
Abstract
Background: People with Parkinson’s often move the trunk in a more in-phase pattern with reduced range of motion. No studies to date have assessed changes to trunk coordination after a dance intervention. The present study aimed to determine the effect of weekly ballet classes on trunk coordination and range of motion during gait for people with Parkinson’s.
Methods: The study follows a non-randomized, controlled project evaluation design. Two inertial sensors were used to record angular displacement of the pelvis and thorax during a 10 m walk for 19 experimental participants and 13 control participants. Coordination was assessed using cross-correlation of the angular displacement of the two body regions.
Results: No significant changes in trunk coordination and range of motion were found across time for both dancing and control groups (p > 0.01). There were also no significant differences between groups on all measures at different time intervals (p > 0.01).
Conclusions: The present study did not demonstrate significant effects of a weekly ballet class on trunk coordination and range of motion during gait for people with Parkinson’s. There is a need to determine optimal dance class frequency and appropriate levels of overload to allow for potential physiological improvements.
PUBLIC INTEREST STATEMENT
People with Parkinson’s are at risk of falling due to instability and dysfunctional gait patterns. Rigidity in the trunk may cause those with Parkinson’s to walk with reduced axial rotation. The present study looked at the effects of a weekly ballet class on trunk coordination and range of motion for this group of people. Ballet places a strong emphasis on whole-body coordination and incorporates many functional movements including rotation in trunk. While research suggests that these movements are useful tools in rehabilitation, the present study found no significant changes across time or between groups. It is possible that the participants were not carrying out these movements often enough and with an appropriate amount of overload to induce the physical changes. Future research should continue to assess potential changes in trunk coordination with increased ballet class frequency, and the impact these changes may have on activities of daily living.
Competing Interest
There are no financial disclosures or personal relationships with other people or organizations that could inappropriately influence (bias) this piece of work.
1. Introduction
Recent studies have evidenced the effect of instability and dysfunctional gait patterns on fall risk for people living with Parkinson’s (Hausdorff, Citation2009). Characteristic features of Parkinsonian gait include a smaller step and stride length, increased double support time, increased cadence, decreased walking velocity, and instability with greater step and stride variability. Individuals tend to walk with a flexed posture and demonstrate a reduced or absent arm swing with rigidity in trunk movements (Hackney, Kantorovich, & Earhart, Citation2007; Morris, Iansek, Matyas, & Summers, Citation1994; Pedersen, Oberg, Larsson, & Lindval, Citation1997; Van Emmerick, Wagenaar, Winogrodzka, & Wolters, Citation1999). This along with the fact that people with Parkinson’s often find they have decreased clearance of the swinging leg from the floor can put them at risk of falling during dynamic situations (Hackney et al., Citation2007; Hausdorff, Citation2009).
The array of difficulties that people may face with their gait can have a detrimental impact on functional mobility and thus participation in everyday activities. Although medications are available to help people cope better with their symptoms, research suggests that these treatments do not fully address gait and balance difficulties and as a result, non-pharmacological options are a necessity (Bloem, Grimbergen, Cramer, Willemsen, & Zwinderman, Citation2001; Hackney & Earhart, Citation2010; Heiberger et al., Citation2011).
Recent research has noted dance as being a beneficial activity for people with Parkinson’s (Earhart, Citation2009; Hackney & Earhart, Citation2010; Houston & McGill, Citation2013). Heiberger et al. (Citation2011) suggest that dance as a physical activity comprises elements that may help to improve rhythmic motor coordination and balance. However, there is insufficient evidence to support this argument as studies in the field have not gone so far as to measure exactly which elements of a dance class elicit change in these variables (McGill, Houston, & Lee, Citation2018)
In the first study that looked at ballet for people with Parkinson’s, Houston and McGill (Citation2013) qualitatively observed that weekly sessions helped to improve the fluency of movement. Actions that encouraged isolation of the upper from the lower body appeared to improve trunk rotation. However, this study did not have a control group and was only of short duration (12 weeks). Ballet places a strong emphasis on whole-body coordination and engagement of postural muscles to maintain proper alignment, possibly more so than other physical activities. Actions such as port de bras (movement of the arms and upper body through various ballet-specific positions) and use of épaulement (a rotation in the upper body bringing one shoulder more forward) encourage rotation of the torso in a coordinated and integrated fashion. This emphasis on axial rotation engages the core muscles, both anteriorly and posteriorly, and has the potential to improve range of motion. This is particularly important for people with Parkinson’s who suffer from rigidity in the torso as an inability to rotate properly can impact upon stability and coordination during gait (Huang, Meijer, & Lin et al., Citation2010; Stokes, Andersson, & Forssberg, Citation1989).
In healthy gait patterns, the pelvis moves into a forward rotation on the side of the swinging leg and an opposite rotation happens near the end of the stance phase. This pelvic motion can be counterbalanced, either by counter-rotating the thorax or by swinging an arm (Crosbie, Vachalathiti, & Smith, Citation1997; Stokes et al., Citation1989). Stokes et al. (Citation1989) suggested that this anti-phase pattern in the trunk helps to reduce the rotational momentum of the body and furthermore, may help to achieve a smoother gait pattern.
Murray, Sepic, Gardner, and Downs (Citation1978) observed that at self-selected speeds, people with Parkinson’s moved the pelvis and thorax in the transversal plane more in-phase as compared with control subjects. More recent research suggests this in-phase pattern may be due to rigidity in the trunk. For instance, Huang et al. (Citation2010) state that to account for a lack of rotation in the trunk, people with Parkinson’s may subsequently move slower, take smaller steps or adapt pelvic-thorax coordination patterns.
As rigidity resulting in reduced range of motion is a cardinal symptom of Parkinson’s and may be hindering trunk coordination, there is a need to look more closely at changes to these variables in the context of gait analysis. Reduced range of motion in the trunk may also be connected to poor posture, difficulties with turning, as well as decreased step and stride length.
Previous studies that focused on the benefits of dance for this population often included gait parameters in their methods (Duncan & Earhart, Citation2012; Hackney & Earhart, Citation2010; Marchant, Sylvester, & Earhart, Citation2010). Common gait measures include the 6-min walk test (6MWT), the Timed Up and Go test (TUG), and biomechanical measures that assess walking velocity. However, these measures only assess how quickly a participant can cover a certain distance over a period of time. The quality of walking and other gait parameters are equally important. More recent studies have attempted to address this issue by including such variables as step and stride length and time spent in stance and swing phase (Marchant et al., Citation2010). However, there is still a lack of research that looks at changes to trunk coordination as a result of participation in dance.
The present study aims to understand the potential benefits of weekly ballet sessions on trunk coordination and range of motion during gait for people with Parkinson’s. The authors hypothesize that the ballet sessions will elicit improvement in both trunk coordination and range of motion for this group of people.
2. Materials and methods
2.1. Project design & protocol
The present study focuses on one aspect of a wider longitudinal study that took place across a 3-year time period. The wider study aimed to understand the physical, mental, emotional, and social benefits of a weekly ballet class for people living with Parkinson’s (Houston & McGill, Citation2015). The present article describes the assessment and results from gait measures of trunk coordination and trunk range of motion.
The research team was asked to evaluate and assess potential benefits of an already existing class for people with Parkinson’s and as such this research follows a non-randomized, controlled, project evaluation design. With regards to the specific protocol, the ballet classes took place every Saturday afternoon at the hosting ballet company’s studios and lasted for 1.5 h each week. Further information about class content is discussed below. The classes had been occurring for approximately 2 years prior to the start of the research project with new people joining at various points before and during the project. The classes, which are still ongoing, take place in 10–12 week blocks across school term times. Quantitative data was collected at the beginning of autumn term in September 2012, and then subsequently after each dancing term until July 2014. There were a total of seven data collections across this time period. All participants had joined the ballet classes and research project by July 2013 and thus to include the maximum amount of participants, 12 months was the longest duration possible for quantitative data analysis.
Data for trunk coordination and range of motion was analysed across the short term (3–5 months) and across a longer term (10–12 months). The researchers wanted to understand whether any potential changes in the short term (after one term of dancing) would carry forward to the long-term analysis. Furthermore, it is possible that changes to trunk coordination and range of motion could occur in the longer term even if not seen in the short term. An analysis map was created to outline when participants had attended a testing session and what measurements they were able to carry out at that testing session. Based on this information short-term and long-term analysis time points were decided on for each individual across the duration of the project. While the exact time points may vary depending on the individual, all short-term analysis represented the equivalent of one term of dancing for a particular individual and all long-term analysis represented one year of dancing for a particular individual.
2.2. Participants
Participants in the dancing group were recruited from an on-going “dance for Parkinson’s” class. Control participants were recruited from local Parkinson’s support groups and also through relationships with members of the dancing group. It was not ethically appropriate to ask participants to stop other forms of physical activity across the duration of the study. As such participants were asked to carry on with their normal activities. Participants in the control group were simply asked to not partake in dance-related activity across the duration of the study (McGill et al., Citation2018).
A total of 19 people diagnosed with Parkinson’s who were dancing once a week volunteered to take part in the research. A total of 13 control participants who were not involved in any dance classes volunteered to form the control group. All participants completed a health and information sheet at each testing session that asked about any changes to medications, recent falls, and any other medical conditions (McGill et al., Citation2018).
At each testing point, participants reported on any other physical activities they were taking part in and how often these were carried out. Almost all participants, in both dancing and control groups, were involved in other physical activities on a weekly or monthly basis. Some examples of activities include golfing, swimming, Pilates, yoga, Tai Chi, Physiotherapy, attending the gym, racket ball, rowing, and exercise/aerobic-based classes. It could be argued that the only way to account for contextual factors such as physical activity outside of the intervention is to look at changes and experiences on a case-by-case basis. Case studies were completed for the wider longitudinal project. As both dancing and control groups were asked to carry on with their normal activities, the only difference between the two groups was the dancing itself.
Attendance for both the ballet classes and the testing sessions was recorded throughout the duration of the research project. Attendance over the course of a term ranged from 25 to 48 people at any ballet class. There was very little evidence of people dropping out of the programme completely and thus adherence was extremely high. While the majority of participants attended over 50% of the ballet classes provided across the time that they were analysed for the study, there were some exceptions to this finding. Reasons for absences included family commitments, illness, hospital appointments, and public transportation problems.
Ethical clearance was gained through the Ethics Committee at the authors' affiliating University, and all participants completed a consent form outlining details of the project prior to the baseline measurement. Inclusion criteria set at the beginning of the study meant that all participants had to be over 55 years of age, show no signs of dementia (as assessed via the Mini-Mental State Exam (MMSE)), be able to walk, or attempt to walk independently with no walking aid, have no back injury or have had recent surgery on the back, and not have gone through Deep Brain Stimulation surgery. If participants met the inclusion criteria above, they were able to participate despite their stage of Parkinson’s. It was not ethically appropriate to ask participants to alter their medication schedule to fit our testing sessions. As such, participants were tested at various levels of their daily condition. All dance participants had been dancing prior to a baseline measurement for at least one term (or 3 months). The majority of participants had been taking part in dance classes for one year or more prior to their baseline measurement (McGill et al., Citation2018). Participant characteristics are outlined in Table .
Table 1. Participant characteristics
2.3. The dance classes
The weekly classes were choreographed and taught by dance artists in the hosting ballet company’s outreach department. As the researchers were observing an on-going dance for Parkinson’s class, they were not able to influence the content of the class, frequency of the classes, or the intensity of the exercises. The researchers were working alongside an arts organisation that had already set out these parameters prior to the onset of the research study. Thus, our aim was to simply observe and measure the effects of a set weekly ballet class on trunk coordination and range of motion during gait for this group of people (McGill et al., Citation2018).
The programme uses the current company repertory as a basis for the content each term and the material is tailored to the participants. The first half of the class began seated and then progressed to standing and travelling work. Table outlines a more detailed description of the class (McGill et al., Citation2018).
Table 2. Ballet exercises and content
2.4. Data collection
Two inertial sensors were placed on the upper and lower spine (T1 and S2, respectively) and secured with double-sided tape. The inertial sensors wirelessly sent information to a receiving box attached to a computer. Angular displacement was gathered at a rate of 180 Hz (Esser, Dawes, Collett, Feltham, & Howells, Citation2011). Angular displacement data in the transverse plane was not only used to understand the coordination patterns between the pelvis and thorax but also provided insight into a range of motion in the upper and lower trunk.
Participants were asked to walk from one side of the room to the other (a distance of 10 m) at a self-selected, natural walking speed. Data was only recorded in one direction to avoid acceleration signals switching from positive to negative values and thus participants stopped after the 10 m walk, data was saved, and the researcher and participant walked back to the same starting point to complete the rest of the trials. Each participant carried out three trials in total at each testing point (McGill et al., Citation2018).
2.5. Data analysis
For each of the three separate trials per participant, per testing session, five stride cycles were analysed from the middle of the data set with the first and last cycles avoided where possible. Prior to determining the five cycles for analysis, the vertical acceleration data was resampled using a 5th order low pass Butterworth filter in Matlab. The cycles were determined by using the vertical acceleration signals to locate heel strikes (Evans, Duncan, & Gilchrist, Citation1991). Where a participant had only completed two trials, a missing data value of 999 was placed in the analysis spread sheet and the two trials were considered for full analysis (McGill et al., Citation2018)
Cross-correlation has been used to study the coordination between movements of different parts of the body (Crosbie, de Faria Negrão Filho, Nascimento, & Ferreira, Citation2013; Lee & Wong, Citation2002; Nelson-Wong, Howarth, Winter, & Callaghan, Citation2009; Shum, Crosbie, & Lee, Citation2007). This method studies the correlation between two different signals at different time lags. The correlation coefficient (otherwise known as the “r” value) measures how similar or opposing the two signals are at a given time lag. At zero lags a coefficient value closer to 1 shows that the two signals are more in-phase whereas a coefficient value closer to −1 shows that the two signals are moving in a more anti-phase pattern. The coefficient values and their respective time lags are therefore a useful tool for measuring coordination patterns between two parts of the body in motion.
The cross-correlation coefficient was determined using Matlab (Mathworks, Citation2015). The time lag between the pelvis and trunk motion was determined as the percentage of gait cycle. When the two signals have a strong positive correlation at a point closer to 0%, the coordination pattern can be classified as more in-phase.
The maximum and minimum angular displacements, and the range of motion for each stride were determined (maximum values represented the movement of the pelvis/thorax in one direction and the minimum values represented movement in the opposing direction).
2.6. Statistical analysis
Normality tests (the Kolmogorov-Smirnov (K-S) test and Shapiro-Wilk test) showed that the data sets did not have normal distributions and thus non-parametric statistics were applied. For all variables, the Friedman test was used to calculate changes across time in both dancing and control groups. Mann Whitney U tests were used to calculate differences between groups at each of the three-time points (baseline, short term, and long term). A Spearman Rank Correlation assessed the relationship between trunk coordination and range of motion in the pelvic and thorax. All statistical tests were carried out in SPSS with a significance level set at p < 0.01.
3. Results
3.1. Initial analysis of motion-time curves
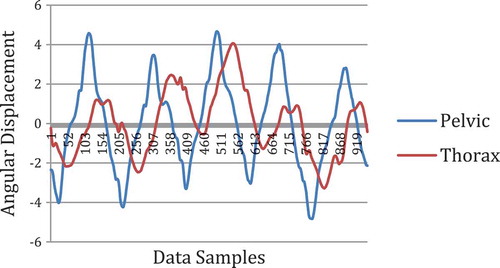
Figure demonstrates an example of a motion-time curve from the present study. In this example the two motion signals do not appear to completely oppose one another but rather are coordinating in a more in-phase pattern.
Figure 1. Example of a motion-time curve.
3.2. Pelvic range of motion (ROM)
Figure presents the changes in pelvic ROM across time for both dancing and control groups. The dancing and control groups did not evidence any significant change across the duration of the study with respect to pelvic ROM (p = 0.105 and p = 0.273, respectively). There were also no significant differences between groups with respect to ROM in the pelvis (baseline (p = 0.933), short term (p = 0.32), long term (p = 0.355)).
Figure 2. Changes to mean pelvic range of motion.
3.3. Thoracic range of motion (ROM)
Figure presents the change in thoracic ROM across time for both dancing and control groups. There were no significant changes across time with respect to thoracic ROM for either the dancing or control group (p = 0.92 and p = 0.15, respectively). There were also no significant differences between groups at various time points (baseline (p = 0.117), short term (p = 0.122), long term (p = 0.15)).
Figure 3. Changes to mean thoracic range of motion.
3.4. Coordination of movements in the upper and lower trunk
Figure presents changes in coordination coefficients across time for both dancing and control groups. The dancing and control groups did not show any significant change across the duration of the study with respect to similarity of movements in the upper and lower trunk (p = 0.368 for both groups). There were also no significant differences between groups across all testing points with regards to this similarity index (baseline (p = 0.368), short term (p = 0.822), long term (p = 0.837)). These results indicate that the degree of similarity between movements in the upper and lower trunk did not significantly change across the study.
Figure 4. Changes to mean coordination coefficient values.
Figure presents changes in time lag across time for both dancing and control groups. There were no significant changes in gait cycle lag across the duration of the study for the dancing group (p = 0.779) or the control group (p = 0.122). There were also no significant differences between groups across all testing points (baseline (p = 0.611), short term (p = 0.138), long term (p = 0.837)).
Figure 5. Change to gait cycle lag.
As the degree of similarity and gait cycle lag did not significantly change across the study, these results indicate that coordination patterns in the trunk did not significantly change as a result of the weekly ballet classes.
3.5. Correlations between trunk coordination and range of motion
There was a significant negative relationship between changes in gait cycle lag and thoracic range of motion in the short term (r = −0.489, p = 0.007). There were no other significant correlations in the short term. There were also no significant correlations between measures of trunk coordination and range of motion in the long term.
4. Discussion
This study assessed changes in trunk coordination and range of motion during gait for people with Parkinson’s after 12 months of weekly ballet sessions. Research has shown that healthy gait patterns show an opposing, anti-phase coordination pattern in the trunk while pathological gait has shown trends towards a more in-phase pattern (Murray et al., Citation1978; Van Emmerik & Wagenaar, Citation1996; Wagenaar & Van Emmerik, Citation1994).
The present study found no significant change across time and no significant differences between groups with respect to trunk coordination and range of motion during gait. Analysis of the time lag data demonstrated that the correlation values were strongest for both groups at less than 10% of the gait cycle. This suggests that subjects in both groups were walking with the trunk almost in phase, that is, the trunk and pelvis were moving together due to the rigidity of the trunk.
With regards to correlations between measures of trunk coordination and range of motion during gait, a significant negative correlation was found between the time lag and range of motion in the thorax during gait. However, this negative relationship was weak (r = −0.4) and not seen in the long-term results. This implies people with better trunk mobility will walk with more in-phase pattern, but such correlation may need to be further established in further research, and the physiological implication is unclear.
Recent research has shown that changes in coordination patterns can occur as a result of walking speed. Van Emmerick et al. (Citation1999) observed a change in thorax–pelvis coordination as a function of walking velocity in healthy subjects. As walking velocity increased, pelvis—thorax coordination shifted from more or less in-phase to more anti-phase. As people with Parkinson’s often demonstrate a decreased walking velocity, it could be that the participants’ self-selected walking speeds were too slow to assume the anti-phase coordination patterns. However, participants may be walking slowly to account for increased axial rigidity (Van Emmerick et al., Citation1999). Further investigation is needed to better understand the relationship between axial rigidity, a reduced walking speed, and trunk coordination during gait for people with Parkinson’s.
Previous dance from Parkinson’s research and experience in the field suggests that class participants, as well as observers often note a distinct change in the fluency and coordination of participants’ gait (Hackney & Earhart, Citation2009; Marchant et al., Citation2010). Given the nature of these observations, the lack of significant change in the present study may seem contradictory. However, the present study used different parameters (cross-correlation) to assess coordination and we looked at trunk coordination in particular, rather than arm and leg coordination. Additionally, when walking during a dance class the participants were often moving to a strong, steady pulse provided by the musical accompaniment. The music along with the verbal cues from instructors, which were not present during the testing sessions, might influence how participants walk in the dance class (Thaut et al., Citation1996).
Participants took part in once-weekly ballet classes across the duration of the study. Previous studies in the field have generally had a dance class frequency of at least 2–3 classes per week with some studies looking at more intensive dance training 3–5 times a week (Duncan & Earhart, Citation2012; Hackney & Earhart, Citation2009; Hackney et al., Citation2007; Marchant et al., Citation2010). The present study found no significant improvements for trunk coordination and range of motion during gait after 12 months of weekly ballet sessions. It is unknown what the results would be if the dance class frequency was increased and thus further investigation is needed (Lopopolo, Greco, & Sullivan et al., Citation2006; Power & Clifford, Citation2013). In addition, many participants in the present study had been participating in ballet classes for at least one year prior to engagement in this study. It is unclear whether this would have influenced the outcome of this study.
The ballet class incorporated the practice of many functional movements including rotation in the trunk and walking with verbal cues encouraging participants to stride out. While research suggests that these functional movements are useful tools in the rehabilitation for people with Parkinson’s (Goodwin, Richards, Taylor, Taylor, & Campbell, Citation2008; Keus, Bloem, Hendriks, Bredero-Cohen, & Munneke, Citation2007; Tomlinson, Patel, & Meek et al., Citation2012), it is possible that the participants were not carrying out these movements often enough and with an appropriate amount of overload to induce the physical changes.
4.1. Limitations
Due to the nature of the project and the fact that the dance classes were taking place alongside the research and not as a result of the study, the researchers were not able to influence the content or frequency of the sessions. As discussed above, it is possible that the participants were not carrying out functional movements often enough to induce physical changes in trunk coordination and range of motion. Furthermore, it was not possible to randomise participants as the dancing group were already involved in the dance sessions at the onset of the research study. As a result, those taking part in the dance classes chose to do this and clearly had an interest in taking part in dancing. However, both the control and dancing groups included people at various stages of Parkinson’s with a wide range of symptoms. Though randomisation was not possible, participant characteristics between groups were not statistically different and the dancing participants’ interest in taking part was the only apparent difference between the two groups.
Participants were not blinded to our research study and understood the aims and objectives. Furthermore, the researchers took part in the classes to gather rich data about participant experiences and thus were not blinded with regards to which participants were in each group. However, biomechanical measures of gait are not subjective and thus the main results described in the above study were likely not influenced by the non-blinded design. With regards to subjective measurements within the wider longitudinal study, participants were encouraged to speak/write honestly and openly about their experiences whether there appeared to be physical benefit from the dance classes or not.
While sample sizes were relatively small, the nature of the study must be taken into consideration. A single dance class generally holds no more than 30 individuals in any setting. Considering the dance artists were working with a group of people with Parkinson’s who need movements to be tailored to their individual abilities and often require assistance with these actions, the dance artists were teaching a reasonable amount of people and maintaining strong health and safety guidelines.
5. Conclusion
The results from the present study demonstrate no significant changes in trunk coordination and range of motion during gait after 12 months of weekly ballet classes for a group of people with Parkinson’s. While the ballet classes incorporated practice of functional movements that have shown to be useful in other rehabilitation programmes for this group of people, it is possible that the movements were not carried out often enough and with the appropriate amount of overload to elicit any potential positive change. It is possible that verbal cues from the instructors and the musical accompaniment may be helping participants to walk more fluently and with improved coordination during the ballet classes. However, further investigation is needed to understand how these changes can benefit people with Parkinson’s in the longer term and outside of the dance context.
Future research should continue to assess potential changes in trunk coordination with increased ballet class frequency, and the impact these changes may have on activities of daily living. Furthermore, there is a need to understand the mechanisms of change with regards to ballet for people with Parkinson’s and if/how specific movements are impacting upon functional mobility.
Cover image
Source: Author.

Acknowledgements
We would like to thank staff members at the English National Ballet for their help and support during the data collections and for allowing us to use their studio space. We would also like to thank the BA dance students at Roehampton University for volunteering to help with data collections and for providing a comfortable and enjoyable testing session for the participants.
Additional information
Funding
Notes on contributors
Ashley McGill
Ashley McGill is a Senior Lecturer in Dance with an interest in dance science, the benefits of dance for other populations, safe dance practice, ballet, and Pilates for dancers. Since completing her MSc in 2008, Ashley joined the dance department at University of Roehampton where she lectured and studied for her doctorate. In 2016 she successfully completed her PhD entitled, “Living with Parkinsonism: does dance help improve the quality of movement, functions and everyday activities?”
Sara Houston
Sara Houston is Principal Lecturer in Dance Studies at the University of Roehampton. She led the English National Ballet Dance for Parkinson’s studies. Her research focuses on the experience of dance for marginalised groups. Her book Dancing with Parkinson’s will be published in August through Intellect Books.
Raymond Y. W. Lee
Raymond Y. W. Lee is a Professor of Biomechanics with an interest in ageing research. He is keen on multidisciplinary research and working with creative and performance art researchers.
References
- Bloem, B. R., Grimbergen, Y. A. M., Cramer, M., Willemsen, M., & Zwinderman, A. H. (2001). Prospective assessment of falls in Parkinson’s disease. Journal of Neurology, 248(11), 950–958.
- Crosbie, J., de Faria Negrão Filho, R., Nascimento, D. P., & Ferreira, P. (2013). Coordination of spinal motion in the transverse and frontal planes during walking in people with and without recurrent low back pain. Spine, 38(5), E286–E292. doi:10.1097/BRS.0b013e318281de28
- Crosbie, J., Vachalathiti, R., & Smith, R. (1997). Patterns of spinal motion during walking. Gait and Posture, 5, 6–12. doi:10.1016/S0966-6362(96)01066-1
- Duncan, R. P., & Earhart, G. M. (2012). Randomized controlled trial of community-based dancing to modify disease progression in Parkinson disease. Neurorehabilitation and Neural Repair, 26(2), 132–143. doi:10.1177/1545968311421614
- Earhart, G. M. (2009). Dance as therapy for individuals with Parkinson disease. European Journal of Physical and Rehabilitation Medicine, 45(2), 231–238.
- Esser, P., Dawes, H., Collett, J., Feltham, M. G., & Howells, K. (2011). Assessment of spatio-temporal gait parameters using inertial measurement units in neurological populations. Gait and Posture, 34, 558–560. doi:10.1016/j.gaitpost.2011.06.018
- Evans, A. L., Duncan, G., & Gilchrist, W. (1991). Recording accelerations in body movements. Medical & Biological Engineering & Computing, 29(1), 102–104. doi:10.1007/BF02446305
- Goodwin, V. A., Richards, S. H., Taylor, R. S., Taylor, A. H., & Campbell, J. L. (2008). The effectiveness of exercise interventions for people with Parkinson’s disease: A systematic review and meta-analysis. Movement Disorders, 23(5), 631–640. doi:10.1002/mds.21922
- Hackney, M. E., & Earhart, G. M. (2009). Effects of dance on movement control in Parkinson’s disease: A comparison of Argentine tango and American ballroom. Journal of Rehabilitation Medicine : Official Journal of the UEMS European Board of Physical and Rehabilitation Medicine, 41(6), 475–481. doi:10.2340/16501977-0362
- Hackney, M. E., & Earhart, G. M. (2010). Effects of dance on gait and balance in Parkinson’s disease: A comparison of partnered and nonpartnered dance movement. Neurorehabilitation and Neural Repair, 24(4), 384–392. doi:10.1177/1545968309353329
- Hackney, M. E., Kantorovich, S., & Earhart, G. M. (2007). A study on the effects of Argentine Tango as a form of partnered dance for those with Parkinson disease and the healthy elderly. American Journal of Dance Therapy, 29(2), 109–127. doi:10.1007/s10465-007-9039-2
- Hausdorff, J. M. (2009). Gait dynamics in Parkinson’s disease: Common and distinct behaviour among stride length, gait variability, and fractal-like scaling. Chaos. doi:10.1063/1.3147408
- Heiberger, L., Maurer, C., Amtage, F., Mendez-Balbuena, I., Schulte-Mo ̈nting, J., & Hepp Reymond, M. (2011). Impact of a weekly dance class on the functional mobility and on the quality of life of individuals with Parkinson’s Disease. Frontiers in Aging Neuroscience, 3(14), 1–15. doi:10.3389/fnagi.2011.00014
- Houston, S., & McGill, A. (2013). A mixed-methods study into ballet for people living with Parkinson’s. Arts & Health: an International Journal for Research, Policy and Practice, 5(2), 103–119. doi:10.1080/17533015.2012.745580
- Houston, S., & McGill, A. (2015). English national ballet dance for Parkinson’s: An investigative study part 2. London: University of Roehampton/English National Ballet. Retrieved from http://roehamptondance.com/parkinsons/wp-content/uploads/2014/05/ENB_Research-Report_FINAL_2.pdf
- Huang, Y., Meijer, O. G., Lin, J. (2010). The effects of stride length and stride frequency on trunk coordination in human walking. Gait and Posture, 31, 444–449. doi:10.1016/j.gaitpost.2010.01.019
- Keus, S. H., Bloem, B. R., Hendriks, E. J., Bredero-Cohen, A. B., & Munneke, M. (2007). Evidence-based analysis of physical therapy in Parkinson’s disease with recommendations for practice and research. Movement Disorders, 22(4), 451–460. doi:10.1002/mds.21244
- Lee, R. Y. W., & Wong, T. K. T. (2002). Relationship between the movements of the lumbar spine and hip. Human Movement Science, 21, 481–494. doi:10.1016/S0167-9457(02)00117-3
- Lopopolo, R. B., Greco, M., Sullivan, D. H. (2006). Effect of therapeutic exercise on gait speed in community dwelling elderly people: A meta-analysis. Physical Therapy, 86, 520–540.
- Marchant, D., Sylvester, J. L., & Earhart, G. M. (2010). Effects of a short duration, high dose contact improvisation dance workshop on Parkinson disease: A pilot study. Complementary Therapies in Medicine, 18(5), 184–190. doi:10.1016/j.ctim.2010.07.004
- Mathworks. (2015). Support: Cross correlation. Author. Retrieved from http://uk.mathworks.com/help/signal/ref/xcorr.html
- McGill, A., Houston, S., & Lee, R. (2018). Effects of a ballet-based dance intervention on gait variability and balance confidence of people with Parkinson’s. Arts and Health: an International Journal for Research, Policy, and Practice. doi:10.1080/17533015.2018.1443947
- Morris, M. E., Iansek, R., Matyas, T. A., & Summers, J. J. (1994). The pathogenesis of gait hypokinesia in Parkinson’s disease. Brain, 117(5), 1169–1181.
- Murray, M. P., Sepic, S. B., Gardner, G. M., & Downs, W. J. (1978). Walking patterns of men with parkinsonism. American Journal of Physical Medicine, 57, 278–294.
- Nelson-Wong, E., Howarth, S., Winter, D. A., & Callaghan, J. P. (2009). Application of autocorrelation and cross-Correlation analyses in human movement and rehabilitation research. The Journal of Orthopaedic and Sports Physical Therapy, 39(4), 287–295. doi:10.2519/jospt.2009.2969
- Pedersen, S. W., Oberg, B., Larsson, L. E., & Lindval, B. (1997). Gait analysis, isokinetic muscle strength measurement in patients with Parkinson’s disease. Scandinavian Journal of Rehabilitation Medicine, 29(1), 67–74.
- Power, V., & Clifford, A. M. (2013). Characteristics of optimum falls prevention exercise programmes for community-dwelling older adults using the FITT principle. European Review of Aging and Physical Activity: Official Journal of the European Group for Research into Elderly and Physical Activity, 10, 95–106. doi:10.1007/s11556-012-0108-2
- Shum, G. L. K., Crosbie, J., & Lee, R. Y. W. (2007). Movement coordination of the lumbar spine and hip during a picking up activity in low back pain subjects. European Spine Journal : Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 16(6), 749–758. doi:10.1007/s00586-006-0122-z
- Stokes, V. P., Andersson, C., & Forssberg, H. (1989). Rotational and translational movement features of the pelvis and thorax during adult human locomotion. Journal of Biomechanics, 22, 43–50.
- Thaut, M. H., McIntosh, G. C., Rice, R. R., Miller, R. A., Rathbun, J., & Brault, J. M. (1996). Rhythmic auditory stimulation in gait training for Parkinson’s disease patients. Movement Disorders, 11(2), 193–200. doi:10.1002/mds.870110213
- Tomlinson, C. L., Patel, S., Meek, C. (2012). Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane Database Systematic Review, 7, CD002817. doi:10.1002/14651858.CD002817.pub2
- Van Emmerick, R., Wagenaar, R. C., Winogrodzka, A., & Wolters, E. C. (1999). Identification of axial rigidity during locomotion in Parkinson disease. Archives of Physical Medicine and Rehabilitation, 80(2), 186–191.
- Van Emmerik, R. E. A., & Wagenaar, R. C. (1996). Effects of walking velocity on relative phase dynamics in the trunk in human walking. Journal of Biomechanics, 29, 1175–1184. doi:10.1016/0021-9290(95)00128-X
- Wagenaar, R. C., & Van Emmerik, R. E. A. (1994). Dynamics of pathological gait. Human Movement Science, 13, 441–471. doi:10.1016/0167-9457(94)90049-3