
Abstract
Unmet need for family planning (FP) remains prevalent worldwide. In Tanzania, 21.7% of women desire to delay pregnancy, but do not use modern contraception despite its free availability at local clinics. Our prior data suggest that this is related to complex gender and religious dynamics in rural communities. To understand how education about FP could be improved, we developed a discrete choice experiment (DCE) to rank preferences of six attributes of FP education. Results were stratified by gender. Sixty-eight women and 76 men completed interview-assisted DCEs. Participants significantly preferred education by a clinician (men = 0.62, p < .001; women = 0.38, p < .001) and education in mixed-gender groups (men = 0.55, p < .001; women = 0.26, p < .001). Women also significantly preferred education by a religious leader (0.26, p = .012), in a clinic versus church, mosque, or community centre (0.31, p = .002), and by a female educator (0.12, p = .019). Men significantly preferred a male educator (0.17, p = .015), whom they had never met (0.25, p < .001), and educating married and unmarried people separately (0.22, p = .002). Qualitative data indicate women who had not previously used contraception preferred education led by a religious leader in a church or mosque. FP education tailored to these preferences may reach a broader audience, dispel misconceptions about FP and ultimately decrease unmet need.
Résumé
Les besoins en planification familiale demeurent largement insatisfaits dans le monde entier. En République-Unie de Tanzanie, 21.7% des femmes souhaitent retarder leur grossesse, mais n’utilisent pas de contraception moderne même si elle est disponible gratuitement dans les dispensaires locaux. Nos précédentes données suggèrent que c’est dû à des dynamiques sexospécifiques et religieuses complexes dans les communautés rurales. Pour comprendre comment il serait possible d’améliorer l’éducation en matière de planification familiale, nous avons mis au point une expérience de choix discrets (ECD) pour classer les préférences de six attributs de l’éducation sur la planification familiale. Les résultats ont été stratifiés par genre. Soixante-huit femmes et 76 hommes ont achevé l’ECD. Les participants préféraient sensiblement l’éducation donnée par un clinicien (hommes = 0.62, p < .001; femmes = 0.38, p < .001) et dans les groupes mixtes (hommes = 0.55, p < .001; femmes = 0.26, p < .001). Les femmes préféraient aussi nettement l’éducation prodiguée par un responsable religieux (0.26, p = .012), dans un dispensaire plutôt qu’une église, mosquée ou centre communautaire (0.31, p = .002), et par une éducatrice (0.12, p = .019). Les hommes préféraient de manière significative un éducateur masculin (0.17, p = .015), qu’ils n’avaient jamais rencontré (0.25, p < .001), et qui informait séparément les personnes mariées et célibataires (0.22, p = .002). Les données qualitatives indiquent que les femmes qui n’avaient pas utilisé précédemment de contraception préféraient être informées par un responsable religieux dans une église ou une mosquée. Une éducation en matière de planification familiale adaptée à ces préférences peut atteindre un public plus large, dissiper les idées erronées sur la contraception et, en fin de compte, diminuer les besoins insatisfaits.
Resumen
La necesidad insatisfecha de planificación familiar (PF) continúa siendo frecuente a nivel mundial. En Tanzania, el 21.7% de las mujeres desean retrasar el embarazo, pero no usan anticoncepción moderna a pesar de que está disponible gratuitamente en las clínicas locales. Nuestros datos anteriores indican que esto se debe a complejas dinámicas de género y religión en las comunidades rurales. Para entender cómo puede mejorarse la educación sobre PF, creamos un experimento de elección discreta (EED) para clasificar las preferencias de seis atributos de la educación sobre PF. Los resultados fueron estratificados por género: 68 mujeres y 76 hombres realizaron el EED asistido por entrevistas. Los participantes prefirieron de manera significativa la educación por un profesional clínico (hombres = 0.62, p < .001; mujeres = 0.38, p < .001) y en los grupos integrados por personas de ambos géneros (hombres = 0.55, p < .001; mujeres = 0.26, p < .001). Las mujeres también prefirieron de manera significativa la educación por un líder religioso (0.26, p = .012), en una clínica versus iglesia, mezquita o centro comunitario (0.31, p = .002), y por una educadora (0.12, p = .019). Los hombres prefirieron de manera significativa un educador (0.17, p = .015), que nunca habían conocido (0.25, p < .001), y educar a las personas casadas y a las solteras por separado (0.22, p = .002). Los datos cualitativos indican que las mujeres que no habían usado anticoncepción anteriormente preferían la educación por un líder religioso en una iglesia o mezquita. La educación sobre PF personalizada según estas preferencias posiblemente llegue a un público más amplio, disipe conceptos erróneos sobre PF y a la larga disminuya la necesidad insatisfecha.
Introduction
Pregnancy spacing can decrease unnecessary deaths of women and children. Interpregnancy intervals shorter than 18 months are associated with increased adverse pregnancy outcomes, including higher maternal mortality among older mothers and increased foetal and infant risks among young mothers.Citation1 Modern contraceptives allow mothers to space childbirth, making pregnancy safer. They also help people to achieve their desired family size and space their children for economic and other reasons. Recognising these benefits, the United Nations’ Sustainable Development Goals (SDGs) therefore include universal access to family planning (FP).Citation2 However, unmet need for FP, defined as lack of modern contraceptive use by a fertile, sexually active woman who does not want to get pregnant within the next two years, is prevalent around the world, affecting 11.5% of all women of reproductive age.Citation2 In Africa, the percentage of women reporting unmet need for FP is more than doubled, at 24.2%.Citation3
Lack of knowledge about FP methods and fear of both life-threatening and non-life-threatening side effects have been cited as primary reasons for non-use of FP.Citation4 Most modern forms of contraception have side effects that can be a barrier to adoption or a cause for discontinued use, but there is a strong distinction between actual and perceived side effects, with the latter often based on misinformation which unnecessarily deters use.Citation5 There is a multi-stage process for addressing barriers to FP use with the ultimate goal of decreasing unmet need for FP. Accessible, acceptable, and accurate education is the first step in this process because it can directly address both lack of knowledge and misinformation about side effects. Equipped with knowledge of FP, individuals can then opt into a form of modern contraception, allowing them to gain greater control over family size and child spacing.
Unmet need is particularly high in northwestern Tanzania where 34% of women report a desire to delay pregnancy but are not using modern contraception, despite its availability at local clinics free of charge.Citation6 Our research team previously reported that gender and religious dynamics in rural Tanzania impact women’s ability to make decisions about FP and that providing education within the context of these factors could increase FP uptake.Citation7 Additionally, Tanzania is a deeply religious country, with 93% of the population reporting religious faith as “very important” to them.Citation8 Related research shows women who regularly attend religious services are less likely to receive information about FP from health workers, which may be due to religious women not requesting such information or to provider bias toward women perceived to be religious.Citation9 Other common major barriers to uptake of modern contraception that are relevant to Tanzanian men and women include misinformation and the cultural deference to male authority.Citation5 There is an urgent need for improved FP education to address these barriers and thus allow individuals to reach the next stage of opting into modern methods of family planning. To our knowledge, no study has investigated FP educational preferences among men and women in sub-Saharan Africa.
This study utilises a discrete choice experiment (DCE) to elucidate and prioritise preferences for receiving FP education among Tanzanian men and women living in rural, highly religious communities. DCEs are particularly effective for challenging situations in which barriers to health services uptake, such as gender and religious faith, are vaguely defined and difficult to address. DCEs provide a methodology for parsing through the nuances of preference to understand which attributes of a service, in our case FP education, should be prioritised to address these barriers in an acceptable and useful way. This is because DCEs provide a quantitative framework rooted in economic theory of utility maximisation that highlights population preferences for a given service by asking participants to make choices between hypothetical alternative scenarios.Citation10
DCE methodology has been used to identify population preferences for characteristics of various health services, including FP, HIV testing and vaccines.Citation11–16 Several DCEs have focused on most desired characteristics of FP service providers and types of contraceptive methods in clinical settings.Citation11–14 Importantly, little is known about preferences for FP education, which is the first step in decreasing unmet need for FP as it precedes usage and could impel or impede uptake. Our goal was to use DCE methodology to determine the highest priorities regarding FP education among adults in rural Tanzania, ultimately in order to design and implement appealing, effective, and far-reaching FP educational programmes.
Methods
Setting
This study was conducted in three representative rural villages in the Mwanza region of Northwestern Tanzania, near Lake Victoria. Selected villages are located one to two hours outside of Mwanza City. In this region of Tanzania, over two-thirds of the population are Christian. Most adults of reproductive age in these villages are married. Current FP education in these villages is provided to women in clinics on a case-by-case basis.
Deriving the DCE
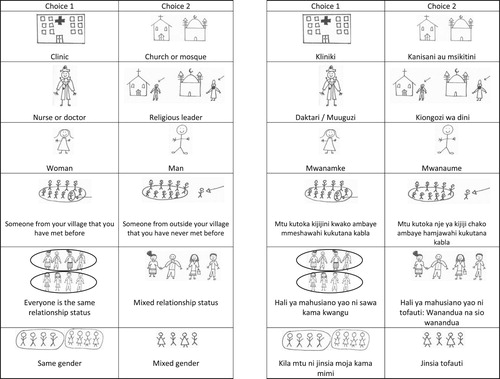
DCE development began with an analysis of 24 focus group discussions which were conducted among Christian and Muslim men and women in the Mwanza region of Tanzania between 2016 and 2017, as previously described.Citation8 Focus groups were separated by gender and religion and participants were asked broadly about their knowledge and perspectives regarding FP and the role of gender and religion in decision-making related to FP. Three study team members (BB, JD, LK) analysed transcripts of discussions to identify possible important attributes independently and then reached consensus by a group process, during which attributes were narrowed down from an initial list of 12 to a final 6. Plausible values for all final attributes, commonly known as attribute levels, were identified. Attribute levels considered all potential options for a given attribute without an opt-out choice. Accompanying images were designed to provide a pictorial representation of choice tasks and were pilot tested, refined, and re-tested with men and women in the Mwanza region.
The final attributes were: (1) where FP education takes place, (2) the profession of the educator, (3) the gender of the educator, (4) the relationship of the participant to the educator, (5) the relationship status of the other participants in the seminar, and (6) the gender of the other participants in the seminar ().
Table 1. Attributes and levels
Experimental design
The final experimental design included 2 attributes with 3 levels and 4 attributes with 2 levels, resulting in 144 possible attribute-level combinations (32 * 24). A full factorial design of this nature would include 10,296 choice sets. In order to limit the number of choice sets, a fractional factorial design was used, which allows for an estimate of preferences from a smaller number of choice sets. The final experimental design was generated using a D-efficient design with zero-priors in Ngene (d-error = 0.042).Citation17 DCE design was optimised for a conditional logit model with categorical terms for each attribute level. A total of 36 choice sets were developed in 3 blocks of 12 each.
Sample size calculations indicated N ≥ 500 * l/j * s where l is the maximum number of attribute levels, j is the number of alternatives in each choice set, and s is the number of tasks a participant will complete.Citation18 Given l = 3, j = 2 and s = 12, we obtain N ≥ 62.5, or 63 participants. We planned to stratify our results by gender, so to ensure adequate power, we calculated that we needed to enrol at least 126 total participants: 63 men and 63 women.
Study procedures
The DCEs were administered in August 2019 by four Tanzanian researchers who were university graduates with training in qualitative research methods, research ethics, and DCE administration. Researchers travelled to three rural villages for one week each. DCEs were administered one-on-one in participants’ local language, Kiswahili, which is spoken by >99% of people in the Mwanza region, and conducted in private locations out of earshot of other community members to ensure confidentiality. Results were recorded on paper. Adults of reproductive age (women aged 18–45 and men aged 18–60) were eligible for participation. Participants were purposively sampled to ensure that both sexes and a range of ages, religious denominations, and marital statuses were represented. Consent was read to each study participant at the beginning of the interview and participants were given sufficient time to ask questions before providing written informed consent. Visual acuity was assessed via a validated eye test using a pictorial eye chart administered by interviewers to ensure participants could clearly see the presentation of choice sets.Citation19 Participants were provided 10,000 Tanzanian shillings (approximately $US 4) for their time and participation. The participant reimbursement was comparable to other research conducted in this area and approved by the local IRB.
Relevant demographic data were collected by researchers, including information about education level, relationship status, and prior FP use. Participants were familiarised with an example choice set, in which researchers described attributes and levels and assisted the participant to ensure they understood the task. Example choice set data were not used in the final analysis. The example choice set was followed by 12 additional choice sets, each individually described by the researcher and visually depicted, as shown in . For each choice set, respondents were asked to choose which hypothetical scenario they preferred. Results were recorded by the researchers. Following the choice sets, participants were asked a series of open-ended questions about which attributes were most important to them and which levels they preferred.
Figure 1. Sample choice task
Data management and statistical analysis
Data was entered into REDCapTM (Research Electronic Data Capture) software at the end of each data collection day. Patterns of choices were analysed in Stata 15.1 (College Station, Texas) using gender-specific conditional logit models with dummy coded variables. Statistical significance of the interaction terms was assessed using Wald tests.
Results
Sample characteristics
Participant demographics
A total of 144 participants, 68 women and 76 men, were enrolled in this study. Characteristics of study participants are shown in . The majority of participants (71%) were married and participants had a median number of four children. Nearly all (91%) study participants identified as religious: 30.5% as Protestant, 32.6% as Catholic, and 25.6% as Muslim. All men (100%) and 48.5% of women reported earning their own money, primarily through agricultural work.
Table 2. Characteristics of study participants
Previous FP knowledge and usage
Three quarters (75%) of participants reported not wanting themselves or their partners to get pregnant in the next year, yet less than half (43.8%) reported that they or their sexual partner were currently using contraception (). Among participants who were currently using FP, the most common methods reported by men were the calendar method (35.5%; 11/31) and condoms (32.3%; 10/31), and the most common methods reported by women were injections (40.6%; 13/32) and implants (37.5%; 12/32). Among participants who previously used FP but were not currently using a method, 53.3% of men and 18.8% of women reported wanting to conceive as their primary reason for discontinued use and 13.3% of men and 50% of women reported negative side effects as their reason for discontinuation. A majority of participants (80%) wanted their partner to receive education about FP.
Table 3. Family planning knowledge and usage of study participants
Results of discrete choice experiment
shows results of gender-specific mixed logit models of participants’ stated choices across 3456 scenarios (144 participants * 12 choice tasks * 2 alternatives). The coefficients indicate the relative likelihood of choosing a scenario with that specific attribute level combination. A larger value indicates a higher likelihood of choosing that level, with p-value noting statistical significance. Our results indicate that men and women most preferred and second most preferred the same attribute-level combination.
Table 4. Results of conditional logit of discrete choice experiment
Among both men and women, an educational seminar led by a nurse or doctor (men = 0.618, p < .001; women = 0.383, p < .001) and a seminar with mixed-gender participants (men = 0.549, p < .001; women = 0.255, p < .001) were both significantly preferred attribute-level combinations. Women also significantly preferred an educational seminar in a clinic (0.31, p = .002), an educational seminar led by a religious leader (0.259, p = .012) and an educational seminar led by a woman educator (0.17, p = .019). Men’s significantly preferred attribute-level combinations included an educational seminar led by someone from outside their village whom they had never met before (0.249, p < .001), an educational seminar separating married and unmarried participants (0.215, p = .002), and an educational seminar led by a man (0.167, p = .015).
Participants’ responses to open-ended questions
Following completion of the DCE, when participants were asked directly about most important attributes, gender of participants was a common responses for both men (30%) and women (29%), in addition to profession of educator (men: 32%, women: 25%). A total of 79% of participants who said gender of participants was most important reported a preference for mixed-gender seminars, with many citing desire to have knowledge similar to their partners’, and the opportunity to learn more about the opposite gender. The remaining 21% who chose gender of participants as most important preferred to be educated separately by gender, saying that they would feel more comfortable to speak openly. Specifically, men expressed feeling intimidated asking questions about FP in front of women. The majority of participants who most highly prioritised a doctor or nurse educator stated it was because they are most knowledgeable about FP (36/41, 88%).
Location of education was identified as the most important attribute by 16.7% of participants (24/144). Nearly half of both men and women who most prioritised this attribute stated that a convenient, easily reachable location is vital (11/24, 45%). Many specifically noted that only women and people with illnesses attend the clinic and/or that a church or mosque is a better location for reaching men (7/11, 64%). Among Muslim participants, 37% preferred education in a mosque compared to 9% of Christian participants who preferred education in a church. Both groups noted this was because they wanted to learn in a respectful, holy place. Some participants (8/144, 6%), mostly men (6/8), said they preferred education from someone from outside their village whom they had never met before, both because they feel more comfortable talking openly and asking questions and because an outside educator is more exciting and they will pay closer attention. A higher percentage of women who had never used contraception reported education in a church (18%) or a religious leader as the educator (14%) as the most important attribute compared to women who had used contraception (6.5% and 0%, respectively).
When asked to describe important attributes of an educational FP seminar that were not listed on our DCE, 17% of respondents mentioned the importance of having frequent educational seminars. A respective 10% and 6% of respondents emphasised the importance of educating men and young people before they are married. Additionally, 8% of respondents specifically mentioned an interest in being educated about all different methods of contraception.
Discussion
Our novel application of DCE methodology elicited men’s and women’s preferences for the delivery of FP education in rural Tanzania and provides unique insights which could improve FP acceptance and effectiveness. In contrast to the typical provision of education by female nurses at local clinics, which reaches predominantly women, our data show that both men and women prioritise being educated by a knowledgeable educator in a setting that reaches all genders. Further, a sizeable minority of people, particularly those who had not previously used FP, prioritised being educated by a religious leader. These multiple strong preferences provide incisive guidance that could be used to transform the ways that education about FP is typically provided.
Both men and women had the strongest preference for a nurse or doctor as an educator. This finding is also supported by analysis of answers to open-ended questions, in which participants indicated that it is important to have a knowledgeable educator to ensure high quality education. Importance of participants’ perception of the educator was also shown in men’s significant preference for an educator from outside their village whom they have never met before. Men explained that an educator from outside the village would be viewed as an expert on the subject, so they would be more likely to pay attention and absorb material. They further indicated that an outside educator would allow them to ask questions without fear of judgement. Thus, an educator who is perceived as knowledgeable and non-judgmental by participants, such as a doctor or nurse from outside the village, is highly prioritised for FP education.
Men and women also preferred FP education presented to a mixed-gender group of participants. Both genders cited desire to have equal knowledge to their partner’s as the primary reason for wanting education in mixed groups, with particular emphasis on men’s need for FP education. This finding was reinforced in both our group’s previous reportCitation7 and in our current analysis of open-ended questions. Women explained that FP education most often occurs at clinics, which men do not attend because of gender roles, leaving men with less knowledge about FP despite their common role as the household’s decision-makers. These qualitative findings suggest that educating participants in an accessible, comfortable location for men could increase the number of men receiving FP education. Therefore, education in a neutral location would meet both men and women’s preferences. Beyond its importance to participants, couple-based education and increased spousal discussion has been shown to increase FP uptakeCitation20,Citation21 and to be more effective than education separated by gender.Citation22 Mixed-gender education would enable both partners to have equal perceived knowledge about family planning, thereby facilitating discussion and possibly shared decision-making.
Yet mixed-gender education was not uniformly prioritised by all. Some men voiced hesitation about asking personal questions in front of women. Also of note, both men and women significantly preferred an educator of their own gender, which would not be possible in a mixed-gender seminar. To avoid this discomfort and allow for an environment where participants can openly ask questions or share concerns, our results suggest that educating genders both together and separately could be beneficial. A hybrid educational seminar that provides mixed-gender education with break-out groups separated by gender and led by a leader of the same gender as the participants could respond to both of these priorities. Alternatively, providing several options of educational interventions, both mixed gender and separated by gender, could address these preferences.
Women who had not previously used FP reported greater interest in education in a church or mosque from a religious leader than in a clinic from a medical professional. These women may lack an understanding of FP and may be less concerned about details of FP than how it fits into the context of their lives from a religious, holistic perspective. Women who had previously used FP, in contrast, were concerned about potential side effects, with many of them citing this concern as their primary reason for discontinued use, despite continued interest in delaying pregnancy. Women with previous FP use are likely to have already received some form of FP education in clinics, and therefore have different opinions about what kind of education may be useful. Discontinued use of FP has been shown to be negatively associated with long-acting FP use, so targeting women who have stopped using FP is important and necessary in increasing FP uptake.Citation23–26 Education that contains a presentation of how different contraceptives work, typical side effects, and how to manage these side effects could help to reduce unmet need of FP, especially because fear of side effects is often based on misinformation and preparing women for side effects could reduce discontinuation.Citation5 Additionally, education that reaches women in the community before they opt into family planning at a clinic, could provide necessary context and information for women to decide about their child spacing. Effective, desired and comprehensive FP education should therefore provide an overview of FP and the ways it can be used, include details about methods and side effects, and be provided to women before they have made a decision about FP. This could either be done within one educational intervention or in a series of sessions.
Combining these multiple strongly preferred priorities, our results indicate that FP education that considers location, educator profession, and participants’ characteristics would be most effective. Education should take place in an accessible location, where both genders feel comfortable, and be led by educators perceived to be experts who are able to discuss details of specific FP methods. Education should provide time for men and women to learn together and for additional discussion separately. Given some participants’ comfortability with religious leaders, education provided by a team of leaders that includes both medical professionals and religious leaders may also be an innovative and effective approach. Of note, these suggestions could be used to create one educational intervention or alternatively could be used as guidance to develop sequential educational seminars, each addressing various elements of preferences indicated.
We note several limitations. First, the number of attributes assessed in the DCE was limited in order to simplify choice sets and shorten the required interview time. Second, because we only included adults in the study, the majority of participants were married. Future research to assess preferences for FP education among unmarried populations and adolescents may reveal distinct preferences. Third, due to the nature of the model used to analyse DCE results, we were not able to stratify by religion, previous or current use of contraception, or desire for pregnancy. Priorities for educational content likely differ between participants who have and have not previously used FP, as suggested by our qualitative data, and future research to illuminate this would be helpful in understanding how FP education can most effectively address these groups, specifically those who are not currently using FP but do not have desire for pregnancy. Lastly, the generalisability of our results to communities outside of Tanzania is unknown, though findings can inform future research.
Despite these limitations, our findings highlight the effectiveness of DCE methodology in understanding nuanced preferences related to FP. Both the use of this methodology and our study’s findings provide an important roadmap for global efforts to increase knowledge about FP among both men and women, which is vital in achieving contraceptive autonomy and universal access to FP.
Ethics statement
All study activities were approved at Institutional Review Boards of the National Institute of Medical Research-Dar es Salaam (NIMR/HQ/R.8a/Vol.IX/2284) and Weill Cornell Medical College (1604017171). Written informed consent was obtained from each participant.
Acknowledgements
We would like to thank the participants for their involvement in this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Schummers L, Hutcheon JA, Hernandez-Diaz S, et al. Association of short interpregnancy interval with pregnancy outcomes according to maternal age. JAMA Intern Med. 2018;178:1661. DOI:10.1001/jamainternmed.2018.4696
- World family planning [highlights] [Internet]. Available from: https://www.un.org/en/development/desa/population/publications/pdf/family/WFP2017_Highlights.pdf
- Family planning/contraception [Internet]. [cited 14 Oct 2019]. Available from: https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception
- Bongaarts J, Bruce J. The causes of unmet need for contraception and the social content of services. Stud Fam Plann. 1995;26:57–75. Available from: http://www.ncbi.nlm.nih.gov/pubmed/7618196
- Campbell M, Sahin-Hodoglugil NN, Potts M. Barriers to fertility regulation: a review of the literature. Stud Fam Plann. 2006;37:87–98. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16832983
- Ministry of Health and Social Welfare. The national road map strategic plan to improve reproductive, maternal, newborn, child & adolescent health in Tanzania (2016–2020) one plan II [Internet]; 2015. Available from: https://www.prb.org/wp-content/uploads/2018/05/National-Road-Map-Strategic-Plan-to-Accelerate-Reduction-of-Maternal-Newborn-and-Child-Deaths-in-Tanzania-2016-2020-One-Plan-II.pdf
- Ministry of Health Community Development Gender Elderly and Children (MoHCDGEC), National Bureau of Statistics Office of the Chief Government Statistician I. Tanzania demographic and health survey 2015–2016 [Internet]. Rockville, MD; 2016. Available from: https://dhsprogram.com/pubs/pdf/FR321/FR321.pdf
- Sundararajan R, Yoder LM, Kihunrwa A, et al. How gender and religion impact uptake of family planning: results from a qualitative study in northwestern Tanzania. BMC Womens Health. 2019;19:99. DOI:10.1186/s12905-019-0802-6
- Pew Forum on Religion and Public Life. Tolerance & tension: Islam and Christianity in Sub-Saharan Africa [Internet]; 2010. [cited 4 Sep 2019]. Available from: https://www.pewforum.org/2010/04/15/executive-summary-islam-and-christianity-in-sub-saharan-africa/
- Dynes MM, Bernstein E, Morof D, et al. Client and provider factors associated with integration of family planning services among maternal and reproductive health clients in Kigoma region, Tanzania: a cross-sectional study, April–July 2016. Reprod Health. 2018;15:152. DOI:10.1186/s12978-018-0593-5
- Mangham LJ, Hanson K, McPake B. How to do (or not to do) … designing a discrete choice experiment for application in a low-income country. Health Policy Plan. 2009;24:151–158. DOI:10.1093/heapol/czn047
- Michaels-Igbokwe C, Lagarde M, Cairns J, et al. Designing a package of sexual and reproductive health and HIV outreach services to meet the heterogeneous preferences of young people in Malawi: results from a discrete choice experiment. Health Econ Rev. 2015;5:9. DOI:10.1186/s13561-015-0046-6
- Michaels-Igbokwe C, Terris-Prestholt F, Lagarde M, et al. Young people’s preferences for family planning service providers in rural Malawi: a discrete choice experiment. PLoS One. 2015;10:e0143287. DOI:10.1371/journal.pone.0143287
- Seston EM, Elliott RA, Noyce PR, et al. Women’s preferences for the provision of emergency hormonal contraception services. Pharm World Sci. 2007;29:183–189. DOI:10.1007/s11096-006-9068-9
- Agyei-Baffour P, Boahemaa MY, Addy EA. Contraceptive preferences and use among auto artisanal workers in the informal sector of Kumasi, Ghana: a discrete choice experiment. Reprod Health. 2015;12:32. DOI:10.1186/s12978-015-0022-y
- Ostermann J, Njau B, Mtuy T, et al. One size does not fit all: HIV testing preferences differ among high-risk groups in Northern Tanzania. AIDS Care – Psychol Socio-Medical Asp AIDS/HIV. 2015;27:595–603. DOI:10.1080/09540121.2014.998612
- Sadique MZ, Devlin N, Edmunds WJ, et al. The effect of perceived risks on the demand for vaccination: results from a discrete choice experiment. PLoS One. 2013;8. DOI:10.1371/journal.pone.0054149
- ChoiceMetrics. No title. Sydney, Australia: ChoiceMetrics; 2012.
- Orme B. Sample size issues for conjoint analysis studies [Internet]; 1998. Available from: www.sawtoothsoftware.com
- Tilahun T, Coene G, Temmerman M, et al. Couple based family planning education: changes in male involvement and contraceptive use among married couples in Jimma zone, Ethiopia. BMC Public Health. 2015;15:682. DOI:10.1186/s12889-015-2057-y
- Link CF. Spousal communication and contraceptive use in rural Nepal: an event history analysis. Stud Fam Plann. 2011;42:83–92. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21834410
- Shakya HB, Dasgupta A, Ghule M, et al. Spousal discordance on reports of contraceptive communication, contraceptive use, and ideal family size in rural India: a cross-sectional study. BMC Womens Health. 2018;18:147. DOI:10.1186/s12905-018-0636-7
- Gebre-Egziabher D, Medhanyie AA, Alemayehu M, et al. Prevalence and predictors of implanon utilization among women of reproductive age group in Tigray region, Northern Ethiopia. Reprod Health. 2017;14:62. DOI:10.1186/s12978-017-0320-7
- Gebremariam A, Addissie A. Intention to use long acting and permanent contraceptive methods and factors affecting it among married women in Adigrat town, Tigray, Northern Ethiopia. Reprod Health. 2014;11:24. DOI:10.1186/1742-4755-11-24
- Tamrie Y, Hanna E, Health MA. Determinants of long acting reversible contraception method use among mothers in extended postpartum period, Durame Town, Southern Ethiopia: a cross. file.scirp.org. Available from: http://file.scirp.org/pdf/Health_2015102016470883.pdf; 2015 undefined
- Zenebe CB, Adefris M, Yenit MK, et al. Factors associated with utilization of long-acting and permanent contraceptive methods among women who have decided not to have more children in Gondar city. BMC Womens Health. 2017;17:75. DOI:10.1186/s12905-017-0432-9