
Abstract
Background
Adherence to evidence-based standard treatment guidelines (STGs) enable healthcare providers to deliver consistently appropriate diagnosis and treatment. Irrational use of antimicrobials significantly contributes to antimicrobial resistance in sub-Saharan Africa (SSA). The best available evidence is needed to guide healthcare providers on adherence to evidence-based implementation of STGs. This systematic review and meta-analysis aimed to determine the pooled prevalence of adherence to evidence-based implementation of antimicrobial treatment guidelines among prescribers in SSA.
Methods
The review followed the JBI methodology for systematic reviews of prevalence data. CINAHL, Embase, PubMed, Scopus, and Web of Science databases were searched with no language and publication year limitations. STATA version 17 were used for meta-analysis. The publication bias and heterogeneity were assessed using Egger’s test and the I 2 statistics. Heterogeneity and publication bias were validated using Duval and Tweedie's nonparametric trim and fill analysis using the random-effect analysis. The summary prevalence and the corresponding 95% confidence interval (CI) of healthcare professionals’ compliance with evidence-based implementation of STG were estimated using random effect model. The review protocol has been registered with PROSPERO code CRD42023389011. The PRISMA flow diagram and checklist were used to report studies included, excluded and their corresponding section in the manuscript.
Results
Twenty-two studies with a total of 17,017 study participants from 14 countries in sub-Saharan Africa were included. The pooled prevalence of adherence to evidence-based implementation of antimicrobial treatment guidelines in SSA were 45%. The pooled prevalence of the most common clinical indications were respiratory tract (35%) and gastrointestinal infections (18%). Overall prescriptions per wards were inpatients (14,413) and outpatients (12,845). Only 391 prescribers accessed standard treatment guidelines during prescription of antimicrobials.
Conclusions
Healthcare professionals’ adherence to evidence-based implementation of STG for antimicrobial treatment were low in SSA. Healthcare systems in SSA must make concerted efforts to enhance prescribers access to STGs through optimization of mobile clinical decision support applications. Innovative, informative, and interactive strategies must be in place by the healthcare systems in SSA to empower healthcare providers to make evidence-based clinical decisions informed by the best available evidence and patient preferences, to ultimately improving patient outcomes and promoting appropriate antimicrobial use.
Supplementary Information
The online version contains supplementary material available at https://doi.org/10.1186/s40545-023-00634-0.
Background
The World Health Organization (WHO) declared antimicrobial resistance (AMR) as a growing global health security and development threat that undermines the effectiveness of antimicrobial agents, threatening the ability to treat common microbial infections [Citation1]. AMR poses a significant economic risk as it leads to higher patient care costs due to prolonged hospitalization, wastage of clinical and human resources, and a demand for the development of novel antimicrobial therapeutics [Citation2, Citation3].
If preventative measures are not taken, the threat of will persist and result in a depletion of resources and an increase in morbidity and mortality on a global scale [Citation4, Citation5]. Low- and middle-income countries (LMICs) suffer greater consequences due to insufficient funding, preventing access to costly second or third-line treatment alternatives [Citation6]. AMR is often a result of misuse and overuse by the patient which is often attributable to inappropriate prescription by the health care provider (HCP) [Citation7].
To combat inappropriate antimicrobial use, the development of standard treatment guidelines (STGs) has been included as part of the WHO’s Global Action Plan initiative; with this implementation, the WHO aims to set guidelines for the purchasing and prescription of antimicrobial medicine [Citation8, Citation9]. STGs help to standardize treatment care by guiding the decisions of prescribers and determine the criteria for diagnosis, prevention, management, and treatment of disease [Citation10, Citation11]. In order for STGs to be effective, they must be continually updated and made accessible to HCPs and patients [Citation12, Citation13].
Studies have shown that when STGs are adhered to, mortality, morbidity, and the costs of health services related to corresponding illness are reduced [Citation14, Citation15]. While the potential of STG use is promising, low rates of STG adherence have been documented in LMICs, where less than half of all patients were treated in accordance with STGs [Citation16–Citation18]. Countries in sub-Saharan Africa (SSA) have made use of STGs, either developing their own based on local context, or adopting the WHO guidelines, altering them to be suitable for resource-limited settings [Citation19–Citation23].
Reasons for lack of adherence to STGs include a lack of skilled human resources, costs of the drugs, quality of the STGs, lack of accessibility to the drugs, lack of access to STGs, and inadequate training of prescribers [Citation24, Citation25]. While the information presented gives us a glimpse of insight into the landscape of adherence to STGs in SSA, this information is not adequate to draw generalizable conclusion regarding patterns of adherence in the area, as most of the current reviews of evidence regarding STG adherence is from HICs [Citation26, Citation27].
A scoping review that analyzed the overuse of medications in low resource settings found that only 10 out of 139 studies reported drivers of non-adherence-specific antimicrobial treatment guidelines [Citation28, Citation29]. Thus, best available evidence on antimicrobial prescriptions in the context of SSA is imperative to understand the adherence of healthcare professionals to their respective STGs and the factors which influence compliance to standard antimicrobial treatment guidelines. This knowledge can be used to inform future interventions to improve prescribing behaviors in SSA in line with the WHOs Global Action Plan initiative’s goal to fill important knowledge gap on antimicrobial stewardship [Citation30].
Therefore, this systematic review and meta-analysis aimed to determine the pooled prevalence of adherence to evidence-based implementation of antimicrobial treatment guidelines among prescribers in sub-Saharan Africa. The pooled data output obtained from this review would serve as region-specific and up-to-date evidence that contributes to comprehensive insights into gaps in the implementation of STGs at point of care and provides actionable recommendations for improvement. It would complement and enhance the knowledge gained from previous reviews by offering a more detailed and context-specific analysis.
Methods
The proposed review were conducted in accordance with the JBI methodology for systematic reviews of prevalence data [Citation31]. The protocol has been registered with PROSPERO (CRD42023389011).
Search strategy
The database search targeted both published and unpublished studies. There was no language and publication year restrictions. A three-step search strategy were used in this review. First, an initial search of PubMed and CINAHL was undertaken, followed by an analysis of the titles, abstracts, and index terms of the articles. Second, all published and unpublished literature were searched using the identified keywords. Additional file 1: Appendix I shows the full search strategy for all databases. Third, the reference lists of all included primary studies were hand-searched for additional relevant studies. The Embase, Scopus, and Web of Science databases were searched. Moreover, Google Scholar, the Africa CDC and WHO platforms, dissertations, and thesis were searched for gray literature. Study authors were contacted if the full text is unavailable.
Study selection
Following the search, all identified citations were collated and uploaded into EndNote 20 and duplicates were removed. Descriptive observational and cross-sectional studies were included. Literature was eligible for inclusion if they reported adherence to STGs among prescribers in SSA. Studies which reported the prevalence of healthcare providers adherence to STGs as the main outcome were included. Literature that reported the clinical indications for which antimicrobials were prescribed for, access, availability, frequency of STG use was included. This review included studies conducted in both public and private health facilities in SSA. Protocols, systematic reviews, meta-analysis, randomized controlled trials, and studies conducted in high-income countries were excluded.
Titles and abstracts were assessed by two independent reviewers (MTB and VS) against the inclusion criteria. The full texts of potentially relevant studies were retrieved and the citation details were imported into the JBI System for the Unified Management, Assessment, and Review of Information (JBI SUMARI) [Citation32]. The full texts of selected citations were assessed in detail against the inclusion criteria by independent reviewers (MTB and VS). Any disagreements that arose between the reviewers at each stage of the selection process were resolved through discussion with a third senior reviewer (SM). The results of the search, study inclusion and exclusion process were reported in full in the final systematic review and presented as a Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram (PRISMA) (Fig. ) [Citation33]. PRISMA 2020 checklist were used to report each section of the manuscript with its corresponding pages (Additional file 1: Appendix II). Studies that reported healthcare providers adherence to evidence-based antimicrobial treatment guidelines in SSA were included. Literature including healthcare professionals from high-income countries, Middle East and North Africa were excluded. Systematic reviews, clinical trials, meta-analysis were excluded.
Fig. 1 PRISMA flow diagram of included studies: Page et al. [Citation96]
![Fig. 1 PRISMA flow diagram of included studies: Page et al. [Citation96]](/cms/asset/66737d60-de2f-43f0-b7d0-b9e1fb3a9faf/jppp_a_12370185_f0001.jpg)
Operational definition
Evidence-based implementation of antimicrobial treatment guidelines
Refers to the systematic and rigorous applications of established clinical recommendations for the use of antimicrobial agents in the treatment of infectious diseases [Citation34]. This approach relies on the uptake of the best available scientific evidence, clinical expertise, and patient preferences to inform healthcare providers about the most effective and safest strategies for prescribing antibiotics [Citation35].
Adherence to evidence-based implementation of antimicrobial treatment guidelines
Refers to compliance with standard treatment guidelines (STG) for antimicrobial treatment at point of care provided that a consistently correct diagnoses and treatments that limit the irrational use of medicines and the negative health consequences that can occur as a result were in place [Citation36, Citation37]. Adherence to guidelines denotes the degree of conformity between the knowledge, cognition and/or action of healthcare professionals who are involved in antimicrobial prescription pursuant with the recommendations of a guideline [Citation38, Citation39]. By adhering to evidence-based guidelines, healthcare providers can optimize patient outcomes, enhance antimicrobial stewardship efforts, and contribute to the overall public health goal of combating antimicrobial resistance [Citation40, Citation41].
Data extraction
The data extraction tool was prepared by MTB using excel spreadsheet. The data were extracted from included studies using the data extraction tool prepared by MTB. The tool includes variables such as the name of the author, publication year, study design, data collection period, sample size, study area, and the prevalence of adherence to standard treatment guidelines (STG) among health care providers. In addition, the tool consists of data on the clinical indications, access and availability of STG, frequency of use of STG. MTB and VS extracted the data. YS and SM cross-checked the extracted data for its validity and cleanness. Any disagreements between the reviewers were resolved through discussion with a third reviewer. Authors of the papers were contacted to request missing or additional data as required.
Assessment of methodological quality
Two independent reviewers critically appraised eligible studies for methodological quality using the JBI critical appraisal checklist for studies reporting prevalence data [Citation42]. Study authors were contacted to request missing or additional data, if required. Any disagreements were resolved through discussion with a third senior reviewer. The results of the critical appraisal were reported in narrative and tabular format. A lower risk of bias (97%) observed after assessment (Table ).
Table 1 Risk bias assessment of included 22 studies
Data synthesis
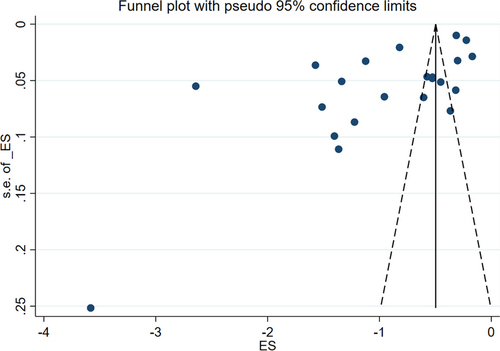
Included studies were pooled in a statistical meta-analysis using STATA version 17.0. Effect size was expressed as a proportion with 95% confidence intervals around the summary estimate. Heterogeneity was assessed using the standard Chi-square I 2 test. A random-effects model using the double arcsine transformation approach were used. Sensitivity analyses were conducted to test decisions made regarding the included studies. Visual examination of funnel plot asymmetry (Fig. ) and Egger’s regression tests were used to check for publication bias [Citation43]. A Forest plot with 95% CI were computed to estimate the pooled magnitude of adherence to evidence-based antimicrobial treatment guidelines among health care providers in sub-Saharan Africa.
Fig. 2 Funnel plot showing symmetric distribution of studies on adherence to evidence-based implementation of antimicrobial treatment guidelines among prescribers in sub-Saharan Africa, 2023
Results
Search
Following the automatic removal of 408 literature as duplicates by EndNote 20, a total of 948 articles were obtained from PubMed, CINAHL, EMBASE, Google Scholar, and SCOPUS, and Web of Science databases. At the title/abstract screening phase (n = 816) and during the full-article screening (n = 110) articles were excluded. Accordingly, 43 studies were eligible for quality assessment. Finally, 22 studies were included in this meta-analysis (Fig. ).
Study characteristics
The total sample size of this systematic review was 17,017, ranging from 75 in Nigeria [Citation44] to 3713 in Ghana [Citation45] (Table ). Three studies were equally reported from Botswana [Citation46–Citation48] Ghana [Citation45, Citation49, Citation50], and South Africa [Citation51–Citation53], respectively (Table ). Two articles were obtained from Namibia [Citation54, Citation55] and Tanzania [Citation56, Citation57] (Table ). Only one literature were obtained from Burkina Faso [Citation58], Ethiopia [Citation59], Kenya [Citation60], Malawi [Citation61], Nigeria [Citation44], South Sudan [Citation62], Sudan [Citation63], Uganda [Citation64], Zambia [Citation65], respectively (Table ).
Table 2 Adherence to standard treatment guidelines (STGs)
The most common clinical indications for antibiotics were respiratory tract infection (RTI) reported by eleven studies [Citation46, Citation49, Citation50, Citation52, Citation55, Citation56, Citation59, Citation61–Citation64], followed by urinary tract infection (UTI) [Citation45, Citation49, Citation56, Citation61], and gastrointestinal disease/infection [Citation52, Citation62, Citation64, Citation65] which were equally indicated by four different studies (Table ). Three articles described diarrhea [Citation47, Citation55, Citation56] as clinical condition (Table ). Equally two studies reported CNS [Citation61, Citation65], co-infection [Citation61, Citation62], Enteric infection [Citation49, Citation61], Sepsis [Citation61, Citation65], STIs [Citation52, Citation53], and Malaria [Citation56, Citation65] clinical indications for antibiotics, respectively (Table ).
Table 3 Clinical indication for prescription
Public health officers (1616), nurses (731), medical doctors (196), and community health workers (151) were the distribution of STGs prescribers according to profession (Table ). Educational qualification of prescribers was medical doctor (1676), clinical nurse (679), specialist (617), and internist (100), respectively (Table ). A total of prescriptions made per ward were 12,845 (outpatient) and 14,413 (inpatient), respectively (Table ). Three studies [Citation54, Citation57, Citation63] reported that only 261 health care providers were aware regarding the use of STGs at point of clinical care (Table ).
Table 4 Access to STGs
Only three studies have reported the frequency of STG use by prescribers [Citation49, Citation51, Citation54], out of which two articles described that healthcare professionals never used STG [Citation49, Citation54] (Table ). Six articles [Citation49, Citation51, Citation54, Citation55, Citation57, Citation63] revealed that 391 health care providers accessed STGs during prescription (Table ). Only two literatures [Citation54, Citation57] reported that continuous professional development (CPD) training on compliance to STGs were delivered to 213 health care workers (Table ). The review was conducted on studies that used the cross-sectional designs (Table ).
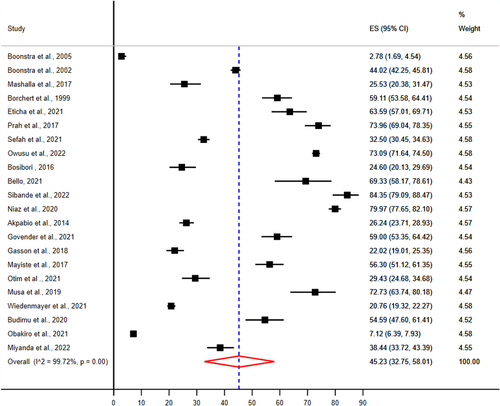
Pooled prevalence of implementation of evidence-based antimicrobial treatment guidelines
The pooled prevalence of adherence to evidence-based implementation of antimicrobial treatment guidelines were 45.23% (95% CI 32.75–58.01%) (Fig. ).
Fig. 3 Pooled prevalence of adherence to evidence-based implementation of antimicrobial treatment guidelines among prescribers in sub-Saharan Africa
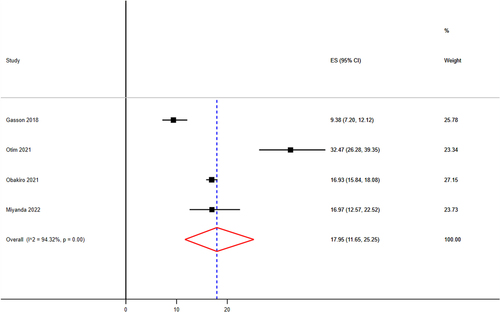
The pooled prevalence of RTI, UTI, and GI
The sample size of RTI ranges from 56 [Citation63] to 902 [Citation64] (Table ). The pooled prevalence of RTI were 34.84 (95% CI 29.00–40.90%) (Fig. ). The lowest and the highest infection from gastrointestinal diseases were 37 [Citation65] and 730 [Citation64] (Table ). The pooled prevalence GI were 17.95% (95% CI 11.65–25.25%) (Fig. ).
Fig. 4 Pooled prevalence of respiratory tract infection as most common clinical indication as prescriptions made in sub-Saharan Africa
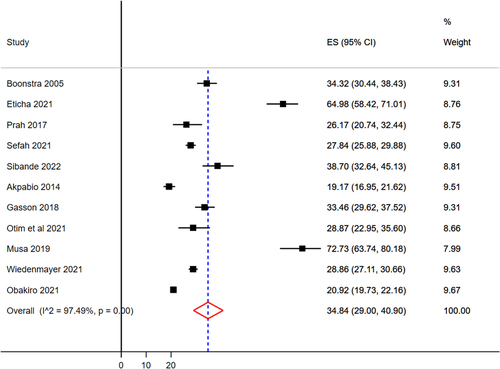
Fig. 5 Pooled prevalence of gastrointestinal tract infection as second most common clinical indication as prescriptions made in sub-Saharan Africa
Discussion
This systematic review and meta-analysis aimed to determine the pooled estimate of implementation of standard treatment guidelines among the prescribers in SSA. A total of 17,017 healthcare professionals who prescribed antimicrobials participated in 22 studies reported from 14 in SSA. The pooled prevalence of adherence to evidence-based antimicrobial treatment guidelines at point of care in SSA were 45%. Lower adherence to evidence-based antimicrobial treatment guidelines can be attributed to healthcare provider-related factors, such as lack of awareness or knowledge about the guidelines [Citation66], doubt regarding their applicability to individual patients [Citation67], limited availability or accessibility of guidelines [Citation68], inadequate resources or infrastructure to support guideline implementation [Citation69], and competing priorities within healthcare settings [Citation70], and patient preferences [Citation71]. Addressing these barriers through targeted educational initiatives, organizational support, and shared decision-making approaches can help improve adherence to evidence-based antimicrobial treatment guidelines and promote optimal patient care [Citation72–Citation74].
This review indicated that only 261 prescribers have awareness regarding the implementation of STG in routine clinical care. Lower awareness among prescribers regarding the use of STG at the point of care can have significant implications for patient care and outcomes [Citation75]. It can lead to variations in clinical practices, with prescribers deviating from evidence-based recommendations [Citation76]. This can result in inconsistent and potentially suboptimal treatment decisions, compromising patient safety and quality of care [Citation77]. Inadequate awareness of guidelines contributes to overuse or inappropriate use of antimicrobial agents, leading to increased healthcare costs, antimicrobial resistance, and adverse drug reactions [Citation78]. Implementation of decision support tools can help improve adherence to guidelines, enhance patient outcomes, and promote the judicious use of antimicrobial treatments [Citation79, Citation80].
This study revealed that only 391 healthcare providers in SSA accessed STG when they prescribed antimicrobials to patients. Limited access to STG for healthcare providers can lead to variability and inconsistency in prescribing practices [Citation81]. This can result in suboptimal or inappropriate use of antimicrobial agents, potentially compromising patient safety and treatment efficacy [Citation82]. The absence of guidelines can hinder the dissemination of evidence-based recommendations, impeding the implementation of best practices and advancements in antimicrobial stewardship [Citation83, Citation84]. Healthcare providers may face challenges in keeping up with the rapidly evolving field of infectious diseases and antimicrobial resistance without access to updated guidelines [Citation85].
Healthcare providers in SSA commonly treated cases of respiratory tract infection (35%) and gastrointestinal diseases (18%). Respiratory tract (35%) and gastrointestinal (18%) infections are highly treated clinical indications in SSA. This could be attributed to their significant burden due to easy transmissibility and environmental factors [Citation86, Citation87].
Limitations of the study
This systematic review and meta-analysis involved cross-sectional studies that comes with limitations related to causality, selection bias, heterogeneity, and the inability to capture temporal and dynamic trends. To overcome these limitations and obtain a more comprehensive understanding of adherence to implementation of evidence-based STGs, future research could consider incorporating other study designs, such as longitudinal studies or randomized controlled trials, in addition to cross-sectional data.
Conclusion
Healthcare professionals’ adherence to evidence-based implementation of standard treatment guidelines for antimicrobial treatment were low in sub-Saharan Africa. Healthcare systems in sub-Saharan Africa must make concerted efforts to enhance prescribers access to standard treatment guidelines through the implementation of mobile clinical decision support applications to optimize compliance with standard treatment guidelines. Innovative, informative, and interactive strategies must be in place by the healthcare systems in sub-Saharan Africa to empower healthcare providers to make evidence-based clinical decisions informed by the best available evidence and patient preferences, to ultimately improving patient outcomes and promoting appropriate antimicrobial use.
Implications for policy and practice
The implementation of evidence-based clinical practice guidelines for antimicrobial treatment involves the systematic integration of the best available evidence into clinical decision-making and patient care [Citation88, Citation89]. These guidelines are developed based on rigorous research and aim to provide healthcare practitioners with recommendations on the appropriate use of antimicrobial agents for specific infections [Citation90]. The implementation process includes raising awareness about the guidelines, promoting their adoption and acceptance among healthcare professionals, providing education and training on their content and implementation strategies, and addressing barriers and challenges to their implementation [Citation91, Citation92]. By effectively implementing these guidelines, healthcare systems can optimize antimicrobial therapy, improve patient outcomes, prevent antimicrobial resistance, and ensure the judicious use of these critical medications in sub-Saharan Africa [Citation93–Citation95].
Author contributions
MTB, SM and VS; was involved in a principal role in the conception of ideas, developing methodologies, writing the manuscript. MTB and VS, were involved in the analysis while MW, YS, and ZEK participated in the analysis, interpretation and writing. YS and ZEK involved in proofreading, and writing. All authors read and approved the final version of the manuscript.
Declarations
Ethics approval and consent to participate
Not applicable. Unlike primary studies, systematic reviews does not include the collection of deeply personal, sensitive, and confidential information from the study participants. Systematic reviews involves the use of publicly accessible data as evidence and are not required to seek an institutional ethics approval before commencement.
Consent for publication
Not applicable.
Competing interests
The authors declare that this study is free of any competing financial and non-financial interests.
Supplementary Information
Abbreviations
| AMR | = | Antimicrobial resistance |
| AHRI | = | The Armauer Hansen Research Institute |
| HCP | = | Health Care Providers/Professionals |
| JBI | = | The Joanna Briggs Institute |
| JBI SUMARI | = | The Joanna Briggs Institute’s System for the Unified Management, Assessment, and Review of Information (SUMARI) |
| LMICs | = | Low- and middle-income countries |
| PRISMA | = | Preferred Reporting Items for Systematic Reviews and Meta-analyses |
| PROSPERO | = | International Prospective Registry of Systematic Reviews |
| SDG | = | Sustainable development goal |
| SSA | = | Sub-Saharan Africa |
| STGs | = | Standard Treatment Guidelines |
| WHO | = | The World Health Organization |
jppp_a_12370185_sm0001.docx
Download MS Word (32.3 KB)Acknowledgements
We would like to acknowledge the Ethiopian Evidence Based Health Care and Development Centre, A JBI Centre of Excellence, and the Armauer Hansen Research Institute for proving the training on comprehensive systematic review, meta-analysis, and access to databases.
Funding
Not applicable.
Availability of data and materials
The data sets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Zhou N, Cheng Z, Zhang X, Lv C, Guo C, Liu H, Dong K, Zhang Y, Liu C, Chang Y-F, et al.Global antimicrobial resistance: a system-wide comprehensive investigation using the Global One Health IndexInfect Dis Poverty202211192 35996187 9395850 10.1186/s40249-022-01016-5
- Shrestha P, Cooper BS, Coast J, Oppong R, Do Thi Thuy N, Phodha T, Celhay O, Guerin PJ, Wertheim H, Lubell YEnumerating the economic cost of antimicrobial resistance per antibiotic consumed to inform the evaluation of interventions affecting their useAntimicrob Resist Infect Control20187198 30116525 6085682 10.1186/s13756-018-0384-3
- Chakaya J, Khan M, Ntoumi F, Aklillu E, Fatima R, Mwaba P, Kapata N, Mfinanga S, Hasnain SE, Katoto P, et al.Global tuberculosis report 2020—reflections on the global TB burden, treatment and prevention effortsInt J Infect Dis2021113Suppl 1S7s12 1:CAS:528:DC%2BB3MXhsFaqt7bI 33716195 8433257 10.1016/j.ijid.2021.02.107
- Dadgostar PAntimicrobial resistance: implications and costsInfect Drug Resist20191239033910 1:CAS:528:DC%2BB3cXhtVertLvL 31908502 6929930 10.2147/IDR.S234610
- Ayukekbong JA, Ntemgwa M, Atabe ANThe threat of antimicrobial resistance in developing countries: causes and control strategiesAntimicrob Resist Infect Control2017647 28515903 5433038 10.1186/s13756-017-0208-x
- Jim ON. Antimicrobial resistance: tackling a crisis for the health and wealth of nations. Rev Antimicrob Resist. 2014.
- Nahar P, Unicomb L, Lucas PJ, Uddin MR, Islam MA, Nizame FA, Khisa N, Akter SMS, Rousham EKWhat contributes to inappropriate antibiotic dispensing among qualified and unqualified healthcare providers in Bangladesh? A qualitative studyBMC Health Serv Res2020201656 32669092 7362537 10.1186/s12913-020-05512-y
- Kamere N, Garwe ST, Akinwotu OO, Tuck C, Krockow EM, Yadav S, Olawale AG, Diyaolu AH, Munkombwe D, Muringu E, et al.Scoping review of national antimicrobial stewardship activities in eight African countries and adaptable recommendationsAntibiotics (Basel)20221191149 36139929 10.3390/antibiotics11091149
- Cuevas C, Batura N, Wulandari LPL, Khan M, Wiseman VImproving antibiotic use through behaviour change: a systematic review of interventions evaluated in low- and middle-income countriesHealth Policy Plan2021365754773 8488384 10.1093/heapol/czab021
- Lahariya C, Sharma S, Agnani M, de Graeve H, Srivastava JN, Bekedam HAttributes of standard treatment guidelines in clinical settings and public health facilities in IndiaIndian J Commun Med2022473336
- Yan M, Chen L, Yang M, Zhang L, Niu M, Wu F, Chen Y, Song Z, Zhang Y, Li JEvidence mapping of clinical practice guidelines recommendations and quality for depression in children and adolescentsEur Child Adolesc Psychiatry20223220912108 35262810 10.1007/s00787-022-01958-z
- Herbella FA, Patti MG, Filho RM, Serodio AM, Adão D, Bastos IBDA, Soares FR, Wagar III CHow changes in treatment guidelines affect the standard of care: ethical opinions using the Chicago 4.0 classification for esophageal motility disorders as exampleForegut202222111115 10.1177/26345161221081038
- Burgers J, van der Weijden T, Grol R. Clinical practice guidelines as a tool for improving patient care. In: Improving patient care: the implementation of change in health care. 2020. pp. 103–129.
- Crimmins EM, Beltrán-Sánchez HMortality and morbidity trends: is there compression of morbidity?J Gerontol B Psychol Sci Soc Sci20116617586 21135070 10.1093/geronb/gbq088
- Kruk ME, Gage AD, Joseph NT, Danaei G, García-Saisó S, Salomon JAMortality due to low-quality health systems in the universal health coverage era: a systematic analysis of amenable deaths in 137 countriesLancet20183921016022032212 30195398 6238021 10.1016/S0140-6736(18)31668-4
- Olayemi E, Asare EV, Benneh-Akwasi Kuma AAGuidelines in lower-middle income countriesBr J Haematol20171776846854 28295193 10.1111/bjh.14583
- Docherty M, Shaw K, Goulding L, Parke H, Eassom E, Ali F, Thornicroft GEvidence-based guideline implementation in low and middle income countries: lessons for mental health careInt J Ment Heal Syst20171118 10.1186/s13033-016-0115-1
- Mondéjar EFConsiderations on the low adherence to clinical practice guidelinesMed Intensiva201741265266
- Odoch WD, Senkubuge F, Masese AB, Hongoro CHow are global health policies transferred to sub-Saharan Africa countries? A systematic critical review of literatureGlob Health202218125 10.1186/s12992-022-00821-9
- Mhazo AT, Maponga CCAgenda setting for essential medicines policy in sub-Saharan Africa: a retrospective policy analysis using Kingdon’s multiple streams modelHealth Res Policy Syst202119172 33941199 8091660 10.1186/s12961-021-00724-y
- Stegmann J-U, Jusot V, Menang O, Gardiner G, Vesce S, Volpe S, Ndalama A, Adou F, Ofori-Anyinam O, Oladehin O, et al.Challenges and lessons learned from four years of planning and implementing pharmacovigilance enhancement in sub-Saharan AfricaBMC Public Health20222211568 35978276 9383683 10.1186/s12889-022-13867-6
- Chakkalakal RJ, Cherlin E, Thompson J, Lindfield T, Lawson R, Bradley EHImplementing clinical guidelines in low-income settings: a review of literatureGlob Public Health201387784795 23914758 10.1080/17441692.2013.815794
- Heen AF, Vandvik PO, Brandt L, Montori VM, Lytvyn L, Guyatt G, Quinlan C, Agoritsas TA framework for practical issues was developed to inform shared decision-making tools and clinical guidelinesJ Clin Epidemiol2021129104113 33049326 10.1016/j.jclinepi.2020.10.002
- Sarwar MR, Saqib A, Iftikhar S, Sadiq TAntimicrobial use by WHO methodology at primary health care centers: a cross sectional study in Punjab, PakistanBMC Infect Dis2018181492 30268106 6162939 10.1186/s12879-018-3407-z
- Sijbom M, Büchner FL, Saadah NH, Numans ME, de Boer MGDeterminants of inappropriate antibiotic prescription in primary care in developed countries with general practitioners as gatekeepers: a systematic review and construction of a frameworkBMJ Open2023135 37197815 10193070 10.1136/bmjopen-2022-065006
- Perumal-Pillay VA, Suleman FSelection of essential medicines for South Africa—an analysis of in-depth interviews with national essential medicines list committee membersBMC Health Serv Res201717117 28061899 5219715 10.1186/s12913-016-1946-9
- Peacocke EF, Myhre SL, Foss HS, Gopinathan UNational adaptation and implementation of WHO Model List of Essential Medicines: a qualitative evidence synthesisPLoS Med2022193 35275938 8956172 10.1371/journal.pmed.1003944
- Albarqouni L, Hoffmann T, Straus S, Olsen NR, Young T, Ilic D, Shaneyfelt T, Haynes RB, Guyatt G, Glasziou PCore competencies in evidence-based practice for health professionals: consensus statement based on a systematic review and Delphi SurveyJAMA Netw Open201812e180281e180281 30646073 10.1001/jamanetworkopen.2018.0281
- Albarqouni L, Palagama S, Chai J, Sivananthajothy P, Pathirana T, Bakhit M, Arab-Zozani M, Ranakusuma R, Cardona M, Scott A, et al.Overuse of medications in low- and middle-income countries: a scoping reviewBull World Health Organ202310113661d 36593777 10.2471/BLT.22.288293
- Hamers RL, Dobreva Z, Cassini A, Tamara A, Lazarus G, Asadinia KS, Burzo S, Olaru ID, Dona D, Emdin F, et al.Global knowledge gaps on antimicrobial resistance in the human health sector: a scoping reviewInt J Infect Dis2023134142149 37301361 10.1016/j.ijid.2023.06.004
- Aromataris E, Stern C, Lockwood C, Barker TH, Klugar M, Jadotte Y, Evans C, Ross-White A, Lizarondo L, Stephenson M, et al.JBI series paper 2: tailored evidence synthesis approaches are required to answer diverse questions: a pragmatic evidence synthesis toolkit from JBIJ Clin Epidemiol2022150196202 35429608 10.1016/j.jclinepi.2022.04.006
- Munn Z, Aromataris E, Tufanaru C, Stern C, Porritt K, Farrow J, Lockwood C, Stephenson M, Moola S, Lizarondo LThe development of software to support multiple systematic review types: the Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI)JBI Evid Implement20191713643
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SEThe PRISMA 2020 statement: an updated guideline for reporting systematic reviewsInt J Surg202188 33789826 10.1016/j.ijsu.2021.105906
- Gagliardi AR, Armstrong MJ, Bernhardsson S, Fleuren M, Pardo-Hernandez H, Vernooij RW, Willson M, Brereton L, Lockwood C, Amer YSThe Clinician Guideline Determinants Questionnaire was developed and validated to support tailored implementation planningJ Clin Epidemiol2019113129136 31152863 10.1016/j.jclinepi.2019.05.024
- Titler MG. The evidence for evidence-based practice implementation. In: Patient safety and quality: an evidence-based handbook for nurses. 2008.
- Borek AJ, Campbell A, Dent E, Moore M, Butler CC, Holmes A, Walker AS, McLeod M, Tonkin-Crine S, Anyanwu PE, et al.Development of an intervention to support the implementation of evidence-based strategies for optimising antibiotic prescribing in general practiceImplement Sci Commun202121104 34526140 8441243 10.1186/s43058-021-00209-7
- Steels S, van Staa TPThe role of real-world data in the development of treatment guidelines: a case study on guideline developers’ opinions about using observational data on antibiotic prescribing in primary careBMC Health Serv Res2019191942 31805940 6896760 10.1186/s12913-019-4787-5
- Hasenbein U, Wallesch CWWhat is "adherence to guidelines"? Theoretical and methodological considerations on a new concept for health system research and quality managementGesundheitswesen2007698–9427437 1:STN:280:DC%2BD2sngtlWktg%3D%3D 17926259 10.1055/s-2007-985388
- Foxlee ND, Townell N, Heney C, McIver L, Lau CLStrategies used for implementing and promoting adherence to antibiotic guidelines in low-and lower-middle-income countries: a systematic reviewTrop Med Infect Disease202163166 10.3390/tropicalmed6030166
- Kakkar AK, Shafiq N, Singh G, Ray P, Gautam V, Agarwal R, Muralidharan J, Arora PAntimicrobial stewardship programs in resource constrained environments: understanding and addressing the need of the systemsFront Public Health20208140 32411647 7198767 10.3389/fpubh.2020.00140
- Adhikari P, Director M, Bhumiratana A, Acharya S, Acharya U, Pant S, Silwal S, Dawadi P, Koirala J, Gyanwali P. 1779. An assessment of antibiotic treatment guideline adherence for common infections in a Tertiary Care Hospital with an established Antimicrobial Stewardship Program in Kathmandu, Nepal. In: Open Forum Infectious Diseases: 2022: Oxford University Press USA; 2022: ofac492. 1409.
- Munn Z, Moola S, Lisy K, Riitano D, Tufanaru CMethodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence dataInt J Evid Based Healthc2015133147153 26317388 10.1097/XEB.0000000000000054
- Copas J, Shi JQA sensitivity analysis for publication bias in systematic reviewsStat Methods Med Res2001104251265 1:STN:280:DC%2BD3MvksF2htw%3D%3D 11491412 10.1177/096228020101000402
- Bello CBAdherence to medication administration guidelines among nurses in a health facility in South-West NigeriaPan Afr Med J202140156 34795835 8571931
- Owusu H, Thekkur P, Ashubwe-Jalemba J, Hedidor GK, Corquaye O, Aggor A, Steele-Dadzie A, Ankrah DCompliance to guidelines in prescribing empirical antibiotics for individuals with uncomplicated urinary tract infection in a Primary Health Facility of Ghana, 2019–2021Int J Environ Res Public Health2022191912413 36231716 9566282 10.3390/ijerph191912413
- Boonstra E, Lindbæk M, Ngome EAdherence to management guidelines in acute respiratory infections and diarrhoea in children under 5 years old in primary health care in BotswanaInt J Qual Health Care2005173221227 15723818 10.1093/intqhc/mzi020
- Boonstra E, Lindbaek M, Khulumani P, Ngome E, Fugelli PAdherence to treatment guidelines in primary health care facilities in BotswanaTrop Med Int Health200272178186 1:STN:280:DC%2BD387htVaitA%3D%3D 11841708 10.1046/j.1365-3156.2002.00842.x
- Mashalla Y, Setlhare V, Massele A, Sepako E, Tiroyakgosi C, Kgatlwane J, Chuma M, Godman B. Assessment of prescribing practices at the primary healthcare facilities in Botswana with an emphasis on antibiotics: findings and implications. Int J Clin Pract. 2017; 71(12).
- Prah J, Kizzie-Hayford J, Walker E, Ampofo-Asiama AAntibiotic prescription pattern in a Ghanaian primary health care facilityPan Afr Med J2017281214 29610652 5878858
- Sefah IA, Essah DO, Kurdi A, Sneddon J, Alalbila TM, Kordorwu H, Godman BAssessment of adherence to pneumonia guidelines and its determinants in an ambulatory care clinic in Ghana: findings and implications for the futureJAC Antimicrob Resist202132dlab080 34223139 8210001 10.1093/jacamr/dlab080
- Govender T, Suleman F, Perumal-Pillay VAEvaluating the implementation of the standard treatment guidelines (STGs) and essential medicines list (EML) at a public South African tertiary institution and its associated primary health care (PHC) facilitiesJ Pharm Policy Pract2021141105 34906236 8670019 10.1186/s40545-021-00390-z
- Gasson J, Blockman M, Willems BAntibiotic prescribing practice and adherence to guidelines in primary care in the Cape Town Metro District, South AfricaS Afr Med J20181084304310 1:STN:280:DC%2BC1MjgtFGhtQ%3D%3D 29629681 10.7196/SAMJ.2018.v108i4.12564
- Matsitse TB, Helberg E, Meyer JC, Godman B, Massele A, Schellack NCompliance with the primary health care treatment guidelines and the essential medicines list in the management of sexually transmitted infections in correctional centres in South Africa: findings and implicationsExpert Rev Anti Infect Ther20171510963972 1:CAS:528:DC%2BC2sXhs1ait77N 28922959 10.1080/14787210.2017.1382354
- Niaz Q, Godman B, Campbell S, Kibuule DCompliance to prescribing guidelines among public health care facilities in Namibia; findings and implicationsInt J Clin Pharm202042412271236 32458227 7476965 10.1007/s11096-020-01056-7
- Akpabio E, Sagwa E, Mazibuko G, Kagoya H, Niaz Q, Mabirizi D. Assessment of compliance of outpatient prescribing with the Namibia standard treatment guidelines in Public Sector Health Facilities. Windhoek: MSH-Namibia. 2014.
- Wiedenmayer K, Ombaka E, Kabudi B, Canavan R, Rajkumar S, Chilunda F, Sungi S, Stoermer MAdherence to standard treatment guidelines among prescribers in primary healthcare facilities in the Dodoma region of TanzaniaBMC Health Serv Res2021211272 33761948 7990379 10.1186/s12913-021-06257-y
- Budimu A, Emidi B, Mkumbaye S, Kajeguka DC. Adherence, awareness, access, and use of standard diagnosis and treatment guideline for malaria case management among healthcare workers in Meatu, Tanzania. J Trop Med. 2020.
- Krause G, Borchert M, Benzler J, Heinmüller R, Kaba I, Savadogo M, Siho N, Diesfeld HRationality of drug prescriptions in rural health centres in Burkina FasoHealth Policy Plan1999143291298 1:STN:280:DyaK1Mvlsl2jtw%3D%3D 10621246 10.1093/heapol/14.3.291
- Eticha EM, Gemechu WDAdherence to guidelines for assessment and empiric antibiotics recommendations for community-acquired pneumonia at ambo university referral hospital: prospective observational studyPatient Prefer Adherence202115467473 33658770 7920623 10.2147/PPA.S295118
- Obegi EB. Antimicrobial prescribing patterns in critical care and compliance to guideline at the Kenyatta National Hospital. University of Nairobi; 2020.
- Sibande GT, Banda NPK, Moya T, Siwinda S, Lester RAntibiotic guideline adherence by Clinicians in medical wards at Queen Elizabeth Central Hospital (QECH), Blantyre MalawiMalawi Med J202234138 37265826 10230578 10.4314/mmj.v34i1.2
- Otim ME, Demaya DK, Al Marzouqi A, Mukasa JAre antibiotics prescribed to inpatients according to recommended standard guidelines in South Sudan? A retrospective cross-sectional study in Juba Teaching HospitalJ Multidiscip Healthc20211428712879 34675535 8522334 10.2147/JMDH.S321990
- Nehal AM Musa HMHaMMAM, Musa NAM, Harron HM, Maatoug MMA. Assessment of medical doctors’ adherence to national protocol for treatment of severe pneumonia in underfive children admitted to Wad-Medani pediatric teaching hospital, Gezira State, Sudan (2018). Clin Pract. 2019; 16(S1): 1381–1388. https://doi.org/10.4172/clinical-practice.1000405.
- Obakiro SB, Napyo A, Wilberforce MJ, Adongo P, Kiyimba K, Anthierens S, Kostyanev T, Waako P, Van Royen PAre antibiotic prescription practices in Eastern Uganda concordant with the national standard treatment guidelines? A cross-sectional retrospective studyJ Global Antimicrob Resist202229513519 10.1016/j.jgar.2021.11.006
- Miyanda PM, Siame B, Chisulo ACAntibiotic prescribing patterns at a level one hospital using national treatment guidelines prescribing indicators in ZambiaJ Prevent Rehabil Med2022415964
- Saunders BI. Inappropriate antibiotic use: a survey of provider prescribing behaviors. 2020.
- Wehking F, Debrouwere M, Danner M, Geiger F, Buenzen C, Lewejohann J-C, Scheibler F. Impact of shared decision making on healthcare in recent literature: a scoping review using a novel taxonomy. J Public Health 2023:1–12.
- Correa VC, Lugo-Agudelo LH, Aguirre-Acevedo DC, Contreras JAP, Borrero AMP, Patiño-Lugo DF, Valencia DACIndividual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: a systematic metareviewHealth Res Policy Syst202018111 10.1186/s12961-020-00588-8
- Tian C, Xu M, Wang Y, Lu J, Wang Y, Xue J, Ge L. Barriers and strategies of clinical practice guideline implementation in China: aggregated analysis of 16 cross-sectional surveys. J Public Health. 2023:1–14.
- Saluja K, Reddy KS, Wang Q, Zhu Y, Li Y, Chu X, Li R, Hou L, Horsley T, Carden FImproving WHO’s understanding of WHO guideline uptake and use in Member States: a scoping reviewHealth Res Policy Syst2022201121 10.1186/s12961-022-00899-y
- Blackwood J, Armstrong MJ, Schaefer C, Graham ID, Knaapen L, Straus SE, Urquhart R, Gagliardi ARHow do guideline developers identify, incorporate and report patient preferences? An international cross-sectional surveyBMC Health Serv Res202020110 10.1186/s12913-020-05343-x
- Engle RL, Mohr DC, Holmes SK, Seibert MN, Afable M, Leyson J, Meterko MEvidence-based practice and patient-centered care: doing both wellHealth Care Manage Rev2021463174 31233424 10.1097/HMR.0000000000000254
- Melnyk BM, Gallagher-Ford L, Fineout-Overholt E. Implementing the evidence-based practice (EBP) competencies in healthcare: a practical guide for improving quality, safety, and outcomes: Sigma Theta Tau; 2016.
- Cullen L, Hanrahan K, Farrington M, Tucker S, Edmonds S. Evidence-based practice in action: comprehensive strategies, tools, and tips from University of Iowa Hospitals & Clinics: Sigma Theta Tau; 2022.
- Saha SK, Thursky K, Kong DC, Mazza DA novel GPPAS model: guiding the implementation of antimicrobial stewardship in primary care utilising collaboration between general practitioners and community pharmacistsAntibiotics20221191158 36139938 9495087 10.3390/antibiotics11091158
- Fadoul Y, Haddad C, Habib J, Zoghbi MPharmaceutical brochures in Lebanon: do they meet WHO recommendations?BMC Primary Care202223118 10.1186/s12875-022-01930-5
- Karasneh RA, Al-Azzam SI, Ababneh M, Al-Azzeh O, Al-Batayneh OB, Muflih SM, Khasawneh M, Khassawneh A-RM, Khader YS, Conway BRPrescribers’ knowledge, attitudes and behaviors on antibiotics, antibiotic use and antibiotic resistance in JordanAntibiotics2021107858 34356779 8300611 10.3390/antibiotics10070858
- Al Rahbi F, Al Salmi I, Khamis F, Al Balushi Z, Pandak N, Petersen E, Hannawi SPhysicians’ attitudes, knowledge, and practices regarding antibiotic prescriptionsJ Global Antimicrob Resist2023325865 10.1016/j.jgar.2022.12.005
- Rawson T, Moore L, Hernandez B, Charani E, Castro-Sanchez E, Herrero P, Hayhoe B, Hope W, Georgiou P, Holmes AA systematic review of clinical decision support systems for antimicrobial management: are we failing to investigate these interventions appropriately?Clin Microbiol Infect2017238524532 1:STN:280:DC%2BC1czjs1Kqsg%3D%3D 28268133 10.1016/j.cmi.2017.02.028
- Eudaley ST, Mihm AE, Higdon R, Jeter J, Chamberlin SMDevelopment and implementation of a clinical decision support tool for treatment of uncomplicated urinary tract infections in a family medicine resident clinicJ Am Pharm Assoc2019594579585 10.1016/j.japh.2019.03.006
- Steffens E, Quintens C, Derdelinckx I, Peetermans WE, Van Eldere J, Spriet I, Schuermans AOutpatient parenteral antimicrobial therapy and antibiotic stewardship: opponents or teammates?Infection201947169181 30443780 10.1007/s15010-018-1250-1
- Venkatesan AM, Kundu S, Sacks D, Wallace MJ, Wojak JC, Rose SC, Clark TW, d'Othee BJ, Itkin M, Jones RSPractice guideline for adult antibiotic prophylaxis during vascular and interventional radiology proceduresJ Vasc Interv Radiol2010211116111630 21029949 10.1016/j.jvir.2010.07.018
- Fischer F, Lange K, Klose K, Greiner W, Kraemer ABarriers and strategies in guideline implementation—a scoping reviewHealthcare (Basel)20164336 27417624 10.3390/healthcare4030036
- McArthur C, Bai Y, Hewston P, Giangregorio L, Straus S, Papaioannou ABarriers and facilitators to implementing evidence-based guidelines in long-term care: a qualitative evidence synthesisImplement Sci202116170 34243789 8267230 10.1186/s13012-021-01140-0
- Pereira VC, Silva SN, Carvalho VKS, Zanghelini F, Barreto JOMStrategies for the implementation of clinical practice guidelines in public health: an overview of systematic reviewsHealth Res Policy Syst202220113 35073897 8785489 10.1186/s12961-022-00815-4
- Serigstad S, Markussen DL, Ritz C, Ebbesen MH, Knoop ST, Kommedal Ø, Heggelund L, Ulvestad E, Bjørneklett RO, Grewal HMS, et al.The changing spectrum of microbial aetiology of respiratory tract infections in hospitalized patients before and during the COVID-19 pandemicBMC Infect Dis2022221763 1:CAS:528:DC%2BB38Xis1GntbbN 36180842 9523652 10.1186/s12879-022-07732-5
- Natarajan A, Zlitni S, Brooks EF, Vance SE, Dahlen A, Hedlin H, Park RM, Han A, Schmidtke DT, Verma R, et al.Gastrointestinal symptoms and fecal shedding of SARS-CoV-2 RNA suggest prolonged gastrointestinal infectionMed202236371387.e379 1:CAS:528:DC%2BB38XhtFyrtbzO 35434682 10.1016/j.medj.2022.04.001
- Foxlee ND, Townell N, Heney C, McIver L, Lau CLStrategies used for implementing and promoting adherence to antibiotic guidelines in low- and lower-middle-income countries: a systematic reviewTrop Med Infect Dis202163166 34564550 8482147 10.3390/tropicalmed6030166
- Peters S, Sukumar K, Blanchard S, Ramasamy A, Malinowski J, Ginex P, Senerth E, Corremans M, Munn Z, Kredo T, et al.Trends in guideline implementation: an updated scoping reviewImplement Sci202217150 35870974 9308215 10.1186/s13012-022-01223-6
- Wu S, Tannous E, Haldane V, Ellen ME, Wei XBarriers and facilitators of implementing interventions to improve appropriate antibiotic use in low-and middle-income countries: a systematic review based on the Consolidated Framework for Implementation ResearchImplement Sci202217130 35550169 9096759 10.1186/s13012-022-01209-4
- Elaine L, Patricia L-W, Cliona OR, Eileen S, Jonathan D, Colm OT, Michael OC, Mark C, Francis B, Martina H, et al.Evidence-based practice education for healthcare professions: an expert viewBMJ Evid Based Med2019243103 10.1136/bmjebm-2018-111019
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, Boyd KA, Craig N, French DP, McIntosh E, et al.A new framework for developing and evaluating complex interventions: update of Medical Research Council guidanceBMJ2021374 34593508 8482308 10.1136/bmj.n2061
- O'Brien EA-O, Clyne B, Smith SA-O, O'Herlihy N, Harkins V, Wallace E. A scoping review protocol of evidence-based guidance and guidelines published by general practitioner professional organisations. LID-53. (2515–4826 (Electronic)).
- Kredo T, Bernhardsson S, Machingaidze S, Young T, Louw Q, Ochodo E, Grimmer KGuide to clinical practice guidelines: the current state of playInt J Qual Health Care2016281122128 26796486 4767049 10.1093/intqhc/mzv115
- Chan WV, Pearson TA, Bennett GC, Cushman WC, Gaziano TA, Gorman PN, Handler J, Krumholz HM, Kushner RF, MacKenzie TD, et al.ACC/AHA special report: clinical practice guideline implementation strategies: a summary of systematic reviews by the NHLBI implementation science work groupCirculation20171359e122e137 28126839 10.1161/CIR.0000000000000481
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al.The PRISMA 2020 statement: an updated guideline for reporting systematic reviewsBMJ2021372n71 10.1136/bmj.n71 33782057 8005924