
Abstract
Abstract: Overweight and obesity has become a major global health challenge that affects virtually all ages. The aim of this study is to assess the prevalence of overweight/obesity and associated factors among adults of Sodo Town, Southern Ethiopia. Community based cross sectional study was conducted from January to February 2016. A total of 370 households were selected from 14,551 household using a simple random sampling technique., Lottery method was used to select an adult individual with age of ≥25 years. Anthropometric measurements (height and weight) was assessed using the World Health Organization) recommended techniques. Data were analyzed using SPSS windows version 20 Software. Both bivariate and multivariable logistic regression analyses were done. Prevalence of overweight was 32.4% and obesity 16.2%. The combined prevalence of overweight/obesity was 48.6%. Factors associated with overweight/obesity were being female (AOR = 4.0; 95% of CI: 1.7−9.4), Age group between 35–44, 45–54 and age >55 were more likely to be overweight/obesity than age group 25–34 (AOR = 28; 95% CI:1.51–5.15), AOR = 2.44; 95%CI:1.12–5.32), AOR = 5; 95%CI:1.94–12-92) respectively. Similarly, having chronic illness (AOR = 2.9;95%CI:1.1–7.2), using Bajaj/car for transportation (AOR = 1.9; 95% of CI:1.1–3.3), spent 3–5 hours in sitting or reclining (AOR = 3.7;95% CI:1.6–8.5), taking one bottle of soft drink per day (AOR = 2.0;95% CI: 1.1–3.7) and those who consumed vegetable ≥3 times per day (AOR = 5.7; 95% of CI1.6–19.7). Prevalence of overweight/obesity among adult population in Sodo Town is high. Therefore, prioritizing counseling dietary modification about the risk of overweight /obesity in community level, provision of early care and treatment of chronic illness, regular physical exercise by avoiding sedentary life style are recommended.
PUBLIC INTEREST STATEMENT
Overweight and obesity has become a major global health challenge. To identify this community based cross sectional study was conducted at Wolaita Sodo town. Prevalence of overweight was 32.4% and obesity 16.2%. The combined prevalence of overweight/obesity was 48.6%. Factors associated with overweight/obesity were being female, age group between 35 and 44 years age more likely to be overweight/obesity. Similarly, having chronic illness, using Bajaj/car for transportation, spent 3–5 hours in sitting or reclining, taking one bottle of soft drink per day and those who consumed vegetable ≥3 times per day were significantly associated.
Prioritizing counseling dietary modification about the risk of overweight/obesity in community level, provision of early care and treatment of chronic illness, regular physical exercise by avoiding sedentary life style are recommended.
1. Introduction
World Health Organization (WHO) defines overweight and obesity as abnormal or excessive fat accumulation in the body that may affect health (W.H.O, Citation2006). Overweight and obesity are considered an increasing public health problem due to their high prevalence in different age groups (Barquera, Citation2010), as well as the short and long term consequence. Obesity is one of the major disorders associated with the development of chronic degenerative diseases and their complications, with a consequent decrease in life expectancy and quality of life in the affected people(Biro & Wien, Citation2010).
According to WHO, overweight and obesity are the risk for non-communicable diseases (NCDs). It is estimated that in 2015, there would be approximately 2.3 billion adults would be overweight and more than 700 million were obese. Globally, 44% of the diabetes burden, 23% of the ischemic heart disease burden and between 7% and 41% of certain cancer burdens are attributable to overweight and obese (W.H.O, Citation2006).The fundamental cause of overweight and obesity is an energy imbalance between calories consumed and calories expended(Organization WH, Citation2012).
Overweight and obesity are the fifth leading risk for global deaths. At least 2.8 million adults die each year as a result of its complication. Africa is experiencing a shift from underweight to overweight along with the rapid socioeconomic and nutritional transition particularly in its urban population. This transformation comes with increased access to energy-dense foods and less strenuous jobs resulting into many people having a positive energy balance and hence becoming overweight or obese (Organization WH, Citation2012; Ziraba et al., Citation2009).
In Addis Ababa, which is the capital and largest city of Ethiopia, the study revealed that overweight and obesity prevalence have been on a continuous increase, while underweight prevalence has decreased between 2000 and 2011(Yibeltal and Uriyoan (Citation2000–2011)). In addition, obesity related NCDs such as cardiovascular diseases and diabetes are the leading causes of death among adults (Misganaw, Citation2012).
Concern about obesity is particularly important in adults because it helps to reduce the risk of related NCD as well as mortality and morbidity with these problems. Studies on the prevalence of overweight/obesity in different parts of the country and identifying high risk groups in the communities are limited. Thus, this study aims at assessing prevalence of overweight and obesity and their associated factors among children and adolescents but it is not well studied among adults.
2. Methods and materials
2.1. Study design and setting
Community based cross-sectional study design was conducted among adults ≥ 25 years in Sodo Town from January to February 2016.Sodo town is the capital city of Wolaita Zone, Southern Ethiopia. The total population is estimated to be 110,659 from which 57,477 are male. The total number of households in the town is 14,551. The town is structured in 3 sub- cities and in 11 administrative units known as “kebele”. There are 2 hospitals, 3 health centers, 11 health posts and more than 21 private health institutions providing health services in the town.
2.2. Inclusion and exclusion criteria
All selected adults aged ≥25 years old were included in this study while adults who had difficulty standing steady or straight for height measurement, and those who were pregnant and unable to talk where excluded.
2.3. Sample size and sampling procedure
Sample size was determined by using single population proportion formula at 95% confidence level, prevalence of overweight among adults of 32.4% in the study of Gonder city (Beyene et al., Citation2014). Margin of error of 5% and by considering 10% non-response rate the total sample size of the study was 370. After determining sample size updated lists of household heads names from each Kebele were collected from the eleven kebeles of Sodo Town. The collected list of names was compiled into one sheet and the serial number was given to all households from 1 to 14,551. By using SPSS windows version 20 Software, 370 households were selected randomly. From the selected households, an adult ≥25 year was selected using a lottery method.
2.4. Data collection procedure
Socio economic, demographic and dietary intake information were collected using a pre-tested structured questionnaire. Weight was measured using a well-calibrated, portable digital scale with participants standing on without shoes and wearing light clothing. The scale was checked before each measurement for zero adjustment. The scale was carefully handled and periodically calibrated to ascertain its accuracy. Weight measurement was taken to the nearest 0.1 kg.
Height was measured using portable studios-meter, which consisted of an anthropometry with a simple triangular headboard. It was taken to make participants stand upright with their shoes off and their head held erect such that the external auditory meatus and the lower border of the eye were in one horizontal plane (Frankfurt plane). The back of the head, shoulder blades, buttocks, calves and heel touched the vertical stand of the stadiometer and arms hanging naturally by the sides. A movable triangular headboard was brought against the crown of the head and height measurement was read at maximum inspiration. The height was measured to the nearest 0.1 cm. All measurements were taken twice by one nurse and one of the assistants and the average was taken. A third measurement was taken if it differed by 0.5 kg in weight and 0.5 cm in height and Body Mass Index (BMI) was calculated using weight and height (kg/m2). Eight diploma nurses as data collectors and two BSc health officers as supervisors were participated in the data collection process.
2.5. Data quality control
The questionnaires were prepared in English and then translated to Amharic and rendered back to English to keep the consistency of the questions. Data collectors and supervisors were trained for two days about the proper filling of questionnaires and on how to measure weight and height. Pre- testing of the questionnaire was made on 19(5%) persons to ensure the reliability of the questionnaire. It was done in a place out of actual study area to check accuracy, to estimate time and any inconsistency and correction was made based on response from pretest. Feedbacks from the pre-test were incorporated into the final questionnaire design. Principal investigator and supervisors checked on the spot and reviewed all the completed questionnaires to ensure completeness and consistency of the information collected.
2.6. Operational definition
Adult꞉ An individual whose age is ≥25 years old.
Obesity꞉ BMI greater or equal to 30 is obese.
Overweight꞉ A BMI greater or equal to 25.0 but less than 30.0 kg/ m2.
Body mass index: Anthropometric measure defined as weight in kilograms divided by height in meters squared (weight (kg)/height (m2).
Sitting or reclining on a typical day: The sum total of time spent watching TV, work on a computer, sitting on the market, driving, sewing clothes on singer and set or lay down in the home in particular day time.
Usual intake: Consumption of the particular food item at least twice a week.
Moderate exercise: Low-impact aerobic exercise classes, brisk walking recreational team sports (volleyball).
Vigorous exercise: Running, football, high-intensity aerobic classes, competitive full-field sports or basketball (Alemu et al., Citation2014).
2.7. Data management and analysis
Data were checked for completeness, coded and entered into EPI INFO version 3.5.1 then exported to SPSS version 20 for analysis. Descriptive statistics using frequency, proportions, mean, standard deviation were performed and tables were used to present the study results. Bivariate and multivariable logistic regression analysis were used to determine the associations between different variables, and odds ratio with 95% confidence intervals for the degree of association between dependent and independent variables for identifying important determinants of overweight/obesity. Variables with p-value of less than 0.25 on bivariate regression analysis were entered to multivariable model. Multivariable analysis was performed following bivariate analysis to adjust for possible confounders. Both crude and adjusted odds ratio (AOR) with 95% confidence interval were reported. During the analysis multicollinearity was checked. In addition, Hosmer and Lemeshow’s goodness-off test was considered to check the model fitness. Statistical significance considered at significance level of 5% or p-value less than 0.05.
2.8. Ethical consideration
The ethical clearance was obtained from the Ethical Review Committee of Wolaita Sodo University (WSU). The letter from WSU was given to the Wolaita Sodo Town administrator and Zonal, Health Office and three sub cities of Sodo town after getting permission from the sub cites. Additional permeation to conduct studies in the area was obtained from district leaders. The study was conducted based on consent of the study subjects after explaining the purpose of the study. Informed verbal consent was obtained from each participant before starting the interview without any obligation or persuading. The data collection was conducted in Amharic language after only explaining their willingness to respond freely. Participants were told that their involvement in the study was on their voluntary basis, and if they were unwilling to participate in the study and wished to quit from the study at any time, it was the participant right without any restriction.
3. Result
3.1. Socio demographic and economic characteristics of the respondents
More than half of the respondents, 234(63.2%) were females. The median age of participant was 35 years with interquartile range (IQR) (28, 45). More than one third 157 (42.4%) were 25–34 age groups. Majority, 269 (72.7%) of the respondents were protestant Christian and the majority, 294(79.5%), were Wolaita by ethnicity.
Regarding their marital status, 312 (84.3%) were married. More than one third 146 (39.5%) of the study participants had attended college or more educational level. Of the study participants 165 (44.6%) were government and non-government employees. More than half, 202 (54.6%) of the respondents were living in households with greater or equal to five family members. One hundred fifty-four (41.6%) were household heads, from, whom 123 (79.9%) are males and 31 (20.1%) are females. Regarding monthly income 139 (37.6%) of the participants get monthly income of ≤1000 Birr. The median income of the participant with IQR was 1688.5 (800.00, 3431.25) Birr. Regarding housing condition of the respondents, majority 304 (82.2%) live in their own houses ().
Table 1. Socio demographic and economic characteristics of the respondents in Sodo Town, 2016
3.2. Physical activity of respondents
Only 21 (5.7%) and16 (4.3%) of the participants were engaged in vigorous and moderate physical activity respectively. Regarding the transportation mechanism, 212 (57.3%) moved from place to place for their duty mainly on foot. One hundred eight (29.2%) of the respondents would sit or recline 3–5 hours in particular day. The median sitting hours of the participant with IQR were 3 (Barquera, Citation2010; Ziraba et al., Citation2009). ()
Table 2. Physical activity of respondents in Sodo Town, 2016
3.3. Health conditions of the respondents
One in ten [39/370 (10.5%)] of the respondent had at least one known chronic illness (18 had hypertension and 15 had diabetes mellitus) of which 32 reported taking regularmedication. But the remaining 6 were neither hypertension nor with diabetes mellitus. Thirteen (3.5%) reported that they consumed alcoholic beverages and very few [4/370 (1.1%)] smoke cigarettes.
3.4. Dietary information of the respondents
More than half, 246 (66.5%), of the respondents reported that they usually ate 4 times a day. Regarding the usual intake, all the participants consumed cereals. Majorities, 305 (82.4%) consumed pulse and legume 266 (71.9%) vegetables and 227 (61.4%), (tea and/or coffee). Furthermore, 83 (22.4%) of the participant consumed milk and milk products, Forty-three (11.6%) tubers, 44 (11.9%) meat, very few 4 (1.1%) fruits and 2 (0.5%) sweets. Regarding 24-hour consumption majorities 185 (50%), reported that they consumed vegetable, 185 (50%), pulse and legume, 161 (43.5%), fruit twice per day. Furthermore, the rest 52 (14.1% of participant responded that they consumed meat, 63 (17%) egg, 89 (24.1%) milk and milk product 116 (31.4%) soft drink once per day. ()
Table 3. Dietary information of the respondents in Sodo Town, 2016
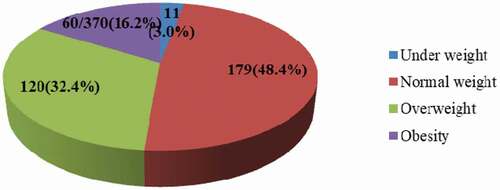
3.5. Prevalence of overweight/Obesity among adults in Sodo town
As indicated on , the prevalence of underweight, normal weight, overweight and obesity among the adults in Sodo town were found to be 3.0% [95% of CI (1.4–4.9)], 48.4% [95% of CI (43.2–53.5)], 32.4% [95% of CI (27.8–37.3)] and 16.2% [95% of CI (12.7–20.5)] respectively. Thus, the combined prevalence of overweight/obesity was found to be 48.6% [95% of CI (43.5–50.0)].
Figure 1. Nutritional status of adults in Sodo Town, 2016
3.6. Factors associated with overweight/obesity
As indicated in the , sex, age, head of household, family size, monthly income, house ownership, chronic illness, 24 hour vegetable, meat, soft drink, usual egg, milk and milk products, meat consumption, means of transport and the number of hours spent on sitting or reclining in a typical day were factors associated with overweight /obesity in bivariate logistic regression. Some variables that were associated with overweight /obesity during bivariate analysis lost their significance in the multivariable model thus, being female, age, presence of chronic illness, means of transport, vegetable, and soft drink consumption and sitting hours retained significance in the multivariable model.
Table 4. Factors associated with overweight/obesity in Sodo Town, 2016
After controlling other factors, the odds of being overweight/obesity was 3.98 times higher for females compared to males (AOR = 3.98; 95%CI:1.7–9.4). Age group between 35–44, 45–54 and age >55 were more likely to be overweight/obesity than age group 25–34 (AOR = 28; 95% CI: 1.5–5.2), AOR = 2.44; 95%CI: 1.1–5.3), AOR = 5; 95%CI: 1.9–12.9) respectively. The odds of overweight/ obesity were 2.9 times higher among those with known chronic illness when compared to those who do not have known chronic illness (AOR = 2.9; 95% CI:1.13–7.2).
Participants who use vehicles (Bajaj, motor bike) for transportation were 1.93 times more likely to have overweight/ obese than those who walk (AOR = 1.94; 95% CI: 1.5–3.3). Respondents who consume one bottle of soft drink within 24 hours were 2 times more likely to have overweight/ obese compared to those who were not consuming any soft drink (AOR = 2.0; 95% CI: 1.1–3.7). Participant who spent 3–5 hours of sitting or reclining were 3.67 times more likely to be overweight/obese than those not specific hours of sitting (AOR = 3.67; 95% CI: 1.6–8.5). Respondents who consuming vegetable three or more than 3 times per day were 5.7 times more likely to be overweight/obese than those not consume vegetable (AOR = 5.68; 95% CI: 1.6–19.7).
4. Discussion
Overweight or obesity in adult population of Sodo town has been found to be a huge public health problem. The prevalence of overweight among adults in Sodo town was found to be 32.4%, whereas the prevalence of obesity was 16.2% thus, the combined prevalence of overweight/obesity was found to be 48.6%.It was observed that there was limited physical activity. Majorities of the respondents spent more day time by sitting in the workplace or in their home. This might lead them to overweight/obese. Some of the factors are not associated with overweight/obesity in this study are monthly income, educational status and physical activity.
High prevalence of overweight/obesity found in our study was similar with previous study conducted in Gonder town; which identified overweight, 32.4% and obesity, 16.2% (Beyene et al., Citation2014). This study was nearly similar for overweight (32.1%). Result in the study conducted in Afghanistan Jalalabad city but obesity finding was relatively higher than this study (27.4%) (Saeed, Citation2015). On the other hand, the prevalence of overweight and obesity in this study was higher than the findings reported from the Balearic Islands in Mediterranean region, Benin and Zambia as overweight 29.4%,19.2%, 24.7% and obesity 11.2%, 7.28%, 16.9% respectively (Coll et al., Citation2015; Gbary et al., Citation2014; Zyaambo et al., Citation2013). In addition, the combined prevalence of overweight/obesity of women in Nigeria was 20.9% (Kandala et al., Citation2014).The difference might be attributable to the feeding habit, low physical activity because of high sedentary lifestyle, and socio demographic and economic variations between study areas.
From the total participants, females account, 234 (63.2%) from whom 132 (56.4%) were overweight/ obese and male account 136 (36.8%) from whom 48 (35.3%) were overweight or obese. This study found that female were almost 4 times more likely to be overweight/obese than males. Similar findings had also been reported in several previous studies conducted in Uganda, Iran, Benin and Panama, which concluded that females are more likely to be overweight or obese than males (Ahmadi et al., Citation2014; Baalwa et al., Citation2010; Gbary et al., Citation2014; Sasson et al., Citation2014). This could be related to the influence of cultural factors (Muhihi et al., Citation2012). At times, female obesity is seen as a sign of wealth and beauty in the African cultural context (Gbary et al., Citation2014).
This study found that higher age (≥55) was 5 times more likely have overweight/obesity compared to lower age group (Lindström, Citation2008–34). This study was supported by a study conducted in Tanzania which indicated that higher age (≥55) year was 5.1 times more likely to be obese compared to age group (Bassett et al., Citation2008; Healy et al., Citation2008; Mohd Sidik & Rampal, Citation2009; Muhihi et al., Citation2012; Ondicho et al., Citation2016; Sasson et al., Citation2014; Shayo & Mugusi, Citation2011) years (Shayo & Mugusi, Citation2011). The recent study conducted in Kenya revealed that participants with higher age group (40–49) years were 7 times more likely to be overweight/obese compared to respondents under 30 years (Ondicho et al., Citation2016). In addition, the result of other studies indicated that higher age was significantly associated with overweight/obesity (Studies from Malaysia and Balearic Islands Mediterranean region) (Coll et al., Citation2015; Mohd Sidik & Rampal, Citation2009). The study revealed that as age increased the proportion of deaths from chronic NCDs also increased (Misganaw, Citation2012). It might be due to the case that as age increases peoples are more likely to lead sedentary lifestyle, this leads them to overweight/obesity and their complication of chronic NCDs.
This study also identified that participants with known chronic illnesses (diabetes mellitus, hypertension) were 2.85 times more likely to be overweight/obese. This study was supported by the study conducted in Afghanistan, which found that diabetes mellitus and high blood pressure both were associated with obesity. This shows that adult population were suffering from different risk factors at the same time (Saeed, Citation2015).Another study revealed that there is emerging evidence on the fact that sedentary time is associated with increased risk of major chronic diseases (Healy et al., Citation2008). In this study, around one third 108 (29.2%) of the participant remain sitting 3–5 hours of daytime on their workplace or in their home. The overweight/obesity observed in this study might be related to this behavior.
Regarding transport mechanism the study found that participants who used their vehicles, cars, Bajaj or motor bike to move from place to place were 1.93 times more likely to be overweight/obese than those who used to walk. Study revealed that those countries with the highest rates of car use for travel have the highest obesity rates (Bassett et al., Citation2008).This might be walking to work or for other duties from place to place promotes energy expenditure and decreases the risk of overweight/obesity (Lindström, Citation2008). In this study, 158 (42.7%) of the respondents used own car, Bajaj/motor bike for transportation, which might lead them to overweight/obesity.
Another finding of this study was participants who spent 3–5 hours sitting or reclining in particular day were 3.67 times more likely to be overweight/obesity compared to those who had no specific sitting hours. This study supported by study conducted in Zambia revealed that participants who spent 3.5 hours or more sitting or reclining on a typical day were 1.23 times more likely to be overweight/obese compared to those that spent less than 1.5 hours (Zyaambo et al., Citation2013). Other studies conducted among Spanish adults, woman in Addis Ababa and India conclude that watching television for longer duration was associated with overweight/ obesity (EDVAC & YOEA, Citation2009; Gouda & Prusty, Citation2014; Tebekaw et al., Citation2014). This might have increased sedentary lifestyle and physical inactiveness and helps in weight gain.
In the current study, soft drink intake is associated with overweight or obesity respondents who consumed at least a bottle of soft drink once within 24 hours were 2 times more likely to be overweight/obese than those who did not consume any soft drinks. The study revealed that participants who consumed ≥1 soft drink per day had a 37% high-risk of obesity (Dhingra et al., Citation2007).This might be as indicated in the review of different nutritional research there was clear associations of soft drink intake with increased energy intake, highly consumption of it is one of the factors that causing weight gain (Malik et al., Citation2006; Vartanian et al., Citation2007).
Another finding of this study was participants who consume vegetable within 24 hours were 5.7 times more likely to be overweight/obese compared to those not consume vegetable. This study supported by study conducted in Ghana among young adults (Sasson et al., Citation2014–36) years revealed that students who consumed fruits and vegetables >3 days per week were 2.6 times more likely to be overweight/obesity compared with those consuming less than 3 times per week (Mogre et al., Citation2015). This result has statistical significance. This might be due to consumption of vegetables as extra food at the top of regular food. There is a need for further study to investigate the relationship between vegetable consumption and overweight/obesity.
4.1. Strength and limitation of the study
Strength of this study includes; use of simple random sampling to draw sample population, r data collectors were adequately trained on anthropometric measurements and their measurement was standardized before the actual data collection. The limitations of this study were use of single 24- hour dietary recall it may be prone to recall bias and regarding usual consumption the study depends on self-report, there might be recall and social desirability bias from respondents
4.2. Conclusion
Prevalence of overweight/obesity among adult population in Sodo Town is high and of important public health concern. The unhealthy lifestyle that is characterized by sedentary life, less or no physical activity and easy accuses of transportation might contribute to this problem. Therefore, it is recommended that counseling dietary modification and about the risk of overweight/obesity in community level should be a national public health priority. Moreover, provision of early care and treatment for chronic illness, regular physical exercise by avoiding sedentary life style are recommended. In addition, further research is needed; results from our study suggest several factors that are associated with overweight/obesity which should be observed through better research design that takes them into consideration.
Authors’ information
AA: is Masters of Science in Human nutrition (MSC), ET: PhD, assistant Professor at Kotebe Metropolitan University, Addis Ababa, Ethiopia: YH: PhD, assistant Professor at the School of Public Health.
Authors’ contributions
AA: designed the study with ET, wrote the proposal, handled data collection, analyzed the data and drafted the paper. ET: guided in the conception and design, approved the proposal with some revisions and involved in the analysis of findings. YH: guided in the conception, approved the proposal, and supervised interviews and data collection, involved in analysis of data.
Competing Interest: The authors declare no conflict of interest.
Ethics approval and consent to participate
The ethical clearance was obtained from the Ethical Review Committee of Wolaita Sodo University (WSU). The letter from WSU was given to the Wolaita Sodo Town administrator and Zonal, Health Office and three sub cities of Sodo town after getting permission from the sub cites. Additional permeation to conduct studies in the area was obtained from district leaders. The study was conducted based on consent of the study subjects after explaining the purpose of the study. Informed verbal consent was obtained from each participant before starting the interview without any obligation or persuading. Participants were told that their involvement in the study was on their voluntary basis, and if they were unwilling to participate in the study and wished to quit from the study at any time, it was the participant right without any restriction.
Acknowledgements
We would like to express gratitude to NORHED project coordinating office for their financial support. We also extend our thanks to data collectors and supervisors who collected data and supervised the collectors. Finally, we would like to appreciate the study participants for their willingness and participation in the study.
Availability of data and material
Data is not available for online access; however, readers who wish to gain access to the data can write to the corresponding author Yoseph Halala at [email protected]
Additional information
Funding
Notes on contributors
Yoseph Halala Handiso
Azalech Ayza is an MSc scholar at Wolaita Sodo University, School of public health, department of nutrition and reproductive health.
Dr. Yoseph Halala Handiso is an Assistant Professor in the school of public health at the
department of nutrition and reproductive health, Wolaita Sodo University. His research interests
include themes on human nutrition and reproductive health, food and nutrition security, agricultural and nutrition liking.
Dr. Elazar Tadesse is human nutrition research at Kotebe Metropolitan University, Addis Ababa, Ethiopia
References
- Ahmadi, M., Moosazadeh, M., Vardanjani, H. M.-E., & Dehghan, A. (2014). Prevalence of obesity and overweight and their related factors among the adults of Mazandaran Province, Iran, in 2010. Electronic Physician, 6(4), 955. DOI:https://doi.org/10.14661/2014.955-961
- Alemu, E., Atnafu, A., Yitayal, M., & Yimam, K. (2014). Prevalence of overweight and/or obesity and associated factors among high school adolescents in Arada Sub city, Addis Ababa, Ethiopia. Journal of Nutrition & Food Sciences, 4. DOI: https://doi.org/10.4172/2155-9600.1000261
- Baalwa, J., Byarugaba, B., Kabagambe, E., & Otim, A. (2010). Prevalence of overweight and obesity in young adults in Uganda. African Health Sciences, 10(4), 367–373. https://www.ajol.info/index.php/ahs/article
- Barquera, S. T. L. (2010). Increasing Public Health Problems. In M. Chapela (Ed.), In the Debate: Diabetes in Mexico, [In Spanish] (pp. 53–13). Universidad Autónoma Metropolitana (UAM) Xochimilco.
- Bassett, D. R., Pucher, J., Buehler, R., Thompson, D. L., & Crouter, S. E. (2008). Walking, cycling, and obesity rates in Europe, North America, and Australia. Journal of Physical Activity and Health, 5(6), 795–814. https://doi.org/https://doi.org/10.1123/jpah.5.6.795
- Beyene, M., Bemnet, A., Bereket, F., & Afework, K. (2014). High prevalence of overweight, obesity, and hypertension with increased risk to cardiovascular disorders among adults in northwest Ethiopia: A cross sectional study. BMC Cardiovascular Disorders, 14(1), 1. http://www.biomedcentral.com/1471-2261/14/155
- Biro, F. M., & Wien, M. (2010). Childhood obesity and adult morbidities. The American Journal of Clinical Nutrition, 91(5), 1499S–505S. https://doi.org/https://doi.org/10.3945/ajcn.2010.28701B
- Coll, J. L., Bibiloni, M., Salas, R., Pons, A., & Tur, J. A. (2015). Prevalence and related risk factors of overweight and obesity among the adult population in the Balearic Islands, a Mediterranean Region. Obesity Facts, 8(3), 220–233. https://doi.org/https://doi.org/10.1159/000435826
- Dhingra, R., Sullivan, L., Jacques, P. F., Wang, T. J., Fox, C. S., Meigs, J. B., D’Agostino, R. B., Gaziano, J. M., & Vasan, R. S. (2007). Soft drink consumption and risk of developing cardiometabolic risk factors and the metabolic syndrome in middle-aged adults in the community. Circulation, 116(5), 480–488. https://doi.org/https://doi.org/10.1161/CIRCULATIONAHA.107.689935
- EDVAC, S. O. B. R. E. P. E. S. O., & YOEA, E. S. P. A. Ñ. O. L. E. S. (2009). Life-style factors associated with overweight and obesity among Spanish adults. Nutricion Hospitalaria : Organo Oficial De La Sociedad Espanola De Nutricion Parenteral Y Enteral, 24(2), 144–151. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4089075/
- Gbary, A. R., Kpozehouen, A., Houehanou, Y. C., Djrolo, F., Amoussou, M. P., Tchabi, Y., Salamon, R., & Houinato, D. S. (2014). Prevalence and risk factors of overweight and obesity: Findings from a cross-sectional community-based survey in Benin. Global Epidemic Obesity, 2(1), 3. https://doi.org/https://doi.org/10.7243/2052-5966-2-3
- Gouda, J., & Prusty, R. K. (2014). Overweight and obesity among women by economic stratum in urban India. Journal of Health, Population, and Nutrition, 32(1), 79. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4089075/
- Healy, G. N., Wijndaele, K., Dunstan, D. W., Shaw, J. E., Salmon, J., Zimmet, P. Z., & Owen, N. (2008). Objectively Measured Sedentary Time, Physical Activity, and Metabolic Risk: The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care, 31(2), 369–371. https://doi.org/https://doi.org/10.2337/dc07-1795
- Kandala, N.-B., Stranges, S., & Kazembe, L. (2014). Geographic variation of overweight and obesity among women in Nigeria: A case for nutritional transition in Sub-Saharan Africa. PloS One, 9(6), e101103. https://doi.org/https://doi.org/10.1371/journal.pone.0101103
- Lindström, M. (2008). Means of transportation to work and overweight and obesity: A population-based study in southern Sweden. Preventive Medicine, 46(1), 22–28. https://doi.org/https://doi.org/10.1016/j.ypmed.2007.07.012
- Malik, V. S., Schulze, M. B., & Hu, F. B. (2006). Intake of sugar-sweetened beverages and weight gain: A systematic review. The American Journal of Clinical Nutrition, 84(2), 274–288. https://doi.org/https://doi.org/10.1093/ajcn/84.2.274
- Misganaw, A. (2012). The double mortality burden among adults in Addis Ababa, Ethiopia, 2006-2009. Preventing Chronic Disease, 9. DOI:https://doi.org/10.5888/pcd9.110142
- Mogre, V., Nyaba, R., Aleyira, S., & Sam, N. B. (2015). Demographic, dietary and physical activity predictors of general and abdominal obesity among university students: A cross-sectional study. SpringerPlus, 4(1), 1. https://doi.org/https://doi.org/10.1186/s40064-015-0999-2
- Mohd Sidik, S., & Rampal, L. (2009). The prevalence and factors associated with obesity among adult women in Selangor, Malaysia. Asia Pacific Family Medicine, 8(1), 1–6. DOI: https://doi.org/10.1186/1447-056X-8-2
- Muhihi, A. J., Njelekela, M. A., Mpembeni, R., Mwiru, R. S., Mligiliche, N., & Mtabaji, J. (2012). Obesity, overweight, and perceptions about body weight among middle-aged adults in Dar es Salaam, Tanzania. International Scholarly Research Notices, 4. DOI: https://doi.org/10.5402/2012/368520
- Ondicho, Z., Omondi, D., & Onyango, A. (2016). Prevalence and Socio-demographic Factors Associated with Overweight and Obesity among Healthcare Workers in Kisumu East Sub-County, Kenya. American Journal of Medicine and Medical Sciences, 6(3), 66–72. https://repository.maseno.ac.ke/handle/123456789/3162
- Organization WH. Obesity and overweight. Fact sheet N 311, updated march 2013. 2012.
- Saeed, K. M. I. (2015). Prevalence and associated risk factors for obesity in Jalalabad city–Afghanistan. Alexandria Journal of Medicine, 51(4), 347–352. https://doi.org/https://doi.org/10.1016/j.ajme.2014.12.004
- Sasson, M., Lee, M., Jan, C., Fontes, F., Motta, J., & Wang, G. (2014). Prevalence and associated factors of obesity among Panamanian adults. 1982–2010. PloS One, 9(3), e91689. https://doi.org/https://doi.org/10.1371/journal.pone.0091689
- Shayo, G. A., & Mugusi, F. M. (2011). Prevalence of obesity and associated risk factors among adults in Kinondoni municipal district, Dar es Salaam Tanzania. BMC Public Health, 11(1), 1. https://doi.org/https://doi.org/10.1186/1471-2458-11-365
- Tebekaw, Y., Teller, C., & Colón-Ramos, U. (2014). The burden of underweight and overweight among women in Addis Ababa, Ethiopia. BMC Public Health, 14(1), 1. https://doi.org/https://doi.org/10.1186/1471-2458-14-1126
- Vartanian, L. R., Schwartz, M. B., & Brownell, K. D. (2007). Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. American Journal of Public Health, 97(4), 667–675. https://doi.org/https://doi.org/10.2105/AJPH.2005.083782
- W.H.O. Obesity and overweight. in WHO Media centre fact sheet Email: mediainquiries@whoint. 2006.
- Yibeltal T, Charles T, and Uriyoan C. (2000-2011). The Rising Overweight-obesity and Its Socio-Demographic Correlates in Addis Ababa.
- Ziraba, A. K., Fotso, J. C., & Ochako, R. (2009). Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health, 9(1), 1. https://doi.org/https://doi.org/10.1186/1471-2458-9-465
- Zyaambo C., BabaniyiO., Songolo P., Adamson S., and Rudatsikira E. (2013). Prevalence and Determinants for Overweight and Obesity among Residents of a Mining Township in Kitwe, Zambia, in 2011: A population-based Survey. Clinical Practice, 4(1), 1–7. https://digitalcommons.andrews.edu/pubs/590