Abstract
This study contributes to current discussions regarding the use of digital solutions and especially (mobile) contact tracingcontact-tracing apps (MCTA) in COVID-19 containment. This study is timely because several countries around the world andworld, including African countriescountries, face an acute shortage of COVID-19 vaccines and as a result complimentary measures and innovative solutions like MCTA can be useful in the containment of COVID-19 disease pandemic. Towardsd this end, the current study integrates the health belief model (HBM) with the theory of reasoned action (TRA) to investigate MCTA acceptability based on data collected from online respondents in Nigeria. The results of the empirical analyses, using PLS-SEM, indicate that perceived disease vulnerability, perceived severity of the disease, but but not perceived barriers ofto taking action, are important determinants of attitude towardsd MCTA. The results further show that, while attitude is positively related to MCTA adoption intention, both perceived disease vulnerability and perceived severity of the disease indirectly contribute to MCTA adoption intention through attitude towardsd MCTA. Overall, the proposed research model explains about 58.8% variation in the intention to adopt MCTA and therefore shines a positive light on the topic that is critical for shaping COVID-19 messaging in different countries of the world and especially in African countries where COVID-19 testing and vaccination drive remain worryingly slow.
PUBLIC INTEREST STATEMENT
Given the grim reality that we currently face, particularly the COVID-19 pandemic, there have been suggestions in the business and academic press that mobile contact-tracing apps (MCTA) could complement existing manual tracing and tracking efforts in the fight against the pandemic. However, an important concern remains whether individuals are willing to use the MCTA, especially since there are already concerns about the possible invasion of an individual’s privacy. On this score, this publication attempts to contribute to the ongoing discussion regarding the acceptance of MCTA by utilizing the Health Belief Model (HBM) with the Theory of Reasoned Action (TRA) to investigate individuals’ attitudes and intentions to adopt the MCTA. Findings from this preliminary study provide essential insights into how governments, especially those in African nations, such as Nigeria, can better craft COVID-19 messaging and ultimately boost the more extensive uptake of MCTA.
1. Introduction
As of April 17, 2020, the total number of confirmed cases of COVID-19 was 139.5 million and with a global death toll of nearly three million people (WHO COVID-19 dashboard, 2020). Indeed, containing the spread of COVID-19 is the biggest priority today, which is the reason why scholars, as well as policymakers and practitioners, from all around the world are contributing their best to tackling the issue. While vaccines have started to be rolled out in different countries around the world, several countries and especially developing nations, such as African nations, face an acute shortage of COVID-19 vaccines and even the World Health Organization acknowledged that Africa has been left behind in the race for COVID-19 vaccines (cf., VOA News, Citation2021). Considering this emerging reality, it is crucially important, therefore, to consider additional measures and/or interventions that can be taken to control community transmission of this deadly coronavirus. Among others, one important intervention that has been recently proposed that can help curb community spread of COVID-19 is the use of digital solutions and especially (mobile) contact tracing apps (henceforth MCTA; Altmann et al., Citation2020; Ferretti et al., Citation2020; Fox et al., Citation2021; Walrave et al., Citation2020). In general, MCTA relies on Bluetooth and/or related technology to alert members of the public if they come in close contact with a possible carrier of the SARS-CoV-2 virus. This solution seems to be a practical and logical one because a vast majority of the people around the world, including African countries such as in Nigeria, own and use mobile phones (Statista, Citation2020).
Despite the potential benefits in using MCTA as a containment measure for COVID-19, anecdotal findings show the biggest obstacle facing MCTA acceptance is the low adoption rates of the app. This in effect raises a vital concern, whether intended users and the citizenry are willing to use mobile contact tracing apps given the fact that earlier research on this topic has raised enormous concerns about possible invasion of individual’s privacy (see Amnesty International, Citation2020; Chan & Saqib, Citation2021; Hassandoust et al., Citation2021; Lin et al., Citation2021; Litan & Lowy, Citation2020). It is important to acknowledge the contributions of those studies that have earlier explored this important subject (Alsaad & Al-Okaily, Citation2021; Duan & Deng, Citation2021; Fox et al., Citation2021; Guillon & Kergall, Citation2020; Hassandoust et al., Citation2021; Li et al., Citation2021; Lin et al., Citation2021; Trang et al., Citation2020) and which their research findings provide us with initial understanding of citizens’ (un)willingness to use MCTA For instance, in Australia and Singapore, where the app has recently been deployed, user adoption is reported to be very low (Abbas & Michael, Citation2020). Similarly, in countries like France, the app entirely failed to take off (Rowe et al., Citation2020). Indeed, without a critical mass adoption of MCTA, its potential benefits in the fight against the community spread of COVID-19 will not be realized. Therefore, the main objective of this study is to contribute to ways in which the use of MCTA can be promoted through broader acceptance of the app (proxied here by adoption intention). This study therefore focuses on a user-centric perspective and by so doing it not only complements emerging discussions on this important topic (e.g., Altmann et al., Citation2020; Fox et al., Citation2021; Walrave et al., Citation2020) but also sheds new light on the topic based on the integration of two well-known theories in the literature. To this end, the current study draws on the health belief model (HBM; Carpenter, Citation2010; Janz & Becker, Citation1984; Rosenstock, Citation1974; Rosenstock et al., Citation1988) as well as the theory of reasoned action (TRA; Ajzen & Fishbein, Citation2005; Fishbein & Ajzen, Citation1975) to investigate determinants of MCTA adoption intention. Altogether, it is expected that the results of this research will implicate ways in which governments can craft their messaging to encourage more members of the public to adopt the app. This paper makes an original contribution to this emerging research stream by identifying how both perceived disease severity and vulnerability positively influence the adoption intention of MCTA through attitudes toward the app. Finally, this study, to our knowledge, represents the first attempt in the literature to employ both HBM and TRA in examining critical issues related to individuals’ voluntary adoption of MCTA in the COVID-19 context and consequently reinforcing the initial contribution of the present study to the literature and ultimately practice.
In the subsequent sections, the paper elaborates on this topic by providing information on the theoretical foundation and hypothesis development, research methods, data analysis and results, discussion, and finally, the research conclusion.
2. Theoretical foundation and hypotheses development
2.1. Health Belief Model (HBM)
The Health Belief Model (HBM) was proposed in the 1950s to understand preventive health behavior (Rosenstock, Citation1974). The action taken by a person to avoid contracting a disease or to detect a disease at an early stage, which may also be referred to as preventive health behavior (Kasl & Cobb, Citation1966). The key assumption of the HBM is that an individual’s propensity to engage in preventive health behavior is largely dependent on certain key factors and/or perceptions, such as perceived susceptibility, perceived severity, and perceived barrier of taking action (Janz & Becker, Citation1984; Rosenstock, Citation1974; Rosenstock et al., Citation1988). This means that people are more likely to take actions proactively to prevent contracting a disease when they perceive that failure to take action can make them more susceptible to the disease (perceived vulnerability) or can result in severe consequences (perceived severity; Carpenter, Citation2010; Rosenstock et al., Citation1988). According to the model, individuals who decide to take actions to prevent a disease also evaluate the feasibility and efficacy (perceived benefit) and the potential negative aspects (perceived barrier) of the proposed preventive health action (Janz & Becker, Citation1984). Several extant studies (Carico et al., Citation2020; Huang et al., Citation2020; Mou et al., Citation2016; Zhang et al., Citation2014) have used the HBM to predict individuals’ intention to engage in preventive health behavior in different contexts and with the above studies providing predictive validity for the theory. All this forms an important basis for employing HBM in the investigation of individual determinants of adoption intention of MCTA and of which adoption of MCTA is understood to be a preventive health behavior, especially in the current pandemic context.
2.2. Theory of reasoned action (TRA)
TRA remains one of the most established theoretical approaches in the social science fields to-date and its parsimony makes it widely attractive for social scientists to employ in their different domains of interests (e.g., Kurtz et al., Citation2021; Madden et al., Citation1992; Zhang et al., Citation2014; Zhao et al., Citation2018). TRA was initially proposed by Fishbein and Ajzen (Citation1975) and it is fundamentally premised on the notion that behavioral intention is positively influenced by attitude as well as by subjective norms. According to these scholars, intention and in this case adoption intention of MCTA is an important precursor to actual behavior, thereby suggesting that in the current pandemic context, actual use of MCTA is predominantly predicated upon the willingness on the part of individuals to download and use MCTA. Importantly, this study focuses on revisiting the empirical links between attitude and behavioral intention in the MCTA context. Accordingly, we define attitude as the positive or negative beliefs that individuals have toward the use of MCTA, while intention reflects the willingness to download and use MCTA (see also, Bagozzi, Citation1981; Fishbein & Ajzen, Citation1975). Taken together, we believe TRA in addition to HBM provides a useful theoretical reference to understand key individual determinants of MCTA adoption intention.
2.3. Hypotheses development
2.3.1. Perceived disease vulnerability and attitude toward MCTA
Perceived disease vulnerability is the individual’s belief about the possibility of contracting a disease (Carico et al., Citation2020; Carpenter, Citation2010; Loke et al., Citation2015). When people perceive that they are susceptible to a certain condition or disease, the perception will affect their attitude toward the disease and so they will be more likely to take preventive action. In this study, we argue that an individual may develop a positive attitude toward MCTA if he/she perceives a greater degree of vulnerability to COVID-19 infection. Similarly, extant studies have found a positive relationship between perceived disease vulnerability and attitude toward the disease (Huang et al., Citation2020; Zhao et al., Citation2018) and consequently leading to the following hypothesis:
H1: Perceived vulnerability to COVID-19 positively influences attitude toward MCTA.
2.3.2. Perceived disease severity and attitude toward MCTA
Perceived severity refers to a person’s appraisal of how severe the result of a possible threat might be (Champion & Skinner, Citation2008; Wu, Citation2020). In the context of this study, perceived disease severity represents an individual’s evaluation of the severity of a COVID-19 infection assuming that the individual failed to engage in preventive health behaviors such as using MCTA and ended up contracting the disease. Literature has established that there is a positive relationship between perceived disease severity and attitude toward the disease (Zhao et al., Citation2018). More so, according to a recent study, perceived disease threat—analogous to perceived disease severity—is a strong predictor of attitude toward mobile health (Birkmeyer et al., Citation2021). Therefore, leading to the following hypothesis:
H2: Perceived severity of COVID-19 positively influences attitude toward MCTA.
2.3.3. Perceived barriers of taking action and attitude toward MCTA
In accordance with past research (Ghavami et al., Citation2016; Janz & Becker, Citation1984), this study defines perceived barriers of taking action as the perception that individuals hold about the negative aspects of engaging in preventive health behavior. According to Rosenstock (Citation1974), the negative aspects of preventive health action, such as cost, pains or inconveniences may hinder a person from taking such actions. In our context, the individual may not be motivated to use MCTA if he/she perceives that the use of the app could be very demanding and especially in terms of cost. In certain situations, the individual-user might even forget to turn on the app notification and therefore might be an important concern and further placing additional responsibility on the user. Taken together, perceived barriers to taking action in the MCTA context implies the inconvenience and cost-related factors that may be associated with the take-up of MCTA. Importantly, there are suggestions in the literature that perceived barriers of taking action can considerably undermine individuals’ attitude toward preventive health behavior (e.g., Deng, Citation2013). Accordingly, the following is hypothesized:
H3: Perceived barriers of taking action negatively influences attitude toward MCTA.
2.3.4. Attitude and intention to adopt MCTA
Consistent with TRA theorists (Fishbein & Ajzen, Citation1975), we argue that individuals who have a positive attitude toward MCTA will be more inclined to use the app. This also means that the intention to download and use MCTA could be significantly hampered by individuals with negative attitudes toward the app. More so, many previous empirical studies including in mobile health (Schuster et al., Citation2017; Zhang et al., Citation2014) and mobile advertising (Kurtz et al., Citation2021) have found that attitudinal formation toward a given object plays an important role in behavioral intention toward the object. Furthermore, in a recent study, although in the internet surfing context, it was found that attitude mediates the influence of both perceived severity and vulnerability on knowledge withholding intentions (Wu, Citation2020). Similarly, within the tourist health context, Huang et al. (Citation2020) concluded that attitude toward preventive behavior strongly mediates the influence of perceived vulnerability on preventive behavior. All this leads to the following hypotheses:
H4: Attitude toward MCTA positively influences the intention to adopt MCTA.
H5: Attitude toward MCTA mediates the influence of (a) perceived disease vulnerability, (b) perceived disease severity and (c) perceived barriers to taking action on the intention to adopt MCTA.
below depicts our research model which is based on the health belief model and the theory of reasoned action.
Figure 1. Proposed research model based on HBM and TRA.
3. Research Methods
3.1. Data collection and sample characteristics
Consistent with research focusing on the pandemic context (Laato et al., Citation2020; Walrave et al., Citation2020), as well as based on social distancing requirements, respondents were recruited online and using platforms such as Facebook and WhatsApp. Regarding the sampling approach, we relied on network referral approach (Kuo et al., Citation2020). This approach, akin to snowballing and respondent-driven sampling network referral sampling is useful when it is hard to reach the respondents (Rohe, Citation2019). Accordingly, although network referral sampling has its limitations, such as lack of control of confidentiality, and the issue of subjective judgment of informants (Johnson, Citation2014), given the COVID-19 pandemic, it was the most appropriate compared to other sampling methods, such as convenient sampling or simple random sampling.
Importantly, participants were assured that their anonymity will be maintained and that the survey results will only serve for scientific purposes. We provided an explanation in the cover page regarding how the COVID-19 contact tracing app (i.e. MCTA) is potentially expected to work and assured the participants that there were no correct or wrong answers to the survey questions. In addition both the well-known Harman factor and collinearity were adopted to gauge the incidence of CMB. Results from Harman’s single-factor test indicate 32.58% as maximum co-variance explained by the most dominant factor in the study, which implies that the present study is not affected significantly by CMB. Results of Harman’s single-factor test are depicted in Appendix A. Further, the variance inflation factor (VIF) values recorded in also indicates that the study is free from CMB as all the VIFs were below the acceptable threshold of 5 (James et al., Citation2013). We sent out 350 online survey links; however, we received 151 complete responses representing a 43% response rate in the end. Further, before we proceeded to run the analysis, we discarded 14 responses from Nigerians living abroad, reducing the sample size to 137 responses for the final analysis. Indeed, this low response rate could be attributed to the Internet survey method used. Although the internet survey method is a useful tool for data collection in studies regarding the public, it has several disadvantages. For instance, Dillman et al. (Citation2014) have noted that in the Internet survey method, factors, such as access to the Internet, poor internet skills, and knowledge may be limitations to some respondents. In all, the data collection lasted for four months (i.e. May to August 2020).
Table 1. Descriptive statistics of research sample
Table 2. Measurement scales, dimensionality statistics, construct reliability and convergent validity
However, to answer the question of whether our 137 sample size was adequate to test the model, we relied on statistical software-the G*Power (Faul et al., Citation2009). Faul et al. (Citation2009) noted that the G*Power is robust in assessing the required minimum sample size and also able to avoid any disturbances geared toward statistical significance. Accordingly, the G*Power analysis of the present study showed that we needed 74 responses as the minimum sample size considering an effect size of 0.15, 0.05 significance level and 0.95 as statistical power (see for details).
3.2. Measurement items and statistical technique
The current study adopts a hypothetico-deductive research paradigm. This approach is well documented for studying social phenomena as in the case of this study—which intends to assist in converting responses into numerical data (Broadbent & Unerman, Citation2011). All the measures used in this study were adapted from previous studies to ensure content validity. The measurement items for perceived barriers of taking action were originally from Deng (Citation2013) but modified to suit the current investigation. The remaining measures used in the study were adapted from Sun et al. (Citation2013). provides a list of the measurement items used in the research. A Likert scale of 5 point scale was used to collect numerical data on the phenomenon under study. The current study relied on path modeling technique and employed ADANCO 2.2 software (Henseler & Dijkstra, Citation2017) to test the proposed model. The primary reason for using path modeling technique has to do with the exploratory nature of the current investigation as well as the fact that it is one of the most widely used techniques in the literature and especially in the last few years (e.g., Dawi et al., Citation2018; Vergara & Maza, Citation2018). Moreover, SEM is as a second generational statistical technique, which provides support in testing a multifaceted relationship associated with both observed and latent variable simultaneously and these unique characteristics of SEM are in sharp contrast with the first generational statistical techniques, such as linear regression, which studies the relationship with one endogenous variable at a time, resulting in imprecise results in the case of mediated/moderated relationships (Iacobucci, Citation2009). In essence, SEM is able to integrate multiple regression and factor analyses and subsequently runs fit indexes (Iacobucci, Citation2009; Tabachnick et al., Citation2007) for further interpretations.
4. Data analysis and results
4.1. Analysis of sample demographics
The results of the analysis show that about 45% of the respondents reported that they have heard about COVID-19 contact tracing app (MCTA). Most of these people had heard about MCTA through social media, while comparatively lesser number of people had heard about it on radio or television. Important details regarding the sample demographics are shown in .
4.2. Measurement model
In accordance with recommendations in the literature (Benitez et al., Citation2020; Hair et al., Citation2019), we assessed the measurement model by inspecting the magnitude and significance of the factor loadings, construct reliability, convergent and discriminant validity. As reflected in , our measurement model meets all the commonly reported thresholds in the literature. Only one item was dropped from the final analysis due to poor loadings and the construct reliability using both rho and Cronbach's alpha exceeds the recommended cut-off value of 0.8. With respect to convergent validity, all average variance extracted values were greater than the often-reported 0.5 threshold in the literature (Benitez et al., Citation2020; Hair et al., Citation2019; Jibril et al., Citation2020).
Table 3. Discriminant validity based on HTMT criterion
The heterotrait–monotrait ratio of common factor correlations (HTMT) was used to assess discriminant validity of the research constructs (; Henseler et al., Citation2015). The HTMT values were found to be below the 0.9 cut-off value (Benitez et al., Citation2020).
4.3. Structural model
Following recent research (Benitez et al., Citation2020), the authors assessed the structural model by first reporting on the fit statistics for the estimated and saturated model (see, ). Thereafter, we assessed the coefficient of determination (R2) and significance of the path coefficients based on a bootstrapping procedure of 4999 resamples. The R2 indicated that 58.8% of adoption intention can be explained by the model. Further, the model explains 17.1% variation in attitude toward MCTA.
Table 4. Results of the overall model fit statistics
The results of the structural model as shown in below indicated support for five out of the seven hypothesized effects. Harman’s single-factor test and the full-collinearity approach (Kock, Citation2015) were employed to study the results, which indicated further that CMB is not a significant risk and thereby reinforcing the validity of the research results.
Table 5. Structural model path analysis
5. Discussion
Considering the prevailing pandemic that the world finds itself in, we undertook this research with the goal of contributing to the emerging discussions on MCTA, especially with respect to factors that can significantly influence the attitudes and intentions of individuals to voluntarily download and use MCTA that is critical to the containment of COVID-19 community spread. This study based on a dual-theoretical lens provide initial support for five out of seven hypothesized effects. The research results reveal that both perceived disease vulnerability and perceived disease severity positively influence attitude toward MCTA, thus validating research hypotheses 1 and 2. Consistent with extant literature (Huang et al., Citation2020; Zhao et al., Citation2018), this finding suggests that individuals who perceive that they are more vulnerable to the COVID-19 infection and also perceive the COVID-19 pandemic to have severe consequences, are more likely to develop a positive attitude toward the initial use of MCTA. Therefore, it is important for governments to continue educating their citizenry about the vulnerability and severity of the COVID-19 disease prevalence, as perceived disease vulnerability and severity have been found to be an important precursor to attitudes toward MCTA. However, in contrast to our expectations, the results show that perceived barriers to taking action do not have a significant negative impact on attitude toward MCTA. Thus, research hypothesis 3 was unsupported. Although this finding deviates from some previous studies (e.g., Deng, Citation2013), it could mean that individuals are not very concerned about the cost of downloading the app and/or the inconvenience that might come with the app use. In other words, the impact of perceived barriers of taking action on attitudes toward MCTA is negligible. In summary, the current study provides some evidence regarding the utility of HBM concepts namely perceived disease severity and perceived disease vulnerability in predicting attitude toward the adoption of MCTA (see, also Rosenstock et al., Citation1988) and by extension it complements the research of Walrave et al. (Citation2020) that was focused on MCTA adoption based on data collected from Belgium.
At the same time, it is important to mention also that the current research differs from Walrave et al.’s (Citation2020) not only regarding the geographic scope of the study but also the fact that the current research finding provides strong statistical relationships between perceived disease severity/vulnerability and attitude toward MCTA, which was not the case in Walrave et al. (Citation2020). Meanwhile, the current finding indicating that both perceived disease severity and vulnerability are influential determinants of attitudes toward using MCTA is akin to the research conclusion in Birkmeyer et al. (Citation2021) regarding the positive correlation between perceived disease threat and attitude toward mobile health. More so, the current research model’s predictive ability and with respect to attitude compares favorably well with those of Birkmeyer and colleagues in the mobile health context. In fact, while Birkmeyer et al.’s study explains 14.1% variation in attitudes, the current model predictive ability is relatively higher as it explains 17.1% variation in attitudes toward MCTA.
Furthermore, and as expected, research hypotheses 4 was empirically validated since it was found that adoption intention of MCTA is positively influenced by attitude toward MCTA. As per the TRA literature (e.g., Ajzen & Fishbein, Citation2005), it is important to note that the current research finding provides validation for TRA in the MCTA context and consequently demonstrating the applicability of TRA in an emergency and pandemic context. At the same time, the current research evidence is largely consistent with the TRA logics (Fishbein & Ajzen, Citation1975) as well as extant empirical research on TRA (Kurtz et al., Citation2021; Zhang et al., Citation2014; Zhao et al., Citation2018).
Finally, the current study has unveiled how HBM concepts, namely perceived disease severity and vulnerability influence MCTA acceptability, which is shown to be attitudes toward MCTA. Importantly, this finding is consistent with findings reported in other fields, such as knowledge behaviors in the internet surfing context (Wu, Citation2020). However, to our knowledge, this is the first initial study within the pandemic and MCTA context to show that individual attitudes toward MCTA mediate the relationship between perceived disease severity, perceived disease vulnerability and willingness to download and use MCTA. In fact, according to the current study, individuals’ evaluation of the potential severity of COVID-19 infection, as well as susceptibility to the disease, motivate them to engage in preventive health behavior by developing a positive attitude toward MCTA and ultimately intention to adopt MCTA. Therefore, this study by combining HBM with TRA has increased our understanding of the individual determinants of MCTA acceptability. It is interesting to note that the proposed model explains about 58.8% variation in the intention to adopt MCTA that is critical in the fight against the community spread of COVID-19.
Therefore, the policy implication of the research finding is that policymakers and especially health authorities in different parts of the world and including African nations should continue to educate members of the public through the conventional media and new media about the significant health risks associated with the novel coronavirus, especially since perceived disease vulnerability and severity have been proven to be positively associated with attitude toward MCTA and, in turn, willingness to download and use MCTA.
6. Conclusion
The goal of this initial study was to develop a sound theoretical understanding of the individual determinants of the intention to download and use MCTA based on HBM and TRA tenets. Our research results have indicated that, while perceived barriers of taking action play a very limited role in influencing attitudes toward MCTA, both perceived disease vulnerability and severity positively influence attitudes toward MCTA and this, in turn, implicates individuals’ intention to adopt MCTA. An important take-home of the current research is the finding that attitude is a key factor through which the HBM concepts of perceived disease vulnerability and severity affect the adoption intention of MCTA. The authors, nevertheless, recognize that the current research is limited in several ways especially as our study should be considered as a preliminary analysis. Notably, an important limitation of the current study is the fact that the current study is based on data collected from a single country and further suffers from limited sample size, although this does not in any way discredits the research findings. We also acknowledge a limitation in the sampling approach considering the general demerits with network referral technique used. Considering this limitation, we recommend that future study tests the proposed model in different cultural and economic contexts and also adopt different sampling approaches, especially probability sampling techniques. It is only through this that we will be able to fully ascertain about the generalizability of the proposed model and the findings thereof. Another limitation concerns the notion that there could be additional factors that lie outside the current research scope and such factors may include individual disposition to trust, COVID-19 skepticism, herding behavior, and concerns relating to government surveillance and intrusion. Therefore, there is a need for future investigation of the role of the highlighted factors in MCTA acceptance. This way, we can develop an enhanced understanding of the individual determinants of MCTA acceptance and especially its voluntary take-up. Lastly, these authors are mindful that adoption intention may not always translate into actual use in practice, and therefore there is a need for future research to investigate this important concern and even the issue of discontinuance use, especially considering the current pandemic dynamics (e.g., lockdown fatigue and COVID-19 conspiracy theories). Notwithstanding the current research limitations, we believe this initial study has shed important light regarding the individual determinants of MCTA acceptability. Therefore, health policymakers and related government bodies are advised to engage actively with members of the public by crafting compelling health messaging around the threats that the novel coronavirus carries as this has been shown to be a strong predictor of attitudes toward MCTA and, in turn, the adoption intention of MCTA.
Acknowledgments
The Corresponding author acknowledges support from Research Project No. IGA/FaME/2021/003 entitled “Consumer behaviour and Performance management of firms in a competitive digital world”.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Alex Ntsiful
Alex Ntsiful is a PhD Student in the Department of Business Administration, Tomas Bata University in Zlin, Czech Republic. In his doctoral thesis, Alex examines how technology adoption in performance management practices translates into superior performance. Primarily, Alex’s research focuses on three key thematic areas: (a) User acceptance of digital technologies at both the firm- and individual-user level, (b) digitalization and performance management research, and (c) concepts of predictive analytics and advanced methodological approaches to research. He holds a Master of Business Administration and Bachelor of Arts in Psychology degrees, both from the University of Ghana. He is also a certified Professional in Human Resource (PHR) from the Human Resource Certification Institute, USA.
References
- Abbas, R., & Michael, K. (2020). COVID-19 contact trace app deployments: Learnings from Australia and Singapore. IEEE Consumer Electronics Magazine, 9(5), 65–15. https://doi.org/10.1109/MCE.2020.3002490
- Ajzen, I., & Fishbein, M. (2005). The influence of attitudes on behaviour. In D. Albarracin, B. T. Johnson, & M. P. Zanna (Eds.), Handbook of attitudes and attitude change (pp. 1–146). Erlbaum.
- Alsaad, A., & Al-Okaily, M. (2021). Acceptance of protection technology in a time of fear: The case of Covid-19 exposure detection apps. Information Technology & People, ahead-of-print(ahead–of–print), ahead-of-print. https://doi.org/10.1108/ITP-10-2020-0719
- Altmann, S., Milsom, L., Zillessen, H., Blasone, R., Gerdon, F., Bach, R., Kreuter, F., Nosenzo, D., Toussaert, S., & Abeler, J. (2020). Acceptability of app-based contact tracing for COVID-19: Cross-country survey evidence. SSRN Electronic Journal 8 (8) 1-9/e19857 . Available at SSRN 3590505. https://doi.org/10.2139/ssrn.3590505
- Amnesty International. (2020). Bahrain, Kuwait and Norway contact tracing apps among most dangerous for privacy. https://www.amnesty.org/en/latest/news/2020/06/bahrain-kuwait-norway-contact-tracing-apps-danger-for-privacy/
- Bagozzi, R. P. (1981). Attitudes, intentions, and behavior: A test of some key hypotheses. Journal of Personality and Social Psychology, 41(4), 607. https://doi.org/10.1037/0022-3514.41.4.607
- Benitez, J., Henseler, J., Castillo, A., & Schuberth, F. (2020). How to perform and report an impactful analysis using partial least squares: Guidelines for confirmatory and explanatory IS research. Information & Management, 57(2), 103168. https://doi.org/10.1016/j.im.2019.05.003
- Birkmeyer, S., Wirtz, B. W., & Langer, P. F. (2021). Determinants of mHealth success: An empirical investigation of the user perspective. International Journal of Information Management, 59, 102351. https://doi.org/10.1016/j.ijinfomgt.2021.102351
- Broadbent, J., & Unerman, J. (2011). Developing the relevance of the accounting academy: The importance of drawing from the diversity of research approaches. Meditari Accountancy Research, 19(1), 7–21. https://doi.org/10.1108/10222521111178600
- Carico, R. R., Sheppard, J., & Thomas, C. B. (2020). Community pharmacists and communication in the time of COVID-19: Applying the health belief model. Research in Social and Administrative Pharmacy 17 (1) 1984–1987 https://doi.org/10.1016/j.sapharm.2020.03.017.
- Carpenter, C. J. (2010). A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Communication, 25(8), 661–669. https://doi.org/10.1080/10410236.2010.521906
- Champion, V. L., & Skinner, C. S. (2008). The health belief model. Health Behavior and Health Education: Theory, Research, and Practice, 4, 45–65.
- Chan, E. Y., & Saqib, N. U. (2021). Privacy concerns can explain unwillingness to download and use contact tracing apps when COVID-19 concerns are high. Computers in Human Behavior, 119, 106718. https://doi.org/10.1016/j.chb.2021.106718
- Dawi, N. M., Jusoh, A., Streimikis, J., & Mardani, A. (2018). The influence of service quality on customer satisfaction and customer behavioral intentions by moderating role of switching barriers in satellite pay TV market. Economics and Sociology, 11(4), 198–218. https://doi.org/10.14254/2071-789X.2018/11-4/13
- Deng, Z. (2013). Understanding public users’ adoption of mobile health service. International Journal of Mobile Communications, 11(4), 351–373. https://doi.org/10.1504/IJMC.2013.055748
- Dillman, D. A., Smyth, J. D., & Christian, L. M. (2014). Internet, phone, mail, and mixed-mode surveys: The tailored design method. John Wiley & Sons.
- Duan, S. X., & Deng, H. (2021). Hybrid analysis for understanding contact tracing apps adoption. Industrial Management & Data Systems, 121(7), 1599–1616. https://doi.org/10.1108/IMDS-12-2020-0697
- Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/BRM.41.4.1149
- Ferretti, L., Wymant, C., Kendall, M., Zhao, L., Nurtay, A., Abeler-Dörner, L., Parker, M., Bonsall, D., & Fraser, C. (2020). Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science, 368(6491 1–7). https://doi.org/10.1126/science.abb6936
- Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. Addison-Wesley.
- Fox, G., Clohessy, T., van der Werff, L., Rosati, P., & Lynn, T. (2021). Exploring the competing influences of privacy concerns and positive beliefs on citizen acceptance of contact tracing mobile applications. Computers in Human Behavior, 121, 106806. https://doi.org/10.1016/j.chb.2021.106806
- Ghavami, M., Harandy, T. F., & Kabir, K. (2016). The effect of educational intervention in promoting safe behaviors in a sample of Iranian primary school students: An application of the health belief model. Global Journal of Health Science, 8(11), e56712–e56712. https://doi.org/10.5539/gjhs.v8n11p242
- Guillon, M., & Kergall, P. (2020). Attitudes and opinions on quarantine and support for a contact-tracing application in France during the COVID-19 outbreak. Public Health, 188, 21–31. https://doi.org/10.1016/j.puhe.2020.08.026
- Hair, J., Risher, J., Sarstedt, M., & Ringle, C. (2019). When to use and how to report the results of PLS-SEM. European Business Review, 31(1), 2–24. https://doi.org/10.1108/EBR-11-2018-0203
- Hassandoust, F., Akhlaghpour, S., & Johnston, A. C. (2021). Individuals’ privacy concerns and adoption of contact tracing mobile applications in a pandemic: A situational privacy calculus perspective. Journal of the American Medical Informatics Association, 28(3), 463–471. https://doi.org/10.1093/jamia/ocaa240
- Henseler, J., & Dijkstra, T. (2017), “Adanco 2.0.1”, Composite Modeling (Kleve: Germany).
- Henseler, J., Ringle, C. M., & Sarstedt, M. (2015). A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the Academy of Marketing Science, 43(1), 115–135. https://doi.org/10.1007/s11747-014-0403-8
- Huang, X., Dai, S., & Xu, H. (2020). Predicting tourists’ health risk preventative behaviour and travelling satisfaction in Tibet: Combining the theory of planned behaviour and health belief model. Tourism Management Perspectives, 33, 100589. https://doi.org/10.1016/j.tmp.2019.100589
- Iacobucci, D. (2009). Everything you always wanted to know about SEM (structural equations modeling) but were afraid to ask. Journal of Consumer Psychology, 19(4), 673–680. https://doi.org/10.1016/j.jcps.2009.09.002
- James, G., Witten, D., Hastie, T., & Tibshirani, R. (2013). An introduction to statistical learning (Vol. 112). Springer.
- Janz, N. K., & Becker, M. H. (1984). The health belief model: A decade later. Health Education Quarterly, 11(1), 1–47. https://doi.org/10.1177/109019818401100101
- Jibril, A. B., Kwarteng, M. A., Pilik, M., Botha, E., & Osakwe, C. N. (2020). Towards understanding the initial adoption of online retail stores in a low internet penetration context: An exploratory work in Ghana. Sustainability, 12(3), 854. https://doi.org/10.3390/su12030854
- Johnson, T. P. (2014). Snowball sampling: Introduction. Wiley StatsRef: Statistics Reference Online.
- Kasl, S. V., & Cobb, S. (1966). Health behavior, illness behavior and sick role behavior: I. Health and illness behavior. Archives of Environmental Health: An International Journal, 12(2), 246–266. https://doi.org/10.1080/00039896.1966.10664365
- Kock, N. (2015). Common method bias in PLS-SEM: A full collinearity assessment approach. International Journal of e-Collaboration, 11(4), 1–10 doi: 10.4018/ijec.2015100101.
- Kuo, Y. F., Lin, C. S., & Wu, C. H. (2020). Why do people intend to back crowdfunding projects? a perspective on social cognitive theory. Journal of Electronic Commerce Research, 21(3), 180–196.
- Kurtz, O. T., Wirtz, B. W., & Langer, P. F. (2021). An empirical analysis of location-based mobile advertising—Determinants, success factors, and moderating effects. Journal of Interactive Marketing, 54, 69–85. https://doi.org/10.1016/j.intmar.2020.08.001
- Laato, S., Islam, A. N., Islam, M. N., & Whelan, E. (2020). What drives unverified information sharing and cyberchondria during the COVID-19 pandemic? European Journal of Information Systems 29 (3) , 288–305 https://doi.org/10.1080/0960085X.2020.1770632.
- Li, T., Cobb, C., Yang, J. J., Baviskar, S., Agarwal, Y., Li, B., and Hong, J. I. (2021). What makes people install a COVID-19 contact-tracing app? Understanding the influence of app design and individual difference on contact-tracing app adoption intention. Pervasive and Mobile Computing, 75, 101439.
- Lin, J., Carter, L., & Liu, D. E. (2021). Privacy concerns and digital government: Exploring citizen willingness to adopt the COVID Safe app. European Journal of Information Systems, 30(40), 389–402. https://doi.org/10.1080/0960085X.2021.1920857
- Litan, R. E., & Lowy, M. (2020). Freedom and privacy in the time of coronavirus. The Brookings Institution. https://www.brookings.edu/research/freedom-and-privacy-in-the-time-of-coronavirus/
- Loke, A. Y., Davies, L., & Li, S. F. (2015). Factors influencing the decision that women make on their mode of delivery: The Health Belief Model. BMC Health Services Research, 15(1), 274. https://doi.org/10.1186/s12913-015-0931-z
- Madden, T. J., Ellen, P. S., & Ajzen, I. (1992). A comparison of the theory of planned behavior and the theory of reasoned action. Personality & Social Psychology Bulletin, 18(1), 3–9. https://doi.org/10.1177/0146167292181001
- Mou, J., Shin, D. H., & Cohen, J. (2016). Health beliefs and the valence framework in health information seeking behaviors. Information Technology & People, 29(4), 876–900. https://doi.org/10.1108/ITP-06-2015-0140
- Rohe, K. (2019). A critical threshold for design effects in network sampling. The Annals of Statistics, 47(1), 556–582. https://doi.org/10.1214/18-AOS1700
- Rosenstock, I. M. (1974). Historical origins of the health belief model. Health Education Monographs, 2(4), 328–335. https://doi.org/10.1177/109019817400200403
- Rosenstock, I. M., Strecher, V. J., & Becker, M. H. (1988). Social learning theory and the health belief model. Health Education Quarterly, 15(2), 175–183. https://doi.org/10.1177/109019818801500203
- Rowe, F., Ngwenyama, O., & Richet, J. L. (2020). Contact-tracing apps and alienation in the age of COVID-19. European Journal of Information Systems 29 (5) , 545–562 https://doi.org/10.1080/0960085X.2020.1803155.
- Schuster, L., Tossan, V., & Drennan, J. (2017). Consumer acceptance of mHealth services: A comparison of behavioral intention models. Services Marketing Quarterly, 38(2), 115–128. https://doi.org/10.1080/15332969.2017.1289791
- Statista. (2020). Mobile phone user penetration as percentage of the population worldwide from 2013 to 2019 Statista Research Department, .
- Sun, Y., Wang, N., Guo, X., & Peng, Z. (2013). Understanding the acceptance of mobile health services: A comparison and integration of alternative models. Journal of Electronic Commerce Research, 14(2), 183.
- Tabachnick, B. G., Fidell, L. S., & Ullman, J. B. (2007). Using multivariate statistics (Vol. 5). Pearson.
- Trang, S., Trenz, M., Weiger, W. H., Tarafdar, M., & Cheung, C. M. K. (2020). One app to trace them all? Examining app specifications for mass acceptance of contact-tracing apps. European Journal of Information Systems, 29(4), 415–428. https://doi.org/10.1080/0960085X.2020.1784046
- Vergara, J. C., & Maza, F. J. (2018). structural equation models applied for evaluating service quality and satisfaction in the healthcare system of Cartagena de Indias D. T. y C (Colombia). Economics and Sociology, 11(2), 200–215. https://doi.org/10.14254/2071-789X.2018/11-2/14
- VOA News. (2021). WHO: Africa left behind in race for COVID-19 vaccine. https://www.voanews.com/africa/who-africa-left-behind-race-covid-19-vaccine
- Walrave, M., Waeterloos, C., & Ponnet, K. (2020). Adoption of a contact tracing app for containing COVID-19: A health belief model approach. JMIR Public Health and Surveillance, 6(3), e20572. https://doi.org/10.2196/20572
- WHO. (2020). WHO coronavirus disease (COVID-19) dashboard. https://covid19.who.int/
- Wu, D. (2020). Empirical study of knowledge withholding in cyberspace: Integrating protection motivation theory and theory of reasoned behavior. Computers in Human Behavior, 105, 106229. https://doi.org/10.1016/j.chb.2019.106229
- Zhang, X., Guo, X., Lai, K., Guo, F., & Li, C. (2014). Understanding gender differences in m-Health adoption: A modified theory of reasoned action model. Telemedicine and e-Health, 20(1), 39–46. https://doi.org/10.1089/tmj.2013.0092
- Zhao, Y., Ni, Q., & Zhou, R. (2018). What factors influence the mobile health service adoption? A meta-analysis and the moderating role of age. International Journal of Information Management, 43, 342–350. https://doi.org/10.1016/j.ijinfomgt.2017.08.006
Appendix A.
Result of Harman’s single-factor test
Figure B1. Sample size adequacy calculation result.
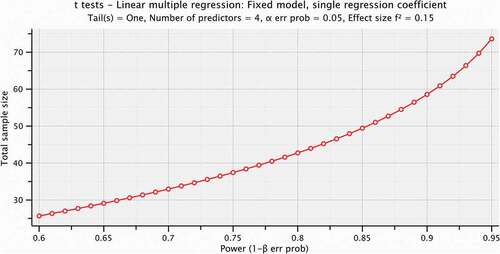
Figure B2. An image showing the structual model result.