
Abstract
Background
Evidently, complementary and alternative medicine (CAM) is a recognized medical practice that efficiently uses multiple treatment therapies and techniques in the prevention and management of a variety of human disorders. Many medical schools have integrated CAM curriculum in medical education system worldwide. Research in knowledge, attitude, and practice (KAP) of diverse health professionals exposed to CAM courses is important from many perspectives including improvement in KAP and teaching skills of faculty, together with capacity building and curriculum development.
Objective and setting
This pre- and post-design cross-sectional study aimed to assess CAM-KAP of two intakes of medical students in Majmaah University, Saudi Arabia.
Methods
The second-year medical students of the first (year 2012–2013) and second (year 2013–2014) intake (n=26 and 39, respectively) were selected for this study. A reliable, 16-item self-administered questionnaire was distributed among all the students for answering before and after the 48-hour CAM course. The data were analyzed using appropriate statistical test of significance.
Results
Medical students’ knowledge and attitude toward CAM significantly improved across some subitems of CAM questionnaire with a positive trend in the rest of its items including their views on CAM practices.
Conclusion
CAM course tends to have a positive impact on KAP of medical students. The preliminary results of this study call for further research with a larger sample in academic settings across the nation.
Introduction
Non-allopathic medical systems have diverse intervention approaches directed toward balancing mind–body–spirit dimension of a whole person with or without disease.Citation1,Citation2 The holistic concept is an ideal principle underlying traditional medical systems/integrative medicine (IM), which include ayurveda, naturopathy and yoga, unani medicine and homeopathy, traditional Chinese and Japanese medicine, and prophetic medicine.Citation3–Citation5 Traditional treatments were used effectively in innumerable diseases since ancient times and continued to survive and flourish, although research in holistic system approaches remained poorly organized.Citation6 However, over the past few decades, research including randomized clinical trials, systematic reviews, meta-analyses, and observational studies into complementary and alternative medicine (CAM) is beginning to reveal empirically the underlying mechanisms of actions and effectiveness of traditional treatment modalities in various diseases,Citation7–Citation11 which accordingly are cost-effective and efficient with minor adverse effects comparable to placebo.Citation12,Citation13 In US, in the year 2007, adults (age over 18) spent $33.9 billion out-of-pocket on visits to CAM practitioners and purchases of CAM products, classes, and materials.Citation14 In another report, Davis and Weeks estimated that over 30 million adults reported out-of-pocket expenditures on CAM services, and of these individuals, 7.2 million were heavy CAM spenders with a mean annual expenditure of $1,385, thus suggesting that out-of-pocket spending on CAM is concentrated.Citation15 A large number of surveys conducted worldwide also evidenced the emerging popularity of CAM use, either adjunctive or alternative, in acute and chronic human diseases, attributable to a variety of plausible reasons including patients’ dissatisfaction with severe adverse effects and high costs of allopathic medications.Citation16,Citation17 Approximately 40% of adults and approximately 11.8% of children had used CAM therapies in the past 12 months in US.Citation16 Furthermore, World Health Organization estimated that approximately 75% of the world’s health care is technically alternative.Citation13 The use of CAM is reported to be more common in poor population and underserved communities of the world.Citation18
In the eastern world, the bedrock of traditional medicine, many traditional medical schools and national centers of CAM were established long time back to meet the increasing demand of health consumers and health providers, to regulate CAM practices with a focus on research and training, and similar developmental trends driven by policy statements of influential bodiesCitation19,Citation20 have been rapidly emerging in the western world.Citation21 Notably, despite several observed challenges and barriers including curriculum being already too full, the resistance by faculty, relative lack of evidence-based CAM contents, unavailability of reliable resources, and development of teaching and assessment tools,Citation22,Citation23 CAM curriculum is increasingly incorporated in many universities of the world to teach medical students about CAM practices, as an elective or mandatory course.Citation24,Citation25 How medical students and professionals perceive CAM and also how they develop their related knowledge base and practice is relatively an old avenue for research in eastern world, although western world has produced huge data on this particular perspective over a few decades.Citation26
Local landscape of CAM
Notably, there is scant literature on knowledge, attitude, and practice (KAP) of CAM among medical students, professionals, and public in eastern Mediterranean region countries. A PubMed search of relevant literature using key word complementary and alternative medicine retrieved a dozen of articles;Citation27–Citation39 however, only few studies assessed the KAP of public, professionals, primary care physicians, and pharmacists.Citation27,Citation30–Citation32,Citation36 The results of these studies suggest that CAM therapies, especially herb preparations and locally known therapies are used by a substantial number of patients, and public and professionals have positive attitudes toward CAM, identified some barriers against CAM, and have good knowledge in CAM, and further express to have more knowledge in CAM and support its integration into primary health careCitation27,Citation30–Citation32,Citation36 and medical schools.Citation39 We found only one study from Kuwait that assessed KAP of CAM therapies among medical and pharmacy students.Citation36 Therefore, this team conducted a KAP study among medical undergraduate students of Majmaah University in the KSA.
Rationale
Over the last 100 years, biomedicine, mainly represented by pharmaceutical industries and phyto-pharmaceuticals, has consistently utilized medications effectively for acute injuries, infectious diseases, and a variety of chronic, noninfectious diseases.Citation17,Citation40 However, a proportion of patients, due to multiple biopsychosocial and cultural reasons, do not use conventional medications and prefer traditional therapies, including herbal products.Citation13,Citation16,Citation18,Citation41,Citation42 In addition, chronic patients do not respond to conventional medications and develop serious adverse effects and other complications that also drive them to seek other forms of CAM treatments.Citation2,Citation17–Citation19 Several surveys have reported the increasing use of traditional therapies by patients and population at large, the latter group use for health promotion, good quality of life, and prevention purposes.Citation13,Citation17,Citation18 Like traditional practitioners, conventional doctors began to use frequently traditional therapies in their practice.Citation43 Notably, several international health organizations and research institutions supported the use of and research and training on traditional therapies across the world.Citation19,Citation20 Furthermore, many medical schools and universities integrated CAM curriculum into their medical education system in the western world.Citation21,Citation24,Citation25 This is to impart required theoretical and empirical knowledge in CAM to medical students and prepare them to practice effectively and efficiently IM in future. All these driving forces were important determinants for adopting CAM curriculum for teaching medical students in Majmaah University. This study assesses the impact of pre- and post-CAM course on attitudes, knowledge, and experience of two intakes of second-year medical students in Majmaah University. Another important rationale is that this CAM course may be adopted by other universities in KSA and Arabian Gulf countries.
Significance
Besides improving KAP of CAM therapies among medical students, the students’ feedback about this course will help curriculum developers to further align it with students’ expressed needs in CAM course. Medical students exposed to CAM course may practice as CAM doctors and also take up advanced studies in IM in future. By extension, they may also disseminate gained CAM information to the community with whom they have frequent discussions at several leisure places in KSA.
Hypothesis
We hypothesize that the exposure of medical students to CAM course will improve their KAP of CAM.
Materials and methods
Setting
The Majmaah University was established in accordance with a decree of the Custodian of the Two Holy Mosques King Abdullah Bin Abdul Aziz Al-Saud and the Prime Minister and Chairman of Higher Education on Ramadan 3, 1430H corresponding to August 24, 2009G. The name of Majmaah University is derived from Majmaah Governorate, located 180 km north of Riyadh city. Majmaah University serves five provinces, which have several cities and villages, and their total population is approximately 250,000. The University’s main campus is located in the south part of Majmaah City. The total area of Majmaah province is 30,000 km2. The Majmaah University is the value-added icon to the people of the region in social, cultural, research, and education pathways. A separate royal decree vide number 194/A and dated ZulHejjah 30, 1430 corresponding to October 17, 2009G was issued to appoint its rector with higher rank to accelerate the establishment of this University. According to the rector, Majmaah University, a beacon of advanced knowledge and enlightenment, shall offer high-quality education to prospective students in the region.Citation44
Study design, sample, and data collection
This cross-sectional study has pre- and post-design. Medical undergraduates of second year from first intake (n=26) of year 2012–2013 and second intake (n=39) of year 2013–2014 were selected for this study. Two students from first intake and three students from intake 2 joined the course late and could not fill out pretest questionnaire. So they were excluded from this study, and the total number of students in the sample was 65, whose pre- and posttest responses were available. Prior to filling out the questionnaire, the participating students were informed the following: the team will be conducting a survey of attitudes, awareness, and self-perceived skills in CAM use, and the participants’ input will be used to construct future CAM educational programs for students and residents, and allied health professionals. The research team will maintain the participants’ anonymity and confidentiality. The survey will never be associated with any information that could identify the participants personally. Only aggregated data of intake 1 and intake 2 from the survey will be reported. As there are no right or wrong answers to any item, the participants must respond to each item according to how they feel about CAM at that point in time. Participation in this study is voluntary. The participants may decide not to complete this survey at any time without penalty. Completion of this survey indicates their consent to participate.
Thereafter, a self-administered questionnaire was given to all participants in a classroom, and they were advised to fill it out before beginning the CAM class. They were guided that if they do not understand any item on the questionnaire, they should feel free to contact one of the team members supervising administration of this questionnaire. All questionnaires were collected and checked carefully for their completeness. If there was any item on the questionnaire unanswered, then that particular student was contacted to complete it before leaving the classroom. Subsequently, the students were taught CAM course longitudinally, and thereafter, they were given the same questionnaire for filling out. They were asked to completely fill out the questionnaire. All questionnaires were collected and checked carefully for their completeness. The specific details of the CAM curriculum and questionnaire are summarized in the following sections.
CAM training course
The Department of Community Medicine of College of Medicine, Majmaah University in collaboration with National Center of Complementary and Alternative Medicine (NCCAM), Ministry of Health, Riyadh developed a comprehensive course on CAM for the academic year 2013–2014. The module title and code of this course are CAM and MEDU 230, respectively. The credit hours for this mandatory course were 2 (2 + 0 + 0) hours, and module duration was 48 hours. Module commencement was in the sixth semester. There were one module coordinator, one associate coordinator, and two module members. Furthermore, 20 module teachers included faculty and NCCAM staff. All teachers have either MD/PhD (17) or MBBS (3) degrees. This module was approved by a number of committees and departments of Majmaah University. This course mainly focused on an overview of CAM and most commonly used CAM modalities worldwide, in addition to CAM therapies in vogue locally. However, all teachers were requested to provide information on their topics and discuss the following competency-based areas, such as basic definitions of CAM and IM, history, epidemiological trends, common clinical indicators and applications, adverse effects and drug–drug interactions, research-based evidence for efficacy, resources for comprehensive CAM information, and training standards for CAM practitioners.Citation45–Citation47
This course proposed CAM teaching in terms of mandatory module, core curriculum lectures, and inclusion in problem-based learning at undergraduate and residency level, and later on followed by continuing education modules as well as research and clinical fellowship. The aims of this module are as follows: to improve future doctors’ knowledge in CAM practices and their place in health care system, to build their communication skills to guide patients about CAM modalities and its credentials and legal and regulatory issues, to develop search skills and critical appraisal of relevant literature related to CAM, to evaluate evidence for the safety and efficiency of CAM techniques, and to develop deeper understanding regarding its integration into conventional medical system – IM. By the end of the module, students should be able to learn the following: 1) to define CAM and related names and terminologies and their differences in meanings (A); 2) to classify CAM modalities and types (A); 3) to identify common CAM practices patients use in the KSA such as Arabic and Islamic traditional healing practices (A, B, D); 4) to computer search for relevant CAM literature and critical appraisal for finding evidence, efficacy, safety, and adverse effects of CAM modalities (E); 5) to identify CAM therapies to which diseases are most responsive (B, C); 6) to develop communication skills to discuss CAM practices with patients (B, D); and 7) to identify the role of NCCAM as a national reference for all CAM-related issues such as practice, regulations, and accreditation (A, B, E). These learning outcomes of five levels were described as follows: A – scientific in their approach to practice, B – proficient in clinical care, C – professional, D – community conscious, and E – scholar. This module contains 13 contents/topics, five seminars together with a field visit to CAM clinic in King Khalid Military Hospital in Hafr El-Baten, and an assignment, each of which is described briefly in this module (available upon request from AM Al-Bedah). All teachers adopted a number of teaching methods; interactive lecturers and assigned students conducted seminar sessions/ presentations using developed guidelines. Each student was advised to submit a report within a week about CAM from evidence to integration assignment, which should be based on a critical appraisal of a paper related to CAM discussing its PICO (population, patient, problem, intervention, comparison and outcome) and quality. Similarly, each student was asked to submit a report about his experience and observations during field visit to the King Khalid Military Hospital. Besides, students were provided reading materials including textbooks and CAM journals. The whole idea of teaching CAM course interactively was that students must participate actively in presentation and discussion and help develop guidelines for seminar sessions and should not sit in the class as passive spectators and consequently develop meaningful knowledge, favorable attitude, and usage of CAM therapies and comprehend its connectivity to biomedical model. The duration of lectures and exams were as follows: each interactive lecture (n=13, each of 2 hours), student-led seminar and assignment (n=6, each of 2 hours), field visit (n=1, 6 hours), midterm exam (n=1, 2 hours), and final exam (n=1, of 2 hours), so the grand total duration of lectures and two examinations was 48 hours.
CAM questionnaire
We searched relevant international literature for identifying questionnaires used in CAM-KAP research in general but especially pre- and post-surveys related to CAM and IM.Citation3,Citation17,Citation48–Citation50 From these researches, we selected an evaluation tool that was used in two surveys.Citation17,Citation50 This validated questionnaire is about CAM survey of knowledge and attitudes of health professional students originated from Kreitzer’s University of Minnesota Academic Health Center and has been used subsequently in many studies.Citation17,Citation50 The questionnaire used in the present study was adapted following suggestions of three CAM experts, two faculty staff, and some second-year medical students. Accordingly in first round, the research team simplified the English wordings of some items and subitems of this questionnaire. This modified questionnaire was pretested on 15 medical students before its application. Students provided no suggestions for any significant changes in the questionnaire. Notably, all components of this questionnaire were retained, which include the following: 1) general attitudes toward CAM; 2) barriers to use CAM practices worldwide; 3) what primary worldview or framework guides people’s personal health views; 4) CAM approaches – “alternative” or mainstream?; 5) effectiveness of CAM modalities; 6) CAM training received by participants; 7) need of further CAM training; 8) personal use of CAM; 9) CAM approaches in participants’ practice; 10) sources of information about CAM; 11) evidence for use of CAM practices; 12) views about CAM as a practitioner; 13) a female case of seasonal allergy and choice of CAM therapies; 14) in a case of acute appendicitis, which CAM therapies are most effective; 15) influence of various factors on people’s response to several approaches to health care, and 16) people’s views about health and healing. Additional questions included were as follows: 1/17) Do you believe that your spiritual or religious beliefs influence your attitudes toward CAM? 2/18) Describe a CAM training you have had. 3/19) Overall comments on CAM practices or education. For items 1, 2, 5, 8, 12, 15, and 16, the research team used five-point Likert scale (strongly agree, agree, neutral, disagree, and strongly disagree) for rating participants’ responses, and some items – 4, 6, 7, 9, and 11 were rated by using four-point Likert scale. The Likert scale was not used to rate medical students’ responses related to items 3, 10, 13, and 14 and three added questions of this tool. We used Likert scale because open-ended questionnaires are filled out completely compared to closed-ended questionnaires.Citation51 The sociodemographic data included only age of participants, and no female student was enrolled in Majmaah University at the time of this study. We have used only these items – 1–3, 10, 12, 15–19 – of this questionnaire in this study as the emitted items do not address specifically individual CAM approach (a second paper addressing the rest of items is forthcoming soon).
Data analysis
The recorded responses on pre- and post-course questionnaires were entered into the computer. The SPSS version 21 was used to analyze the data. Pretest data related to first (n=26) and second (n=39) intakes of medical students were merged, and similarly, posttest data of two intakes were also merged. Participants’ strongly agree and agree and strongly disagree and disagree responses were pooled for analysis purpose. Their neutral responses were considered as such. Missing responses were merged with disagree responses. Besides frequency distribution, we used 3×2 and 2×2 contingency tables for comparing data. Nonparametric χ2 test was used for comparing pre- (Group 1) and posttest (Group 2) responses of medical students. P-value ≤0.05 was considered significant.
Ethical considerations
The research protocol was submitted to the ethics committee of the NCCAM, Riyadh and Majmaah University, and both committees approved the protocol. The Institutional Review Board number is NCCAM-5 vide dated 6.2.1435H corresponding to Gregorian December 10, 2013.
Results
General attitudes toward CAM
The mean age of participants was 21.13±0.97 (range =7, minimum and maximum age =20 and 27, respectively). Medical students’ general attitudes toward CAM revealed the following statistically significant results when their pre- and posttest responses were compared (): 1) participants disagreed that CAM is a threat to public health (χ2=6.46, df=2, P=0.039); 2) according to medical students’ views, health care providers should be able to advise their patients about commonly used CAM therapies (χ2=7.69, df=2, P=0.013); and 3) they opined that CAM practices need to be included in their medical school curriculum (χ2=7.52, df=2, P=0.023). However, the rest of pre- and posttest responses related to other questions did change in the direction of favorable attitudes but without statistical significance.
Table 1 General attitudes toward CAM
Barriers against CAM use
According to participants’ perceptions, several significant barriers to CAM use in western world were medical school concerns about legal problems (χ2=13.75, df=2, P=0.001), lack of both competent CAM providers (χ2=14.64, df=2, P=0.0006) and appropriate equipment (χ2=9.04, df=2, P=0.011), and being too time consuming (χ2=5.998, df=2, P=0.049) (). As regards other barriers including lack of evidence for practices, lack of staff training, and lack of reimbursement, there was a trend in the direction of agree responses with no statistical significance.
Table 2 Barriers to use of CAM practices in western medical settings
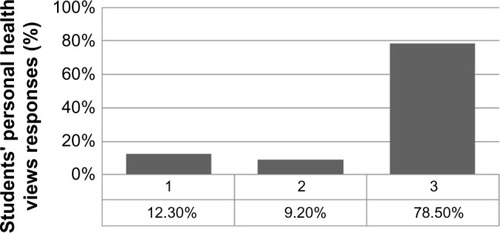
Health worldview/framework and personal health views
In response to what primary worldview or framework guides their personal health views, majority of participants (78.5%) informed that combination of western biomedicine and traditional Chinese medicine directs their health understandings ().
Figure 1 Distribution of students’ primary worldview or framework guides by their personal health views (pretest responses only).
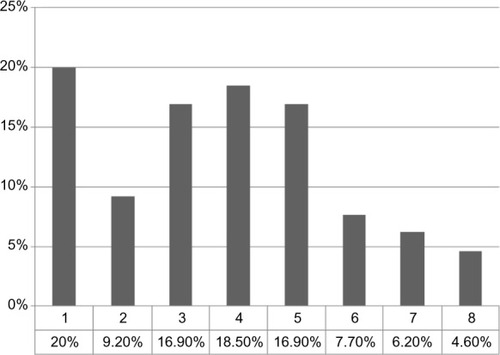
Sources of CAM information
The participants observed that their most important sources of CAM information were peer professionals, scientific journals, mass media, and Internet ().
Figure 2 Distribution of students’ sources of information about CAM (pretest responses only).
Abbreviation: CAM, complementary and alternative medicine.
Views about CAM as a practitioner
Medical practitioners tend to have variable views regarding use of CAM therapies (). According to this survey, participants’ responses to question number 1, 5, 9, 12, 14, and 16 () were statistically significant between their pre- and posttest views. Students disagreed that it is ethical for practitioners to advise CAM therapies to patients that involve the use of subtle energy fields in and around the body for medical purposes (χ2=9.53, df=2, P=0.0085). They also strongly disagreed with the statement that it is irresponsible for practitioners to recommend acupuncture to patients with conditions like chemotherapy-related nausea and vomiting or headache (χ2=9.28, df=2, P=0.0096). Furthermore, participants agreed strongly that patients whose practitioners are knowledgeable of multiple medical systems and CAM practices, in addition to conventional medicine, do better than those whose practitioners are only familiar with conventional medicine (χ2=6.19, df=2, P=0.045). Students’ response rate increased significantly posttest regarding improved outcomes associated with strong relationship between patient and practitioner, a kind of therapeutic intervention (χ2=9.32, df=2, P=0.009). Furthermore, medical students agreed significantly that counseling on nutrition by a physician is associated with the prevention of chronic diseases (χ2=8.158, df=2, P=0.016). Medical students viewed that delivery of better care to patients is strongly associated with those practitioners who strive to understand themselves than those who do not (χ2=7.259, df=2, P=0.0265). Students’ responses related to the rest of questions improved positively but without achieving statistical significance.
Table 3 Statements relate to views you may have as a practitioner
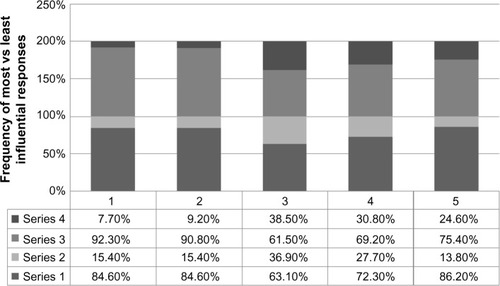
Health care pathways
When participants’ responses to which of the following components influence, the most or the least, to health care approaches were analyzed, none of them was significantly associated with health care models: spiritual and religious beliefs (χ2=1.88, df=1, P=0.169), knowledge of CAM (χ2=1.14, df=1, P=0.285), cultural values (χ2=0.033, df=1, P=0.856), personal experience (χ2=0.148, df=1, P=0.669), and research and evidence (χ2=2.426, df=1, P=0.119) ().
Figure 3 Comparison of contribution to participants’ pre-(series 1 and 2) and posttest (series 3 and 4) (most vs least influential, respectively) responses by five approaches to health care.
Abbreviation: CAM, complementary and alternative medicine.
Public views about health and healing
People’s views about health and healing were significantly supported by student participants in the following areas (): connectivity between social stress and development of physical diseases (χ2=12.255, df=2, P=0.0022), reasonable discussion with patients about their health is associated with improvement in patients’ health (χ2=7.515, df=2, P=0.0233), and practitioners’ time voluntarily spent in serving underserved communities (χ2=7.004, df=2, P=0.0301). With regard to other health and healing areas, there was a favorable trend but without achieving statistical significance.
Table 4 Statement of people’s views about health and healing
Participants’ responses to additional questions
In response to three additional questions, the participants reported the following (a mix of pre- and post-exposure): 1) Spiritual and religious beliefs are integral part of complementary and alternative therapies, and hence, there needs to be special focus on the cultural belief system when faculty is in the process of developing CAM curriculum and teaching and instructing on such topics of great significance to the medical students and the community. 2) None of the participants had formal training in CAM in the past, but they reported to have frequent discussion on local CAM products among community members, and therefore, they suggested that teaching of CAM therapies must involve global view in general but local context in particular with regulation of CAM practices supported by legislation. 3) At global level, the use of CAM modalities is on the rise, and simultaneously, practitioners frequently encounter patients who take both CAM and modern medications, and thus, all medical schools should integrate CAM course in their curriculum in Saudi Arabia and other Gulf countries. These summarized views of participants reverberate with the perceptions of medical students, allied students, and professionals around the world.Citation1,Citation2,Citation17,Citation21,Citation24,Citation25,Citation27,Citation28,Citation43
Discussion
According to this study, the participants reported that CAM is not a threat to public health, reflecting a positive attitude toward CAM practices,Citation10 but this finding is inconsistent with other researchers.Citation17 Generally, CAM treatment modalities are safe; there are potential dangers in special circumstances.Citation13 Though costs of CAM therapies are not explored in this study, there is converging evidence that they are highly cost-effective and cost saving, and therefore, the treatment costs are relatively low.Citation12,Citation13 Therefore, the CAM modalities and health systems are easily accessible to public health needs at a macro social levelCitation52 including poor patients and underserved communities who are unlikely to pay high costs of modern medications.Citation53 Furthermore, medical students supported the notion that physicians should be able to advise their patients about commonly used CAM therapies, drug interactions, and efficacy issues consistent with other studies.Citation46 In the Saudi context, the commonly used and supported CAM therapies include cupping (hijama), cautery, recitation from holy Quran, acupuncture, herbal preparations, apitherapy (use of honey and bee products), camel urine, aromatherapy, massage, biofeedback, therapeutic touch, and exercise, although there are many forms of CAM interventions used worldwide.Citation1–Citation5,Citation7–Citation9 Notably, most of medical students expressed that CAM course needs to be integrated into their medical school curriculum, and this trend is consistent with other studies.Citation8,Citation54,Citation55 The long-term implications of this finding are many, including CAM capacity building in relation to clinical practice, research, teaching, and training.
According to many studies, the barriers against integration of CAM curriculum and use of CAM therapies exist across the world.Citation22,Citation23,Citation56 In the context of western medical settings, the present study reported a number of barriers, including legal issues raised by medical schools and institutions, relative lack of competent CAM providers, lack of appropriate equipment, and CAM therapies being too time consuming, and these findings are compatible with other western studies.Citation22,Citation23,Citation57 According to this research, although other barriers including lack of evidence for practices, lack of staff training, and lack of reimbursement did not achieve statistically significant association with participants’ views, there were identifiable trends in the direction of agree responses expressed by medical students. Notably, these barriers are commonly reported in other studies.Citation22,Citation23,Citation37,Citation57 It is questionable whether or not similar barriers against use of CAM interventions apply to Saudi medical settings because participants’ responses relate to western medical settings. A review of relevant literature in Arabian Gulf countries found some studies that addressed multiple perspectives of CAM therapies, but only few discussed the issue of barriers against the use of CAM modalities.Citation37 The research team suggests that KAP studies should also include exploration of barriers against use of CAM therapies in Middle East countries including KSA.
Besides two frameworks that guide personal health development and its understanding, another worldview is a hybrid model, IM, which focuses on a holistic approachCitation58 that benefits patients and promotes health of the population. According to this research, most medical students observed that integrated medical system guides their personal health views, which is consistent with other studies.Citation58,Citation59 Integrated medicine approaches are used in the management of patients who present with diverse, chronic diseases and health problems.Citation60 The present study quite rightly supported the integrated model of care associated with better outcomes and good quality of life.Citation58 Medical students tend to collect information on CAM from multiple sources as revealed in this study. Accordingly, medical students reported that their most important sources of CAM information were peers, scientific journals, media, and Internet, and these results are partially consistent with other reports.Citation30 Predictably, this CAM info-source scenario would change in future when CAM course will be integrated into main curriculum of all medical schools in KSA.
According to this survey, medical students reported variable views regarding use of CAM therapies. Students strongly disagreed with the statement that it is ethical for practitioners to advise CAM therapies to patients that especially involve the use of subtle energy fields in and around the body for medical purposes, which is incompatible with international dataCitation61 could be attributed to lack of knowledge in biomagnetic field therapies. Healing touch, therapeutic touch (biomagnetic touch), massage, Yoga, moxibustion, laser acupuncture, homeopathy, and Reiki are some of the CAM modalities that use the concept of energy biofields in ameliorating various diseases.Citation62,Citation63 These CAM therapies initially met ethics and regulatory challenges,Citation64 but this scenario is substantially changed. CAM therapies used worldwide are now supported by guidelines.Citation16,Citation65,Citation66 Though energy medicine has its proponents and opponents, the relevant energy biomagnetic therapies are increasingly recognized with evidence-based data to be used in a variety of diseases with better outcome.Citation61–Citation63 The participants also strongly disagreed with the statement that it is irresponsible for practitioners to recommend acupuncture to patients with conditions like chemotherapy-related nausea and vomiting or headache, and this is compatible with other international randomized controlled trials and systematic reviews.Citation67 Acupuncture, in its different invasive and noninvasive forms including laser acupuncture, is recommended either as an adjunct or as an alternative in various conditions including chemotherapy-induced nausea and vomiting, headache, migraine, low back pain, and also in anesthesia practice.Citation68,Citation69
According to this survey, majority of participants agreed that patients whose practitioners have knowledge in multiple medical systems, CAM practices, and conventional medicine do better than those whose practitioners are only familiar with conventional medicine, and this view matches with international studies.Citation8,Citation17 In another way, physicians with vast medical knowledge and multiple skills could discuss with the patient a variety of disease-related issues and put forward more than one option to be accepted, the best one, by the patient, that would fit into patient-centered approach currently in vogue in CAM/IM.Citation70–Citation72 In the similar vein, medical students also attested to the fact that the improved outcome is strongly associated with professional relationship between patient and practitioner, which is considered a kind of therapeutic intervention.Citation73 Literature suggests that the development and sustainment of healthy rapport with patient throughout the process of treatment and based on effective communication is an ideal philosophy that underlies good adherence, better outcome, and improved quality of life of health consumers.Citation74,Citation75 Currently, nutrition has achieved an exceptional place in CAM therapies, mainly for cancer survivors.Citation76,Citation77 In line with this therapeutic development, medical students agreed significantly that counseling on nutrition by a physician is associated with the prevention of chronic diseases. Consequently, nutrition counselors need to be available in medical settings at all levels. Dietary tips matching with needed lifestyle changes and chronic care model guidelines are the core intervention issues in the prevention of chronic diseases, related complications, disabilities, and mortality.Citation76–Citation78 Medical students viewed that delivery of better care to patients is strongly associated with those practitioners who themselves strive to understand than those who do not, which is supported by other researchers.Citation79 The self-evaluation done by using self-evaluation tools, and negatively associated with stress and mediated by orientation to goals,Citation80 is reported to provide insights into one’s competency gaps, that is, strengths and weaknesses, and consequently, practitioners need to improve their knowledge, clinical practice, research scholarship, and teaching and training skills.Citation79,Citation81 As a result, practitioners tend to not only improve their practice considerably but also provide benefit to patients who would otherwise opt for better health care. A note of caution is that physician’s ability to self-assess is mostly inaccurate, and external assessment is preferred.Citation79
Notably, participants’ individual health pathways in terms of spiritual and religious beliefs, knowledge of CAM, cultural values, personal experience, and research and evidence did not contribute significantly to various approaches to health care, which is inconsistent with other studies.Citation82–Citation87 Notably, these approaches may collectively guide health care models; however, not supporting exclusively individual approach by medical students in this study is in line with the concept of multimodal/multifaceted strategyCitation79,Citation88 in the prevention, management, and rehabilitation of patient with simple-to-complex diseases such as chronic pain, cancers, functional bowel disorders, stroke, and depressionCitation53,Citation89–Citation92 and in surgical applications.Citation93
People at large have different views about health and healing, which is a program of IM.Citation82,Citation86 According to this research, medical students supported the notion that social stress is related to the development of physical (and psychological) diseases.Citation94 Evidently, overwhelming or aggregated stress over a period of time is reported to cause homeostatic changes in the body, ultimately leading to psychological and physical conditions, which are relieved by stress management methods and other CAM therapies including stress-coping strategies and provision of social supports.Citation94,Citation95 Patients’ involvement (including caretakers and public) in discussion and shared decision making about their treatment on long- and short-term bases, a recent trend and based on research evidence, is associated with improvement in patients’ health, knowledge/literacy, well-being and satisfaction, adherence, and outcome with good quality of life,Citation96,Citation97 and this view of people is also supported by the participants of the present study. This autonomous ideology, ethically sound, gives patients complete control on their health and health-related perspectives.Citation96–Citation98 The public demands that practitioners should voluntarily spend some time (4 hours per week) in serving underserved communities is also evidenced in this study, which invigorates morality and altruistic attitude of physicians and also helps not only in promoting the health of the poor population but also lessen their financial burden.Citation99
Limitations
There are several significant limitations to this cross-sectional research. There were many statistically negative results but with positive trends in KAP of medical students in this survey. However, this means that after gaining some knowledge, medical students formed favorable attitude toward CAM practice. The research team suggests that in future, besides further simplifying questionnaire, teachers should focus additionally on those areas of CAM-KAP, which were not significantly changed following exposure of Majmaah University medical students to CAM course. This is a survey of second-year male medical students in one university, and hence, its results are not generalizable to female medical students and other universities in KSA. As regards female medical students’ attitude toward CAM, inconsistent findings were reported across transatlantic countries,Citation100–Citation102 and researchers called for further intersex KAP studies on CAM. Similarly, the results may not be applicable to other health professionals such as nursing or dental students and third-, fourth-, or fifth-year students as their KAP tend to differ from first- and second-year students.Citation8,Citation49,Citation73 First-year students, especially female, are reported to show more interest in, positive attitude toward, and personal use of CAM than second-/third-year studentsCitation8,Citation17,Citation49,Citation73,Citation103 attributed to cohort effectCitation73 and continuing exposure to orthodox medical training.Citation49 We did not use any other test of significance because pre- and posttest data of individual participant were not aligned and individual participant’s anonymity was preserved on pre- and posttest questionnaire. Overall, the preliminary results of this research should be interpreted cautiously. The strength of this study is that 100% of students filled out the questionnaire. Also, this survey makes some sense of Majmaah University medical students’ responses regarding their improved general attitude, knowledge, and practice views about CAM, and possibly, their improved KAP of CAM may persist over the years of medical training.Citation3
Conclusion
In summary, the preliminary findings of this survey are partially compatible with international data on medical students’ KAP of CAM modalities, and CAM course tends to have positive impact on KAP of medical students of Majmaah University.
Author contributions
Abdullah MN Al-Bedah and Mohammed Othman Al-Rukban conceptualized the paper design. Naseem Akhtar Qureshi, Mohammed Abdullah Al Mansour, Mohamed KM Khalil, Ibrahim S Elsubai, Elsadiq Yousif Mohamed, Khalid Altohami Medani, Waqas Sami Mahmoud, Ahmed Tawfik El Olemy, Asim AH Khalil, Abdullah Almudaiheem, and Meshari Saleh Alqaed made the literature search and helped in analyzing the data. Naseem Akhtar Qureshi drafted the paper and all authors critically revised it a number of times.
Acknowledgments
The NCCAM supported this study. College of Medicine, Majmaah University distributed the questionnaires to two intakes of second-year medical students, collected the data, and entered in the computer for analysis. Teachers affiliated to NCCAM and Majmaah University developed CAM curriculum and delivered the course to medical students.
Disclosure
The authors report no conflicts of interest in this work.
References
- KarffSERecognizing the mind/body/spirit connection in medical careVirtual Mentor2009111078879223206945
- HaylockPJAdvanced cancer: a mind-body-spirit approach to life and livingSemin Oncol Nurs201026318319420656142
- LieDABokerJComparative survey of complementary and alternative medicine (CAM) attitudes, use, and information-seeking behaviour among medical students, residents and facultyBMC Med Educ200665817156463
- QureshiNAAl-BedahAMMood disorders and complementary and alternative therapiesNeuropsychiatr Dis Treat2013963965823700366
- UjalaVRashmiSPankajGSamtaGBhuvneshvarKAllopathic vs ayurveda practices in tertiary care institutes of urban North IndiaInd J Pharmacol2007395254
- ChiappelliFProloPCajulisOSEvidence-based research in complementary and alternative medicine I: historyEvid Based Complement Alternat Med20052445345816322801
- CramerHLaucheRDobosGCharacteristics of randomized controlled trials of yoga: a bibliometric analysisBMC Complement Altern Med20141432825183419
- AkanHIzbirakGKasparECKnowledge and attitudes towards complementary and alternative medicine among medical students in TurkeyBMC Complement Altern Med20121211522862993
- BusseJWKulkarniAVBadwallPGuyattGHAttitudes towards fibromyalgia: a survey of Canadian chiropractic, naturopathic, physical therapy and occupational therapy studentsBMC Complement Altern Med200882418513441
- AdrianFClareMGMedical students’ attitudes towards complementary and alternative medicineJ Complement Altern Med200392275284
- LiuJPeiMZhengCA systems-pharmacology analysis of herbal medicines used in health improvement treatment: predicting potential new drugs and targetsEvid Based Complement Alternat Med2013201317
- HermanPMPoindexterBLWittCMWittCMEisenbergDMAre complementary therapies and integrative care cost-effective? A systematic review of economic evaluationsBMJ20122e001046
- WHO News: New alternative medicine guide launched amidst increasing reports of adverse reactionsBull World Health Org2004828635636
- NahinRLBarnesPMStussmanBJBloomBCosts of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States,2007Natl Health Stat Report20091811419771719
- DavisMAWeeksWBThe concentration of out-of-pocket expenditures on complementary and alternative medicine in the United StatesAltern Ther Health Med201218364222894889
- BarnesPMBloomBNahinRLComplementary and alternative medicine use among adults and children: United States, 2007Natl Health Stat Report20081212319361005
- Halterman-CoxMSierpinaVSSadoskiMSandersCCAM attitudes in first- and second-year medical students: a pre-and post-test course surveyIntegr Med2009763442
- WolskoPWareLKutnerJAlternative/complementary medicine:wider usage than generally appreciatedJ Altern Compelent Med20006321326
- Institute of Medicine of the National AcademiesComplementary and Alternative Medicinein the United StatesWashington, DCNational Academies Press2005
- Education and Training of Health Care Practitioners. The WhiteHouse Commission on Complementary and Alternative Medicine Policy2015 Available from: http://www.whccamp.hhs.gov/fr4.htmlAccessed January 2, 2015
- BrokawJJTunnicliffGRaessBUSaxonDWThe teaching of complementary and alternative medicine in US medical schools: a survey of course directorsAcad Med200277987688112228082
- SierpinaVSSchneeweissRFrenkelMABulikRMaypoleJBarriers, strategies, and lessons learned from complementary and alternative medicine curricular initiativesAcad Med2007821094695017895653
- FrenkelMAryeEBThe growing need to teach about complementary and alternative medicine; questions and challengesAcad Med20017625125411242575
- LevineSMWeber-LevineMLMayberryRMComplementary and alternative medicalpractices: training, experience, and attitudes of a primary care medical schoolfacultyJ Am Board Fam Pract200316431832612949033
- BhattacharyaBPrograms in the United States with complementary and alternative medical education opportunities: an ongoing listingJ Altern Compl Med200067790 CarlstonMThe revolution in medical education: complementary medicine joins the curriculumHealthcare Forum J19984162529
- ChaterjiRTractenbergREAmriHLumpkinMAmorosiSBHaramatiAA largesamplesurvey of first- and second-year medical student attitudes toward complementaryand alternative medicine in the curriculum and in practiceAltern Ther Health Med2007131303517283739
- ElolemyATAl-BedahAMNPublic knowledge, attitude and practice of complementary and alternative medicine in Riyadh region, Saudi ArabiaOman Med J201227202622359720
- Al-RowaisNMohammadAGAl-RukbanMAbdulghaniHMTraditional healers in Riyadh region: reasons and health problems for seeking their advice. A household surveyJ Altern Complement Med20101619920420105037
- Al-ZahimAAAl-MalkiNYAl-AbdulkarimFMAl-SofayanSAAbunabHAAbdoAAUse of alternative medicine by Saudi liver disease patients attending a tertiary care center: prevalence and attitudesSaudi J Gastroenterol201319758023481133
- Al-BedahAMNElolemyATKhalilMKMKnowledgeand attitude of health professionalsin Riyadh region, Saudi Arabia, toward complementary and alternative medicineJ Family Community Med2012192939922870412
- Abdullah Al-RowaisNAl BedahAMKhalilMKKnowledge and attitudes of primary care physicians towards complementary and alternative medicine in the Riyadh region, Saudi ArabiaForsch Komplement Med201219712
- Al-BedahAMKhalilMKElolemyATThe use of and out-of-pocket spending on complementary and alternative medicine in Qassim province, Saudi ArabiaAnn Saudi Med201333328228923793433
- JaziehARAl SudairyRAbulkhairOUse of complementary and alternative medicine by patients with cancer in Saudi ArabiaJ Altern Complement Med201218111045104922906212
- GadAAl-FarisEAl-RowaisNAl-RukbanMUse of complementary and alternative medicine for children: a parents’ perspectiveComplement Ther Med201321549650024050586
- Al-FarisEAAl-RowaisNMohamedAGPrevalence and pattern of alternative medicine use:the results of a household surveyAnn Saudi Med20082841018299652
- AlkharfyKMCommunity pharmacists’ knowledge, attitudes and practices towards herbal remedies in Riyadh, Saudi ArabiaEast Mediterr Health J201016998899321218728
- AwadAIAl-AjmiSWaheediMAKnowledge, perceptions and attitudes toward complementary and alternative therapies among Kuwaiti medical and pharmacy studentsMed Princ Pract201221435035422377503
- AllamSMoharamMAlarfajGAssessing patients’ preference for integrating herbal medicine within primary care services in Saudi ArabiaJ Evid Based Complement Altern Med2014193205210
- Al-RukbanMOAlBedahAMKhalilMKEl-OlemyATKhalilAAAlrasheidMHStatus of complementary and alternative medicine in the curricula of health colleges in Saudi ArabiaComplement Ther Med201220533433922863648
- SubhoseVSrinivasPNarayanaABasic principles of pharmaceutical science in ayurvedaBull Indian Inst Hist Med Hyderabad200535839217333665
- TilburtJCKaptchukTJHerbal Medicine Research and Global Health: An Ethical AnalysisBull WHO Available from: http://www.who.int/bulletin/volumes/86/8/07-042820/en/Accessed January 6, 2015
- GogtayNJBhattHADalviSSKshirsagarNAThe use and safety of non-allopathic Indian medicinesDrug Safety2002251005101912408732
- GawdeSRShettyYCPawarDBKnowledge, attitude, and practices toward ayurvedic medicine use among allopathic resident doctors: a cross-sectional study at a tertiary care hospital in IndiaPerspect Clin Res20134317518024010059
- Majmaah University, Saudi Arabia2014 Available from: http://mu.edu.sa/en/about/historyAccessed December 15, 2014
- KliglerBKoithanMMaizesVCompetency-based evaluation tools for integrative medicine training in family medicine residency: a pilot studyBMC Med Educ20077717442108
- PearsonNJChesneyMAThe CAM education program of the national center for complementary and alternative medicine: an overviewAcad Med2007821092192617895649
- LeeMYBennRWimsattLIntegrating complementary and alternative medicine instruction into health professions education: organizational and instructional strategiesAcad Med2007821093994517895652
- SchneiderCDMeekPMBellIRDevelopment and validation of IMAQ: integrative medicine attitude questionnaireBMC Med Educ20033512946276
- FurnhamAMcGillCMedical students’ attitudes about complementary and alternative medicineJ Altern Complement Med20039227528412804081
- KreitzerMJMittenDHarrisIShandelingJAttitudes toward CAM among medical, nursing, and pharmacy faculty and students: a comparative analysisAltern Ther Health Med2002864447505312440838
- GriffithLECookDJGuyattGHCharlesCAComparison of open and closed questionnaire formats in obtaining demographic information from Canadian general internistsJ Clin Epidemiol199952997100510513763
- GaleNThe sociology of traditional, complementary and alternative medicineSociol Compass20148680582225177359
- BazarganMAniCOHindmanDWCorrelates of complementary and alternative medicine utilization in depressed, underserved African American and Hispanic patients in primary care settingsJ Altern Complement Med200814553754418537468
- YildirimYParlarSEyigorSAn analysis of nursing and medical students’ attitudes towards and knowledge of complementary and alternative medicine (CAM)JCN2010191157116620492061
- AlisOGanimeSNuranBMumtazMMNazanBIsikBAn analysis of nursing and medical students’ attitudes towards and knowledge of complementary and alternative medicine (CAM)J Altern Complement Med20071391007101018047448
- FonfaAEPatient perspectives: barriers to complementary and alternative medicine therapies create problems for patients and survivorsIntegr Cancer Ther20076329730017761643
- YeoASYeoJCYeoCLeeCHLimLFLeeTLPerceptions of complementary and alternative medicine amongst medical students in Singapore – a surveyAcupunct Med2005231192615844436
- KatherineKWhat is Integrative Medicine? Experts Explore New Ways to Treat the Mind, Body, And spirit – All at the Same Time2015 Available from: http://www.webmd.com/a-to-z-guides/features/alternative-medicine-integrative-medicineAccessed January 1, 2015
- AgbajeEOBabatundeEOA KAP study of the attitude and practice of traditional medicine in contemporary Nigerian communityCent Afr J Med2005515–6586217432433
- TamWWSWongELYWongFCYCheungAWLCitation classics in the integrative and complementary medicine literature: 50 frequently cited articlesEur J Integr Med201241e77e83
- JainSMillsPJBiofield therapies: helpful or full of hype? A best evidence synthesisInt J Behav Med20101711619856109
- EdenDFeinsteinDThe Basic Grid Booklet2015 Available from: http://innersource.net/em/images/downloads/pdf_files/Basic_Grid_Booklet-feb-2014.pdfAccessed January 12, 2015
- AndersonJGTaylorAGEffects of healing touch in clinical practice: a systematic review of randomized clinical trialsJ Holist Nurs201129322122821228402
- ErnstECohenMHStoneJEthical problems arising in evidence based complementary and alternative medicineJ Med Ethics20043015615915082809
- CAMDOCModel Guidelines for the Practice of Complementary Therapies (CAM) by Medical Doctors in the European Union2015 Available from: http://www.camdoc.eu/Pdf/Model%20Guidelines%20CAM%20Practice.pdfAccessed January 10, 2015
- NCCAMClinical Practice Guidelines2015 Available from: http://nccam.nih.gov/health/providers/clinicalpractice.htmAccessed January 7, 2015
- LeeAFanLTYStimulation of the wrist acupuncture point P6for preventing postoperative nausea and vomitingCochrane Database Syst Rev20093CD003281
- LeeAChanSAcupuncture and anaesthesiaBest Pract Res Clin Anaesthesiol200620230331416850779
- WangSMHarrisRELinYCGanTJAcupuncture in 21st century anesthesia: is there a needle in the Haystack?Pain Med20131166
- SchollIZillJMHarterMDirmaierJAn integrative model of patient-centeredness – a systematic review and concept analysisPLoS One201499e10782825229640
- SaundersPATractenbergREChaterjiRPromoting self-awareness and reflection through an experiential mind-body skills course for first year medical studentsMed Teach200729877878417852720
- ElderWRakelDHeitkemperMUsing complementary and alternative medicine curricular elements to foster medical student self-awarenessAcad Med2007821095195517895654
- DeSylviaDStuberMFungCCBazargan-HejaziSCooperEThe knowledge, attitudes and usage of complementary and alternative medicine of medical studentsEvid Based Complement Altern Med201120115
- Bakić-MirićNMBakićNMSuccessful doctor-patient communication and rapport building as the key skills of medical practiceMed Biol20081527479
- GolinCEThorpeCDiMatteoMRAccessing the Patient’s World – Patient-Physician Communication about Psychosocial Issues2015 Available from: www.jblearning.com/samples/0763749613/49613_CH07.pdfAccessed January 10, 2015
- DixonSNutrition in complementary and alternative medicineSemin Oncol Nurs2012281758422281312
- WhayneTFJrMaulikNNutrition and the healthy heart with an exercise boostCan J Physiol Pharmacol201290896797622812658
- WagnerEHAustinBTDavisCHindmarshMSchaeferJBonomiAImproving chronic illness care: translating evidence into actionHealth Aff20012066478
- DavisDAMazmanianPEFordisMVan HarrisonRThorpeKEPerrierLAccuracy of physician self-assessment compared with observed measures of competenceJAMA200629691094110216954489
- MorrisMLMessalCBMeriacJPCore self-evaluation and goal orientation: understanding work stressHuman Res Dev Q2013243562
- AAPAPhysician Assistant’s Competencies: A Self-Evaluation Tool Available from: http://www.nccpa.net/pdfs/competencies%20Self%20Evaluation%20Tool.pdfAccessed January 9, 2015
- RumunAJInfluence of religious beliefs on healthcare practiceInt J Educ Res2014243748
- Campinha-BacoteJThe process of cultural competence in the delivery of healthcare services: a model of careJ Transcult Nurs20021318118412113146
- EntwistleVAFranceEFWykeSHow information about other people’s personal experiences can help with healthcare decision-making: a qualitative studyPatient Educ Couns2011853e291e29821652162
- SackettDLRosenbergWMCGrayJAMHaynesRBRichardsonWSEvidence based medicine: what it is and what it isn’tBMJ199631271728555924
- PuchalskiCMPostSGSloanRPPhysicians and patients’ spiritualityVirtual Mentor2009111080481523206948
- JohnsonMBBertrandSWFermonBColemanJFPathways to healing: person-centered responses to complementary servicesGlob Adv Health Med20143181624753990
- KehletHMultimodal approach to postoperative recoveryCurr Opin Crit Care200915435535819617822
- RosenbergEIGenaoIChenIComplementary and alternative medicine use by primary care patients with chronic painPain Med2008981065107218564996
- MaoJJPalmerSCStratonJBCancer survivors with unmet needs were more likely to use complementary and alternative medicineJ Cancer Surviv20082211612418648980
- van TilburgMALPalssonOSLevyRLComplementary and alternative medicine use and cost in functional bowel disorders: a six month prospective study in a large HMOBMC Complement Altern Med200884618652682
- ShahSHEngelhardtROvbiageleBPatterns of complementary and alternative medicine use among United States stroke survivorsJ Neurolog Sci20082711–2180185
- FleckensteinJBaeumlerPIGurschlerCAcupuncture for post anaesthetic recovery and postoperative pain: study protocol for a randomised controlled trialTrials20141529225047046
- ThoitsPAStress and health: major findings and policy implicationsJ Hlth Social Behavior201051SS41S53
- AdliMUrban Stress and Mental Health2015 Available from: http://files.lsecities.net/files/2011/11/2011_chw_4030_Adli.pdfAccessed January 12, 2015
- JoostenEADeFuentes-MerillasLde WeertGHSenskyTvan der StaakCPde JongCASystematic review of the effects of shared decision-making on patient satisfaction, treatment adherence, and health statusPsychother Psychosom20087721922618418028
- WilsonSRStrubPBuistASBetter Outcomes of Asthma Treatment (BOAT) Study GroupShared treatment decision making improves adherence and outcomes in poorly controlled asthmaAm J Respir Crit Care Med201018156657720019345
- CoulterAParsonsSAskhamJWhere are the Patients Indecision-Making About Their Own Care?2015 Available from: http://www.who.int/management/general/decisionmaking/WhereArePatientsin-DecisionMaking.pdfAccessed January 14, 2015
- GoldsteinAOCallesonDCurtisPCommunity service by North Carolina family physiciansJ Am Board Fam Pract200518485615709064
- SmithBWDalenJWigginsKTChristopherPJBernardJFShelleyBMWho is willing to use complementary and alternative medicineExplore2008435936718984547
- ChezRAJonasWBCrawfordCA survey of medical students’ opinions about complementary and alternative medicineAm J Obstet Gynecol2001185375475711568810
- GreenfieldSMBrownRDawlatlySLReynoldsJARobertsSDawlatlyRJGender differences among medical students in attitudes to learning about complementary and alternative medicineComplement Therapies Med2006143207212
- GreenfieldSMInnesMAAllanTFWearnAMFirst year medical students’ perceptions and use of complementary and alternative medicineComplement Therapies Med20021012732