
Abstract
Egg freezing (EF) technology has improved significantly over the last decade, giving women more choice over their reproductive futures. Despite this advance, EF brings forth contentious ethical and regulatory issues. Policies controlling access to EF vary around the world and there is a lack of consensus about who should have access and what criteria are relevant in making these decisions. This study aimed to identify views of women about access to EF for both “medical” and “non-medical” risks to infertility. An online survey was administered to women aged between 18 and 60 years in Victoria, Australia between April and May 2018. A total of 1,066 individuals initiated the survey. The median age of the participants was 28 years and 81% were <40 years old. Almost all participants (98%) supported access to medical EF in situations where treatments (e.g. chemotherapy) or illnesses threaten fertility. Support for access to EF for non-medical indications was lower; 75% supported EF for “lack of suitable partner”, followed by “financial insecurity to raise a child” (72%) and “career/educational advancement” (65%). Older respondents (aged ≥40 years) were less likely than their younger counterparts to support all indications for non-medical EF. Our findings indicate broad support for EF. However, the variation in support between indications for non-medical EF suggests that individuals do not think about access to EF simply in terms of medical necessity. To reflect public views, future policy may need to consider access to EF beyond the medical/non-medical distinction.
Résumé
La technologie de congélation ovocytaire s’est sensiblement perfectionnée ces dix dernières années, donnant aux femmes davantage de choix sur leur avenir reproductif. En dépit de ces progrès, la congélation ovocytaire suscite des questions éthiques et régulatrices controversées. Les politiques contrôlant l’accès à cette technique varient dans le monde et un consensus fait défaut sur les personnes qui devraient y avoir accès et les critères pertinents pour prendre ces décisions. L’étude souhaitait connaître les idées des femmes sur l’accès à la congélation ovocytaire pour les risques « médicaux » et « non médicaux » de stérilité. Une enquête en ligne a été administrée à des femmes âgées de 18 à 60 ans à Victoria, Australie, entre avril et mai 2018. Au total, 1066 personnes ont commencé l’enquête. L’âge médian des participantes était de 28 ans et 81% avaient moins de 40 ans. Presque toutes les participantes (98%) approuvaient l’accès à une congélation ovocytaire médicale dans les situations où des traitements (par exemple la chimiothérapie) ou des maladies menacent la fécondité. Le soutien à l’accès pour des raisons non médicales était plus faible; 75% appuyaient la congélation ovocytaire en cas de « manque de partenaire approprié », 72% en cas « d’insécurité financière pour élever un enfant » et 65% pour privilégier « l’avancement de la carrière/de l’éducation ». Les répondantes plus âgées (de 40 ans ou plus) avaient moins de probabilités que les plus jeunes de soutenir toutes les indications pour une congélation ovocytaire non médicale. Nos résultats indiquent un large soutien à la congélation des ovocytes. Néanmoins, la variation du soutien entre les indications pour la congélation ovocytaire non médicale suggère que les personnes ne conçoivent pas l’accès à cette technologie simplement du point de vue de la nécessité médicale. Pour traduire les idées de l’opinion publique, les futures politiques devraient peut-être envisager l’accès à la congélation ovocytaire au-delà de la distinction médicale/non médicale.
Resumen
La tecnología de congelación de óvulos (CO) ha mejorado de manera significativa en la última década, por lo cual las mujeres tienen más opciones para determinar su futuro reproductivo. A pesar de este avance, la CO suscita asuntos éticos y normativos contenciosos. Las políticas que controlan el acceso a la CO varían en todo el mundo y hay falta de consenso sobre quién debería tener acceso y qué criterios son pertinentes para tomar estas decisiones. El objetivo de este estudio era identificar los puntos de vista de las mujeres sobre el acceso a la CO por riesgos “médicos” y “no médicos” de infertilidad. Se administró una encuesta en línea a mujeres entre 18 y 60 años, en Victoria, Australia, entre abril y mayo de 2018. Un total de 1066 mujeres iniciaron la encuesta. La edad media de las participantes fue de 28 años y el 81% tenía <40 años. Casi todas las participantes (98%) apoyaron el acceso a la CO médica en situaciones donde los tratamientos (ej., quimioterapia) o enfermedades ponen en riesgo la fertilidad. Hubo menos apoyo para acceder a la CO por indicaciones no médicas; el 75% apoyó la CO por “falta de una pareja adecuada”, seguido de “inseguridad financiera para criar a un niño” (72%) y “avance profesional/educativo” (65%). Las encuestadas de edad más avanzada (≥40 años) eran menos propensas que las más jóvenes a apoyar todas las indicaciones para la CO no médica. Nuestros hallazgos indican amplio apoyo para la CO. Sin embargo, la variación en apoyo entre las indicaciones para la CO no médica indica que las personas no piensan en el acceso a la CO simplemente en términos de necesidad médica. Para reflejar las opiniones públicas, futuras políticas posiblemente deban considerar el acceso a la CO más allá de la distinción médica/no médica.
Introduction
In many affluent nations there has been a shift in the timing of parenthood.Citation1 In Australia, the median age of mothers has risen from 26.3 years in 1978Citation2 to 31.3 years in 2017.Citation3 The reasons for this shift are multifactorial; however, one element is thought to be lifestyle-related, with women describing a desire for career-development or building financial security before having children.Citation4,Citation5 While fulfilling these goals lends to greater gender equality and expands options for women, it can also have some severe limitations in terms of achieving family goals. When women postpone childbearing, they risk not reaching their parenting aspirations, as the chances of conceiving decrease with age.Citation6,Citation7
Oocyte cryopreservation or “egg freezing” (EF) is a method of fertility preservation that may extend fertility beyond the natural time that a woman is fertile. Eggs are collected using Assisted Reproductive Technology (ART), cryopreserved by vitrificationCitation8 and placed in storage until a later time when they can be used to create embryos through in vitro fertilisation (IVF). The freezing process halts the aging of eggs and enables women to consider pregnancies at a later time. Initially EF was only offered to women at risk of infertility from medical treatments such as chemotherapy, or from illness such as premature ovarian failure (referred to as “medical” EF). However, more recently EF has become an option for women faced with the prospect of age-related infertility (referred to as “non-medical” EF). Of the emerging cohort of women accessing non-medical EF, the majority report that the reason for choosing to freeze eggs is due to not having a partner with whom to have children.Citation9–12 It has been suggested that it is the growing popularity of non-medical EF that is driving the dramatic increase in EF cycles seen worldwide.Citation13–15
EF is offered around the world; however, policies and laws control access to EF in different ways. Some nations enforce a distinction between the “medical” and “non-medical” use of EF; for example, non-medical EF is prohibited in FranceCitation16 and Singapore,Citation17 and only permitted in Turkey for women with a low ovarian reserve or history of premature ovarian failure.Citation18 In other nations, varying age limits are enforced; Israel restricts access only to women aged between 30 and 41 years,Citation19 in Germany EF is restricted to women between the ages of 20–49 years, and in Denmark only a maximum age of 46 is specified.Citation16 While cross-border differences in healthcare are to be expected, the variety of approaches to managing EF indicate a lack of consensus about who should have access to EF, or what criteria are relevant in making these decisions. In addition, the inconsistencies between criteria challenge the rationale behind these requirements, which raises difficult questions about fair ways to govern access to EF.
In Australia the regulation of ART varies across states and territories. In the state of Victoria, ART is governed by the Assisted Reproductive Treatment Act 2008 (Vic). This Act was drafted at a time when EF was considered experimentalCitation20 and access to EF was limited to women with a medical indication requiring fertility preservation. A recent review into the 2008 Act, commissioned by the Victorian Government, reported that there is confusion over which parts of the Act apply to EF.Citation21 Furthermore, some stakeholders suggested that EF is outside the legislative scope of the Act as it does not meet the current definitions of an ART “treatment procedure”, because EF does not involve attempts at fertilisation to produce embryos.Citation21 Notwithstanding this confusion, both medical and non-medical EF are currently offered in many clinics around Australia, with government funding only available for medically indicated EF.
The treatment scope of EF has dramatically changed since the Victorian 2008 Act was enacted and yet there has been no significant update to legislation, policy or guidelines to reflect these advancements. As demand for EF is likely to continue to increase, it is timely to review our approach to this technology. Since novel technologies like EF have broader societal and ethical consequences, consultation with key stakeholders is crucial to understand the real-world experience of potentially affected individuals and the competing interests of those involved.Citation22 Previous exploratory studies from Europe, Canada and the US have reported that most people support medical EF, but have some reservations about the use of EF for non-medical indications.Citation23–27 However, to date no equivalent study has been conducted in Australia. The aim of this study was to explore attitudes about access to EF for both medical and non-medical reasons in Victoria, Australia. The state of Victoria was the first jurisdiction in the world to introduce legislation on ARTs (Infertility (Medical Procedures) Act 1984) and is generally acknowledged as a leader in the development of ART technologies and the regulation of ARTs.Citation28,Citation29 Therefore, Victoria is a key state to review public opinion on emerging reproductive technologies. Data about public attitudes significantly contribute to understanding the acceptance of EF and can be used to inform evidence-based policy and guidelines worldwide.
Materials and methods
An anonymous, online, cross-sectional survey of the general public was conducted in Australia between April 2018 and May 2018. The survey, hosted through the Research Electronic Data Capture (REDCap) platform, was advertised predominantly through online social media campaigns via Facebook and parenting forums such as The BubHub. Interested participants were invited to follow a link to undertake the survey. The survey comprised 35 questions that were adapted, with permission, from the Fertility Preservation Survey developed in Canada by Daniluk and Koert.Citation23 The survey collected standard demographic data and included questions that addressed; the timing of parenthood, fertility intentions, beliefs about EF (medical and non-medical) and decision-making considerations in regard to EF. An overview of those results was presented in part at the annual meeting of the European Society of Human Reproduction and Embryology.Citation30 This paper reports on responses to part of the survey: the questions that sought participants’ views about whether access to medical and non-medical EF should be permitted. Throughout the paper we refer to access to EF by women, however the authors acknowledge that access to EF may also be relevant to individuals that do not identify as women.
Participants were asked to respond, via a 5-point Likert scale (strongly disagree/disagree/undecided/agree/strongly agree), to questions about whether they agreed that access to EF should be allowed in the following situations:
To preserve fertility for women who are about to undergo treatments that could render them infertile in the future (e.g. chemotherapy for cancer)
To preserve fertility for women who have medical conditions that could render them infertile in the future (e.g. endometriosis, premature menopause)
To preserve fertility for women delaying childbearing because they do not have a partner
To preserve fertility for women delaying childbearing for career or educational advancement
To preserve fertility for women delaying childbearing because they do not believe that they are financially secure enough to raise a child
In the following analysis, the responses “Agree” and “Strongly Agree” were combined and referred to as responses in support of the statement, and the responses “Disagree” and “Strongly Disagree” were combined and referred to as responses not supporting the statement. At the conclusion of the survey, participants were invited to provide free-text comments on any other factors that were important to them regarding EF. The comments were further analysed to identify those that related to EF access.
Participants
The survey was open to residents of Australia aged between 18 and 60 years. The age range selected was to include those currently in their reproductive lifespan, and those who had passed their reproductive years but could have accessed ARTs in their lifetime. This paper reports on data from females who reside in the state of Victoria. While we received a small number of responses from all states and territories in Australia and from people identifying as a gender other than female, the number of responses was too low for meaningful comparisons and they have been excluded.
Statistical analysis
Data were summarised using frequencies and percentages. Socioeconomic status was measured using Socio-Economic Indexes for Areas (SEIFA) developed and designed by the Australian Bureau of Statistics.Citation31 SEIFAs are indices that rank geographic areas on a scale of 1–10 according to socioeconomic advantage and disadvantage, taking into account factors such as income levels, unemployment levels and educational attainment. This study applied the Australian Bureau of Statistics disadvantage indices: the higher the score the lower level of disadvantage.Citation32
The association between participants’ attitudes towards medical EF and their demographics or parenting intentions and experiences were assessed using Chi-squared tests. The relationship between non-medical EF and participant demographics was established using logistic regression adjusting for age, highest level of education, relationship status and socioeconomic status, and results were reported as Odds Ratios (OR) with their 95% confidence intervals (CI). Models for the relationship between parenting intentions and experiences, and attitudes towards non-medical EF were adjusted for age, highest level of education and relationship status, as they were deemed the most likely to confound the relationship, based on the unadjusted analyses. Analyses were conducted using Stata Statistical Software version 15 (StataCorp. 2017. College Station, TX: StataCorp LL).
Free-text comments collected from the final open-ended question were uploaded into NVivo version 12 (NVivo qualitative data analysis Software; QSR International Pty Ltd. Version 12, 2018). NVivo allowed for keyword searching and thematic analysis, as described by Braun and Clarke,Citation33 was used to identify common themes across participants’ comments. This process involved assigning codes to represent features of each data entry. Once the dataset was coded, the resulting codes were then grouped into broader themes. The themes were then reviewed to ensure they were representative of the codes and allocated a name. A report of the themes, with a selection of representative extracts was produced and reviewed by co-authors.
Ethical approval
The research study was approved by the Monash University Human Research Ethics Committee on the 9th March 2018 (project number 10843).
Results
A total of 1,066 females initiated the survey. From these, 410 were excluded from analysis as they either initiated the survey but did not enter any further data or did not reside within the geographical area of interest, which left 656 participants.
Demographics
Demographic data for the participants are outlined in . The median age of the sample was 28 years and most participants were of high socio-economic status. The majority of participants identified as heterosexual women (87%) and at the time of the survey, about a quarter of participants were single and about half were either living with a partner or married. Approximately two thirds of participants were not affiliated with any religion (65%). Participants were almost evenly distributed across education levels, and approximately three quarters were employed (full time and part time).
Table 1. Demographics and parenting intentions and experiences from an online survey of women aged 18–60 years
Parenting intentions and experiences
Participants’ parenting intentions and experiences are reported in . Most participants were childless (76%) and the majority (89%) had a secondary experience with infertility, i.e. they indicated that they knew someone who had difficulty conceiving or who had experience with ARTs, including EF. Half of the participants (53%) reported that having a biologically related child is important to them and a similar proportion either had or wanted 1–2 children (56%). When asked their views about the maximum age that a woman should attempt to conceive, carry and give birth to a child, half the respondents indicated over the age of 40 years, and approximately three quarters considered the ideal age for a woman to conceive their first child to be <30 years.
Attitudes towards medical EF
Overall, there was unanimous support (98%) for access to EF for situations where medical treatments or illnesses threaten fertility. There was no significant relationship between age, education level, relationship status or socio-economic status and support for both examples of medical EF. Similarly, there was no significant relationship between parenthood, secondary experience with infertility, number of desired children, importance of having biological children or the ideal age a woman should conceive their first child, and level of support for medical EF. While there was a significant difference in support for medical EF between participant opinions of the perceived oldest age a woman should conceive a child, the level of support did not drop below 96% in either subgroup ().
Table 2. Support for access to egg freezing for medical reasons by participant’s demographic characteristics and parenting intentions and experiences
Attitudes towards non-medical EF
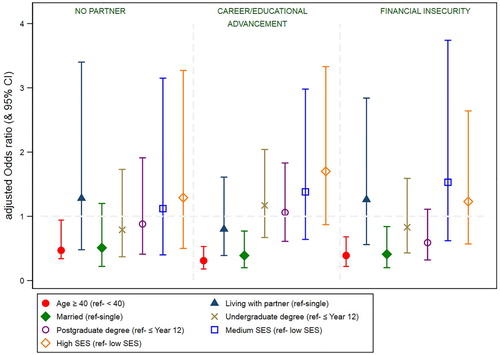
In relation to access to EF for non-medical risks to fertility, there was strong support (≥65%) for all indications among the respondents; “lack of suitable partner” was the highest supported indication (75%), followed by “financial insecurity” (72%) and “career/educational advancement” (65%). Several participants were undecided on whether EF should be available for non-medical risks to fertility (16.9%, 15.7% and 18.8%, respectively). There was no significant relationship between education level or socio-economic level and attitudes towards non-medical EF. There were varied levels of support for non-medical EF across age groups and marital status (). Respondents who were aged ≥40 years were less likely to support EF for lack of suitable partner (65% vs. 77%, OR: 0.47, 95% CI: 0.24–0.94, p = 0.032), career/educational advancement (45% vs 69%, OR: 0.31, 95% CI: 0.18–0.53, p < 0.001) and financial insecurity (52% vs 77%, OR: 0.39, 95% CI: 0.22–0.68, p = 0.001) than respondents who were <40 years. Similarly, married respondents were less likely to support EF for career/educational advancement (55% vs 72%, OR: 0.39, 95% CI: 0.20–0.77, p = 0.007) and financial insecurity (60% vs 77%, OR: 0.41, 95% CI: 0.20–0.84, p = 0.014) than respondents who were single.
Figure 1. The relationship between non-medical egg freezing (EF) and participant demographics. Symbols represent the adjusted Odds Ratio (OR) and the bars indicate the 95% confidence intervals. The OR were adjusted for age, highest level of education, relationship status and socioeconomic status
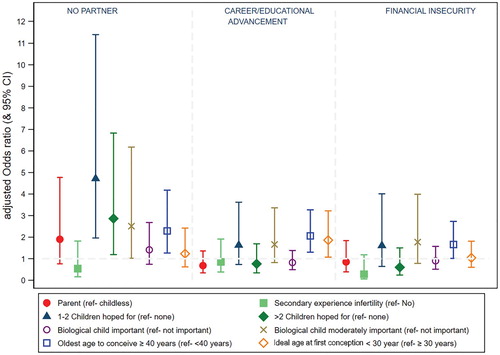
presents the relationship between parenting intentions and experiences, and respondents’ attitudes towards non-medical EF. Participants who indicated ≥40 years as the oldest age a woman should try to conceive a child, were significantly more likely to support all indications for non-medical EF than those who believed this age should be <40 years (lack of suitable partner: 79% vs 71%, OR: 2.29, 95% CI: 1.26–4.18, p = 0.007; financial insecurity: 74% vs 69%, OR: 1.66, 95% CI: 1.01–2.73, p = 0.047; career/educational advancement: 70% vs 59%, OR: 2.06, 95% CI: 1.30–3.27, p = 0.002). Perceiving <30 years as the ideal age to first conceive, considering having biologically related children as moderately important and desiring one or more children were all significantly associated with increased support for different indications for non-medical EF (). Compared with those who did not want a child, participants who hoped for 1–2 children were almost five times more likely to be supportive of non-medical EF for “lack of suitable partner” (80% vs. 68%, OR: 4.72, 95% CI: 1.96–11.40, p = 0.001). While the likelihood was lower for those who wanted more than two children, support for non-medical EF for “lack of suitable partner” was still twice higher than that of participants who did not want children (80% vs. 68%, OR: 2.86, 95% CI: 1.19–6.83, p = 0.018). There was no significant relationship between parenthood, or secondary experience of infertility, and support for all examples of non-medical EF.
Figure 2. The relationship between non-medical egg freezing (EF) and participant parenting intentions and experiences. Symbols represent the adjusted Odds Ratio (OR) and the bars indicate the 95% confidence intervals. The ORs for the relationship between parenting intentions and experiences, and attitudes were adjusted for age, highest level of education and relationship status
Open text findings
In the additional comments section provided at the end of the survey, thoughts or concerns related to EF access were identified and summarised into three broad themes: Reasons for who should have access to EF, Women’s autonomy and informational needs and Cost is a barrier.
Reasons for who should have access to EF
Participants offered a variety of reasons to explain their views about when access to EF should be allowed. While some participants supported universal access: “everyone should have access to fertility treatments, including EF”, others suggested priority should be given to those who face medical treatments or illnesses that may render them infertile. As explained by one participant: “for those with conditions or health concerns that threaten fertility, [they] should have the human right to sustain their eggs in any which way they see fit”. Another participant elaborated: “[EF should] only be used if there is a genuine medical reason not to put your career first because that is a choice not a necessity”. Some participants explained that the risks associated with EF procedures and the “unknown factors like the impacts on the children conceived”, prevented them from supporting non-medical EF.
Women’s autonomy and informational needs
Many participants in the study highlighted the importance of reproductive autonomy. As explained by one participant: “it’s all about giving women options and the power to choose when and which stage of their lives they would like to get pregnant”. Another participant elaborated: “women should be supported with whatever choices that they feel they need to make”. However, many participants alluded to an informational barrier to EF, with one participant claiming, “despite personal and family history of fertility issues I learnt most of what I know about [EF] from this survey”. Another participant reflected on their own experience with infertility: “if I knew 10 years ago what I know now, I would have frozen my eggs. I thought I had all the time in the world”. Participants called for “more information” and “increased awareness and knowledge” to support women “to make an informed decision”.
Cost is a barrier
The cost of EF was addressed extensively, with many participants linking accessibility with affordability: “cost is the limiting factor. It needs to be more affordable”. Participants reflected on their own experiences: “I’ve never looked into [EF] as it has always seemed like an unattainable, expensive procedure”. Another participant commented: “career driven friends and I have discussed [EF] as a future option for us, however the extraordinary costs is a significant barrier”. One participant expressed their belief that “any woman should have [EF] available to them at a reasonable cost”, since, as reasoned by another participant: “ … having children is very important to most women”.
Discussion
To our knowledge, this is the first Australian study to explore views about access to egg freezing. We surveyed a self-selected group of women from Victoria, Australia about their views on whether EF should be permitted for medical and non-medical reasons and examined the influence of demographics and parenting intentions and experiences on opinions of EF. The level of support for medical EF was at least 94% across all demographic subgroups, with only minor differences in support seen between the perceived oldest age a woman should conceive a child. In contrast, there was considerable variation in support for non-medical EF across participant demographic groups; younger age (<40 years) and considering ≥40 years to be the oldest age a woman should conceive a child, were significantly associated with increased support for all three indications for non-medical EF.
Our results suggest there is stronger support overall for medical EF than there is for non-medical EF. This is consistent with the findings of previous studies; a recent study from Sweden that surveyed women aged 30–39 years on the acceptability of medical and non-medical EF also found that there was stronger support for medical EF than there was for non-medical EF (94% vs. 70%, respectively).Citation27 Similarly, a Canadian study reported that 91.4% of the childless women they surveyed were supportive of medical EF, whereas only 66% of them supported non-medical EF.Citation23 This variation in support suggests that medical and non-medical indications for EF are perceived differently and that medical reasons are judged to be more acceptable reasons for seeking access to EF.
While support for medical EF appeared to be independent of the possible reasons for seeking medical EF (97.9% and 97.7% in support for EF due to treatment and illness, respectively), support for non-medical EF was dependent on the reason it was sought. Our results are consistent with those of a UK-Danish study that surveyed women aged 18–68 years and reported less support for non-medical EF when it is sought to delay parenting to allow career advancement or further education (66%, cf. 65% in our study) and more support for EF when it is sought because of the lack of suitable partner (85%, cf. 75% see in our study).Citation24 In contrast, an American study that surveyed men and women aged 18–65 years, reported non-medical EF for “career/educational advancement” was the highest supported (72.1%) indication for EF amongst the other reasons for seeking non-medical EF (lack of partner: 63%, financial insecurity: 58%).Citation25
The variation in support for the different indications of non-medical EF suggests that participants did not consider the indications for non-medical EF to be analogous. Findings from the analysis of qualitative data suggest a possible explanation for the diminished support EF for “career/educational advancement” received in our study. As explained by one participant, EF for “career/education advancement” “ … is a choice not a necessity”. Our findings add support to a view reported in the literature suggesting that EF is more acceptable when it is sought for reasons that are related to misfortune or beyond an individual’s control (e.g. a cancer diagnosis, or not having a partner) as opposed to reasons that are perceived to be a lifestyle choice (e.g. for career or educational goals).Citation34 As elaborated by Mertes,Citation35 the negative portrayal of the “careerist woman” choosing to delay bearing children to focus on her career, presents the decision to access EF as an egoistic choice.
Views about the permissibility of EF for career building are concerned with women’s reproductive choices and which choices are justifiable. In her discussion on reproductive choices, PetropanagosCitation36 argues that women’s childbearing decisions cannot be considered in isolation from their social environment. PetropanagosCitation36 reasons there are many obstacles in the education sector and in the workplace that influence women’s childbearing decisions. Such obstacles could include: the cost and availability of childcare options,Citation37 the structure of parental leave policies,Citation38 or whether a workplace offers flexible working arrangements.Citation39 Indeed, studies indicate that highly educated women are more likely to have children later in life and not reach their desired family size.Citation40 Further, women report that the support or lack of support that pregnant women receive in their workplace influences their decision about when they may have children.Citation41 Therefore, considering the barriers women face in the workplace, their decision to seek EF may be more multifaceted than simply a preference for career progression and delayed childbearing.
Furthermore, as MertesCitation35 argues, the emerging demographic profile of the women accessing non-medical EF does not support the notion that women are seeking EF so that they can delay parenthood to continue to build their careers. Current research supports Mertes’s argument and shows that most of the women accessing EF are doing so in their late 30s and identify as wanting children but not having found a partner yet.Citation9–12 Further, analysis of data collected through qualitative interviews found that women view EF as their best option to allow more time to find a partner, while also conserving their chances of genetic parenthood in the future.Citation42 This suggests that when women access EF, they are motivated by a diminished ovarian reserve and a desire for genetic parenthood, rather than by a preference for career advancement over having children. It is, however, important to note that while EF may temporally reassure women, the risk of failed treatment and the implications of shifting the timing of childbearing raise ethical concerns that require further consideration. Further research is required to explore people's attitudes towards non-medical EF, in particular to clarify reasons that might explain the variation in support for different indications for non-medical EF and also to understand the ambivalence towards non-medical EF, as indicated by the small group of participants who were undecided on whether access should be permitted.
The current study revealed that participants share two other concerns about EF. Firstly, many participants alluded to an informational barrier, indicating that the lack of public awareness of EF could prevent women from accessing this technology. The claim that women are unfamiliar with EF is not surprising as many studies have identified that people of reproductive age have a poor understanding of fertility and of the capacity of ARTs to overcome problems with infertility.Citation5,Citation23,Citation43–45 In addition, the information available to individuals through ART clinic websites may not be accessible to the lay public. Recent audits of ART clinic websites indicated the quality of information provided is poor and often not up to industry standards.Citation46,Citation47 In some cases, information on treatments and success rates was considered misleading and was found to aggressively market some ART procedures,Citation48 including non-medical EF.Citation49 Our findings provide further evidence of the need to improve the quality of the resources on fertility and fertility preservation.
Secondly, while most of our participants supported access to EF, many noted the costs of EF are prohibitive. In Australia, EF costs approximately AU$10,000 per cycle.Citation50 For individuals with a medical indication for EF a rebate is available through the publicly funded health care system, Medicare.Citation51 However, women seeking non-medical EF are not eligible to receive the rebate and must self-fund the costs. Therefore, while all women are theoretically able to request EF, unequal funding and the high procedural costs of EF effectively exclude people who cannot afford the procedure. The issue of affordability is relevant to many ARTs, where the associated costs are an insuperable barrier to accessing treatment.Citation51 The report from the recent review into ART legislation in Victoria recommended the establishment of public ART services to support those who face financial difficulties to access fertility treatments in the private sector.Citation21 While it is unclear whether a public clinic would offer non-medical EF, the establishment of publicly funded clinics is one step to broaden access to ART services. Other possibilities include a discussion of whether public funding, via medical benefits, should be extended to include both medical and non-medical EF.
Limitations
The online format of the survey, and the predominant use of online recruitment may have limited the number of people who could access the survey. In addition, the participants self-selected their involvement in this study and, therefore, the views reported may not be representative of all Victorian women. However, this study was not seeking to be representative, but rather to provide a snapshot of the opinions of interested individuals on access to EF and to collect data that were previously unknown in Australia. It is possible that the results contain a selection bias in favour of EF, because people interested in, or experienced with, infertility might be more likely to respond positively to new ARTs. Further, while experience with pregnancy complications, infertility or ARTs may influence participant responses, these data were not collected. Future research could explore the influence gravidity, parity and other factors such as sexuality have on opinions towards EF.
Conclusion
Results from this research add to the limited data on the public’s attitudes towards EF and their views about when access to EF should be permitted. Our findings concur with previous studies and social commentaries suggesting that there is widespread support for EF; however, there is more support for medical EF than there is for non-medical EF. Further, the findings suggest that people do not consider the possible reasons for requiring non-medical EF to be analogous as support for each reason varied. The current surge of interest in EF requires careful policy responses that consider cultural, demographic and financial determinants which influence ART usage. Further research is required to consider the ethical implications of increased reliance on EF as well as the implications and potential risks of postponing childbearing till later years. Current research is under way to explore funding options for EF and the ethical issues associated with the rationing of EF funding based on medical and non-medical distinctions.
Author contributions
MJ, GF, NMR and SC contributed to the conception and design of the study. MJ was responsible for data collection, and MJ and SMG conducted data analysis. MJ drafted the manuscript and all authors reviewed and contributed to the final version.
Acknowledgements
Thank you to Judith Daniluk and Emily Koert for providing the initial questionnaire used to structure our study. Thank you to the staff at the Office of Strategic Marketing and Communications at Monash University for their assistance with recruitment material. Finally, thank you to all the participants in the study for giving their time and sharing their views.
Disclosure statement
No potential conflict of interest was reported by the author(s).
ORCID
Molly Johnston http://orcid.org/0000-0002-3786-0843
StellaMay Gwini http://orcid.org/0000-0002-0295-4575
Sally Catt http://orcid.org/0000-0002-7604-4507
Additional information
Funding
References
- OECD Family Database. (2018). SF2.3: age of mothers at childbirth and age-specific fertility. [cited 2019 Jun 12]. Available from: https://www.oecd.org/els/soc/SF_2_3_Age_mothers_childbirth.pdf.
- Australian Bureau of Statistics. (1999). Australian fertility continues to decline – ABS. [cited 2018 Nov 6]. Available from: http://www.abs.gov.au/ausstats/[email protected]/mediareleasesbyTopic/B4DC277C919906B8CA2568A900136367?OpenDEFument.
- Australian Bureau of Statistics. (2018). Births registered, summary statistics for Australia(a). [cited 2018 Dec 20]. Available from: http://www.abs.gov.au/AUSSTATS/[email protected]/mf/3301.0.
- Hammarberg K, Clarke VE. Reasons for delaying childbearing – a survey of women aged over 35 years seeking assisted reproductive technology. Aust Fam Physician. 2005;34:187–188. 206.
- Hickman LC, Fortin C, Goodman L, et al. Fertility and fertility preservation: knowledge, awareness and attitudes of female graduate students. Eur J Contracept Reprod Health Care. 2018;23:130–138. doi: 10.1080/13625187.2018.1455085
- Cooke L, Nelson SM. Reproductive ageing and fertility in an ageing population. Obstet Gynaecol. 2011;13:161–168.
- Steiner AZ, Jukic AMZ. Impact of female age and nulligravidity on fecundity in an older reproductive age cohort. Fertil Steril. 2016;105:1584–1588. doi: 10.1016/j.fertnstert.2016.02.028
- Cobo A, Domingo J, Perez S, et al. Vitrification: an effective new approach to oocyte banking and preserving fertility in cancer patients. Clin Transl Oncol. 2008;10:268–273. doi: 10.1007/s12094-008-0196-7
- Baldwin K, Culley L, Hudson N, et al. Running out of time: exploring women’s motivations for social egg freezing. J Psychosom Obstet Gynaecol. 2018;40:1–8.
- Inhorn MC, Birenbaum-Carmeli D, Birger J, et al. Elective egg freezing and its underlying socio-demography: a binational analysis with global implications. Reprod Biol Endocrinol. 2018;16:70. doi: 10.1186/s12958-018-0389-z
- Pritchard N, Kirkman M, Hammarberg K, et al. Characteristics and circumstances of women in Australia who cryopreserved their oocytes for non-medical indications. J Reprod Infant Psychol. 2017;35:108–118. doi: 10.1080/02646838.2016.1275533
- Stoop D, Maes E, Polyzos NP, et al. Does oocyte banking for anticipated gamete exhaustion influence future relational and reproductive choices? A follow-up of bankers and non-bankers. Hum Reprod. 2015;30:338–344. doi: 10.1093/humrep/deu317
- Balkenende EME, Dahhan T, Van Der Veen F, et al. Reproductive outcomes after oocyte banking for fertility preservation. Reprod Biomed Online. 2018;37:425–433. doi: 10.1016/j.rbmo.2018.07.005
- Gürtin ZB, Shah T, Wang J, et al. Reconceiving egg freezing: insights from an analysis of 5 years of data from a UK clinic. Reprod BioMed Online. 2018;38:272–282. doi: 10.1016/j.rbmo.2018.11.003
- Human Fertilisation & Embryology Authority. (2018). Egg freezing in fertility treatment London. [cited 2018 Nov 15]. Available from: https://www.hfea.gov.uk/media/2656/egg-freezing-in-fertility-treatment-trends-and-figures-2010-2016-final.pdf.
- Shenfield F, De Mouzon J, Scaravelli G, et al. Oocyte and ovarian tissue cryopreservation in European countries: statutory background, practice, storage and use. Hum Reprod Open. 2017; 1.
- Tan SQ, Tan AW, Lau MS, et al. Social oocyte freezing: a survey among Singaporean female medical students. J Obstet Gynaecol Res. 2014;40:1345–1352. doi: 10.1111/jog.12347
- Calhaz-Jorge C, De Geyter CH, Kupka MS, et al. (2020). Survey on ART and IUI: legislation, regulation, funding and registries in European countries: The European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Human Reproduction Open, (supplement 1).
- Beit-Or MY. (2011). From now on: any woman aged 30-41 can freeze an egg [in Hebrew]. [cited 2019 Jul 10]. Available from: https://www.ynet.co.il/articles/0,7340,L-4015199,00.html.
- The Practice Committees of the American Society for Reproductive Medicine and the Practice Committee of the Society for Assisted Reproductive Technology. Ovarian tissue and oocyte cryopreservation. Fertil Steril. 2008;90:241–246. doi: 10.1016/j.fertnstert.2008.05.007
- Gorton M. (2019). Helping Victorians create families with assisted reproductive treatment: Final report of the Independent Review into Assisted Reproductive Treatment. 2019. Melbourne: The Victorian Government. Available from: https://www2.health.vic.gov.au/hospitals-and-health-services/patient-care/perinatal-reproductive/assisted-reproduction/regulatory-review.
- Althaus C, Bridgman P, Davis G. Consultation. The Australian policy handbook. 6th ed. Crows Nest: Allen & Unwin; 2018.
- Daniluk JC, Koert E. Childless women’s beliefs and knowledge about oocyte freezing for social and medical reasons. Hum Reprod. 2016;31:2313–2320. doi: 10.1093/humrep/dew189
- Lallemant C, Vassard D, Nyboe Andersen A, et al. Medical and social egg freezing: internet-based survey of knowledge and attitudes among women in Denmark and the UK. Acta Obstet Gynecol Scand. 2016;95:1402–1410. doi: 10.1111/aogs.13024
- Lewis EI, Missmer SA, Farland LV, et al. Public support in the United States for elective oocyte cryopreservation. Fertil Steril. 2016;106:1183–1189. doi: 10.1016/j.fertnstert.2016.07.004
- O’brien Y, Martyn F, Glover LE, et al. What women want? A scoping survey on women’s knowledge, attitudes and behaviours towards ovarian reserve testing and egg freezing. Eur J Obstet Gynecol Reprod Biol. 2017;217:71–76. doi: 10.1016/j.ejogrb.2017.08.024
- Wennberg AL, Rodriguez-Wallberg KA, Milsom I, et al. Attitudes towards new assisted reproductive technologies in Sweden: a survey in women 30–39 years of age. Acta Obstet Gynecol Scand. 2016;95:38–44. doi: 10.1111/aogs.12781
- Hammarberg K. (2017). Victoria’s world-first change to share sperm or egg donor’s names with children. [cited 2019 Dec 2]. Available from: https://theconversation.com/victorias-world-first-change-to-share-sperm-or-egg-donors-names-with-children-72417.
- Johnson L. (2019). Removing donor anonymity retrospectively in Victoria, Australia – two years on. 2019. [cited 2019 Dec 2]. Available from: https://www.bionews.org.uk/page_142862.
- Johnston M, Richings N, Catt S, et al. (2019). Freezing for future fertility: does the Australian public support oocyte cryopreservation? In: Abstracts of the 35th Annual Meeting of the European Society of Human Reproduction and Embryology, Hum Reprod; 34: Issue Supplement_1: i349.
- Australian Bureau of Statistics. (2013a). IRSD. [cited 2019 Apr 5]. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/2033.0.55.001main+features100052011.
- Australian Bureau of Statistics. (2013b). Census of population and housing: SEFio-Economic Indexes for Areas (SEIFA), Australia, 2011, cat. No. 203.0.55.001. [cited 2019 Apr 5]. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/2033.0.55.001main+features100132011.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi: 10.1191/1478088706qp063oa
- Sándor J, Vicsek L, Bauer Z. Let us talk about eggs! Professional resistance to elective egg vitrification and gendered medical paternalism. Med Health Care Philos. 2018;21:311–323. doi: 10.1007/s11019-017-9805-y
- Mertes H. The portrayal of healthy women requesting oocyte cryopreservation. Facts Views Vis ObGyn. 2013;5:141–146.
- Petropanagos A. Reproductive “choice” and egg freezing. Cancer Treat Res. 2010;156:223–235. doi: 10.1007/978-1-4419-6518-9_17
- Daley J, Mcgannon C. Submission to the productivity commission inquiry on childcare and early childhood learning. Carlton: Grattan Institute; 2014.
- Productivity Commission. Paid parental leave: support for parents with newborn children. Canberra, Australia; 2009.
- Flexcareers. (2016). Australian working mothers cry out for flexible working arrangements. [cited 2019 Oct 14]. Available from: https://blog.flexcareers.com.au/2016/01/22/australian-working-mothers-cry-out-for-flexible-working-arrangements/.
- Rendall M, Aracil E, Bagavos C, et al. Increasingly heterogeneous ages at first birth by education in Southern European and Anglo-American family-policy regimes: A seven-country comparison by birth cohort. Popul Stud (Camb). 2010;64:209–227. doi: 10.1080/00324728.2010.512392
- Metcalfe A, Vekved M, Tough S. Educational attainment, perception of workplace support and its influence on timing of childbearing for Canadian women: a cross-sectional study. Matern Child Health J. 2014;18:1675–1682. doi: 10.1007/s10995-013-1409-4
- Waldby C. “Banking time”: egg freezing and the negotiation of future fertility. Cult Health Sex. 2015;17:470–482. doi: 10.1080/13691058.2014.951881
- Boivin J, Sandhu A, Brian K, et al. Fertility-related knowledge and perceptions of fertility education among adolescents and emerging adults: a qualitative study. Hum Fertil (Camb). 2018;10:1–9.
- Pedro J, Brandão T, Schmidt L, et al. What do people know about fertility? A systematic review on fertility awareness and its associated factors. Ups J Med Sci. 2018;123:71–81. doi: 10.1080/03009734.2018.1480186
- Prior E, Lew R, Hammarberg K, et al. Fertility facts, figures and future plans: an online survey of university students. Hum Fertil. 2018;30:1–8.
- Avraham S, Machtinger R, Cahan T, et al. What is the quality of information on social oocyte cryopreservation provided by websites of Society for Assisted reproductive technology member fertility clinics? Fertil Steril. 2014;101:222–226. doi: 10.1016/j.fertnstert.2013.09.008
- Morris M. (2016). IVF industry criticised for “misleading claims, aggressive marketing”. [cited 2019 Oct 8]. Available from: http://www.abc.net.au/news/2016-02-09/ivf-industry-criticised-over-\misleading-claims’/7152508.
- ACCC. (2016). IVF “success rate” claims under the microscope. [cited 2019 Oct 8]. Available from: https://www.accc.gov.au/media-release/ivf-success-rate-claims-under-the-microscope.
- Mohammadi L, Aranda D, Martínez-Martínez S. The narratives of fertility clinic’s websites in Spain. El Profesional de la Información. 2019;28:1–13.
- Bowden T. (2015). Fertility doctors warn women not to leave it too late to freeze eggs for IVF, even though science is improving odds. [cited 2019 Nov 20]. Available from: https://www.abc.net.au/news/2015-05-15/fertility-doctors-warn-women-not-to-leave-it-too-late-to-freeze/6473282.
- Harris K, Burley H, Mclachlan R, et al. Socio-economic disparities in access to assisted reproductive technologies in Australia. Reprod Biomed Online. 2016;33:575–584. doi: 10.1016/j.rbmo.2016.07.012