
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
The medical poverty trap can lead to the impoverishment of households and further impoverishment of the poor. The most crucial factor known at this point is that it is closely related to the socio-economic characteristics of the households. Because the income level of the household is among the crucial determinants of out-of-pocket health expenditure, the increase in out-of-pocket health expenditures will have a significant negative impact on equality and access. Research on child mortality and its determinants reveals that public health researchers address typical issues. Interdisciplinary studies are needed to determine the dynamics of the health field. For this reason, this study aims to examine the effects of income and health expenditures on child mortality and to make suggestions in terms of both child health and social development. As a result of the counting data model, it was determined that the most influential variable increasing child mortality was income inequality, and the decreasing variable was the ratio of out-of-pocket health expenditures to total health expenditures. The study results support the necessity of considering the factors mentioned in determining policies toward achieving higher quality and welfare increasing targets as a result of economic development. If children have equal rights, their development will be completed healthily, and stronger families and societies will emerge.
PUBLIC INTEREST STATEMENT
Children are one of the basic building blocks that play an essential role in determining societies’ future and ensuring their development. Infant and child mortality rates, which are one of the leading indicators of development, are an essential indicator of society’s income level and health status. In terms of social inequality, it is also critical that all children are provided with equal opportunities without discrimination to ensure their fundamental human rights. Interdisciplinary studies are needed to determine the dynamics of the health field. Findings from this research assist policymakers in developing strategies.
1. Introduction
Children play an essential role in determining a society’s future development. The effect of children on this development is only possible by ensuring their active participation in society. In order to realize this participation, sociological, physiological, and psychological needs must be met, and children’s rights must be protected. Individuals under the age of 18 are defined as “children” in the Convention on the Child’s Rights, as signed by Turkey in 1990. This agreement outlines the right of children to live, fully participate in social life, and develop fully regardless of their gender, religion, and origin (UNICEF, Citation1990). It is also essential in social inequality that a child’s fundamental rights are provided equally without discrimination. If children have these rights, their healthy development will be completed, and stronger families and societies will emerge. Improving a society’s human capital includes factors such as health and education (Öngel et al., Citation2014, p. 586). For this reason, protection of children’s rights and providing equal opportunities play essential roles in a country’s development.
Infant and child mortality rates, which are among the primary indicators of development, are essential indicators of income level and health. These rates are also among the most important criteria used in evaluating the effectiveness of the country’s health services (UNICEF, Citation1991, p. 115). Increase in a society’s health level is typically a positive reflection of its economy (Mushkin, Citation1962, p. 132). Therefore, it is important to consider health expenditures as investment expenditures and understand their contribution to income and economic growth (Mushkin, Citation1962, p. 143). Blum, Roemer, and Lerer made various classifications for health status determinants. The common feature of these classifications is that health is a substantial indicator of a country’s development; however, it is also necessary to consider factors such as environment and behavior (Barlas et al., Citation2014, p. 576). Primarily, the fact that a child’s health begins before the child is born and it is related to household income which is an important point to consider. A mother’s nutritional status and social condition affect fetal health. Thus, it is necessary to provide appropriate income and health conditions for a mother, who is a child’s only environment. The circumference of a child gradually expands from the age of six months. If there is a lack of income and basic health needs in the family and community circles, new dangers will inevitably arise
Determining how much a country should spend on health services is determined by a budget, which is determined by politicians. According to the health economy approach, appropriate resources should be determined to ensure efficiency with health input such as health care production and delivery (health service supply), consumption (health service demand), use of all kinds of resources in this area, distribution among sectors (resource allocation), the financing of health services, and the economic consequences of regulations concerning individual and public health, the creation of health policies. Evaluation of the results is the main topic in health economics. In determining these, public health expenditures for individuals and society and management expenditures in which health services are measured are examined. The main objective in determining and regulating these expenditures is the regulation of the health services market. One of the primary methods in regulating the financing of the market is out-of-pocket health expenditures. However, due to increases in these expenditures there is a burden on households, which ultimately affects the poor in terms of access to healthcare services. For this reason, adopting the principle of equality in access to health opportunities for the poor is a critical point in determining financing policies. An increase in out-of-pocket health expenditures in the household budget can lead to the impoverishment of households and further impoverishment of the poor (Van Doorslaer et al., Citation2007; Wagstaff, Citation2001). This situation, which is called the “medical poverty trap”, is among the main reasons pushing individuals and households into poverty in many countries of the world (Whitehead et al., Citation2001). It is expected that the level of out-of-pocket health expenditures will be lower in a country where the social state approach is dominant. However, its share in total health expenditures is increasing in Turkey and all over the world. At this point, the most crucial factor known is that households are closely related to their socioeconomic characteristics. If out-of-pocket health spending becomes widespread and the primary source of health financing, it will significantly negatively impact equity and access. Therefore, identifying the relationships and especially determining the impact on child health will help policymakers make the most appropriate intervention in equal health care.
2. Literature review
Various definitions have been made in the literature on health policy, which is the main determinant of a country’s health indicators. In its most general form; It is defined as a political decision that includes all the actions that affect the institutions providing services within the health systems, the services provided by these institutions and the financing of these services (Koivusalo, Citation2009: 297). In line with Corman and Grossman (Citation1985), health expenditures for individuals below a certain income level are essential factors in reducing infant and child mortality rates. However, the fair distribution of these expenditures to the most vulnerable segment of society will have a more significant effect on reducing the number of deaths. Japan, which has maintained a relatively low per capita income since Second World War, is an example of the effective use of health expenditures in reducing child mortality, as the country made direct investments in public health, thus increasing life expectancy at birth (Johansson & Carl, Citation1987, p. 235). Preston (Citation1975), who examined the effects of income level on health, revealed the “Preston curve,” which shows no linear relationship between income and life expectancy. The author stated that, due to the increase in per capita income level, life expectancy is improving rapidly (Preston, Citation2007: 484). Further, Rodgers (Citation1979) determined that both income and income inequality are decisive factors in the differentiation of countries’ health outcomes, stating that the life expectancy in low- and high-income countries varies between five to 10 years.
As of 2017, 118 out of 195 countries have under-five mortality rates below the United Nations Sustainable Development Goal of less than 25 deaths per 1000 live births (United Nations, Citation2020). The under-five mortality rate is a significant public health problem, especially in East African countries. When we look at the studies on this subject, it is seen that the provision of health facilities, higher wealth status, and adequate birth interval are significantly associated with a lower risk of death under the age of 5. In particular, economic growth seems to be associated with an increase in the poor-rich differences in under-five mortality rates (Houweling et al., Citation2005, p. 1263). Also, regardless of national development, the poor have less access to health care, resulting in differences in mortality rates (Peters et al., Citation2008). Studies on income status in the health field are typically discussed in the context of total income and income inequality hypotheses. Preston (Citation1975) and Deaton (Citation2003), according to the absolute income hypothesis, revealed that policies will increase welfare levels by increasing health outcomes due to increasing income levels in the countries. The income inequality hypothesis further claims that policies that correct income distribution are necessary. Kawachi and Kennedy (Citation1999) further stated that, due to high-income inequality, low human capital investments in countries and poor people could not benefit from economic opportunities. Social capital, which disappears as a result of income inequality, increases the conflict between the poor and the rich and decreases welfare levels. As a result, relative social deprivation and adverse health conditions occur. Subramanian and Kahveci (Citation2004), in another critical study that discussed in the context of the income inequality hypothesis, claimed that poor people gather in the same regions due to income inequality. Political inequalities occur with the decrease in social capital, and health outcomes are negatively affected. Studies considered within the income inequality hypothesis note that mortality rates in poor populations are mainly due to social and political inequalities; as such, the relationship between socioeconomic status and health indicators has become an important subject. Relationships between income-health status and income-death rates have also been examined (Lindahl, Citation2002, p. 1). Yılmaz and Akdede (Citation2016), in their study using data from 149 countries between 2002 and 2012, confirmed that the effects of GDP per capita, female education level, income inequality, environmental health, and demographic structure on child mortality rate are high. Studies that directly examine the relationship between income and health in Turkey are limited, however.
Çoban (Citation2008), in examining the effects of education inequality, income, and income inequality on infant and adult mortality, stated that income inequality and health inequality negatively affect infant mortality rates. In addition, it has been determined that as income level increases infant deaths decrease. Tüylüoğlu and Tekin (Citation2009), in examining the effects of income level and health spending on life expectancy and infant mortality rates with the 2003 data of 176 countries, found that health expenditures were more effective on life expectancy and infant mortality than income level. In another study examining the effect of income and income inequality on health outcomes in Turkey, Çukur and Bekmez (Citation2011) found that income increase was in a negative relationship with infant and under-5-year-old mortality rates, and the relationship between income inequality and infant and under-5-year-old mortality rates was positive. Kahveci (Citation2004), in examining socioeconomic criteria, revealed that infant and child deaths occur more often in low-income families. Household income level affects children the most, and death and morbidity rates are the macro indicators of these effects.
Turkey has long faced high infant and child mortality rates, noting a rate of over 100 per 1,000 in infant mortality until the 1980s. This situation did not show a similar view with the level of economic development. The literature refers to this situation as the “Turkish Riddle” (Akşit & Akşit, Citation1989, p. 571). Although there has been progress in lowering infant and child mortality in the country, reducing inequality and differentiation in socio-economic groups has not been achieved sufficiently. Child mortality is one of the most important indicators of development and social equality in a country. Poverty shows its destructive effects mostly on children and causes families, in particular, to not meet their children’s needs adequately. As a result, the rate of malnutrition is lower in children of rich families compared with children of poor families; in addition, diarrhea and acute respiratory infections, which are relatively easy to treat, have low mortality rates when compared to diseases such as tuberculosis and malaria (Tüylüoğlu & Tekin, Citation2009, p. 8).
Worldwide, 600 million children live below the poverty line. In connection with poverty, 30,500 girls and boys under the age of five die every 14 days due to preven0table causes such as malnutrition and disease (Children’s Foundation, Citation2020). When evaluated in terms of child health, the most common effect of poverty is malnutrition, which causes more than one-third of the deaths of children under the age of five in the world; further, blindness, stunting, developmental retardation, and low IQ are also considered a result of poverty. Many studies show a strong relationship between malnutrition and stunting in Turkey and abroad (Konuk Şener & Ocakçı, Citation2014, p. 61) Hatun et al. (Citation2003), in examining the effects of poverty on child health, determined that economic inadequacy is the main reason for the increase in child mortality and morbidity rates. Filmer and Pritchett (Citation1999) argued that public health expenditures on infant and child mortality are relatively low, and the effect of per capita income, income distribution, women’s education, ethnic fragmentation, and the dominant religion is much higher. Dhrifi (Citation2018) found that health spending reduces child mortality in the middle- and high-income countries. In low-income countries, he stated that health expenditures did not affect children’s health. Helmert and Shea (Citation2014), Kaplan et al. (Citation2016) stated a direct relationship between death levels and income inequality. Rahman and Alam (Citation2021) stated that the total fertility rate and urbanization positively affect the child mortality rate. In addition, the adverse effects of women’s education, life expectancy at birth, and economic growth rate were determined. Rodriguez and Ve Neives (Citation2018), a one-way causality relationship from health expenditures to GDP in OECD and Latin American countries, Kouassi et al.’s (Citation2018), between health expenditures and economic growth of 14 SADC (South African Development Community) countries They found a positive relationship. In the studies conducted by Park and Nam (Citation2019), and Mohamoud et al. (Citation2019), a statistically significant relationship was found between the percentage of urban population and infant mortality rate. In another study, it was stated that the under-five mortality rate is related to the distribution of health personnel, female literacy and high GDP (Robinson & Wharrad, Citation2000, p. 28). Pašalić et al. (Citation2020) examined the demographic characteristics of Republika Srpska and made policy recommendations. The impact of the age structure of the population on the workforce has been emphasized in the country, which has significant demographic inequalities regarding spatial development and weak demographic resources and characteristics. It was stated that this would pose a significant challenge for policymakers and society. For this reason, it has been stated that new economic, tax, health, retirement, education, social, family, and other policies that affect the demographic structure should be shaped. Studies in the field of health are frequently handled from a national macro-economic perspective.
However, in the studies in the literature, it has been determined that the total health expenditures are frequently discussed. But, WHO stated that reducing out-of-pocket health expenditures is an important step for access to universal health services and quality of life (Evans et al., Citation2012). Because if out-of-pocket health expenditures exceed the household income, it will inevitably create a severe obstacle in front of health services. If this situation is detected, there is a need for either health plan implementations or health subsidies. Studies on child mortality and its determinants reveal that public health researchers typically address these issues. It can be said that interdisciplinary studies are needed to determine the dynamics of the health field. From this point of view, this study aimed to examine the effects of income and health expenditures on child mortality and make suggestions regarding children’s right to life and social development.
Findings from relational studies can be difficult to generalize or attribute to causal relationships, as they can be both a cause and a consequence of socioeconomic and health system development. Therefore, opposite findings can be expected in studies that adopt different methods and variables. Thus, the importance of studying child mortality is still worth exploring. On the other hand, changes in health indicators are caused not only by the country’s macroeconomic variables but also by the legal system adopted, the level of corruption in the country, the efficiency level of the public in the country, and the unemployment level, inflation, etc. It is also affected by political and economic variables. For this reason, it is necessary to determine what effect these political-economic variables have on fundamental health indicators. Evaluation, policy development, and assurance are essential components of health systems (Benjamin, Citation2020, p. 2).
3. Method
Counting data consists of positive values and generally does not reveal a normal distribution feature. In a study in which counting data is used, biased parameter estimators can be encountered if the linear regression method is used. For this reason, methods that take into account the original distribution of the data should be preferred. In this study, a negative binomial regression model, a generalization of Poisson regression, was used.
3.1. Negative binomial regression analysis
Counting data consists of the number of occurrences of any event due to the trials made within the specified period. In the case of discrete data, inconsistent and ineffective results are obtained in the analyzes to be made with linear regression models. Census data for rare events or events with a mean < 10 are almost always skewed and abnormal. Therefore, classical techniques that assume normality are not sufficient. It is one of the methods shown in addition to the classical linear regression analysis since it cannot be obtained due to the assumption of normality due to discreteness (Frome et al. Citation1973:935–940; Frome Citation1983:665–674). However, the most critical limitation of the method is the equality of variance and mean. In the census data application, this situation is generally not achieved. The overdispersion, which occurs due to the variance being more significant than the mean, usually causes model-building problems (Miaou, Citation1994, pp. 471–482). Ignoring the overdispersion in the Poisson regression model causes the variances to be underestimated. However, the predictions obtained using methods such as the maximum likelihood method of the regression parameters are consistent. (Yip Karen & Yau Kelvin, Citation2005, pp. 153–163). When excessive scattering occurs in the dataset, it is more appropriate to use Negative Binomial (NB) Regression Analysis, which considers scattering (Jean Philippe et al., Citation2007, pp. 110–131).
Since these models also model the difference in propagation, they prevent parameter estimators from giving biased results. In addition to these models, it is used in zero value-weighted Poisson and zero value-weighted negative binomial models to prevent problems from propagation. Apart from modeling the propagation, these models also eliminate problems in the case of significantly zero values in the analyzed data. The negative binomial regression in the Poisson regression model, which generalizes the assumption that variance equals the calculated mean, is based on a Poisson-gamma mixed distribution.
The most common negative binomial regression is the NB2 model, and the probability density function is given in EquationEq. (1(1)
(1) ), where a is the probability of occurrence of an event and d is the propagation parameter:
If d = 0 in EquationEq. (1(1)
(1) ), the regression is reduced to Poisson. Regression coefficients can mostly be estimated using the similarity method (A.C. Cameron & Trivedi, Citation1986, p. 32). The negative binomial regression model is given in EquationEq. (2
(2)
(2) ), and maximum likelihood estimation is given in EquationEq. (3)
(3)
(3) . It is obtained as
expressing the exponential mean.
When choosing between a negative binomial regression, which is a particular case of the Poisson regression model, the d value obtained from the estimation is examined. If the value of d is different from the value of zero, negative binomial regression is preferred. If it is not statistically significant, Poisson regression and negative binomial regression are the same (Arı & Önder, Citation2013, p. 169). Deciding on the appropriate regression model is the last step, and goodness-of-fit tests are used. In addition, the Akaike information criterion (AIC) is often used to select the most suitable model. This criterion establishes a balance between the number of parameters in the models and the goodness of fit (De Jong & Heller, Citation2008, pp. 62–63).
Marginal effects and relative risks are used to interpret the coefficients of the estimated model. Marginal effects interpret how a unit in the explanatory variables in the model will increase or decrease the value of the dependent variable on average. Relative risks are in converting the estimates obtained to the value of any event in a specific time interval. It is used to investigate the causal relationship between outcome and risk factors (İşçi Güneri & Durmuş, Citation2020, p. 56).
4. Findings
The relationship between child health and household income starts before a child is born and is contingent on income-level deprivation and meeting primary health needs. From this point of view, this study aimed to examine the effect of income status and health expenditures on mortality of children in the 0- to 5-year-old age group in Turkey. The variables used in the study were obtained from the World Bank. The Infant and Child Mortality Monitoring Program from 2009 to 2018, which is included in the Turkish child health policy, has been examined. Summary information on child deaths in the relevant years in Turkey is given in . (Child Mortality by Years in Turkey (2009–2018).
Figure 1. Child Mortality by Years in Turkey (2009–2018)
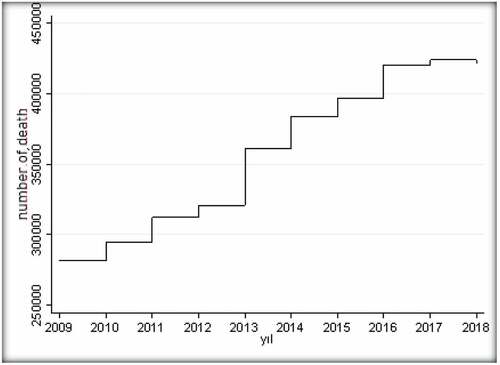
shows that the total number of child deaths in Turkey increased by 0.03% between 2009 and 2018. Descriptive statistics of the variables examined within the scope of addressing this situation are given in .
Table 1. Descriptive Statistics of the Variables
The correlation between the number of child deaths and other variables, which are among the variables whose descriptive statistics are given in (Descriptive Statistics of the Variables) and are aimed to be analyzed, has been examined. It has a high positive correlation of 0.8134 with the Gini coefficient used to express a country’s income distribution equality. In addition, the number of child deaths has a high positive correlation with the number of poor children with 0.7905, a moderate negative correlation with the ratio of out-of-pocket health expenditures to total health expenditures with −0.4222, and a positive correlation with the number of children living in unemployed households with a household head of 0.5391. It has a moderate correlation. In the stationarity analysis of the variables used, it was observed that the variables did not contain a unit root, that is, they were stationary. Classical Poisson regression estimation was performed before the census data was used to examine the number of child deaths after the analysis of the stationarity of the variables. However, the propagation parameter of the classical Poisson regression was calculated as 1.83; further, it was determined that the data showed excessive propagation because it was more significant than 1. In addition, it was decided that there is excessive spread as a result of obtaining statistically significant LR likelihood ratio test statistics (0.0000 < 0.05). For this reason, the negative binomial model was estimated by five iterations, and the results are given in . The model was estimated with robust standard errors technique to avoid the autocorrelation problem (A. C. Cameron & Trivedi, Citation2009).
Table 2. Negative Binomial Regression Estimation Results
The results in indicate all variables were statistically significant (p < 0.05). Accordingly, the negative binomial regression model is given in EquationEq. (4)(4)
(4) .
The spread parameter of EquationEq. (4)(4)
(4) differs significantly from zero and indicates that it is not equivalent to the Poisson distribution. For this reason, it has been determined that it is not suitable for Poisson distribution, and the use of the negative binomial regression model is more appropriate. As a result of the model’s link, it was concluded that the line probability value was determined as 0.008 (<0.05); further, the model was generally evaluated well and was determined correctly by obtaining the hatsq probability value as 0.083 (>0.05). In cases where the conditional variance exceeds the conditional mean, negative binomial and generalized negative binomial regressions are used. Although it was determined that classical Poisson regression was not suitable, the negative binomial regression model generalized with negative binomial regression was also evaluated according to the information criteria, and the results are given in . (Information Criteria for Regression Estimates)
Table 3. Information Criteria for Regression Estimates
In selecting the most suitable model, it is expected that the AIC and BIC criteria are minor and the likelihood values are the highest. In this case, the results in determined that the negative binomial regression model should be used. In order to make the coefficient interpretations of the model, the IRR values are calculated, and the results are given in . (Negative Binomial Regression Estimation Results)
Table 4. Negative Binomial Regression Estimation Results
In line with the results given in , in order for the determined relative risk ratios to be considered statistically significant, the odds ratio should not contain a value of 1, indicating equality in the confidence interval (Alpar, Citation2017, p. 607). The examination determined that there is no variable containing the value 1. While other variables are fixed, the average number of child deaths is 137299.9. The Gini coefficient variable determined the increased number of child deaths. According to other variables, the Gini coefficient has an approximately 1.26-fold effect on the number of child deaths . In the number of child deaths, the number of poor children, and the number of children living in unemployed households, the households increase by 0.999 times. The ratio of out-of-pocket health expenditures to total health expenditures has a 1.0783-fold decreasing effect on child deaths.
5. Conclusion and evaluation
This study examined the effect of income and health expenditures on child deaths in the 0- to 5-year-old age group in Turkey. The most appropriate harmful binomial regression method was used among the available models because the dependent variable is counting data. In line with the findings, it was determined that the most influential variable on child mortality figures was the Gini coefficient. Recently, different results obtained in studies examining the effect of income inequality on health outcomes brought along methodological discussions (Çukur & Bekmez, Citation2011, p. 34). However, since the relationship between these variables plays an important role in affecting social policies, the interest in health expenditures is increasing worldwide. In line with the study’s findings, it was noteworthy that the distribution of income should be addressed due to its large effect on child mortality. This situation of income inequality in terms of child mortality is essential in determining intervention policies. The need for economic and social policies aimed at eliminating inequality is essential in eliminating inequalities. In addition, it has been determined that the number of poor children and the number of children living in unemployed households has an increasing effect on child mortality. Income inequality and poverty are essential factors that need to be addressed in regard to Turkey’s socioeconomic problems. The results of the study support this situation experienced by children who are more at risk of being exposed to the adverse effects of poverty than adults. The previous finding supports the statement that infant and child deaths are seen more in low-income families when Kahveci’s (Citation2004) socioeconomic criteria are taken into account. For this reason, it is essential to generalize health services, make regulations on health rights, regulate income distribution, and eliminate social inequality, especially in society’s poor segments.
Out-of-pocket health expenditures, which express direct payments made by households or patients for receiving healthcare services, are an essential indicator in determining a country’s living standards. At the same time, health expenditures made by governments to increase economic efficiency are also crucial for the accumulation of human capital. In countries with high wealth levels, resource allocation to health services is higher than in countries with lower wealth levels. However, spending only on health may not necessarily mean better health outcomes. In order to achieve better results, various factors such as public health services, environmental conditions, and income status need to be addressed together. A country’s high-income level is not sufficient for health. It is also essential to ensure justice in income distribution because there is a rapid increase in the level of health in countries where justice is provided in income distribution.
This study’s findings determined that out-of-pocket health expenditures have a decreasing effect on child mortality. However, it has also been observed that the number of poor children in households where the head of the household is unemployed, income inequality has an increasing effect on child mortality. From this point of view, controlling the impact of out-of-pocket health expenditures on households, determining the coverage of health insurance by considering the poor segments of the society, determining the ability to pay by separating health expenditures from the essential expenditures of households, and ensuring justice in the distribution of income throughout the country are essential factors in determining a child’s health. It is also essential for a country’s economy that it is accessible to all segments of the society, including high-cost treatment methods, and that the income distribution is balanced. A country’s social and economic indicators at the development level need to be addressed. Contributions, which are a source of financing for out-of-pocket expenditures, are a financial barrier to accessing health services, especially in low- and middle-income countries. For example, as a result of the abolition of the contribution fee for services received in primary health care units in Uganda in 2001, the use of health services among the poor has increased. In Vietnam, poor individuals receive health care only in emergencies due to out-of-pocket expenses. However, at this point, meeting health expenditures with a third-party payment system may also bring an unnecessary increase in demand. This behavior of individuals may also cause inefficient use and insufficiency of resources. As a result, it may cause adverse health status of individuals who cannot benefit from health services adequately. With the increase in the number of people, a heavy burden may arise on the poor. Therefore, to ensure the sustainability of the health financing system, it is recommended to increase insurance coverage and determine appropriate policies.
The study results support the necessity of considering the factors mentioned in determining policies toward achieving higher quality and welfare increasing targets as a result of economic development. If children have equal rights, their healthy development will be completed, and stronger families and societies will emerge. For this reason, it is also essential for policymakers to elaborate on the studies in this field, examine child health regionally, and offer solutions. It can be said that child health is a human rights issue, which hinges on a society’s economic development.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors

Gökten Öngel
Md., Ph.D. Gökten Öngel is a specialist doctor at Istanbul Training and Research Hospital. Her public research interests are child health and diseases.
İsmail Erkan Çelik
İsmail Erkan Çelik is a Ph.D. lecturer at Doğuş University in Istanbul and Chairman of the Board of Trustees of Concept Vocational School. His general research interests are banking and finance.
Gözde Bozkurt
Gözde Bozkurt is a research assistant at Beykent University in Istanbul, Turkey, and a Ph.D. student at Marmara University. Her general research interests are econometrics and behavioral economics.
References
- Akşit, B. T., & Akşit, B. (1989). Sociocultural determinants of infant and child mortality. Social Science & Medicine, 28(6), 571–13. https://doi.org/10.1016/0277-9536(89)90251-7
- Alpar, R. (2017). Uygulamalı çok değişkenli istatistiksel yöntemler (5 ed.). Detay Yayıncılık.
- Arı, A. & Önder, H. (2013). Farklı veri yapılarında kullanılabilecek regresyon yöntemleri. Anadolu Tarım Bilimleri Dergisi, 28(3), 168–174. https://doi.org/10.7161/anajas.2013.28.3.168
- Barlas, E., Şantaş, F., & Kar, A. (2014). Temmuz Türkiye’de bölgesel bebek ölüm hızlarının sağlık ekonomisi perspektifinden karşılaştırmalı analizi. Paper presented at the International Conference on Eurasian Economies, Beykent University, Istanbul.
- Benjamin, G. C. (2020). Ensuring health equity during the COVID-19 pandemic: The role of public health infrastructure. Pan American Journal of Public Health, 44 , 1–4. https://doi.org/10.26633/RPSP.2020.70
- Cameron, A. C., & Trivedi, P. K. (1986). Econometric models based on count data: Comparisons and applications of some estimators. Journal of Applied Econometrics, 1(1), 29–53. https://doi.org/10.1002/jae.3950010104
- Cameron, A. C., & Trivedi, P. K. (2009). Microeconometrics using Stata. Stata Press.
- Children’s foundation. Retrieved July 21, 2021 from https://www.cocukvakfi.org.tr/wpcontent/uploads/2020/12/22_Yenibinyilin-Dunya-Cocuklari-Sayisal-Cocuk-uyari-Raporu.pdf
- Çoban, S. (2008). The Relationship among Mortality Rates, Income and Turkey and the Euro Area. MPRA, Paper No:13296.
- Corman, H., & Grossman, M. (1985). Determinants of neonatal mortality rates in the U.S. Journal of Economics, 4(3), 213–236. https://doi.org/10.1016/0167-6296(85)90030-X
- Çukur, A., & Bekmez, S. (2011). Türkiye’de gelir, gelir eşitsizliği ve sağlık ilişkisi: Panel veri analizi bulguları. Gaziantep Üniversitesi Sosyal Bilimler Dergisi, 10(1), 21–40. ISBN:1303-0094/2149-5459.
- De Jong, P., & Heller, G. Z. (2008). Generalized linear models for insurance data. Cambridge University Press.
- Deaton, A. (2003). Health, inequality, and economic development. Journal of Economic Literature, 41(1), 113–158. https://doi.org/10.1257/jel.41.1.113
- Dhrifi, A. (2018). Health-care expenditures, economic growth and infant mortality: Evidence from developed and developing countries. CEPAL Review, 125, 69–91. https://doi.org/10.18356/02c1a26c-en
- Evans, D. B., Saksena, P., Elovainio, R., & Boerma, T. (2012). Measuring progress towards universal coverage. World Health Organization.
- Filmer, D., & Pritchett, L. (1999). Child mortality and public spending on health: How much does money matter? Social Science & Medicine, 49(10), 1309–1323. https://doi.org/10.1016/S0277-9536(99)00150-1
- Frome, E. D., Kutner, M. H. V. B., & J. J. (1973). Regression Analysis of Poisson- Distributed Data. Journal of American Statistical Association, 68(344), 935–940.
- Frome EL. 1983. The Analysis of Rates Using Poisson RegressionModels, Biometrics, 39, 665–674.
- Hatun, Ş., Etiler, N., & Gönüllü, E. (2003). Yoksulluk ve çocuklar üzerine etkileri. Çocuk Sağlığı ve Hastalıkları Dergisi, 46, 251–260. https://www.cshd.org.tr/uploads/pdf_CSH_61.pdf.
- Helmert, U., & Shea, S. (2014). Social inequalities and health status in Western Germany. Public Health, 108(5), 341–356. https://doi.org/10.1016/S0033-3506(05)80070-8
- Houweling, T. A. J., Kunst, A. E., Caspar, W. N. L., & Mackenbach, J. P. (2005). Determinants of under-5 mortality among the poor and the rich: A cross-national analysis of 43 developing countries. International Journal of Epidemiology, 34(6), 1257–1265. https://doi.org/10.1093/ije/dyi190
- İşçi Güneri, Ö., & Durmuş, B. (2020). Aşırı ya da eksik yayılım durumunda poisson ve negatif binom regresyon modellerinin karşılaştırılması. Uluslararası Doğu Anadolu Fen Mühendislik ve Tasarım Dergisi, 2(1), 48–66 https://dergipark.org.tr/tr/pub/ijeased/issue/50819/703566.
- Jean Philippe, B., Michel, D., & Montserrat, G. (2007). Risk classification for claim counts: Mixed poisson, zero-inflated mixed poisson and hurdle models. North American Actuarial Journal, 11(4), 110–131. https://doi.org/10.1080/10920277.2007.10597487
- Johansson, S. R., & Carl, M. (1987). Exposure, resistance and life expectancy: Disease and death during the economic development of Japan, 1900-1960. Population Studies, 41(2), 207–235. https://doi.org/10.1080/0032472031000142776
- Kahveci, Ö. (2004). Mayıs Ekonomik ve sosyal boyutuyla yoksulluk ve aile. 4. Aile Şurası Aile ve Yoksulluk Bildirileri.
- Kaplan, G. A., Pamuk, E. R., Lynch, J. W., Cohen, R. D., & Balfour, J. L. (2016). Inequality in income and mortality in the United States: Analysis of mortality and potential pathways. British Medical Journal, 312(7037), 999–1003. https://doi.org/10.1136/bmj.312.7037.999
- Kawachi, I., & Kennedy, B. P. (1999). Income inequality and health: Pathways and mechanisms. Health Service Resources, 34(1 Pt 2), 215–227. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1088996/
- Koivusalo, M. (2009). The shaping of global health policy. In L. Panitch & ve C. Leys (Eds.), Morbid symptoms: Health under capitalism içinde (13-29) (1. ed.). Merlin Press.
- Konuk Şener, D., & Ocakçı, A. F. (2014). Yoksulluğun çocuk sağlığı üzerine çok boyutlu etkileri. Ankara Sağlık Hizmetleri Dergisi, 13(1), 57–68. https://dergipark.org.tr/tr/pub/ashd/issue/40341/482046
- Kouassi, E., Akinkugbe, O., Kutlo, N. O., & Ve Brou, J. M. (2018). Health expenditure and growth dynamics in the SADC region: Evidence from non-stationary panel data with cross section dependence and unobserved heterogeneity. International Journal of Health Economics and Management, 18(1), 47–66. https://doi.org/10.1007/s10754-017-9223-y
- Lindahl, M. (2002). Estimating the effect of income on health and mortality using lottery prizes as exogenous source of variation in income. The Journal of Human Resources, 40(1), 144–168. https://doi.org/10.3368/jhr.XL.1.144
- Markova, N.K. (2006). How does the introduction of health insurance change the equity in the health care provision in Bulgaria? International Monetary Fund Working Paper, 06/285. 1–41. https://doi.org/10.5089/9781451865455.001
- Miaou, S. P. (1994). The relationship between truck accidents and geometric design of road sections: Poisson versus negative binomial regressions. Accident Analysis and Prevention, 26(4), 471–482. https://doi.org/10.1016/0001-4575(94)90038-8
- Mohamoud, Y. A., Kirby, R. S., & Ehrenthal, D. B. (2019). Poverty, urban-rural classification and term infant mortality: A population-based multilevel analysis. BMC Pregnancy and Childbirth, 19(1), 1–11. https://doi.org/10.1186/s12884-019-2190-1
- Mushkin, S. J. (1962). Health as an investment. The Journal of Political Economy, 70(5), 129–157. https://doi.org/10.1086/258730
- Öngel, V., Altındağ, E., & Öngel, G. (2014). Temmuz Kişi başına sağlık harcamalarının sağlık göstergeleri üzerindeki etkileri: MINT ve BRIC ülkelerinin karşılaştırmalı analizi. Uluslararası Avrasya Ekonomileri Konferansı’nda sunulan bildiri, Beykent Üniversitesi, İstanbul.
- Park, M. B., & Nam, E. W. (2019). National level social determinants of health and outcomes: Longitudinal analysis of 27 industrialized countries. SAGE Open, 9(2), 1–8. https://doi.org/10.1177/2158244019854496
- Pašalić, S., Mastilo, Z., Đurić, A., & Marković, D. (2020). Demographic trends and the educational system of the republic of Srpska. Economics, 8(1), 93–113. https://doi.org/10.2478/eoik-2020-0007
- Peters, D. H., Garg, A., Bloom, G., Walker, D. G., Brieger, W. R., & Rahman, M. H. (2008). Poverty and access to health care in developing countries. Annals of the New York Academy of Sciences, 1136(1), 161–171. https://doi.org/10.1196/annals.1425.011
- Preston, S. H. (1975). The changing relation between mortality and level of economic development. Population Studies, 29(2), 231–248. https://doi.org/10.1080/00324728.1975.10410201
- Preston, S. H. (2007). The Changing Relation Between Mortality and Level of Economic Development. International Journal of Epidemiology, 36, 484–490.
- Rahman, M. M., & Alam, K. (2021). The role of socio-economic and female Indicators on child mortality rate in Bangladesh: A time series analysis. OMEGA. OMEGA - Journal of Death and Dying , 003022282199361. https://doi.org/10.1177/0030222821993616
- Robinson, J., & Wharrad, H. (2000). Invisible nursing: Exploring health outcomes at a global level. Relationships between infant and under-5 mortality rates and the distribution of health professionals, GNP per capita, and female literacy. Journal of Advanced Nursing, 32(1), 28–40. https://doi.org/10.1046/j.1365-2648.2000.01458.x
- Rodgers, G. B. (1979). Income and Inequality as Determinants of Mortality: An International Cross-Section Analysis. Population Studies, 33, 343–351.
- Rodriguez, A. F., & Neives, V. M. (2018). Health care expenditures and GDP in Latin American and OECD countries: A comparison using a panel cointegration approach. International Journal of Health Economics and Management, 19(), 1–39.
- Tüylüoğlu, Ş., & Tekin, M. (2009). Gelir düzeyi ve sağlık harcamalarının beklenen yaşam süresi ve bebek ölüm oranı üzerindeki etkileri. Çukurova Üniversitesi İİBF Dergisi, 13(1), 1–31. https://dergipark.org.tr/tr/pub/cuiibfd/issue/4151/54474
- UNICEF. (1990). Retrieved April 03, 2022 from https://www.unicef.org/turkey/%C3%A7ocuk-haklar%C4%B1na-dair-s%C3%B6zle%C5%9Fme
- UNICEF. (1991). Türkiye’de anne ve çocuklarının durum analizi (2 ed.). Yeniçağ Matbaası.
- United Nations. Transforming our world: The 2030 Agenda for sustainable development. Retrieved 25 March 2020 from https://sustainabledevelopment.un.org/post2015/transformingourworld
- Van Doorslaer, E., O’Donnell, O., Rannan-Eliya, R. P., Somanathan, A., Adhikari, S. R., Garg, C. C., Harbianto, D., Herrin, A. N., Huq, M. N., Ibragimova, S., Karan, A., Lee, T.-J., Leung, G. M., Lu, J. F. R., Ng, C. W., Pande, B. R., Racelis, R., Tao, S., Tin, K., … Zhao, Y. (2007). Catastrophic payments for health care in Asia. Health Economics, 16(11), 1159–1184. https://doi.org/10.1002/hec.1209
- Wagstaff, A. (2001). Poverty and Health Jeffrey D. Sachs Macroeconomics and Health: Investing in Health for Economic Development . (World Health Organization Working Paper Series, (Paper No. WG1:5). http://apps.who.int/iris/bitstream/handle/10665/42435/924154550X.pdf;jsessionid=167EA3119022F26B2E7F3AF0B8522955?sequence=1).
- Whitehead, M., Dahlgren, G., & Evans, T. (2001). Equity and health sector reforms: Can lowincome countries escape the medical poverty trap? The Lancet, 358(9284), 833–836. https://doi.org/10.1016/S0140-6736(01)05975-X
- Yılmaz, G. S., & Akdede, S. H. (2016). Kamu sağlık harcamalarının etkililiği: Panel veri analizi. Adnan Menderes Üniversitesi Sosyal Bilimler Enstitüsü Dergisi, 3(2), 85–110. https://doi.org/10.30803/adusobed.287990
- Yip Karen, C. H., & Yau Kelvin, K. W. (2005). On modeling claim frequency data in general insurance with extra zeros. Insurance. Insurance: Mathematics and Economics, 36(2), 153–163. https://doi.org/10.1016/j.insmatheco.2004.11.002