some referred to grandfathers—who tended to be so few that they were invariably excluded from the analysis.
There is little consensus or harmony among measurement, so meta analysis of outcomes is not possible and future research may need to examine domains of impact and aim at a consensus of measurement for cross study comparability.
Overall the studies provide a tantalising basket of potential interventions with an emerging evidence base of efficacy. Given the fact that grandparents play a very fulsome role in child care and thus in child development, this is an area of study which needs an improved evidence base and some much-needed attention. The evidence based on only eight studies and 696 grandparents cannot provide a confidant base from which to scale up such provision. This is in sharp contrast to the sound evidence base on parenting interventions with clear efficacy and an agreed concept of the core elements needed for effective intervention components. For many key outcomes in child development, behaviour and experience, there was limited or no data.
With parenting interventions the resounding bulk of the literature relates to mothers, but there is an emerging literature on fathers. For grandparents, the evidence is very skewed towards grandmothers and studies on grandfathers are wanting. Despite being included in some studies, the numbers are small, and the data are usually discarded or conflated. The important role of men in child development needs to be explored and grandfather inclusion should be considered in future studies.
The few studies that were available for review seem to suggest consistent benefits for the grandparents themselves in terms of their mental health and wellbeing as well as cautious evidence that this permeates to the child’s behaviour.
The literature base is generally impoverished and the various roles of grandparents cannot be disaggregated. Targeted or specific interventions may differ from generalised interventions. There also may be merit in understanding how the grandparenting role is undertaken and this may affect the intervention needs. For example grandparent care as a result of a court order may differ from grandparent care in the presence of parental illness or death. Full time responsibility for the child may also bring different challenges to part time caring responsibilities. Families may be viewed as social institutions and this is all the more so in contexts where there is limited public welfare systems or general social service provision. This is often in the poorest and most challenged settings, invariable in low-resource environments. In these contexts, grandparents traditionally play a key role, and they may be well suited to specific provision and intervention. Given the paucity of studies, there was no possibility of breaking down the review according to low-middle and high-resource settings. Future research in low-resource settings may be particularly needed. The nature of the grandparenting responsibility, whether it is sole care or supplemental care needs to be considered. The review shows benefits for the grandparents as well as the child. In this era of improved life expectancy, there may well be upward intergenerational considerations regarding the benefits of grandparenting and how such roles and responsibilities can influence cognitive aspects of ageing.
In all, the varied roles of grandparents need to be fully appreciated if grandparenting skills are to be enhanced and interventions tailored. Given the efficacy of parenting interventions, the gaps in terms of grandparenting are lamentable. Child wellbeing and family thriving needs to acknowledge and include the important role of grandparents. They have a key role to play, and this has potential to benefit multiple recipients such as the child, their parents and the grandparents themselves. Many more studies, with specific control for the variety of situations, contexts and environments are needed. If interventions for grandparents are to be rolled out in the same way as parenting interventions—especially at scale—more evaluation is crucial.
Ethical approval
The study is a systematic review and thus used only secondary published material with no requirement for ethical approval.
Informed consent
No direct contact with participants as this is a systematic review, and thus informed consent was not required. However, as part of the quality standard of the systematic review, ethical approval and consent measured are featured in the quality assessment.
Additional information
Funding
Notes on contributors
Lorraine Sherr
The authors are a team of Psychologists under the guidance of Prof Lorraine Sherr. The work was undertaken to expand the understanding of families, child care and optimum child development.
References
- Abidin, R. (1995). Parenting Stress Index–Manual (3rd.) Odessa, FL: PAR Psychological Assessment Resources.In: Inc .
- Achenbach, T. M., & Rescorla, L. (2001). ASEBA school-age forms & profiles. Burlington, VT: Aseba.
- Achenbach, T. M., & Rescorla, L. A. (2000). Manual for the ASEBA preschool forms & profiles: An integrated system of multi-informant assessment; Child behavior checklist for ages 1 ½–5; Language development survey; Caregiver-teacher report form. Burlington, VT: University of Vermont.
- Anderson, S. G., Liu, M., & Liao, M. (2013). Subsidized child care by grandparents: Profiles of caregivers in an emerging public service context. Journal of Women & Aging, 25(3), 242–259. doi:10.1080/08952841.2013.791599
- Arnold, D. S., O’leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The parenting scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5(2), 137. doi:10.1037/1040-3590.5.2.137
- Barlow, J., Bergman, H., Kornør, H., Wei, Y., & Bennett, C. (2016). Group‐based parent training programmes for improving emotional and behavioural adjustment in young children. The Cochrane Library, 8, 1–171. doi:10.1002/14651858.CD003680.pub3.
- Barlow, J., Smailagic, N., Huband, N., Roloff, V., & Bennett, C. (2014). Group-based parent training programmes for improving parental psychosocial health. Cochrane Database of Systematic Reviews (Online), 6(5), 1–204
- Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck depression inventory-II. San Antonio, 78(2), 490–498.
- Black, M. M., Walker, S. P., Fernald, L. C., Andersen, C. T., DiGirolamo, A. M., Lu, C., … Devercelli, A. E. (2017). Early childhood development coming of age: Science through the life course. The Lancet, 389(10064), 77–90. doi:10.1016/S0140-6736(16)31389-7
- Boon, H., Ruiter, R. A., James, S., Van Den Borne, B., Williams, E., & Reddy, P. (2009). The impact of a community-based pilot health education intervention for older people as caregivers of orphaned and sick children as a result of HIV and AIDS in South Africa. Journal of Cross-Cultural Gerontology, 24(4), 373. doi:10.1007/s10823-009-9101-2
- Burke, Y., Hosein, M., Morton, I., Purgato, M., Adi, A., Kuzrok, M., … Wa, T. 2018. Psychosocial inerventions for disruptive behaviour problems in children in low and middle income countries: A systematic review and met-analysis. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 59: 982–993. 2018, Apr 6 Epub doi: 10.1111/jcpp.12894.
- Caldwell, B. M., & Bradley, R. H. (2003). Home inventory administration manual. Little Rock, Arkansas: University of Arkansas for Medical Sciences.
- Carlo, G., Mestre, M. V., Samper, P., Tur, A., & Armenta, B. E. (2011). The longitudinal relations among dimensions of parenting styles, sympathy, prosocial moral reasoning, and prosocial behaviors. International Journal of Behavioral Development, 35(2), 116–124. doi:10.1177/0165025410375921
- Chamberlain, P., & Reid, J. B. (1987). Parent observation and report of child symptoms. Behavioral Assessment, 9(1), 97–109.
- Clottey, E. N., Scott, A. J., & Alfonso, M. L. (2015). Grandparent caregiving among rural African Americans in a community in the American South: Challenges to health and wellbeing. Rural Remote Health, 15(3), 3313.
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. doi:10.2307/2136404
- Coore Desai, C., Reece, J. A., & Shakespeare-Pellington, S. (2017). The prevention of violence in childhood through parenting programmes: A global review. Psychology, Health & Medicine, 22(sup1), 166–186. doi:10.1080/13548506.2016.1271952
- Deal, A. G., Trivette, C. M., & Dunst, C. J. (1988). Family functioning style scale. Enabling and Empowering Families: Principles and Guidelines for Practice, 1, 177–184.
- Derogatis, L. R., & Spencer, P. (1993). Brief symptom inventory: BSI. Saddle River, NJ: Pearson Upper.
- Di Gessa, G., Glaser, K., Price, D., Ribe, E., & Tinker, A. (2016). What drives national differences in intensive grandparental childcare in Europe? The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 71(1), 141–153. doi:10.1093/geronb/gbv007
- Di Gessa, G., Glaser, K., & Tinker, A. (2016). The impact of caring for grandchildren on the health of grandparents in Europe: A lifecourse approach. Social Science & Medicine (1982), 152, 166–175. doi:10.1016/j.socscimed.2016.01.041
- Dunst, C., Jenkins, V., & Trivette, C. (1984). Family support scale: Reliability and validity. Journal of Individual, Family, and Community Wellness, 1(4), 45–52.
- Dunst, C. J., & Leet, H. E. (1985). Family resource scale. Morganton, NC: Western Carolina Center.
- Dunst, C.J., & Leet, H.E. (1987). Measuring the adequacy of resources in household with young children. Child: Care, Health & Development, 13, 111-125.
- Dunst, C.J., & Trivette, C.M. (1989). Toward experimental evaluation of the family, infant and pre-school program. In H. Weiss & F. Jacobs (Eds.), Evaluating Family Programs. New York, NY: Aldine Publishing, 315-346.
- Eyberg, S. M., & Pincus, D. (1999). Eyberg child behavior inventory and sutter-eyberg student behavior inventory-revised: Professional manual. Odessa, FL: Psychological Assessment Resources.
- Folkman, S., & Lazarus, R. S. (1985). If it changes it must be a process: Study of emotion and coping during three stages of a college examination. Journal of Personality and Social Psychology, 48(1), 150. doi:10.1037/0022-3514.48.1.150
- Furlong, M., McGilloway, S., Bywater, T., Hutchings, J., Donnelly, M., Smith, S. M., & O’Neill, C. (2010). Behavioural/cognitive–Behavioural group-based parenting interventions for children age 3–12 with early onset conduct problems [Protocol]. Cochrane Database of Systematic Reviews, 1
- Gardner, F., Leijten, P., Mann, J., Landau, S., Harris, V., Beecham, J., … Scott, S. (2017). Could scale-up of parenting programmes improve child disruptive behaviour and reduce social inequalities? Using individual participant data meta-analysis to establish for whom programmes are effective and cost-effective. Southampton (UK): NIHR Journals Library.
- Heymann, J., Earle, A., Rajaraman, D., Miller, C., & Bogen, K. (2007). Extended family caring for children orphaned by AIDS: Balancing essential work and caregiving in a high HIV prevalence nations. AIDS Care, 19(3), 337–345. doi:10.1080/09540120600763225
- Higgins, J. P., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., … Sterne, J. A. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj, 343, d5928. doi:10.1136/bmj.d5928
- Hutchings, J., Bywater, T., Daley, D., Gardner, F., Whitaker, C., Jones, K., … Edwards, R. T. (2007). Parenting intervention in Sure Start services for children at risk of developing conduct disorder: Pragmatic randomised controlled trial. Bmj, 334(7595), 678. doi:10.1136/bmj.39126.620799.55
- Kelley, S. J., Whitley, D., & Sipe, T. A. (2007). Results of an interdisciplinary intervention to improve the psychosocial well-being and physical functioning of African American grandmothers raising grandchildren. Journal of Intergenerational Relationships, 5(3), 45–64. doi:10.1300/J194v05n03_04
- Kelley, S. J., Yorker, B. C., Whitley, D. M., & Sipe, T. A. (2001). A multimodal intervention for grandparents raising grandchildren: Results of an exploratory study. Child Welfare, 80(1), 27.
- Kirby, J. N., & Sanders, M. R. (2014). A randomized controlled trial evaluating a parenting program designed specifically for grandparents. Behaviour Research and Therapy, 52, 35–44. doi:10.1016/j.brat.2013.11.002
- Kmet, L. M., Lee, R. C., & Cook, L. S. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of fields (Vol. 22). Edmonton, CA: Alberta Heritage Foundation for Medical Research Edmonton.
- Knerr, W., Gardner, F., & Cluver, L. (2013). Improving positive parenting skills and reducing harsh and abusive parenting in low-and middle-income countries: A systematic review. Prevention Science, 14(4), 352–363. doi:10.1007/s11121-012-0314-1
- Landry, S. H., Smith, K. E., & Swank, P. R. (2003). The importance of parenting during early childhood for school-age development. Developmental Neuropsychology, 24(2–3), 559–591. doi:10.1080/87565641.2003.9651911
- Lee, L., Packer, T. L., Tang, S. H., & Girdler, S. (2008). Self‐management education programs for age‐related macular degeneration: A systematic review. Australasian Journal on Ageing, 27(4), 170–176. doi:10.1111/j.1741-6612.2008.00298.x
- Littlewood, K. A., Strozier, A. L., & Whittington, D. (2014). Kin as Teachers: An early childhood education and support intervention for kinship families. Children and Youth Services Review, 38, 1–9. doi:10.1016/j.childyouth.2013.11.026
- Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck depression and anxiety inventories. Behaviour Research and Therapy, 33(3), 335–343.
- McCallion, P., Janicki, M. P., & Kolomer, S. R. (2004). Controlled evaluation of support groups for grandparent caregivers of children with developmental disabilities and delays. American Journal on Mental Retardation, 109(5), 352–361. doi:10.1352/0895-8017(2004)109<352:CEOSGF>2.0.CO;2
- McCubbin, H., Olson, D., & Larsen, A. (1981). Family crisis oriented personal scales (F-COPES). In H. I. McCubbin, A. I. Thompson, & M. A. McCubbinEds., Family assessment: Resiliency, coping and adaptation-inventories for research and practice. 1996. 455–507. New York, NY: Free Press.
- McDonald, L., FitzRoy, S., Fuchs, I., Fooken, I., & Klasen, H. (2012). Strategies for high retention rates of low-income families in FAST (Families and Schools Together): An evidence-based parenting programme in the USA, UK, Holland and Germany. European Journal of Developmental Psychology, 9(1), 75–88. doi:10.1080/17405629.2011.632134
- Mhaka-Mutepfa, M., Cumming, R., & Mpofu, E. (2014). Grandparents fostering orphans: Influences of protective factors on their health and well-being. Health Care for Women International, 35(7–9), 1022–1039. doi:10.1080/07399332.2014.916294
- Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Group, P. (2009). Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Physical Therapy, 89(9), 873–880.
- N’zi, A. M., Stevens, M. L., & Eyberg, S. M. (2016). Child directed interaction training for young children in kinship care: A pilot study. Child Abuse & Neglect, 55, 81–91. doi:10.1016/j.chiabu.2016.03.001
- Ogden, T., & Hagen, K. A. (2008). Treatment effectiveness of parent management training in Norway: A randomized controlled trial of children with conduct problems. Journal of Consulting and Clinical Psychology, 76(4), 607. doi:10.1037/0022-006X.76.2.341
- Pianta, R. C. 1992. Child-parent relationship scale, Vol. 427. Unpublished measure: Richmond, Virginia: University of Virginia.
- Pierce, G. R., Sarason, I. G., & Sarason, B. R. (1991). General and relationship-based perceptions of social support: Are two constructs better than one? Journal of Personality and Social Psychology, 61(6), 1028. doi:10.1037/0022-3514.61.6.1028
- Piquero, A., Farrington, D.P., Welsh, B., Tremblay, R., & Jennings, W. (2009). Effects of early family/parenting training programs on antisocial behavior and delinquency. Journal of Experimental Criminology, 5(2), 83-120.
- Pulgaron, E. R., Marchante, A. N., Agosto, Y., Lebron, C. N., & Delamater, A. M. (2016). Grandparent involvement and children’s health outcomes: The current state of the literature. Families, Systems & Health : the Journal of Collaborative Family Healthcare, 34(3), 260–269. doi:10.1037/fsh0000212
- Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. doi:10.1177/014662167700100306
- Samms-Vaughan, M. (2008). Comprehensive longitudinal studies of child health, development and behaviour in Jamaica: Findings and policy impact. The West Indian Medical Journal, 57(6), 639–644.
- Sanders, M. R., & Woolley, M. (2005). The relationship between maternal self‐efficacy and parenting practices: Implications for parent training. Child: Care, Health and Development, 31(1), 65–73. doi:10.1111/j.1365-2214.2005.00487.x
- Sandler, I. N., Schoenfelder, E. N., Wolchik, S. A., & MacKinnon, D. P. (2011). Long-term impact of prevention programs to promote effective parenting: Lasting effects but uncertain processes. Annual Review of Psychology, 62, 299–329. doi:10.1146/annurev.psych.121208.131619
- Squires, J. B., & Potter, D. D. (1999). The ASQ user’s guide. Baltimore MD: Brookes Publishing Company.
- Strozier, A.L., & Krisman, K. (2007). Capturing caregiver data: An examination of kinship care custodial arrangements. Children and Youth Services Review, 29(2), 226-246.
- Wagner, M., Iida, E., & Spiker, D. (2001). The multisite evaluation of the parents as teachers home visiting program: Three-year findings from one community. Menlo Park, CA: SRI International.
- Walker, S. P., Chang, S. M., Vera-Hernández, M., & Grantham-McGregor, S. (2011). Early childhood stimulation benefits adult competence and reduces violent behavior. Pediatrics, 127(5), 849–857. doi:10.1542/peds.2010-2231
- Ware, J., Jr, Kosinski, E., & Keller, S. D. (1996). A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233.
- Yancura, L. A. (2013). Justifications for caregiving in white, Asian American, and native Hawaiian grandparents raising grandchildren. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 68(1), 139–144. doi:10.1093/geronb/gbs098
- Zauszniewski, J. A., Musil, C. M., Burant, C. J., & Au, T. Y. (2014). Resourcefulness training for grandmothers: Preliminary evidence of effectiveness. Research in Nursing & Health, 37(1), 42–52. doi:10.1002/nur.21574
- Zubrick, S. R., Ward, K. A., Silburn, S. R., Lawrence, D., Williams, A. A., Blair, E., … Sanders, M. R. (2005). Prevention of child behavior problems through universal implementation of a group behavioral family intervention. Prevention Science, 6(4), 287. doi:10.1007/s11121-005-0013-2
- Zwi, M., Jones, H., Thorgaard, C., York, A., & Dennis, J. A. (2011, Dec). Parent training interventions for Attention Deficit Hyperactivity Disorder (ADHD) in children aged 5 to 18 years. Cochrane Database of Systematic Reviews (Online), 7(12), CD003018.
Appendix 1: Search Strategy
Search conducted March 2017
PsychINFO search
1. intervention.mp. or exp INTERVENTION/(215,950)
2. case-control.mp. (8827)
3. exp Intervention/or exp Experimental Methods/or control condition.mp. (105,451)
4. exp Intervention/or randomised control trial.mp. (83,071)
5. (control or comparison).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures] (534,228)
6. comparative.mp. (51,099)
7. exp Experiment Controls/or experimental control.mp. (1853)
8. time-series.mp. or exp Time Series/(6918)
9. (“before and after”).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures] (79,626)
10. exp skill/or parenting skill.mp. (81)
11. parenting.mp. (36,334)
12. parenting intervention.mp. (412)
13. exp grandchild/or exp grandparent/or grandparent*.mp. (4225)
14. (pre and post).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures] (31,120)
15. 10 or 11 or 12 (36,334)
16. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 9 or 14 (827,620)
17. 13 and 15 and 16 (98)
Medline search
1. intervention.mp. or exp INTERVENTION/(439,591)
2. case-control.mp. (282,010)
3. exp Intervention/or exp Experimental Methods/or control condition.mp. (8902)
4. exp Intervention/or randomised control trial.mp. (630)
5. (control or comparison).mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (3,116,458)
6. comparative.mp. (2,096,298)
7. exp Experiment Controls/or experimental control.mp. (976)
8. time-series.mp. or exp Time Series/(19,518)
9. (“before and after”).mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (617,913)
10. exp skill/or parenting skill.mp. (24)
11. parenting.mp. (20,572)
12. parenting intervention.mp. (233)
13. exp grandchild/or exp grandparent/or grandparent*.mp. (2559)
14. (pre and post).mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (105,553)
15. 10 or 11 or 12 (20,572)
16. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 9 or 14 (5,368,369)
17. 13 and 15 and 16 (44)
Embase search
1. intervention.mp. or exp INTERVENTION/(666,220)
2. case-control.mp. (179,545)
3. exp Intervention/or exp Experimental Methods/or control condition.mp. (10,381)
4. exp Intervention/or randomised control trial.mp. (1184)
5. (control or comparison).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading] (4,387,560)
6.comparative.mp. (1,028,910)
7. exp Experiment Controls/or experimental control.mp. (1202)
8. time-series.mp. or exp Time Series/(35,640)
9. (“before and after”).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading] (846,117)
10. exp skill/or parenting skill.mp. (101,212)
11. parenting.mp. (16,728)
12. parenting intervention.mp. (262)
13. exp grandchild/or exp grandparent/or grandparent*.mp. (3844)
14. (pre and post).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading] (197,290)
15. 10 or 11 or 12 (116,912)
16. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 9 or 14 (6,246,787)
17. 13 and 15 and 16 (49)
