
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Breast cancer is a foremost cause of death worldwide, ranks fifth among causes of death from all types of cancers; this is the most common cause of cancer death in women among both developing and developed countries. Breast cancer ranks first among the most frequent cancers in women of Ethiopia. In spite of the high incidence, mortality rate, and survival status among breast cancer patients was not determined in Ethiopia. The purpose of this study was to identify factors affecting the time to death among breast cancer patients attending anti-cancer treatment from September 2015 till December 2018 at Ayder Comprehensive Specialized Hospital. Methods: Hospital-based retrospective cohort study was conducted among breast cancer patients. Kaplan-Meier survival curve together with log-rank test was deployed to test for variations in the survival among predictor variables. Cox regression was used at a 5% level of significance to determine the net effect of each independent variable on the time to death of breast cancer clients. Results: From the Cox proportional model, patients with age, educational status, residence, Baseline Tumor size &Pathology type (LIC) were found to be a statistically significant effect (p < 0.05) on the risk of mortality due to breast cancer and the median survival time of breast cancer patient was 34.50 months. Conclusion: the finding of this study showed that age, educational status, residence, Baseline Tumor size &Pathology type (LIC) were influential affecting time to death of breast cancer patient at the Hospital. It is recommended to make interventions based on these risk factors.
PUBLIC INTEREST STATEMENT
This study was about Breast cancer in Ayder referral hospital _ Ethiopia. Breast cancer destroys the lives of many young individuals in developing countries. As it is known that the main predictive factors for Breast cancer patients are more health variables for this disease, data about its pathophysiological variables are important for interpretation in disease. The study presents data of the normal cohort of the Ayder, Registry. In many cases, due to a lack of awareness for women from health workers practices, these diseases claim lots of lives of the community who should not have otherwise died. With regular research and dissemination, among other interventions, it is very possible to contain these diseases. More researches are still encouraged in this area and also in other breast cancer.
1. Background
Cancer is a group of diseases that causes by the uncontrolled growth and spread of abnormal cells anywhere in the body (Diabate et al., Citation2018. Breast cancer is a type of malignant tumor, which it starts in the cells of the breast tissue that is made up of glands for milk production, called lobules, and the ducts that connect the lobules to the nipple. The majority of breast cancer cases are classified as either invasive or noninvasive. The invasive type of breast cancer is distributed in the whole body; but not the noninvasive (Abay et al., Citation2018). Cancer constitutes enormous burdens in more and less economically developed countries. Based on Global Cancer statistics about 14.1 million new cancer cases and 8.2 million deaths occurred worldwide in 2012(Torre et al., Citation2015).
Breast cancer is the most commonly diagnosed cancer and the second leading cause of cancer death among African women. In Africa from 92,600 cases, 50,000 deaths in 2008 (Jemal et al., Citation2012). In sub-Saharan Africa, breast cancer is one of the non-communicable diseases and the most commonly diagnosed cancer in women (Brinton et al., Citation2014). The average age of diagnosis of breast cancers among African women tends to be young, with estimates that a majority of cancers develop among women 50 years or younger; a considerably younger age than seen in Caucasian populations (Sighoko et al., Citation2013). Breast cancer is the second most often occurring cancer next to cervical cancer among women in Ethiopia. It is estimated that around 10,000 Ethiopian women have breast cancer with thousands of more cases unreported as women living in rural areas often seek treatment from traditional healers before seeking help from the government health system (Lemlem et al., Citation2013).
Research from Vietnam studied that educational status affects the risk of mortality such that with a higher level of education there is approximately 10% risk reduction death. And Marital status has also a prognostic factor for mortality of women with breast cancer, (Lan et al., Citation2013). Age has a significant effect on women breast cancer patients. It indicated that the mortality of breast cancer is high as age increases. (Rezaianzadeh et al., Citation2009). A study conducted in the United States on the effects of some risk and prognostic factors contributing to the survival of breast cancer patients shows that tumor size, lymph node metastasis status, and tumor extension had a significant effect on breast cancer survival (Desantis et al., Citation2013). Alcohol consumption increases the risk of mortality due to breast cancer. The risk of breast cancer in women about 7% to 12% for each 10 g (roughly one drink) of alcohol consumed per day (Desantis et al., Citation2013). A study conducted by Addis Ababa University on the effects of some risk factors contributing to the survival of breast cancer patients shows that stage and pathology type had a significant effect on breast cancer survival (Kantelhardt et al., Citation2014). Tomi F A. et al.,(Citation2015) suggest modest positive associations between urbanization and residential area socioeconomic environment and breast cancer incidence.
Breast cancer is a foremost cause of death worldwide, ranks fifth among causes of death from all types of cancers; this is the most common cause of cancer death in women among both developing and developed countries. Breast cancer ranks first among most frequent cancers in women of Ethiopia. In spite of the high incidence, mortality rate, and survival status among breast cancer patients was not determined in Ethiopia(Areri et al., Citation2018). In Ethiopia according to World Health Organization estimation, an age standardize incidence case of breast cancer was 12,956 and mortality rate was 25 per 100,000 women (World Health Organization, Citation2017). As a result, to avert this burden currently the Ethiopian Federal Ministry of Health (EFMOH) prepared a task force to address the issue of non-communicable diseases with special emphasis on cancer. Overall, the fundamentals parts of the strategic framework is to reduce the incidence, mortality and improve the quality of life of cancer patients (Nuño et al., Citation2012). Regardless of the adequate data on the incidence and survival rates of breast cancer in the western countries, survival data were scanty in Africa, and Asia countries (Kene et al., Citation2010; Mensah et al., Citation2016; Parkin et al., Citation2014).
Even though the number of people living with breast cancer is increasing from year to year; it has emerged as one of the rapidly increasing non-communicable disease and a major public health challenge in developing countries like Ethiopia (Kantelhardt et al., Citation2014) with a consequence of Chronicity, disability and death. Although the prevalence of breast cancer is substantially increasing in Ethiopia as well as in the study area, as far as my knowledge there is no explanatory studies that documented on the area of the risk of time to death due to breast cancer among breast cancer patients after taking anti-cancer treatment by using survival analysis.
The aim of this study is to investigate the risk of time to death due to breast cancer among breast cancer patients from September 2015 till December 2018 at Ayder comprehensive specialized hospital. Specifically, 1) To estimate the survival time of breast cancer patients, 2) To compare survival time among the different groups of breast cancer patients, 3) To determine the factors and/or covariates that affect the survival of breast cancer patients. Findings of this study could help to provide evidence-based information to health care authorities, other stakeholders to design interventions that can decrease the incidence and mortality of breast cancer clients
2. Methodology
The study was conducted at Ayder comprehensive specialized hospital from September 2015 till December 2018. The hospital is found in Mekelle town, Tigray region, Northern part of Ethiopia. It is located around 782 km from Addis Ababa, the capital city of Ethiopia.
Tigray region has 18 public hospitals and 170 health centers
with a total population of 4,316,988.
2.1. Data Source
Source of data for this study was the patient’s chart from the data record office at comprehensive specialized hospital. The patients ‘chart was used to extract the necessary information from different BC recording formats.
3. Inclusion and Exclusion Criteria
3.1. Inclusion Criteria
The study includes all BC patients and started Anti-cancer treatment since September 2015 and have at least two follow up until December 2018 in Ayder comprehensive specialized hospital.
3.2. Exclusion Criteria
This study excludes those patients who had incomplete variable registration cards, a person died by other accidents and those patients who started anti-cancer treatment from other healthcare institutions.
3.3. Study design
A facility-based retrospective cohort study design was conduct in Ayder Comprehensive Specialized Hospital. The study was focused on investigate the determinant factors that affects time to death among breast cancer patients with joint modeling of longitudinal change in tumor cell level at Ayder Comprehensive Specialized Hospital.
3.4. Study population
The study population consists of all breast cancer patients who were under follow up and started the anti-cancer treatment and have at least two follow up until December 2018. From the total registered breast cancer patients at the hospital, only 186 of them were included in the study.
3.5. Method of Data Collection
The data was collected from patient charts based on those variables to be considered in this study. Both the longitudinal and survival data were extracted from the patient’s chart which contains demographic and clinical variables of BC patients under treatment follow up.
3.6. Operational definition
Censoring: When we say Observations are called censored if the information about their survival time is incomplete. An individual loss follow-up during the study period (drop out from the study)(Collett, Citation2015).
Survival time: the period that a patient Stays in life after starting the anti-cancer treatment.
Time: the period which patients visiting to the hospital during the follow up every three months.
Minimum follow up time: the period that a patient who had two longitudinal measurements after started the anti-cancer treatment.
4. Study variables
4.1. Outcome variables
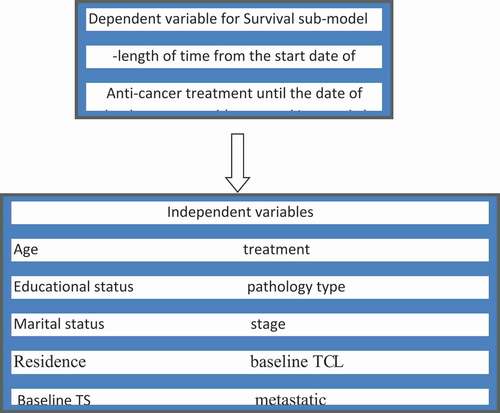
The main outcome variable for survival data analysis is time to death due to breast canceror censored (in month).
4.2. Independent variables
Several clinical and demographic variables were considering in this study for survival cases. They are mentioned here below.
Figure 1. Schematic/diagrammatic/representation of joint model for breast cancer patients
4.3. Statistical Models
The analysis done by the Cox proportional-hazards model for the time-to-death data. The data were analyzed by using STATA12 to present the categorical descriptive statistics and R version 3.6.1 to analysis the Cox.
4.4. Descriptive Statistics
By considering the descriptive statistics for variables, total of 186 breast cancer patients were included in this study. Out of these, 22(11.83%) were dead and 119(64%) patients their residence in rural. When we consider based on death for educational status of the patients, 17(18.09%) of patients are illiterate, 3(6.38%) of them are primary educated,1(14.29%) of them are secondary educated and 1(2.63%) are tertiary educated. Among 186 breast cancer patients, 47(97.92%), 42(97.67%), 53(82.81%), and 22(70.97%) were censored forthemin stages stage-1, stage-2, stage-3 and stage-4, respectively.
121(65.1%) of the patient uses surgery treatment and 33(17.7%) chemotherapy where as the remaining used both surgery and chemotherapy treatment. Considering the pathology type of BC patients, 94(50.5%) of breast cancer patients are ductal carcinoma in-situ71(38.2%) lobular carcinoma in-situ & 8(4.3%) were ductal invasive carcinoma. But the rest of them were lobular invasive carcinoma. The median age, B tumor cell, B tumor size & B_HGL of BC patients were given as 47,246,12 &12.8, respectively. and also, the median survival time of BC patient was 34.50 months.
4.5. Analysis of Survival Data
Kaplan-Meier Estimates and Log-rank Tests.
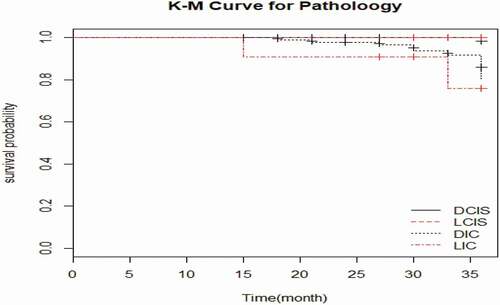
The breast cancer patients whose pathology type was LCIS have longest survival probability than the patients who were Ductal carcinoma in-situ, Ductal invasive carcinoma and Lobular invasive carcinoma. The patients whose stage was stage-4 has smallest survival probability than the patients, whose stage was stage-1, stage-2 and stage-3.
Figure 2. Kaplan-Meier of pathology type
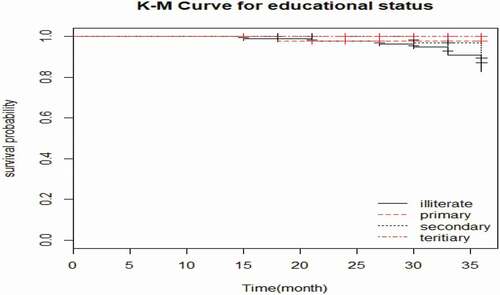
when we compare by using education status, the patient whoe education status was illiterate category had shorter survival probability than primary, secondary and tertiary categories.
Figure 3. Kaplan-Meier of educational status
The BC patients who used the treatment both surgery & chemotherapy has smallest survival probability than the patients, who used the treatment surgery and chemotherapy. The survival probability of the breast cancer patients who came from urban is longer than the patients who came from rural areas.
Based on Table-4 result of long rank test, Educational Status, Treatment, Pathology type and Residence were statistically significance difference in the risk of mortality among breast cancer patients at 25% level of significance. however, there is no significant difference in the risk of mortality between categories of Marital Status, Stage and Metastatic at 25% level of significance. Because this Table was important for selection of candidate variables to pass for multivariate analysis.
Based on the above Table-5 variable Age, B tumor size & B tumor cell are statistically significance difference on Univariate analysis of Cox regression model at 25% level of significance. this helps for selection of variables in the final cox regression model.
5. Variable Selection and Cox PH Assumption
To determine the variables to be included in the multivariable Cox survival model we used variables whose p-value <0.25 for & Table-5 on the above. Educational status, Age,B tumor size,B tumor cell, pathology type, treatment and residence were the candidate variables in the multivariate cox regression model. However, marital status, stage, metastatic & B-HGL were not included in the multi-variate cox regression model.
Table 1. Log rank test for categorical independent variables
Table 2. Univariate analysis of Cox regression model for continuous variables
Table 3. Proportional hazard model assumption
Table 4. Shows the Cox proportional hazards model for the selected variables
The proportional hazards assumption asserts that the hazard ratios are constant overtime. That means the risk of failure must be the same no matter how long subjects have been followed. In order to test this assumption GLOBAL test was used. The result of the GLOBALtest is displayed on Table 6.From the above output (Table 6, it is clear to see that the p- value of GLOBAL is insignificant. This indicates that the PH assumption is not violated. Therefore, we can assume the proportionality assumption is met.
Cox proportional hazards model
After checking the assumption of proportional hazard, the survival data was analyzed based on
Cox proportional hazard model. The results are presented below.
From the following results of the multivariable analysis presented in Table-7 show that the estimated AHR, 95% CI and p-value of the covariates in the final cox regression model for age, educational status, residence, Baseline Tumor size &Pathology type (LIC) were found to be statistically significant effect at 5% level of significance on the risk of mortality due to breast cancer. The remaining variables which were found to be non-significant at 5% of significance level in the multivariable analysis of the final cox regression model.
6. Discussion
From the study using Cox proportional hazard model, age, educational status, residence, Baseline Tumor size &Pathology type (LIC) were found to have a statistically significant effect at a 5% level of significance on the risk of mortality due to breast cancer. But, the remaining variables like B tumor cell, Chemotherapy and Surgery $ chemotherapy was found to be non-significant at 5% of significance level in the multivariable analysis of the final cox regression model.
The educational status of patients is another prognostic factor that significantly predicts the death of patients. The result obtained from this study indicates that the time to death for tertiary education patient is longer than the secondary and primary one. Improving educational status increases the chance of recovery. This result confirms the result obtained from the previous studies ((Lan et al., Citation2013). Residence of the patient is a strong predictor of the time death of a breast cancer patient. This means a patient who lives in urban has more chance to survive than a patient who lives in rural. This result is in accordance with the studies a systematic review and meta-analysis by (Tomi F A. Et al.,Citation2015).
One of the factors that affects recovery from breast cancer is the patient’s age with the hazard of (HR = 1.06)). This result is in accordance with the study in breast cancer in Southern Iran: (Rezaianzadeh et al., Citation2009). Baseline Tumor size &Pathology type (LIC) of a patient is also a prognostic factor that significantly predicts the survival time to death of breast cancer patients. these results are comparable with an earlier study in the united States by (Desantis et al., Citation2013). the median survival time of breast cancer the patient was 34.50 months.
7. Conclusion
The finding of this study showed that age, educational status, residence, Baseline Tumor size &Pathology type (LIC) were influential affecting time to death of breast cancer patient at the Hospital.
8. Recommendation
Health professionals, Governments and non-governmental organization should increase awareness about cancer screening at early stage and also should make influence for women to diagnose at early stage to improve the risk of mortality. In addition to this, the Health Sector of Tigray Region should plane to make facilitating and cancer screening program at rural area of that Region to illuminate the risk of mortality.
9. Limitation of the study
The study was conducted based on secondary data which might have incomplete. Finally, as different literature pointed out, there are different factors that are assumed to have impacts on the survival of obstetric fistula patients such as poorly differentiated histology grade, surgical margin involvement and positive lymph node status . However, data on these variables could not be available in hospital records, so these variables were not integrated in this study.
Abbreviations
AIC: Akaike Information Criterion;BC:Breast Cancer; BIC:Bayesian Information Criterion; CI: Confidence interval; HMIS: health management information system;AHR:Adjusted hazard Ratio; LMM:Linear Mixed Model; PH:Proportional Hazard; TCL:Tumor cell level; TS:Tumor size;WHO: World Health Organization
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of University of Gondar institution and the University research committee declarations with comparable ethical standards for confidentiality.
Competing interests
The authors declare they have no competing interests.
Acknowledgements
We wish to extend our thanks for all individuals involved in the study from the University of Gondar,Ethiopia.
Availability of data and materials
The datasets analyzed during the current study were available from the corresponding
author on reasonable request.
Additional information
Funding
Notes on contributors

Endeshaw Assefa Derso
The main research topic of our group is Breast cancer, a major public health problem in developing countries. We investigate risk factors and pathophysiological mechanisms, which cause or are associated with Breast cancer. Additionally, we work on improving the present Breast cancer diagnostics. The basis for all this research work is survival analysis of Breast cancer. Thus, we perform studies with the aim of investigating covariates by using survival analysis.
References
- Abay, M., Tuke, G., Zewdie, E., Abraha, T. H., Grum, T., & Brhane, E. (2018). Breast self-examination practice and associated factors among women aged 20–70 years attending public health institutions of Adwa town, North Ethiopia. BMC Research Notes, 11(1), 622. https://doi.org/https://doi.org/10.1186/s13104-018-3731-9
- Akinyemiju, T. F., Genkinger, J. M., Farhat, M., Wilson, A., Gary-Webb, T. L., & Tehranifar, P. (2015). Residential environment and breast cancer incidence and mortality: A systematic review and meta-analysis. BMC Cancer, 15(1). https://doi.org/https://doi.org/10.1186/s12885-015-1098-z
- Areri, H. A. B. T. A. M. U. A. B. E. R. A., Shibabaw, W. O. N. D. I. M. E. N. E. H., Mulugeta, T. E. F. E. R. A., Asmare, Y. A. R. E. D., & Yirga, T. A. D. E. S. S. E. (2018). Survival status and predictors of mortality among breast cancer patients in adult oncology unit at black lion specialized hospital. The preprint erver for biology. https://doi.org/https://doi.org/10.1101/636431
- Brinton, L. A., Figueroa, J. D., Awuah, B., Yarney, J., Wiafe, S., Wood, S. N., Ansong, D., Nyarko, K., Wiafe-addai, B., & Clegg-lamptey, J. N. (2014). Breast cancer in Sub-Saharan Africa: Opportunities for prevention. Breast Cancer Research and Treatment, 144(3), 467–478. https://doi.org/https://doi.org/10.1007/s10549-014-2868-z
- Collett, D. (2015). Modelling survival data in medical research. Chapman and Hall/CRC.
- Desantis, C., Siegel, R., & Jemal, A. (2013). Breast cancer facts and figures 2013-2014. American Cancer Society, 2013, 1–11. American Cancer Society, Atlanta, Georgia
- Diabate, M., Coquille, L., & Samson, A. (2018). Parameter estimation and treatment optimization in a stochastic model for immunotherapy of cancer. arXiv Preprint Ar Xiv, 1806.01915.
- Jemal, A., Bray, F., Forman, D., O’brien, M., Ferlay, J., Center, M., & Parkin, D. M. (2012). Cancer burden in Africa and opportunities for prevention. Cancer, 118(18), 4372–4384. https://doi.org/https://doi.org/10.1002/cncr.27410
- Kantelhardt, E., Zerche, P., Mathewos, A., Trocchi, P., Addissie, A., Aynalem, A., Wondemagegnehu, T., Ersumo, T., Reeler, A., Yonas, B., Tinsae, M., Gemechu, T., Jemal, A., Thomssen, C., Stang, A., & Bogale, S. (2014). Breast cancer survival in Ethiopia: A cohort study of 1,070 women. International Journal of Cancer, 135(3), 702–709. https://doi.org/https://doi.org/10.1002/ijc.28691
- Kaplan, E. L., & Meier, P. (1958). Nonparametric estimation from incomplete observations. Journal of the American Statistical Association, 53(282), 457–481. https://doi.org/https://doi.org/10.1080/01621459.1958.10501452
- Kene, T. S., Odigie, V. I., Yusufu, L. M., Yusuf, B. O., Shehu, S. M., & Kase, J. T. (2010). Pattern of presentation and survival of breast cancer in a teaching hospital in north Western Nigeria. Oman Medical Journal, 25(2), 104. https://doi.org/https://doi.org/10.5001/omj.2010.29
- Lan, N., Laohasiriwong, W., & Stewart, J. (2013). Survival probability and prognostic factors for breast cancer patients in Vietnam. Global Health Action, 6(1), 18860. https://doi.org/https://doi.org/10.3402/gha.v6i0.18860
- Lemlem, S. B., Sinishaw, W., Hailu, M., Abebe, M., & Aregay, A. (2013). Assessment of knowledge of breast cancer and screening methods among nurses in university hospitals in Addis Ababa, Ethiopia, 2011. ISRN Oncology, 2013, 1–8. https://doi.org/https://doi.org/10.1155/2013/470981
- Mensah, A. C., Yarney, J., Nokoe, S. K., Opoku, S., & Clegg-Lamptey, J. (2016). Survival outcomes of breast cancer in Ghana: An analysis of clinicopathological features. Open Access Library J, 3, 1–11. https://doi.org/https://doi.org/10.4236/oalib.1102145
- Nuño, R., Coleman, K., Bengoa, R., & Sauto, R. (2012). Integrated care for chronic conditions: The contribution of the ICCC framework. Health Policy, 105(1), 55–64. https://doi.org/https://doi.org/10.1016/j.healthpol.2011.10.006
- Parkin, D. M., Bray, F., Ferlay, J., & Jemal, A. (2014). Cancer in africa 2012. Cancer Epidemiology and Prevention Biomarkers, 23(6), 953–966. https://doi.org/https://doi.org/10.1158/1055-9965.EPI-14-0281
- Rezaianzadeh, A., Peacock, J., Reidpath, D., Talei, A., Hosseini, S. V., & Mehrabani, D. (2009). Survival analysis of 1148 women diagnosed with breast cancer in Southern Iran. BMC Cancer, 9(1). https://doi.org/https://doi.org/10.1186/1471-2407-9-168
- Sighoko, D., Kamaté, B., Traore, C., Mallé, B., Coulibaly, B., Karidiatou, A., Diallo, C., Bah, E., Mccormack, V., Muwonge, R., Bourgeois, D., Gormally, E., Curado, M. P., Bayo, S., & Hainaut, P. (2013). Breast cancer in pre-menopausal women in West Africa: Analysis of temporal trends and evaluation of risk factors associated with reproductive life. The Breast, 22(5), 828–835. https://doi.org/https://doi.org/10.1016/j.breast.2013.02.011
- Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet‐tieulent, J., & Jemal, A. (2015). Global cancer statistics, 2012. CA: A Cancer Journal for Clinicians, 65(2), 87–108. https://doi.org/https://doi.org/10.3322/caac.21262
- World Health Organization. Cancer country profiles 2017. http://www.who.int/cancer/country-profiles/idn_en.pdf. Accessed June 20, 2017.