
Abstract
Background
The purpose of this study was to investigate the exposure of Belgian residents in urology, general surgery, and gynecology to laparoscopic surgery and to training of laparoscopic skills in dedicated training facilities.
Methods
Three similar specialty-specific questionnaires were used to interrogate trainees in urology, general surgery, and gynecology about their exposure to laparoscopic procedures, their acquired laparoscopic experience, training patterns, training facilities, and motivation. Residents were contacted via their Belgian specialist training organization, using Survey Monkey as an online survey tool. Data were analyzed with descriptive statistics.
Results
The global response rate was 58%. Only 28.8% of gynecology respondents, 26.9% of urology respondents, and 52.2% of general surgery respondents felt they would be able to perform laparoscopy once they had finished their training. A total 47% of urology respondents, 66.7% of general surgery respondents, and 69.2% of gynecology respondents had a surgical skills lab that included laparoscopy within their training hospital or university. Most training programs did not follow the current evidence about proficiency-based structured simulation training with deliberate practice.
Conclusion
Belgian resident training facilities for laparoscopic surgery should be optimized.
Introduction
For many gynecological, abdominal, and urological procedures, laparoscopy has replaced the open surgical approach. This minimally invasive technique offers many benefits to patients, in terms of cosmesis, postoperative pain, length of hospital stay, and return to daily activities.
The surgical competencies required to perform laparoscopic surgery are challenging and require surgical trainees go through an intensive learning period.Citation1 Medicolegal regulations, increasing patient expectations, and time constraints imposed by the European Working Time Directive make it increasingly difficult for trainees to learn these complex procedures on patients in theater. Furthermore, feedback on surgical performance has an important impact on the learning curve but is not always easy during laparoscopic surgery in theater.
Therefore, numerous training methods have been developed to supplement patient-related operating experience. Surgical simulation training in dedicated skills labs is one such method, which aims to teach trainees technical and nontechnical skills outside operating theater without compromising patient safety. Simulation training offers a safe environment for practice and error, opportunities for feedback, and assessment and standardized experience for trainees.Citation2 While simulation cannot completely replace clinical learning, the potential benefits of simulation training are widely recognized. Therefore, there is considerable interest in the implementation of surgical simulators in training programs as an adjunct to clinical learning.Citation3
Training in a simulation lab has shown to dramatically improve residents’ skills in the simulated environment.Citation4 The ultimate goal of a simulation program is to show transferability of these lab-acquired skills to the clinical setting, meaning that improvements in clinical operative performance can be objectively quantified after simulation training. Training until proficiency, distributed training, and deliberate practice all have shown to be important factors to gain most benefit out of a simulation program.Citation5–Citation8 Repeated studies have shown that a well-designed simulation training program has significant impact on the clinical learning curve.Citation9,Citation10
This survey focused on the implementation of structured training in minimally invasive surgery in Belgium, in urology, general surgery, and gynecology, and evaluated whether the current training curricula are evidence-based.
Material and methods
Questionnaire
A previously validated questionnaire about the current state of minimally invasive surgery training for general surgery residents in Canada was adapted for Belgian residents.Citation11,Citation12 This questionnaire has also been used for similar purposes in the Netherlands.Citation13 A few questions (eg, possibility for deliberate practice and training until proficiency) were added to check whether Belgian surgical education applies the current evidence-based principles about simulation training. Three similar questionnaires were developed for trainees in gynecology, general surgery, and urology. Only the questions about specialty-specific surgical procedures were different.
While Belgium has three official languages (Dutch, French, and German), all medical trainees are required to have a basic knowledge of English, and so the questionnaire was kept in its original language. Survey Monkey was used to design the questionnaire and gather data.
Respondents
Each specialty-specific questionnaire was presented to the specific specialty organization for residents: the European Society for Residents in Urology Belgium (ESRU.BE), the Belgian Association of Surgical Trainees (BAST), and the Flemish association for obstetrics and gynecology (Vlaamse Vereniging voor Obstetrie en Gynaecologie [VVOG]) for the Flemish (Dutch-speaking) gynecology trainees. There was no specific trainee organization for obstetrics and gynecology in Belgium.
As no specific ethical board existed for this kind of research, the questionnaire was discussed in detail within each trainee organization. None of the organizations had any ethical concerns. Residents were informed that they were not obliged to complete the questionnaire but that by filling in the survey, they gave consent to participation. They were assured that all data would be anonymized.
After agreement of ESRU.BE, BAST, and VVOG, each organization emailed the web link to the questionnaire to all its trainees. Together with this web link, an introduction to the questionnaire, informing the residents about the importance of the questionnaire for future training opportunities, was sent. Also, the concept of anonymity of the respondents was stated. Residents could only complete the questionnaire once because an internet protocol (IP)-lock was incorporated in the web link.
To maximize the response rate, two emails were sent with 2 months in between, and all the residents who completed the questionnaire could participate in a draw for an iPad mini.
The questionnaire addressed basic personal and practice demographics, laparoscopic training during residency, interest and performance of laparoscopy, laparoscopic simulation training, and factors influencing implementation of laparoscopy training in current residency. The complete questionnaire can be found in Supplementary material. For some questions, multiple answers were possible.
Data were reviewed and analyzed using standard descriptive statistics. Statistical analysis was performed using SPSS Statistics for Windows, Version 20.0 (IBM Corp, Armonk, NY, USA). Graphs were made with Prism 5 (GraphPad Software Inc., La Jolla, CA, USA).
Results
Demographics
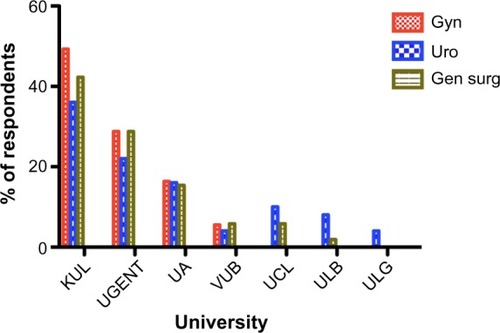
The questionnaire was emailed to 315 trainees. The global response rate was 58% (64% for urology trainees, 67% for general surgery trainees, and 51% for gynecology trainees). Mean age of the respondents was 27.9 years for general surgery trainees, 29.1 years for urology trainees, and 27.5 years for gynecology trainees. Among the respondents, 63.5%, 59.3%, and 12.3% were males in urology, general surgery, and gynecology, respectively. A total 32% of urology trainees were involved in a PhD program compared with 7.7% of general surgery trainees and 8.2% of gynecology trainees. shows the distribution according to the year of training, and shows the distribution according to the different Belgian universities.
Figure 1 Percentage of respondents over the different training years.
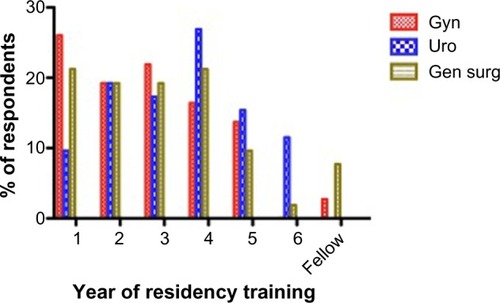
Figure 2 Distribution of respondents across the different Belgian universities.
Ready for practice
Only 28.8% of gynecology respondents, 26.9% of urology respondents, and 52.2% of general surgery respondents felt they would be able to perform laparoscopic surgery once they had finished their training program. Most of them reported they would need an extra laparoscopic fellowship once their residency was finished, to be able to perform advanced laparoscopic surgery (95.5%, 88%, 91% for gynecology, urology, and general surgery, respectively).
When taking a detailed look at the respondents who had laparoscopy in their career plan, only 16.7% felt prepared to perform laparoscopic procedures. In correspondence, 83.3% of them indicated they would need an extra fellowship to be able to perform advanced laparoscopic procedures.
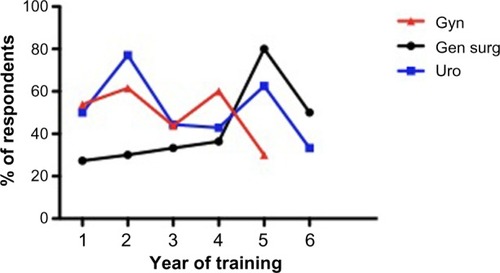
When asked whether they were ready for general practice within their specialization once their training program was finished, 50% of gynecology residents, 52% of urology residents, and 38% of general surgery residents gave a positive answer ().
Figure 3 Ready for general practice within their specialty at the end of their residency.
Skill labs
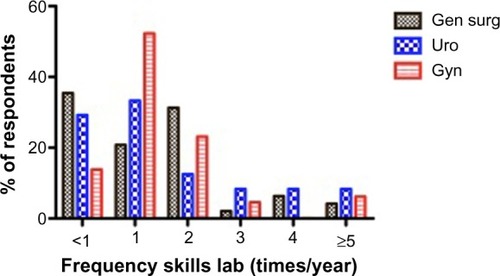
In all, 48% of urology respondents, 66.7% of general surgery respondents, and 69.2% of gynecology residents stated they had access to a laparoscopic skills lab in their training hospital or university. Surprisingly, they did not get to use that skills lab very often ().
Figure 4 Frequency of skills labs per year.
A total 47% of the urology trainees, 36.7% of general surgery, and 70.5% of gynecology trainees who only had the possibility of getting skills lab training reported that their performances were measured during training. In most cases, “time to complete an exercise” was the only performance measurement, except for gynecology trainees, among whom 5.5% reported the use of a procedure-specific score. A total 15% of urology trainees, 10.7% of general surgery trainees, and 37.2% of gynecology trainees had to reach a certain proficiency score on these exercises, but for none of the trainees was it necessary to reach a proficiency score to be able to perform laparoscopy in theater.
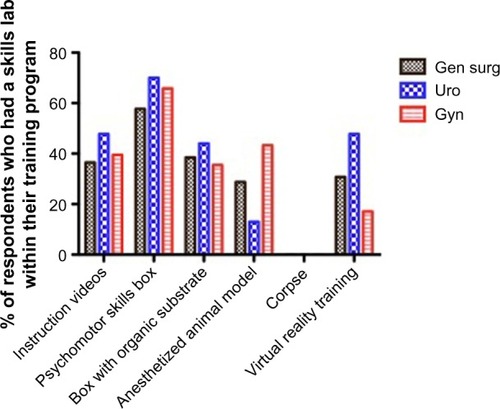
For most trainees, the duration of the skills labs was more than 1.5 hours, even up to a full day. Only a minority had training sessions between 30 minutes to 1.5 hours (). The distribution of exposure to different types of exercises for different specialties is shown in .
Figure 5 Duration of skills labs.
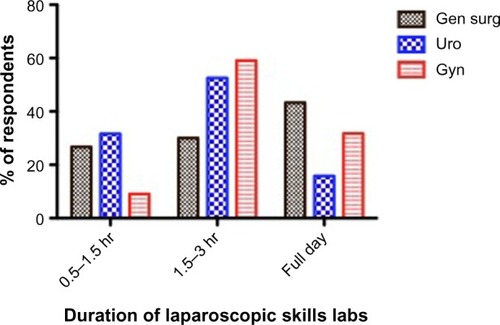
Figure 6 Types of exercises.
Most respondents (56.3% for general surgery, 50% for gynecology, 57.6% for urology) did not have any laparoscopy training before their residency started. About one-third of respondents (35.4% for general surgery, 31.3% for gynecology, and 33.3% for urology) had a short introduction course. Only a very small minority had a full course of several days with examination, but this in the context of a scientific study about laparoscopy training and simulation.
Nearly all trainees (except 5% of general surgery trainees) said that laparoscopic skills lab training was rather important or very important for their future career. Nearly all respondents said that the laparoscopic skills training they received was rather helpful or very helpful for their performance in the operating room (OR). For 5% of general surgery trainees and 2.3% of urology trainees, it made no difference.
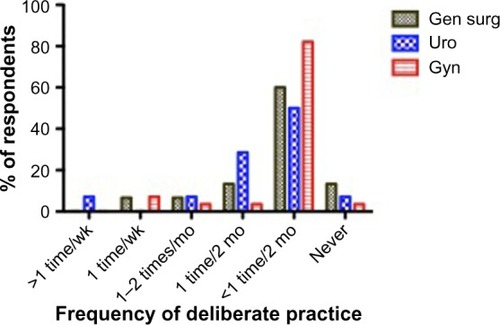
Only 26% of urology respondents, 28.8% of general surgery respondents, and 38.4% of gynecology respondents had the possibility of performing deliberate practice in their skills lab. However, of those who had the possibility of performing deliberate practice, the majority did not use that possibility very often (). The reasons mentioned for not going to the practice lab more often were (in order): lacking time to go to the lab, not enough exercises available, unpractical opening hours, or unpractical location.
Figure 7 Frequency of deliberate practice for those who had the possibility of performing deliberate practice.
In all, 26% of gynecology residents, 36% of general surgery residents, and 52% of urology residents received extra laparoscopy training not organized by their training program or university. All of the respondents who followed such an extracurricular course said this course was very helpful.
For all gynecology residents who followed an extracurricular course, this course was paid by the trainee him/herself, while for urology registrants, the course was paid for by industry or organized by the ESRU.BE and funded by industry. For all general surgery trainees, this extracurricular course was paid for by industry. Most extracurricular courses took place at the Research Institute against Digestive Cancer (Institut de Recherche Contre les Cancers de l’Appareil Digestif [IRCAD])/European Institute of TeleSurgery (EITS) in Strasbourg, France and were paid by industry (for 54% of urology trainees and 55.6% of general surgery trainees). None of the gynecology trainees followed a course in IRCAD. Some other mentioned centers were the International Centre for Endoscopic Surgery (Centre International de Chirurgie Endoscopique [CICE]) in Clermont-Ferrand France and the Endoscopic Training Centre Antwerp (ETCA) or Rotterdam Training Center, each named by two respondents. A total 28% of general surgery respondents took an extra course, paid for by industry, at the Centre for Surgical Technologies – KU Leuven. For 80% of gynecology trainees who took an extra course, this was also at the Centre for Surgical Technologies – KU Leuven.
None of the gynecology trainees, but 13.5% (seven) of urology trainees and 5.8% of general surgery trainees (three) said they had a personal training box at home; four of them never used this box, three of them did once a month, one did once a week, and the others did less than once every 2 months. Five of these seven students reported they did not use this home box more often because they did not have time; three of them said the camera quality was poor; three of them said that the instruments were poor; and one said there were not enough exercises available.
Training possibilities in the OR
For basic laparoscopic procedures among general surgery trainees during their first 3 years of training, nearly all trainees reported to have performed less than 25 laparoscopic appendectomies and less than 25 cholecystectomies. One third-year trainee had performed between 51 and 100 laparoscopic appendectomies and between 101 and 125 cholecystectomies. All fifth- and sixth-year trainees had performed more than 25 laparoscopic appendectomies and more than 25 lap cholecystectomies, and all of them felt comfortable performing these procedures on their own. A total 50% performed more than 100 laparoscopic cholecystectomies, and 50% performed less than 50.
Only 20.5% of urology trainees, 28.8% of general surgery trainees, and 25.9% of gynecology trainees reported there were enough training opportunities to learn advanced laparoscopy during their training. On a Likert scale between 1 and 5, they could point out the reason why they thought they had not learned enough advanced laparoscopy in theater. The summary is found in . summarizes advanced laparoscopic case experience at the end of the fifth and sixth training year (and fourth and fifth training year for gynecology), and shows which procedures residents believed they would be able to perform competently upon completion of their residency.
Table 1 Why did residents not get the chance to perform advanced laparoscopic cases?
Table 2 (Advanced) laparoscopic case experience at the end of the fifth and sixth training year (fourth and fifth for gynecology)
Table 3 Which of the following procedures will you be able to perform at the end of your training?
Discussion
Based on this survey, it is clear that laparoscopy training in Belgium should be improved.
Although a general response rate of 58% is not very high, respondents were evenly distributed across the different disciplines, years of training, and training university according to the Belgian situation. The VVOG sent the web link to their student members and recently graduated consultants, who were not allowed to complete the questionnaire, while the ESRU.BE and BAST, as resident organizations, only contacted the trainees. This incorrectly lowered the global response rate. For general surgery, the response rate (67%) was much better than for a previous questionnaire study in the same study population (26%).Citation14 For all these reasons, the current cohort is a very representative sample of urology, gynecology, and general surgery trainees in Belgium.
The vast majority of respondents are exposed to laparoscopic procedures although only a minority have the possibility to perform advanced laparoscopic procedures. As a result, most residents did not feel they would be comfortable to perform laparoscopic procedures by the end of their training. For gynecology trainees and general surgery trainees, residents were certain they would be able to perform basic laparoscopic procedures (diagnostic laparoscopy, tubal sterilization, appendectomy, and cholecystectomy). Compared with a similar study for general surgery residents in Belgium, in the current study, all final-year trainees performed more laparoscopic appendectomies and cholecystectomies, and all performed “enough” of both procedures, as was deemed necessary in that previous study.Citation14 However, also in the current study, most of the trainees did not have enough exposure to advanced laparoscopic cases. In urology, there are no basic laparoscopic procedures performed and an extensive learning curve for advanced procedures was reported.Citation15 Moreover, this translates into a lower urology cohort that felt able to perform urological laparoscopy at the end of their residency. A recent pan-European survey for training of European urology residents in laparoscopy also showed a similar cohort of only 23% of residents who stated they would have satisfactory laparoscopy skills at the end of their training.Citation16 A recent basic laparoscopic skills evaluation for European urology residents showed that even the level of basic laparoscopic skills in final-year residents is low.Citation17 In Canada, 33.9% of final-year residents performed more than 20 laparoscopic nephrectomies, and 68% performed more than ten.Citation18 None of the final-year urology trainees in Belgium said they had performed more than ten laparoscopic nephrectomies. This is an enormous difference. Are there not enough cases available, or do urology trainees lack laparoscopic skills? Probably both, but it is clear that only urology residents responded that the limited number of available cases appeared to be an important factor for why those residents thought their training opportunities were affected. Although most final-year residents did not perform more than ten laparoscopic nephrectomies during their residency, more than 50% of all urology trainees (first to sixth year) believed they would be able to perform a laparoscopic nephrectomy at the end of their residency. This stands in sharp contrast with the reported learning curves and underscores the significant gap between what residents initially expect from their training, on the one hand, and the limited number of procedures they will in reality be able to perform independently during their training, on the other hand. For general surgery trainees, perceived “end of training” laparoscopic abilities for most procedures are comparable with their Canadian counterparts. Belgian trainees felt more comfortable with bariatric surgery (45.9% vs 2.3%), while Canadian trainees felt more comfortable with laparoscopic sigmoid surgery (29.7% vs 52.3%).Citation11
Lack of theater time is one of the most frequently mentioned reasons explaining why residents thought they did not have enough opportunities to learn advanced laparoscopy. A recent Irish study showed that after the introduction of the European Working Time Directive, the reduction of working hours was accompanied by a decline in operative experience during residency.Citation20 Similar results were obtained in a previous British study.Citation19 Also for gynecology trainees, there appears to be a lack of surgical training.Citation21
The detrimental effects of lack of OR time can partially be overcome by offering laparoscopic simulation training.Citation22 The purpose of training outside theater is to provide residents with all the necessary basic skills to enable a “jump start” in theater so that more time can be spend focusing on the surgical procedure itself rather than on basic skill acquisition to perform the procedure.
Our study shows that about two-thirds of the trainees in gynecology and general surgery had the possibility of attending a laparoscopic simulation course in a dedicated skills lab related to their training center. For urology residents, this was only 47.9%. This is an enormous difference from a recent Canadian study, in which 85.7% of urology residents had access to a laparoscopic skills lab.Citation18 All our respondents reported the courses had a positive impact on their performance in the OR and a positive influence on their future career. However, when critically evaluating these courses, most of these courses were poorly designed. Firstly, the vast majority had the possibility of training only once a year or less in the simulation lab. Secondly, training sessions lasted more than 1.5 to 3 hours or even a full day. Various studies have shown the positive impact of more frequent, distributed, and shorter training sessions, and the lack of retained skills during longer training sessions.Citation5,Citation22 Thirdly, only a minority of trainees had to reach a certain proficiency score during training, and none of them had to obtain a proficiency score to be allowed to perform laparoscopy in theater. Proficiency-based training is a necessary component of an evidence-based simulation curriculum. This training allows for variation between students in the amount of training time and number of practice trials needed, while keeping mastery constant.Citation1 Stefanidis et al clearly showed that laparoscopic skill acquisition and transfer of simulation skills to the operating theater were better when those skills were learned in a proficiency-based training curriculum.Citation7,Citation23 Fourthly, only a very small minority had the possibility of performing deliberate practice. In addition, those who had access to deliberate training facilities report they rarely used that possibility due to lack of time, unpractical location, or lack of interest. This is a confirmation of earlier studies.Citation24,Citation25
When a preclinical proficiency-based laparoscopy course is given to medical students with an interest in a surgical career, deliberate practice was done intensively.Citation1 Furthermore, a preclinical proficiency-based course for medical students is easier to organize and has a positive impact on the real learning curve.Citation26
Many urology and general surgery trainees had a simulation course at an expensive international training center, offered by a medical company. Unfortunately, none of the gynecology trainees had the same opportunity. However, gynecology trainees received more training in animal labs at their local training center. Although it is beneficial for residents that the lack of structured simulation training in their core training programs can be compensated by industry-funded training courses, this creates ethical dilemmas and limits a resident’s independence. Also, the funding that industry is allowed to sponsor is diminishing. Furthermore, there is some controversy about the usefulness of short procedure-based courses taught by surgeons experienced in minimally invasive surgery.Citation27
Based on our finding, we formulate a number of suggestions to improve simulation training in Belgium. Of course we agree that resident organizations, together with specialty organizations, organize and coordinate industry-sponsored courses. But on its own, this is definitely not sufficient. Current educational evidence has to translate to the implementation of more laparoscopic simulators in all training hospitals. In 1999, this was also one of the important suggestions in the previous survey; however, most training centers still do not offer this possibility to their trainees.Citation14 Simulation boxes do not have to be expensive. Enough studies have shown that low-fidelity models are sufficient to acquire basic laparoscopic skills.Citation28–Citation30
Residents should also be encouraged to buy or construct a training system for training at home. Although our respondents who already had a training box at home were not that happy with their personal system, recent studies evaluated some promising examples.Citation31–Citation33 Further, performing deliberate distributed practice at home should be easier to fit into a resident’s schedule.
Adequate and efficient feedback, together with a minimum requirement for practice time, obligatory assessment, and corresponding consequences, should be set in order to stimulate residents to practice at home.Citation34 Moreover, proficiency scores should be communicated, and certification should be introduced. Residents should also be confronted with the results of surgical education research showing that only proficiency scores on the simulator correlate with improved clinical performance.
Surgical services are also increasingly organized into subspecialties. Subspecialty training and fellowships can be a good alternative for advanced laparoscopic procedures. A recent review showed the effectiveness of mentorship programs for advanced urological laparoscopy. Unfortunately, such programs are not widespread.Citation35 Also for general surgery, procedures like adrenal surgery, splenectomy, hepatic and pancreatic resection, and rectal surgery may be better reserved for subspecialty fellows. This also means that Belgian subspecialty training programs have to be developed further.
A concerning finding is that only half of the respondents felt ready to go out into general practice. As shown in , final-year trainees felt less prepared than did second-to-final-year trainees. It is possible that this has nothing to do with their available skills and knowledge, but more with being uncertain and afraid about upcoming responsibilities. A previous study also showed that the residents’ perceived degree of skills was lower than that actually assessed by their senior tutors.Citation36
Competency-based medical education with trustworthy professional activities and surgical portfolios will both help surgical trainers to identify those trainees who need more experience and will make trainees feel more comfortable about their gained experience.Citation37
Recently, a simple model for teaching and assisting residents, to guide faculty and resident interaction in the OR, and designating a resident’s earned level of autonomy for a given procedure, was developed.Citation38 Also, use of procedure-based assessments, undertaken on a regular basis when an index procedure is performed, will be interesting.Citation39 We propose these tools together with an online logbook or portfolio, to monitor resident’s autonomy for different procedures and to find out how to optimize surgical training for each resident personally. This opens an area for further research.Citation40
Author contributions
GDW selected and updated the survey questions, analyzed the data, and wrote the manuscript. WE helped optimize the questionnaire and revised the article critically for important intellectual content. DDR made substantial contributions to the conception of the study, helped perform the data analysis, and revised the article critically for important intellectual content. GP designed the online survey, helped gather all the data, and revised the article critically for important intellectual content. All authors gave final approval of the manuscript.
Acknowledgments
We express our great appreciation of the BAST, ESRU-BE, and VVOG, who agreed to collaborate and distributed the web link to the questionnaire to their residents. Special thanks to Pieter Uvin, François Legrand, Jan Bontinck, Lieven Depypere, and Marleen Parisis. Also, we thank all the residents who took the time to complete the questionnaire.
Disclosure
DDR is on the advisory board of Astellas, Bard, Medtronic, Apogepha, Allergan, and AMS, but these companies are not involved in the topic of this manuscript. The authors report no other conflicts of interest in this work.
References
- De WinGVan BruwaeneSAllenCDe RidderDDesign and implementation of a proficiency-based, structured endoscopy course for medical students applying for a surgical specialtyAdv Med Educ Pract2013410311523901308
- PalterVNGrantcharovTPSimulation in surgical educationCMAJ2010182111191119620351120
- SchoutBMHendrikxAJScheeleFBemelmansBLScherpbierAJValidation and implementation of surgical simulators: a critical review of present, past, and futureSurg Endosc201024353654619633886
- ZendejasBBrydgesRHamstraSJCookDAState of the evidence on simulation-based training for laparoscopic surgery: a systematic reviewAnn Surg2013257458659323407298
- De WinGVan BruwaeneSDe RidderDMiserezMThe optimal frequency of endoscopic skill labs for training and skill retention on suturing: a randomized controlled trialJ Surg Educ201370338439323618450
- KorndorfferJRDunneJBSierraRStefanidisDTouchardCLScottDJSimulator training for laparoscopic suturing using performance goals translates to the operating roomJ Am Coll Surg20052011232915978440
- StefanidisDAckerCHenifordBTProficiency-based laparoscopic simulator training leads to improved operating room skill that is resistant to decaySurg Innov2008151697318387999
- CrochetPAggarwalRDubbSSDeliberate practice on a virtual reality laparoscopic simulator enhances the quality of surgical technical skillsAnn Surg201125361216122221516035
- PalterVNOrzechNReznickRKGrantcharovTPValidation of a structured training and assessment curriculum for technical skill acquisition in minimally invasive surgery: a randomized controlled trialAnn Surg2013257222423023013806
- De WinGVan BruwaeneSVan CalsterBDe RidderDMiserezMAn evidence based laparoscopic simulation curriculum shortens the clinical learning curve and reduces surgical complicationsBr J Surg2015102Suppl 119
- QureshiAVergisAJimenezCMIS training in Canada: a national survey of general surgery residentsSurg Endosc20112593057306521512882
- ChiassonPMPaceDESchlachtaCMMamazzaJPoulinECMinimally invasive surgery training in Canada: a survey of general surgerySurg Endosc200317337137712436233
- SchijvenMPBerlageJTJakimowiczJJMinimal-access surgery training in the Netherlands: a survey among residents-in-training for general surgerySurg Endosc200418121805181415809795
- NavezBPenninckxFLaparoscopic training: results of a Belgian survey in trainees. Belgian Group for Endoscopic Surgery (BGES)Acta Chir Belg1999992535810352732
- AbboudiHKhanMSGuruKALearning curves for urological procedures: a systematic reviewBJU Int2014114461762924053179
- FurrielFTLagunaMPFigueiredoAJNunesPTRassweilerJJTraining of European urology residents in laparoscopy: results of a pan-European surveyBJU Int201311281223122824053711
- BrinkmanWMTjiamIMSchoutBMResults of the European Basic Laparoscopic Urological Skills examinationEur Urol201465249049624231256
- PrestonMABlewBDBreauRHBeikoDOakeSJWattersonJDSurvey of senior resident training in urologic laparoscopy, robotics and endourology surgery in CanadaCan Urol Assoc J201041424620165577
- BlencoweNSParsonsBAHollowoodADEffects of changing work patterns on general surgical training over the last decadePostgrad Med J201187103479579921984742
- BreenKJHoganAMMealyKThe detrimental impact of the implementation of the European working time directive (EWTD) on surgical senior house officer (SHO) operative experienceIr J Med Sci2013182338338723288473
- MossELBredakiFEJonesPWHollingworthJLuesleyDMChanKKIs gynaecological surgical training a cause for concern?: a questionnaire survey of trainees and trainersBMC Med Educ2011113221668984
- MackaySMorganPDattaVChangADarziAPractice distribution in procedural skills training: a randomized controlled trialSurg Endosc200216695796112163963
- StefanidisDKorndorfferJRSierraRTouchardCDunneJBScottDJSkill retention following proficiency-based laparoscopic simulator trainingSurgery2005138216517016153423
- ChangLPetrosJHessDTRotondiCBabineauTJIntegrating simulation into a surgical residency program: is voluntary participation effective?Surg Endosc200721341842117180282
- van DongenKWvan der WalWARinkesIHSchijvenMPBroedersIAVirtual reality training for endoscopic surgery: voluntary or obligatory?Surg Endosc200822366466717704889
- De WinGVan BruwaeneSAggarwalRLaparoscopy training in surgical education: the utility of incorporating a structured preclinical laparoscopy course into the traditional apprenticeship methodJ Surg Educ201370559660524016370
- RogersDAElsteinASBordageGImproving continuing medical education for surgical techniques: applying the lessons learned in the first decade of minimal access surgeryAnn Surg2001233215916611176120
- TanSCMarlowNFieldJA randomized crossover trial examining low-versus high-fidelity simulation in basic laparoscopic skills trainingSurg Endosc201226113207321422648100
- MatsumotoEDHamstraSJRadomskiSBCusimanoMDThe effect of bench model fidelity on endourological skills: a randomized controlled studyJ Urol200216731243124711832706
- BergDAMilnerREFisherCAGoldbergAJDempseyDTGrewalHA cost-effective approach to establishing a surgical skills laboratorySurgery2007142571272117981192
- KorndorfferJRBellowsCFTekianAHarrisIBDowningSMEffective home laparoscopic simulation training: a preliminary evaluation of an improved training paradigmAm J Surg201220311722172481
- KielyDJStephansonKRossSAssessing image quality of low-cost laparoscopic box trainers: options for residents training at homeSimul Healthc20116529229821613971
- BahsounANMalikMMAhmedKEl-HageOJayePDasguptaPTablet based simulation provides a new solution to accessing laparoscopic skills trainingJ Surg Educ201370116116323337687
- van EmpelPJVerdamMGStrypetMVoluntary autonomous simulator based training in minimally invasive surgery, residents’ compliance and reflectionJ Surg Educ201269456457022677599
- HayDKhanMSVan PoppelHCurrent status and effectiveness of mentorship programmes in urology – A systematic reviewBJU Int Epub2272014
- YapSADeLairSMTanakaSTKurzrockEACurrent perceptions of resident training in laparoscopic nephrectomyUrology20097351067107119394507
- Ten CateOCompetency-based education, entrustable professional activities, and the power of languageJ Grad Med Educ2013516724404218
- DaRosaDAZwischenbergerJBMeyersonSLA theory-based model for teaching and assessing residents in the operating roomJ Surg Educ2013701243023337666
- BeardJDMarriottJPurdieHCrossleyJAssessing the surgical skills of trainees in the operating theatre: a prospective observational study of the methodologyHealth Technol Assess2011151ixxi121227024
- PeerarGVan HumbeeckBDe LeynPThe development of an electronic portfolio for postgraduate surgical training in FlandersActa Chir Belg2015