
Abstract
Traditions practices within sub-Saharan Africa (SSA) varies from one culture to another, and are specifically community related. There are traditional harmful practices that rob men of their health, quality of life, their marriages, family wellbeing and they are rarely express in the literature. We aimed to highlight the prevalence of traditional practices among men that could have implications for their health, wellbeing and economic contributions. We systematically searched Pubmed, EMBASE, AJOL and Google Scholar for population-based studies touching traditional practices that affect men aged 15–59 across SSA. The paper reviewed were those published between January 2000 to December 2018. We employed a random-effects meta-analysis to determine different harmful traditional practices among men in SSA. The review yielded only 15 relevant articles based on the inclusion and exclusion criteria. The study identified the practices of groom-flogging, adolescent fatherhood, low sexual debut, polygyny, multiple sexual partnership, concubinage, hegemonic masculinity, circumcision, drinking in excess, cohabitation and sexual coercion as common but divergent practices among men in SSA. The authors suggest that these practices, especially concubinage, boy’s fatherhood and groom-flogging could not be free from health hazards (such as STIs, HIV, stress among boys and suicidal attempt) and should be brought to public discourse. The study concludes that every traditional practice that affects health could possibly affect life expectancies, productivity and threaten the achievement of health-for-all agenda and sustainable development goal in SSA countries. The authors therefore recommend the policy interventions and international discourse on traditional practices that affect men’s health and provision of healthcare services for men in SSA.
PUBLIC INTEREST STATEMENT
Literature is saturated with studies on traditional harmful practices that affect women and girls including massive intervention strategies to curb or stop such practices and polarized with huge funding. Till date, it is hardly heard that some of these practices are not colossally benign to men and boys also. Our study explored literatures and discovered various traditional practices that are injurious to men's wellbeing and reproductive health, especially. The study is premised on seeking equitable reproductive health for men without also impairing women rights or health, therefore the study investigates the traditional practices that affect men’s health generally and reproductive health especially. The authors conclude that traditional practices varied within sub-Saharan Africa, and are associated with men sexuality and fundamental to men’s quality of life. Therefore, every attempt to spur economic and sustainable development should consider intervention in these practices that could impair men’s economic productivities, especially in agrarian nations where men dominate food production, agriculture and employment sectors.
1. Introduction
Different traditional harmful practices that affect women in sub-Saharan African (SSA) countries are popular (African African Union, Citation2003; Igberase, Citation2012; Oleribe & Alasia, Citation2006), whereas those that rob men of their health, quality of life, their marriages and family wellbeing, including education are not known. Traditional harmful practices within Africa varied from one culture to another, and are specifically community related. They are basically, the reflections of values and beliefs held by the members of the community that have spanned generations. As the name implies, the practices are rooted in cultural and social norms, including beliefs and interpretations of religion tenets (Gender and Development Network [GADN], Citation2013; Mackie and LeJeune (Citation2009); Winter, Thompson, & Jeffreys, Citation2002). While these practices have been linked to negative health implications for women health status, the community and society at large (Dixon-Mueller, Citation1993; Glasier, Gülmezoglu, Schmid, Moreno, & Van Look, Citation2006; Oleribe & Alasia, Citation2006), they may not also benign to men (Dixon-Mueller, Citation1993; Glasier et al., Citation2006; Oleribe & Alasia, Citation2006). Therefore, to achieve any health agenda (in holistic manner), it is expedient to interrogate these practices, incorporate them into community-based health programmes or national health programmes/agenda for plausible health and wellbeing of both gender (Oleribe & Alasia, Citation2006).
Specifically, from the time immemorial, the popular aspects of traditional practices in the literature are those practices that affect girls and women. These are forms of discriminatory practices that violate girl and women rights, prominent examples which are traditional harmful practices. Traditional harmful practices are described conventionally as all behaviour, attitudes including practices which affect the fundamental rights of girls and women negatively (African Union, Citation2003; GADN, Citation2013; Mackie and LeJeune Citation2009; Ras-Work Citation2006; Wadesango, Rembe, and Chabaya Citation2011; Winter et al., Citation2002). This general definition, is oblivion of the two-sides of gender (boys/men, girls/women) but overlay with women and girls’ concerns, which could be perhaps due to the position of women in reproductive health processes. Till date, so much has been presented about the traditional harmful practices as they affect women and girls, little is often heard about men’s health, or reproductive health as being affected by traditional harmful practices. The authors therefore considered that it is high time we asked and confirmed whether similar practices are done against boys and men, and whether these practices are benign to men without negative implications to their health, especially in terms of their reproductive health.
Cultural practices and beliefs that relates to men sexuality are fundamental to men’s quality of life. These could influence the attitude and behaviour of men towards female gender or their spouses, crucial in achieving desire support for women in terms of family planning, empowerment, and access to reproductive health services (Amoo et al., Citation2018, Citation2017, Citation2017). Their behaviour underlie all women conditions that developmental programs are striving to achieve (Amoo et al., Citation2018, Citation2017). There is the practice of polygyny in which a man married more than one wife at a time. There is also the practice of hypogamy where the woman in higher social status marries a man from lower social strata (Amoo et al., Citation2018; Dunkle et al., Citation2004; Jewkes & Morrell, Citation2010). The perspective of harmful traditional practices as being currently treated is appalling and a situation where there is exclusively concern on women's health could heighten gender inequality in health and could be also be regarded as harmful practice.
Also, African manhood emphasizes toughness, strength and expression of prodigious sexual success and excesses (Dunkle et al., Citation2004; Jewkes & Morrell, Citation2010). Women are, instead, not to resist men dominance but embrace compliance and be tolerance even to violent and hurtful behaviour of their spouses, including infidelity (Dunkle et al., Citation2004; Jewkes & Morrell, Citation2010). The health consequences of this are innumerable. In addition, the traditional culture of masculinity and other practices related to it make men to engage in risky practices (Jewkes & Morrell, Citation2010; Khunou, Citation2013; Mahalik, Burns, & Syzdek, Citation2007; Mathewson, Citation2009), that often associated with aggression, violence and disregard for safety (Jewkes & Morrell, Citation2010; Khunou, Citation2013; Mahalik et al., Citation2007; Mathewson, Citation2009), with adverse effects on their health. Very related is the drinking habit of men in SSA. Comparing between gender, traditional African men drink and smoke to excess than women which in turn could increase their biological dispositions to heart disease and related problems (Mathewson, Citation2009). This singular practice could trigger violence, murder and vulnerability to auto crash, vulnerability to civil conflict and the spread of the HIV/AIDS pandemic through sexual incontinence (Amoo et al., Citation2017; Bingenheimer, Citation2010; LeClerc-Madlala, Citation2009; Ricardo, Citation2005). In addition, Men’s lower life expectancy is commonly linked to their health-related beliefs, traditional poor health-seeking behaviour that is related to masculinity (Courtenay, Citation2009). For these reasons, the notion that masculinity is bad for health is now widely accepted. Hegemonic masculinity portrays men as uncaring, indifferent to their own healthcare needs and generally risk takers (Jewkes & Morrell, Citation2010; Khunou, Citation2013; Mathewson, Citation2009; Viitanen & Colvin, Citation2015).
Although, there is no definite defined age at marriage for men in SSA. However, traditionally, male lower age at sex debut and adolescent fatherhood are often condoned while girl-child’s pregnancy is openly and popularly decried (Amoo et al., Citation2018; Odimegwu, Akinyemi, Banjo, Olamijuwon, & Amoo, Citation2018; Pettifor et al., Citation2005). These practices also include multiple or concurrent partnership (known as practice of concubinage) that is often regarded as sign of wealth for men (Amoo et al., Citation2018; Dunkle et al., Citation2004; Odimegwu, Amoo, & De Wet, Citation2018). The traditional sex preference syndrome could also be unbenign to men and the society. African society values male child for lineage perpetuation (Wusu & Amoo, Citation2014, Citation2016). Also, men’s and boy’s work on farms reflecting in male-biased sex ratios. These often fuel sex-selective abortion or infanticide of female foetus (Alesina, Giuliano, & Nunn, Citation2018; Odimegwu et al., Citation2018) Alesina et al., Citation2018). Other consequence includes high male-based sex ratio (Alesina et al., Citation2018). Male perpetration of intimate partner violence (IPV) against women in SSA is widespread with rhetorical and empirical evidences suggesting men’s peer networks as key factor (Mulawa, Reyes, Foshee, Halpern, Martin, Kajula & Maman, Citation2018). Apart from the victim of IPV suffering from negative health consequences including mental health and reproductive health outcomes, the circumstances surrounding the violence and disintegration of the family or relationship could also have long-term effect on the men (Mulawa, Reyes, Foshee, Halpern, Martin, Kajula & Maman, Citation2018).
Studies have, however, investigated traditional practices of girl-child marriage, forced marriage, female genital mutilation, widowhood rites and other practices that affect women dignity and have developmental consequences. For example, the tradition of incision or cutting, popularly called “Efidan” which is in the form of scarification involving scratching, etching, burning/branding or superficially cutting designs, pictures or words into the skin as a permanent body modification that often results into scars with ill-health consequences if unmanaged properly (Garve, Garve, Türp, Fobil, & Meyer, Citation2017). There is “Fulani sharo” tradition where rival suitors underwent the ordeal of caning as a means of eliminating those who were less persistent. Prospective groom-beating is performed on adolescent boy to show that the victim boy is ready for family and life responsibilities (Encyclopedia Britannica, Citation2019; Oleribe & Alasia, Citation2006). The Fulani sharo that connotes flogging is often a public ceremony in which the prospective young suitor is continuously whipped by a challenger (another suitor) and he (the boy) must show no signs of pain, otherwise he loses the wife to the rival. It is traditionally held to test the level endurance, strength and perseverance of young males to withstand the pains emanating from severe flogging (Encyclopedia Britannica, Citation2019). There is also male circumcision which is widely accepted and practiced as a rite of passage performed on adolescence (Borgdorff et al., Citation2018; Young et al., Citation2012). Cultural and religion practices are interwoven in SSA. While the culture such as the religion dimension encourages certain practices that undervalue women; the strict dominance of male even in matters related to women social needs or reproductive services, and the practice of purdah system (wife seclusion). There is also “wife-gifts” called “Sadakiar” in Nupe (Oleribe & Alasia, Citation2006; Osita-Oleribe, Citation2007), and also known as “Iyawo-Sara” practiced among the Muslims, but more dominant in Kwara State, Nigeria. The wife-gifts relates to practice of giving out a daughter to any man of parent’s (father’s) choice without the consent of the daughter or even the boy/man involved. It is a forced solemnisation that bind both new couples together under Islamic religion and often welcome without resistance.
The increasing awareness of these practices (especially as they affect women) has, to certain degree, met with corresponding commitments both at the globally level and across Africa to address these menaces. Specifically, the campaign against harmful traditional practices affected women has been intensified since 1950s, and in 1993, the World Conference on Human Rights in Vienna signalled to the whole world that “women rights are human rights”; and also the Declaration on the Elimination of Violence against Women (Winter et al., Citation2002). There are Cairo conference of 1994, the 1995 Beijing International Conference on Population and Development (ICPD), Vision-2020 (by International Planned Parenthood Federation). The Convention on the elimination of all forms of discrimination against women (CEDAW) adopted by United Nations General Assembly encouraged the modification of all social, cultural conducts that could have negative impacts on the health and wellbeing of women (Amoo, Citation2017; Winter et al., Citation2002). There are laws preventing young girls from being married off in various countries nowadays, but there are no law preventing a child-boy from inheriting a widow much older than him as wife and sometimes as the first wife. It is customarily expected that a man of title should have several wives.
There are also the 2000 Millennium Development Goals (MDGs), Sustainable Development Goals SDGs (2015) and the African Union Agenda 2063 with focus on elimination of girl-child marriage and forced marriage; support for women empowerment, including free basic education for girls (Adebowale & Palamuleni, Citation2014; African Union, Citation2015a, Citation2015b; Amoo, Citation2017; UNICEF, Citation2011, Citation2014; United Nations Population Fund [UNFPA], Citation2004). This also include laws and regulations against human-trafficking and application of criminal laws to under-age sex, child-bride and sex work (Chersich et al., Citation2013).
Researchers, stakeholders realized that there are significant differences in risk factors for, and in, sexual behaviour between gender. They have credence to the fact that culturally in SSA settings, men play dominant roles in most affairs, especially the decisions related to women’s reproductive health care and services and general wellbeing of the family. Biologically and social-wise, whatever affect men reproductively could have direct and multiplier effects also on their spouses, their offspring and the society at large. One begins to wonder, why the silence over the needs of men from research parlance, and stakeholders. Men are co-resident with women, and if traditional practices have impact on women’s health, are the men immune to such effects?
The study is premised on seeking equitable reproductive health for men without also impairing women rights, health and wellbeing. That every man has right to reproductive health, to be able to include women in their decision on fertility, enjoy own sexuality that is free of threat of infection or disease, and support for women wellbeing towards safe reproduction processes. The study therefore investigates the traditional harmful practices that affect men’s reproductive health in SSA. The understanding of the existence of practices that affect men’s health and analysis of the interplay between factors sustaining these practices could be critical to the processes of social change and require policy direction towards improvement of health, wellbeing of men, their longevity and eradication of values that are inimical to both men and women health in the society.
2. Methods and materials
2.1. Search strategy and selection criteria
The methodology was anchored on systematic review of existing cross sectional or cohort studies, to identify population-based articles that are related to traditional harmful practices affecting men in SSA. Our search engines included PubMed database, EMBASE, and Google Scholar and AJOL. Only studies published from 1970 were included to underscore the practices that are relatively old and those that are currently on-going. Besides, the period covered the post-independence of virtually all countries reviewed within SSA. The period could also be regarded as pre-and-post several international developmental agenda such as ICPD, Beijing Conference, and so on. Online journals were also searched including scanned reference lists of identified reports. The search terms used were traditional practices, harmful practices, men health, men reproductive health, and SSA or Africa). These search terms were obtained from medical subject headings (MeSH). We included studies of traditional practices, harmful practices that used numerical estimates for category of the harmful practices, prevalence, age category of men involved and other factors related to harmful practices that affect men reproductive health in SSA (apart from culture). Titles and abstracts of studies were reviewed for relevance, and full-texts of studies on men’s traditional practices prevalence were accessed for further screening. The reference lists of accessed full-texts were also checked for additional studies.
All non-human studies were excluded, other studies without clearly defined study designs, methodologies or harmful practices that affect women were also excluded in the study (Figure ). Overall there are no language restrictions.
Figure 1. Study selection flow chart.
2.2. Procedures
We extracted all data onto a template in Microsoft Excel file format. We abstracted data systematically by age and various severity categories of traditional practices, including the number of cases or incidence of practices that could affect men’s health (reproductive health, especially), and their corresponding 95% confidence intervals (CIs) for cases identified (with Stata 14). The data were extracted by two independent reviewers and emerging disagreement was resolved after discussion. We also contacted authors who were reachable for additional data wherever data in the published studies were not conducive to inclusion in the meta-analysis. Specifically, in few of the studies where the prevalence rates were not indicated, the first authors were contacted for the original data where prevalence were extracted for this study.
A random effect meta-analysis (DerSimonian and Laird method) was conducted on extracted crude prevalence rate of traditional practices and their determinants to accommodate heterogeneity across studies included in the analysis (IntHout, Ioannidis, & Borm, Citation2014; Jackson, White, & Thompson, Citation2010). Overall summaries of the meta-estimates (and CIs) were reported separately. We accounted for variation in sample sizes from each data-point and controlled for year of publication to generate estimates of prevalence for each of the practices. Heterogeneity between studies was assessed using I-squared (I2) statistics, and subgroup analysis was conducted to detect causes of heterogeneity when appropriate.
3. Results
Our search returned 262 studies. After screening titles for relevance (studies estimating men’s traditional practices), 180 studies were excluded. We therefore assessed 83 full-text papers. After applying the screening criteria, 66 studies were excluded because they could not provide prevalence statitics on traditional practices, population figures or relevant estimates from which prevalence statistics can be calculated. A total of 15 studies were retained for review. Table shows the region, country and the study year. The study covered three regions in Africa. The East Africa region had the highest number of studies, while West Africa and South Africa have the least and there was one national data.
Table 1. Characteristics of studied population
Also, from trend analysis studies such as Amoo et al. (Citation2018) the last prevalence rate estimated was used as the recent prevalence rate for this study.
3.1. Prevalence of male circumcision in Nigeria
From all studies, the highest prevalence of male circumcision was reported in 1992. The forest plots were used to give a visual assessment of the pooled prevalence along with 95% confidence intervals (95% CIs) of male circumcision use by the sub-regions studied. We used the I2 statistic to evaluate heterogeneity in male circumcision prevalence between the retained studies. From the random effects meta-analysis, the estimated overall proportion of tobacco use in SSA was 60.3% (Figure ). In the regional subgroup analysis, the East African zone had the highest proportion of male circumcision (67.9%, 95% CI 60.5–75.2), followed by the South African region at 35.6% (95% CI 19.5–51.6) (shown Table —Figure ).
Table 2. Characteristics of the included studies
The forest plots were used to give a visual assessment of the pooled prevalence along with 95% confidence intervals (95% CIs) of male circumcision use by the sub-regions studied. We used the I2 statistic to evaluate heterogeneity in male circumcision prevalence between the retained studies. From the random effects meta-analysis, the estimated overall proportion of male circumcision in SSA was 60.3% (Figure ). In the regional subgroup analysis, the East African zone had the highest proportion of male circumcision (67.9%, 95%CI 60.5–75.2), followed by the South African region at 35.6% (95% CI 19.5–51.6) (Figure ). The forest plot provided a “blobbogram” (graphical) display of estimated results for several cross-sectional studies reviewed on traditional harmful practices that affect men in SSA. The graph is commonly used for representing a meta-analysis results (Lewis & Clarke, Citation2001).
Male circumcision is almost absolute tradition for all men in Kenya with the prevalence rate as high as 93.6% (95%CI 93.08–94.12) and relatively 100% in sub-culture within Eastern Africa such as Amhara, Oromiya, Benishangul-Gumuz, Gambela and Dire Dawa (Figure ). The rate of circumcision in the southern Africa is relatively different. Apart from Lesotho where the crude prevalence rate shows that more than two-third men experience male circumcision 79% 95%CI (77.0–80.9), the prevalence rates in other countries within this region are very low. The prevalence rate in Malawi, Mozambique, Namibia and Zimbabwe are 20.7 (95% CI 19.6–21.8), 49.7 (95% CI 47.9–51.5), 28.7 (95% CI 27.0–30.3), 24.8 (95% CI 23.9–25.6), 10.0 (95% CI 9.7–11.5), respectively (as shown in Figure ).
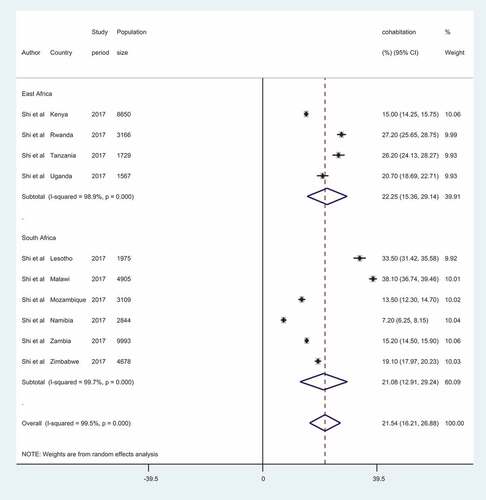
In terms of cohabitation, nearly one out of every five men in the Eastern Africa practice cohabitation. The practice cut across Kenya, Rwanda, Tanzania and Uganda as contained in the articles reviewed. In a study involving 8650 in Kenya, 15% (95%CI 14.2–15.7) are cohabitating. The prevalence actually ranges from 15% (Kenya) to 27% in Rwanda. Among the few studies available on traditional practices that affect men in Lesotho, 33.5% of men are cohabitating (95%CI 31.4–35.5), result indicated 38.1% (95%CI 36.7–39.4) for Malawi, 15.2% (95%CI 14.5–15.9) for Zambia, 13.5% (95%CI 12.3–14.7) for Mozambique, 19.1% (95%CI 17.9–20.3) for Zimbabwe. However, Namibia recorded a low rate of 7.2% (Figure ). The overall cohabitation I2 statistic showed 99.7% heterogeneity in the retained studies.
Figure 2. Crude prevalence rate of male circumcision in Africa, by zones.
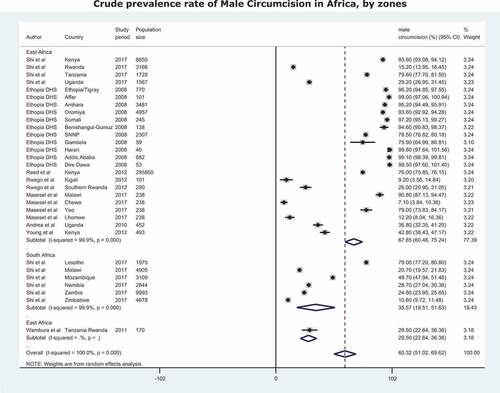
Figure 2. (Continued).
4. Discussion
The study identified some traditional practices (e.g. efidan, sharo, boy’s fatherhood, groom-flogging) that are rarely expressed in the literature but which could rob men of their health, quality of life, their marriages and family wellbeing. The study could serve as reflections on men’s health, and generate insights on the effects of the identified but unsuspected traditional practices that could affect men’s reproductive health specifically. The result of the analysis could be used to support formulation of policies and relevant advocacy towards men’s wellbeing and reproductive health. Specifically, it could suggest a modification or extension of CEDAW resolution on elimination of all discrimination against women and girl-child to include men and male-child rights especially the sacrilege surrounding the passage of rites relating to men.
The study is a complimentary gender balancing research in the treatment of traditional practices that affect men health (Dixon-Mueller, Citation1993; Glasier et al., Citation2006; Oleribe & Alasia, Citation2006) without unmindful of the fact that there could be similar practices that have corresponding effect on men as well. The identification of men’s excessive drinking and smoking habit (compared to women) as predictor of gender violence, risky behaviour including auto crash and avoidable spread of STIs/HIV has implication for low life expectancy among the men in SSA. Considering the region’s economic activity that is male-dominated, this could impair economic productivity and consequently difficulty in the attainment of sustainable development agenda (SDG 2 and 8). The goals emphasis food production, sustainable agriculture, productive employment and sustainable economic growth. Also, the study identified hegemonic masculinity, circumcision, adolescent fatherhood, low sexual debut, bread-winnership, cohabitation, sexual coercion, multiple or concurrent partnership (or concubinage), male-sex preference, network gender norms as the prevailing common traditional practices in the region.
The established linkage between traditionally believed prodigious sexual success in multiple sexual partnership and men’s health could spur appropriate checks on men sexual behaviour in the region. It could also soften the men dominance (including sexual dominance) on their spouses and sexual partners (Amoo et al., Citation2018, Citation2017; Dunkle et al., Citation2004; Jewkes & Morrell, Citation2010; LeClerc-Madlala, Citation2009; Ricardo, Citation2005). The study therefore presented an insight into the necessity of equal gender treatment of traditional practices in SSA and plausible achievement of national health programmes/agenda (Oleribe & Alasia, Citation2006). While the study may not be the first in this area, it has reduced the rarity of studies on traditional harmful practices that affect men in SSA.
A prominent implication of the findings from this study is that it could influence the attitude and behaviour of men towards female gender or their spouses, and may be crucial for the achievement of support for women in terms of family planning, empowerment and access to reproductive health services (Amoo et al., Citation2018, Citation2017). While the review identified male circumcision, sexual debut, multiple sexual partnership, as connected with health issues (Amoo et al., Citation2018; Borgdorff et al., Citation2018; Dunkle et al., Citation2004; Odimegwu et al., Citation2018; Young et al., Citation2012). The study also highlighted other suspected practices that have negative impacts on health of men and their family wellbeing. These include concubinage, boy’s fatherhood, groom-flogging and poor health-seeking behaviour. These practices could not be health-hazard free and would require public discourse or research scrutinizing. However, the fact that practices that affects health could possibly affect productivity and life expectancy, among others, they can be investigated as part of the factors that influences low life expectancy among men in SSA. The findings could also help to determine and proffer solutions to men health needs generally in SSA. Improvement in men’s own health is crucial to their full participation in spouse or partner health affairs.
Specifically, by implication, the review indicated that polygyny, multiple sexual partnership, concubinage are different nomenclatures ascribed to sexual infidelity and incontinence among men which are being tolerated for centuries in SSA region. These practices are not benign in nature. Multiple sexual partnership or sexual infidelity (and incontinence) are potent avenues for the spread of sexually transmitted infections, HIV and AIDS (Amoo et al., Citation2017; Bingenheimer, Citation2010; Ricardo, Citation2005), and increasing level of fertility at the expense of family wellbeing and men good health (Wusu & Amoo, Citation2016). Notwithstanding, these obvious health and wellbeing consequences, the fact that the end of these practices are not in sight currently calls for concern and should attract every stakeholder’s attention.
5. Conclusion and recommendations
The study concludes that the popular practices of male circumcision, early sexual debut and multiple sexual partnership among men in the region of study have been linked to negative impacts on health of men and their family wellbeing, and should be treated as public health concerns. Also, the highlighted practices of concubinage, boy’s fatherhood and groom-flogging, among others, are suspected not to be free from health hazards and should be brought to public discourse, especially in those countries where it is being practiced. While the study considered that every traditional practice that affects health could possibly affect life expectancy and could possibly explain the lowlife expectancy among men in these regions. The study also indicated that the poor health-seeking behaviour (often aggravated by masculinity syndrome) among men) could be inimical to healthy living and wellbeing of men and pose serious threat to the achievement of health for all agenda and sustainable development goal among countries of SSA. The authors recommend that while there are provisions of interventions (including international discourse) and healthcare services for women, it should not be at the expense of men’s health.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical consideration
The study does not involve direct human participants or animals. It is a systematic review of existing literature. All papers reviewed were from reputable outlets (PubMed, embassy, AJOL, etc) and must have certified the ethical standards as required.
Acknowledgements
The authors acknowledge all authors whose works where reviewed and cited in this manuscript. The authors also appreciate the Covenant University Centre for Research, Innovation and Development (CUCRID) for the funding of the publication of this article.
Additional information
Funding
Notes on contributors
Emmanuel O. Amoo
Emmanuel O. Amoo is a senior lecturer at Covenant University, Nigeria. He works on men’s health, sexual relationships, boy-fatherhood, coping strategies and family demography. He is an author, co-author, reviewer and editor with reputable journals.
Adebanke Olawole-Isaac
Adebanke Olawole-Isaac lectures in Demography and Social Statistics, Covenant University. Adebanke has successfully executed funded research projects with grants from reputable institutions. She has co-authored publications in sexual and reproductive health, non-communicable diseases, and migration.
Mofoluwake P. Ajayi
Mofoluwake P. Ajayi is a medical sociologist with Sociology Department, Covenant University. She works on coping strategies and sociological applications to development.
Olujide Adekeye
Olujide Adekeye is a Professor of Counselling Psychology with Covenant University, Nigeria. His research interest revolves around drug and substance abuse, HIV/AIDS, and relationship counselling.
Oluwatomisin Ogundipe
Oluwatomisin Ogundipe holds PhD in health economics, MA in Virginia State University, USA. She works on gender development issues, health evaluation/interventions, child and maternal health outcomes.
Oluwatomike Olawande
Oluwatomike Olawande is a lecturer at the Department of Sociology, Covenant University (Nigeria).
References
- Adebowale, S. A., & Palamuleni, M. E. (2014). Childbearing dynamics among married women of reproductive age in Nigeria: Re-affirming the role of education. Etude De La Population Africaine, 27(2), 301–318. http://aps.journals.ac.za/pub/article/view/476
- African Union. (2003). Protocol to the African Charter on Human and People’s Rights on the Rights of Women in Africa. 1–17. Retrieved from http://197.220.255.230:8080/jspui/bitstream/123456789/213/2/Protocol_Rights%20women%20in%20Africa.pdf
- African Union. (2015a). AGENDA 2063. Report of the Commission on the African Union Agenda 2063. The Africa We Want in 2063. ASSEMBLY OF THE UNION Twenty-Fourth Ordinary Session 30–31 January 2015 Addis Ababa, ETHIOPIA. Retrieved from http://www.fasngo.org/assets/files/25%20GIMAC/Final%20docs/Report%20of%20the%20Commission.pdf
- African Union. (2015b). Common African Position (CAP) on the Post-2015 Development Agenda. Retrieved from http://www.who.int/pmnch/development_agenda.pdf?ua=1
- Alesina, A., Giuliano, P., & Nunn, N. (2018). Traditional agricultural practices and the sex ratio today. PloS One, 13(1), e0190510.
- Amoo, E. O. (2017). Trends and determinants of female age at first marriage in sub-Saharan Africa (1990–2014): What has changed? African Population Studies, 31(1), 3573–3585.
- Amoo, E. O., Igbinoba, A., Imhonopi, D., Banjo, O. O., Ajaero, C. K., Akinyemi, J. O., … Solanke, L. B. (2018). Trends, determinants and health risks of adolescent fatherhood in sub-Saharan Africa. Ethiopian Journal of Health Sciences, 28(4). Retrieved from https://www.ajol.info/index.php/ejhs/article/view/175550
- Amoo, E. O., Olawole-Isaac, A., Okorie, N., Ajayi, M. P., Adekola, P. O., Amana, T. R., & Olu-Owolabi, F. (2018). Spousal desertion and coping strategies among women with cervical cancer in Nigeria: A schematic framework for wellbeing. African Population Studies, 32(1), 4012–4021. Retrieved from http://aps.journals.ac.za/pub/article/view/1172
- Amoo, E. O., Omideyi, A. K., Fadayomi, T. O., Ajayi, M. P., Oni, G. A., & Idowu, A. E. (2017). Male reproductive health challenges: Appraisal of wives coping strategies. Reproductive Health, 14(1), 90.
- Amoo, E. O., Oni, G. A., Ajayi, M. P., Idowu, A. E., Fadayomi, T. O., & Omideyi, A. K. (2017). Are Men’s reproductive health problems and sexual behavior predictors of welfare? American Journal of Men’s Health, 11(3), 487–497. doi:10.1177/1557988315598832
- Bingenheimer, J. B. (2010). Men’s multiple sexual partnerships in 15 sub‐Saharan African Countries: Sociodemographic patterns and implications. Studies in Family Planning, 41(1), 1–17.
- Borgdorff, M. W., Kwaro, D., Obor, D., Otieno, G., Kamire, V., Odongo, F., … Joseph, R. (2018). HIV incidence in western Kenya during scale-up of antiretroviral therapy and voluntary medical male circumcision: A population-based cohort analysis. The Lancet HIV, 5(5), e241–e249.
- Chersich, M. F., Luchters, S., Ntaganira, I., Gerbase, A., Lo, Y.-R., Scorgie, F., & Steen, R. (2013). Priority interventions to reduce HIV transmission in sex work settings in sub-Saharan Africa and delivery of these services. Journal of the International AIDS Society, 16, 1.
- Courtenay, W. (2009). Theorising masculinity and men’s health. Men’s Health: Body, Identity and Social Context, 9–32. Retrievd from https://books.google.com.ng/books?id=9hexN6JAVrYC&printsec=frontcover#v=onepage&q&f=false
- Dixon-Mueller, R. (1993). The sexuality connection in reproductive health. Studies in Family Planning. Studies in Family Planning, 24(5), 269–282.
- Dunkle, K. L., Jewkes, R. K., Brown, H. C., Gray, G. E., McIntryre, J. A., & Harlow, S. D. (2004). Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. The Lancet, 363(9419), 1415–1421.
- Encyclopedia Britannica. (2019). Government and society. Retrieved from Cultural milieu website https://www.britannica.com/place/Nigeria/Government-and-society#ref517330
- Garve, R., Garve, M., Türp, J. C., Fobil, J. N., & Meyer, C. G. (2017). Scarification in sub‐Saharan Africa: Social skin, remedy and medical import. Tropical Medicine & International Health, 22(6), 708–715.
- Gender and Development Network (GADN). (2013). Harmful traditional practices: Your questions, our answers (pp. 32). Retrieved from Gender & Development Network, London website https://static1.squarespace.com/static/536c4ee8e4b0b60bc6ca7c74/t/54b561ebe4b02a643c1c7ac6/1421173227982/GADN+Harmful+Traditional+Practices.pdf
- Glasier, A., Gülmezoglu, A. M., Schmid, G. P., Moreno, C. G., & Van Look, P. F. (2006). Sexual and reproductive health: A matter of life and death. The Lancet, 368(9547), 1595–1607.
- Igberase, G. (2012). Harmful cultural practices and reproductive health in Nigeria. Continental Journal of Tropical Medicine, 6(1), 27.
- IntHout, J., Ioannidis, J. P., & Borm, G. F. (2014). The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Medical Research Methodology, 14(1), 25.
- Jackson, D., White, I. R., & Thompson, S. G. (2010). Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta‐analyses. Statistics in Medicine, 29(12), 1282–1297.
- Jewkes, R., & Morrell, R. (2010). Gender and sexuality: Emerging perspectives from the heterosexual epidemic in South Africa and implications for HIV risk and prevention. Journal of the International AIDS Society, 13(1), 6.
- Khunou, G. (2013). Men’s health: An analysis of representations of men’s health in the Sowetan newspaper. Communicatio (South African Journal for Communication Theory and Research), 39(2), 182–193.
- LeClerc-Madlala, S. (2009). Cultural scripts for multiple and concurrent partnerships in southern Africa: Why HIV prevention needs anthropology. Sexual Health, 6(2), 103–110.
- Lewis, S., & Clarke, M. (2001). Forest plots: Trying to see the wood and the trees. Bmj, 322(7300), 1479–1480.
- Mackie, G., & LeJeune, J. (2009). Social dynamics of abandonment of harmful practices: A new look at the theory. Innocenti Working Paper, IWP-2009-06.
- Mahalik, J. R., Burns, S. M., & Syzdek, M. (2007). Masculinity and perceived normative health behaviors as predictors of men’s health behaviors. Social Science & Medicine, 64(11), 2201–2209.
- Mathewson, S. H. (2009). Constructions of masculinity and health-related behaviours among young men in Dakar, Senegal ( Working Paper Series, No. 09–91). Development Studies Institute, London School of Economics and Political Science, Houghton Street, London. Retrieved from http://www.lse.ac.uk/internationaldevelopment/pdf/wp/wp91.pdf
- Mulawa, M. I., Reyes, H. L. M., Foshee, V. A., Halpern, C. T., Martin, S. L., Kajula, L. J., & Maman, S. (2018). Associations between peer network gender norms and the perpetration of intimate partner violence among urban tanzanian men: A multilevel analysis. Prevention Science, 19(4), 427-436.
- Odimegwu, C. O., Akinyemi, J. O., Banjo, O. O., Olamijuwon, E., & Amoo, E. O. (2018). Fertility, family size preference and contraceptive use in sub-Saharan Africa: 1990–2014. African Journal of Reproductive Health, 22(4), 44–53. doi:10.29063/ajrh2018/v22i4.5
- Odimegwu, C. O., Amoo, E. O., & De Wet, N. (2018). Teenage pregnancy in South Africa: Where are the young men involved? South African Journal of Child Health, 12(SPE), s44–s50.
- Oleribe, E., & Alasia, D. (2006). Culture and health: The effect of Nupe cultural practice on the health of Nupe people. Nigerian Journal of Medicine: Journal of the National Association of Resident Doctors of Nigeria, 15(3), 325–328.
- Osita-Oleribe, O. E. (2007). Neglect of Girl Child Education: Bridging the gap. A case study of a Nigerian agrarian northern community. International NGO Journal, 2(2), 030–035.
- Pettifor, A. E., Rees, H. V., Kleinschmidt, I., Steffenson, A. E., MacPhail, C., Hlongwa-Madikizela, L., … Padian, N. S. (2005). Young people’s sexual health in South Africa: HIV prevalence and sexual behaviors from a nationally representative household survey. Aids, 19(14), 1525–1534.
- Ras-Work, B. (2006). The impact of harmful traditional practices on the girl child. United Nations Division for the Advancement of Women (DAW) in Collaboration with UNICEF. Italy, UNICEF Innocenti Research Centre, (EGM/DVGC/2006/EP.4) (p. 1–13). Retrieved from http://www.womenssupportproject.co.uk/vawtraining/content/harmfulculturalpractices/277234/userfiles/file/resources/nationalresources/Impact%20on%20girl.pdf
- Ricardo, C. (2005). Young men and the construction of masculinity in sub-Saharan Africa: Implications for HIV/AIDS, conflict, and violence. Presented at the Metanexus Institute. Philadelphia: University of Pennsylvania.
- UNICEF. (2011). The State of the World’s Children 2011-Executive Summary: Adolescence an Age of Opportunity. Retrieved from https://www.unicef.org/adolescence/files/SOWC_2011_Main_Report_EN_02092011.pdf
- United Nations Children’s Fund (UNICEF). (2014). The state of the world’s children 2015: Reimagine the future: Innovation for every child (pp. 1–124). New York: Division of Communication, United Nations Children’s Fund (UNICEF).
- United Nations Population Fund [UNFPA]. (2004). Programme of Action Adopted at the International Conference on Population and Development, Cairo, September 5-13, 1994. E/25,000/2004. United Nations Population Fund. Retrieved from https://www.unfpa.org/sites/default/files/event-pdf/PoA_en.pdf
- Viitanen, A. P., & Colvin, C. J. (2015). Lessons learned: Program messaging in gender-transformative work with men and boys in South Africa. Global Health Action, 8(1), 27860.
- Wadesango, N., Rembe, S., & Chabaya, O. (2011). Violation of women’s rights by harmful traditional practices. The Anthropologist, 13(2), 121–129. Retrieved from https://www.tandfonline.com/doi/abs/10.1080/09720073.2011.11891187
- Winter, B., Thompson, D., & Jeffreys, S. (2002). The UN approach to harmful traditional practices. International Feminist Journal of Politics, 4(1), 72–94.
- Wusu, O., & Amoo, E. O. (2014). Sub-Saharan African Children and Adolescents: Economic Gain or Burden? In C. Odimegwu & J. Kekevole (eds.), Continuity and Change in Sub-Saharan Africa Demography (pp. 192-209). Routledge Taylor and Francis Group. ISBN 13:978-0-415-71194-4.
- Wusu, O., & Amoo, E. O. (2016). Fertility behaviour and wealth situation in Nigeria: Evidence from 2013 demographic and health survey. Social Indicators Research, 128(1), 1–14. doi:10.1007/s11205-015-1016-4
- Young, M. R., Odoyo-June, E., Nordstrom, S. K., Irwin, T. E., Ongonga, D. O., Ochomo, B., … Bailey, R. C. (2012). Factors associated with uptake of infant male circumcision for HIV prevention in western Kenya. Pediatrics-English Edition, 130(1), e175.